Various exams and tests are available to diagnose the source of an individual’s sciatica symptoms. The way your healthcare professional diagnoses sciatic nerve pain may depend on their specialty as well as on the cause of sciatica.
If you suspect you may have sciatica, however, it’s essential to first contact a spine specialist who may be able to properly diagnose any spinal health issues which may be causing your sciatic nerve pain. You might suspect you’ve got sciatica if you’re experiencing shooting pain in the low back and down one or both of your legs, or if you’ve been experiencing numbness, weakness or tingling and burning sensations in your legs.
Throughout your healthcare visit, your doctor or spine specialist will ask you specific questions and also carry out a few basic examinations and tests. This is to attempt to identify the reason for your sciatica and create an appropriate treatment program for you, or a method to manage your pain and other symptoms associated with sciatica as well as to help you recover.
As you are able to learn within our previous article on the common causes of sciatica, there are numerous spinal health issues that can lead to sciatic nerve pain, or sciatica. Your treatment plan will be determined depending on the main cause of your pain, therefore it is important to get an accurate diagnosis with a qualified and experienced spine specialist.
Furthermore, your spine specialist will ask about your current symptoms and remedies you may have used to alleviate sciatica. They will also ask other common questions, such as:
When did the sciatic nerve pain start?
Where do you feel pain? Is it all of the way down your leg? Is it in both legs? Does it stop at your knees?
On a scale from 1 to 10, with 10 being the worst pain possible, rate your pain.
Are you currently experiencing tingling sensations or weakness in your legs and/or feet?
What physical activities did you recently participate in?
Does walking uphill or downhill increase pain?
What else have you done to relieve your sciatic nerve pain? Have you tried particular medications or exercises?
Does anything reduce the pain or make it worse?
Your spine specialist will even execute physical and neurological examinations to determine if any of the symptoms of sciatica may be due to these health issues.
In the physical examination, a healthcare professional will observe the patients position, range of motion, and physical condition, noting any motion which causes pain. The healthcare professional will also feel your spine, notice its curvature and alignment, and feel for muscle strain. Through the neurological exam, the spine specialist will examine your reflexes, muscle strength, and other nerve changes.
To properly diagnose the cause of your sciatica, you might need to have some imaging evaluations. You could have an x-ray or a computed tomography (CT or CAT) scan. When it’s possible that a bulging or herniated disc or spinal stenosis may be causing your sciatica, a healthcare professional may order a magnetic resonance imaging (MRI) test.
Collectively, all these exams and tests will give your spine specialist a more comprehensive view of your sciatic nerve pain. Using this information, they will most probably be in a better position to make a diagnosis of the underlying cause of your sciatica.
Chiropractic Diagnosis for Sciatica
It’s very important that sciatica be correctly diagnosed by a healthcare professional in order for it to be treated correctly. A chiropractor is a qualified and experienced spine specialist who focuses on the diagnosis, treatment and prevention of a variety of injuries and conditions associated with the musculoskeletal and nervous system, including sciatica, Because many ailments can cause symptoms of sciatica, the chiropractor’s first step before beginning treatment is to determine the reason for the patient’s sciatica.
By studying about the patient’s medical history and administering physical and neurological examination, the doctor of chiropractic, or chiropractor, can get a thorough diagnosis of a patient’s sciatica. A chiropractor can also refer patients to receive diagnostic testing to more accurately determine the source of the health issues. As mentioned above, diagnostic testing includes MRI, X-ray, CT scan and/or electro diagnostic tests, such as nerve conduction velocity or electromyography. The examinations and diagnostic tests can also help determine the probable contraindications to chiropractic care as well as other treatment methods.
Chiropractic Treatment for Sciatica
It is worth remembering that the purpose of chiropractic care is not only to reduce sciatica but its objective is to help maximize the human body’s potential to heal itself, treating the symptoms at the source. Chiropractic care is non-invasive, drug-free, and natural way of healing the human body. After a proper diagnosis of the true cause of a patient’s sciatica is determined, the chiropractor may begin treatment accordingly.
The chiropractor will attempt to ascertain the cause of the sciatica so that a sciatica treatment plan might be administered. Chiropractic treatment for sciatica can include, cold therapies, ultrasound, spinal adjustments or manual manipulations, TENS, among other treatment methods. These treatment options have their own way of treating the sciatica symptoms.
Ice/Cold therapy helps reduce inflammation so that sciatic pain may be controlled. Ultrasound is heat created by sound waves entering deep into the tissues to decrease muscle spasms, stiffness, and pain. TENS unit or transcutaneous electrical nerve stimulation is a small box battery-powered portable machine which stimulates muscles. Spinal adjustments and manual manipulations function by correcting misaligned vertebral bodies, or subluxations, in order to restore them into an appropriate position in the spinal column so that nerve irritability and inflammation is decreased thereby preventing spasm, pain and other back symptoms.
Dr. Alex Jimenez’s Insight
A chiropractor is a spine specialist which can properly diagnose the source of a patient’s sciatica through the use of physical and neurological exams and tests. Diagnostic procedures may require a healthcare professional to check the individual’s muscle strength as well as their reflexes, for instance, the chiropractor may ask the patient to walk on their toes or heels, or they may ask the patient to lift their legs one at at time, while lying on their back. Symptoms of sciatica will generally worsen during these type of exams and tests. Furthermore, a doctor of chiropractic may request for imaging diagnostic tests to more effective determine the cause of the patient’s sciatic nerve pain, however, these may not be required unless the symptoms are severe.
Chiropractic care has increasingly become one of the most frequently recommended alternative treatment options for sciatica. To receive a proper diagnosis of your sciatic nerve pain, seek immediate medical attention from a spinal specialist, such as a chiropractor. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
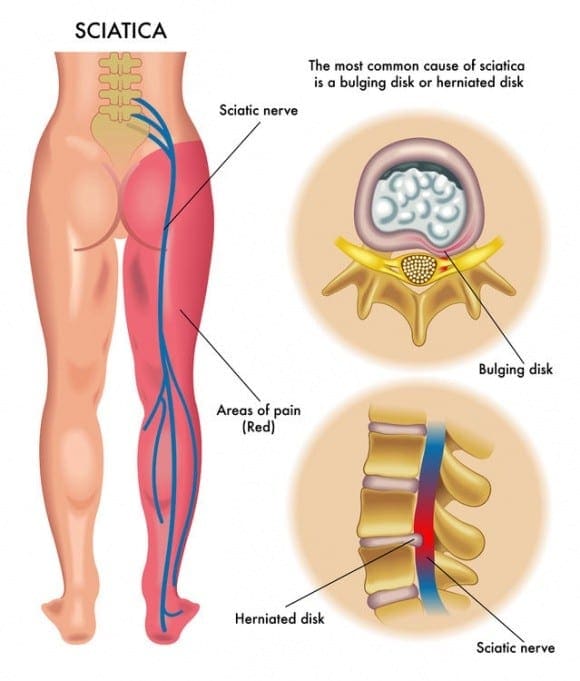
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Several lumbar spine (lower back) disorders can cause sciatica. Sciatic nerve pain is frequently described as mild to extreme pain at the right or left leg. Sciatica is caused by compression of one or more of the five sets of nerve roots in the lower spine. Sometimes doctors call sciatica a radiculopathy.
Radiculopathy is a medical term used to describe pain, numbness, tingling sensations, and weakness in the arms or legs caused by a nerve root issue. If the nerve problem is in the neck, it is referred to as a cervical radiculopathy. But since sciatica affects the low back, or the lumbar spine, it is known as a lumbar radiculopathy.
Pathways to Reduce Sciatic Nerve Pain
Five sets of nerve roots at the lumbar spine unite to create the sciatic nerve. Starting in the rear of the pelvis (sacrum), the sciatic nerve runs in the back, under the buttock, and downward through the hip area into every leg and foot. Nerve roots aren’t “solitary” structures but are part of the body’s whole nervous system capable of transmitting pain and feeling to other areas of the body.
Radiculopathy occurs when compression of a nerve root from a disc rupture (herniated disc) or bone spur (osteophyte) happens in the lumbar spine before it joins the sciatic nerve.
Causes of Sciatic Nerve Pain
Several spinal disorders can lead to spinal nerve pain and compression or lumbar radiculopathy. The 6 leading causes of sciatic nerve pain are:
a bulging or herniated disc
lumbar spinal stenosis
spondylolisthesis
trauma from an injury
piriformis syndrome
spinal tumors
Lumbar Bulging Disc or Herniated Disc
A bulging disc is also known as a contained disc disorder. This means that the gel-like center (nucleus pulposus) of an intervertebral disc stays “contained” within the tire-like outer wall (annulus fibrosus) of the intervertebral disc.
A herniated disc occurs when the nucleus pulposus breaks through the annulus fibrosus. It’s known as a “non-contained” disc disorder. If the disc bulges or herniates, disc material can push against an adjacent nerve root and compress delicate nerve tissue and lead to sciatica.
The results of a herniated disc may often be worse. When the herniated disc causes direct compression of the nerve root from the inside of the bony spinal canal, the disc material itself also includes an acidic, chemical irritant (lipoic acid) which causes nerve irritation. In both situations, nerve compression and irritation cause pain and inflammation, often leading to extremity numbness, tingling sensations, and muscle fatigue.
Lumbar Spinal Stenosis
Spinal stenosis is a nerve compression disease most frequently affecting older adults. Leg pain similar to sciatica may happen as a result of lumbar spinal stenosis. The pain is generally positional, frequently brought on by actions like standing or walking and relieved by sitting down.
Spinal nerve roots branch outward in the spinal cord through passageways called neural foramina comprised of bone and ligaments. Between each set of vertebrae, situated on the left and right sides, is a foramen. Nerve roots pass through those openings and extend outward beyond the spinal column to innervate different areas of the human body. Whenever these passageways become narrow or obstructed causing nerve compression, the term foraminal stenosis is utilized.
Spondylolisthesis
Spondylolisthesis is a disease that most often affects the lumbar spinal column. It’s characterized by a single vertebra slipping forward over an adjacent vertebra. When a vertebra slips and is displaced, spinal nerve root compression occurs and often triggers sciatic nerve pain. Spondylolisthesis is categorized as developmental (discovered at birth, develops through childhood) or acquired from spinal illness, injury or physical strain (eg, lifting weights).
Trauma from an Injury
Sciatica can result from sciatic nerve compression brought on by external forces into the lumbar or sacral spinal nerve roots. Examples include automobile accidents, falling down as well as football and other sports injuries. The impact may injure the nerves or, sometimes, fragments of broken bone may compress the nerves.
Piriformis Syndrome
Piriformis syndrome is named for the piriformis muscle and the pain generated if the muscle irritates the sciatic nerve. The piriformis muscle is located at the lower part of the spine, joins to the thighbone and also aids in hip rotation. The sciatic nerve runs beneath the piriformis muscle. Piriformis syndrome develops when muscle spasms develop in the piriformis muscle thereby compressing the sciatic nerve. It may be difficult to diagnose and treat due to the lack of x-ray or magnetic resonance imaging (MRI) findings.
Spinal Tumors
Spinal tumors are abnormal growths which are either benign or cancerous (malignant). Luckily, spinal tumors are infrequent. But if a spinal tumor develops in the pelvic region, there’s a danger for sciatica to grow as a result of nerve compression.
If you feel you’ve got sciatica, call a healthcare professional. The first step toward relieving pain would be a proper diagnosis.
Sciatic pain normally improves within about 4 to 6 weeks. Weakness and numbness may take more time to resolve. Symptomatic treatment such as cold packs, anti-inflammatory medications, and physical therapy/stretches/exercise may help ease discomfort and promote return to regular activities. Surgery to take pressure from the nerve is generally reserved for cases of severe pain. Alternative treatment options, such as chiropractic care, can help improve symptoms of sciatic nerve pain.
Dr. Alex Jimenez’s Insight
Sciatica is correctly defined as a collection of symptoms, rather than a single injury or condition, caused by the compression or irritation of the sciatic nerve. Also known as sciatic nerve pain, sciatica is generally an indication of a serious underlying health issue along the length of the lumbar spine, or low back. Sciatica can develop as a result of a variety of injuries and/or aggravated conditions, including but not limited to, a bulging or herniated disc, trauma or due to piriformis syndrome caused by sports injuries. Because sciatic nerve pain can manifest due to many health issues, diagnosing it can often be challenging. Fortunately, a doctor of chiropractic, or chiropractor, can properly diagnose sciatica in order to follow-up with the best treatment.
Chiropractic for Sciatic Nerve Pain
Diagnosis of sciatica Is crucial. A chiropractor assesses the patient and reviews medical history to ascertain what is causing the patient’s sciatic nerve pain. Chiropractic care is based on the principle which limited spinal motion results in pain and decreased function. Chiropractic care helps the body heal itself with non-invasive (non-surgical), drug-free treatment.
Chiropractic treatment methods for sciatic nerve pain include:
Ice/Cold therapy reduces inflammation and assists control sciatic nerve pain.
Ultrasound is mild warmth made by sound waves which penetrates deep into the soft tissues. It boosts circulation and reduces muscle spasms, cramping, swelling, stiffness, and pain.
Spinal Adjustments (Manual Manipulations). Spinal adjustments and manual manipulations are in the heart of chiropractic care. Manipulation supports restricted motion of the spine and helps restore misaligned vertebral bodies with their appropriate status in the spine. Adjustment techniques vary in the swift high velocity push to people who unite minimal force and mild pressure. Mastery of every technique is an art which requires great skill and precision. Spinal adjustments and manual manipulations are the treatment methods that differentiates chiropractic care from other medical disciplines.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Chiropractic Therapy: Sandra Rubio discusses how Dr. Alex Jimenez and his staff can help relieve your sciatica symptoms. Chiropractic care can improve pain and discomfort as well as reduce irritation and inflammation caused by sciatica. In addition, a chiropractor like Dr. Jimenez can also provide nutritional and fitness advice for sciatic nerve pain. Other treatment methods, like deep-tissue massage, can help relieve sciatica symptoms. Dr. Alex Jimenez is the homeopathic, non surgical choice for sciatic nerve pain and its associated symptoms.
Chiropractic Therapy For Sciatica Pain
Sciatica is generally caused by the compression of lumbar or sacral nerves or by compression of the sciatic nerve. When sciatica is caused by compression of a dorsal nerve root, it’s known as lumbar radiculopathy. This can occur because of a spinal disk bulge or spinal disk herniation (a herniated intervertebral disc), or by roughening, enlarging, or misalignment (spondylolisthesis) of the fascia, or as a consequence of degenerated discs which can reduce the diameter of the lateral foramen by which nerve roots exit the spine.
Our objective is to alleviate your pain and restore freedom, in�treating��our�sciatica�sufferers. Employing state of the art x-ray/fluoroscopic and ultrasound helps our experts pinpoint what�s going on. For treating sciatica we believe in the ability of medicine. By stimulating the body�s natural healing response, these procedures let us naturally provide long-term and deep pain relief.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of each and every one of my patients.
I assure you, I will only accept the best for you�
God Bless You & Your Health�?
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Sciatica Sufferers:Sciatica is a common back ailment that affects approximately 1 in 10 adults in the United States. It is most prevalent in people between the ages of 25 and 45. Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock and back of leg. The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their home, or just enjoying their life. Traditionally, doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
What Is Sciatica?
Sciatica is a condition that affects the lower back, specifically pain that travels along the sciatic nerve path. This path originates in the lower back and extends down each side of the hip, buttocks, and down the leg to the feet. Usually, only one side is affected during a case of sciatica.
Sciatica commonly occurs when there is a spinal condition, such as a bone spur on the spine, a herniated disk, or when a condition like spinal stenosis (narrowing of the spine) compresses the nerve. The result is inflammation, numbness, pain, and stiffness in the leg that is affected.
While sciatica pain can be severe, the majority of the time the condition is resolved in a matter of weeks without surgical intervention. Some doctors may suggest surgery if the patient experiences extreme weakness in the leg or has problems with their bowel or bladder. Most of the time doctors will prescribe medication to treat the pain and relax the muscles that surround the sciatic path in an effort to provide the patient with some relief.
How Chiropractic Treatments Help Sciatica Sufferers
Chiropractic has been shown to be very effective in treating sciatica by helping the body heal itself. It is non-invasive and does not use medications, making it an optimal choice for many patients. There are various treatments that a chiropractor may use or recommend. They may be used alone or in conjunction with other therapies.
Adjustments. Spinal manipulation, or adjustments, is the core of chiropractic treatment. It helps to realign the spine, freeing restricted movement and helps bring the body back into its proper alignment so that it functions better and more effectively. It also helps to reduce the pain that is associated with nerve inflammation, particularly that associated with sciatica.
Ultrasound. A very mild heat that is created by sound waves at a frequency that is beyond human hearing providing deep tissue penetration. This therapy stimulates circulation and aids in reducing muscle spasms, stiffness, swelling, pain, and cramping.
Ice or Cold Therapy. This therapy helps to reduce and control the pain of sciatica, as well as reduce inflammation.
TENS. Transcutaneous electrical nerve stimulation is a therapy that employs a TENS unit, a small battery powered, portable box that stimulates the muscles. It uses electrical currents at variable intensities to help control pain and reduce the occurrence of muscle spasms. Some chiropractors and physical therapists use larger versions of this device in their offices, but many use the portable units because they are more convenient.
A chiropractor may incorporate exercises and nutritional recommendations into their treatment for sciatica sufferers. This often depends on the patient�s individual needs, the severity of the condition, and their lifestyle and habits. A variety of chiropractic techniques may also be used to treat sciatica. Since each patient is different, the chiropractor will talk with the patient to better understand what they do on a day-to-day basis and what may be causing the sciatic pain to occur. From there they will treat the problem from the patient�s perspective, seeking the best, most effective approach.
If you or a loved one is suffering from this condition, please give us a call. Our Doctor of Chiropractic is here to help!
Is sciatica a spinal disorder or a symptom of a spinal disorder?�The term sciatica is commonly used to describe pain traveling in the distribution of the sciatic nerve, therefore it is more accurate to state that it is a symptom of a spinal disorder not a spinal disease itself.
Frequent symptoms of sciatica are listed below.
Sciatica usually affects one side of the human body, although it may affect both.
Pain from sciatic nerve pain may feel dull, sharp, burning, or accompanied by irregular shocks of shooting pain starting in the buttock and traveling downward into the thigh and/or leg.
Sciatica may also extend below the knee and might be felt at the feet.
Occasionally, symptoms of sciatic nerve pain include tingling sensations and numbness.
Sitting and attempting to stand up could be painful and challenging.
Coughing and sneezing can intensify the pain.
Where is the Sciatic Nerve?
Sciatic nerve fibers start at the 4th and 5th lumbar vertebra (L4, L5) and the first few segments of the sacrum. The nerve passes through the sciatic foramen, a nerve passageway just beneath the piriformis muscle which rotates the thigh laterally, towards the rear of the extension of the hip and into the lower part of the gluteus maximus, or the muscle in the buttocks,� that helps with thigh extension. The sciatic nerve then runs vertically down to the rear of the thigh, behind the knee and branches out into the hamstring muscles, or the calf, and farther downward into the feet.
Sciatica Caused by Nerve Compression
Compression of the sciatic nerve may cause any of the above-cited symptoms. Rarely is neurological damage permanent and paralysis is rarely a threat due to sciatica since the spinal cord ends before the first vertebra of the lumbar spine.
When to seek immediate medical attention for sciatica: Increasing back or leg weakness and/or bladder or bowel incontinence is a sign of cauda equina syndrome, a severe illness requiring emergency treatment. If you are experiencing these symptoms at the moment, please seek immediate medical attention from a qualified and experienced back pain specialist.
Certain lumbar spinal diseases can cause or lead to sciatica symptoms, including:
Herniated discs are the usual cause of sciatica in the lumbar spine.
Degenerative disc disease, a natural biological process related to aging, is known to cause disc weakness that may be a precursor to disc herniation.
Lumbar spinal stenosis is a narrowing of one or more neural passageways due to disc degeneration and/or facet arthritis. The sciatic nerve may become impinged as a consequence of these changes.
Isthmic spondylolisthesis results from a stress fracture frequently at the 5th lumbar vertebra (L5). The fracture together with disc space collapse may enable the vertebra to slide forward on the first sacral segment (S1). The slippage might cause the L5 nerve root to become pinched as it leaves the spine, developing into symptoms of sciatica.
Spinal tumors and illnesses are other ailments that may compress the sciatic nerve, but this is rare.
How Your Doctor Diagnoses Sciatica
A healthcare professional’s diagnosis of your pain and other symptoms may include discussing your medical history, recent accidents or injuries (eg, falls) as well as also a review of your current medicines (both over-the-counter and prescription drugs). Your doctor may additionally perform a physical evaluation using one or more movement evaluations to help determine the origin or causes of your pain. During the neurological portion of the evaluation, your reflexes and muscle strength are tested. If needed, they may order imaging studies, like an x-ray, CT scan, or even an MRI. The imaging tests can help confirm their diagnosis.
Furthermore, a healthcare professional may ask you a few questions, such as:
“How did the pain develop?”
“On a scale from 1 to 10, with 10 being the worst pain possible, rate your pain.”
“Is the pain caused by walking uphill or downhill?”
“How does the pain affect activities of daily living?”
“What kind of treatment was attempted and what was effective?”
Not all buttock and leg pain is sciatica as there are a number of different structures in the spine that can cause these kinds of pain. For example, the sacroiliac joint, or the joint between the pelvis and sacrum, the smallest segment of the spine, may cause or refer pain to the buttock as well as a sprain of the facet joints, which would be the connecting joints at the rear part of the spine. A bulging or herniated disc�can also refer pain down into the leg. If buttock and leg pain symptoms are correlated with any neurologic signs of numbness or weakness, it is “true sciatica” and has to be evaluated by a spine care expert, such as a chiropractor. If severe neurologic symptoms occur along with bowel and/or bladder control problems, it needs to be evaluated as soon as possible.
Chiropractic Diagnosis
In the assessment of lower back pain and sciatica, differential diagnosis using a “triage” concept of classifying back injuries and/or conditions to one of three categories helps guide the chiropractor when determining the source of the patient’s symptoms. These categories of chiropractic diagnosis include:
Potentially severe: tumor, infection, fracture, major neurological issues, such as cauda equina, local open wound or burn, prolonged bleeding (hemophilia), artificial joint enlargement, pacemaker problems and joint infection
Nerve issues: whenever the nerve roots from the lower back are pinched or compressed, they may cause� radiculopathy or sciatica. Typical causes of nerve root pinching and irritation include aherniated disc, spondylolisthesis and spinal stenosis
Non-specific: mechanical back pain in the lumbar spinal column. This type of lower back pain is the most frequent presentation, also contains pain for that there is not any identifiable cause.
Once the chiropractor has categorized the patient’s source of their sciatica, they may begin with the proper treatment. With chiropractic diagnosis of potentially serious injuries and/or conditions, the chiropractor will generally refer the patient to a relevant medical specialist, and as appropriate, the chiropractor might co-manage the patient’s care along with other back pain healthcare professionals. With this classification, chiropractic care may be used accordingly to avoid further spinal health issues.
In addition, with chiropractic diagnosis of a nerve root problem causing sciatica and/or non-specific causes of low back pain, chiropractors normally describe the symptoms experienced on the following scale:
Acute (symptoms lasting less than 6 months)
Subacute (symptoms lasting between 6 and 12 months)
Persistent (symptoms lasting for 12 months or more)
Recurrent/flare up (symptoms are similar to original symptoms and return sporadically or due to exacerbating circumstances).
Dr. Alex Jimenez’s Insight
Through the use of several physical evaluations and neurological assessments, a doctor of chiropractic is able to properly diagnose the source of a patient’s sciatica symptoms. Once a diagnosis has been established, a chiropractor will follow-up with the best, most recommended treatment for the individual’s specific needs and requirements. A spinal misalignment, or subluxation, is the most prevalent cause of sciatica. Spinal adjustments and manual manipulations are the most common treatment methods used to help carefully restore the natural alignment of the spine. A variety of other treatment methods can also be used by a doctor of chiropractic, to help speed up the patient’s recovery process. If the diagnosis of a patient’s sciatica symptoms determines that the source of their sciatic nerve pain is severe, a chiropractor may also refer the patient to the most appropriate healthcare professional to continue treatment.
These back pain or sciatica symptoms might be further broken down as mild, moderate or severe in pain. Once a chiropractor has properly diagnosed your sciatica symptoms, they may utilize a series of treatment modalities, including spinal adjustments and manual manipulations, among other well-known alternative treatment options, to help improve sciatic nerve pain.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Sciatica is described as a series of intense and painful symptoms in one or both legs along the course of the sciatic nerve. The pain is generally felt at the back of the leg and runs from the buttocks down the back of the thigh into the calf and foot. The pain may begin suddenly or start gradually, and is typically distinguished by a sharp, shooting, or electric shock-like in quality. Movement of the lower extremities often worsens the symptoms. Pain may be uniformly spread along the leg, but there are certain areas where pain may be more intense. Also,� pain is frequently associated with numbness and/or tingling sensations along the sciatic nerve.
Sciatica can result from any health issue that causes pressure or irritation of the nerve roots that compromise the sciatic nerve. This pressure may result from a variety of injuries and/or aggravated conditions, such as a ruptured intervertebral disc, narrowing of the bony spinal canal, medically referred to as spinal stenosis, or infrequently from infection or tumor. The sciatic nerve is the longest and largest nerve in the body; it measures three-quarters of an inch in diameter and it originates from the sacral plexus; a network of nerves found in the low back, or the lumbosacral spine. The lumbosacral spine refers to the lumbar spine and the sacrum combined. The sciatic nerve and its associated nerves allow movement and enable feeling, known as motor and sensory functions, in the thigh, knee, calf, ankle, foot, and toes.
About the Sciatic Nerve
The sciatic nerve begins in your low back, which is known as the lumbar spine. The nerve roots are in the L4 and L5 vertebrae (the ‘L’ means lumbar, as well as the numbers indicate the degree of the vertebra found along the spine). The sciatic nerve also travels throughout your pelvic area, or the sacrum. In most individuals, the sciatic nerve runs beneath the piriformis muscle, which functions by moving your thigh from side to side. From there, the sciatic nerve descends through the buttocks and the back of your thighs. Behind your knee, smaller nerves branch out from the sciatic nerve and journey down to your toes.
Your sciatic nerve is a part of an intricate arrangement of the human body’s nervous system. The nervous system is responsible for transmitting pain and feelings, as well as other sensations, to other parts of the body. Therefore, when an injury and/or a condition presses on a nerve, you are going to feel it, and many of the times it won’t feel great. With sciatica, a health issue on your low back, such as a herniated disc, for instance, permeates the sciatic nerve, which then transmits pain down your legs.
The sciatic nerve exits the sacrum in the pelvic area of the body through a nerve passageway called the sciatic foramen. At the top part of the sciatic nerve, two branches form; the articular and muscular branches. The articular branch goes to the hip joint. The muscular branch serves the leg flexor muscles, which are the muscles that enable movement. Other complicated nerve structures are also involved, both the peroneal nerves and the tibial nerves. The peroneal nerves originate from the nerve roots in the fourth and fifth vertebrae of the lumbar spine (L4-L5) and first and second levels of the sacrum (S1-2). When the peroneal nerves leave the pelvis, they move down the front and side of the leg and along the outer side of the knee to the foot.
The tibial nerves originate from the nerve roots in L4-5 and S1-3. The tibial nerves move in the front of the knee and then back into the foot, through the heel, sole and toes. In case your sciatic nerve is compressed or irritated, it can cause pain along these pathways; this is how sciatic pain can “spread” or radiate to some of the other parts of the body.
Common Questions and Answers of Sciatica
What is causing my pain? Your sciatic nerve pain, or sciatica, may be commonly caused by but not limited to a bulging disc or a herniated disc, degenerative disc disease, piriformis syndrome, pregnancy, spinal stenosis, a spinal tumor or other spinal illness, spondylolisthesis, or due to trauma from a injury. Any one of those conditions, among others, can put pressure on the sciatic nerve or related nerve roots in your low back. That stress is what causes your pain and other symptoms.
Will I need surgery? Most patients with lumbar radiculopathy respond positively to non-surgical treatments, such as chiropractic care, therefore, spine surgery for sciatica symptoms is seldom needed to treat it. However, there are situations when you might want to check with your healthcare professional about considering spinal surgery, particularly if:
You have bowel or bladder dysfunction. This is rare, but it might happen with spinal cord compression.
You have spinal stenosis, and your doctor believes that surgery is your best way to take care of it.
You are having other neurologic dysfunctions, such as intense or severe leg weakness.
Your symptoms become severe and/or non-invasive treatments are no longer effective.
What types of surgery are used for lumbar radiculopathy? Two frequent spinal surgeries for sciatica are:
Discectomy or microdiscectomy: In both these procedures, the surgeon removes part or all of a herniated disc that is pushing in your sciatic nerve and causing the symptoms. The distinction between the processes is that a microdiscectomy is a minimally invasive operation. The surgeon uses microscopic magnification to operate through a really small incision with very tiny instruments. Because the surgery is minimally invasive, you should recover more quickly from a microdiscectomy.
Laminectomy or laminotomy: These processes both involve a part of the spine known as the lamina, a bony plate that protects the spinal canal and spinal cord. A laminectomy involves the removal of the whole lamina; a laminotomy removes only a section of the lamina. These processes can produce more space for the nerves, therefore reducing the likelihood of the nerves being compressed or pinched.
Can I utilize over-the-counter drugs and/or medications to deal with my pain? Over-the-counter non-steroidal anti-inflammatory drugs, or NSAIDs, can help reduce swelling and inflammation while relieving your pain. You and your doctor have plenty to choose from. You may use acetaminophen (eg, Tylenol), ibuprofen (eg, Advil), or naproxen (eg, Aleve). However, the use of drugs and/or medications only temporarily relieves the symptoms of sciatica without treating the source of the pain. Make sure to talk to a healthcare professional regarding the utilization of these and continue to seek the most appropriate treatment for your sciatic nerve pain, such as chiropractic care.
How Chiropractic Can Help Treat Sciatica
Sciatica is a frequent issue for a lot of people that is identified by pain that begins in the lower back or buttocks, then radiates into one or both legs. It may vary in terms of frequency and severity, but it may often be constant.
The pain from sciatica can often be severe, and in addition, it can be very sharp. It may be associated with tingling sensations, burning, or numbness and weakness. What people may not realize is that it’s a collection of symptoms, an indication that something isn’t right, rather than a single type of injury and/or condition itself. The problem which leads to pain is generally a misalignment, or subluxation, of the lumbar spine. The sciatic nerve begins in the lower back and extends to the lower leg. That is why the pain may often be felt everywhere along the sciatic nerve.
A chiropractor commonly treats patients with symptoms of sciatica. Spinal adjustments and manual manipulations will aim to realign the spine, taking the pressure from the sciatic nerve and often bringing immediate relief. When the stress is off, the body can begin to heal itself. While spinal adjustments and manual manipulations are probably most frequently used, other treatments may be provided, particularly if common chiropractic care may not be advisable. Other treatment modalities might include using ultrasound, a TENS, or transcutaneous electrical nerve stimulation, device, or ice therapy. Ultrasound warms the region and increases circulation, which can lessen the swelling and muscular tension. A TENS device brings relief using a minor electric current to relax muscle spasms and also to increase endorphins. Furthermore, physical therapy, massage and or a series of stretches and/or exercises, may also help improve sciatica.
Dr. Alex Jimenez’s Insight
Chiropractic care is a popular, alternative treatment option commonly utilized to help treat symptoms of sciatica. Sciatica is characterized as a collection of symptoms, rather than a single injury or condition. A chiropractor can help diagnose the source of a patient’s sciatic nerve pain, or sciatica, in order to properly determine the best treatment for their specific health issue. Spinal adjustments and manual manipulations can be utilized to help carefully correct the alignment of the spine, restoring the natural integrity of the spine and allowing the body to heal itself, without the need for drugs and medications or surgery.
In certain individuals, sciatica may fix itself, possibly happening just once or a few times throughout their lifetime. But, it’s important to remember that if an injury and/or aggravated condition is not treated effectively, symptoms may worsen. A chiropractor can help provide relief from your sciatic nerve pain. Physical activity will most likely be recommended to strengthen the muscles in the back to help prevent sciatica as well as to speed up the recovery process. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Sciatica is a condition characterized by painful symptoms, often originating from the lower back all the way down to the toes. Sciatica is brought on by the irritation of the sciatic nerve. The sciatic nerve begins around the lumbar spine and runs down to the feet. Sciatica can be caused by the irritation of the sciatic nerve anywhere along its length. But the most frequent cause of sciatica is irritation to the sciatic nerve either in the lower back or in the gluteal region caused by poor posture.
Sciatica generally presents itself as a very specific collection of symptoms. If you can’t pin-point exactly where your pain is (i.e. if the entire leg just aches or if your symptoms are quite vague), it’s unlikely that you have sciatica. Sciatica typically runs as a band of pain through the low back and the buttocks, and also down the hamstring, occasionally traveling as low as the calf muscle and even the feet and toes. If you experience a sensation similar to pins and needles and/or numbness, the severity of your sciatica is much worse than if you just have pain.
Poor Posture Reasons For Sciatica
Poor workplace ergonomics can be a significant contributing aspect to the development of sciatica. Further, if you already have sciatica, inadequate workstation ergonomics is very likely to make it worse. A leading ergonomic issue in regard to sciatica is increased back pain that’s brought on by poor posture while sitting and standing. It you embrace a slouched or slumped position, or you lean forward at your desk, you place a tremendous amount of strain on your lumbar spine. This can result in your lower back muscles going into spasm. The sciatic nerve has to operate through those muscles. If they are spasmodic, there is a heightened likelihood that the sciatic nerve will end up irritated and develop symptoms of sciatica.
Sitting for extended periods of time is just another issue, for two reasons:
First, in sitting, your bodyweight is transferred from your upper body to your pelvis, throughout the lumbar spine. This implies that there is a continuous, and dull, compressive force going through the lower spine. Over time, this may result in irritation to the nerves as they leave the spinal cord canal. This is much more of a problem for people who have sciatica. Sciatica will frequently cause inflammation around the nerve root where it exits the spinal canal. This means there’s less “wiggle” room for the nerve to move and continuous compression may impinge this nerve, causing symptoms.
Second, the sciatic nerve runs throughout the gluteal region. Especially, it runs through a muscle called the piriformis muscle, which happens to be in about the region of your sitting bone. When you sit, you really literally sit on the piriformis muscles along with the sciatic nerve. Therefore, when you sit you’re compressing the sciatic nerve. Compression that is constant could lead to the piriformis muscle moving into spasm. Similarly to above, in the event the piriformis muscle goes into spasm, the sciatic nerve is very likely to be compacted and irritated, leading to some kind of sciatic symptoms.
Furthermore, healthcare professionals say that poor posture may cause more than just back pain and sciatica. Poor posture may actually cause a variety of health issues, according to research studies.
Effects of Poor Posture
Posture is an important part of preventing issues which range from back pain to fatigue. When the spine is properly aligned, the spine is stabilized and supported, however as you slouch or practice other methods of poor posture, your spine no longer gets the support it needs to remain balanced, leading to many health issues. The following health issues may also present themselves as a result of poor posture.
Sore Muscles
The most common effect of poor posture includes sore muscles. As you slouch, the muscles have to work harder to keep the spine protected and stabilized. The extra work on these muscles may cause muscle stiffness and fatigue. This can lead to chronic health issues with sore and tight muscles from the neck all the way down to the lower spine. Two big muscle groups which bare the brunt of these problems are the flexors and extensors of the back, which allow you to bend forward and lift objects.
Spinal Curvature
Among the most serious health issues that could happen with bad posture is developing a severe spinal curvature. As stated by the Chiropractic Resource Organization, the human spine has four natural curves which form an “s” shape. When poor posture is practiced, the spine can experience pressure, gradually influencing the spine curves to modify their positions. The spine is particularly designed to help absorb shock and keep you balanced, but as the spinal column position changes, this capacity becomes compromised.
Subluxations
Once the spinal curve is altered, one major problem that may occur are subluxations, or spinal misalignments. Vertebral subluxations occurs when a vertebrae becomes misaligneds from the rest of the spine. This also affects the total integrity of the remaining spine. These misalignments can eventually lead to chronic health issues, such as stress and aggravation of neighboring spinal nerves.
Blood Vessel Constriction
As bad posture changes the alignment of the spine, the consequent movement and subluxations can cause problems with blood vessel constriction. The constriction of the arteries across the spine can cut off blood supply to the cells of their muscles, which may influence nutrient and oxygen supply. Blood vessel constriction can also raise your chances of clot formation and issues using deep vein thrombosis.
Nerve Compression
One of the most frequent side effects of bad posture is nerve compression. As the spine changes in shape, the resulting movements or subluxations can put stress on the surrounding spinal nerves. Since the nerves which connect to the spine come from all over the body, these pinched nerves can not only cause neck and back pain but might also cause pain in other unrelated regions of the body.
In a 2013 study conducted Japan done by Kamitani et al, posture was connected to a decrease in lifespan and in activities of daily living. The study concluded that posture had a significant impact on quality of life as well as life expectancy.
Dr. Alex Jimenez’s Insight
Whether you’re slouching over your laptop, looking down at your mobile phone, bending over to pick up a box or simply sitting behind a desk for an extended amount of time, all of these regular activities can negatively affect your posture. Poor posture can not only cause back pain and symptoms of sciatica, it can manifest into a wide array of health issues if not properly corrected in time. Various research studies have even demonstrated that poor posture can affect longevity and life expectancy. Chiropractic care can help carefully restore the alignment of the spine, to recover the human body from the effects of poor posture.
Correcting Poor Posture to Improve Sciatica
The first thing that needs to be done to correct poor posture is to find a diagnosis from a healthcare professional, such as a chiropractor or physical therapist. They will be able to aid you with a treatment program and with hands-on therapy to alleviate your symptoms. Chiropractic care is a well-known, alternative treatment option which focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated to the musculoskeletal and nervous system. Also, an ergonomic evaluation is a good idea. It is best practice to allow an expert to perform an ergonomic assessment for you when you’re injured, as opposed to attempting to do it yourself. This is because of the probability of making things worse when it is not done properly.
But if an ergonomic appraisal isn’t a possibility for you, consider these hints:
?Try to integrate some standing into your daily work day, to decrease the constant pressure on the sciatic nerve.
Take regular walks during your working day and consider a stretch to your gluteal area.
Make sure your workstation is set up ergonomically to prevent additional exacerbation, paying special attention to the following:
Ensure you are not leaning forwards;
Make sure that your backrest is large enough so that the lumbar support is comfortably supporting the lower spine;
Ensure your seat cushion isn’t too tough;
Ensure that your feet are well supported;
Make sure your office chair is not too low, as this promotes slouching.
One last note, sciatica may be a difficult condition to take care of. So where possible, involving a healthcare professional, such as a chiropractor, or doctor of chiropractic, is in your best interests, towards correcting your poor posture and improving symptoms of sciatica, among others.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Our objective is to alleviate your pain and restore freedom, in�treating��our�sciatica�sufferers. Employing state of the art x-ray/fluoroscopic and ultrasound helps our experts pinpoint what�s going on. For treating sciatica we believe in the ability of medicine. By stimulating the body�s natural healing response, these procedures let us naturally provide long-term and deep pain relief.
Our objective is to alleviate your pain and restore freedom, in�treating��our�sciatica�sufferers. Employing state of the art x-ray/fluoroscopic and ultrasound helps our experts pinpoint what�s going on. For treating sciatica we believe in the ability of medicine. By stimulating the body�s natural healing response, these procedures let us naturally provide long-term and deep pain relief.










