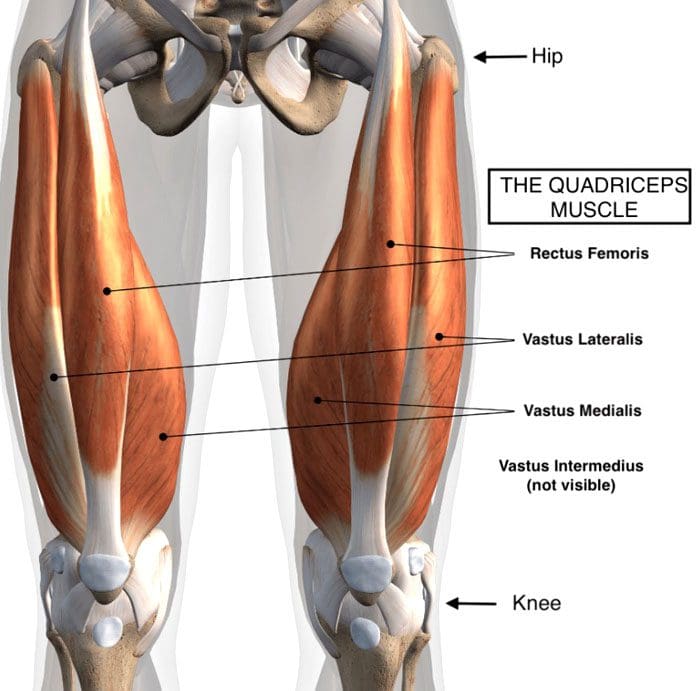
The quadriceps muscle consists of four muscles in front of the thigh that connects to the knee right below the knee cap. These muscles straighten the knee for walking, running, and jumping. They also help bend the knee for squatting. They move the leg forward when running and fire/transmit electrical impulses when the foot hits the ground to absorb shock. When jumping, the muscles provide stability coming down as well as when standing on one leg.
Quadriceps Strain
Thigh strains are common in sports. Most players are sidelined because of this injury when compared to strains in the hamstrings or groin. Factors that can increase the risk of injury include:
Exhaustion
Muscle weakness
The strength of the quadriceps to the hamstrings is uneven, causing one set to get overused.
Consistent sprinting and/or kicking
Previous strain and/or injury
The quadriceps is made up of four muscles. One is the rectus femoris, which gets injured the most. It’s the only muscle that crosses two joints – the hip joint and the knee joint.
Symptoms and Injury Grades
Individuals commonly report a pulling/stretching sensation in the front of the thigh. Common symptoms include:
Pain
Swelling
Bruising
Muscle tenderness
For minor quadriceps strains or tears, moderate to dull pain presents along with stiff movement.
Grades categorize the severity of the strain:
Grade 1 presents with mild discomfort in the thigh with no loss of strength.
Grade 2 presents with moderate pain, swelling, and some loss of strength.
Grade 3 is a complete rupture of the fibers. Individuals are in severe pain and unable to walk.
Grade 3 is where surgery is required.
Symptoms can vary depending on the type of injury that has been sustained and the severity. There is pain and localized swelling for both strains and contusions. If a muscle rupture has happened, there could be a bump/lump within the muscle or a gap in the muscle. If rupture of the Quadriceps Tendon has occurred, individuals often report hearing a pop when the injury happens. The swelling often makes straightening the leg difficult or impossible.
Injury causes
Thigh strains usually happen when slowing down/decelerating after a sprint. This can be because the individual takes too small or too large steps causing the muscles to overstretch, much like a rubber band that, if overstretched, tears, and if under stretched, it bunches up, which can cause spasms and tears.
Treatment
In the initial stages after a quadriceps strain, it is recommended to follow the RICE Procedure for 24 hours: This includes:
Rest
Ice
Compression
Elevate
The leg needs to be rested every 2-3 hours in 20-minute sessions.
A bandage can provide added support.
For slight tears and strains, it is recommended to stretch the quadriceps gently.
This helps prevent the muscles from experiencing shortening. This happens by the formation of scar tissue that pulls the muscle/s, making them shorter.
Gentle stretches allow the muscles to heal with minimal shortening. This helps prevent further and/or re-injury.
Chiropractic Physical Therapy Rehabilitation
After the acute stage of the injury, receiving regular chiropractic sports adjustments, physical therapy massage, coupled with strength training exercises will speed up recovery.
Physical therapy massage will remove scar tissue and keep the muscle/s loose and flexible.
Exercises for strengthening the muscles after injury will be recommended according to the individual’s condition/case.
Following correct post-injury-care, exercises, and physical therapy.
Healing time can be 4- 6 weeks.
Body Composition
Strength Training: The Inverted Row
This workout targets the back muscles, spine and scapular stabilizers, deep abdominals, and arms. Everyday activities that require various types of pulling motion, lifting, etc., become easier. To perform:
Lie flat on your back.
Grab a stable barbell or set of straps that are above you.
Pull your upper body up as high as possible while keeping the back straight.
Squeeze the shoulder blades together at the top.
Complete as many reps as possible.
Once enough strength and endurance have been built, try a pullup.
References
Kary, Joel M. “Diagnosis and management of quadriceps strains and contusions.” Current reviews in musculoskeletal medicine vol. 3,1-4 26-31. 30 Jul. 2010, doi:10.1007/s12178-010-9064-5
Hillermann, Bernd, et al. “A pilot study comparing the effects of spinal manipulative therapy with those of extra-spinal manipulative therapy on quadriceps muscle strength.” Journal of manipulative and physiological therapeutics vol. 29,2 (2006): 145-9. doi:10.1016/j.jmpt.2005.12.003
Wenban, Adrian B. “Influence of active release technique on quadriceps inhibition and strength: a pilot study.” Journal of manipulative and physiological therapeutics vol. 28,1 (2005): 73. doi:10.1016/j.jmpt.2004.12.015
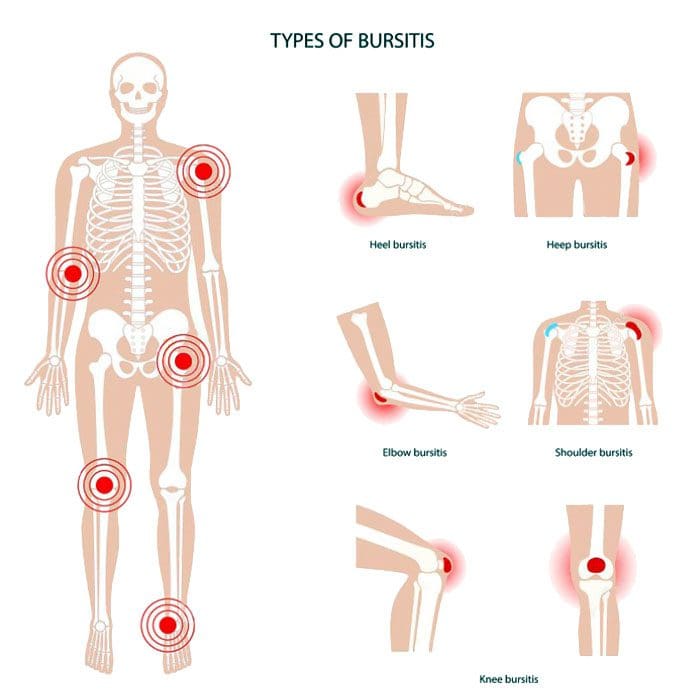
Bursitis types: This is a condition that affects the bursae, which are the small, fluid-filled sacs that provide cushion for the:
Muscles
Tendons
Bones near joints
The bursae make it easier for tissues to slide over each other. The body has around one hundred and sixty bursae. However, only a few become clinically affected. These include the:
Wrist
Elbow
Shoulder
Hips
Knees
The base of the big toe and heel
The condition typically presents near joints constantly being used repetitively, like a job, sports, house/yard chores, etc. What happens is one or more of the bursae sacs become inflamed, resulting in pain.
Causes
Inflamed or irritated bursae typically cause it from overuse or intense/vigorous activity.
It can also be caused by bacterial infection.
Arthritis and gout can also cause bursitis.
Another cause is age.
As tendons age, they can tear easily, lose their elasticity, and can’t take too much stress.
Intense physical activities can lead to bursitis. These include:
Gardening
Typing
Working with a computer mouse
Throwing
Golf
Tennis
Manual tasks
Carpentry
These types of activities can lead to incorrect posture, overuse, and injury/damage.
Symptoms
The main symptom is pain in and around the affected area that worsens with movement. Depending on the severity of the strain and the length of time it has been going on, the pain can be intense with active and passive movements. Other symptoms include:
Tenderness
Stiffness
For some individuals, it can present as acute, with the intensity increasing.
This happens when movement aggravates the condition.
Bursitis Types
Four major types include:
Prepatellar
Trochanteric
Olecranon
Retrocalcaneal
Prepatellar Bursitis
Prepatellar is an inflammation of the sac situated between the skin and the patella/kneecap. The most common causes are trauma from a fall and direct pressure/friction from repetitive kneeling. This is one of the bursitis types that can get infected. Overproduction of liquid places pressure on the other areas of the knee, causing swelling. Most individuals report swelling and knee pain just over the front of the knee.
Trochanteric Bursitis
This bursitis type goes over the lateral area of the hip. There is a distinctive tenderness and aching pain. This type is more common for individuals with arthritis conditions and fibromyalgia. This condition is also seen after surgery, mainly osteotomies. The bursa can become inflamed in case of injury or overuse. It tends to affect middle-aged or older folks. Common causes include:
Muscle tears
Hip injuries
Tight hip or leg muscles
Disc disease of the low back
Leg-length inequality
Improper walking technique from a minor injury or strain
Overuse of the gluteal muscles
Flat feet
Improper footwear
Olecranon Bursitis
Olecranon is a common bursitis type. It is diagnosed by the appearance of swelling over the elbow. The swelling happens just behind the olecranon process of the ulna. The bursa can become infected. This bursitis does cause blood to rupture out, and fluid could be present. Individuals are advised to avoid leaning or resting on the elbows.
Retrocalcaneal Bursitis
This is characterized by pain in the Achilles tendon. Chronic inflammation of the bursa is brought on by friction, supination, and overpronation. The flexibility of the calf muscles can be significantly reduced. Severe pain and swelling of the posterior soft tissue in front of the Achilles tendon are common symptoms. This bursitis type is often accompanied by mid-portion insertional tendinosis.
Risk Of Getting Bursitis
Anybody at any age can develop bursitis, but older individuals, specifically those in their forties and beyond, are more susceptible. This comes from all the wear and tear of the muscles and bones.
Risk Factors
Overpronation of the foot
Leg length deviation
Osteoarthritis
Obesity
Tight hamstring muscles
Incorrect physical training
Not stretching properly
Body Composition
When Inflammation Becomes Permanent
When white blood cells cause inflammation, it’s signaling that the body’s immune system works properly. The process works like this:
Inflammation activates
White blood cells attack the foreign invader
The invader is neutralized
The inflammation deactivates
This is how the body’s defense system naturally works. But, white blood cells are not the only type of cell that emit cytokines. Adipocytes or fat cells are another type of cell that can emit cytokines and cause inflammation. Scientists have learned that fat is an active endocrine organ that secretes various proteins and chemicals, including inflammatory cytokines. The body stores excess calories as fat to be used later for energy. When the body keeps adding more adipose tissue, cytokines are released by the fat cells, triggering inflammation. Obesity is characterized as a state of low-grade, chronic inflammation. Increased fat cells place the body in a constant state of stress activating immune responses. This means the body is in a constant state of inflammation with the immune system switch permanently on.
References
Aaron, Daniel L et al. “Four common types of bursitis: diagnosis and management.” The Journal of the American Academy of Orthopaedic Surgeons vol. 19,6 (2011): 359-67. doi:10.5435/00124635-201106000-00006
Coelho, Marisa et al. “Biochemistry of adipose tissue: an endocrine organ.” Archives of medical science: AMS vol. 9,2 (2013): 191-200. doi:10.5114/aoms.2013.33181
Khodaee, Morteza. “Common Superficial Bursitis.” American family physician vol. 95,4 (2017): 224-231.
Although it is not officially summer, the past few weeks sure feels like it. Especially for those with joint discomfort and pain. As the body ages, individuals may notice their joints have some mobility/flexibility issues in the summer heat. Again, the heat and humidity are the culprits. The hotter it is, the more the body is susceptible to inflammation and swelling. The more prone an individual’s body is to swelling, the more pain can present. Barometric pressure can also have some form of impact on joint health. The pressure changes can cause the joints to become more sensitive. When the pressure changes, individuals often speak of their joints feeling tighter combined with stiffness, leading to a cycle of swelling and pain.
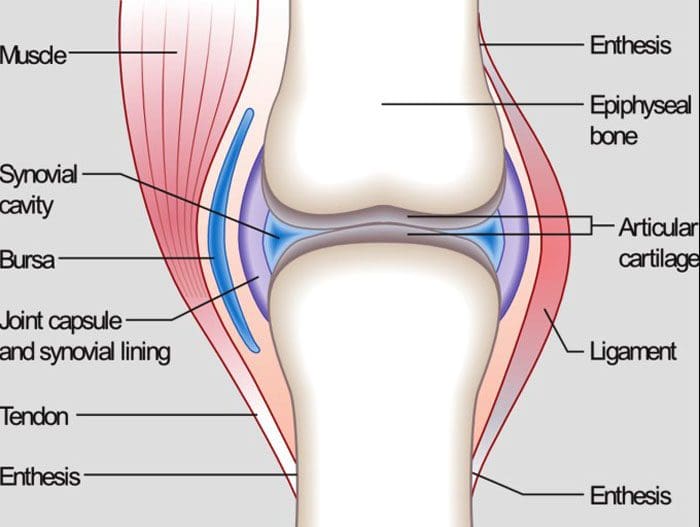
Joint Anatomy
Whether it’s the hip, knee, elbow, or hand, all of the body’s joints have fluid in them. It is a gel-like substance known as synovial fluid. This is what lubricates the joints and keeps them functioning smoothly. However, the temperature and humidity levels can change the thickness of the fluid in the joints. This means that the synovial fluid can become inflamed with the weather changes. This is a symptom when the joints begin to feel like they cannot move and/or are becoming stiff. Joint inflammation can become more common and chronic as the body gets older.
Weather and the joints
The summer heat and humidity can affect the joint because:
The tendons, ligaments, and muscles expand in this type of weather
The heat can restrict individuals from moving around. Non-use stiffens the joints
Joints that have worn down cartilage could have exposed nerves that are reacting to the temperature changes
Humidity causes the body to lose water by sweating. This can reduce the fluid around the joints leading to stiffness, immobility, and pain.
However, not everyone has joint problems in the summer heat. Many have joint issues when it’s cold, damp, or raining. Other’s are at their best in cool, dry weather. It depends on an individual’s body and how their joints react when the temperature changes.
Maintaining joint health for the summer heat
When joint discomfort or pain presents in the summer, there are a few easy ways to gain relief.
Properly Hydrate the Body
Water and sports drinks maintain the fluid levels in the body, specifically, it keeps the joints moving. One way to hydrate the body can be achieved by eating healthy fruits and vegetables. Water-rich fruits and vegetables include:
Watermelon
Oranges
Strawberries
Tomatoes
Cucumbers
Spinach
Celery
Over-The-Counter pain ointments and creams
Arthritis and anti-inflammatory creams/ointments can ease joint pain by allowing more blood circulation in the affected areas.
Dressing for the heat
Wear loose, natural fiber, breathable clothing that allows the body to move freely while maintaining a cool temperature.
Relax in the air conditioning
Get into the air conditioning. The cool air can help reduce joint inflammation.
Get in the Water
Swimming or just wading through doing some light exercise in the water cools the body’s core. In addition, the buoyancy of the water relieves pressure on the joints.
Body Composition Testing
Body Water
The body is made up of as much as 2/3’s water. Even though much of the body is made up of water, the percentage of body composition changes based on functional needs. Essential functions of water include:
Water is the building block to almost every cell in the body
It regulates the body’s temperature through sweating and respiration
Carbohydrates and proteins for energy are transported via the water in the blood
Water assists in the removal of metabolic waste through urination
It is part of the shock-absorbing system that protects the brain and spinal cord
Water is part of the saliva and fluid that lubricates the joints
The amount of water in the body depends on various factors. This includes:
Age
Gender
Physical activity
It is referred to as Total Body Water or TBW.
TBW is constantly changing with gains and losses of fluid in healthy adults. The body can detect irregularities and compensate for losses and/or gains to make sure that the systems are balanced.
The information herein is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. In addition, we provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Morton, Darren, and Robin Callister. “Exercise-related transient abdominal pain (ETAP).” Sports medicine (Auckland, N.Z.) vol. 45,1 (2015): 23-35. doi:10.1007/s40279-014-0245-z
Peeler, Jason et al. “Managing Knee Osteoarthritis: The Effects of Body Weight Supported Physical Activity on Joint Pain, Function, and Thigh Muscle Strength.” Clinical journal of sports medicine: official journal of the Canadian Academy of Sports Medicine vol. 25,6 (2015): 518-23. doi:10.1097/JSM.0000000000000173
Quick, D C. “Joint pain and weather. A critical review of the literature.” Minnesota medicine vol. 80,3 (1997): 25-9.
Timmermans, Erik J et al. “The Influence of Weather Conditions on Joint Pain in Older People with Osteoarthritis: Results from the European Project on OSteoArthritis.” The Journal of rheumatology vol. 42,10 (2015): 1885-92. doi:10.3899/jrheum.141594
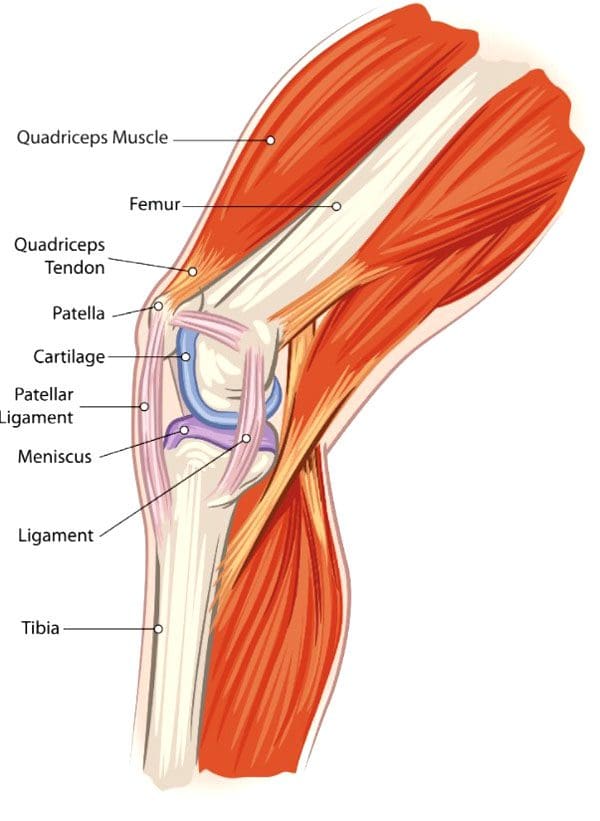
Knee Injuries, Surgeries, and Vitamin D Status. The knee joint is one of the largest and complex joints. It connects the thigh bone to the shinbone, which has a very important role in:
Supporting the body’s weight
Facilitating movement
Allowing the ability to bend the knee
Because of the complexity of the knee joint, it is highly susceptible to injuries. The most common injuries include tears in the:
Ligaments
Tendons
Cartilage
The kneecap itself can be fractured and/or dislocated.
Tears
Meniscal Tears
The meniscus is the cartilage between the knee joint that absorbs the impact/shock when running, playing sports, yard work, hiking, bicycling, etc. It cushions the joint and maintains stability.
Meniscus tears are common in sports that have a lot of jumping, starting/stopping quickly, changing direction suddenly, like volleyball, basketball, tennis, soccer, football. This is when the meniscus tears. Surgery can be required, depending on the severity/extent of the injury and tear.
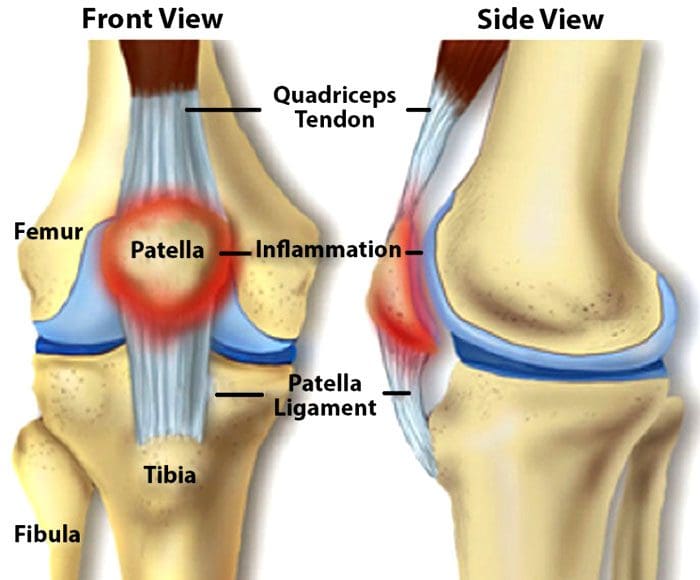
Tendon Tears
The patellar tendon works with the knee muscles in the front of the thigh to straighten the leg. Tears in the patellar tendon are common among middle-aged individuals and those that participate in running or jumping sports.
A complete tear is considered a disabling injury that requires surgery for full functional recovery.
Fortunately, most tears are partial and require rest and chiropractic/physical therapy to heal.
Dislocation
Knee dislocations happen when the knee bones shift out of position. This can happen after a fall, car crash, or high-speed impact. It can also be caused by twisting the knee while the foot stays planted. Dislocations require relocation. However, sometimes a dislocated kneecap corrects itself and returns to the proper position. Other cases can require a mild sedative to allow a doctor to relocate the knee. Dislocations generally take around six weeks to fully heal.
Anterior Cruciate Ligament – ACL Injury
The anterior cruciate ligament or ACL is knee tissue that joins the upper and lower leg bones and maintains the knees’ stability. The ACL can be torn if the lower leg over-extends forward or if the leg gets twisted. ACL injuries are common knee injuries and account for around 40% of sports-related injuries. These injuries can range from a small tear in the ligament to a severe injury where the ligament tears completely or gets separated from the bone. Treatment depends on the severity of the injury. Depending on various factors including the severity of the tear, surgery could be required.
Knee Surgery
For most cases, surgery is done using arthroscopytechnology. This procedure uses small incisions to insert a camera and surgical instruments into the joint. Usually, two or three incisions are needed with recovery time being quicker than large incision surgery where the whole knee is opened. Minimally invasive arthroscopic surgery is preferred by sports medicine experts. With this procedure:
There is no need to cut the tendons or muscles
Bleeding is reduced
Small incisions decrease scarring
Recovery time is shorter
However, sometimes a large incision is required for complex surgical techniques. Common knee surgery procedures include:
Arthroscopy Surgery
This method allows the ability to see inside the knee joint. The procedure is often recommended for:
Diagnosis
Minor repairs to ligaments and/or tendons
Cartilage or bone that needs to be removed
Total Knee Replacement
A full knee replacement is known as arthroplasty. When the joint is damaged beyond repair from injury or disease, an implant is placed in the knee joint restoring function. A small amount of cartilage and bone from the shinbone and thigh bone gets removed for perfect placement of the new knee joint.
Revision Knee Replacement
Most knee replacements last around 15 – 20 years. For individuals that have knee replacement early, then a new operation for new implants could be required. Here, the surgeon removes the original prosthesis and replaces it with a new one.
Partial Knee Replacement
Some knee injuries do not require complete replacement. Here, only the worn-out portion of the joint is replaced. As an example, the cartilage that has been lost in an area of the knee can be repaired with a partial replacement.
Vitamin D Status
A study on athletes that underwent ACL surgery looked at their vitamin d status and how it affected their recovery.
The research concluded that vitamin D status had no effect on surgery outcomes.
However, those with the lowest vitamin D status had three times the failure rate than those with higher vitamin D
The average age of the individuals was around twenty-four and were healthy athletes.
Each of the patients in this study had their vitamin levels measured before the operation and were grouped based on their vitamin D status:
Group 1 vitamin D below 20 ng/mL – considered deficient
Group 2 vitamin D between 20-30 ng/mL – considered low but in a technical range
Group 3 vitamin D above 30 ng/mL – considered sufficient, but not optimal
All were followed for two years with their surgery recovery being measured with two systems.
The Lysholm score, which is a 100 point scoring system that looks at an individual’s knee functions that include:
Mechanical locking
Instability
Pain
Swelling
Stair climbing
Squatting
The WOMAC score is a scoring system that measures:
After 2 years, the Lysholm score and the WOMAC scores were similar.
However, there was a difference in the graft failure rate which was about 6% in group 1 with the lowest vitamin D and around 2% in groups 2 and 3. This shows that the lowest vitamin D status has three times the failure rate compared with those that had increased vitamin D levels. Vitamin D is a known anti-inflammatory with metabolic functions that are documented. Therefore, vitamin D does improve surgical success and recovery in healthy athletes.
Body Composition
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Brambilla, Lorenzo, et al. “Outcome of total hip and total knee arthroplasty and vitamin D homeostasis.” British medical bulletin vol. 135,1 (2020): 50-61. doi:10.1093/bmb/ldaa018
European Journal of Orthopedic Surgery and Traumatology, January 2021
Zhang, Hao et al. “Vitamin D Status and Patient Outcomes after Knee or Hip Surgery: A Meta-Analysis.” Annals of nutrition & metabolism vol. 73,2 (2018): 121-130. doi:10.1159/000490670
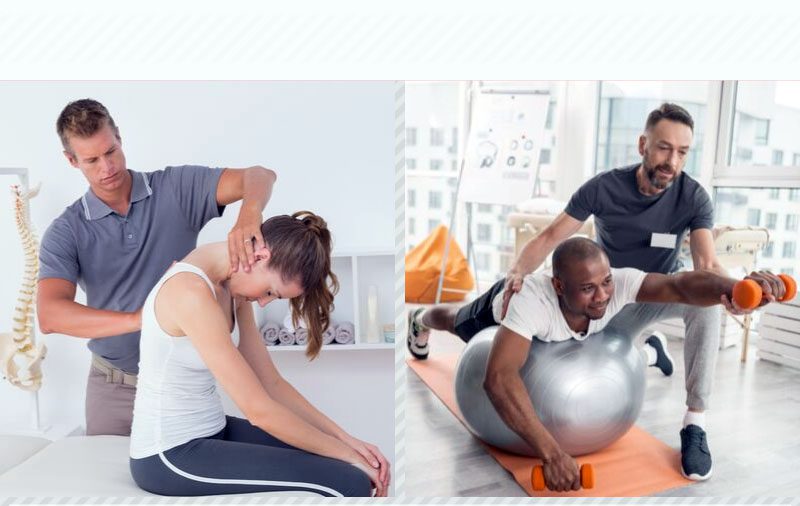
Chiropractic treatment and physical therapy are treatment methods/approaches that are conservative, non-invasive, and are both practical options. Both address health concerns, like various types of pain, automobile, work, sports, and personal injuries. Both are focused on helping individuals achieve long-term results and maintain health.
Chiropractic and physical therapy are usually done in combination, as they complement one another. There are benefits and similarities between the two treatment options. Here are some general guidelines to decide which treatment option is best for your needs.
Primary symptoms
Chiropractors are known for the ability to provide quick relief to individuals dealing with pain and stiffness in the joints, particularly the spine. They are experts in spinal realignment and proper posture. If flexibility is limited or the joints are locking up, a chiropractor is the recommended choice.
Physical therapists or PTs are the experts in body biomechanics and soft tissue injuries. If an individual finds themselves moving differently because of pain or injury, training and exercise will help movement and maximum recovery.
Treatment style
Chiropractors follow a meticulous expert-based protocol for achieving the best results. They provide a hands-on approach to treatment that requires regular follow-ups and maintenance. This is an approach that some individuals prefer. Physical therapy treatment/rehabilitation programs are typically short-term. The average treatment usually lasts only 12 weeks. A physical therapist’s primary objective is to provide a fundamental understanding of how to move properly and self-manage symptoms for the long term. This usually includes a balanced exercise program.
Insurance coverage
Insurance plans vary in what is covered. The first step is to see what an individual’s insurance will cover. Benefits can be found online or by calling a representative to see how to get the care/treatment needed. Most plans cover some form of physical therapy. Chiropractic is also usually covered by insurance providers. Skipping the insurance can also be done with chiropractic clinics providing affordable options.
Options
There is no clear-cut answer as to which to see. A physical therapist or chiropractor. Individuals should follow a doctor’s recommendations as to which treatment type would benefit them. If no recommendations have been given then take a look at a clinic’s website to see what they are about. Fortunately, many chiropractic clinics include physical therapists as part of their medical team. Both chiropractic and physical therapists provide dynamic benefits for increasing and maintaining overall health.
Body Composition
Hydration Guidelines
Drink according to thirst
The body knows when it needs water. Therefore drink when you are thirsty, not before. An adequate fluid intake should be timed according to feelings of thirst.
Estimate hourly sweat loss
Those that exercise or engage in regular physical activities for prolonged periods should weigh themselves before engaging in the exercise/activity. Then drink according to thirst as the event goes on, then weigh yourself after the activity. The goal is to maintain the same weight or be slightly less. If an individual weighs more than what they drank, then they drank too much.
Excess water consumption
If an individual is not thirsty, the recommendation is to not drink water in excess. Nausea and even vomiting could ensue. A simple indicator to determine if enough water is being consumed is to check urine color. If it is colorless or slightly yellow then an individual is drinking enough water.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
American Association of Physical Therapists. www.apta.org
Cherkin, D C et al. “A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain.” The New England journal of medicine vol. 339,15 (1998): 1021-9. doi:10.1056/NEJM199810083391502
Fritz, Julie M. “Physical therapy in a value-based healthcare world.” The Journal of orthopaedic and sports physical therapy vol. 42,1 (2012): 1-2. doi:10.2519/jospt.2012.0101
Shrier I. Does stretching help prevent injuries? Evidence-based Sports Medicine. Williston, VT: BMJ Books; 2002.
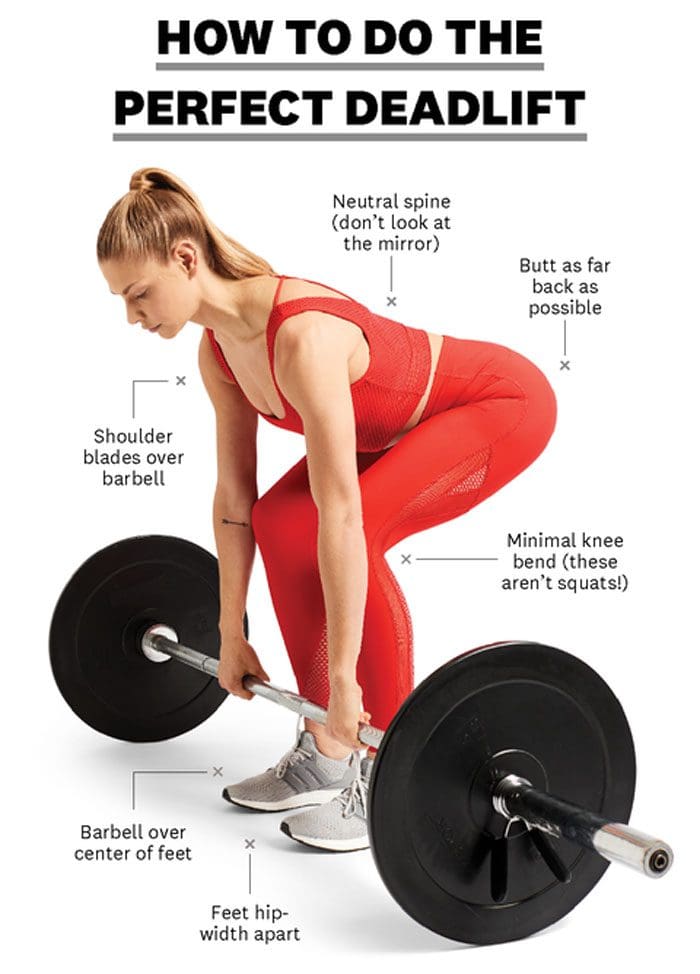
The deadlift is a weight training exercise that helps build muscle, strength, and stamina. It works legs, core, buttocks, and the back when performed correctly. Using an improper form or overdoing it can cause injury to the lower back. Recovering from a deadlifting injury usually takes a couple of days or a week. However, this depends on the severity of the injury. Recovery can be helped through:
Home remedies
Chiropractic treatment
Massage
Natural back pain relief tips
Back Injury After Deadlifting
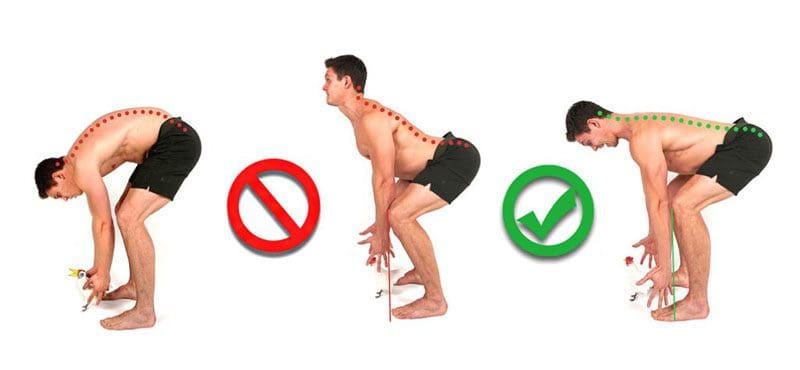
Most individuals will feel sore after a strenuous workout. But there is a difference between soreness and injury. Most of the time injuries from deadlifts are caused by not using proper form. Getting the form right is not easy, it does take practice, so do not feel bad if an injury presents.
Soreness vs Injury
Most of the time telling the difference between natural soreness from a workout and pain from an injury is pretty straightforward. But sometimes it is not as easy to tell the difference. Soreness is typically characterized by:
Stiffness
Tightness
Muscle ache
Fades after two or three days
Muscle soreness tends to be shallow and spread out over a muscle group. Pain from an injury causes sharp and persistent pain, especially with certain movements. Injury pain is deeper and can be described as stabbing or sharp.
Common Deadlifting Injuries
The deadlift has a wide range of motion and incorporates several different joints. Most injuries sustained during a deadlift are low-back injuries. Usually a sprain or a strain. But it is possible to sustain a more serious injury like a herniated disc.
Sprains vs Strains
Sprains and strains are different although many use the terms interchangeably.
A sprain happens when the ligaments that hold a joint together tear.
A strain happens when the muscles tear or are overworked to the point of injury.
Herniated Disc
A herniated disc happens when the gel-like fluid cushion between the vertebrae begins to protrude out. This can cause pain from the disc pressing on surrounding nerves or go unnoticed. Fortunately, sprains, strains, and herniated discs can all be treated conservatively. Seeing a medical professional is recommended to rule out serious conditions.
Injury Lower Back Pop
Some individuals experience an audible pop in the spine during a deadlift. For those that experience a pop but no pain accompanying it, it is likely gas escaping from a joint in the back. Those that experience discomfort or pain with the popping are encouraged to seek out medical attention.
Healing a Back Injury
Healing a back injury depends on the severity. The more severe, the longer it will take to heal. Most injuries can be addressed at home. Individuals that cannot stand up straight or there is debilitating pain with normal movements should see a medical professional like a:
Physical therapist
Chiropractor
Physician
Rest and let the body recover
It can be tempting to get back to the gym as soon as possible, but this is not recommended until the back truly feels normal. It is recommended to rest for a few days, allowing any swelling, inflammation to go down.
Ice and heat
Applying ice to the back every few hours for 15 to 20 minutes is recommended for the first three days, then heat can be incorporated. After three days if there is still pain, incorporate heat to get more blood flowing in and around the area. Use the ice for 15 to 20 minutes, wait 30 minutes, then apply the heat for 15 minutes.
Chiropractor
Seeing a chiropractor during any stage of recovery can be beneficial. As chiropractors are musculoskeletal specialists that can realign the body back to its proper form. If four days or more have passed and the pain is not going away, make an appointment with a certified chiropractor or spine specialist.
Time of Recovery
Most individuals recover within a week or two. For more severe injuries, like a herniated disc can take 6 to 8 weeks. Seeing a medical professional can help speed the process and promote healing. Additional tips include:
Deadlifting can be done safely and properly without sustaining an injury. A personal trainer or a sports chiropractor can analyze an individual’s lifting form and offer recommendations to prevent injury.
Body Composition
Foods Good for Collagen Production
Healthy nutrition can facilitate optimal collagen synthesis without supplementation. Protein sources that work with non-essential amino acids contribute to increased collagen production. High-quality protein sources support this process. Vegetarian protein sources include legumes or tofu are good alternatives. Collagen synthesis requires vitamin C, copper, and zinc.
Vitamin C regulates the synthesis pathway
Zinc stimulates the body to produce more collagen
Copper activates an enzyme that helps mature/strengthen the collagen
Sources of copper include nuts, seeds, whole grains, and chocolate
Most importantly is plenty of vitamin C-rich foods like:
Bell peppers
Broccoli
Citrus fruits
Leafy greens
Tomatoes
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Bengtsson, Victor et al. “Narrative review of injuries in powerlifting with special reference to their association to the squat, bench press and deadlift.” BMJ open sport & exercise medicine vol. 4,1 e000382. 17 Jul. 2018, doi:10.1136/bmjsem-2018-000382
Seeing A Chiropractor Regularly for Injury Prevention and Maintenance. A common question that comes up is how often is it necessary to visit a chiropractor? Everyone is different and the frequency of treatment depends on each individual’s specific situation/condition, health goals, and needs. Here are a few guidelines to keep in mind that can help get an idea of what to expect.
Seeing a Chiropractor
Chiropractors are the top experts in addressing underlying issues concerning the spine and musculoskeletal system. The most common reasons for seeking chiropractic treatment are musculoskeletal:
As an example, back pain is one of the top causes of disability. The workforce and medical community are seeing the effectiveness of chiropractic in reducing medical costs and loss of productivity. Spinal misalignment is an overlooked problem that can lead to a variety of health issues, including chronic pain and poor blood and nerve circulation. Restoring alignment is the first step in building sustainable health and achieving optimal quality of life.
Effective Treatment
Chiropractic treatment follows three stages. There is an emphasis on each stage and a specific focus for working toward long-lasting optimal health. Each phase is also associated with a different range of treatment protocols to achieve the best results.
Stage 1 Pain Relief
Starting treatment when the pain is at its most intense means the first step is bringing relief as quickly as possible. This is accomplished through:
Adjustments
Ultrasound
Heat and Ice
Massage
T.E.N.S
Stretching
Exercise
Other techniques to stabilize the individual
Stage 2 Restorative Care
Once the pain is relieved, the focus turns to long-term healing of affected tissues like the:
Muscles
Ligaments
Neural tissues
This helps with long-term recovery while reducing the risk of worsening or creating further injury/s.
Stage 3 Maintenance Care
This final stage is the monitoring stage. The chiropractic provider understands how important it is to regularly monitor an individual’s health and alignment to address any issues that come up and deal with them before they worsen or lead to other problems. Monitoring prevents unnecessary distress and helps the individual get back to their normal life.
Optimal Results
Achieving lasting results for symptoms cannot be done with a quick one size fits all treatment. With the guidance of a chiropractor, the individual will learn to recognize subtle changes in their body to alert them to adjusting lifestyle habits. Contact Injury Medical Chiropractic and Functional Medicine Clinic to determine what treatment and frequency offer the best results.
Body Composition
Inflammation That Can Become Permanent
When white blood cells cause inflammation, this is a sign that the body’s immune system is properly functioning. Inflammation starts, the white blood cells attack the invader, it is neutralized, and the inflammation recedes. This is how the body’s defense system works naturally. But the white blood cells are not the only type of cell that has the ability to release cytokines. A second type of cell that can release cytokines and cause inflammation are adipocytes/fat cells. The body stores excess calories as fat so that the body can use it later for energy.
Scientists have learned that fat is an active endocrine organ. It can secrete a host of proteins and chemicals, including inflammatory cytokines. When the body keeps adding more and more adipose tissue cytokines are released by the fat cells, triggering inflammation. Obesity is characterized as a state of low-grade, chronic inflammation.This means that increased fat cells put the body in a constant state of stress and immune response.This means that the body is always in a state of inflammation and the immune system is permanently switched on. Perpetual, never-ending inflammation is not healthy for the body.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Hadler, N M. “Chiropractic.” Rheumatic diseases clinics of North America vol. 26,1 (2000): 97-102, ix. doi:10.1016/s0889-857x(05)70123-x
Iben, Axén, et al. “Chiropractic maintenance care – what’s new? A systematic review of the literature.” Chiropractic & manual therapies vol. 27 63. 21 Nov. 2019, doi:10.1186/s12998-019-0283-6
Goertz, Christine M et al. “Effect of Usual Medical Care Plus Chiropractic Care vs Usual Medical Care Alone on Pain and Disability Among US Service Members With Low Back Pain: A Comparative Effectiveness Clinical Trial.” JAMA network open vol. 1,1 e180105. 18 May. 2018, doi:10.1001/jamanetworkopen.2018.0105
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine