Dr. Alex Jimenez has a great therapy for cervical sprains. He is great with his hands; he has been able to relieve a lot of headaches and a lot of cervical sprains with the special techniques that he has.
Sandra Rubio
Vertigo is the sensation of spinning or a rocking whenever you’re still. It tends to last for hours even days. Medically, it is distinct from dizziness since it involves the feeling of motion. Vertigo is a health issue affecting the internal ear, particularly in the semicircular canals. These structures line with cells within the inner ear that are responsible for providing feedback on our position, and they act like a gyroscope for your own body.
Causes for Vertigo
Various causes can cause vertigo. The reason may be central or peripheral. While peripheral problems�are due to a health issue in the inner ear, central problems can�occur in the brain or spinal cord. Small crystals within the ear, known as otoconia, can also become loose and lead to irritation in a health issue called benign paroxysmal positional vertigo or BPPV. A�buildup in the inner ear can also lead to vertigo. Headaches, head injuries, strokes, tumors, and multiple sclerosis may also cause vertigo.
Head injuries can increase the risk factor for developing vertigo. Additionally, drugs and/or medications like aspirin, blood pressure prescriptions, and even antidepressants have been found to cause vertigo. For some people, vertigo�is caused by alcohol consumption.
Diagnosis and Treatment for Vertigo
To diagnose vertigo, a health professional will need a full record of your signs and symptoms, including recent illnesses, previous medical problems, and�use of drugs and/or medications. Afterward, a physical exam is performed. For vertigo, these often feature a neurological examination to examine brain function and determine if it is peripheral or central.
The health issue may pinpoint signs or symptoms of abnormal eye movement. The Dix-Hallpike test or the roll test may be done to determine this diagnosis. The evaluation repositions the head and tracks symptoms. The head is quickly transferred from side to side. An MRI or a CT scan can also help exclude structural issues. Electronystagmography may additionally be carried out to diagnose the health issue. A vertigo diagnosis is essential before following up with the best treatment.
The most effective treatments in the event of peripheral vertigo include partial repositioning movements. It’s called the canalith repositioning procedure or the Epley maneuver. Particular head movements are performed to move the crystals back into place. Cawthorne head exercises may also be performed to achieve this in a series of eye and head movements. These improve vertigo and contribute to the decreased sensitivity of the nerves. However, this needs to be done on a regular basis for optimum results. A qualified and experienced healthcare professional, such as a chiropractor, can perform these types of treatments.
Furthermore,�chiropractic care can help correct any spinal misalignments, or subluxations, which may be contributing to vertigo. Chiropractic care is a safe and effective alternative treatment option which focuses on the treatment of a variety of injuries and conditions associated with the musculoskeletal and nervous system. A chiropractor may also offer lifestyle modifications to help speed up the recovery process. Although some drugs and/or medications, such as�Meclizine, can be used to manage vertigo, keep in mind that these may only provide temporary relief.
Vertigo may occur due to health issues in the inner ear as well as due to disturbances in the pathways of the nervous system. Regardless of the cause, the persistent sensation of dizziness, followed by other symptoms, can ultimately impact an individual’s quality of life. Many healthcare professionals like chiropractors can help treat symptoms of vertigo.
Dr. Alex Jimenez D.C., C.C.S.T.
Prognosis for Vertigo
Most patients with peripheral vertigo can find substantial relief with treatment. It’s been suggested that the Epley maneuver in cases of BPPV cures as many as 90 percent of affected patients. It is unlikely that vertigo will persist past a few days, although there is a 15 percent recurrence of BPPV in the first year after an episode. Tests for any structural�problems of the brain, spinal cord, or ear may be necessary if vertigo continues.
If you are feeling dizzy with an awareness of motion, you might have vertigo. Ensure that your world stops spinning with the help of a certified and experienced chiropractor. Many trained in the Epley maneuver and the Cawthorne head exercises for vertigo. A chiropractor can even offer you instruction on how to do these exercises. Contact a healthcare professional to complete an analysis of your symptoms and follow up with treatment.� The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
I have worked with several chiropractors in the professional area and he’s (Dr. Alex Jimenez) very good as a doctor, he’s awesome. He educates you and he really cares about his patients, along with the staff. Dr. Alex Jimenez makes you feel very welcomed.
Araceli Norte
Balance is something which many people take for granted throughout the majority of their life. In the early stages, as infants become toddlers, they learn to keep their balance, we cheer and then celebrate. They�also learn how to develop their balance when riding a bike. As we age, however, our balance becomes a little bit less reliable, where we often need to work to remain on our own two feet. When our equilibrium starts to falter, we realize just how much we heavily depend on our ability to stay balanced.
Reduction of equilibrium will happen to even the most powerful of individuals. For some, this means having to use a walking stick to help them move around or spending time in a wheelchair. As is correct with balance and gait disorders caused by neurological health issues, equilibrium issues can become worse over time. Problems like vertigo can block you from ever feeling genuinely secure. It is essential to concentrate on regaining your balance by focusing on improving your gait while this occurs.
Slip and fall injuries or accidents are a constant worry for seniors as well as for those who have physical difficulties or balance and gait disorders. Most of the time, those concerns aren’t unfounded. As a matter of fact, falls have been accounted as a�significant cause of severe injury-related health issues in the United States. In this article, we will discuss equilibrium and the type of treatment options available which can help improve balance.
Causes of Balance & Gait Disorders
The speed and style in which you walk are referred to as your gait. It is fundamental to seek proper treatment if you have to work on your walking. It’s also very common among athletes, although this is a process which many individuals often only have to do after suffering an injury in their lower extremities. Runners use treatment as a means to improve leg and foot motion as well as to increase stability and pace.
An individual’s ability to maintain balance while moving along with your gait is interrelated; you can not master one without focusing on the other. Chiropractic care will help you learn these skills to decrease your risk of injury, while at the same time increasing your confidence and independence. Before seeking treatment for balance and gait disorders, however, it’s essential to understand the causes of these health issues.
There are numerous factors which might affect your ability to keep balance. One of which is muscle atrophy. In this case, it is not an injury that holds you back. Instead, it’s often a natural process resulting in structural and functional weakness. Loss of balance stems from the sensation of “running out of steam.” The increased fatigue means that you are more likely to injure yourself, creating a flow of imbalance. Exhaustion, poor posture, and slow reflexes can ultimately make moving more difficult than it is.
Your ability to keep equilibrium depends on far more than a pair of healthy feet and caliber sneakers. Your balance and gait are also connected to your nervous system. Each of the following body parts listed below can play a significant role in your ability to stay balanced, these include:
Inner ears
Eyes
Joints
Muscles
Nervous system
Cognitive functions
Treatment which enhances balance and gait works with the different�parts listed above to keep them functioning correctly. Balance and gait treatment�comes with a selection of advantages, with preventing injuries being at the top of the list. You’re also more inclined to feel confident beyond lessening your chances of falling or feeling dizzy. Besides, those aches and pains caused by poor posture are also likely to decrease.
�
Maintaining balance in your body is essential but when you have balance and gait disorders, this can often be difficult to achieve. Chiropractic care can help keep balance in your life. Spinal adjustments and manual manipulations can help improve overall health and wellness. For balance, chiropractic care can help provide strength, flexibility and mobility, making sure the body is functioning properly.
Dr. Alex Jimenez D.C., C.C.S.T.
Chiropractic Care for Balance & Gait Disorders
Chiropractic care, along with physical therapy, is considered to be one of the most effective treatments for balance and gait disorders. Working with an experienced chiropractor can enable you to regain your stamina by adopting new approaches regarding posture and movement. Exercises can help you feel more confident and more aware on your feet, and strength to the muscles will lessen fatigue as well as decreasing your chance of injury.
The very first thing to expect when meeting a chiropractor for the treatment of balance and gait disorders is a complete evaluation. You’ll be asked to walk, and the healthcare professional will take notes concerning your step style, foot placement, and pace. Possible health issues associated with your own strength will be identified and a treatment plan will be designed to ascertain which exercises will be ideal for your specific requirements. Checking balance is also a part of this assessment.
Hip and ankle problems frequently lead to balance and gait disorders, as does poor posture. Strength and flexibility exercises can help. These usually�involve leg lifts while seated in a chair, or “knee marching.” Chiropractors and physical therapists may even have you practice walking heel-to-toe, standing on one leg, or they may monitor�the movement of your thumb with your eyes as you move it in various positions.
It’s essential to seek immediate medical attention to find a proper diagnosis and continue with treatment for balance and gait disorders. A qualified and experienced chiropractor and can restore your confidence as well as to promote appropriate recovery. Contact a healthcare professional to regain your freedom. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
The human body is an intricate machine, and everything is connected so when something goes wrong in one area, it can cause problems in other areas. The back carries a lot of the stress in the body so when there is a problem with the hips, knees, or a foot dysfunction, the spine can bear at least some of the brunt of the pain and other effects.
Pronation describes the way that the foot rolls inward during its normal motion. The foot turns inward, flattening out, as the heel�s outer edge strikes the ground.
For the foot to function correctly, there must be a significant degree of pronation. However, excessive pronation, or overpronation, can cause injury and damage to the foot and ankle. It creates the arch in the foot to flatten, and the ligaments, tendons, and muscles under the foot overstretch.
What is Supination and Oversupination
Supination describes the way the foot rolls outward during its normal motion. It occurs during the push off part of the gait, mainly when running when the heel lifts. The heel leaves the ground, and the movement carries through as weight transfers to the forefront and toes. It moves the body in a forward direction.
When there is excessive supination or oversupination, it strains the tendons and muscles that provide stabilization for the ankle. Causing the ankle to roll, causing injury to the ankle including overpronation sprain, a torn tendon, or ligament rupture.
Conditions and Injuries Caused by Overpronation and Oversupination
Overpronation and oversupination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees, hips, and back as well. Some of the more common injuries and conditions include:
Flat feet or posterior tibial tendon dysfunction
Ankle Sprains
Achilles tendinitis
Arch pain
Plantar fasciitis
Corns
Shin splints
Heel pain
Tight calves
Calluses
Knee pain
Patellar tendonitis
Hip pain
Tight hip flexors
Back pain
Sciatica
Herniated disks
How Foot Problems can Cause Back Pain
Foot Dysfunction can very easily cause a domino effect that extends all the way to the back. The feet are the foundation of the body and when there is a problem with the way they function it can cause the entire body to shift out of alignment.
For instance, overpronation of the foot causes a series of internal changes that extend up through the leg. The femur may rotate causing hip pain and inflammation of the sacroiliac joint which leads to back pain. Other misalignments in the body that are caused by foot problems can also lead to chronic lower back pain as well.
Chiropractic to Treat Foot Problems
Chiropractic seeks to find the cause of the conditions it is used to treat, including pain, instead of just treating symptoms. Because of this, the chiropractor will work to find the cause of the pain, in this case, overpronation and overpronation, and correct it � or the effects of the condition � in addition to treating the back pain.
Typically, overpronation and oversupination, are caused by muscle imbalances in the foot, ankle, and lower leg. Improper shoes, misalignment in the body, and other issues can cause these muscle imbalances. The chiropractor will work with the patient to find the cause of the foot problem so that can be corrected, then work to the damage or injury done.
Foot Dysfunction & Back Pain Chiropractic Treatment
Of course, I’m prone to injuries and Dr. Alex Jimenez has been helping me. I’ve known him for about six years and every time something comes up, either it’s a small injury or a major one, he’s always been there and he’s always helped me get back to my feet to start playing sports again really fast.
Madison Hill
Ankle pain refers to any type of pain or discomfort in the ankle. This pain could generally be due to an injury, such as a sprain, or due to another health issue. As stated by the National University of Health Sciences, or NUHS, an ankle sprain is one of the most frequent causes of foot pain, making up 85 percent of all ankle injuries. A sprain occurs when the ligaments tear or are overstretched.
Most ankle sprains are lateral sprains, which occur when the foot rolls, causing the ankle to twist toward the ground. This action rips or stretches the ligaments, which connect two bones or cartilages and holds a joint together. A sprained ankle often swells and lumps for a temporary amount of time. However, it might take a couple of weeks to get a severe injury like this to�heal completely.
Once healed, the sprained ankle is occasionally permanently weaker and less stable compared to the other ankle. According to a paper released by the American Academy of Family Physicians, or AAFP, the highest risk for ankle sprains includes a previous ankle sprain. Although, ankle sprains are not the only cause of foot pain. Below, we will discuss several common causes of foot and ankle pain as well as their treatment.
Causes of Ankle and Foot Pain
The ankle is a hinge joint formed by the assembly of three bones: the tibia, the fibula, and the talus. The bony knobs on both sides are called the malleoli. Overall, the ankle is an intricate structure. These constructions provide support for walking and standing. Also, stability is provided by the ligaments on the surface of the ankle. Additionally, some tendons also attach to the muscles of the ankle.
Ankle pain may be brought on by various ailments, such as sprain, strain, arthritis, gout, and tendinitis, among others. These kinds of injuries can occur on both sides of the joint. There can be pain and discomfort as well as swelling. A sprain is considered to be the most frequent cause of foot pain. As�mentioned above, a sprain is generally caused when the ankle rolls or twists so the ankle moves toward the ground, tearing or overstretching the ligaments of the ankle that hold the bones together.
An x-ray is typically done to rule out a fracture. The remedy for an ankle strain or sprain generally includes restricting the total amount of weight-bearing on the ankle, getting rest and applying ice. Drugs and/or medications can reduce symptoms. Chiropractic care can also help diagnose and treat ankle sprains and strains. Ankle and foot pain may also be due to:
Arthritis, specifically osteoarthritis,
Gout
Tendinitis
Nerve injury or disease, such as sciatica
Blocked blood vessels
Infection from the joint
While ankle strains and sprains are the most common form of foot pain, arthritis can also frequently lead to ankle pain. Arthritis is the inflammation of the joints, although multiple kinds of arthritis may lead to pain in the joints. Foot pain can be caused by three common forms of arthritis: osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis.
Osteoarthritis is a degenerative condition where the cartilage slowly begins to wear away. Osteoarthritis�causes the natural wear and tear of the joints associated with age. Older adults are more inclined to develop osteoarthritis. In most cases, an individual’s pain and discomfort, including swelling and�stiffness, among other symptoms may worsen over time.
Rheumatoid arthritis is a chronic autoimmune disease. This health issue may severely impact the foot and ankle joints. With rheumatoid arthritis, the human body’s immune cells attack the synovium covering the foot joints. Joint deformity is common with rheumatoid arthritis. A fungal or bacterial infection causes septic arthritis. If the septic arthritis is among the ankle regions, this may result in foot pain.
Following an injury, post-traumatic arthritis can develop from trauma or damage to the ankle or foot. Previous fractures and dislocations are the most common ailments that may lead to post-traumatic arthritis. Like gout, which we will discuss further below, the joints begin to wear away, although it may take several years for this to happen after the injury.
Gout occurs when uric acid accumulates in the human body. This higher than average concentration of uric acid, which is generally a by-product of the human body’s normal breakdown of older cells, can deposit crystals in the joints, causing sharp pain. Pseudogout is a similar illness where calcium deposits build up in the joints. Indicators of gout and pseudogout include soreness, swelling, and redness.
Tendinitis is a swelling of the tendon. In the ankle, it may frequently involve the anterior tibial tendon or the Achilles tendon. Tendinitis can result from an overuse injury or disorders like rheumatoid arthritis and ankylosing spondylitis. All types of tendinitis trigger pain, inflammation, and tenderness. Drugs and/or medications, applying ice and immobilizing the region are often the first line of treatment for tendinitis. Chiropractic care can also be helpful in the treatment of tendinitis. Casting may be required if the patient’s tendinitis is severe or advanced.
�
Foot pain can commonly occur due to ankle injuries. In the United States alone, approximately 2 million acute ankle sprains occur every year, one of the most prevalent causes of ankle pain. Chiropractic care is a popular alternative treatment option which can help treat a variety of health issues, including foot and ankle pain.
Dr. Alex Jimenez D.C., C.C.S.T.
Chiropractic Care for Foot and Ankle Pain
Chiropractors utilize a mixture of treatment techniques and methods to ease ankle and foot pain. Chiropractic care is a safe and effective, alternative treatment option which focuses on the diagnosis, treatment, and prevention of a variety of injuries and conditions associated with the musculoskeletal and nervous system, including foot and ankle pain.
Soft tissue and joint mobilizations are done to restore proper mechanics and muscle activation. Manual therapy may be used to improve the mobility of the ankle and foot along with reducing pain. Furthermore, a chiropractor may recommend a series of lifestyle modifications to help promote a faster recovery process. Exercises are targeted to the areas that were affected. Balance training might also be implemented.
Some treatment modalities that chiropractors utilize to treat injuries to the foot and ankle include ultrasound, electrical stimulation, heat and ice treatment, and massage. These treatment methods increase circulation to enhance recovery, decrease inflammation, reduce pain and improve mobility. When you visit a healthcare professional, a full evaluation is done, goals are discussed along with an individualized treatment program which is intended to target your specific treatment requirements.
Home Treatment for Ankle and Foot Pain
For immediate at-home treatment of foot and ankle pain, the RICE system is generally recommended. The RICE treatment includes:
Rest: Avoid putting weight on the ankle. Try to move as little as possible for the first couple of days. If you have to walk or run, consider using a cane or crutches.
Ice: Begin by putting a bag of ice in your ankle for a minimum of 20 minutes at a time. Repeat this three to five times every day for three days. This�treatment helps decrease pain. Give yourself about 90 minutes between sessions.
Compression: Wrap your injured foot with an elastic bandage, such as an ACE bandage. Don’t wrap it too tightly to where your feet turn blue or your ankle becomes numb.
Elevation: Whenever possible, keep your ankle raised over heart level on a pile of pillows or another type of support arrangement to promote healing.
It’s possible to take over-the-counter drugs and/or medications, such as acetaminophen or ibuprofen, to relieve swelling and pain, however, these are often only offer temporary relief from the symptoms. Make sure to talk to a certified and qualified healthcare professional regarding any home treatment options to prevent further injury and symptoms.
If�you are suffering from foot pain or ankle pain, do not delay anymore. Chiropractors can help patients who suffer from foot, and ankle pain and they can help you, too. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is attributed�to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Ever since he started chiropractic care with Dr. Alex Jimenez and continued rehabilitation at Push, Bobby Gomez has experienced great improvements on his back and hip pain. Since birth, Bobby had problems walking due to an uneven pelvic tilt. However, treatment has helped him gain more muscle on his legs, giving him more strength, flexibility and mobility to further improve his gait. Thanks to chiropractic care and rehabilitation, Bobby Gomez has become more confident and at peace with himself, highly recommending Dr. Alex Jimenez as the non-surgical choice for hip pain.
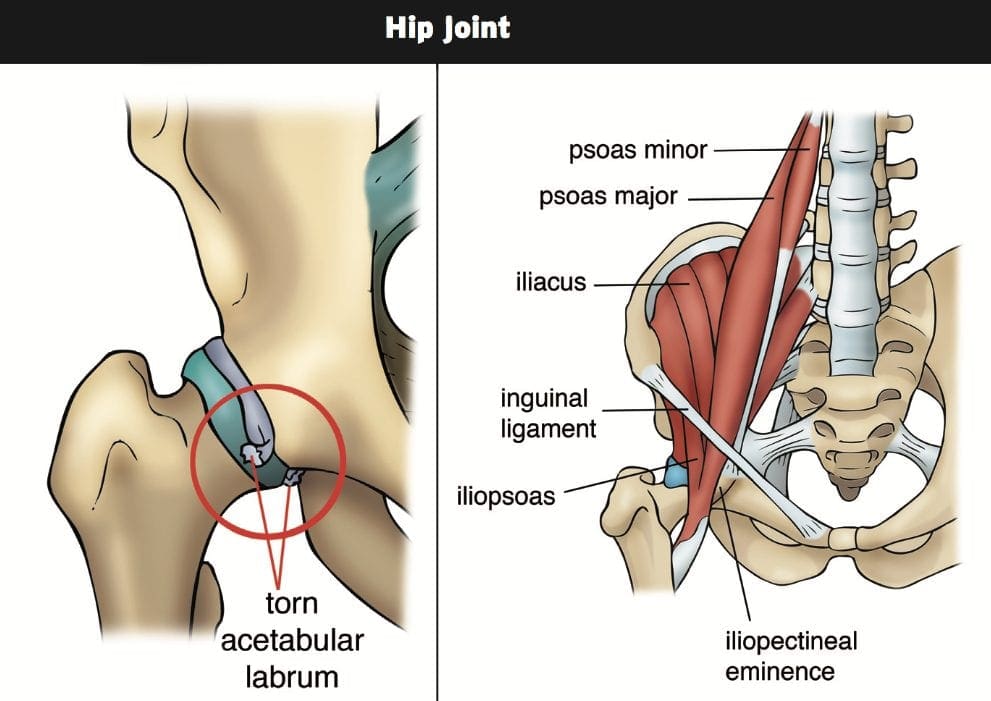
Chiropractic Hip Pain Treatment
Pain in the hip is the experience of pain from the joints or muscles in the hip region, a condition arising from any of a number of variables. Occasionally it is associated with back pain. Causes of pain around the hip joint may be extra-articular, or referred pain from neighboring structures, including the sacroiliac joint, spine, symphysis pubis, or the inguinal canal. Clinical tests are accommodated to identify the source of pain as intra-articular or extra-articular. The flexion-abduction-external spinning (FABER), internal range of motion with overpressure (IROP), and scour tests reveal sensitivity worth in identifying individuals with intra-articular pathology.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Chiropractic treatment is dedicated to finding and correcting spinal misalignments. Many seek chiropractic care to alleviate pain and other health-related symptoms. One condition that is sought out constantly, is relief from lower back pain.
31 million Americans experience low back pain at any given time. This condition affects many, but finding the exact cause can be a challenge. Chiropractors are spinal specialists that are trained to not only alleviate pain but also find and help correct the cause of the problem.
Prevention Is The Best Defense
Prevention is the best cure for any condition/ailment. When a someone sees a chiropractor, they not only find relief for their condition, but they learn ways to prevent they symptoms in the future. Using proper exercise and ergonomics, they can ease the discomfort before it starts. Great results are gained by individuals that listen to instructions.
Treatment Options
Treatment options are plentiful. Based on the diagnosis they will suggest the ones that will benefit you the most. These treatments may include one or more of the following:
Spinal adjustments delivered either by hand or instrument like an Activator
Hot or cold compresses
Physical therapy modalities like Interferential Therapy or TENS
Massage Therapy or some other form of soft tissue work
Spinal decompression therapy
Relief
Prescription medication could still be required to help reduce levels. The good news is that the meds can be decreased quicker than usual, as the spine misalignments are corrected, nerve compression is alleviated and the inflammation is reduced. This alone is well worth the investment of time and money to see a chiropractor.
Exercise & Physical Rehabilitation
As the treatment progresses from pain relief to rehabilitation, a chiropractor will recommend exercises to help strengthen the core muscles. These muscles help stabilize and protect the lower back. These exercises are performed at the office or specialized fitness center with certified physical therapists/trainers to make sure you understand how to do them without re-aggravating the original condition. Once educated on the purpose and how to perform them correctly, you�ll be able to continue at home in conjunction with spinal adjustments during maintenance care.
Surgery Options
Depending on the condition, surgery can be avoided if chiropractic treatment is implemented before injury/s or pain worsen. A chiropractor can help avoid surgery by correcting the problem.
Make sure you follow the recommendations after a consultation and examination are performed. The examination may require X-rays or MRIs.
A chiropractor is the ideal medical professional to consult with for any unexplained pain in the musculoskeletal system. They are highly qualified professionals that their specialty is treating conditions like lower back pain and they are very affordable. If you or a loved one have pain in the lower back, gives us a call. We�re here to help!
Dr. Alex Jimenez is excellent, he’s patient, he gets right to the point of the situation, and then helps you with your stretching and therapy to make sure that it doesn’t continue. I recommend him for everybody in El Paso, the whole state of Texas. He should be in every town, move to San Antonio. -�Ottis Hamlet
Are you aware of how dependent you are on the use of your hands for everyday tasks? As humans, we rely tremendously on the proper function of our hands, wrists and elbows to perform many physical activities. Many people may not understand how essential this can be until they encounter an injury or condition which impedes them from using their hands.
Hand, wrist and elbow pain can cause a wide variety of problems, preventing you from being able to take part in even some of the simplest, ordinary chores without experiencing painful symptoms. Based on the severity of the pain, health issues affecting your hands, wrists or elbows can prevent people from driving, utilizing a computer or other electronic devices, cooking dinner and it can even make working difficult.
To make matters worse, the condition of your hands can ultimately affect the entire condition of your upper extremities. An injury or aggravated condition along a single part of the hand, such as a finger, could cause pain to radiate through the wrist and elbow, into the arm and shoulder. Below, we will discuss the common causes of hand pain and their treatment.
Common Causes of Hand Pain
While many instances of hand pain, wrist pain and elbow pain may resolve on their own, a minor inconvenience can quickly become a much bigger health issue if left untreated. Painful symptoms can slow us down as we’re attempting to go about our day and chances are that the need to finish a job will continue to aggravate the pain and cause discomfort. If you experience chronic hand pain symptoms, you may want to visit a doctor immediately.
Because our arms and hands are interconnected, an injury or condition to any part of the upper extremities can end up causing anything from tingling sensations and numbness in the fingers to pain and discomfort in the arms. A qualified and experienced healthcare professional, such as a chiropractor, can help you understand the source of your hand pain as well as determine the best treatment option for your specific health issue.��
There are many health issues which might lead to pain and discomfort in the hands, elbows and wrists. Common causes of hand pain include:
Joint pain
Arthritis
Tendonitis
Tennis/Golf Elbow
Fractures
Sprains
Carpal tunnel syndrome
Carpal Tunnel Syndrome
One of the most common causes of hand pain is the result of a chronic condition called carpal tunnel syndrome. Carpal tunnel syndrome, or CTS, is a painful syndrome caused by a pinched nerve in the wrist which causes pain, tingling sensations and numbness in the hand and arm. The pain usually feels like a�profound and intense hand cramp although cramping is not a common symptom associated with carpal tunnel syndrome.
Carpal tunnel syndrome develops due to heightened stress and pressure on the median nerve, frequently due to highly repetitive movements with the hand and wrist. Some of the most common tasks in today’s society,�such as writing, typing on a keyboard, playing with video games, gardening, and anything else which requires repetitive alternative or lifting hand motions, have become one of the leading causes of carpal tunnel syndrome.
As mentioned above, several common symptoms of carpal tunnel syndrome, or CTS, may cause�severe pain in the hand, wrist and elbow, as well as result in tingling sensations and numbness which may radiate from the fingers up to the arm. Research studies have also found that patients who may be experiencing hormone fluctuations are at an increased risk of developing the condition. However, people who are most at risk of developing CTS have been found to be those who work in a position that requires them to engage in repetitive motions with their hands.
Many healthcare professionals recommend surgical interventions to treat carpal tunnel syndrome but many patients have experienced relief from their hand pain through the use of alternative treatment options, such as chiropractic care,. Moreover, wearing a brace, working to counteract repetitive motions and taking steps to decrease stress and pressure on the hand can help improve pain associated with carpal tunnel syndrome.
While a number of these treatment techniques and methods can be performed at home by the patient, it’s essential to seek immediate medical attention from a qualified and experienced healthcare professional to avoid further damage. A chiropractor can help treat hand pain. Below, we will describe how chiropractic care may improve chronic hand pain symptoms.
Because we depend tremendously on the use of our hands, injuries and/or conditions which result in hand pain, such as carpal tunnel syndrome, can be very debilitating, ultimately affecting every aspect of an individual’s quality of life. Chiropractic care is a safe and effective, alternative treatment option which can help treat hand pain. Through a series of exercise and physical activity programs, chiropractic care can help restore normal hand function and reduce hand pain. -�Dr. Alex Jimenez D.C., C.C.S.T.
Chiropractic Care for Hand Pain
Chiropractic care is a healthcare profession which utilizes spinal adjustments and manual manipulations to treat a variety of injuries and conditions associated with the musculoskeletal and nervous system. For a doctor of chiropractic, or chiropractor, the first step for managing hand, wrist or elbow pain is to evaluate the source of the symptoms.�
After the diagnosis, the chiropractor’s next priority is to use a series of alternative treatment options to relieve the patient’s hand pain as soon as possible. A chiropractor may use spinal adjustments and manual manipulations to carefully correct any spinal misalignments, or subluxations, which may be causing referred hand pain.
After that, a chiropractor may recommend a series of lifestyle modifications, including exercise and physical activity programs, in order to promote recovery and begin focusing on building the patient’s assortment of motion, particularly flexibility maneuvers. Stretches and exercises for building strength will be included following the patient’s treatment plan, in order to ensure no additional damage occurs.
When you’re ready to start, contact a chiropractor to set up an appointment to get yourself on the road to relieving your hand, wrist and/or elbow pain.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine