When sciatica or other radiating nerve pain presents, can learning to distinguish between nerve pain and different types of pain help individuals recognize when spinal nerve roots are irritated or compressed or more serious problems that require medical attention?
Spinal Nerve Roots and Dermatomes
Spinal conditions such as herniated discs and stenosis can lead to radiating pain that travels down one arm or leg. Other symptoms include weakness, numbness, and/or shooting or burning electrical sensations. The medical term for pinched nerve symptoms is radiculopathy (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020). Dermatomes could contribute to irritation in the spinal cord, where the nerve roots cause symptoms in the back and limbs.
Anatomy
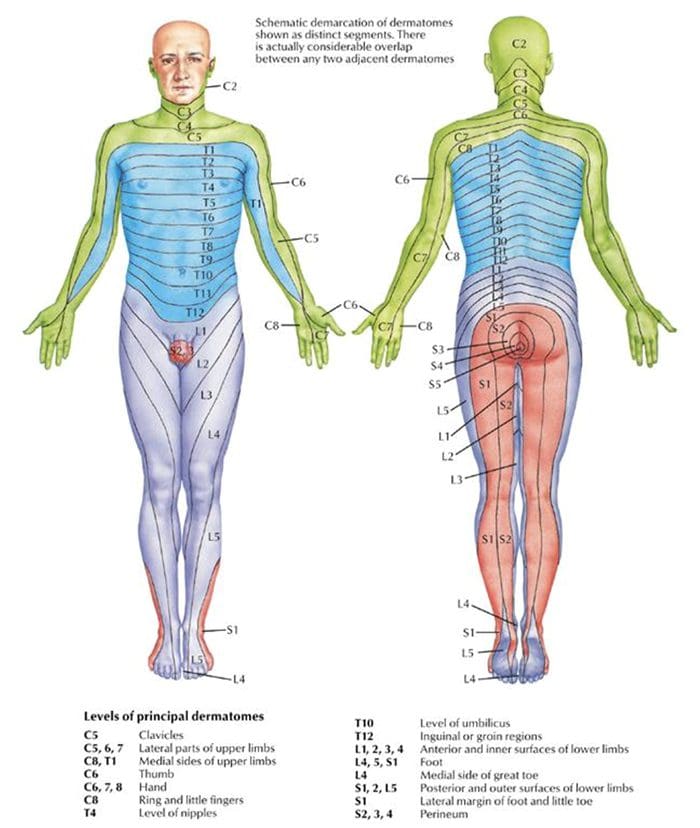
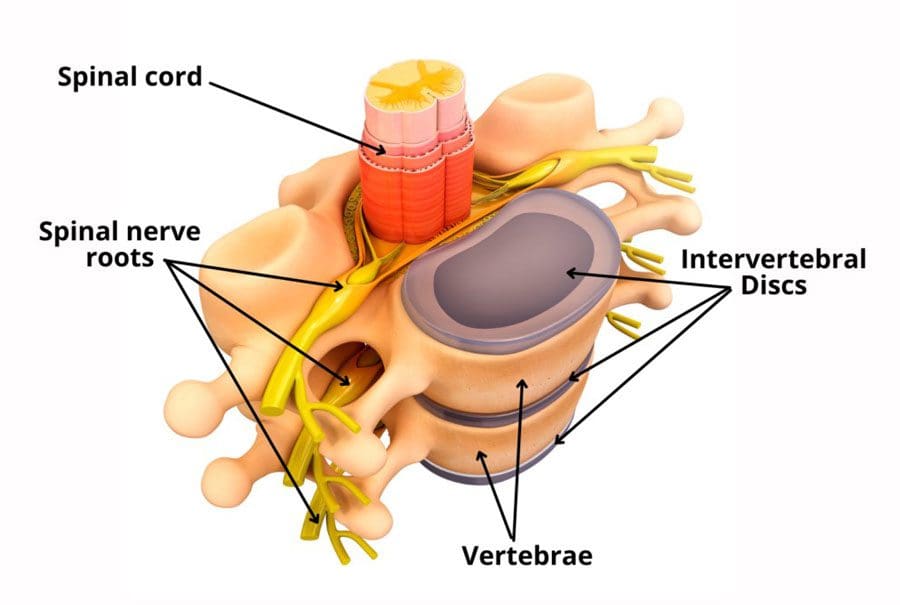
The spinal cord has 31 segments.
Each segment has nerve roots on the right and left that supply motor and sensory functions to the limbs.
The anterior and posterior communicating branches combine to form the spinal nerves that exit the vertebral canal.
The 31 spine segments result in 31 spinal nerves.
Each one transmits sensory nerve input from a specific skin region on that side and area of the body.
These regions are called dermatomes.
Except for the first cervical spinal nerve, dermatomes exist for each spinal nerve.
The spinal nerves and their associated dermatomes form a network all over the body.
Dermatomes Purpose
Dermatomes are the body/skin areas with sensory input assigned to individual spinal nerves. Each nerve root has an associated dermatome, and various branches supply each dermatome off that single nerve root. Dermatomes are pathways through which sensational information in the skin transmits signals to and from the central nervous system. Sensations that are physically felt, like pressure and temperature, get transmitted to the central nervous system. When a spinal nerve root becomes compressed or irritated, usually because it comes into contact with another structure, it results in radiculopathy. (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020).
Radiculopathy
Radiculopathy describes symptoms caused by a pinched nerve along the spine. Symptoms and sensations depend on where the nerve is pinched and the extent of the compression.
Cervical
This is a syndrome of pain and/or sensorimotor deficiencies when nerve roots in the neck are compressed.
It often presents with pain that goes down one arm.
Individuals may also experience electrical sensations like pins and needles, shocks, and burning sensations, as well as motor symptoms like weakness and numbness.
Lumbar
This radiculopathy results from compression, inflammation, or injury to a spinal nerve in the lower back.
Sensations of pain, numbness, tingling, electrical or burning sensations, and motor symptoms like weakness traveling down one leg are common.
Diagnosis
Part of a radiculopathy physical examination is testing the dermatomes for sensation. The practitioner will use specific manual tests to determine the spinal level from which the symptoms originate. Manual exams are often accompanied by diagnostic imaging tests like MRI, which can show abnormalities in the spinal nerve root. A complete physical examination will determine if the spinal nerve root is the source of the symptoms.
Treating Underlying Causes
Many back disorders can be treated with conservative therapies to provide effective pain relief. For a herniated disk, for example, individuals may be recommended to rest and take a nonsteroidal anti-inflammatory medication. Acupuncture, physical therapy, chiropractic, non-surgical traction, or decompression therapies may also be prescribed. For severe pain, individuals may be offered an epidural steroid injection that can provide pain relief by reducing inflammation. (American Academy of Orthopaedic Surgeons: OrthoInfo. 2022) For spinal stenosis, a provider may first focus on physical therapy to improve overall fitness, strengthen the abdominals and back muscles, and preserve motion in the spine. Pain-relieving medications, including NSAIDs and corticosteroid injections, can reduce inflammation and relieve pain. (American College of Rheumatology. 2023) Physical therapists provide various therapies to decrease symptoms, including manual and mechanical decompression and traction. Surgery may be recommended for cases of radiculopathy that don’t respond to conservative treatments.
Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility, and mobility Fitness Training, and Rehabilitation Systems for all ages. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers to bring El Paso, the top clinical treatments, to our community.
Reclaim Your Mobility: Chiropractic Care For Sciatica Recovery
References
National Institutes of Health: National Institute of Neurological Disorders and Stroke. (2020). Low back pain fact sheet. Retrieved from https://www.ninds.nih.gov/sites/default/files/migrate-documents/low_back_pain_20-ns-5161_march_2020_508c.pdf
American Academy of Orthopaedic Surgeons: OrthoInfo. (2022). Herniated disk in the lower back. https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
American College of Rheumatology. (2023). Spinal stenosis. https://rheumatology.org/patients/spinal-stenosis
For individuals who suffer from migraine headaches, can incorporating physical therapy help decrease pain, improve mobility, and manage future attacks?
Migraine Physical Therapy
Cervicogenic migraine headaches can cause pain, limited motion, or confusing symptoms like dizziness or nausea. They may originate from the neck or cervical spine and be called cervicogenic headaches. A chiropractic physical therapy team can assess the spine and offer treatments that help improve mobility and decrease pain. Individuals may benefit from working with a migraine physical therapy team to perform treatments for specific conditions, quickly and safely relieving pain and returning to their previous level of activity.
Cervical Spine Anatomy
The neck is comprised of seven stacked cervical vertebrae. The cervical vertebrae protect the spinal cord and allow the neck to move through:
Flexion
Extension
Rotation
Side bending
The upper cervical vertebrae help support the skull. There are joints on either side of the cervical level. One connects to the back of the skull and allows motion. This suboccipital area is home to several muscles that support and move the head, with nerves that travel from the neck through the suboccipital area into the head. The nerves and muscles in this area may be a source of neck pain and/or headaches.
Symptoms
Sudden motions can trigger symptoms of cervicogenic migraine, or they may come on during sustained neck postures. (Page P. 2011) The symptoms are often dull and non-throbbing and may last several hours to days. Symptoms of cervicogenic migraine headache may include:
Pain on both sides of the back of the head.
Pain in the back of the head that radiates to one shoulder.
Pain on one side of the upper neck that radiates to the temple, forehead, or eye.
Pain in one side of the face or cheek.
Reduced range of motion in the neck.
Sensitivity to light or sound
Nausea
Dizziness or vertigo
Diagnosis
Tools a physician may use may include:
X-ray
MRI
CT scan
Physical examination includes neck range of motion and palpation of the neck and skull.
When first visiting a physical therapist, they will go through medical history and conditions, and questions will be asked about the onset of pain, symptom behavior, medications, and diagnostic studies. The therapist will also ask about previous treatments and review medical and surgical history. Components of the evaluation may include:
Palpation of the neck and skull
Measures of neck range of motion
Strength measurements
Postural assessment
Once the evaluation is completed, the therapist will work with the individual to develop a personalized treatment program and rehabilitation goals. Various treatments are available.
Exercise
Exercises to improve neck motion and decrease pressure on cervical nerves may be prescribed and may include. (Park, S. K. et al., 2017)
Cervical rotation
Cervical flexion
Cervical side bending
Cervical retraction
The therapist will train the individual to move slowly and steadily and avoid sudden or jerky movements.
Postural Correction
If forward head posture is present, the upper cervical spine and the suboccipital area could compress the nerves that travel up the back of the skull. Correcting posture may be an effective strategy for treatment and can include:
Performing targeted postural exercises.
Utilizing a supportive neck pillow for sleep.
Using a lumbar support when sitting.
Kinesiology taping may help increase tactile awareness of back and neck position and improve overall postural awareness.
Heat/Ice
Heat or ice may be applied to the neck and skull to help decrease pain and inflammation.
Heat can help relax tight muscles and improve circulation and may be used before performing neck stretches.
Massage
If tight muscles are limiting neck motion and causing head pain, a massage can help improve mobility.
A special technique called suboccipital release loosens the muscles that attach the skull to the neck for improved motion and decreased nerve irritation.
Manual and Mechanical Traction
Part of the migraine physical therapy plan may involve mechanical or manual traction to decompress the neck’s discs and joints, improve motion in the neck, and decrease pain.
Joint mobilizations may be used to improve neck motion and manage pain. (Paquin, J. P. 2021)
Electrical Stimulation
Electrical stimulation, like electro-acupuncture or transcutaneous neuromuscular electrical stimulation, may be used on the neck muscles to decrease pain and improve headache symptoms.
Therapy Duration
Most migraine physical therapy sessions for cervicogenic headaches last about four to six weeks. Individuals may experience relief within a few days of starting therapy, or symptoms may come and go in different phases for weeks. Some experience continued migraine headache pain for months after starting treatment and use techniques they learned to help control symptoms.
Injury Medical Chiropractic and Functional Medicine Clinic specializes in progressive therapies and functional rehabilitation procedures focused on restoring normal body functions after trauma and soft tissue injuries. We use Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our natural programs use the body’s ability to achieve specific measured goals. We have teamed up with the city’s premier doctors, therapists, and trainers to provide high-quality treatments that empower our patients to maintain the healthiest way of living and live a functional life with more energy, a positive attitude, better sleep, and less pain.
Chiropractic Care For Migraines
References
Page P. (2011). Cervicogenic headaches: an evidence-led approach to clinical management. International journal of sports physical therapy, 6(3), 254–266.
Headache Classification Committee of the International Headache Society (IHS) (2013). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia : an international journal of headache, 33(9), 629–808. https://doi.org/10.1177/0333102413485658
Rana M. V. (2013). Managing and treating headache of cervicogenic origin. The Medical clinics of North America, 97(2), 267–280. https://doi.org/10.1016/j.mcna.2012.11.003
Park, S. K., Yang, D. J., Kim, J. H., Kang, D. H., Park, S. H., & Yoon, J. H. (2017). Effects of cervical stretching and cranio-cervical flexion exercises on cervical muscle characteristics and posture of patients with cervicogenic headache. Journal of physical therapy science, 29(10), 1836–1840. https://doi.org/10.1589/jpts.29.1836
Paquin, J. P., Tousignant-Laflamme, Y., & Dumas, J. P. (2021). Effects of SNAG mobilization combined with a self-SNAG home-exercise for the treatment of cervicogenic headache: a pilot study. The Journal of manual & manipulative therapy, 29(4), 244–254. https://doi.org/10.1080/10669817.2020.1864960
Footwear can cause lower back pain and problems for some individuals. Can understanding the connection between footwear and back problems help individuals find the right shoes to maintain back health and relieve pain?
Footwear Back Pain
The back provides the strength for physical activities. Back pain affects daily life and can have various causes. Unhealthy posture, walking, twisting, turning, bending, and reaching can contribute to back problems that result in pain. According to the CDC, 39% of adults report living with back pain (Centers for Disease Control and Prevention, 2019). Improper footwear can also contribute to back pain. Selecting footwear carefully can help bring pain relief and help maintain spinal health. Individuals can enjoy less pain and manage symptoms by choosing shoes that maintain spinal alignment and protect the feet from blunt impact.
Understanding the Back Pain-Footwear Connection
Improper footwear could be the cause of lower back pain. What impacts the bones at the bottom of the neuromusculoskeletal system radiates upward and affects the spine and back muscles. What footwear is used travels upward, impacting gait, posture, spinal alignment, and more. When back problems originate from the feet, these are biomechanical issues. Biomechanics means how the bones, joints, and muscles work together and how changes in external forces impact the body.
Movement
When the feet impact the ground, they are the first extremities to absorb shock for the rest of the body. Individuals will start to walk differently if they have a problem or change in their feet. Wearing shoes with improper support can increase the wear and tear on the muscles and joints, leading to awkward and unnatural movement. For example, consider the difference between standing on tiptoes in high heels and the natural flat-footed state. Well-cushioned shoes help absorb impact and lessen pain sensations. The pressures on each of the joints shift balance, which causes instability problems with less pressure on some and more on others. This creates an imbalance that leads to pain and joint conditions.
Posture
Maintaining a healthy posture is another factor in preventing or alleviating back pain. With the right footwear, the body can maintain a healthier stance and the right curvature throughout the spine, and it helps distribute the weight evenly. This results in decreased stress on ligaments, muscles, and joints. (Harvard Health Publishing. 2014) It’s recommended to see an orthopedist to get to the root of an individual’s condition. For some, a herniated disc, sciatica, automobile collision, fall, unhealthy ergonomics, or a combination, as well as other underlying issues, may be contributing to their back pain.
Shoe Types and Their Impact on The Back
How various shoes impact posture, potentially causing or relieving back pain.
High Heels
High heels can definitely contribute to back pain. They change body posture, causing a domino effect on the spine. The body’s weight is shifted to increase pressure on the balls of the feet, and the spine’s alignment becomes altered. High heels also affect how the ankles, knees, and hips move when walking, balance, and how the back muscles operate, all of which can worsen back pain.
Flat Shoes
Flat shoes may not be the best choice for spinal health. If they lack arch support, they can cause the foot to roll inward, known as pronation. This can contribute to misalignment, which can strain the knees, hips, and lower back. However, they can be a decent choice if they provide arch support. When wearing flat shoes with healthy support, the weight is distributed evenly on the feet and the spine. This helps maintain correct posture, which can help prevent and/or alleviate back pain.
Sneakers, Tennis, and Athletic Shoes
Sneakers, tennis, and athletic shoes can relieve back pain with thorough cushioning and support. Choosing the right ones involves determining the activity that will be done in them. There are tennis, running, basketball, pickleball, skating shoes, and more. Research what features will be needed for the sport or activity. This could include:
Heel cups
Insole cushioning
Wide base
Other features to meet individual foot needs.
It is recommended that athletic shoes be changed every 300 to 500 miles of walking or running or with any signs of unevenness when placed on a flat surface, as worn-out soles and degraded materials can increase the risk of injury and back pain. (American Academy of Podiatric Sports Medicine, 2024). If a certain pair puts the legs, hips, or ankles into an unnatural position or impedes regular movement, it may be time to replace them.
Choosing the Right Shoes
The ideal solution for choosing shoe wear is to get a gait analysis and a review of how you walk and run. Various healthcare professionals may offer this service to tailor each individual’s search for the right shoes for back pain. In gait analysis, individuals are asked to run and walk, sometimes on camera, while a professional notes physical tendencies, like when the foot hits the ground and whether it rolls inward or outward. This provides data on affected posture, movement, pain levels, how much arch support is needed, and what type to wear to help prevent back pain. Once the analysis is complete, it will guide you on what to look for, such as what level of arch support, heel height, or material is best for you.
Injury Medical Chiropractic and Functional Medicine Clinic specializes in progressive, cutting-edge therapies and functional rehabilitation procedures focused on clinical physiology, total health, practical strength training, and complete conditioning. We focus on restoring normal body functions after trauma and soft tissue injuries. We use Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our programs are natural and use the body’s ability to achieve specific measured goals rather than introducing harmful chemicals, controversial hormone replacement, unwanted surgeries, or addictive drugs. We have teamed up with the city’s premier doctors, therapists, and trainers to provide high-quality treatments that empower our patients to maintain the healthiest way of living and live a functional life with more energy, a positive attitude, better sleep, and less pain.
Benefits of Using Custom Foot Orthotics
References
Centers for Disease Control and Prevention. (2019). Back, lower limb, and upper limb pain among U.S. adults, 2019. Retrieved from https://www.cdc.gov/nchs/products/databriefs/db415.htm
Harvard Health Publishing. (2014). Posture and back health. Harvard Health Education. https://www.health.harvard.edu/pain/posture-and-back-health
American Academy of Podiatric Sports Medicine. Ayne Furman, D. F., AAPSM. (2024). How do I know when it is time to replace my athletic shoes?
For individuals who are dealing with back pain and problems, could knowing how to improve and maintain intervertebral disc health help alleviate symptoms?
Intervertebral Disc Health
The spinal column comprises 24 movable bones and 33 bones called vertebrae. The vertebral bones are stacked on top of each other. The intervertebral disc is the cushioning substance between the adjacent bones. (Dartmouth. 2008)
Bones
The vertebral bones are small and round in an area called the vertebral body. In the back is a bony ring from which protrusions extend and arches and pathways are formed. Each structure has one or more purposes and includes: (Waxenbaum JA, Reddy V, Williams C, et al., 2023)
Stabilizing the spine.
Providing a space for the connective tissue and back muscles to attach.
Providing a tunnel for the spinal cord to pass through cleanly.
Providing a space where nerves exit and branch out to all areas of the body.
Structure
The intervertebral disc is the cushioning that sits between the vertebrae. The design of the spine allows it to move in various directions:
Flexion or bending
Extension or arching
Tilting and rotation or twisting.
Powerful forces act upon and influence the spinal column to produce these movements. The intervertebral disc absorbs shock during movement and protects the vertebrae and spinal cord from injury and/or trauma.
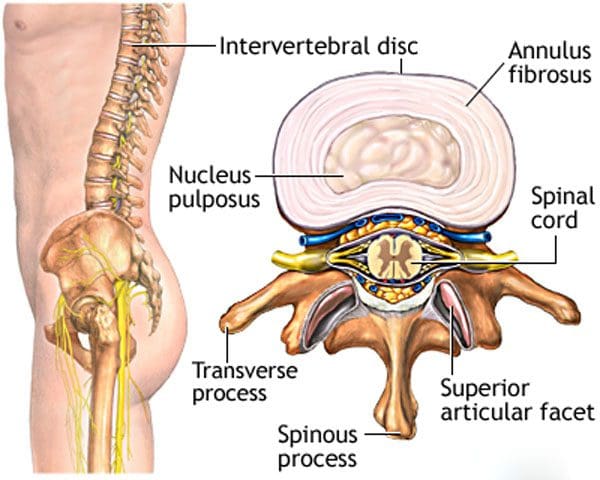
Ability
On the outside, strong woven fiber tissues form an area called the annulus fibrosis. The annulus fibrosis contains and protects the softer gel substance in the center, the nucleus pulposus. (Y.S. Nosikova et al., 2012) The nucleus pulposis provides shock absorption, flexibility, and pliability, especially under pressure during spinal movement.
Mechanics
The nucleus pulposus is a soft gel substance located in the center of the disc that allows elasticity and flexibility under stress forces to absorb compression. (Nedresky D, Reddy V, Singh G. 2024) The swivel action alters the tilt and rotation of the vertebra above and below, buffering the effects of spinal motion. The discs swivel in response to the direction the spine moves. The nucleus pulposus is made mostly of water, which moves in and out through small pores, acting as byways between the vertebra and disc bone. Body positions that load the spine, like sitting and standing, push the water out of the disc. Lying down on the back or in a supine position facilitates water restoration into the disc. As the body ages, the discs lose water/dehydrate, leading to disc degeneration. The intervertebral disc has no blood supply, which means that for a disc to receive necessary nutrition and for waste removal, it must rely on water circulation to stay healthy.
Care
Some ways of maintaining intervertebral disc health include:
Paying attention to posture.
Changing positions frequently throughout the day.
Exercising and moving around.
Applying correct body mechanics to physical activities.
Sleeping on a supportive mattress.
Drinking plenty of water.
Eating healthy.
Maintaining a healthy weight.
Drinking alcohol in moderation.
Quitting smoking.
At Injury Medical Chiropractic and Functional Medicine Clinic, we treat injuries and chronic pain syndromes by improving an individual’s ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. Our chiropractic team, care plans, and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Acupuncture, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Beyond the Surface: Understanding the Effects of Personal Injury
References
Dartmouth Ronan O’Rahilly, MD. (2008). Basic Human Anatomy. Chapter 39: The vertebral column. In D. Rand Swenson, MD, PhD (Ed.), BASIC HUMAN ANATOMY A Regional Study of Human Structure. W.B. Saunders. https://humananatomy.host.dartmouth.edu/BHA/public_html/part_7/chapter_39.html
Waxenbaum, J. A., Reddy, V., Williams, C., & Futterman, B. (2024). Anatomy, Back, Lumbar Vertebrae. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/29083618
Nosikova, Y. S., Santerre, J. P., Grynpas, M., Gibson, G., & Kandel, R. A. (2012). Characterization of the annulus fibrosus-vertebral body interface: identification of new structural features. Journal of anatomy, 221(6), 577–589. https://doi.org/10.1111/j.1469-7580.2012.01537.x
Nedresky D, Reddy V, Singh G. (2024). Anatomy, Back, Nucleus Pulposus. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30570994
Can knowing treatment options for a dislocated hip help individuals expedite rehabilitation and recovery?
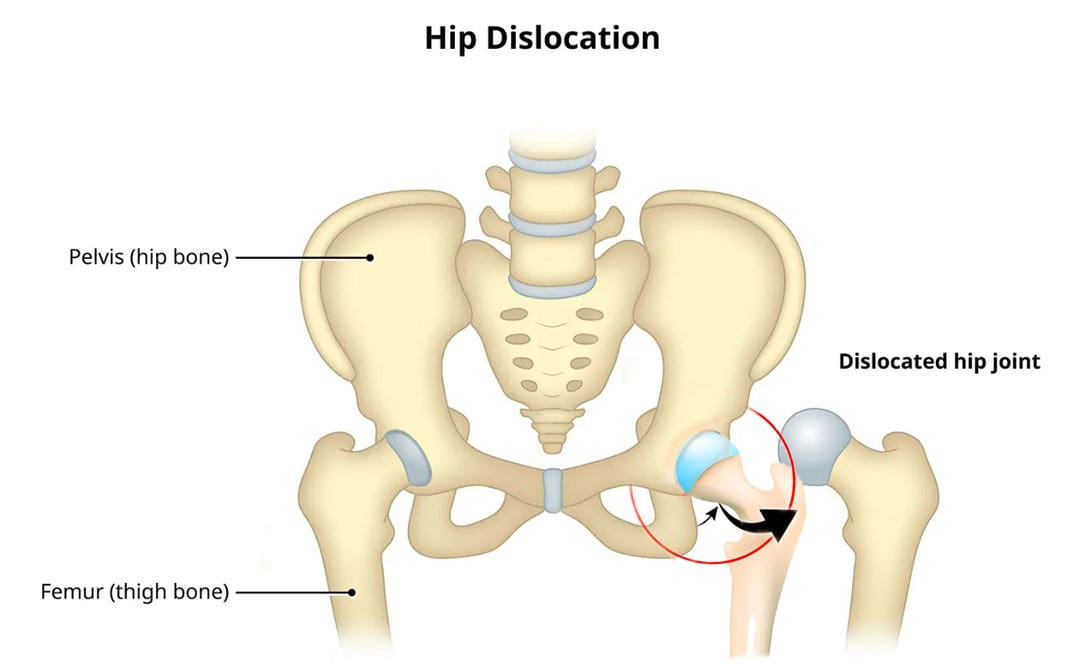
Dislocated Hip
A dislocated hip is an uncommon injury but can happen due to trauma or following hip replacement surgery. It usually occurs after severe trauma, including motor vehicle collisions, falls, and sometimes sports injuries. (Caylyne Arnold et al., 2017) A dislocated hip can also occur after hip replacement surgery. Other injuries like ligament tears, cartilage damage, and bone fractures can occur alongside the dislocation. Most hip dislocations are treated with a joint reduction procedure that resets the ball into the socket. It is usually done with sedation or general anesthesia. Rehabilitation takes time and could be a few months before full recovery. Physical therapy can help restore motion and strength in the hip.
What Is It?
If the hip is only partially dislocated, it’s called a hip subluxation. When this happens, the hip joint head only partially emerges from the socket. A dislocated hip is when the head or ball of the joint shifts or pops out of the socket. Because an artificial hip differs from a normal hip joint, the risk of dislocation increases after joint replacement. A study found that around 2% of individuals who undergo total hip replacement will experience hip dislocation within a year, with the cumulative risk increasing by approximately 1% over five years. (Jens Dargel et al., 2014) However, new technological prosthetics and surgical techniques are making this less common.
Hip Anatomy
The hip ball-and-socket joint is called the femoroacetabular joint.
The socket is called the acetabulum.
The ball is called the femoral head.
The bony anatomy and strong ligaments, muscles, and tendons help to create a stable joint. Significant force must be applied to the joint for a hip dislocation to occur. Some individuals report feeling a snapping sensation of the hip. This usually is not a hip dislocation but indicates a different disorder known as snapping hip syndrome. (Paul Walker et al., 2021)
Posterior Hip Dislocation
Around 90% of hip dislocations are posterior.
In this type, the ball is pushed backward from the socket.
A hip dislocation increases the risk of developing joint arthritis following the injury and can raise the risk of needing a hip replacement later in life. (Hsuan-Hsiao Ma et al., 2020)
Developmental Dislocation of the Hip
Some children are born with developmental dislocation of the hip or DDH.
Children with DDH have hip joints that did not form correctly during development.
This causes a loose fit in the socket.
In some cases, the hip joint is completely dislocated.
Joint reduction is the most common way to treat a dislocated hip. The procedure repositions the ball back into the socket and is usually done with sedation or under general anesthesia. Repositioning a hip requires significant force. A hip dislocation is considered an emergency, and reduction should be performed immediately after the dislocation to prevent permanent complications and invasive treatment. (Caylyne Arnold et al., 2017)
Once the ball is back in the socket, the healthcare provider will look for bone, cartilage, and ligament injuries.
Depending on what the healthcare provider finds, further treatment may be necessary.
Fractured or broken bones may need to be repaired to keep the ball within the socket.
Damaged cartilage may have to be removed.
Surgery
Surgery could be necessary to return the joint to its normal position. Hip arthroscopy can minimize the invasiveness of certain procedures. A surgeon inserts a microscopic camera into the hip joint to help the surgeon repair the injury using instruments inserted through other small incisions.
Hip replacement surgery replaces the ball and socket, a common and successful orthopedic surgical procedure. This surgery may be performed for various reasons, including trauma or arthritis, as it is common to develop early arthritis of the hip after this type of trauma. This is why many who have a dislocation ultimately need hip replacement surgery. As a major surgical procedure, it is not without risks. Possible complications include:
Infection
Aseptic loosening (the loosening of the joint without infection)
Hip dislocation
Recovery
Recovering from a hip dislocation is a long process. Individuals will need to walk with crutches or other devices early in recovery. Physical therapy will improve the range of motion and strengthen the muscles around the hip. Recovery time will depend on whether other injuries, such as fractures or tears, are present. If the hip joint was reduced and there were no other injuries, it may take six to ten weeks to recover to the point where weight can be placed on the leg. It could be between two and three months for a full recovery. Keeping weight off the leg is important until the surgeon or physical therapist gives the all-clear. Injury Medical Chiropractic and Functional Medicine Clinic will work with an individual’s primary healthcare provider and other surgeons or specialists to develop an optimal personalized treatment plan.
Chiropractic Solutions for Osteoarthritis
References
Arnold, C., Fayos, Z., Bruner, D., Arnold, D., Gupta, N., & Nusbaum, J. (2017). Managing dislocations of the hip, knee, and ankle in the emergency department [digest]. Emergency medicine practice, 19(12 Suppl Points & Pearls), 1–2.
Dargel, J., Oppermann, J., Brüggemann, G. P., & Eysel, P. (2014). Dislocation following total hip replacement. Deutsches Arzteblatt international, 111(51-52), 884–890. https://doi.org/10.3238/arztebl.2014.0884
Walker, P., Ellis, E., Scofield, J., Kongchum, T., Sherman, W. F., & Kaye, A. D. (2021). Snapping Hip Syndrome: A Comprehensive Update. Orthopedic reviews, 13(2), 25088. https://doi.org/10.52965/001c.25088
Cornwall, R., & Radomisli, T. E. (2000). Nerve injury in traumatic dislocation of the hip. Clinical orthopaedics and related research, (377), 84–91. https://doi.org/10.1097/00003086-200008000-00012
American Academy of Orthopaedic Surgeons. (2021). Hip dislocation. https://orthoinfo.aaos.org/en/diseases–conditions/hip-dislocation
Kellam, P., & Ostrum, R. F. (2016). Systematic Review and Meta-Analysis of Avascular Necrosis and Posttraumatic Arthritis After Traumatic Hip Dislocation. Journal of orthopaedic trauma, 30(1), 10–16. https://doi.org/10.1097/BOT.0000000000000419
Ma, H. H., Huang, C. C., Pai, F. Y., Chang, M. C., Chen, W. M., & Huang, T. F. (2020). Long-term results in the patients with traumatic hip fracture-dislocation: Important prognostic factors. Journal of the Chinese Medical Association : JCMA, 83(7), 686–689. https://doi.org/10.1097/JCMA.0000000000000366
American Academy of Orthopaedic Surgeons. (2022). Developmental dislocation (dysplasia) of the hip (DDH). https://orthoinfo.aaos.org/en/diseases–conditions/developmental-dislocation-dysplasia-of-the-hip-ddh/
Can incorporating acupressure provide effective relief and benefits for individuals looking to try natural treatments for common health ailments?
Acupressure
Acupressure is a type of complementary medicine that is rising in popularity due to its simplicity and accessibility. It can assist in treating various diseases and conditions. (Piyush Mehta et al., 2016) Anyone can learn it, and no special equipment is required. It is an effective and safe therapeutic option with no known side effects. (Youngmi Cho et al., 2021) It is a cost-effective intervention similar to acupuncture. (Lukas Israel et al., 2021)
What Is It?
The concept of acupressure activates acupoints or pressure points across meridians or channels connected to various organs to balance energy and promote health. Practitioners believe that the quality or state of a person’s energy determines their health. (Piyush Mehta et al., 2016) Acupressure is the stimulation of acupoints using either the fingers or a tool. Massage techniques like Amma, Shiatsu, Tui Na, and Thai massage incorporate acupressure in their treatments and follow the same energy channels as acupuncture.
The Way It Works
Acupressure works similarly to acupuncture. The Gate Control Theory theorizes that pleasure impulses reach the brain four times faster than pain impulses. Continuous pleasurable impulses close the neural gates and block slower messages, like pain. According to this theory, acupressure improves the pain perception threshold. (Piyush Mehta et al., 2016) Stimulating acupoints activates functional responses, like releasing hormones. These hormones serve various functions, physical, like regulating organ function, and mental, like regulating emotions, and releasing them can help improve health and well-being. (Piyush Mehta et al., 2016)
Acupressure is a simple and effective intervention that can be self or professionally administered.
Acupoints are activated in the elbows, fingers, feet, knuckles, palms, or thumbs.
Though acupressure doesn’t require specialized tools, they are available for convenience.
Some practitioners used Bian stones to activate acupoints.
Acupressure is often used alongside modern medicine, as it treats common or coexisting symptoms, such as anxiety or stress. Some of the conditions for which acupressure may be effective include.
Stress and Fatigue Reduction
Stress and fatigue are common but often arise alongside other ailments or conditions if persistent or severe, anxiety and fatigue can significantly affect quality of life by reducing an individual’s ability to participate in daily activities. In a study looking at shift work nurses who experience stress and fatigue from the intensity of their work, acupressure significantly reduced their symptoms. (Youngmi Cho et al., 2021) In studies with breast cancer survivors, acupressure was also used to decrease fatigue levels and was shown to be an effective and low-cost option for managing persistent fatigue alongside standard care for breast cancer. (Suzanna Maria Zick et al., 2018) (Suzanna M Zick et al., 2016)
Can Help With Anxiety and Depression
Depression and anxiety can be part of a disorder or exist on their own. Acupressure may help alleviate some of the anxiety and depression that arise as part of a condition or ailment. In the shift work nurses study, acupressure helped decrease anxiety levels. (Youngmi Cho et al., 2021) In other studies, acupressure reduced anxiety scores and improved depressive symptoms in individuals with mild to moderate symptoms. (Elizabeth Monson et al., 2019) (Jingxia Lin et al., 2022) (Suzanna Maria Zick et al., 2018)
Pain Reduction
Individuals experience physical pain for a variety of reasons. Pain can come from temporary sports injuries, work, sudden awkward movements, and/or chronic illness. Acupressure can effectively reduce pain as a complementary therapy. (Elizabeth Monson et al., 2019) In a study, athletes who had a musculoskeletal sports injury reported decreased pain intensity after three minutes of acupressure therapy. (Aleksandra K Mącznik et al., 2017) In another study, breast cancer survivors showed significant improvements with acupressure. (Suzanna Maria Zick et al., 2018)
Nausea Relief
Nausea and vomiting are conditions that are common for those who are pregnant or undergoing chemotherapy. It also can be a medication side effect or arise with migraine or indigestion. There is evidence that acupressure may be effective in alleviating symptoms. Some researchers believe a particular type of acupressure known as auricular acupressure is the most effective for treating chemotherapy-induced nausea and vomiting alongside standard treatment. (Jing-Yu Tan et al., 2022) However, further research is needed to determine whether this is a viable, ongoing option for treating nausea and vomiting. (Heather Greenlee et al., 2017)
Sleep Better
Acupressure can be an effective and low-cost option for managing breast cancer symptoms. One study found relaxing acupressure techniques improved sleep quality and quality of life in breast cancer survivors. Additionally, researchers note that relaxing acupressure is more effective for improving sleep and quality of life than stimulating acupressure. (Suzanna M Zick et al., 2016)
Allergy Reduction
Allergic rhinitis is inflammation caused by an allergic reaction. Previous trials have found that acupressure could improve overall health by reducing seasonal allergic rhinitis symptoms and the need for allergy medication. (Lukas Israel et al., 2021) Researchers also noted that individuals are likely to adhere to self-applied acupressure therapy as a form of self-massage. (Lukas Israel et al., 2021)
Always consult a healthcare provider before starting acupressure treatments, especially if you have any pre-existing health conditions. At Injury Medical Chiropractic and Functional Medicine Clinic, we treat injuries and chronic pain syndromes by developing personalized treatment plans and specialized clinical services focused on injuries and the complete recovery process. Flexibility, mobility, and agility programs are tailored for all age groups and disabilities. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Enhance Performance with Functional Foot Orthotics
References
Mehta, P., Dhapte, V., Kadam, S., & Dhapte, V. (2016). Contemporary acupressure therapy: Adroit cure for painless recovery of therapeutic ailments. Journal of traditional and complementary medicine, 7(2), 251–263. https://doi.org/10.1016/j.jtcme.2016.06.004
Cho, Y., Joo, J. M., Kim, S., & Sok, S. (2021). Effects of Meridian Acupressure on Stress, Fatigue, Anxiety, and Self-Efficacy of Shiftwork Nurses in South Korea. International journal of environmental research and public health, 18(8), 4199. https://doi.org/10.3390/ijerph18084199
Israel, L., Rotter, G., Förster-Ruhrmann, U., Hummelsberger, J., Nögel, R., Michalsen, A., Tissen-Diabaté, T., Binting, S., Reinhold, T., Ortiz, M., & Brinkhaus, B. (2021). Acupressure in patients with seasonal allergic rhinitis: a randomized controlled exploratory trial. Chinese medicine, 16(1), 137. https://doi.org/10.1186/s13020-021-00536-w
Zick, S. M., Sen, A., Hassett, A. L., Schrepf, A., Wyatt, G. K., Murphy, S. L., Arnedt, J. T., & Harris, R. E. (2018). Impact of Self-Acupressure on Co-Occurring Symptoms in Cancer Survivors. JNCI cancer spectrum, 2(4), pky064. https://doi.org/10.1093/jncics/pky064
Zick, S. M., Sen, A., Wyatt, G. K., Murphy, S. L., Arnedt, J. T., & Harris, R. E. (2016). Investigation of 2 Types of Self-administered Acupressure for Persistent Cancer-Related Fatigue in Breast Cancer Survivors: A Randomized Clinical Trial. JAMA oncology, 2(11), 1470–1476. https://doi.org/10.1001/jamaoncol.2016.1867
Monson, E., Arney, D., Benham, B., Bird, R., Elias, E., Linden, K., McCord, K., Miller, C., Miller, T., Ritter, L., & Waggy, D. (2019). Beyond Pills: Acupressure Impact on Self-Rated Pain and Anxiety Scores. Journal of alternative and complementary medicine (New York, N.Y.), 25(5), 517–521. https://doi.org/10.1089/acm.2018.0422
Lin, J., Chen, T., He, J., Chung, R. C., Ma, H., & Tsang, H. (2022). Impacts of acupressure treatment on depression: A systematic review and meta-analysis. World journal of psychiatry, 12(1), 169–186. https://doi.org/10.5498/wjp.v12.i1.169
Mącznik, A. K., Schneiders, A. G., Athens, J., & Sullivan, S. J. (2017). Does Acupressure Hit the Mark? A Three-Arm Randomized Placebo-Controlled Trial of Acupressure for Pain and Anxiety Relief in Athletes With Acute Musculoskeletal Sports Injuries. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine, 27(4), 338–343. https://doi.org/10.1097/JSM.0000000000000378
Tan, J. Y., Molassiotis, A., Suen, L. K. P., Liu, J., Wang, T., & Huang, H. R. (2022). Effects of auricular acupressure on chemotherapy-induced nausea and vomiting in breast cancer patients: a preliminary randomized controlled trial. BMC complementary medicine and therapies, 22(1), 87. https://doi.org/10.1186/s12906-022-03543-y
Greenlee, H., DuPont-Reyes, M. J., Balneaves, L. G., Carlson, L. E., Cohen, M. R., Deng, G., Johnson, J. A., Mumber, M., Seely, D., Zick, S. M., Boyce, L. M., & Tripathy, D. (2017). Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA: a cancer journal for clinicians, 67(3), 194–232. https://doi.org/10.3322/caac.21397
Ho, K. K., Kwok, A. W., Chau, W. W., Xia, S. M., Wang, Y. L., & Cheng, J. C. (2021). A randomized controlled trial on the effect of focal thermal therapy at acupressure points treating osteoarthritis of the knee. Journal of orthopaedic surgery and research, 16(1), 282. https://doi.org/10.1186/s13018-021-02398-2
Certain neurological disorders can cause acute episodes of peripheral neuropathy, and for individuals diagnosed with chronic peripheral neuropathy, can physical therapy help improve the ability to move around safely along with medications, procedures, and lifestyle adjustments to help control and manage symptoms?
Peripheral Neuropathy Treatments
Peripheral neuropathy treatment includes symptomatic therapies and medical management to help prevent worsening nerve damage.
For acute types of peripheral neuropathy, medical interventions and therapies can treat the underlying process, improving the condition.
For chronic types of peripheral neuropathy, medical interventions and lifestyle factors can help to prevent the condition’s progression.
Chronic peripheral neuropathy treatment focuses on controlling the pain symptoms and protecting areas of diminished sensation from damage or infection.
Self-Care and Lifestyle Adjustments
For individuals who have been diagnosed with peripheral neuropathy or are at risk of developing the condition, lifestyle factors play a significant role in managing symptoms and preventing nerve damage from worsening and can even prevent the condition from developing. (Jonathan Enders et al., 2023)
Pain Management
Individuals can try these self-care therapies and see if and which help reduce their discomfort and then develop a routine that they can work off of. Self-care for pain symptoms include:
Placing a warm heating pad on painful areas.
Placing a cooling pad (not ice) on painful areas.
Covering the area or leaving it uncovered, depending on comfort levels.
Wear loose-fitting clothes, socks, shoes, and/or gloves not made with material that can cause irritation.
Avoid using lotions or soaps that can cause irritation.
Use soothing creams or lotions.
Keeping the painful areas clean.
Injuries Prevention
Diminished sensation is one of the most common effects that can lead to problems like stumbling, difficulty getting around, and injuries. Preventing and regularly checking for injuries can help avoid complications like infected wounds. (Nadja Klafke et al., 2023) Lifestyle adjustments to manage and prevent injuries include:
Wear well-padded shoes and socks.
Inspect feet, toes, fingers, and hands regularly to look for cuts or bruises that may not have been felt.
Clean and cover cuts to avoid infections.
Use extra caution with sharp utensils like cooking and work or gardening tools.
Disease Management
Lifestyle factors can help prevent disease progression and are closely correlated with the risks and underlying causes. To help prevent peripheral neuropathy or its progression can be done by: (Jonathan Enders et al., 2023)
Maintain healthy glucose levels if you have diabetes.
Avoid alcohol for any peripheral neuropathy.
Maintain a well-balanced diet, which can include vitamin supplements, especially for vegetarians or vegans.
Over-the-Counter Therapies
A few over-the-counter therapies can help with painful symptoms and can be taken as needed. Over-the-counter pain therapies include: (Michael Überall et al., 2022)
Topical lidocaine spray, patch, or creams.
Capsaicin creams or patches.
Topical Icy Hot
Non-steroidal anti-inflammatory medications – Advil/ibuprofen or Aleve/naproxen
Tylenol/acetaminophen
These treatments can help relieve painful symptoms of peripheral neuropathy, but they do not help improve diminished sensation, weakness, or coordination problems. (Jonathan Enders et al., 2023)
Prescription Therapies
Prescription therapies for treating peripheral neuropathy include pain medications and anti-inflammatories. Chronic types of peripheral neuropathy include:
Alcoholic neuropathy
Diabetic neuropathy
Chemotherapy-induced neuropathy
The prescription treatments for chronic types differ from the treatments for acute types of peripheral neuropathy.
Pain Management
Prescription treatments can help manage the pain and discomfort. Medications include (Michael Überall et al., 2022)
Sometimes, a prescription strength supplement or vitamin B12 given through injection can help prevent progression when peripheral neuropathy is associated with a severe vitamin deficiency. Prescription treatment can help treat the underlying process in some types of acute peripheral neuropathy. Treatment for acute peripheral neuropathy, such as Miller-Fisher syndrome or Guillain-Barré syndrome, can include:
Corticosteroids
Immunoglobulins – immune system proteins
Plasmapheresis is a procedure that removes the liquid portion of blood, returning the blood cells, which modifies the overactivity of the immune system. (Sanja Horvat et al., 2022)
Researchers believe there is an association between these conditions and inflammatory nerve damage, and modifying the immune system is beneficial for treating symptoms and the underlying disease.
Surgery
In some cases, surgical procedures can benefit individuals who have certain types of peripheral neuropathy. When another condition is exacerbating the symptoms or process of peripheral neuropathy, surgery may help relieve symptoms and prevent disease progression. This has proved effective when nerve entrapment or vascular insufficiency are factors. (Wenqiang Yang et al., 2016)
Complementary and Alternative Medicine
Some complementary and alternative approaches can help individuals cope with the pain and discomfort. These treatments can serve as an ongoing option for those who have chronic peripheral neuropathy. Options can include: (Nadja Klafke et al., 2023)
Acupuncture involves the placement of needles in specific areas of the body to help reduce pain symptoms.
Acupressure involves applying pressure on specific areas of the body to help reduce pain symptoms.
Massage therapy can help relax muscle tension.
Meditation and relaxation therapies can help manage symptoms.
Physical therapy can also serve as an important component of living with chronic peripheral neuropathy and recovering from acute peripheral neuropathy.
Physical therapy can help strengthen weak muscles, improve coordination, and learn how to adapt to sensory and motor changes to get around safely.
Individuals considering complementary or alternative treatment are encouraged to speak with their primary healthcare provider to determine whether it is safe for their condition. Injury Medical Chiropractic and Functional Medicine Clinic will work with the individual’s healthcare provider and/or specialists to develop an optimal health and wellness treatment solution to provide pain relief and improve quality of life.
Peripheral Neuropathy: A Successful Recovery Story
References
Enders, J., Elliott, D., & Wright, D. E. (2023). Emerging Nonpharmacologic Interventions to Treat Diabetic Peripheral Neuropathy. Antioxidants & redox signaling, 38(13-15), 989–1000. https://doi.org/10.1089/ars.2022.0158
Klafke, N., Bossert, J., Kröger, B., Neuberger, P., Heyder, U., Layer, M., Winkler, M., Idler, C., Kaschdailewitsch, E., Heine, R., John, H., Zielke, T., Schmeling, B., Joy, S., Mertens, I., Babadag-Savas, B., Kohler, S., Mahler, C., Witt, C. M., Steinmann, D., … Stolz, R. (2023). Prevention and Treatment of Chemotherapy-Induced Peripheral Neuropathy (CIPN) with Non-Pharmacological Interventions: Clinical Recommendations from a Systematic Scoping Review and an Expert Consensus Process. Medical sciences (Basel, Switzerland), 11(1), 15. https://doi.org/10.3390/medsci11010015
Überall, M., Bösl, I., Hollanders, E., Sabatschus, I., & Eerdekens, M. (2022). Painful diabetic peripheral neuropathy: real-world comparison between topical treatment with lidocaine 700 mg medicated plaster and oral treatments. BMJ open diabetes research & care, 10(6), e003062. https://doi.org/10.1136/bmjdrc-2022-003062
Horvat, S., Staffhorst, B., & Cobben, J. M. G. (2022). Intravenous Lidocaine for Treatment of Chronic Pain: A Retrospective Cohort Study. Journal of pain research, 15, 3459–3467. https://doi.org/10.2147/JPR.S379208
Yang, W., Guo, Z., Yu, Y., Xu, J., & Zhang, L. (2016). Pain Relief and Health-Related Quality-of-Life Improvement After Microsurgical Decompression of Entrapped Peripheral Nerves in Patients With Painful Diabetic Peripheral Neuropathy. The Journal of foot and ankle surgery: official publication of the American College of Foot and Ankle Surgeons, 55(6), 1185–1189. https://doi.org/10.1053/j.jfas.2016.07.004
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




 Shoe Types and Their Impact on The Back
Shoe Types and Their Impact on The Back
 Ability
Ability