Companies are doing what they can to keep operations moving and workers employed. Those that are able to work-from-home are doing so. But working from home is new to many and creates new challenges of converting an area in the house, apartment, etc, to become the workspace.
Back pain is common whether at the office or at the house. Everyday activities like the way you sit or lift can cause back pain if you�re not careful. At the house, it can be easy to lose track of time working. However, sitting with the wrong chair, at an improper height is not great for the body and overall health.
Working from Home and Back Pain
You probably thought you�d be comfortable working while lounging in bed or slouching on the sofa. However, after a few hours,�you would have a sore back, neck, or shoulders muscles. Working on a laptop for hours daily�at the kitchen counter or hunched over a coffee table and not sitting at a table or desk with a proper chair can lead to pain.�The best way to reduce and avoid back/neck pain is to make a few changes to the workstation.
Setting Up The Workspace
A comfortable workspace will increase productivity and physically help you feel good.
Working comfortably for hours, maintaining proper posture, it would be wise to invest in practical office appliances that can support physical well-being. Proper office ergonomics include:
The correct chair height
Footrest
Working desk posture that keeps muscles and joints comfortable
Choosing the ergonomic office chair is important, considering you will be using it for back support. Office chairs are not a one size fits all. The choice could be the difference between having continuing back pain or improving comfort, health, and overall productivity.
Ergonomic Back Support
Despite the adjustable ergonomic chair, you might still have back pain while working. Consider the following because it might not be the chair that�s not working.
Keep Moving Around
Step counts could take a dive when working from home. Exercise and stretching at regular intervals are extremely important to protecting the spine throughout the day. Remembering to do this at home can be harder than working in an office environment. Use an automatic reminder on the phone. Our bodies need regular low-impact aerobic activity. It provides the tissues with vital blood flow and helps minimize back pain.
Be Sure To Check Your Posture
The spine is not fixed in abnormal positions. Sitting and slouching forward for a long time will contribute to back pain. The advantages of sitting straight:
Keeps the Joints Aligned
Keeps the Bones Aligned
Supports the Muscles
Supports the Ligaments
Prevents Muscle Fatigue
Sit all the way back in your chair and take full advantage of the lower back support. The knees should be bent at a 90-degree angle with the feet flat on the floor or on a footrest.
Proper Screen Height
The height of the computer screen should not be too high or too low. Your eyes should aim at the center of the screen without having to crane your neck up or down. It should be directly in front to avoid tilting or turning your head. A laptop should be raised anywhere from 5 to 10 inches to provide the proper height.
Speaker Setting
Don’t go for the multitask when it comes to the phone. Having the phone between your neck/shoulder and working at the same time can lead to stressing your back and hurting/injuring the muscles. Turn on the speaker or use a headset to avoid the awkward neck position.
Breathe Deep
Proper breathing keeps the body and the muscles in the mid and lower back nicely relaxed. Improper breathing can make the nervous system react, causing pain or discomfort. Breathing exercises can be a way to target lower back pain/s. No special equipment is needed and can be done anywhere, anytime. Concentration is the key. Inhale and bring the navel towards the spine and then exhale. This exercise will engage the core muscles and will support the upper body.
While we have this time at home, working, teaching, we might be realizing that the chairs we are using are great for kicking back or sitting only for a short while. It could be time for a proper office chair with back support for those with back pain, as well as to help prevent poor posture conditions that can generate back pain.
Here are a few of the top picks for back pain. Experts offer guidance on how to purchase an ergonomic office chair. Author of the book Wellness by Design�is a consumer guide to optimizing your home for physical and mental health. Hopefully, this will aid you as you navigate chairs for back pain.
Posture Importance
One way proper posture is gained is by walking with a book on your head. That won’t be necessary, as good office chairs that offer back support lend themselves to healthy posture, which helps back pain. Studies confirm that improved ergonomics greatly decreases back pain. Proper posture keeps your body positioned to minimize stress on the muscles, joints, ligaments. Sitting the wrong way for a long time drains you and can cause fatigue, back pain or aching neck after a long day.
What to Look For
When it comes to chairs for back pain you want the best ergonomic office chair for your home. Keep an eye out for these key elements.
Adjustable
This is important, as our bodies are all different and require different settings for optimal posture. A chair should have adjustments for the seat, arms and back. The more adjustability the chair offers in terms of height and angle, the more it can be customized to your body.
Rolls Easy
A chair that rolls easily is one essential component for back pain support and prevention. Easily rolling allows you to stay close to your work, move around the work area comfortably, and optimal visibility. Be sure the construction of the casters is heavy-duty and that it will roll on your floor’s surfaces.
Durability
Durability goes a long way. Established brands with a reputation for high quality shows their confidence in the chair�s ability to serve you long-term. It might be a bit expensive but it�s an investment in health and productivity. The United States Department of Labor offers a how-to guide to create the best ergonomics set up for you. Their guide includes the backrest, seat, armrests and the chair base. Chairs for back pain are focused on the overall comfort of the individual.
The right chair helps position your body so that you don’t activate trigger points and lets you roll smoothly so that you�re consistently working in a more ergonomic fashion.
Best Budget
The best chair for a budget was the Zipcode Design Bret Ergonomic Mesh Task Chair, which runs about $159.99 depending on where you shop. This office chair checks off many ergonomic guidelines set by the Department of Labor and is price friendly. The chair has a five-legged sturdy�base, casters that move easily and a backrest that follows the natural curve of the spine.
Best Mid-Range
The best mid-range model is the Tempur-Pedic TP9000 Mesh Task Chair, $318.99. The Tempur-Pedic company that makes mattresses have created an office chair that helps the body. It is created with memory foam has straightforward levers that allow you to adjust the armrests and seat easily. Easy-to-clean material is another benefit when working from home.
Best High-end Option
The best high-end model is the Herman Miller Aeron Chair, $1,395. This one is priced pretty high because of its plush ergonomic features. Think of chairs for back pain as an investment for your health and high quality of life. This is a cult-favorite chair that was designed 20 years ago and has sold over 7 million. It is completely customizable, from the chair size, level of back support, preferred tilt and seat angle, custom armrests and custom casters made for your floor type.
Honorable Mention
An honorable mention is the Humanscale� Freedom Task Swivel Desk Chair, $1,049.
This is a sleek cutting-edge office chair for back pain. The seat relies on body weight and physics for its ergonomic superiority and checks off the Department of Labor�s recommendations for optimal office chairs. It has adjustable arms, independent-adjustable seat and more.
Methods in treating inflammation are the focus of this video. Dr. Alex Jimenez presents a discussion of natural ways to treat inflammatory cascades. Knowing what are the best supplements are presented. This is a safe alternative that is well researched.
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
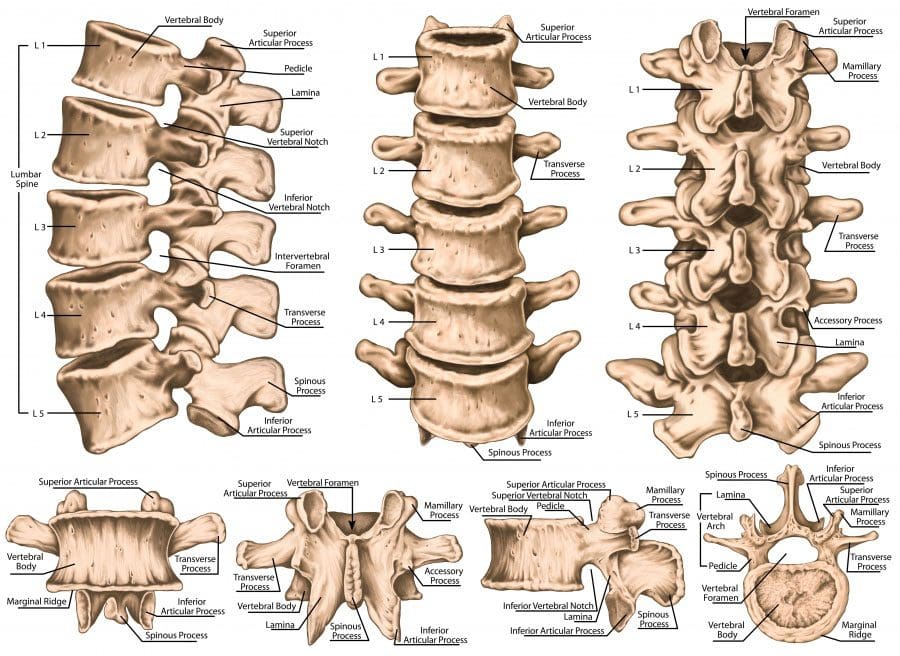
The lumbar spine is the lower back that starts below the last thoracic vertebra T12 and ends at the top of the sacral spine or sacrum S1. Each lumbar spinal level is numbered from top to bottom, L1 to L5, or L6. The low back bodies are larger, and thicker structures of dense bone. From the front or anterior, the vertebral body has a rounded shape.
The posterior bony structure is a different lamina, which is a thin bony plate that shields and protects access to the spinal canal. There are vertebral arches that create the hollow spinal canal for lumbar nerve structures and the cauda equina.
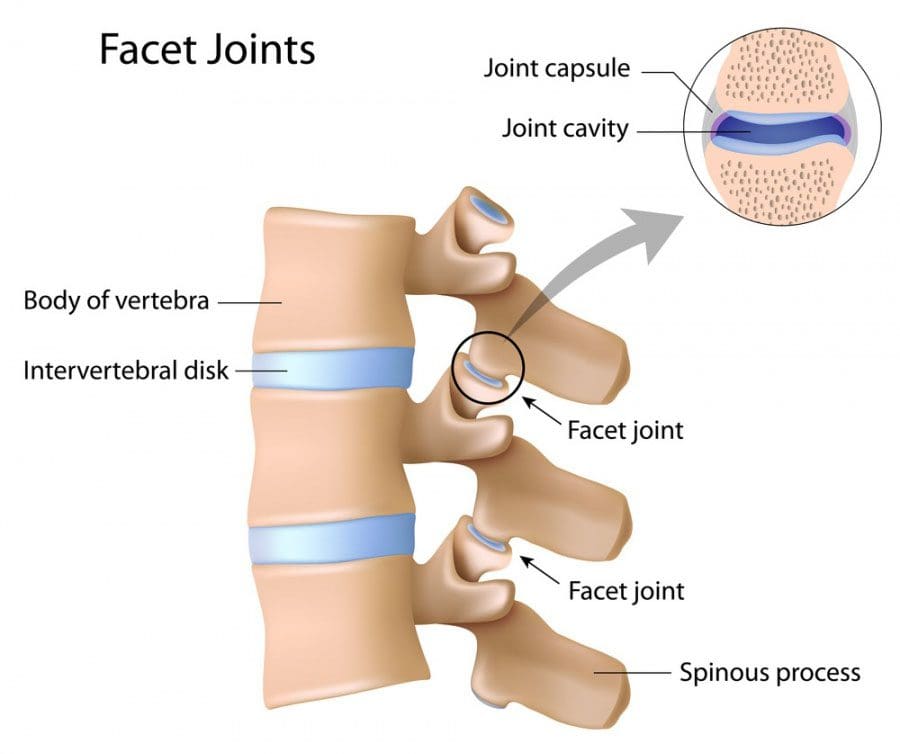
Lumbar Structure Strong Joint Complex
One intervertebral disc together with the facet joints forms a strong joint complex that allows the spine to bend and twist. One pair of facet joints from the top or superior vertebral body connects the lower or inferior set of facet joints. The facet joints are synovial joints, which means they are lined with cartilage and the capsule holds synovial fluid that enables joints to glide during movement. Think of it as hydraulics with smooth fluid motion.
Facet joint syndrome can develop from aging and degenerative spinal changes causing low back pain. The lumbar discs are secured in place by the fibrous endplates of the superior and inferior vertebral bodies.
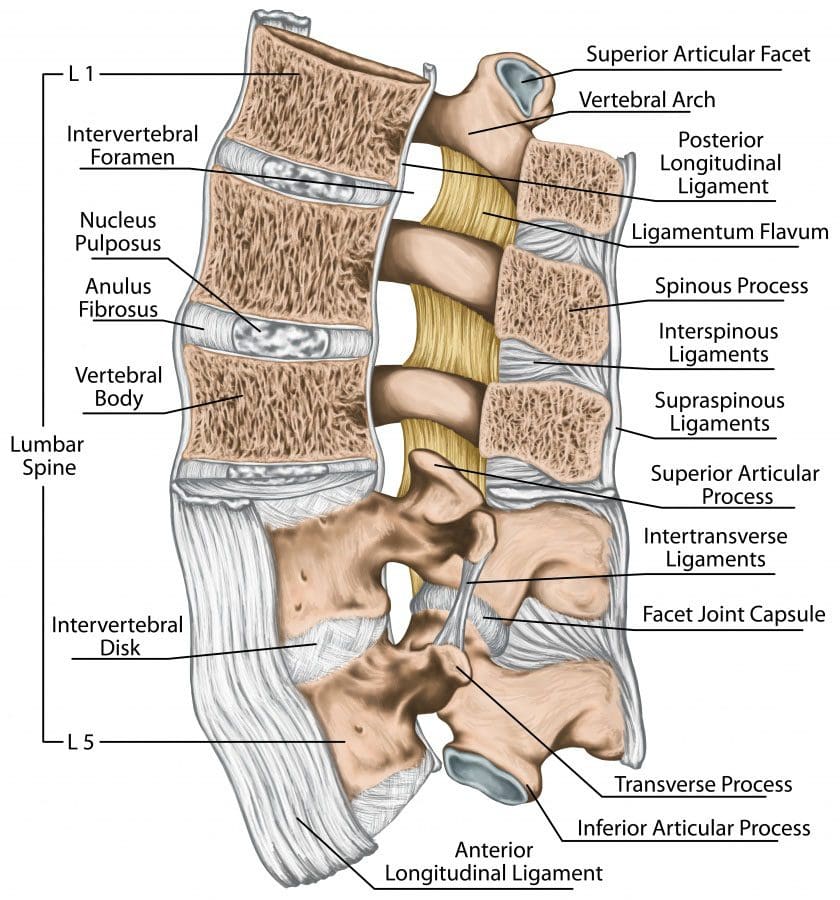
The jelly/gel center of each disc called the nucleus pulposus is surrounded by the annulus fibrosis, which is a tough layer of fibrocartilage that you can think of as a radial tire.
Discs are integral to the joint complex and function to:
Hold the superior and inferior vertebrae together
Take the weight
Absorb and distribute shock and forces when moving about
Create an open nerve passageway called foramen or neuroforamen
The neuroforaminal spaces on either side of the disc allow nerve roots to exit the spinal canal and leave the column.
Lumbar disc herniation is a common cause of low back pain that can spread out into one or both legs. This is called lumbar radiculopathy. This condition can develop when the nerves are compressed.
Low Back Support
Lumbar Ligaments
Tendons
Muscles
Systems of strong fibrous bands of ligaments hold the vertebrae and discs together and stabilize the spine by helping to prevent over/excessive movements.
The 3 major spinal ligaments are the:
Anterior longitudinal ligament
Posterior longitudinal ligament
Ligamentum flavum.
Spinal tendons attach muscles to the vertebrae and together work to limit excessive movement.
Lumbar Spine Nerves
The spinal cord comes to an end between the first and second lumbar vertebrae(L1-L2). Below this is the remaining nerves that form the cauda equina which is a bundle of nerves that looks like a horse�s tail. These nerves send messages between the brain and the lower body structures, including the:
Large intestine
Bladder
Abdominal muscles
Perineum
Legs
Feet
Protect Your Back
Around 80% of adults will see a doctor for low back pain at some point. Therefore take care of your lumbar spine to help avoid painful, unnecessary wear-and-tear. You can minimize the risk of a low back injury/pain by:
Losing weight. Even a loss of 5 pounds can help reduce back pain.
Strengthening the core/abdominal muscles. The abdominal and low back muscles work together to form a supportive band around the waist and low back. Stronger muscles help stabilize the low back and reduce the risk of injury.
Stopping smoking. Nicotine reduces blood flow to the spine’s structures. This includes the lumbar discs and accelerates age-related degeneration.
Proper posture and proper body mechanics. When lifting objects keep your spine erect and use your legs. Ask for help with heavy objects. The lumbar spine is can bend and twist simultaneously, try to avoid doing this, as it is a perfect setup for a strain or sprain.
Get Rid of Low Back Pain with Custom Foot Orthotics
PODCAST: Dr. Alex Jimenez and his crew focus on making several facts about the COVID-19 pandemic clear. Currently, there is no definitive cure for COVID-19. But what can we do then you may ask? Dr. Alex Jimenez, chiropractor in El Paso, TX, and his crew presents Antiviral Strategies that have scientific substantiations from healthcare professionals around the world. In a moment where information is spread without scientific support, we must look into the research studies that have sound science evidence in order to understand non-fiction from what the true science has presented. These are difficult times and very scary times. We present a body of information present from the works of Dr. Alex Vasquez. His information at time cryptic and found in his writings do shed some light and direction which many of us can take in order to prepare for optimal support from our own immunity. The scientific community is clear. Again, at this time there is no cure for COVID-19. This does not mean we must not look at a way to optimize our immunity. Specifically, since there is much that has been studied in the ways the Antiviral Stategies can prepare our bodies. Dr. Alex Jimenez and his crew continue to discuss Antiviral Strategies and how these can improve our immune system. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
PODCAST: Dr. Alex Jimenez, chiropractor in El Paso, TX, and Dr. Marius Ruja, chiropractor in El Paso, TX, ultimately discuss the reasons why choosing a functional medicine approach can safely and effectively improve overall health and wellness. The world has shifted in health care. There’s no time more than now which has started to look to the cause of disease as the present day focused on functional medicine approaches, methods and protocols. We discuss the “why” to choose the option of functional medicine in the present day health care system. Functional medicine focuses on natural treatment approaches to promote the healing of the human body. In this day and age, functional medicine may be essential to help improve our immune system. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share with us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
PODCAST: The COVID-19 pandemic has elevated our country into a heightened level of awareness. We start with our families and we start in our homes. Dr. Alex Jimenez, chiropractor in El Paso, TX, and Dr. Mario Ruja, chiropractor in El Paso, TX, discuss their perspective on the COVID-19 pandemic as healthcare professionals. Following the CDC’s guidelines, including staying at home, and washing your hands, has been recommended to help control the COVID-19 pandemic, among other CDC guidelines. Dr. Alex Jimenez and Dr. Mario Ruja continue to discuss the changes that the world is going through as countries learn to deal with the COVID-19 pandemic and other modern circumstances. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine