Bobby Gomez describes how each visit with Dr. Alex Jimenez and to PUSH Fitness with Daniel Alvarado has resulted in great improvements in the stability of his shoulders as well as in the placement of his hips. Although Bobby Gomez’s recovery has been progressing gradually, he discusses the tremendous changes he has experienced mentally, emotionally and physically. Bobby Gomez highly recommends Dr. Alex Jimenez as the non-surgical choice for neck and back pain, as well as shoulder and hip pain.
Shoulder Pain Treatment
Cerebral palsy (commonly known as CP) affects ordinary motion in various areas of the human body and has many degrees of severity. CP causes problems with posture, gait, muscle tone and coordination of movement. Some children with CP have coexisting conditions, such as eyesight and hearing impairment. These disorders are brought on by brain damage and aren’t a direct result of cerebral palsy. Cerebral palsy does not affect life expectancy. Based on the way in which the condition is handled, motor abilities can improve or decrease over time. While severity and symptoms vary, most individuals with this condition go on to direct a rich, fulfilling life.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Truide Torres recibi� atenci�n quiropr�ctica con la Dra. Alex Jim�nez debido al dolor que experiment� a lo largo de su espalda baja, caderas y piernas. Ella fue diagnosticada con dolor en el nervio ci�tico, com�nmente conocida como ci�tica. La ci�tica puede ocurrir cuando los discos intervertebrales, que se encuentran a lo largo de la columna vertebral, comprimen o afectan el nervio ci�tico en la parte inferior de la espalda. Truide Torres experiment� un alivio tremendo de sus s�ntomas una vez que recibi� atenci�n quiropr�ctica con la Dra. Alex Jimenez y pudo regresar a sus actividades cotidianas. Truide Torres recomienda altamente la atenci�n quiropr�ctica para el dolor del nervio ci�tico.
Tratamiento de Ci�tica
Los doctores en Quiropr�ctica (DC) regularmente tratan la ci�tica. La ci�tica se caracteriza por un dolor que se origina en la parte inferior de la espalda o las nalgas, que se desplaza hacia una o ambas piernas. El dolor del nervio ci�tico var�a en intensidad y frecuencia. La ci�tica generalmente es provocada por la compresi�n del nervio ci�tico. Los trastornos conocidos por causar ci�tica incluyen subluxaciones de la columna lumbar (cuerpos vertebrales desalineados), discos herniados o abultados (discos deslizados), embarazo y parto, tumores y dolencias no espinales como diabetes, estre�imiento o estar sentado en el bolsillo trasero. El dolor a menudo es sordo, doloroso, agudo, como un diente, alfileres y agujas o similar a las descargas el�ctricas. Otros s�ntomas relacionados con la ci�tica incluyen sensaci�n de ardor, entumecimiento y hormigueo.tor.
Tenemos la bendici�n de presentarle la Cl�nica Premier de bienestar y lesiones de El Paso.
Como Cl�nica de Rehabilitaci�n Quiropr�ctica y Centro de Medicina Integrada de El Paso, nos enfocamos apasionadamente en tratar pacientes despu�s de lesiones frustrantes y s�ndromes de dolor cr�nico. Nos enfocamos en mejorar su capacidad a trav�s de programas de flexibilidad, movilidad y agilidad dise�ados para todos los grupos de edad y discapacidades.
Si ha disfrutado de este video y / o le hemos ayudado de alguna manera, no dude en suscribirse y compartirnos.
Chiropractor Near Me: Due to his previous back injury history, George Lara suffered a recent back injury which he was unfortunately unable to recover from through traditional treatment. That’s when the VA recommended him to seek chiropractic care with Dr. Alex Jimenez, ultimately changing his quality of life. George Lara had degenerative disc disease, or DDD, and sciatic nerve pain before receiving treatment with Dr. Alex Jimenez. George Lara describes how much his life has improved with chiropractic care and he’s grateful of the services and care he received. George Lara recommends Dr. Alex Jimenez as the non-surgical choice for back pain, among other spine health issues.
Chiropractor Near Me
Chiropractic care is a means to diagnose and treat health problems that affect the nerves, muscles, bones, and joints of the body. A healthcare provider who supplies chiropractic care is known as a chiropractor. Adjustment of the spine, known as manipulation, is the basis of care. Chiropractors also use other kinds of treatments. Your physician will ask about your goals for your health history and therapy. It’s important to inform your physician about any physical problems you may have which make it difficult for you to do particular things.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
You try to do all the right things when it comes to taking care of your spine. You lift the right way, exercise, practice good posture, stretch, drink plenty of water, and take frequent breaks to walk around if you are seated for an extended period of time. Those are all excellent habits to keep, but there is something else that you should be doing � and it is one of the most overlooked and undervalued health practices. Rest!
Running On Empty: The Silent Epidemic
Stress can do severe damage to your emotional and mental health, but it can also hurt your body as well. Many people carry stress in their lower backs which means that when stress goes up it can result in lower back pain. It can also make you more sensitive to pain.
It is estimated that 66 percent of all doctor visits have a stress related component. What�s more, 50 percent of people who suffer from stress rate it as moderate to high. We live in a culture that makes it commonplace to run on empty. The problem with that is sooner or later you are going to crash and your body will bear the brunt.
Rest is important for helping you alleviate and manage stress, but recent studies show that 1 in 3 adults don�t get enough sleep. There is another reason to get your seven to nine hours in, though, that is directly related to spinal health.
What Rest Can Do For Your Spinal Health
When you rest you give your body time to replenish depleted stores of energy. Adequate sleep improves your immune function, memory, metabolism, learning, and healing. You will be more alert, happier, and have more energy. It is also very beneficial is you are trying to lose weight.
Excess weight can put pressure on your spine and cause it to curve, causing back pain. This is especially true if you carry your weight in your abdomen. That extra weight in the front pulls your spine into a sway back curve making it painful to stand for long periods of time.
When you lay down and rest you allow your entire spine, associated muscles, and other parts of your body to rejuvenate and relax. You probably don�t realize it, but your muscles in your back and abdomen work all day to keep your body properly supported. Even when sitting there are muscles engaged. Laying down allows all of those muscles to finally relax.
Rest also allows your spinal discs to rehydrate. The spine is made up of fluid filled discs that sit between the vertebrae, acting as a cushion. As you go about your day, thanks to gravity, your discs become compressed. This compression causes the disc to lose fluid (which is about 88 percent water). This can cause pain if the discs are not properly rehydrated � and that is a two-step process of drinking adequate water and getting enough rest.
Drinking water will put the fluids into your body, but as long as you are upright, the compression will continue. Laying down to go to sleep takes that pressure off of your spine so there is no compression and the body can naturally rehydrate the discs. A few hours here and there is not really effective because it does not give the body enough time to do its job. This means that you need to get the recommended seven to nine hours of sleep each night.
Along with all the other great, healthy reasons to get a good night�s sleep, you not have one more to add to the list. A healthy spine will keep you standing tall and help keep you mobile, It is important to do all you can to take care of it.
Injury Medical Clinic: Neck Pain Care & Treatments
Posture Tips: Good posture is more important than many people realize. Many a mother has followed her child around, reminding him or her to �stand up straight!� Not everyone knows all the reasons that this is important, but they should. Good posture is essential to good spinal health as well as good overall health.
People with good posture sleep better, feel better, and have fewer aches and pains in the joints, back, neck, and head. It helps you have better digestion, improves your organ function, and helps to make your chiropractic treatments even more effective. These top posture tips will help you stand straight and tall while enjoying better health.
Posture Tips
Posture Tips: Be Aware
Being aware of poor posture is the first step in being able to correct it. When you feel your spine starts to curve, your shoulders hunch, or your back sway, stop and take a moment to pull your body back into proper alignment. Pretend that there is a string that goes through your entire body from the top of your head.
In your mind, pull that string up, raising your chin slightly so that it is parallel to the floor. Pull your shoulders back and allow your arms to hang naturally at your side. Bend your knees slightly (soft knees) with your feet about shoulder width apart. Tuck in your stomach and roll your pelvis forward so your back is not swayed. Keep your weight mostly on the balls of your feet. Think tall. Take deep breaths and allow yourself to get an idea of what this, good posture, feels like.
Posture Tips: Use The Wall
Using the wall or floor can help you get a feel for how to shift your pelvis. If you have a habit of tilting your pelvis back so that you have a sway back, you need to learn how to roll it forward to get it straight.
A person can develop a sway back out of habit, due to injury, or if they carry a lot of abdominal fat. It can cause a great deal of pain and just making the adjustment to straighten your spine will make a tremendous difference.
To get the feel for straightening your back, stand flat against a wall. Keep your feet directly under you. Now try to press the small of your back into the wall. Feel how your body shifts as your pelvis rolls forward. Pay attention to that sensation so you can duplicate it without using the wall. You can also do this while lying on your back with your knees slightly bent. Practice arching your back and then pressing it against the floor to get a feel for that motion.
Posture Tips: Stay Active
Regular exercise and stretching are very important for good posture. What many people don�t realize, though, is that good posture is absolutely vital while you are exercising. This is called �form.� You need to practice good form while you are doing weight bearing exercises, cardio, and stretching. If you don�t it can lead to injury or pain.
Your chiropractor can advise you on various exercises and the proper form for them. If you work out at a gym or at home, learn about good form for the exercises that you do. Fitness professionals can help you with this and are well worth the investment.
Posture Tips: Get Regular Chiropractic Treatment
Chiropractic treatments can help correct poor posture, but even if you are working on it yourself it is important to get regular chiropractic care. There are several reasons for this. First, your chiropractor can make adjustments to your spine, providing you with a much wider range of motion and better mobility. Your chiropractor can also recommend exercises for you and show you how to do them properly. If you have weight issues he or she can provide you with advice on diet and lifestyle changes. Taking advantage of the whole body wellness that chiropractic offers will not only improve your posture, it will improve your life.
Why Chiropractic Combined With Glucosamine & Chondroitin Sulfates Are A Win-Win For Degenerative Disc Disease Sufferers.
The most effective treatments are often found in the natural ones. The human body has this incredible ability to provide its own healing. Often we can aid that process through nutrition, exercise, and lifestyle changes. While there are some people who do reach for medications and invasive means of pain control, the truth is the best cure is the natural one. This is also true of degenerative disc disease. There are several natural treatments that help relieve the pain and even stop the progression of the disease. Common treatments include chiropractic, glucosamine, and chondroitin sulfates.
What Is Degenerative Disc Disease (DDD)?
In a healthy spine the discs that lie between the vertebrae and cushion them are filled with fluid. They allow the spine to move, flex, bend, and twist. Over time they may lose some of their cushion as part of the aging process.
Degenerative disc disease occurs when the discs of the spine collapse and degrade. In extreme cases, the discs can completely collapse causing the vertebrae�s facet joints to rub against each other. This leads to osteoarthritis. The condition is accompanied by pain, inflammation, and loss of mobility.
How Do Glucosamine & Chondroitin Sulfates Help Degenerative Disc Disease?
Glucosamine and chondroitin sulfates are substances that occur naturally in the body. It is an essential element in cartilage maintenance and regeneration. They help to form new cartilage from within existing cartilage. They can actually help to rebuild the discs that have begun to degrade. Often they are taken as nutritional supplements.
Studies show that long term use of glucosamine and chondroitin sulfate do indeed not just help arrest the development of spinal disc degeneration, they can also help to reverse the symptoms, especially if begun in the early stages of the disease. Treatment that incorporates these supplements result in decreased pain and improved range of motion. Patients may also notice strengthening of the back and increased flexibility. This is true even in patients who are older, in their 50�s and 60�s.
Patients may start noticing a decrease in pain as early as six months after beginning to take the supplement. After taking it consistently, the other benefits present over time. What is also important to note is that neither glucosamine nor chondroitin sulfate cause any adverse side effects. These supplements are safe and effective.
Chiropractic For Degenerative Disc Disease
Chiropractic is a complementary treatment to combine with glucosamine and chondroitin sulfate for degenerative disc disease. Chiropractic alone is very effective for many spine and neck disorders, including degenerative disc disease. It is a natural, non-invasive treatment that does not use medications but instead incorporates lifestyle changes, diet, and exercise recommendations to provide whole body wellness. While chiropractic works very well to treat pain, improve mobility, and increase flexibility, it has actually been proven to stop the progression of degenerative disc disease and even reverse its effects.
Using chiropractic for degenerative disc disease and combining it with supplements that include glucosamine and chondroitin sulfate is a very effective system for relieving the pain and other symptoms. In several studies, many patients saw improvement and decrease in symptoms faster than patients who used the supplements alone. Combining these treatments is usually the best course of action to help patients suffering from this devastating disease.
When treating any condition, it is always best to go the most natural route possible. The fewer synthetic substances and manufactured toxins that are introduced into the body, the better chance the patient has of a more thorough and faster healing or at the very least a dramatic decrease in symptoms.
Injury Medical Clinic: Herniated Disc Treatment & Recovery
Three Steps: Your lower back needs protection, strength and nourishment to help prevent and reduce lower back pain.
Adding these 3 steps to one’s day can help take stress off your lower back:
Three Steps
1. Work On A Stand-Up Desk For Part Of The Day
Too much sitting is common in the cause of low back pain. Posture while sitting, forward leaning in order to look at a computer screen, affects the natural alignment of the lower spine by placing a heavy load on the lumbar discs and joints.
Many people are utilizing standup desks for part of their workday. Standup desks come in a variety of shapes, functionality, and price ranges. They can be inexpensive to fully adjustable, automatic models.
If lower back pain is already an issue, only stand for part of the day and gradually increase to longer standing times. Cushioned and standing mats add additional comfort, as well as, exercise benefits. Standing more, along with quick walks and/or quick stretches at the half hour can break up the extended sitting cycle.
2. Stretch Hamstrings On A Daily Basis
Hamstrings are the large muscles that run down the back of each thigh. They can quite easily become tight. If they become very tight then the hamstring/s will transfer stress across the lower back and can lead to back pain.
There are a variety of hamstring stretches that are gentle on the back and easy to do: pick one or two that work for you and are easy to incorporate it into a daily routine.
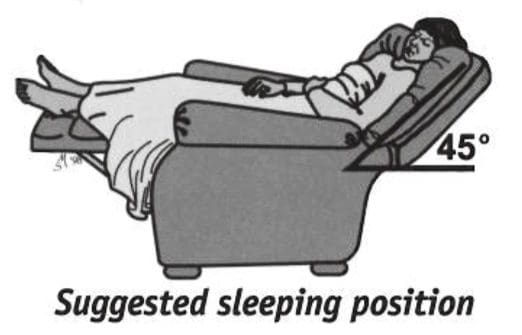
3. Sleep In A Reclined Position
People with lower back pain feel more support when the lower back is in a slightly reclined position, along with the knees supported and elevated. This is true for lower back diagnoses, such as osteoarthritis, spinal stenosis, and lumbar degeneration.
If it is difficult to sleep on your back, try resting in this position in a reclining chair or bed before going to sleep.
Sleeping the most comfortable in a supported, reclined position can come from switching to an adjustable bed, aka (adjustable base). Just like the stand-up desks, these models range from basic to sophisticated options.
A new development now is that online mattress companies now offer mattress bases that are fully adjustable, and some offer free delivery/setup. Consider a new mattress with an adjustable base that goes with the mattress. This combination may work to help your back.
We encourage back pain supplementation with chiropractic treatment and any type of steps one can take to help prevent and reduce lower back.
Injury Medical Clinic: Sciatica Treatments & Recoveries
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine