PODCAST: Daniel Alvarado of Push Fitness Center and Dr. Alex Jimenez discuss the complications of losing weight. How to keep a focus and how to work our to the sticking point. An Ernest Discussion. Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Daniel (Danny) Alvarado, owner of the PUSH Fitness Center, continues to discuss the importance of weight loss and how people and athletes can continue the effort to stay healthy. Metabolic syndrome is characterized by 5 risk factors, including excess waist fat, high blood pressure, high blood glucose or sugar, high triglycerides, and low HDL or good cholesterol levels. Diet and lifestyle modifications, such as participating and engaging in exercise and physical activity, can ultimately help improve the 5 risk factors associated with metabolic syndrome and a variety of health issues, including diabetes, stroke, and heart disease. Dr. Alex Jimenez and Daniel (Danny) Alvarado discuss how motivation is one of the most fundamental elements in the continued effort to stay healthy. Following a diet and lifestyle modifications that are unique to each individual can also help promote overall well-being. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Subscribe: http://bit.ly/drjyt
Facebook Fitness Center Page: https://www.facebook.com/PUSHftinessathletictraining/
Yelp: El Paso Rehabilitation Center: http://goo.gl/pwY2n2
Yelp: El Paso Clinical Center: Treatment: https://goo.gl/r2QPuZ
PODCAST: Dr Alex Jimenez, chiropractor in El Paso, TX, Kenna Vaughn, health coach, Truide Torres, Alexander Jimenez, and Astrid Ornelas discuss metabolic syndrome. The following podcast will focus on a deeper look at understanding metabolic syndrome. Metabolic syndrome is a collection of conditions which can increase the risk of developing a variety of health issues, including diabetes, stroke, and heart disease. Moreover, risk factors such as excess waist fat, high blood sugar, high blood pressure, high triglycerides, and low HDL levels. Diet and lifestyle modifications can ultimately help promote weight loss which can help improve metabolic syndrome and its associated health issues. Several different types of nutraceuticals, including Niacin or vitamin B3, vitamin D, DHEA, Nrf2, and green tea, among others. Weight loss is important to help improve metabolic syndrome. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Smart supplementation along with proper nutrition is one of the biggest factors and plays a large role in an individual’s health. You are what you eat is true. Feeding the body with vital vitamins and minerals promotes growth and healing. Filling up on processed, fatty foods does the opposite. The bones in the spine and throughout the body need nutrients to continue to rebuild and maintain strength throughout life.
A balanced diet rich in:
�Calcium
Vitamin D
Magnesium
This is the best way to nourish the body’s bones and ward off spinal problems, like spinal fractures, and osteoporosis. Inadequate diets or medical issues can create nutritional gaps. This is where vitamins or mineral supplements come in. Supplements are not a cure-all, but they can create a safetyhealth net when taken properly.
Supplement Smart
These supplements for bone health, fill in nutritional gaps. They are not necessary if the key nutrients the body needs from a proper diet are already there. However, individuals use supplements as a replacement for certain foods, this is not how they should be used. Actual food supplies multiple nutrients, along with minerals, and vitamins that are beneficial for health and are not found in supplements.
Taking a Supplement to Strengthen the Spine
The body’s dietary needs change throughout life, so adding supplements as you age or during pregnancy can help maintain health. Calcium and vitamin D requirements vary based on age and sex.When it comes to protecting spine bone health, certain individuals may need supplements to ensure their bodies are processing calcium and vitamin D properly.
This includes:
Individuals who had intestinal bypass procedure
Those with food absorption conditions, like Celiac or Crohn�s disease
People who eat few or no dairy products, like vegans or those that are lactose intolerant
Is a calcium supplement right for you?
The only way to definitively know is by having a conversation with your doctor. Then you can supplement smart.
Supplement Safety
Because nutritional supplements can be purchased over the counter, individuals assume�incorrectly�that they are completely safe. Dietary supplements can interfere with absorption, other supplements, medications, and can be toxic if taken in high doses.
For example:
Calcium and iron supplements can prevent each other from being fully absorbed when taken together. This is true of many minerals, including magnesium, because they get into�absorption�competition with each other and so are best taken separately.
Supplements taken together can cause too much of either one to be absorbed. This is the case with high-dose vitamin D supplements, which can cause too much calcium absorption.
Too much calcium can increase raise the risk of having a heart attack or stroke. Taking more than 1,000-1,200 mg of calcium per day is pointless because the body cannot process that much calcium at once.
Are your supplements helping or hurting you? The best way to know is to talk to your doctor whenever you change medication or a supplement program, even when just adding a new vitamin to the mix. An underused resource for supplement advice is a pharmacist. They will know whether the mix of supplements and medicines being taken pose any risk of negative interaction. And a pharmacist can help recommend a trustworthy product.
Supplement Success
Here are a few tips to get the most benefits if you and your doctor think a calcium supplement can help support spinal bone health.
Buy supplements with the USP symbol. This indicates that the supplement has been independently evaluated and certified.
Take your supplement as directed, ideally with a meal.
Take doses no higher than 500-600 mg, no more than 2-3 times a day, for a maximum of 1,000-1,200 mg.
Drink plenty of water as some supplements can cause constipation.
Do not take calcium supplements with a high-fiber meal or laxative. This can interfere with calcium absorption.
Supplements Support Spine Health
Remember that supplements are exactly that supplements. Eating foods rich in calcium, vitamin D, and magnesium is the best way to build/maintain strong healthy spinal bones and prevent debilitating health problems. If you are concerned about your diet, talk with your doctor or a health coach about a smart supplementation regimen to meet your nutritional needs.
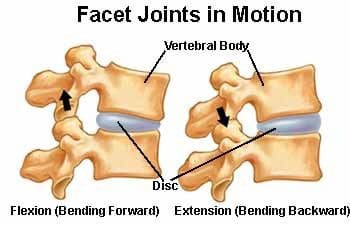
Facet joint syndrome also called facet joint sprain is a common cause of back pain. The joint/s in our bodies connect two or more bones and their primary function is to promote motion. In the spine, the joints connecting each vertebra are known as facet joints. Like any other joint, each facet joints� job is to generate healthy movement and provide stability for each motion segment.
The disc/s function as spacers that support motion between the vertebral bodies. This creates a tri-relationship between the intervertebral disc and the facet joints. Degeneration or damage/injury to one affects the other. The effects of aging and/or traumatic injury can damage the facet joints and is the leading cause of back pain known as facet joint syndrome.
There are a variety of treatments that are used, but the most mainstream involves pain medication which can have undesirable side effects and can lead to addiction. Chiropractic is a proven, reliable treatment for pain relief and discomfort of facet joint syndrome. It restores mobility and flexibility while providing pain relief. Individuals notice significant alleviation from the pain and inflammation with chiropractic and is often recommended to those with the condition.
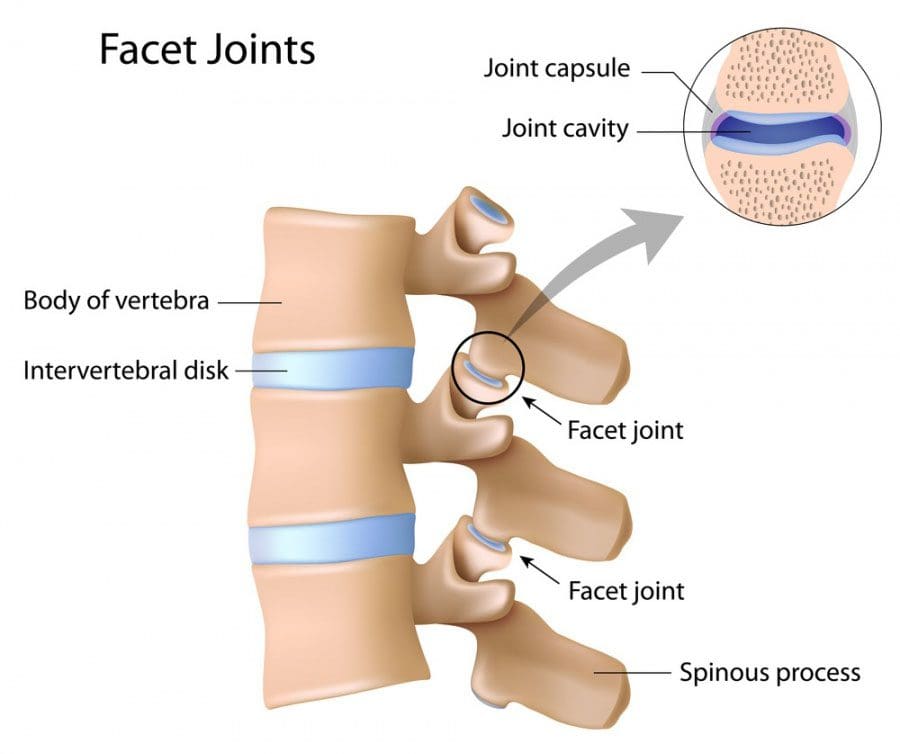
Facet joint syndrome
The joints are located at the back of the spine. At each level, there are two joints, one on each side of the spine. The facet joints are enclosed in a capsule. The capsule contains synovial fluid and the surface is covered with hyaline cartilage. These joints are constructed in this fashion because of their role in the body. This role is to control excessive or extensive movement, which includes hyperextension and rotation. This helps to stabilize the spine.
Facet joint syndrome happens when there is an injury or damage to the joints. There are a variety of causes, but basically, it is a sprain that is brought on by excessive movement. This damages the joint capsule and results in inflammation, swelling, and pain.
The pain triggers a protective mechanism in the spine called a reactive muscle spasm which causes difficulty moving comfortably and severe, sudden pain. It is difficult to sit and rest because of its integral function of supporting the body. Severe sprains can take weeks to heal, normally 2 to 6 weeks. The�daily pain and lack of mobility make everyday activities difficult and a normal lifestyle almost impossible.
Chiropractic/Physical Therapy
Chiropractic is a proven, effective treatment for facet syndrome.� A chiropractor will conduct a physical exam, discuss medical history, and send you for diagnostic tests like x-rays and MRIs. Once they have a clear picture of the condition and a facet joint syndrome diagnosis has been confirmed, they will discuss a recommended course of treatment that can include:
Exercise
They recommend exercises�specific�to the condition that helps relieve the pain while strengthening the muscles in the back.
Poor Posture
Posture is extremely important for spinal health and general wellness.
A chiropractor will help you achieve a proper, healthy posture along with exercises to do at home to maintain posture and retrain your body.
Heat/Ice
Heat wraps, hot showers or ice packs and cold pads can be recommended to help control pain and swelling.
Changes
Depending on job type, you may be advised to take frequent breaks if you sit all day or shorten your commute. Certain activities won�t be do-able for some time until your back heals.
Spinal manipulation
Spinal manipulation is the most standard chiropractic treatment. A chiropractor may include other treatments/therapies depending on the specific condition and lifestyle.
Chiropractic is a safe, effective, non-invasive, and drug-free way to treat facet joint syndrome, relieve back pain, and help you regain mobility. Talk to your chiropractor about treatment options. Our uplifting southwest community surrounded by its infinite beauty is a fantastic place to live and enjoy our families; it is, therefore, our mission to help each of our patients to live,�to�love,�to�matter�and�to�thrive�pain-free�in this beautiful special place.
Dr. Alex Jimenez, a chiropractor in El Paso, TX, Kenna Vaughn, Truide Torres, and Astrid Ornelas discuss what it is that they do and why they do it. Chiropractic care is a safe and effective, alternative treatment option that focuses on the diagnosis, treatment, and prevention of a variety of health issues associated with the musculoskeletal and nervous system, including neck pain, back pain, low back pain, and sciatica, among other health issues within the scope of chiropractic care. Dr. Alex Jimenez utilizes spinal adjustments and manual manipulations, among other well-known chiropractic care treatment methods and techniques, to help provide pain relief and promote overall health and wellness. Dr. Alex Jimenez, Kenna Vaughn, Truide Torres, and Astrid Ornelas discuss how they patients, from chiropractic care to educating them on diet and lifestyle changes, to help patients achieve their nutrition and fitness goals. According to Dr. Alex Jimenez, Kenna Vaughn, Truide Torres, and Astrid Ornelas, chiropractic care and functional medicine are treatment options that can naturally support well-being. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Dr. Alex Jimenez, a chiropractor in El Paso, TX, Kenna Vaughn, Truide Torres, Alexander Jimenez, and Astrid Ornelas, discuss how chiropractic care can ultimately help treat sciatica or sciatic nerve pain. The sciatic nerve is the largest and longest nerve in the human body. It runs from the lower back, down the buttocks and hips, and into the legs, knees, and feet. Sciatica can be caused by a variety of health issues which result in the compression or impingement of the sciatic nerve. Dr. Alex Jimenez, Kenna Vaughn, Truide Torres, Alexander Jimenez, and Astrid Ornelas discuss sciatica or sciatic nerve pain in further detail to ultimately help educate patients on their symptoms. Diet and lifestyle modifications, including nutraceuticals and exercise or physical activity, can be beneficial for patients with sciatic nerve pain. Furthermore, sciatica or sciatic nerve pain is a collection of symptoms rather than a single injury or underlying condition. Dr. Alex Jimenez, Kenna Vaughn, Truide Torres, Alexander Jimenez, and Astrid Ornelas conclude the podcast by describing how they each can help patients achieve overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Dr. Alex Jimenez and Dr. Mario Ruja discuss basal metabolic rate, BMI, and BIA. Body mass and body fat can be measured in a variety of ways, however, several measurement tools may ultimately be inaccurate for many athletes. According to Dr. Alex Jimenez and Dr. Mario Ruja, calculating an individual�s body mass and body fat utilizing various tools is essential to determine overall health and wellness. BMI uses a person�s height divided by twice their weight. The results may be inaccurate for athletes because their body mass and body fat is different, in terms of weight, compared to the average person. Dr. Alex Jimenez and Dr. Mario Ruja demonstrate that BIA, or bioelectrical impedance analysis, and various other tools, such as the DEXA test, the Tanita scale, and the InBody, among others, can help more accurately determine an athlete�s body mass and body fat. Basal metabolic rate, BMI, and BIA is essential for parents that have young athletes as well as for the general population. Healthcare professionals that have these tools available can ultimately help provide individuals with the results they may need to maintain overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine