I got into a car accident, I was rear-ended on Valentine’s Day and things weren’t quite right in my body, the aches and pains started coming. So after I visited another chiropractor and talked to my client, they told me about this place and when I came I was like, okay, I’m not going back to the other place. And that’s how I head about him (Dr. Alex Jimenez) and I’m so grateful. – Terry Peoples
Based on information referenced by the National Highway Traffic Safety Administration, or NHTSA, approximately more than three million individuals are injured annually in automobile accidents throughout the United States alone. While the unique conditions of every car crash can ultimately result in a wide variety of injuries, some types of automobile accident injuries are more common than others.
Fortunately, a majority of automobile accident injuries may resolve on their own without the need for treatment, however, more significant health issues caused by the auto collision may require some amount of treatment and/or rehabilitation and others may unfortunately become permanent if left untreated. It’s fundamental for the victim of an automobile accident to seek immediate medical attention in order for them to receive a proper diagnosis for their motor vehicle injuries before proceeding with the most appropriate treatment option for them.
Prior to following any necessary medical procedure, understanding some of the most common automobile accident injuries can help you become aware of the steps you can take to ensure that you are getting the proper care for your health issues. Furthermore, the type and severity of motor vehicle accidents suffered by the victims involved in a car crash may largely depend on several variables, including:
Was the individual wearing a seat belt?
Did the person’s car get hit from the back, side or front?
Was the occupant facing straight ahead in the seat? Or was the person’s head or body turned in a particular direction?
Was the incident a low-speed collision or a high-speed crash?
Did the car have airbags?
There are two broad categories of automobile accident injuries: impact injuries and penetrating injuries. Impact injuries are generally characterized as those caused when a portion of the individual’s body hits some part of the interior of the car. Frequently, this can be a knee hitting a dashboard or the head hitting the seat rest or the side window during an auto collision. Penetrating injuries are generally characterized as open wounds, cuts and scrapes. Shattering glass or loose items flying inside the car on impact can often cause these types of automobile accident injuries. Below, we will discuss the most common automobile accident injuries and describe them in detail.
Soft Tissue Injuries
Soft tissue injuries are some of the most common types of automobile accident injuries. A soft tissue injury is typically characterized as trauma, damage or injury to the body’s connective tissue, including tendons, ligaments and muscles. Soft tissue injuries can vary depending on the type of connective tissue it affects as well as on the grade and severity of the harm. Because soft tissue injuries do not involve open wounds, it may be challenging to diagnose these type of automobile accident injuries.
A whiplash-associated disorder, most frequently referred to as a whiplash injury to the neck and upper back, is a type of soft tissue injury. In this form of harm, the muscles, tendons and ligaments are stretched beyond their natural range due to the abrupt movements imposed on the neck and head from the force of the impact at the point of collision. These same mechanisms may additionally cause soft tissue injuries in other regions of the body, such as the back. Automobile accidents can also often cause mid-back and low-back muscle sprains, and at times, these may cause severe back injuries and even aggravate underlying conditions due to the sheer force from the impact on the spine.
Cuts and Scrapes from Automobile Accident Injuries
During an auto collision, any loose objects inside the car can immediately become projectiles which can be thrown about the vehicle’s interior. This includes cell phones, coffee glasses, eyeglasses, purses, books, dash-mounted GPS systems, etc.. If one of these objects strikes your body at the time of the incident, they can easily cause cuts and scrapes as well as cause additional trauma, damage or injuries.
Occasionally, these cuts and scrapes are relatively minor and require no immediate medical attention. More severe cases of these type of automobile accident injuries, however, could create a relatively large open wound and may require stitches to prevent blood loss. Cuts or scrapes can also occur when your airbag deploys from the auto collision.
Head Injuries
Head injuries in the form of automobile accident injuries can take a number of forms, where some can be considered comparatively minor and others can virtually be quite severe. The sudden stop or shift in direction by a motor vehicle during an car crash can cause an individual’s head and neck to jolt or jerk abruptly and unnaturally in any direction, overstretching the complex structures of the cervical spine beyond their normal range, leading to muscle strains and whiplash-associated disorders.
The head itself can also be injured during an auto accident. Impact with a side window or with the steering wheel may cause cuts, scrapes and bruises to the head, as well as even deeper lacerations. More severe collision impacts can cause a closed head injury. In that circumstance, the fluid and tissue inside the skull are damaged due to the abrupt movement or impact of the head. Less acute closed head injuries often result in concussions, while the most severe head injuries can cause brain damage.
Chest Injuries
Chest injuries are also common auto accident injuries. These type of injuries are usually identified as contusions or bruises, however, these can also take the form of much more severe injuries, like fractured ribs or internal injuries. Drivers often experience chest injuries due to their position behind the steering wheel, which offers very little space to move before the torso collides with the steering wheel. If an individual’s body is thrown forward during a motor vehicle collision, even if their chest doesn’t impact the steering wheel or dashboard, the torso will experience tremendously high amounts of force, specifically against the shoulder harness or seat belt, which may cause severe bruising.
Arm and Leg Injuries
The very same sheer forces which unexpectedly throw a person’s head and neck back-and-forth during a car crash can behave similarly on arms and legs. If your vehicle experiences a side impact, your arms and legs may be tossed hard against the door. In addition, if you’re a passenger, your legs typically have very little room to move. As a result, automobile accidents often cause an occupant’s knees to strike the dashboard or even chairs in front of them.
Based on the circumstance of the auto collision, automobile accident injuries to your arms and legs may include bruises, scrapes and cuts, however, sprains and even fractures in both the upper and lower extremities can happen. Keep in mind that some injuries aren’t apparent following a car accident. It may take days, weeks, or even months for symptoms to manifest. Therefore, if you’ve been involved in an automobile accident, it is best to seek immediate medical attention.
Dr. Alex Jimenez’s Insight
After being involved in an auto accident, it may sometimes take days, weeks, even months for symptoms to manifest completely. For your own health and wellness, it’s essential to seek immediate medical attention following the car crash. While many types of injuries can occur, there are several common automobile accident injuries which can develop due to the sheer force of the impact, such as whiplash-associated disorders. Whiplash is a prevalent auto accident injury which is characterized as a type of neck injury which happens when the complex structures surrounding the cervical spine are stretched far beyond their natural range of motion. Chiropractic care is a safe and effective treatment option which can treat a variety of auto accident injuries.
Chiropractic Care After an Automobile Accident
Many healthcare professionals are qualified and experienced�in the treatment of a variety of automobile accident injuries, especially chiropractors. Chiropractic care is a well-known, alternative treatment option which focuses on the diagnosis, treatment and prevention of numerous injuries and/or conditions associated with the musculoskeletal and nervous system. If you’ve been involved in an auto collision, chiropractic care can offer substantial benefits towards your current well-being, supporting your recovery process.
After a car collision, you may experience pain and discomfort, decreased range of motion, stiffness or soreness. Remember that these symptoms may not always manifest immediately after a motor vehicle accident. Through the use of spinal adjustments and manual manipulations, chiropractic care will help you manage painful symptoms, as well as help enhance flexibility, increase strength and improve mobility, promoting a faster recovery. In addition, it can prevent long-term symptoms from developing, such as migraines and chronic pain. The sooner you get chiropractic care after a car wreck, the more likely you are to recover fully.
By carefully restoring the original alignment of the spine, chiropractic care helps reduce pain and other painful symptoms. Furthermore, a chiropractor can recommend a series of exercises and physical activities to help pump oxygen, blood and nutrients to the injury site and enhance recovery. A doctor of chiropractic will develop a personalized treatment program targeted to your specific automobile accident injuries. Chiropractic care also makes it possible to avoid the need for surgical interventions. It strengthens ligaments, tendons and muscles, which shield the body’s structures. It’s also a far more cost-effective solution.
Chiropractic care can also restore function in patients with older vehicle collision injuries. You are still able to benefit from chiropractic care even if you had an accident years back. Employing spinal adjustments and manual manipulations, as well as rehabilitation techniques, it helps relieve old pain and improve function. Additionally, it is a non-invasive treatment option, and you won’t end up needing to rely on pain drugs and/or medications for relief of your symptoms.
Chiropractors can even treat vertigo resulting from a car crash. In as little as one treatment, they could fix a dysfunction in the vestibular system. Other types of chiropractic care treatment techniques include massage, ultrasound, ice and cold treatment, specific exercises and physical activities, and even nutritional advice. Chiropractic care is a safe and effective treatment approach which can help treat automobile accident injuries without the need for drugs and/or medications as well as surgery.
If you suffered a car accident injury, don’t delay any longer. Contact a chiropractor and allow them to help you follow the best treatment path. Chiropractors can provide you a consultation to perform a comprehensive evaluation and make a treatment strategy targeted to your injuries.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
I went through the physical therapy, and then I used chiropractic care, as well as crossfit, to kinda get me to that 100% mark. And I haven’t had a problem since, I continue to do crossfit and I use chiropractic care to make sure my body is aligned. It gives me that extra sense of feeling that I’m not gonna injure myself again, that my body is feeling good and 100%. I never have that feeling in the back of my mind, that, you know, I’m gonna injure myself. Sometimes I forget I even had a surgery and I think I can attribute that to a combination of chiropractic care and to the overall training aspect of crossfit. – Andrew Hutchison
There are a variety of causes for both hip pain and knee pain. While the hip joint can withstand a tremendous amount of wear-and-tear, it’s not indestructible. With age and usage, the hip cartilage can begin to degenerate, resulting in hip pain. Tendons and ligaments at the hip may also get excessive overused and can start to demonstrate signs of wear-and-tear over time. The anatomy of the knee, however, is more complex. The knee is collectively made up of bones, pads of cartilage and a joint capsule. Trauma or damage from an injury or degeneration associated with aging may cause knee pain.
Causes of Hip Pain
Hip pain is the general term used to define pain felt in or around the hip joint. Certain injuries and/or conditions may commonly cause hip pain. Arthritis, especially rheumatoid arthritis, are the primary culprits of hip pain in older individuals. Both may result in the breakdown of cartilage in the hip joint and can cause inflammation in the area. Combined with pain and discomfort, there’s generally also reduced range of motion in the hip as well as stiffness. Bursitis may also result in hip pain. The bursae are sacs of fluid which function by helping to reduce friction between the joints. If these become inflamed, however, they can lead to pain. Typically, it’s only repetitive movements that irritate the hip joint and result in pain.
Similar to bursitis, tendinitis can also lead to inflammation and is usually caused by repetitive stress from movements. Muscle or tendon strain can be a result of overuse. Repeated physical activities can additionally place unnecessary amounts of pressure on the ligaments, tendons and joints of the hip, especially in those which support the buttocks. If some of these are inflamed, the hip won’t be able to function normally and there will be painful symptoms as a result. Below, we will describe the various causes of hip pain as well as discuss their effects on the structure of the hip in detail.�Hip pain isn’t always felt in the hip itself as it may also be felt in the groin or thigh.
Tendonitis
The most frequent cause of severe hip pain is inflamed tendons, or tendonitis. This can generally be due to excessive exercise or physical activities. This health issue can be quite debilitating but it usually heals within a couple of days with proper care.
Arthritis
As mentioned above, one of the most common causes of chronic hip pain is arthritis. Arthritis can cause painful, stiff and tender joints, and it can cause walking problems. Various types of arthritis can cause hip pain, including:
Osteoarthritis might be the final result of age-related degeneration in the cartilage that surrounds the joints.
Trauma, damage or injury to a joint, like a fracture, may cause traumatic arthritis similar to atherosclerosis.
Infectious arthritis is a result of an infection in the joint caused by the degeneration of cartilage.
Rheumatoid arthritis is a result of the human body’s immune system attacking its own joints. This type of arthritis can ultimately destroy joint bones and cartilage.
Osteoarthritis is a a lot more commonly diagnosed than rheumatoid arthritis.It’s fundamental to understand the different types of arthritis as these can be powerful diagnostic tools to help effectively treat hip pain.
Trochanteric Bursitis
Another possible cause of hip pain involves a health issue medically referred to as trochanteric bursitis, as previously mentioned. This condition occurs when the bursa, which are liquid-filled sacs near the hip joint, become inflamed. Any number of variables can lead to trochanteric bursitis, such as hip injury, overuse of the joints, underlying health issues, or even the presence of other conditions like rheumatoid arthritis. This condition is reportedly much more common in females than in males.
Hip Fractures
Hip fractures are common causes of hip pain which most frequently occur in older adults and in people who have osteoporosis, which is a weakening of the bones associated with age and various other factors. Hip fractures cause very sudden and extreme hip pain, where they will require immediate medical attention. There are complications that can happen due a fractured hip, like a blood clot in the leg. A hip fracture usually requires surgical interventions to be corrected. Additionally, you may be required to seek further care from a qualified healthcare professional in order to engage in a rehabilitation program.
Less Common Causes of Hip Pain
There are additional, less common conditions that can result in hip pain. These include snapping hip syndrome and osteonecrosis, or avascular necrosis. Below, we will discuss these two health issues in detail.
Snapping Hip Syndrome
Snapping hip syndrome, which most commonly occurs in athletes, especially dancers, is characterized by a snapping noise or feeling from the hip. By way of instance, this snapping may happen when you’re walking or getting up from a chair. The problem is usually painless, but it can cause pain in several cases. Snapping hip with pain is generally an indication of a tear in the hip cartilage or other structure surrounding the hip joint.
Osteonecrosis
Osteonecrosis, also known as avascular necrosis, occurs when blood isn’t able to reach the bones, either permanently or temporarily. This can cause the reduction of bone. The cartilage of individuals with this condition is normal initially, however, it will eventually collapse as the disease evolves. Finally, bones may crack or crumble. It’s not always clear what triggers osteonecrosis. Joint harm, heavy usage of steroid drugs or alcohol, and cancer treatments could put you at greater risk of developing this condition, however, the cause is never determined in many osteonecrosis cases.
Causes of Knee Pain
Similar to hip pain, arthritis, especially rheumatoid arthritis and osteoarthritis, may commonly cause knee pain. With the breakdown of cartilage associated with osteoarthritis in the knee, the bones can begin to rub against one another, causing pain and discomfort which could eventually lead to other painful symptoms. Rheumatoid arthritis is a chronic inflammatory disorder of the joints and it can affect the soft tissue which lines the knee joints. The final result is inflammation, joint damage and joint pain at the knee. The knee joint is very prone to accidents. Typical knee injuries include: meniscal injuries, anterior cruciate ligament injuries and tendon injuries.
The meniscus might be damaged when the knee is bent and twisted in an unnatural way, where ligaments and tendons could also be overstretched and ultimately torn as a result. If it is not repaired, the probability of developing osteoarthritis increases. Any abrupt change in movement can additionally injure the anterior cruciate ligament. Nearly all causes of knee injury and knee pain are the result of a blow to the surface of the knee. Exercises or physical activities which could harm the complex structures of the knee include jogging and jumping. A dislocated kneecap is still another frequent source of knee pain. This occurs when the patella is moved from place and it can be very debilitating.
Temporary knee pain differs from chronic knee pain. Persistent knee pain is not always attributable to one incident. It the result of many causes or conditions.Persistent knee pain is characterized as long-term pain, swelling, or sensitivity in a single or both knees. The reason behind your knee pain can determine the symptoms you develop. Many conditions may cause or lead to chronic knee pain, and lots of treatments exist. Every person’s experience with chronic knee pain will most likely be different. Understanding the causes of knee pain can be a powerful diagnostic tool which can help healthcare professionals properly determine the proper treatment option for your specific health issue.�Common causes of knee pain include:
osteoarthritis: pain, inflammation and joint destruction brought on by degeneration of a joint.
tendinitis: pain in the knee which worsens when climbing, taking stairs, or walking up an incline.
bursitis: inflammation caused by repeated overuse or trauma of the knee.
chondromalacia patella: damaged cartilage under the kneecap.
gout: arthritis brought on by the buildup of uric acid.
Baker’s cyst: a buildup of synovial fluid, fluid which lubricates the joint, supporting the knee.
rheumatoid arthritis, or RA: a chronic autoimmune inflammatory disease that causes painful swelling, joint deformity and bone erosion.
dislocation: dislocation of the kneecap most commonly caused by trauma, damage or injury.
meniscus tear: a rupture in one or more of the soft tissues in the knee.
torn ligament: tear at one of the four ligaments in the knee, the most commonly injured ligament is the anterior cruciate ligament, or the ACL.
bone tumors: osteosarcoma, is the second most common bone cancer, which most commonly occurs in the knee.
Dr. Alex Jimenez’s Insight
While the hip and knee joints are capable of sustaining various degrees of stress when performing physical activities, trauma, damage or injury as well as the degeneration of these complex structures, can ultimately lead to knee and hip pain. The balance of the human body as a whole is fundamental towards overall health and wellness. Therefore, if an individual experiences hip or knee pain, the entire structure and function of their body can be tremendously affected. It’s important for a person with knee or hip pain to seek immediate medical attention from a qualified and experienced healthcare professional, such as a chiropractor or physical therapist, in order to restore the balance of their entire body.
Treatment for Knee and Hip Pain
The treatment of hip pain is based upon the cause. For many instances of trauma, damage or injury, rest is generally enough to enable the hip to heal. By way of instance, exercise-associated hip pain is normally eliminated within a couple of days. When you have arthritis, a healthcare professional may sometimes prescribe drugs and/or medications to help relieve stiffness and pain. Furthermore, your physician will refer you to a doctor who can provide additional information regarding the cause of your hip pain along with recommending an alternative treatment option, such as chiropractic care and physical therapeutics, that will explain to you how you can perform rehabilitation exercises to help maintain joint strength, mobility and flexibility.
For injuries, therapy typically involves bed rest and the use of drugs and/or medications, such as naproxen, to alleviate pain, swelling and stiffness. Hip fractures, malformation of the hip and some injuries may require surgical intervention to repair or replace the hip. In hip replacement surgery, a surgeon will replace a broken hip joint with an artificial one. Although hip replacement surgery will need rehabilitation to become accustomed to the new joint, this type of treatment option is often considered.
Alternative Treatment Options
Some holistic remedies can offer relief from hip pain. Make certain you discuss treatment options with your doctor before considering any treatment option. Potential alternative treatment options include visiting a chiropractor for a spinal adjustment or manual manipulation. Chiropractic care is a well-known treatment approach which focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractic care can help carefully re-align the spine as well as help reduce pain and discomfort, improve swelling and inflammation and even increase strength, flexibility and mobility on other structures of the human body. Physical therapeutics can also help treat both hip and knee pain.
There are many benefits of physical therapeutics, including increased range of motion, reduction of pain, less inflammation and swelling, as well as an overall improvement of quality of life. The first steps a chiropractor or physical therapist will perform if you have hip pain will consist of tests, such as a gait evaluation, range of motion measurement and intensity measurements. Afterwards, the healthcare professional will create a personalized treatment program. Treatment techniques may also include ultrasound and ice. There will also be specific exercises and stretches to help boost hip strength, mobility and flexibility to decrease pain. For knee pain, tests are also done along with active and passive treatments. Chiropractic care and physical therapeutics can help promote healing without the need for drugs and/or medications, and surgical interventions.
Bursitis, a frequent cause of knee pain, can be treated in the following ways:
Ice the knee for 15 minutes once an hour for three of four hours. Do not apply the ice directly to the knee, instead, cover your knee with a cotton towel. Put ice in a plastic zip-close bag, then place the bag on the towel.
Wear cushioned, flat shoes that support your toes and do not worsen your pain.
Avoid sleeping on your side. Use cushions positioned on both sides of your body to keep you from rolling on your side. When lying on the side, keep a pillow between your knees.
Stay seated when possible. Should you need to stand, prevent hard surfaces and maintain your weight evenly distributed on both legs.
Participate or engage in weight loss programs and strategies to lose weight if you are overweight or obese, to reduce the amount of stress that is placed on the knees.
If you are experiencing hip pain, knee pain or some other type of joint pain, make sure to contact a qualified healthcare professional, in order to receive a proper diagnosis to begin the best treatment approach for your specific health issue. Trained and skilled doctors will take you on the path to better healing. Make sure you prepare a one-on-one consultation to acquire a comprehensive examination and say good-bye to your pain. Healthcare professionals are devoted to providing you with a healthy and wholesome lifestyle.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
My treatment with Dr. Alex Jimenez has been helping me by simply making me less tired. I’m not experiencing as many headaches. The headaches are going down dramatically and my back feels much better. I would highly recommend Dr. Alex Jimenez. He’s very friendly, his staff is very friendly and everybody goes well beyond what they can do to help you. –Shane Scott
Neck pain can develop due to a variety of reasons, and it can vary tremendously from mild to severe. Most of the population has suffered from this well-known nagging health issue; however, did you know that headaches can sometimes be caused by neck pain? While these headaches are commonly referred to as cervicogenic headaches, other types, such as cluster headaches and migraines, have also been determined to be caused by neck pain.
Therefore, it’s fundamental to seek a proper diagnosis if you’ve experienced headaches or neck pain to determine the root cause of your symptoms and decide which treatment option will be best for your specific health issue. Healthcare professionals will assess your upper back, or the cervical spine, including your neck, the base of the skull and cranium, and all the surrounding muscles and nerves to find the source of your symptoms. Before seeking help from a doctor, it’s essential to understand how neck pain can cause headaches. Below, we will discuss the anatomy of the cervical spine or neck and demonstrate how neck pain is connected to headaches.
How Neck Pain Causes Headaches
The muscles between the shoulder blades, the upper portion of the shoulders, and those surrounding the neck, or cervical spine, may all cause neck pain if they become too tight or stiff. This can generally occur due to trauma or damage from an injury, as well as in consequence of bad posture or poor sitting, lifting, or work habits. The tight muscles will make your neck joints feel stiff or compressed, and it can even radiate pain toward your shoulders. Over time, the balance of the neck muscles changes, and those specific muscles that support the neck become weak. They can ultimately begin to make the head feel heavy, increasing the risk of experiencing neck pain as well as headaches.
The trigeminal nerve is the primary sensory nerve that carries messages from the face to your brain. Furthermore, the roots of the upper three cervical spinal nerves, found at C1, C2, and C3, share a pain nucleus, which routes pain signals to the brain and the trigeminal nerve. Because of the shared nerve tracts, pain is misunderstood and thus “felt” by the brain as being located in the head. Fortunately, many healthcare professionals are experienced in assessing and correcting muscular imbalances, which may lead to neck pain and headaches. Moreover, they can help to relieve muscle tension, enhance muscle length and joint mobility, and retrain correct posture.
What Causes Neck Pain and Headaches?
Cervicogenic headaches, otherwise known as “neck headaches,” are caused by painful neck joints, tendons, or other structures surrounding the neck, or cervical spine, which may refer to pain to the bottom of the skull, to your face or head. Researchers believe that neck headaches, or cervicogenic headaches, account for approximately 20 percent of all headaches diagnosed clinically. Cervicogenic headaches and neck pain are closely associated, although other types of headaches can also cause neck pain.
This type of head pain generally starts because of an injury, stiffness, or lack of proper functioning of the joints found at the top of your neck, as well as tight neck muscles or swollen nerves, which could trigger pain signals that the brain then interprets as neck pain. The usual cause of neck headaches is dysfunction in the upper three neck joints, or 0/C1, C1/C2, C2/C3, including added tension in the sub-occipital muscles. Other causes for cervicogenic headaches and neck pain can include:
Cranial tension or trauma
TMJ (JAW) tension or altered bite
Stress
Migraine headaches
Eye strain
The Link Between Migraines and Neck Pain
Neck pain and migraines also have an intricate connection with each other. While in some cases, severe trauma, damage, or injury to the neck can lead to severe headaches like migraines; neck pain might result from a migraine headache in different situations. However, it’s never a good idea to assume that one results from the other. Seeking treatment for neck pain when the reason for your concern is a migraine often will not lead to effective pain management or pain relief. The best thing you can do if you’re experiencing neck pain and headaches is to seek immediate medical attention from specialized healthcare professional to determine your pain’s cause and the symptoms’ root cause.
Unfortunately, neck pain, as well as a variety of headaches, are commonly misdiagnosed or even sometimes go undiagnosed for an extended period. One of the top reasons neck pain may be so challenging to treat primarily because it takes a long time for people to take this health issue seriously and seek a proper diagnosis. When a patient seeks a diagnosis for neck pain, it may already have been a persistent problem. Waiting an extended amount of time to take care of your neck pain, especially after an injury, may lead to acute pain and even make the symptoms more difficult to control, turning them into chronic pain. Also, the most frequent reasons people seek treatment for neck pain, and headaches include the following:
Chronic migraines and headaches
Restricted neck function, including difficulties moving the head
Soreness in the neck, upper back, and shoulders
Stabbing pain and other symptoms, particularly in the neck
Pain radiating from the neck and shoulders to the fingertips
Aside from the symptoms mentioned above, individuals with neck pain and headaches can also experience additional symptoms, including nausea, diminished eyesight, difficulty concentrating, severe fatigue, and even difficulty sleeping. While there are circumstances in which the cause of your headaches or neck pain may be apparent, such as being in a recent automobile accident or suffering from sport-related trauma, damage, or injuries, in several instances, the cause may not be quite as obvious.
Because neck pain and headaches can also develop as a result of bad posture or even nutritional problems, it’s fundamental to find the origin of the pain to increase the success of treatment, in addition to enabling you to prevent the health issue from happening again in the future. It’s common for healthcare professionals to devote their time working with you to ascertain what could have caused the pain in the first place.
A Health Issue You Can’t Ignore
Neck pain is typically not a problem that should be ignored. You may think that you’re only experiencing minor neck discomfort and that it’s irrelevant to any other health issues you may be having. Still, you can’t know for sure more frequently than not until you receive a proper diagnosis for your symptoms. Patients seeking immediate medical attention and treatment for their neck-centered problems are surprised to learn that some of the other health issues they may be experiencing may be correlated, such as neck pain and headaches. Thus, even if you think you can “live with” not being able to turn your neck completely, other health issues can develop, and these problems might be more challenging to deal with.
There are circumstances in which a pinched nerve in the neck is the main reason for chronic tension headaches, where a previous sports injury that was not adequately addressed before is now the cause of the individual’s limited neck mobility and in which a bruised vertebrae at the base of the neck induces throbbing sensations throughout the spine, which radiates through the shoulders into the arms, hands, and fingers. You might also blame your chronic migraines on a hectic schedule and stressful conditions. However, it might be a consequence of poor posture and the hours you spend hunched over a computer screen. Untreated neck pain might lead to problems you never expect, such as balance problems or trouble gripping objects. This is because all the neural roots located on the upper ligaments of the cervical spine or neck are connected to other parts of the human body, from your biceps to each of your tiny fingers.
Working with a healthcare professional to relieve the root cause of your neck pain and headaches may significantly enhance your quality of life. It may be able to eliminate other symptoms from turning into a significant problems. While another health issue or nutritional deficiency generally causes the most common causes of chronic migraines, you might also be amazed to learn how often the outcome may be resolved with concentrated exercises and stretches recommended by a healthcare professional, such as a chiropractor. Additionally, you may understand that the health issues you’ve been having often develop from compressed, pinched, irritated, or inflamed nerves in your upper cervical nerves.
Dr. Alex Jimenez’s Insight
Although it may be difficult to distinguish the various types of headaches, neck pain is generally considered to be a common symptom associated with head pain. Cervicogenic headaches are very similar to migraines, however, the primary difference between these two types of head pain is that a migraine occurs in the brain while a cervicogenic headache occurs in the base of the skull or in the cervical spine, or neck. Furthermore, some headaches may be caused by stress, tiredness, eyestrain and/or trauma or injury along the complex structures of the cervical spine, or neck. If you are experiencing neck pain and headaches, it’s important to seek help from a healthcare professional in order to determine the true cause of your symptoms.
Treatment for Neck Pain and Headaches
Foremost, a healthcare professional must determine the cause of an individual’s symptoms through the use of appropriate diagnostic tools as well as to make sure they have the utmost success in relieving the headache and neck pain without prolonging the duration of the symptoms and extra cost of incorrect therapy. Once an individual’s source of neck pain and headaches has been diagnosed, the kind of treatment a patient receives should depend on the type of headache. As a rule of thumb, treatment starts once the diagnosis has been made. A healthcare professional will work with you to create a treatment plan appropriate for your specific health issues. You’ll be taken through procedures that help build flexibility and strength in your sessions.
Chiropractic care is a well-known alternative treatment option focusing on diagnosing, treating, and preventing various musculoskeletal and nervous system injuries and conditions. A chiropractic doctor or chiropractor can help treat neck pain and headache symptoms by carefully correcting any spinal misalignments, or subluxations, in the cervical spine or neck, through spinal adjustments and manual manipulations, among other therapeutic techniques. Chiropractors and physical therapists may also utilize a combination of gentle Muscle Energy Techniques, muscle building, joint slides, Cranio-sacral therapy, and specific posture and muscle re-education to lower the strain being placed on the structures surrounding the cervical spine. The staff will also help you understand how to better position yourself during your daily life to prevent relapses, like ergonomic and posture tips. Contact a healthcare professional for them to be able to assist you immediately.
In cases where alternative treatment options have been utilized without any results or sometimes used together with other complementary treatment approaches, pain drugs and medications may be contemplated, such as non-steroidal anti-inflammatory drugs (NSAIDs) and anti-seizure agents such as gabapentin, tricyclic anti-depressants, or migraine prescriptions. If pain medications prove ineffective, injections may be contemplated, including peripheral nerve blocks, atlantoaxial joint blocks administered at C1-C2, or aspect joint blocks administered in C2-C3. Surgical interventions may also be other treatment options. However, healthcare professionals suggest attempting all other treatment options before considering surgery. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please ask Dr. Jimenez or contact us at 915-850-0900.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once. The spine is a complex structure of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and aggravated conditions, such as herniated discs, eventually lead to back pain symptoms. Sports or automobile accident injuries are often the most frequent cause of back pain; however, sometimes, the simplest movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through spinal adjustments and manual manipulations, ultimately improving pain relief.
Chiropractic care is a drug-free, nonsurgical treatment for many types of conditions and to help manage pain. As more and more medical professionals are recognizing its effectiveness and viability for treating many issues in the body, chiropractic is gaining popularity and becoming the treatment of choice for many patients with chronic pain, back problems and other issues. In particular, it has been found to be a very effective treatment for spondylolisthesis. It can not only relieve the pain, but often return the patient�s mobility as well.
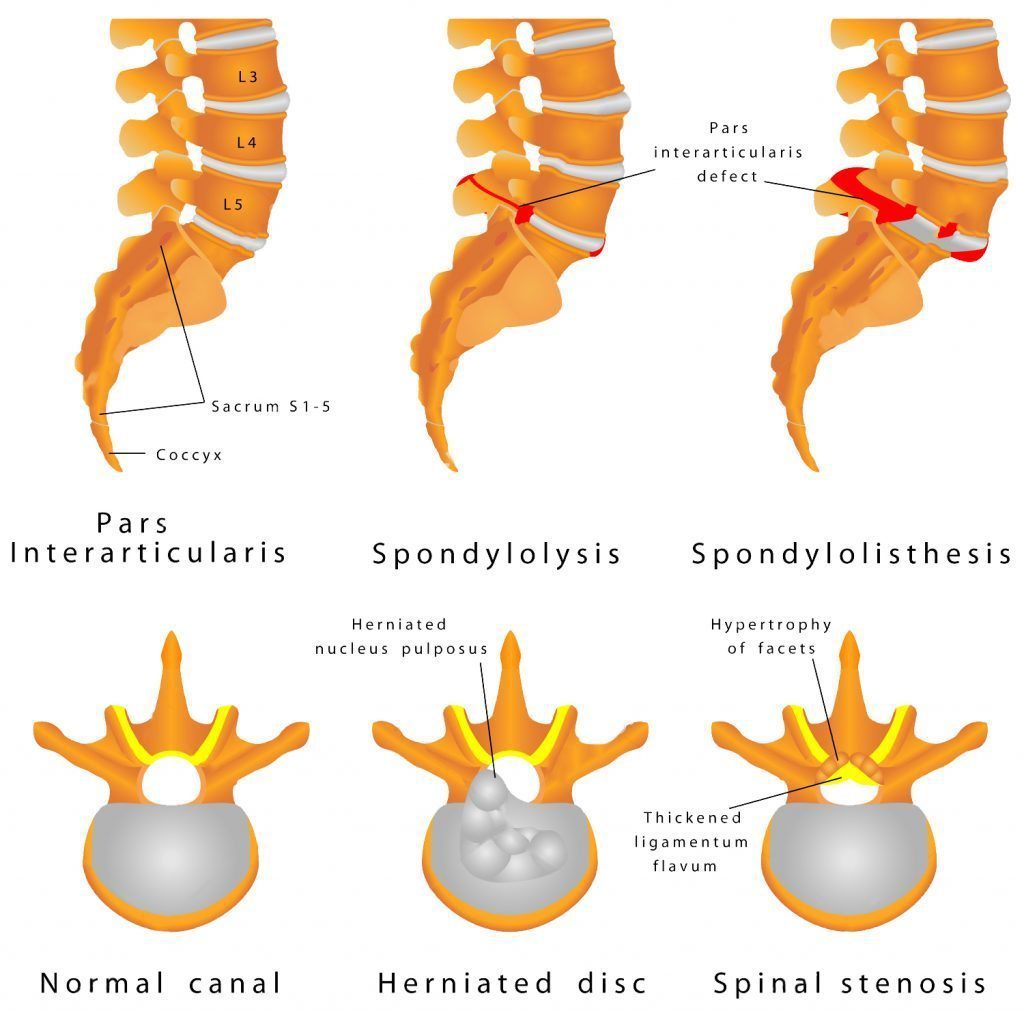
What Is Spondylolisthesis?
Spondylolisthesis is a condition in which one vertebra slides forward over the vertebra that is below it. It is typically confined to the lumbosacral, or lower back area. It can become painful, causing lower back pain and weakness or numbness in one or both legs, when it causes the nerve roots or spinal cord to be squeezed. In severe cases, a patient can lose control of their bowel or bladder function, but this is fairly rare. However, any patient who begins to lose bowel or bladder control should contact their doctor immediately.
In some cases, a person�s vertebra can slip out of place without any symptoms being present. Sometimes the symptoms don�t show up until months or even years later. Symptoms of spondylolisthesis may include:
Low back pain
Pain in the buttock area
Pain that radiates from the lower back down one or both legs
Spondylolisthesis is diagnosed by a doctor or chiropractor who may conduct several diagnostic tests. Typically, the doctor will take X-rays of the patient�s back to rule out certain conditions, especially if they suspect spondylolisthesis.
The X-ray will allow the doctor to see if any of the patient�s vertebrae have slipped out of place, or are cracked or fractured. An MRI or CT scan may also be ordered to better view the spine and see the extent of the damage.
What Are The Treatments For Spondylolisthesis?
The treatment for spondylolisthesis is based on the actual damage identified by the doctor, the pain and mobility problems that the patient is experiencing, and the overall severity of the condition. Rest is the first course of treatment as well as ceasing the physical activities that may have caused the damage in the first place.
Pain may be managed by non-steroidal anti-inflammatory drugs such as naproxen and ibuprofen. Acetaminophen may also be administered for pain.
Other treatments for spondylolisthesis include:
Bracing
Weight loss (if the person is obese or overweight)
Physical therapy to strengthen the core
Epidural steroid injections
Surgery (in severe cases such as damage to the spinal cord or nerve root)
There are several types of surgery that may be used to treat spondylolisthesis. The surgeon may remove tissue or bone in order to relieve pressure on the nerves or spinal cord. Sometimes the doctor may opt for fusing the damaged bones into place so they can no longer slip. In some cases, both procedures are done. This type of treatment is usually a last resort because recovery can be lengthy and the patient will have to wear a back brace or cast while their back is healing.
Is Chiropractic Effective For Treating Spondylolisthesis?
Chiropractic is a drug-free, noninvasive treatment for spondylolisthesis. It is often a preferred treatment because the patient does not have to undergo painful surgery or take medication that could have undesirable side effects. There are three primary spinal manipulation techniques that may be used by the chiropractor:
Spinal manipulation specific to the restricted or impaired joints
Flexion-distraction technique which is a slow, gentle pumping action
Instrument assisted manipulation uses an instrument to apply gentle force to the spine
Chiropractic care has been found to be very effective in treating this condition, but prevention is always the best course of action. Regular exercise, healthy weight management, and regular chiropractic visits can help ward off many spine related conditions including spondylolisthesis.
TMJ dysfunction: The temporomandibular joints, TMJ, are the lower jaw hinges that sit on either side of the head in front of each ear. They are responsible for the lower jaw opening, closing, sliding, and rotating. The TMJs are the most body�s most complex joints. The typical person uses them more than 5,000 times a day by talking, laughing, yawning, chewing, eating, smiling, and swallowing.
What Is TMJ Dysfunction?
TMJ dysfunction occurs when one or both joints become inflamed or injured causing pain and immobility in the jaw area. Because these joints are used so often and tend to be far more mobile than most other joints in the body, they can be prone to pain.
It is important that both joints work together because if they don�t it could result in more pressure on one joint than the other and this could cause the pain and discomfort that is associated with TMJ dysfunction.
What Are The Symptoms Of TMJ Dysfunction?
There are many symptoms of TMJ dysfunction and they may vary depending on the patient, the extent of inflammation or injury, and the cause of the dysfunction. The symptoms may appear suddenly when there is injury to the joint, or they can gradually develop over a period of months or even years. They may be mild and barely noticeable or they can be severe and debilitating. The most common symptoms of TMJ dysfunction include:
Jaw pain
Jaw pain when moving the joint such as chewing or talking
Popping or clicking of the joint
Pain in the face or side of the neck
Locking jaw
Headaches
Toothache
Earache
Clogged or �stopped up� ear
Ringing in the ears (tinnitus)
TMJ dysfunction can significantly impact a person�s quality of life because the pain prevents them from doing many things they normally do, and often the jaw itself simply no longer functions as it should.
What Causes TMJ Dysfunction?
Damage to the joint is the primary cause of pain associated with TMJ dysfunction. This can be the result of trauma such as:
Subtle movements done repetitively can also cause TMJ dysfunction:
Grinding teeth
Holding a phone between the head and shoulder
Clenching teeth
Nail biting
Gum chewing (excessive)
Eating hard or tough foods
How Can Upper Neck Misalignment Cause TMJ Dysfunction?
When the upper neck sustains trauma such as whiplash it can cause a misalignment. This can also cause TMJ dysfunction in a couple of ways. It can cause one side to work harder or sustain more pressure than the other, or it can put excess pressure on the trigeminal nerve. This causes irritation and inflammation.
When left untreated, the condition can become severe. The misalignment keeps the joints from working as they should because opening and closing the jaw pinches the disc. This results in painful spasms in the shoulder and neck muscles when the patient does simple, everyday activities like talking, smiling, eating, or laughing.
Chiropractic For TMJ Dysfunction
Chiropractic can be a very effective treatment for TMJ dysfunction, especially if it is due to neck misalignment. A chiropractor will perform spinal adjustments in order to realign the spine and neck, bringing the body back into balance. This will allow the jaw to work as it should, minimizing rubbing or friction in the joint.
The patient may also be told to apply heat, massage, and do special exercises for TMJ dysfunction that will help the joints heal and help to minimize the pain.
This condition is not always easy to diagnose so it is wise to talk to your chiropractor and get a diagnosis before attempting any treatment or home remedies for TMJ. Regular chiropractic treatment can not only relieve the pain of TMJ and help to heal it, it can also help prevent it. Your chiropractor can be a great ally in this endeavor.
Injury Medical Clinic: Shoulder Pain Chiropractic Treatment
One of my friends recommended me, over and over, and just extended how good he�(Dr. Alex Jimenez, D.C.) was. So I gave it a shot. I had really bad sciatica and it was killing me, I couldn’t walk, but he has been helping me out, I can walk now… I couldn’t walk more than 25 yards, it (sciatica) was really affecting me. I had to get some help. I can’t say enough about Dr. Jimenez, he’s been helping me out, I can walk.
Edgar M. Reyes
According to the American Association of Neurological Surgeons, approximately 75 to 85 percent of individuals in the United States alone will experience some form of back pain throughout their lifetime, where 50 percent will suffer more than one episode within a year. Back pain is one of the most common complaints frequently reported among the general population and it is often a symptom which could indicate the presence of another underlying condition. Back pain can be caused by a variety of factors, some due to bad habits, such as improper posture, and others due to injuries from accidents. Other health issues, such as degenerative disc disease, or DDD, and arthritis can also result in back pain.�While the causes can vary, they share the same symptoms.
Bak pain can include upper back pain, middle back pain and lower back pain, often connected to sciatica, or sciatic nerve pain, a condition characterized by the compression or impingement of the sciatic nerve found in the low back. Back pain and sciatica have been closely associated with several common health issues. Often times, sciatica, or sciatic nerve pain, is caused by an underlying health issue along the lumbar spine. The sciatic nerve is the longest nerve in the human body, which connects to nerve roots in the region of the lower back and runs through the buttocks, down along the hips and into the back of each leg. Further sections of this nerve then branch out from the calf to the foot and into the toes. Sciatica can be identified by the following symptoms.
Low back pain which radiates down one or both legs
Leg and/or foot pain along with tingling and burning sensations
Numbness in the leg, feet and/or toes
Persistent pain and discomfort on one or both sides of the buttocks
Intense painful symptoms in the lower extremities
Having difficulties when sitting and while getting up
It’s essential to understand that back pain and sciatica are not generally considered to be a specific health issue themselves but rather, they are usually only considered to be a collection of several symptoms associated with an underlying injury and/or condition. A proper diagnosis of the root cause of your symptoms is additionally important in order to safely and effectively treat back pain and sciatica. As mentioned above, numerous factors can cause back pain and sciatica symptoms. Below, we will discuss some of the most common spine health issues which can cause back pain and sciatica, including degenerative disc disease, lumbar spinal stenosis, lumbar herniated disc and spondylolisthesis. Approximately 90 percent of sciatica cases are due to disc herniations.
Degenerative Disc Disease
The degeneration of the intervertebral discs, found between each vertebrae of the spine, is a natural process which often occurs with age, while for some individuals, however, it can begin to develop earlier than usual. In a healthy spine, the intervertebral discs function as shock absorbers between the bones of the spine, which ultimately provide height and allow the back to remain flexible while resisting forces. As we begin to get older, these rubbery discs begin to shrink and lose integrity. Almost everyone will demonstrate signs of wear-and-tear along their spinal discs over time, but not everyone will experience degenerative disc disease, or DDD. Although not actually a disease, DDD refers to a condition in which pain with the degeneration of the intervertebral discs.
One or more degenerated discs along the length of the spine may irritate a nerve root and cause sciatica. This condition is commonly characterized when a reduced disc becomes exposed. Bone spurs can also develop with disc degeneration and can lead to sciatica. Symptoms of degenerative disc disease, or DDD, frequently occur along the lower back, however, they can also develop in the neck, depending on the location of the degenerated discs. Common symptoms of DDD include, pain and discomfort, particularly when sitting, bending, lifting or twisting, tingling sensations and/or numbness in the extremities, and lessened symptoms when walking and moving, as in with changing positions or lying down. Weakness in the leg muscles or foot drop may be a sign that there is damage to the nerve root.
Lumbar Spinal Stenosis
Another common cause of back pain and sciatica is lumbar spinal stenosis. The natural degeneration of the spine which occurs with age can cause a variety of changes to the spine. Lumbar spinal stenosis is brought on by a gradual narrowing of the spinal canal that is common in the aging process and it generally affects people over the age of 50. When the space around the spinal cord narrows, it can place unnecessary amounts of pressure on the spinal cord and nerve roots. Additionally, it can be the result of a bulging disk, enlarged aspect joints, or an overgrowth of tissue. Only a small number of individuals are born with spine health issues which can develop into lumbar spinal stenosis. This is known as congenital spinal stenosis and it is frequently diagnosed in men.
Arthritis, or the degeneration of any joint in the body, has been attributed to be the most common cause of spinal stenosis. As the intervertebral discs begin to wear-and-tear naturally begin, they can lose water content and eventually dry out, ultimately losing height and even collapsing. This can place pressure on the facet joints, the joints which provide flexibility and movement to the spine, resulting in arthritis. As a result, the ligaments around the structures of the spine can increase in size, lessening the space for the nerves. Also, the human body may respond by growing new bone, additionally narrowing the space for the nerves to pass through. Symptoms of lumbar spinal stenosis may include, pain, tingling or burning sensations, numbness and weakness, as well as less painful symptoms when leaning forward or sitting.
Lumbar Herniated Disc
A herniated disc is a condition which can occur anywhere along the length of the spine, however, it most commonly affects the lower back or lumbar spine. It may also be referred to as a bulging, protruding or ruptured disc. A lumbar herniated disc is considered to be one of the most common causes of back pain in the lower back, as well as sciatica. An intervertebral disc begins to herniate when the soft, jelly-like nucleus, known as the nucleus pulposus, pushes against its outer ring, known as the annulus fibrosus, due to wear-and-tear or a sudden injury. With persistent pressure, the jelly-like nucleus may push through the disc’s outer ring or it may cause the ring to bulge, putting additional pressure on the spinal chord and its surrounding nerve roots.
Moreover, the intervertebral disc material can release chemicals and/or substances which may ultimately irritate the surrounding structures of the spine, contributing to nerve inflammation. When a nerve root becomes irritated, it can potentially lead to symptoms of pain and discomfort, numbness and weakness in one or both legs, otherwise referred to as sciatica, or sciatic nerve pain. An individual may also develop a herniated disc without ever experiencing any symptoms. A lumbar herniated disc is generally caused by the natural degeneration of the spine and discs, however, trauma and/or injury may also result in lumbar disc herniations. Symptoms of a lumbar herniated disc includes sciatica, tingling sensations, numbness, weakness, and loss of bladder or bowel control in severe cases. This last symptoms will require immediate medical attention.
Spondylolisthesis
Spondylolisthesis is another common cause of back pain and sciatica, particularly in young athletes. Repeated stress on the lower back, or lumbar spine, can create a crack or stress fracture in one of the vertebrae. In these cases, however, the stress fracture can often weaken the bone so much, to the point where it is unable to maintain its proper position in the spine, ultimately causing the vertebra to begin to shift or slip out of place. This condition is what is commonly known as spondylolisthesis. In children and adolescents, spondylolisthesis can occur through periods of rapid growth, by way of instance, during an adolescent growth spurt. This condition frequently occurs as a result of overuse, overstretching, or hyperextension, and even due to genetics.
Many healthcare professionals characterize spondylolisthesis as either low grade or high grade, depending on how much the vertebrae have shifted or slipped out of place. A high grade slip is generally identified when more than 50 percent of the width of the fractured vertebra slips forwards onto the vertebra beneath it. Individuals with high grade cases of spondylolisthesis will commonly describe experiencing significant levels of pain and discomfort as well as nerve injury. In the majority of instances, however, individuals with spondylolisthesis will not experience any obvious symptoms, as a matter of fact, most are unaware of the condition till an x-ray is taken for an unrelated injury and/or condition. Individuals with spondylolisthesis may experience back pain and sciatica, including muscle spasms, back stiffness and tight hamstrings.
Dr. Alex Jimenez’s Insight
Back pain is one of the most common reasons why individuals often miss days from work or go to the doctor, as it has also become one of the leading causes of disability worldwide. As a matter of fact, it has been statistically determined that approximately 80 percent of people will or have experienced back pain at least once throughout their life. Fortunately, a variety of treatments are available which can help ease the symptoms of back pain. It’s essential to understand back pain and sciatica, a collection of symptoms commonly associated with spine health issues along the lower back, in order to seek proper diagnosis and continue with an appropriate treatment plan in order to relieve your symptoms of back pain and sciatica.
Treatment for Back Pain and Sciatica
Chiropractic care is a well-known, alternative treatment option commonly utilized to help diagnose, treat and prevent back pain and sciatica. Since there are many factors which can contribute to symptoms of back pain and sciatic nerve pain, a doctor of chiropractic’s, or chiropractor’s, initial step would be to determine the root cause of the patient’s symptoms. Determining a diagnosis involves a thoughtful review of the patient’s health history, and a physical and neurological examination. Diagnostic testing may involve an x-ray, MRI, CT scan and/or electrodiagnostic tests, such as a nerve conduction speed evaluation or an electromyography. These examinations and tests help determine possible contraindications to treatment.
The aim of chiropractic care is to help promote the human body’s potential to heal itself. It is based on the scientific principle that limited spinal motion results in pain and reduced function and performance. Chiropractic care is non-invasive, or non-surgical, and drug-free. The type of chiropractic treatment provided is dependent upon the cause of the individual’s back pain and sciatica. A treatment program may include many distinct treatments and therapies, like ice/cold therapies, ultrasound, TENS, and spinal adjustments or manual manipulations. If the doctor of chiropractic decides that the patient’s spinal health issue requires treatment by a different kind of physician, then the individual may be referred to another healthcare professional.
Physical therapeutics for these conditions is also effective and generally has two components: active and passive. Passive physical therapeutics consist of ultrasound, electric stimulation, heat and ice packs as well as iontophoresis. Active physical therapeutics modalities include stretching exercises, back exercises and low-impact aerobic conditioning. Manual physical therapeutics, such as spinal adjustments and/or manual manipulations, might be integrated in part by a chiropractor. Physical therapists normally recommend 20 minutes of dynamic lumbar stabilization exercises every day. Core muscle strengthening is also important in treating back pain. Low-impact aerobics are also important and include water therapy, biking, and walking.
Physical therapeutics are an important element of treating spinal health issues. If you meet with a physical therapist, there will be a full assessment. Tests will be performed and an individualized treatment plan will be developed based on the patient’s goals. If you’re experiencing back pain or sciatica, don’t wait any longer for relief. Contact a healthcare professional to establish a one-on-one consultation and complete evaluation. Many chiropractors and physical therapists are certified, experienced and dedicated to helping you feel better. They have helped many others recover from spinal health issues and can help you too. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Many headaches that people classify as migraines are actually not migraines at all. Two of the most common headaches confused with migraines are sinus headaches and occipital neuralgia.
The condition can be debilitating but there are treatments, including chiropractic, that are very effective. Understanding occipital neuralgia can help patients better manage it so they can minimize the pain and symptoms of the condition.
What Is Occipital Neuralgia?
Occipital neuralgia is a neurological condition that affects the occipital nerves which run from the top portion of the spinal cord, through the scalp, transmitting messages to and from the brain. There are two greater occipital nerves, one on each side of the head, from between the vertebrae located in the upper neck through the muscles that are located at the base of the skull and back of the head.
While they do not cover the areas on or near the ears or over the face, they can extend over the scalp as far as the forehead. When those nerves are injured or become inflamed, occipital neuralgia is the result. A person with this condition may experience pain at the base of their skull or the back of their head.
What Are The Symptoms Of Occipital Neuralgia?
Pain is the prevalent symptom of occipital neuralgia. It often mimics the pain of migraine headaches or cluster headaches and is described as throbbing, burning, and aching.
There may also be intermittent shooting or shocking pain. Typically, the pain begins at the base of the skull but may radiate along the side of the scalp or in the back of the head. Other symptoms include:
Pain is experienced on one side (but sometimes both sides)
Pain behind the eye of the side that is affected
Tenderness in the scalp
Sensitivity to light
Pain triggered by neck movement
What Causes Occipital Neuralgia?
Irritation or pressure to the occipital nerves are what actually cause the pain. This may be due to tight muscles in the neck that squeeze or trap the nerves, injury, or inflammation.
However, much of the time doctors are unable to determine the cause. There are several medical conditions linked to occipital neuralgia:
Tight neck muscles
Diabetes
Trauma or injury to the back of the head
Gout
Tension in the neck muscles
Whiplash
Inflammation of the blood vessels in and around the neck
Infection
Neck tumors
Cervical disc disease
Osteoarthritis
What Are The Treatments For Occipital Neuralgia?
Occipital neuralgia treatment focuses on pain relief. It often begins with conservative treatments that include:
In more severe cases the patient may be prescribed a stronger anti-inflammatory medication, muscle relaxants or in some cases an anticonvulsant medication.
If these therapies are not effective or do not bring about the desired level of pain relief, then doctors may recommend percutaneous nerve blocks and steroids. Sometimes surgery is recommended in cases where the pain is severe, chronic, and is unresponsive to more conservative treatments.
Chiropractic For Occipital Neuralgia
Chiropractic was once considered an �alternative� treatment for occipital neuralgia, but now it is often a regular part of recommended patient care. The advantage of chiropractic over medication or surgery is that chiropractic does not come with the side effects of drugs or the risks of surgery.
Another advantage is that chiropractic seeks to correct the root of the problem, not just manage the pain like other treatments.
Chiropractic treatment for occipital neuralgia may include lift adjustments, heat, massage, and traction. This will bring the body back into proper alignment and take the pressure off of the nerves as it loosens the neck muscles.
The patient stands a better chance of staying pain free when taking this treatment route.
Injury Medical Clinic: Doctor Of Chiropractic Near Me
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine