El Doctor de Medicina Funcional Explica el Cuidado de Enfermos y el Cuidado de Salud
Hoy analizaremos los fundamentos de la medicina funcional y c�mo puede construir una relaci�n saludable entre m�dico y paciente.
Si visita al m�dico porque ha experimentado migra�as, eczema, s�ndrome del intestino irritable y depresi�n, lo m�s probable es que lo refieran a cuatro especialistas diferentes e incluso se le receten un m�nimo de cuatro medicamentos diferentes. Un enfoque de la medicina funcional comprende que puede haber problemas comunes de salud que pueden estar causando los s�ntomas de un paciente. Una vez que llegue al origen del problema, se puede solucionar los problemas de salud que crean los s�ntomas.
La medicina funcional pregunta: “�Por qu� tiene esos s�ntomas y c�mo podemos tratar la fuente del problema y mejorar su salud y bienestar general?”, en lugar de “�Qu� enfermedad tiene y qu� medicamento usa para tratarla?”
�Que es el Cuidado de Enfermos y el Cuidado de Salud?
Hola a todos, mi nombre es Dr. Alex Jim�nez. Soy quiropr�ctico y practicante de medicina functional en El Paso, Texas. Estoy muy contento/a de poder presentarles la primera parte de “C�mo Tomar el Control de su Salud”, donde analizaremos las diferencias entre �el Cuidado de Enfermos y el Cuidado de la Salud”. Por lo tanto, con frecuencia escucho a las personas hablar sobre lo dif�cil que es encontrar al m�dico adecuado, a alguien que est� dispuesto a trabajar con ellos, que los escuche y que est� abierto a satisfacer sus demandas mientras les ense�a todo lo que necesitan saber sobre sus problemas. Un m�dico que acepta avances innovadores en la ciencia y los enfoques de sistemas para determinar la fuente del problema. Esto se conoce como medicina funcional, y discutiremos m�s de eso en un minuto.
Mi objetivo en este momento es mostrarle c�mo puede encontrar al m�dico adecuado y establecer la mejor relaci�n con ellos para obtener la atenci�n que merece. Es importante hacerle varias preguntas a su m�dico para determinar si son adecuados para usted, si est�n dispuestos a trabajar con usted, a escucharlo y si est�n abiertos a sus solicitudes, as� como a aprender sobre los problemas que se les presentan. En lugar de no est�r familiarizado con ellos o que no sigan nuevos enfoques de tratamiento si se les presenta. A modo de ejemplo, si el m�dico que elige dice que la nutrici�n no tiene nada que ver con una enfermedad, entonces probablemente deber�a buscar otro m�dico. Ahora hablemos sobre las preguntas que debe hacerle a su m�dico sobre su salud y bienestar general para estar informado sobre lo que est� sucediendo en su propio cuerpo.
He hablado con pacientes que han visitado a numerosos m�dicos con la esperanza de encontrar una respuesta sobre por qu� no se sienten bien o tienen alg�n tipo de enfermedad. Muchos son referidos frecuentemente a uno o m�s especialistas y, en algunos casos, reciben Prozac, o se les dice que todos sus s�ntomas est�n en su cabeza o a veces incluso se les dice que no hay nada de malo despu�s de que todos los resultados de su laboratorio son normales. Y es frecuente que estos mismos pacientes sean enviados a varios m�dicos por cada parte de su cuerpo en lugar de ser enviados a un m�dico que pueda diagnosticar y tratar su cuerpo por completo. Si acude al m�dico y tiene migra�as, eczema, s�ndrome del intestino irritable y depresi�n, en la mayor�a de los casos, se le enviar� a cuatro especialistas diferentes y se le administrar�n, al menos, cuatro medicamentos diferentes, en lugar de visitar a un especialista que pueda comprender la fuente subyacente del problema y tratar la ra�z de los s�ntomas.
�Alguna vez ha visitado a un m�dico que, despu�s de explicarles sus s�ntomas, dice: “Oh, hice un panel de sangre completo y todo regreso normal”. Esto podr�a significar una de dos cosas, ya sea que est� loco o que les esta faltando algo. Y estoy seguro de que a menudo falta algo porque no buscan las respuestas en los lugares correctos. Es como una persona que deja caer sus llaves en la calle y cuando su amigo lo ve buscando debajo de una farola, dice: “Oye, �qu� est�s haciendo?”, Dice: “Estoy buscando mis llaves”. Entonces dice, �Pues d�nde las perdiste “. Y el dice:” Bueno, las perd� por la calle “.”� Entonces por qu� est�s buscando aqu�? “” Bueno, la luz est� mejor aqu� “. Y desafortunadamente, eso pasa mucho en la medicina. Los m�dicos buscar�n respuestas donde los problemas son f�ciles de encontrar. Y ese es el prop�sito de este video. Para ayudarlo a comprender c�mo puede encontrar la fuente de los problemas de salud subyacentes que lo hacen sentir mal.
Esto me recuerda a un caso de una mujer que vi en mi consultorio que ten�a artritis psori�sica, una afecci�n autoinmune que le caus� erupciones en todo el cuerpo junto con dolor e inflamaci�n en las articulaciones. Como resultado, ella consum�a grandes cantidades de drogas y / o medicamentos que sumaban alrededor de $60,000 d�lares al a�o o m�s. Tambi�n ten�a otros problemas de salud, ten�a reflujo �cido, s�ndrome del intestino irritable, pre-diabetes, migra�as, insomnio y depresi�n. Esta mujer visit� a muchos especialistas diferentes y estaba tomando recetas para tratar cada uno de sus s�ntomas. Cuando lleg� el momento de verla, todo lo que hice fue llegar a la fuente del problema.
Entonces, durante el diagn�stico, me dije a m� mismo: “Bueno, esta paciente tiene inflamaci�n, pero �cu�l es la causa de su inflamaci�n?” Y en lugar de recomendarla a muchos otros especialistas para que pudiera recibir medicamentos para sus migra�as, reflujo �cido, depresi�n, etc., me dije a m� mismo: “Oh, todos estos s�ntomas son inflamatorios, entonces, �cu�l es la ra�z de la inflamaci�n?” Bueno, resulta que la paciente tuvo problemas con su intestino todo el tiempo. Luego la ayud� a eliminar los “bichos malos” en su intestine, recomend�ndole una dieta anti-inflamatoria, inclu� algunos suplementos, aceite de pescado, vitamina D, probi�ticos. Sinceramente, remedios naturales realmente b�sicos. Cuando regres� seis semanas despu�s, todos sus s�ntomas hab�an desaparecido. Se hab�a retirado todos sus medicamentos recetados y hab�a perdido 20 libras. No le dije que dejara de tomar sus medicamentos, simplemente lo hizo por su propia cuenta. Fue absolutamente extraordinario y eso es lo que sucede cuando se trata la fuente de los problemas de salud subyacentes de un paciente. Y no tiene que hacer mucho para llegar a la ra�z del problema.
Entiendo que es posible que no siempre se pueda trabajar con un m�dico que est� capacitado en medicina funcional, de lo que hablaremos en un minuto. Sin embargo, es posible encontrar un m�dico que est� dispuesto a trabajar con usted, qui�n va a escuchar, qui�n tendr� la mente abierta y qui�n ser� su compa�ero durante su viaje hacia la salud y el bienestar en general. A lo largo de este video, analizar� las pruebas de laboratorio convencionales y las pruebas de laboratorio de medicina funcional innovadora, demostrando todo con el prop�sito de crear bienestar en lugar de verlo todo desde la perspectiva de la enfermedad para encontrar la fuente de los problemas de salud de un paciente y corregir los desequilibrios a trav�s de un enfoque de medicina funcional.
Tomando el Control de el Cuidado de Enfermos y el Cuidado de Salud
La medicina funcional a menudo se conoce como el futuro de la medicina, pero muchos m�dicos la ofrecen actualmente si visita el lugar correcto. El prop�sito de la medicina funcional es diagnosticar y tratar la causa de una variedad de enfermedades mediante la evaluaci�n del cuerpo por completo, en lugar de analizar cada colecci�n de �rganos de forma independiente a trav�s de especialistas independientes. La medicina funcional trata todo el sistema, no solo los s�ntomas. Los m�dicos que practican la medicina funcional con frecuencia se preguntan: “�Por qu� tiene el paciente estos s�ntomas y c�mo puedo corregir las causas y mejorar su salud y bienestar general?”, En lugar de “�Qu� enfermedad tiene el paciente y qu� medicamento utilizan para tratarlo?�
He sido un quiropr�ctico practicante por m�s de 25 a�os. Y he presenciado innumerables milagros todos los d�as. Mis pacientes no solo encuentran alivio de sus s�ntomas, realmente logran alcanzar el bienestar general. Desafortunadamente, nuestro sistema de salud actual est� roto. Muchos m�dicos se ven tremendamente afectados debido a las limitaciones de tiempo establecidas por las compa��as de seguros para pagar las facturas, lo que hace que se apresuren a acudir a sus citas. A la vez, este ciclo continuo con frecuencia puede terminar dejando a los pacientes con preguntas sin respuesta y frustraci�n. Nuestro sistema de atenci�n m�dica actual hace que las personas se sientan impotentes, a menudo manteni�ndolas atrapadas con sus enfermedades.
Como parte de este sistema de salud, es importante que entendamos que algunas enfermedades no son tan f�ciles de tratar como un resfriado. Varias enfermedades tampoco se desarrollan de forma aleatoria. La mayor�a de las enfermedades que existen en la actualidad est�n relacionadas con su entorno y como estos factores externos e internos interact�an con sus genes y estilo de vida para influir en su salud y bienestar.
Lo que hoy conocemos como el enfoque de la �medicina convencional� se conoce generalmente como el juego de �nombrarlo, culparlo y domesticarlo�. Primero, el m�dico diagnosticar� al paciente y le proporcionar� una etiqueta, por ejemplo, dicen que un paciente tiene depresi�n. Ahora tienen el nombre de la enfermedad. Y finalmente, el m�dico tratar� la enfermedad con medicamentos recetados. Al final, el paciente se queda tomando un antidepresivo. Sin embargo, la depresi�n puede ser causada por una amplia gama de factores y la soluci�n no es necesariamente un antidepresivo. Este tipo de pr�ctica no solo est� desactualizada, sino que en realidad se considera bastante inseguro a largo plazo. Y a menudo no proporciona a los pacientes los resultados que necesitan. Las personas son diagnosticadas err�neamente y con frecuencia quedan enfermas sin recibir realmente la atenci�n adecuada que merecen.
La medicina convencional tambi�n puede ser �til en las etapas finales de algunas enfermedades, as� como para enfermedades agudas. Si tiene una emergencia o se siente muy enfermo, si se rompe un hueso, o si tiene una infecci�n, la medicina convencional, los cuidados intensivos, los medicamentos pueden ser la soluci�n adecuada y deber�amos estar sumamente agradecidos por ellos. Pero este no es el enfoque que necesitamos para prevenir y curar enfermedades cr�nicas. Si realmente entendi�ramos c�mo cuidar nuestros cuerpos como deber�amos, la mayor�a de nosotros no nos sentir�amos tan enfermos. Y muchas personas seguiran sinti�ndose enfermas, pero no tiene que hacerlo, no es normal. Muchos m�dicos ahora entienden que se requiere un cambio para convertir todo nuestro sistema de atenci�n de enfermos en uno que realmente respalde la atenci�n m�dica.
Me gustar�a capacitarlo para ayudar a transformar el futuro del campo de la medicina al tomar su bienestar en sus propias manos. A lo largo de los pr�ximos videos, compartir� con usted c�mo puede encontrar un m�dico que tenga en cuenta sus valores y creencias personales para que pueda lograr los resultados que est� buscando mientras se encuentra en un entorno seguro y c�modo. Puede aprender a ser su propio defensor de la salud y convertirse en un verdadero socio con su m�dico. Y hay muchos otros m�dicos y practicantes de medicina funcional como yo que est�n esperando para ayudar.
Adem�s, compartir� con usted c�mo puede encontrar al mejor m�dico y tambi�n le proporcionar� muchas otras herramientas para ayudarlo a ser el l�der de su salud y bienestar en general. Ademas de c�mo puede tomar el control de su propio bienestar. Incluyendo el trabajo de laboratorio que debe solicitar a su m�dico y c�mo entender qu� significa la informaci�n y qu� debe hacer con ella. Una de las formas m�s comunes en que los m�dicos utilizan los laboratorios es evaluar qu� es lo que no funciona cuando el paciente no se siente bien y analizar el final de un continuo de la enfermedad. Si su funci�n cambia, sus c�lulas hep�ticas pueden estar muriendo. Sin embargo, si son normales, muchos m�dicos dicen: “Oh, usted es normal”. Pero en realidad puede no ser normal. La buena noticia es que puede encontrar desequilibrios antes para tratarlos a tiempo.
Aunque est� cambiando lentamente, muchos m�dicos tienen la costumbre de no darles a los pacientes sus an�lisis de laboratorio reales. Y si este no es el caso, varios m�dicos no brindan explicaciones detalladas de las pruebas de laboratorio del paciente que no sean “Sus pruebas de laboratorio regresaron normales” o “Su colesterol esta un poco alto” o “Su nivel de az�car en la sangre esta alto”. Como quiropr�ctico, creo que todos deber�an tener acceso a sus an�lisis de laboratorio y que estos deben explicarsele al paciente. Tenemos que empezar a democratizar la medicina. Y esto se ha vuelto m�s fundamental que nunca.
Ahora, �por qu� es esto tan importante? Aproximadamente 133 millones de estadounidenses se ven afectados por enfermedades cr�nicas y ese n�mero es a�n mayor dependiendo de c�mo se define la enfermedad cr�nica. Aproximadamente uno de cada dos individuos en los Estados Unidos tiene pre-diabetes o diabetes tipo 2. La tasa de una variedad de enfermedades, incluyendo problemas digestivos, enfermedades al�rgicas, enfermedades del coraz�n, enfermedades autoinmunes, c�ncer, obesidad, diabetes tipo 2 y demencia, ha aumentado. Donde aproximadamente uno de cada tres ni�os nacidos hoy tendr�n diabetes tipo 2 durante su vida y una de cada dos personas mayores de 85 a�os y una de cada cuatro personas mayores de 75 a�os tendr� demencia.
Problemas de salud como estos se est�n manifestando en toda nuestra poblaci�n a un ritmo tremendo y pueden afectar a todos, ya sea personalmente o a trav�s del sufrimiento de un ser querido. Adem�s, las enfermedades cr�nicas han causado una carga econ�mica dram�tica en nuestro pa�s.
Sin embargo, la raz�n por la que estoy tan feliz de compartir este video con ustedes es porque hay mucho que podemos hacer para cambiar el futuro de nuestro sistema de atenci�n m�dica. Muchos m�dicos y yo tenemos el conocimiento que necesitamos para disminuir o incluso eliminar el sufrimiento de tantas personas y para salvar la econom�a. Todos los d�as en mi consultorio, veo que los pacientes recuperan su calidad de vida despu�s de que esperaban sufrir toda su vida debido a enfermedades cr�nicas como el reflujo �cido, el s�ndrome del intestino irritable, los dolores de cabeza, la fatiga y la artritis, entre otros problemas de salud. Problemas como alergias, problemas hormonales, obesidad, diabetes, enfermedades del coraz�n, enfermedades autoinmunes y depresi�n. Y los pacientes realmente pueden mejorar y prosperar, no solo enfrentar o controlar su enfermedad. En unos pocos meses, incluso semanas, de visitarnos a m� y a mi personal, las vidas de los pacientes pueden cambiar enormemente.
La medicina funcional analiza c�mo funciona el cuerpo humano por completo, y su enfoque m�s b�sico es comprender primero los factores, los genes y los desencadenantes de la enfermedad, y c�mo el estilo de vida y las aportaciones ambientales, incluyendo la dieta, el estr�s, las toxinas, los al�rgenos y los microbios , interact�an con el cuerpo humano para crear desequilibrios que com�nmente pueden conducir a problemas cr�nicos de salud.
Entonces, d�jenme tomar un momento para discutir algo. El cuerpo humano es un sistema. Y todo este sistema est� formado por “sistemas peque�os” que interact�an din�micamente. Pero, cuando uno o m�s de estos sistemas se desequilibran, puedes enfermarte. Y cuando estos sistemas se equilibran de nuevo, te vuelves sano. Y eso es lo que es la medicina funcional. La medicina funcional es simplemente comprender las causas de los desequilibrios en el cuerpo humano y el tratamiento para restablecer el equilibrio y proporcionar necesidades esenciales a todos los sistemas del cuerpo humano. Creando salud y bienestar en general es una ciencia. Y los m�dicos logran esto utilizando el historial m�dico detallado de un paciente, combinado con pruebas de laboratorio espec�ficas. Los m�dicos que siguen un enfoque de medicina funcional, como yo, a modo de ejemplo, generalmente eval�an su intestino y su microbioma, que no son muchos los m�dicos que analizan esto. Tambi�n queremos analizar su sistema inmunol�gico y si la inflamaci�n lo est� afectando, algo que llamamos defensa y reparaci�n. Y queremos saber c�mo sus mitocondrias producen energ�a con los alimentos y el ox�geno. Los profesionales de la medicina funcional desean saber si tiene alguna disfunci�n en la producci�n de energ�a, que suele ser la fuente de numerosas enfermedades, como la enfermedad de Alzheimer y el autismo, la diabetes tipo 2 y la fatiga, entre muchas otras. Tambi�n determinamos su carga t�xica y su capacidad de desintoxicaci�n, involucrando la funci�n de otros sistemas de comunicaci�n en su cuerpo, como sus hormonas. Finalmente, evaluamos su sistema estructural, desde sus c�lulas hasta sus estructuras biomec�nicas y c�mo �stas interact�an con sus creencias, emociones y m�s.
He usado estos procedimientos, una y otra vez, para ayudar a revertir las enfermedades cr�nicas en mis pacientes y educarlos sobre c�mo lograr la salud y el bienestar a largo plazo, al mismo tiempo que aprended como convertirse en las mejores versiones de s� mismos. Todos tenemos la oportunidad de curar o mejorar enormemente los problemas de salud o problemas que a menudo se diagnostican con la medicina convencional. La medicina funcional ofrece la oportunidad de descubrir el bienestar general a cualquier edad.
De hecho, trat� a un hombre llamado George, que ten�a 63 a�os, pesaba 300 libras y ten�a una variedad de problemas de salud. Ten�a reflujo �cido, problemas de sinusitis, diabetes, problemas card�acos, angina, problemas de pr�stata, disfunci�n sexual y edema en las piernas. Y como resultado, estaba bajo una amplia gama de medicamentos. Un d�a vino a mi oficina y me dijo: “�Me puede ayudar?”. Le dije: “S�, pero tendr� que hacer todo lo que yo le diga”.
Entonces, le recomend� una dieta anti-inflamatoria, que consist�a de alimentos integrales y una cantidad baja de az�car, y le aconsej� que tomara una variedad de suplementos para optimizar su nutrici�n, mientras lo guiaba a participar en ejercicios y actividades f�sicas. Dentro de un a�o, fue como un milagro, el paciente hab�a perdido 155 libras, revirti� todos sus problemas de salud y dej� de usar sus medicamentos. Ahora, �l est� planeando el resto de su vida, cuando antes de venir a visitarme, estaba planeando el final de su vida. Otra paciente que trat�, llamada Isabel, luch� contra una enfermedad autoinmune. Ten�a solo 10 a�os y ya estaba bajo un mont�n de drogas, esteroides, inmunosupresores e incluso quimio. Resulta que su dieta y la exposici�n a metales pesados ??estaban afectando sus intestinos y causando inflamaci�n. Ahora, simplemente trat� la fuente de sus problemas y su enfermedad autoinmune desapareci�. Dej� de usar sus medicamentos recetados y, en conjunto, su calidad de vida mejor� y prosper�.
La medicina funcional es un enfoque de tratamiento alternativo que se centra en las interacciones entre factores externos o ambientales, as� como factores internos asociados con los sistemas gastrointestinal, endocrino e inmunol�gico del cuerpo humano. Encontrar el m�dico adecuado puede hacer una gran diferencia cuando se trata de obtener atenci�n m�dica en vez de atenci�n por enfermedad. La medicina funcional trata la fuente del problema en lugar de tratar solo los s�ntomas. Como quiropr�ctico y practicante de medicina funcional, mi objetivo principal es brindar a los pacientes la atenci�n que merecen por sus problemas de salud, as� como educarlos sobre los fundamentos de la medicina funcional. El prop�sito de este art�culo es ayudar a los pacientes a encontrar al m�dico adecuado y establecer una relaci�n sana entre m�dico y paciente. Dr. Alex Jimenez D.C., C.C.S.T.
Informacion General Sobre el el Cuidado de Enfermos y el Cuidado de Salud
Durante las pr�ximas semanas, repasaremos algunos de los principios y conceptos fundamentales que me ayudaron a encontrar la causa subyacente de la enfermedad a trav�s del uso de la medicina funcional. Y eso los ayudar� a alcanzar la salud y el bienestar general.
En nuestro pr�ximo video, le ense�ar� c�mo puede tomar sus propias medidas para comprender su propio bienestar y qu� puede hacer para mejorar sus signos vitales. Este procedimiento ayudar� a proporcionarle datos e informaci�n de referencia importantes para ayudarlo a comprender mejor sus riesgos de salud. Tambi�n le permitir� evaluar y analizar su propio progreso a medida que trabaja para alcanzar sus objetivos de bienestar finales.
En el tercer video, voy a tratar de cubrir todo sobre nutrici�n. Le explicar� c�mo podemos evaluar su estado nutricional y c�mo puede utilizar los alimentos como tratamiento para comenzar a cambiar su salud y bienestar general lo mas antes posible. Su dieta es una de las partes m�s eficientes que puede controlar para crear un estilo de vida m�s saludable. Estar� compartiendo consejos y trucos para una mejor nutrici�n.
Debido a que las hormonas pueden afectar casi todos los aspectos de nuestra salud, tambi�n los vamos a destacar en el cuarto video. Desafortunadamente, la mayor�a de los m�dicos no entienden los niveles �ptimos de hormonas ni son conscientes de los m�todos adecuados para evaluar las hormonas. Lo preparar� para tener una conversaci�n efectiva con su m�dico sobre qu� tipo de prueba hormonal realmente importa, qu� significan y qu� puede hacer al respecto.
En el video cinco, me centrar� en la salud del coraz�n, discutiendo la presi�n arterial alta, colesterol alto y enfermedades cardiovasculares. Estas condiciones son extremadamente comunes, y desafortunadamente, la medicina convencional frecuentemente trata de tratarlas simplemente controlando los s�ntomas. Reducir el colesterol, disminuir la presi�n arterial, eso no resuelve la ra�z de los problemas. La mayor�a de las veces, el aumento de los niveles de az�car en la sangre, la obesidad y la diabetes son la causa de las enfermedades cardiovasculares. Voy a demostrar c�mo podemos prevenir y revertir estas enfermedades utilizando modificaciones en su estilo de vida, incluyendo la nutrici�n, para mejorar la salud del coraz�n.
En el sexto video, hablar� sobre la obesidad y la diabetes, trastornos metab�licos que van desde la grasa m�nima y la resistencia moderada a la insulina hasta la prediabetes y la diabetes tipo 2. Lo bueno de estos trastornos metab�licos, sin embargo, es que son completamente reversibles. Pero la mayor�a de los m�dicos convencionales no saben que es reversible. Voy a ense�arles c�mo pueden recuperar un metabolismo saludable y c�mo revertir la gama de problemas relacionados con la diabetes, que, como aprender�, son muchas enfermedades diferentes.
En el video siete, hablar� sobre el sistema inmunol�gico, en particular sobre la inflamaci�n oculta y la enfermedad. Como se describe que la inflamaci�n es la causa subyacente de la mayor�a de las enfermedades cr�nicas, continuamos observando tasas crecientes de enfermedades autoinmunes y alergias, que son se�ales de que nuestro sistema inmunol�gico no funciona correctamente. Sin embargo, la inflamaci�n tambi�n est� asociada con la obesidad, la diabetes tipo 2, las enfermedades del coraz�n, el c�ncer, la demencia e incluso la depresi�n. Le explicar� c�mo puede hablar con su m�dico sobre las pruebas de inflamaci�n, qu� significan los marcadores y c�mo puede cuidar su sistema inmunol�gico a un nivel m�s profundo.
En el video ocho, vamos a pasar al tema del metabolismo y las mitocondrias. Ahora, cada una de nuestras c�lulas contiene cientos o miles de mitocondrias, los generadores de energ�a de nuestras c�lulas. Cuando estos se da�an, podemos sufrir una variedad de problemas, como dolor, p�rdida de memoria, fatiga y muchos otros s�ntomas. Voy a explicar c�mo podemos cuidar sus mitocondrias a nivel celular y por qu� esta es una pieza vital de salud y bienestar �ptimos.
Luego, en el video nueve, vamos a explorar el significado de la desintoxicaci�n o el sistema de desintoxicaci�n del cuerpo humano y por qu� esto es una parte esencial del proceso de curaci�n. Desde el moho hasta los metales pesados ??y otras toxinas, explicar� lo que debe saber para evitar las toxinas y c�mo puede eliminar las que ya tiene para optimizar su capacidad de desintoxicaci�n. Con la cantidad de toxinas a las que estamos expuestos de manera regular, es importante identificar las causas que pueden estar afect�ndote y c�mo puedes comenzar a eliminarlas de inmediato. Afortunadamente, esto es algo que puede hacer f�cilmente para crear un estilo de vida m�s limpio para usted y sus seres queridos.
Finalmente, en el video diez estaremos hablando sobre la digesti�n. La salud digestiva es uno de los temas m�s discutidos en la medicina funcional. Debido a que nuestro sistema digestivo es el centro de nuestra salud, al diagnosticar problemas en este sistema, podemos mejorar todo, desde la salud mental, la absorci�n de nutrientes y el riesgo cardiovascular hasta la funci�n del sistema inmunol�gico. En el d�cimo video, los guiar� a trav�s de las pruebas disponibles para controlar su salud intestinal, as� como lo que puede hacer para mejorar su propia salud digestiva, lo antes posible.
Estoy muy contento de que me acompa�en en esta serie de videos porque el futuro de la medicina depende de ello. Cuando se aprende c�mo puede impactar su bienestar al ser proactivo y al asociarse con su m�dico, todo cambia. A trav�s de la medicina funcional, tambi�n puede ayudar a transformar nuestro sistema de atenci�n m�dica en un sistema de atenci�n m�dica real.
Entonces, terminemos este video con las preguntas que desea hacerle a su m�dico cuando los entreviste para ver si pueden ser un socio para usted y su salud y bienestar en general. Estas son solo algunas preguntas de alto nivel para comenzar con su discusi�n. �Est� dispuesto a trabajar conmigo como socio para mi bienestar?, �Cu�l es su punto de vista sobre nutrici�n y salud? �Cree que la comida es medicina? �Est� dispuesto a darme copias de los resultados de mis pruebas y explicarme qu� significan? La raz�n por la que nos hacemos estas preguntas es para asegurarnos de que su m�dico est� dispuesto a trabajar con usted y comprender el papel de la medicina funcional.
�
Estoy muy feliz de ser parte de su camino hacia una mejor salud y bienestar. Muchas gracias por acompa�arme el dia de hoy. El alcance de nuestra informaci�n se limita a problemas quiropr�cticos y de salud de la columna, as� como a temas y discusiones de medicina funcional. Para seguir discutiendo el tema, no dude en preguntarle al Dr. Alex Jimenez o comun�quese con nosotros al�915-850-0900�.
Curado por el Dr. Alex Jim�nez
Discusi�n del Tema Adicional: Dolor de Espalda Agudo
El dolor de espalda es una de las causas m�s frecuentes de discapacidad y d�as perdidos en el trabajo en todo el mundo. El dolor de espalda se atribuye a la segunda raz�n m�s com�n para las visitas al consultorio del m�dico, superada �nicamente por infecciones respiratorias superiores. Aproximadamente el 80 por ciento de la poblaci�n experimentar� dolor de espalda al menos una vez a lo largo de su vida. La columna vertebral es una estructura compleja formada por huesos, articulaciones, ligamentos y m�sculos, entre otros tejidos blandos. Las lesiones y / o afecciones agravadas, como las hernias de disco, pueden provocar s�ntomas de dolor de espalda. Las lesiones deportivas o las lesiones por accidentes automovil�sticos suelen ser la causa m�s frecuente de dolor de espalda; sin embargo, a veces los movimientos m�s simples pueden tener resultados dolorosos. Afortunadamente, las opciones de tratamiento alternativo, como la atenci�n quiropr�ctica, pueden ayudar a aliviar el dolor de espalda mediante el uso de ajustes de la columna vertebral y manipulaciones manuales, lo que finalmente mejora el alivio del dolor. �
De XYMOGEN�Las f�rmulas profesionales exclusivas est�n disponibles a trav�s de profesionales de atenci�n m�dica con licencia seleccionados. La venta por internet y el descuento de f�rmulas XYMOGEN est�n estrictamente prohibidos.
Con orgullo�El Dr. Alexander Jimenez�hace que las f�rmulas de XYMOGEN est�n disponibles solo para los pacientes bajo nuestro cuidado.
Llame a nuestro consultorio para que podamos asignar una consulta m�dica para acceso inmediato.
Si eres paciente de�Injury Medical & Chiropractic�Clinic, puedes preguntar por XYMOGEN llamando�915-850-0900.
Para su conveniencia y revisi�n de la�XYMOGEN�productos por favor revise el siguiente enlace. *XYMOGEN-Descargar-Catalogo
* Todas las pol�ticas de XYMOGEN anteriores se mantienen estrictamente.
Truide Torres desarroll� dolor de espalda durante su embarazo. Y, como resultado de su empeoramiento del dolor y la incomodidad, no pudo continuar participando y participando en sus actividades f�sicas regulares. Truide Torres analiza c�mo encontr� alivio para el dolor de espalda con el Dr. Alex Jimenez, a pesar de sus dudas iniciales sobre la atenci�n quiropr�ctica durante su embarazo. El Dr. Alex Jimenez y su personal ayudaron a Truide Torres a sentirse c�moda y segura al educarla sobre los beneficios de la atenci�n quiropr�ctica durante el embarazo. Truide Torres recomienda al Dr. Alex Jimenez como la opci�n no quir�rgica para el dolor de espalda y el tratamiento durante el embarazo, entre otros problemas de salud. La atenci�n quiropr�ctica es una opci�n de tratamiento alternativa segura y eficaz que corrige los desajustes o subluxaciones de la columna, mediante ajustes de la columna y manipulaciones manuales. Los quiropr�cticos est�n capacitados para trabajar con mujeres embarazadas y no se conocen contraindicaciones para recibir atenci�n quiropr�ctica durante el embarazo.
Quiropr�ctica para el embarazo
�
Tenemos la suerte de presentarle a la Cl�nica Premier de Atenci�n de Lesiones y Bienestar de El Paso.
Como Cl�nica de Rehabilitaci�n Quiropr�ctica y Centro de Medicina Integrada de El Paso, nos enfocamos apasionadamente en el tratamiento de pacientes despu�s de lesiones frustrantes y s�ndromes de dolor cr�nico. Nos enfocamos en mejorar su capacidad a trav�s de programas de flexibilidad, movilidad y agilidad dise�ados para todas las edades y discapacidades.
Queremos que viva una vida llena de m�s energ�a, actitud positiva, mejor sue�o, menos dolor, peso corporal adecuado y educaci�n sobre c�mo mantener esta forma de vida.
Te aseguro que solo aceptar� lo mejor para ti …
Si ha disfrutado de este video y le hemos ayudado de alguna manera, no dude en suscribirse y recomendarnos.
Teachers do a lot in a day. They stand for long periods of time, they stoop and bend, pick up children, carry stacks of papers, and sit for long periods while they grade papers. It�s no wonder that so many teachers end up with aching backs! While low back pain is the number one cause of disability worldwide, it�s easy to see how teachers may be more susceptible to experiencing it.
Chiropractic care can help keep teachers standing upright and moving about � as well as other great benefits. A teacher with back pain can�t be as effective as they would be if they weren�t in pain. It makes it harder for them to do their job. Regular chiropractic care can help offset what their body goes through in a day and relieves the pain so they can do what they love � shape young minds.
What Teachers Do
Teaching is a tough profession. The typical teacher arrives at school before it starts (usually between 6:30 am, and 7:30 am) and they don�t leave until well after the last bell has rung (often between 3:30 pm and 5:30 pm). They grade exams during their vacations and spend hours preparing lessons, quizzes, activities, and tests. In middle and high school, they teach five or six classes a day which means a lot of talking and a lot of standing. Combine the stress with the physical demands of the job, and it�s no wonder aching feet and backs are the bane of a teacher�s existence.
The Impact of Teaching on the Body
There have been several studies that explore the effects of the physical demands that are put upon a teacher. One study analyzed the incidence of musculoskeletal disorders in special education teachers and teachers� aides. It found that the three areas most affected were the wrist, shoulder, and back. It found that 86% of the teachers who participated had physical pain and musculoskeletal condition. Another study examined teachers in a municipal school network in Brazil. It found that:
41.1% complained of foot, leg, and knee pain (lower limbs)
23.7% complained of shoulder, neck, and wrist pain (upper limbs)
41.1% complained of back pain
A third study that assessed teachers in Malaysia reported that 62.5% of the teachers surveyed complained of low back pain.
How Chiropractic Care Helps Teachers with Low Back Pain
Several studies show that chiropractic care is a very effective treatment for back pain. The chiropractor will perform a spinal manipulation to bring the spine (and body) into proper alignment. He may also offer advice on exercises, stretching, and ways to improve posture as well as recommending lifestyle changes and what to look for in supportive shoes. Chiropractic�s whole-body approach not only helps relieve back pain, it helps prevent it as well.
Additional Benefits Teachers can Gain from Chiropractic
While less back pain is great news for teachers, there are other benefits they can reap form chiropractic as well. That�s because it doesn�t focus solely on the back or pain, it looks at the whole body. Every day teachers put a lot of stress on their bodies, bending over to help a child with their work, standing to give a lecture, sitting for hours grading papers, and reaching to write on the blackboard. All of this can take a toll on the body, not just physically, but in other ways as well. It can result in headaches, insomnia, and even frequent illness. A chiropractor can address all those things and make recommendations regarding lifestyle and diet as well as spinal manipulation.
This allows the patient to gain whole body benefits from chiropractic.
When you spend a lot of time behind the wheel, whether you are going on a long trip or your job requires you to drive around town all day, it can be a real pain � in the back. Many car seats may be comfortable for short rides, but they are not built to support the back on the long hauls. However, there are some things that you can do to offset a non-back friendly seat design and alleviate, or even prevent, back pain while driving.
Create a Comfortable Space
Before you settle in behind the wheel, you want to make sure that you are comfortable. Keeping things like your wallet and cellphone in your pocket may be convenient when you are moving about, but can be an irritant when you are sitting on them mile after mile. Wear comfortable clothing and shoes. Any discomfort can put stress on your body so even if it is not necessarily pain related, it can exacerbate pain as your body�s sensitivity heightens in response to the pressure.
Adjust your seat so that you are comfortable, but sitting reasonably upright. If you recline, it could put stress on your neck and upper back, causing pain. Your seat should also be high enough so that you can place your feet flat on the floor � at least for a while (you can do this while driving if you have cruise control). There should be a slight bend in your elbows as you reach for the steering wheel and you should not have to stretch to reach the pedals. Make sure that your mirrors are adjusted so that you don�t have to bend or crane your neck to get good visibility.
Put Together a Healthy Back Kit
Bring along some things to help keep your back comfortable and pain-free � even if you�ve never experienced back pain while driving. There is always a first time. Some of the items you might want to bring along include:
A towel that you can roll up and place behind the small of your back
A lumbar support pillow
A cold or hot pack
Something for pain relief
A cushion for your car seat to absorb the vibration
Water (so you can stay hydrated)
Essential Oil like lavender or peppermint (put a few drops in a carrier oil and apply to the sore areas)
Take Breaks and Move a Little
Driving straight through without any breaks is never a good idea. It can make you more tired, stiff and sore � and less alert on the road. Instead, take breaks to get out of the car, walk around, and stretch. When you move, you stimulate your circulation which brings oxygen and vital nutrients to your muscles. You�ll feel better, be more alert, and will be less likely to experience back pain.
Stopping every hour or so will help considerably with alleviating back pain. It doesn�t have to be a big production, walk around for a few minutes, stretch your neck, shoulders, and back, then get back on the road. In between stops you can move your ankles up and down or rotate them to increase circulation to the lower leg. You should also adjust your position or your seat about every 20 minutes. Even these slight movements can help keep the blood flowing which will prevent your muscles from getting stiff and sore.
Regular chiropractic care, as well as a consistent exercise routine, can help prevent back pain in many situations, including while driving. Your chiropractor can also recommend some back strengthening exercises and stretches that will help make your spine even healthier.
Each chemical reaction which occurs in the human body requires enzymes and each one of these processes needs a coenzyme. But what are coenzymes? They are vitamins and minerals. Approximately 37 billion, billion chemical reactions occur in the human body every second.
That is why proper nutrition and a balanced diet rich in whole foods with vitamins and minerals is fundamental towards overall health and wellness. The majority of people in the United States are vitamin and/or mineral deficient. But, how do you know if you�re a part of the 90 percent of individuals with enough deficiencies to develop disease? We will discuss the tests you can utilize to find out if you�re vitamin and/or mineral deficient and what you can do about it.
What�is�Nutrition?
Hello, welcome to part three of �Taking Control of your Healthcare�. Today, we will discuss one of the fun topics of functional medicine: nutrition. Unfortunately, nutrition is one of the most essential conversations that many doctors aren�t willing to have with their patients. The average medical doctor learns about disease and malnutrition rather than learning how to use nutrition as treatment or even how to use nutritional therapies to achieve optimal health and wellness.
I personally believe that food can be utilized as a form of medicine. That it should be the foundation of medical practice, not an afterthought in medicine. There is no better treatment than proper nutrition. Approximately 90 percent of individuals in the United States aren�t getting the essential nutrients they require for healthy bodily functions. And more than that probably aren�t getting enough nutrients to prevent diseases associated with nutritional deficiencies. However, what is ultimately needed to achieve optimal well-being? More than 98 percent of Americans are deficient in omega-3, 80 percent in vitamin D, 50 percent in magnesium, and 10 percent in vitamin C. Nutrient deficiencies can also continue to cause health issues for years.
Acute diseases, such as rickets, scurvy, beriberi, or iron deficiency anemia, are often the most talked about health issues associated with nutrient deficiency, however, there�s also something known as long latency deficiency diseases. So, how much vitamin D do we need to not get rickets? Not a lot, only 30 units really. And how much do we need to not get osteoporosis? Perhaps about 3,000 to 4,000 units per day. Now, how much folate do we need to not get anemia? Also not very much. But, how much do we need to prevent heart disease, cancer, and dementia? You definitely need a lot more units per day.
Each chemical reaction which occurs in the human body requires enzymes and each one of these processes needs a coenzyme. But what are coenzymes? They are vitamins and minerals. Approximately 37 billion, billion chemical reactions occur in the human body every second.
That is why proper nutrition and a balanced diet rich in whole foods with vitamins and minerals is fundamental towards overall health and wellness. The majority of people in the United States are vitamin and/or mineral deficient. But, how do you know if you�re a part of the 90 percent of individuals with enough deficiencies to develop disease? There are only several nutrients which we are generally tested for. And for a majority of these, doctors aren�t aware of what the optimal values should be which can make correcting the nutrient deficiency so much difficult to do.
Taking Control of Your Nutrition
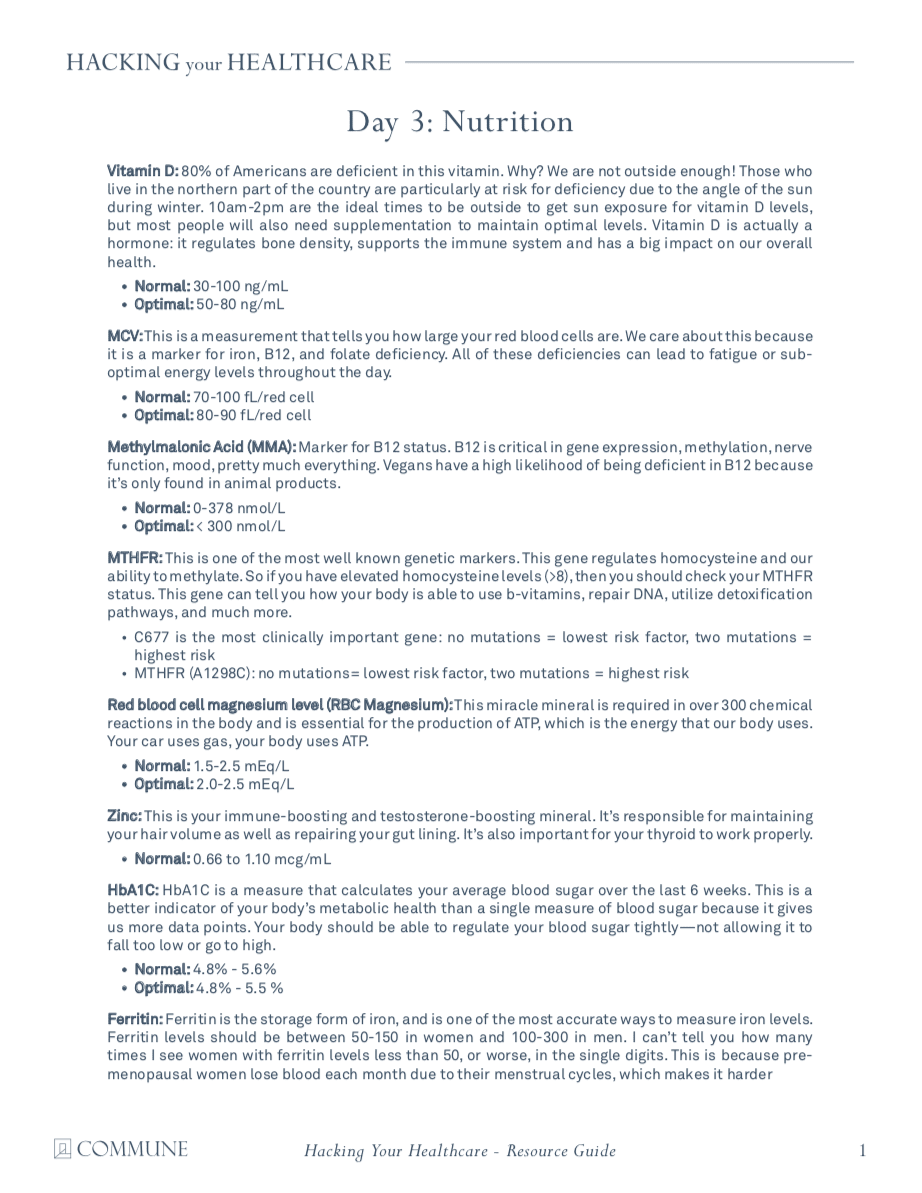
One of the most fundamental nutrients you need to measure is vitamin D. Although it�s referred to as a vitamin, it�s actually more like a hormone and it�s produced from cholesterol. This is yet another reason why cholesterol is essential. Approximately 80 percent of the population is deficient in vitamin D. Unless you�re in the sun 20 minutes every day between 10:00am and 2:00pm, you might need to take vitamin D supplements. In order to supplement properly, however, we need to know from what level you are starting at first. By way of instance, optimal vitamin D levels should be anywhere between 50 and 80 nanograms per milliliter of blood. The recommended amount of vitamin D we can supplement is about 2,000 to 4,000 units.
If you have lower vitamin D levels or if you have genetic problems, you may actually need to supplement with up to 10,000 units of vitamin D. That�s why it�s fundamental to work with a doctor or functional medicine practitioner who can measure and test your nutrient levels as well as help you optimize them. Most supplements contain about 400 units which is 10 times less than the amount most of us need. The optimal levels are generally just over 20. This is way too low. In one research study, women with vitamin D levels between 45 and 60 experienced reduced preterm labors by up to 60 percent. Vitamin D is also essential to help build strong bones and muscles, to improve immune system function, to prevent cancer, and ultimately, to help you live longer. It�s incredible.
Another measurement or test that�s performed by most doctors but is not always interpreted correctly is referred to as the MCV or mean corpuscular volume. The MCV measurement evaluates the size of your red blood cells in a test called CBC, or complete blood count, which is one of the most common blood panels ordered by healthcare professionals. So, if you are deficient in nutrients, your cells can either become smaller or larger. By way of instance, if your cells are too big, it could be a signs of a folate or vitamin B12 deficiency.
B vitamins are essential in numerous chemical reactions within the human body. They help us produce energy as well as help us regulate gene expression in order to create proteins that will ensure our overall health and wellness. If our B vitamins are too low, we could eventually develop an iron deficiency, anemia, or it could even cause a genetic disorder.
Optimal levels of B vitamins should be between 80 to 90. B complex vitamin supplements can help easily optimize levels of B vitamins. But, why would anyone be deficient in B vitamins? Is their diet not providing them with enough nutrients? Are they vegan? Are they taking any drugs and/or medications that prevent vitamin B12 absorption? Moreover, B vitamins are depleted during times of high stress which, as a practicing chiropractor, I can say it happens frequently to a majority of the population in the United States alone.
MCV is not the only measurement or test which evaluates a patient�s levels of B vitamins. Homocysteine is an alternative marker we will discuss in future articles which demonstrates B6, folate, and B12 levels. However, both the MCV and the homocysteine measurement or test only demonstrates that one or more of these nutrients may be deficient. It doesn�t necessarily tell us which one. Therefore, some additional, follow up evaluations may be required.
The MMA, or methylmalonic acid, measurement or test also shows vitamin B12 levels. Ultimately, vitamin B12 is essential for many processes in the human body, including energy production, gene expression, methylation, nerve function, and mood, among many other processes. Vegans have a higher chance of developing a B12 deficiency because it�s only found in animal products. Folate is another fundamental B vitamin. It can be determined directly in the blood, but, homocysteine is a more precise marker for folate levels.
In this section, we�re also going to discuss genetics because there is a measurement or test which can demonstrate a lot more regarding the status of your B vitamins and your ability to utilize them. Our genes are capable of making proteins. We have approximately 20,000 genes which are designed to create proteins. And one third of all the proteins they make are for our enzymes. Enzymes convert molecules into other molecules. These enzymes are also largely dependent on specific nutrients. One of the most fundamental genes which can be affected is known as MTHFR, or methylenetetrahydrofolate reductase. But you can just call it MTHFR.
MTHFR is essential because it helps regulate methylation, homocysteine, and folate, which are vital towards our overall health and wellness. When you have elevated levels of homocysteine, you should check your methylation status by looking for the MTHFR gene through a simple blood test.
Methylation is a key biochemical process which is fundamental towards the proper function of most of the human body�s systems. It triggers billions of times each second. And it ultimately helps control homocysteine, a substance which can damage blood vessels and has been associated with dementia, heart disease, and cancer, among other health issues. Methylation also helps repair your DNA on a regular basis as it helps recycle molecules necessary for detoxification, or getting rid of toxins. It also helps control your mood and it helps manage inflammation. Methylation is critical.
But, to make sure that methylation is active, the human body needs optimal levels of B vitamins. Without enough B vitamins, the methylation process can break down and the effects can be destructive. This is where we start seeing an increase in birth defects, such as spina bifida, down syndrome, and more miscarriages.
MTHFR is frequently abnormal in approximately 35 percent of the population. Methylation breakdown can also increase the risk of developing health issues like osteoporosis and diabetes, cervical dysplasia or cancer, including colon cancer and lung cancer, and even depression, pediatric cognitive dysfunction as well as mood and behavioral disorders, dementia, and stroke. Methylation is truly a key biochemical process.
When we discuss genetics, we have to understand that our environment can alter our genes. So, what if you have an MTHFR variation in your genes? First of all, not all mutations cause health issues. One mutation, by way of instance, known as C677T, is one version of the gene which is more significant than another version of the gene, known as A1298C. Now there�s no need to worry about these gene variations. They serve as examples to demonstrate you the quality of these mutations and how they function. People with these variations of the gene, by way of instance, might only need more folate or they might need a particular type of folate known as methylfolate. This is where a functional medicine practitioner can help their patients.
A genetic test can let you known if you have one of these gene variations. But, don�t get stressed. There�s a lot you can do to optimize your overall health and wellness. Many patients have visited my office after they find out they have these variations in their genes. And they quickly learn that they do have the option to take control of their well-being. However, what you do control is not your genes, you control your gene expression.
If you alter your healthy eating habits, you alter your nutrients. If you alter your environment, you alter which genes become active and which genes become inactive. And with these mutations, you can do just about the same thing by simply following the proper nutrition. When you find a doctor or functional medicine practitioner that�s willing to work with you, they�re going to tell you what lifestyle modifications you should follow to prevent health issues.
So, we�ve only just discussed the B vitamins. Next, we will discuss another fundamental nutrient in the human body: magnesium. Magnesium is a super essential mineral. Approximately 48 percent of people in the United States consume less than the required amount of magnesium from food. Magnesium is necessary in over 300 chemical reactions in the human body. It is also fundamental in the production of ATP, or the energy the human body utilizes as fuel.
A magnesium level blood measurement or test can help determine if you have a deficiency. Magnesium can also help reduce anxiety, calm the nervous system, and improve sleep. It is also an essential nutrient in the management of blood sugar levels. If you�ve been told by a healthcare professional that you have an average blood sugar level of over five and a half in something known as A1c, then magnesium can help.
Also, it�s very easy to know if you have a magnesium deficiency by looking at your current diet and symptoms. Do you eat enough magnesium rich foods like dark, leafy greens, beans, nuts and seeds? Or do you eat a lot of processed foods? Perhaps you also have symptoms such as anxiety, insomnia, constipation, muscle twitching, muscle cramps, PMS, and/or palpitations. If you have one or more of the symptoms I just mentioned, you may have a magnesium deficiency.
Next, we will talk about zinc, the immune-boosting and testosterone-boosting mineral in the human body. This important nutrient is in charge of maintaining your hair volume as well as repairing your gut lining. It�s also responsible for making sure your thyroid is functioning properly. Zinc can be easily measured or tested in the blood and unfortunately, it�s another nutrient we are highly deficient in, in the United States. Additionally, you can also look at your alkaline phosphatase levels, which can be calculated through a liver function evaluation on a regular blood panel. High levels of alkaline phosphatase may indicate the presence of cancer or bone problems, among other health issues, however, low levels of alkaline phosphatase may indicate a zinc deficiency, because it�s a zinc-dependent enzyme.
Finally, the last fundamental nutrient we are going to discuss is iron. Iron is frequently deficient in vegans and vegetarians, or in women in general due to menstruation. Iron is necessary for transporting oxygen throughout the human body and it�s ultimately essential for brain health and wellness. Iron is also important for hair and nails, sleep, and so many other things.
Ferritin is a stored type of iron and it�s this nutrient which helps you see your iron levels. Optimal ferritin levels should be between 50 to 150 in women and 100 to 300 in men. And many times I�ve seen women visit my office who have ferritin levels of less than 50, or worse, in the single digits. This is because pre-menopausal women lose blood every month due to their menstrual cycles and it becomes so much harder for them to maintain proper ferritin levels. Many women also eat way less than what they�re supposed to be eating every day. High levels of ferritin, on the other hand, could be a sign of inflammation, generally caused by insulin resistance to sugar, or it could be a sign of hemochromatosis or iron storage disease, a very dangerous genetic disorder.
Having decreased levels of ferritin can also make you feel tired, and it can cause hair loss, it can cause insomnia. So, even if your blood count is normal, if your ferritin levels are low or your iron levels are low, it can also cause these symptoms. That�s why if you experience symptoms of fatigue, it�s essential to measure or test your ferritin levels. And it can be easily supplemented.
Aside from ferritin, a low MCV can also determine if you have an iron deficiency. Iron deficiencies can cause red blood cells to become very small and that can be demonstrated in low MCV levels, which evaluate the size of your red blood cells. Additionally, transference saturation, serum iron, TIBC, or total iron binding capacity, and hemoglobin, can provide us with a more in depth look at your iron status to distinguish different causes of anemia. These are included on a regular iron blood panel in a lab test.
We�ve discussed several nutrients which can be ordered by a majority of healthcare professinals with access to conventional lab testing. Furthermore, there�s another test which can tell us more about which type of nutrients we need based on our genes. It�s called the DNA health test and it�s provided by a company called DNAlife. This test evaluates a variety of genetic markers associated with detoxification, lipid metabolism, and inflammation, including the MTHFR gene and other B vitamin markers. Now, DNA Health demonstrates the different genes we evaluate. And most of these are common genes, they�re those we can do something about. We analyze the genes we can change based on your nutrition and other lifestyle factors.
It shows us the MTHFR gene, other B vitamin markers, genes that control B6, folate, and B12 as well as demonstrating how they function and whether you have nutrient deficiencies. Then it tells us which nutrients you will need to supplement and how much we will need to give to you. It�s tremendously helpful.
There was an individual who had two variables of the MTHFR gene. This woman had miscarriage after miscarriage after miscarriage. She visited her doctor for an evaluation and it turns out that she had a folate-regulating mutation. So her doctor then started giving her the proper amount of folate she needed and she started having healthy babies. Sometimes, nutrition can be that powerful towards improving a patient�s overall health and wellness.
The DNA health test can help personalize your approach when optimizing your well-being based on your genetics. What we measure utilizing the DNA health test provide well-established insights about your genes as well as what you can do about them.
A micronutrient test known as the individualized optimized nutrition profile or the ION panel, are alternative test options which can also provide information about your current nutritional status. This test is by Genova. This is a robust test which measures all the essential vitamins and minerals, fatty acids, organic acids, and antioxidants you currently have. Ultimately, this test looks for imbalances, insufficiencies, or deficiencies, rather than looking for a specific disease. It looks for things that a majority of doctors never look at.
Functional medicine practitioners or doctors look at patient�s amino acid levels, mineral levels, and even toxin levels from heavy metals like mercury, lead, arsenic, and many more. We also look at your antioxidant levels, vitamin A and vitamin E levels, as well as your CoQ10 antioxidant and beta carotene status. We can determine if a person eats vegetables or not if, by way of instance, they have low levels of beta carotene. We also look at vitamin D levels, essential fatty acids, including your omega-3 fats and your omega-6 fats. We can tell if a person eats junk food. We can tell if a person is eating fish. And We can tell if a person is eating too much olive oil or saturated fats. It�s all demonstrated in these measurements and tests.
An OAT test, or organic acids test, also looks at what is known as organic acids. This test demonstrates a wide array of parameters associated with your mitochondria, which we will discuss in the next article, your B vitamins, your neurotransmitters, your gut flora, and your detoxification. It�s ultimately a comprehensive test which shows me if a patient is well or sick. It shows me where the imbalances are and where I need to recommend lifestyle modifications. It also helps provide clues about other health issues.
By way of instance, if your mitochondria aren�t functioning correctly because you have decreased levels of essential amino acids or you have increased oxidative stress or if you simply have low levels of selenium and zinc, there�s a possibility that you might have some form of toxic overload due to heavy metals. And that�s precisely what I would go looking for. Signs like these provide a lot of information about what we can do to treat a patient. And an experienced functional medicine practitioner or doctor can determine what�s really going on with a patient or they can help patients discover how to optimize their overall health and wellness.
Nutrition is the study of nutrients in food and how the human body utilizes nutrients as well as the relationship between diet, disease and overall health and wellness. Nutrients are a source of nourishment, including carbohydrates, proteins, fats, vitamins, minerals, fiber and water. Functional medicine focuses on the use of food as a form of medicine. A balanced nutrition can help prevent as well as treat a variety of health issues. Similarly, nutrition in functional medicine involves how certain diseases and conditions may be associated with dietary factors, such as poor diet or malnutrition, food allergies and food intolerances. Dr. Alex Jimenez D.C., C.C.S.T.
Understanding Your Nutrition
As good functional medicine doctors we�re often left asking ourselves, why is it that so many people in the United States are overfed but undernourished? Or, why is it that Americans eat too many calories and too few nutrients? The leading causes for the widespread nutritional deficiencies are the following: First, humans evolved from eating wild foods which contained tremendously higher levels of nutrients. Second, the soil we currently utilize to grow our crops in has become greatly depleted of nutrients. Hybridization techniques from industrial farming are yielding animals and vegetables to have decreased levels of nutrients. Third, processed foods have absolutely no nutrients, which is why they frequently have to be fortified. And last but not least, exposure to environmental toxins, lack of sunlight, chronic stress, and poor diet, including increased alcohol, caffeine, and sugar consumption, can increase our nutritional needs, much of which we�re already not getting enough from our current nutrition.
Well you might not need any vitamins, however, if you can meet certain conditions. Perhaps if you only hunted and gathered wild food and if you weren�t exposed to environmental toxins. Or maybe if you went to sleep with the sun and woke up with the sun, sleeping nine hours a night. And if you experienced absolutely no amount of chronic stress. Ultimately if you only drank pure, clean water and breathed pure, clean air. Then, you probably wouldn�t need any vitamins. But the rest of us that don�t follow these conditions, we do need them.
And with that thought, we wrap up this article. In the next article, we will talk about hormones. Hormones can affect almost every aspect of our well-being, and many healthcare professionals don�t understand what our optimal hormone levels should be or even when to test them and what to do about it once they do. Measuring and testing hormone levels should be standard practice, and many patients have never had a blood panel to look at their hormones. It�s fundamental to know as well as understand what�s going on inside your own body. And that�s why this next article is so important. You won�t want to miss our next update. See you soon.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Low back pain which gradually influenced his quality of life was developed. David Garcia was unable to walk as his symptoms worsened and his back pain became excruciating. He first visited Dr. Alex Jimenez, chiropractor in El Paso, TX, following a recommendation from his sister. Dr. Jimenez managed to supply David Garcia with all the aid he deserved for his low back pain, restoring his well-being. David Garcia clarifies the wonderful service Dr. Alex Jimenez and his team have given him to offer him relief from his painful symptoms and he highly recommends chiropractic care as the non-surgical pick for low back pain, among other health problems.
Chiropractic Non-Surgical Relief
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Assembly lines have long been the standard for factory workers. Henry Ford got the ball rolling on December 1, 1913, when he created the very first assembly line to mass produce a car. Workers stood for hours, doing the same tasks over and over. Although Ford took steps to reduce at least some of the damage, many factory workers still went home with aching backs and feet, migraines, fallen arches, and repetitive motion injuries.
Now, more than a hundred year later, some things have changed. According to the United States Department of Labor Bureau of Labor Statistics, there were 1,834,000 assembly line and fabrication jobs in 2014. Technology is better, and some tasks can be automated making some people�s jobs more manageable � and, unfortunately, eliminating some as well.
Despite the great strides in technology, there are still some things that haven�t changed all that much. The working conditions in many factories are often still not as healthy as they could be. Many workers are still required to stand for long periods of time and perform repetitive motions for hours without a break. This can lead to injuries, pain, and certain conditions that can cause immobility, inflexibility, and even disability. The good news is, chiropractic can help.
Working in a Standing Position Can Be Bad For Your Health
Many assembly line jobs require that the worker stand for long periods of time. While standing is a natural posture for humans and, by itself does not pose any real harm or health problem, working in a standing position every day isn�t good for you. It can lead to muscle fatigue, stiff shoulders and neck, swelling of the legs and feet, low back pain, varicose veins, fallen arches, and sore feet � to name a few.
Another problem with standing for extended or frequent periods of time without any breaks (such as walking or stretching) can cause the joints in the feet, knees, hips, and spine to become locked or immobilized temporarily. If the behavior continues, it can cause degenerative damage, leading to rheumatic diseases because the ligaments and tendons become damaged.
Other Assembly Line Related Health Problems
Barring traumatic injury due to an accident, working in a factory environment can cause problems with mobility, pain, and flexibility. The nature of the job places specific demands on the human body that can lead to certain types of injuries and health conditions, which include:
Repetitive motion injury � When a worker performs the same task that involves the same movements over and over, it can lead to certain types of injuries. Carpal tunnel is common repetitive motion injury.
Overexertion � Lifting, pulling, even standing can take a toll on the body, especially when it is done without adequate breaks. The person can get muscle fatigue, pulled muscles, and pulled tendons.
Body movement injuries � When the worker is continuously reaching, twisting, crawling, and bending, it can cause problems with the muscles and joints.
Chiropractic can Help Assembly Line Workers
Chiropractic care can help keep bodies flexible and help with range of motion. It is a very effective, non-invasive treatment for pain and can help with joint and muscular problems as well. Regular chiropractic treatments can help you better manage your body�s response to your work environment. It can also undo many of the ill effects that that type of work can cause.
You can enjoy more pain-free days without invasive surgeries or medications that leave you groggy, nauseous, or worse. When you sit down with your chiropractor, he or she will talk to you about your medical history as well as your current lifestyle. After a complete evaluation, you will be given a plan of action that may include lifestyle changes, dietary changes, and recommended supplements in addition to spinal manipulation. Chiropractic is all about whole body wellness, and that is what will help you perform better on your job and recover faster.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine