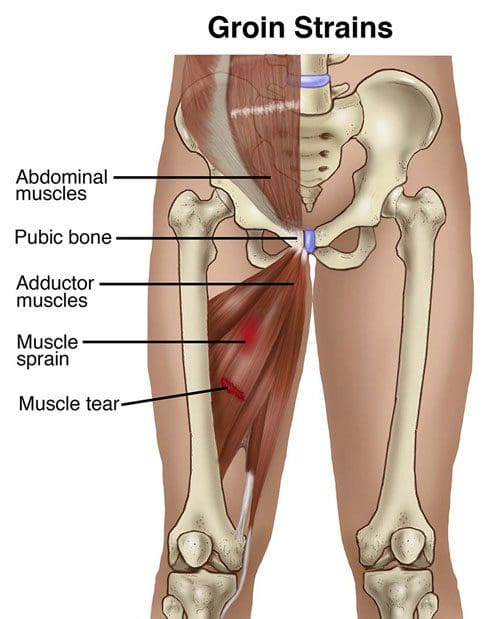
An adductor muscle strain is characterized as an acute injury to the muscles of the groin. Although a variety of muscles in the human body can be injured, the adductor longus, medius, magnus, and the gracilis are some of the most well-known muscle groups to be affected by an injury.� Strains are muscle tears which generally occur due to the powerful contraction of the muscles against resistance, often during what is referred to as an eccentric load. � �
An eccentric load describes some muscle contraction while the muscle is lengthening, versus concentric, where the muscle is shortening during some muscle contraction. Most weight-lifting exercises and physical activities involve concentric contraction. By way of instance, bench press involves eccentric contraction. Moreover, tears can occur at the origin of the muscle, at the muscle-tendon junction, or inside the belly of the muscle(s). Tears most frequently happen at the muscle-tendon junction. The least common tendon injury occurs at the region of its bony attachment. �
Adductor muscle strains may be graded I-III depending upon their seriousness. A grade I injury involves a moderate strain with some pain and discomfort, tenderness, and bleeding, but no fiber disruption. The adductor muscle’s overall integrity is maintained although a Grade II injury involves further damage. A grade III injury involves disruption resulting in a loss of tendon integrity. Most adductor muscle strains are considered to be grade I or II injuries. �
Causes and Symptoms of an Adductor Strain
As previously mentioned above, an adductor muscle strain occurs during acute muscle contraction, such as during kicking, pivoting or skating. Factors which can predispose a person to injury include failure to properly stretch or warm up and fatigue from overuse. The risk of experiencing an adductor strain increases with sports involving strides like sprinting, soccer, and hockey. Sports with repeated movements like football, martial arts, and gymnastics can also substantially increase the risk of experiencing an adductor strain. Struggling to warm up, stretch or be properly conditioned can also cause injury. �
The symptoms associated with an adductor muscle strain most commonly involve a variety of painful symptoms which are most frequently related to other types of muscle strain. Common symptoms of an adductor muscle strain include a sudden onset of pain and discomfort, occasionally accompanied by the feeling of a pop in the inner section of the thigh as well as the inability to maintain action after the first onset of painful symptoms. Because an adductor strain may cause groin or hip pain, many patients and healthcare professionals may confuse this type of injury with sciatica or sciatic nerve pain. �
Diagnosis and Treatment for an Adductor Strain
A healthcare professional can diagnose an adductor muscle strain through the patient’s medical history and a physical evaluation. Clinical findings include tenderness to palpation or touch, bruising through the inner thigh, as well as swelling and heat within the region of the injury. With acute tears, there might be a palpable defect over the area of the injury. Motion testing of the hip is normal, however, pain generally occurs while the patient is asked to contract the muscles. In these cases, asking the patient to bring their leg towards midline can ultimately cause pain and is generally accompanied by weakness. �
X-rays are often not utilized to diagnose an adductor muscle strain, however, they are appropriate in instances in which there are tenderness at the site of bony insertion or in young patients and/or athletes. In children, the attachment sites of a muscle and/or tendon are weaker and vulnerable to fracture. MRI can provide the precise location of an injury and the extent might help estimate return to play, or in rare cases, help identify any other cases which may require surgical interventions. �
Many adductor muscle strains respond positively to conservative treatment. The utilization of ice therapy and anti-inflammatory medicine are appropriate for acute muscle strains. As symptoms improve, stretching and exercises are generally not recommended. The healthcare professional may suggest a physical therapy program. Surgery may be required for adductor muscle tendon tears. Repair entails an open incision within the site of injury and reattachment of the tendon. Surgery is also essential in patients who have chronic pain whose symptoms don’t respond to conservative therapy. �
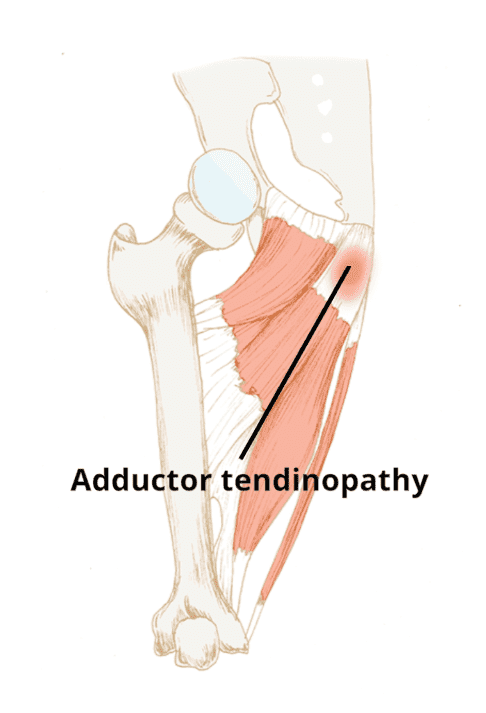
What is Adductor Tendinopathy?
Adductor tendinopathy is generally characterized as pain on palpation of the adductor tendons, adduction of the legs and/or of the injured leg. Pain can develop gradually or cause a sudden and severe, sharp pain. A swelling or a lump may also be experienced from the adductor muscle(s), stiffness at the groin area or an inability to contract or extend the adductors. In acute cases, exercises and physical activities will be restricted because the tendon can’t sustain repeated tensile loading. �
�
Causes and Symptoms of Adductor Tendinopathy
The adductors are triggered in many sports such as, running, soccer, horse riding, gymnastics, and swimming. The repetitive movements and the continuous change of direction in physical activities activate the adductor tendon, which makes athletes more prevalent to develop adductor tendinopathy and other groin injuries. Other causes of adductor tendinopathy can include over-stretching of the adductor tendons or a sudden increase in training, especially in the type of training. �
Adductor tendinopathy may occur due to considerable leg length discrepancy which affects gait pattern. Poor or abnormal movement patterns may also overly stress the adductor tendons. Muscular length gaps, strength imbalances or muscular weakness in the thoracic or the abdominals can also be powerful in developing adductor tendinopathy. Other causes include a failure to properly warm-up, inactivity, fatigue, obesity, age-related weaknesses, genetics or degeneration. �
Diagnosis and Treatment for Adductor Tendinopathy
A healthcare professional can safely and effectively develop an appropriate treatment plan following a thorough diagnosis or further investigations could be undertaken, including ultrasound, MRI or CT scans. Achieving pain relief through the utilization of NSAIDs may be ineffective due to the non-inflammatory nature of the injury. Steroid injections are also not necessarily recommended due to potential tendon rupture if these are injected directly into the tendon. �
Physical therapy is often recommended for the treatment of adductor tendinopathy, although there’s no golden standard for the proper rehabilitation of the adductor tendon. Recovery is extremely variable across individuals because the injury may be degenerative or even due to previously failed healing. Strengthening exercises and physical activities are also recommended to promote proper healing. Treatment should be customized to the patient to avoid recurrence. �
Other treatment for adductor tendinopathy generally consists of avoiding exercise or physical activity in the first 48 hours. The patient should then apply the RICE treatment three times per day for 10-20 minutes to help reduce swelling and inflammation from any sudden trauma. If the painful symptoms have decreased, blood flow stimulation therapy could be started to help promote the healing process. Active treatment is subsequently suggested to follow up with rehabilitation. �
Furthermore, the goal of rehabilitation is to restore the adductor muscle and tendon properties where strength training is beneficial to the adductor structure, muscle building, and biomechanics. Recent research studies have also demonstrated that an eccentric based exercise program is the most effective as well as heavy-slow eccentric and concentric exercises for enhancing both function and symptoms. For effective treatment identifying the stage of the tendinopathy is also essential. �
Differential Diagnosis of Hip Pain and Discomfort
�
Most commonly well-known as a groin strain, an adductor muscle strain is a type of injury which affects one of a group of muscles found at the top of the thigh. Meanwhile, adductor tendinopathy can affect the tendons of the adductor muscles. Both of these type of injuries can ultimately cause a variety of painful symptoms and they generally require time to heal properly. Because of the location of the injury, many patients and healthcare professionals may confuse groin injuries with sciatica without proper diagnosis. Proper diagnosis is essential to follow-up with proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Fibromyalgia Magazine
The purpose of the article was to discuss adductor muscle strain, tendinopathy, and sciatica. It has also been observed that patients with adductor injuries may confuse their symptoms for sciatica. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Degenerative disc disease is a condition where the degradation or wearing away of your spinal discs leads to pain and discomfort. Everyone�s discs wear down, but not every person experiences pain. That is the difference!
What are the Four Stages of DDD
Two of the main components of the spine are the vertebrae and the discs. The discs sit between vertebrae to provide cushion, support, and flexibility. Each disc is made up of a soft inner layer and a tough outer layer. Over time, or due to injury, the discs can lose their integrity, begin to thin and even tear in certain cases. Compromised discs increase the likelihood of pressure on nerves and friction between the vertebrae.
Like many diseases, degenerative disc disease has several possible stages. As the stages progress, the negative symptoms become more pronounced.
1st Stage
The first stage of degenerative disc disease may go unnoticed by the individual but can be identified by a chiropractor or other medical professional. The loss of the natural curvature of the spine can indicate the beginning of degenerative disc disease. Pain may not be apparent, but extra pressure is being placed on the spine which can lead to more rapid aging of the spine, nerves, joints, etc.
2nd Stage
The degradation of discs becomes more apparent in the second stage. They may look thinner, and it is common to see deformations in the bone, such as bone spurs. The curvature of the spine will become more unnatural and the spinal canal may become more narrow. Stage 2 is often where you will begin to notice some pain and discomfort.
3rd Stage
Stage 3 is marked by a more extreme change in the posture and curvature of the spine, along with more pain and loss of mobility. Nerve damage is common and scar tissue typically begins to form. Discs are even thinner than before, which can sometimes cause even more deformation of the bones.
4th Stage
The final stage of degenerative disc disease is the most severe and is typically considered irreversible. Discs are at their thinnest or gone altogether. The flexibility of the spine is extremely limited and pain is often considerable. Nerve damage can be severe and the bones of the spine may even begin to fuse together.
Doctor explaining various spine diseases by the example of plastic models
How Can Chiropractic Help DDD?
Chiropractic care is a preferred treatment option for degenerative disc disease for a variety of reasons. Because it is gentle and non-invasive, chiropractic is much less likely to create undesirable side effects�which are common with prescription medications and surgery. Obviously, the earlier the stage of degenerative disc disease, the more successful treatment can be. But chiropractic can be helpful even in the most extreme cases of degenerative disc disease.
Chiropractic treatments may include:
Chiro Adjustments
One of the most effective ways to treat degenerative disc disease is to ensure the spine is in proper alignment. Loss of alignment, which can happen due to injury or just day to day life, puts extra stress on the spine which can accelerate the degradation of discs. Adjustments bring back alignment.
Spine Decompression
Spinal decompression uses gentle but firm pressure to bring space back between the vertebrae. Space allows blood flow to return and healing to happen. Decompression is an important treatment to complement adjustments.
Now is the Time to Treat DDD
The best time to seek treatment for your back and neck pain is right now. Our chiropractic team can help you feel better and live a healthier life. Please contact us now to learn more!
Hamstring injuries are several of the most common types of injuries among athletes. These makeup for the most days or even weeks missed each year amongst AFL football players. The majority of partial or complete tears include either the hamstring muscle belly or the distal musculotendinous junction. However, a proximal hamstring injury is ultimately uncommon. In the total hamstring injury spectrum, it makes up for under 10 percent of hamstring injuries, among other health issues. �
Anatomy
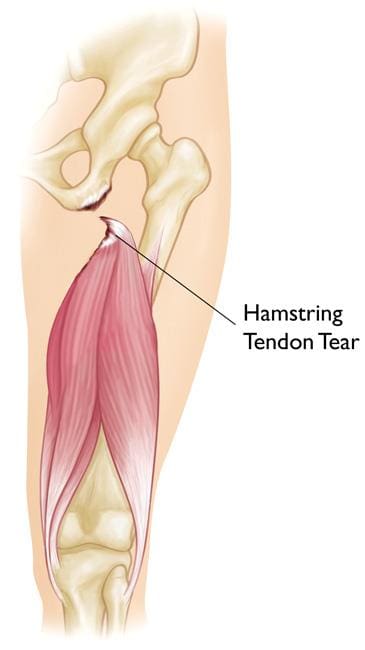
The hamstring makes up the majority of the muscle mass of the rear of the thigh. It is fundamental for shoving off, landing and leaping, especially for volatile activity, such as Pilates. The hamstring consists of 3 muscles, each utilizing a common proximal attachment through a big tendon to the ischial tuberosity of the pelvis or the big bone found in the buttocks. This proximal attachment gives a fixed point from which muscle contraction can impact a more distal activity. The hamstring gives some extension of the hip but the primary activity is movement around the knee.� It is largely responsible for knee flexion. �
The 3 muscles, the biceps femoris, the semitendinosus, and the semimembranosus, originate in the posterior thigh and attach distally around the knee through tendons to bony landmarks, crossing the joint. The biceps femoris then attaches laterally into the head of the fibula on the exterior of the knee. The semitendinosus and the semimembranosus attach to the medial side of the upper tibia. Because the sciatic nerve travels closely along with the attachment of the proximal hamstring tendon to the ischium, it may become injured along with the hamstring and ultimately cause the well-known symptoms of sciatica. �
�
Mechanism of Injury
The proximal hamstring tendon can become injured through progressive stretching or through sudden and intense contraction when the hip is forcefully flexed over an extended knee. In younger patients with an average proximal hamstring tendon, this can occur through sprinting or hurdling, however, the most common athletes affected in this instance involves waterskiiers who fall forward with an extended knee. In elderly patients, proximal hamstring injuries occur through a different type of trauma, such as slipping on a wet surface or even doing the “splits” inadvertently. �
Proximal hamstring injuries could include complete tendon ruptures or incomplete/partial tears. In young patients, the bone together with the tendon is frequently avulsed or fractured in the pelvis or the ischium. In older patients, the tendon usually avulses or tears from the bone of the ischium at its attachment point. Occasionally, the tendon may tear in its midsubstance, leaving a stump of tendon still attached to the bone. Frequently this type of injury is referred to as a partial tear. �
�
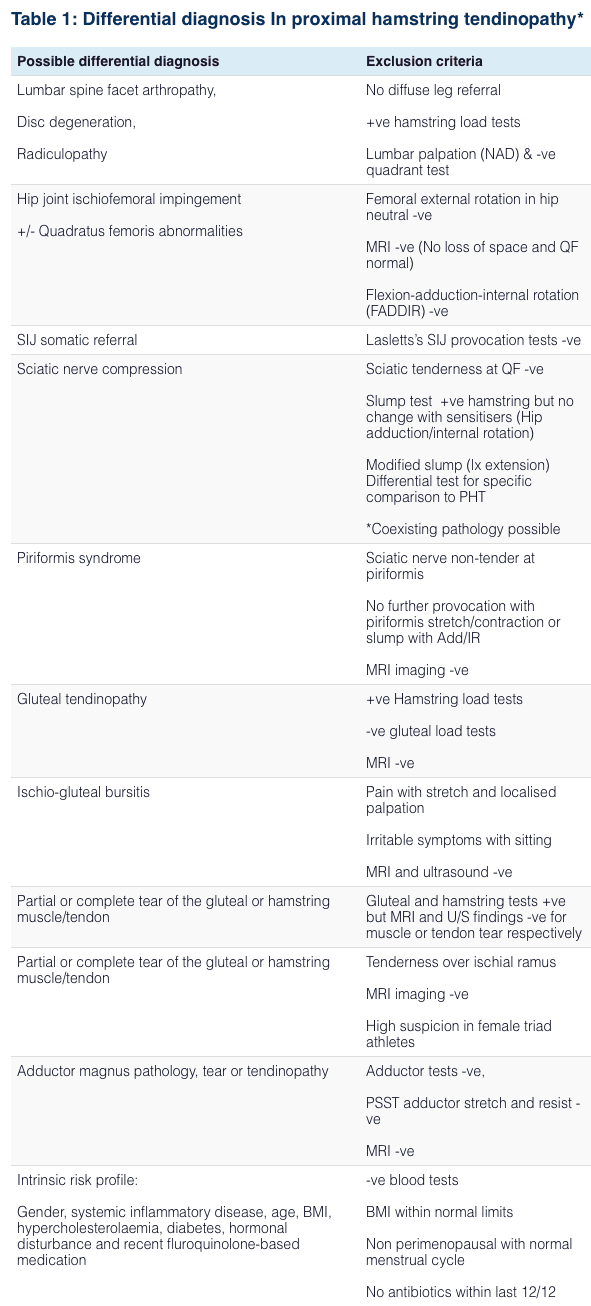
Diagnosis for Proximal Hamstring Injury
A proximal hamstring injury may commonly occur due to a sports-related injury and/or accident where the patient will experience something “go” deep in their buttocks. If the incident is being observed, the sufferer may often be seen holding their buttock or upper thigh. The person is generally not able to continue with the activity and when on the ground, they may need help to get up and to walk. There is normally immediate pain and weight bearing on the affected leg while it may also be painful to sit on the affected buttock. During the next 24 to 48 hours, there is swelling and bruising which appears over the buttocks region and extends down the rear of the thigh into the lower leg. Occasionally, the patient may also experience a “pins and needles” sensation in the lower leg and/or foot, similar to sciatica. Decreased movement in the foot may be seen with a foot fall. These injuries generally require immediate medical attention to diagnose the health issue. �
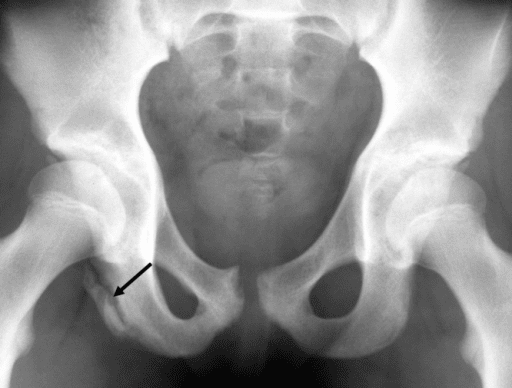
X-rays are fundamental in younger patients to rule out an avulsion fracture of the ischial tuberosity. Ultrasound may be undertaken and will help determine the presence of a hematoma, or blood collection, in the buttock and upper thigh which can also detect tendon tears. MRI scans are the best choice of diagnosis and it is highly accurate at determining the site of injury, whether the tear is partial or complete and whether there has been any retraction of the tendon end to the thigh. �
� �
�
Treatment for Proximal Hamstring Injury
Initial treatment for proximal hamstring injury must be symptomatic, where measures will be taken to help decrease pain and swelling with icing, analgesia, and the utilization of crutches to help walking. As the pain begins to settle, a few gentle movements of the leg may be undertaken along with the aid of a healthcare professional. When the diagnosis of a proximal hamstring injury is made, it’s fundamental to follow-up with the proper treatment choices. �
Conservative treatment using a rehabilitation program may be appropriate in sedentary older patients or in those with partial tendon tears at which a significant percentage of this tendon is still intact. Conservative treatment is usually also undertaken in most instances of bone avulsion fracture where the bone fragment is sitting near the ischium. Surgery is generally recommended for younger, athletic patients or for elderly victims where there is a complete tendon tear. �
Surgery generally involves an overnight stay in the hospital and the process itself is performed under general anesthesia. An incision is made in the buttock/upper thigh where the torn tendon end is identified, mobilized if it’s retracted down to the thigh and repaired back down onto the bone utilizing bone anchors or transosseous sutures. The sciatic nerve is also protected during the surgery. After surgery, painkillers may be required. Healthcare professionals may recommend patients to rest lying on their back with a pillow under the knees to allow the hamstring to be in a relaxed position. �
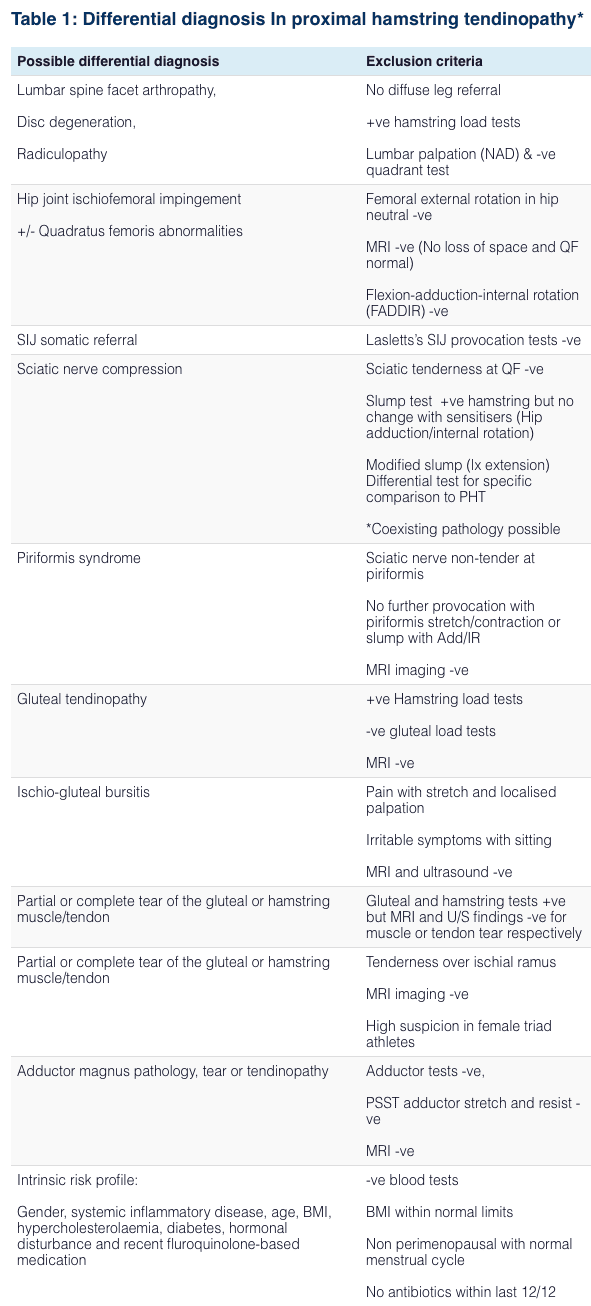
Differential Diagnosis of Hip Pain and Discomfort
� �
Tendon injuries are common health issues which frequently affect the athletic population. While Achilles tendon and patella tendon injuries are some of the most well-known types of tendon injuries, proximal hamstring injuries can still affect many athletes. Proximal hamstring injuries are health issues which can cause a variety or problems for people if they’re not properly diagnosed and treated. Understanding the differences between proximal hamstring injuries and it’s symptoms, including sciatica, can help both the patient and the doctor achive recovery. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
The purpose of the article was to discuss proximal hamstring injuries and sciatica. It has also been observed that patients with proximal hamstring injuries may confuse their symptoms for sciatica. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited. � Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care. � Please call our office in order for us to assign a doctor consultation for immediate access. � If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
� * All of the above XYMOGEN policies remain strictly in force. �
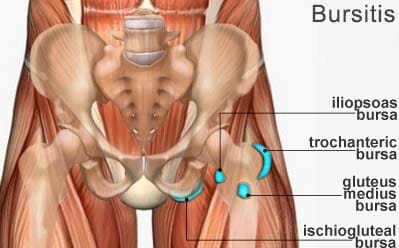
A bursa is a fluid-filled sac which functions by helping to decrease friction around the joints. However, when the fluid inside a bursa becomes infected or irritated due to excessive movement, the bursa can become swollen, causing pain and discomfort, ultimately making it difficult to move the affected joint. This health issue is commonly known as bursitis. �
Although bursitis generally occurs in the knee, called �housemaid�s knee�, or in the elbow, called �tennis elbow�, it can occur in any joint in the human body. When it occurs in the buttocks, it is known as ischiogluteal bursitis. In this instance, the bursa is found between the ischial tuberosity at the base of the pelvis and the tendon of the hamstring muscle. �
�
Symptoms of Ischiogluteal Bursitis
The symptoms of ischiogluteal bursitis can be similar to those of hamstring tendonitis. Several of the most common symptoms associated with ischiogluteal bursitis include pain and discomfort as well as tenderness in the buttocks region. Painful symptoms may frequently occur when stretching the hamstring muscle or flexing the knee against resistance. �
The symptoms of ischiogluteal bursitis can also be similar to those of sciatic nerve pain. Sciatica is a collection of symptoms characterized by pain, discomfort, tingling sensations, and numbness. While the symptoms of ischiogluteal bursitis may be similar to those of sciatica, sciatic nerve pain occurs when the sciatic nerve is irritated, compressed or impinged. �
Ischiogluteal bursitis associated with a sports-related injury and/or aggravated underlying condition, such as fibromyalgia, the pain and discomfort may slowly increase after exercise or physical activity. The symptoms may also worsen when sitting for extended periods of time. Ischiogluteal bursitis caused by an infection can ultimately be followed by a fever. �
Causes of Ischiogluteal Bursitis
The three most common causes of bursitis are generally due to injury or trauma, infection, and crystal deposits. Trauma can include repetitive movements or a blow to the region. By way of instance, the injury could occur due to a fall. Occasionally, trauma or injury can cause blood to leak into the bursa, causing ischiogluteal bursitis, or any other type of bursitis. �
Infection septic bursitis, or an infection in the bursa, generally occurs in the joints which are located closer to the surface of the human body. This health issue frequently affects men, however, it does not seem to be a leading cause of ischiogluteal bursitis. Crystal deposits can also form around the joints when there is too much uric acid in the human body. People with gout can develop bursitis because it is also caused by crystal deposits and it shares many similar symptoms with bursitis.
Diagnosis of Ischiogluteal Bursitis
Bursitis can generally be easily diagnosed by a healthcare professional, however, due to the similar symptoms of ischiogluteal bursitis, hamstring tendonitis, and even sciatica, it may be difficult to diagnose. However, tendonitis can often be relieved by deep tissue massage while bursitis will not and may actually worsen after a deep tissue massage. Proper diagnosis is fundamental in order for healthcare professionals to follow-up with the correct treatment for ischiogluteal bursitis. �
Treatment of Ischiogluteal Bursitis
In most instances, bursitis can be treated by resting the affected region and treating the swelling by utilizing cold therapy. When using an ice pack or similar cold pack, it should be wrapped in a cloth to avoid skin damage. The healthcare professional may also recommend a non-steroidal anti-inflammatory medication to reduce painful symptoms and swelling. �
As for people that have bursitis caused by an infection, an antibiotic is often prescribed to ultimately help fight the infection, relieving pain and discomfort in several days. If the painful symptoms continue for over a week, the doctor may suggest additional treatment approaches, such as draining of the bursa followed by a corticosteroid injection to reduce inflammation. �
Differential Diagnosis of Hip Pain and Discomfort
� �
Ischiogluteal bursitis is a well-known health issue characterized by pain and discomfort in the buttocks which is commonly caused by sitting for extended periods of time. In a variety of instances, ischiogluteal bursitis may also be caused due to an injury or aggravated underlying condition, such as fibromyalgia. Because ischiogluteal bursitis may occur due to inflammation, the widespread painful symptoms of fibromyalgia may also trigger other health issues. Furthermore, ischiogluteal bursitis may share similar symptoms to sciatica, due to the location of the health issue. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
The purpose of the article was to compare ischiogluteal bursitis and sciatica. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Gluteus Tendinopathy and Sciatica Symptoms in Fibromyalgia
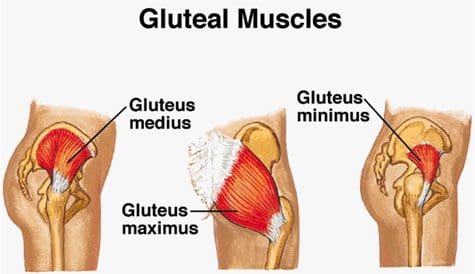
Gluteus medius tendinopathy (GMT), also known as dead butt syndrome (DBS), is a painful health issue caused by the inflammation of the tendons in the gluteus medius muscle. The gluteus medius (GM) is one of the smallest, less-known muscles of the buttocks which ultimately functions by providing stability and support to the structures of the hip and pelvis, especially throughout weight-bearing physical activities. Although GMT most commonly affects athletes, it can also affect people starting a new exercise program, during an intense workout routine or due to an underlying health issue. �
Healthcare professionals have reported an increased number of GMT cases over the past several years. While many doctors and functional medicine practitioners believe that this may perhaps be due to how many people participate and engage in exercise or physical activities after sitting down for extended periods of time, many GMT cases may actually be due to a well-known health issue called fibromyalgia. In the following article, we will discuss gluteus medius tendinopathy (GMT), or dead butt syndrome (DBS), fibromyalgia and how these two conditions can also be associated with sciatica symptoms. �
�
Sciatica and Gluteus Medius Tendinopathy Causes in Fibromyalgia
The common symptoms associated with gluteus medius tendinopathy, or GMT, include pain and discomfort, stiffness, and weakness in the hip or buttocks region. The painful symptoms can generally worsen throughout weight-bearing exercises, such as walking, running, and/or climbing. For many people, the pain and discomfort associated with dead butt syndrome, or DBS, can radiate down the hips, buttocks, and legs or thighs, similar to sciatica and hamstring tendinopathy. Sciatica is a collection of symptoms characterized by pain and discomfort, tingling sensations, and numbness along the sciatic nerve. �
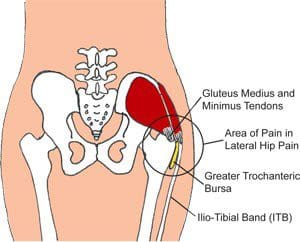
Many patients diagnosed with GMT also report experiencing painful symptoms when lying in bed on the affected hip or buttocks region as well as pain, discomfort, stiffness, and weakness throughout the night and upon rising in the morning. Moreover, if DBS progresses past the initial stage, the hip bursa may become inflamed, another health issue known as trochanteric bursitis, which may also cause swelling, tenderness, redness or warmth in the hip. In people with fibromyalgia, the widespread pain and discomfort caused by the inflammation of the condition may also ultimately cause GMT symptoms. �
The role of the gluteus medius muscle is to contract the weight-bearing hip throughout walking and running. When this small, lesser-known muscle triggers, the hip flexors release and vice versa. However, when the tendon becomes inflamed due to an injury or an aggravated underlying condition, such as fibromyalgia, the gluteus medius can fail to trigger appropriately, hence why the “dead butt” term is utilized as an alternate name for this health issue. People sitting down for extended periods of time may cause their hip flexors to become tight and failure to stretch before physical activities can cause DBS. �
Furthermore, poor gluteal or buttocks and hip muscle control cause excess stress on the gluteal medius tendon and/or muscle. Several athletes, especially runners, generally avoid utilizing cross-training and weight-lifting in order to help strengthen the larger muscles which support the pelvis when running, however, the hip’s and buttock’s smaller tendons and muscles may take on the excess pressure. If left untreated, gluteus medius tendinopathy (GMT), or dead butt syndrome (DBS) may lead to complications,�including trochanteric bursitis, IT band syndrome, and plantar fasciitis, among other health issues.
Differential Diagnosis of Hip Pain and Discomfort
� �
Fibromyalgia is widespread pain and discomfort throughout the human body. People with this painful condition can experience a variety of symptoms, including sciatica or sciatic nerve pain. Doctors and functional medicine practitioners believe that fibromyalgia can aggravate how the human body feels painful sensations by affecting how the human brain processes pain signals. Fibromyalgia and sciatica are two well-known conditions which can commonly coexist together. However, many fibromyalgia sufferers have also reported experiencing gluteal medius tendinopathy (GMT), or dead butt syndrome (DBS), a painful health issue caused by the inflammation of the tendons in the gluteus medius muscle. Because fibromyalgia is often associated with increased inflammation and painful symptoms, GMT or DBS and sciatica can commonly develop together. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
People with fibromyalgia experience widespread pain and discomfort as a result of their medical condition, however, healthcare professionals have demonstrated that fibromyalgia may also cause other symptoms and health issues to manifest, such as sciatica, or sciatic nerve pain, and gluteal tendinopathy. The purpose of the article above was to demonstrate and compare fibromyalgia, sciatica and gluteal tendinopathy symptoms. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Carpal tunnel syndrome, or CTS, is a condition where the nerve that runs from the forearm into the hand gets compressed. Carpal tunnel can cause significant pain and result in numbness that makes using your hand practically impossible.
Carpal tunnel affects�approximately 3% of the population. Carpal tunnel sufferers, fortunately, there are effective treatments that do not require surgery. Chiropractic care can help relieve the pain of carpal tunnel, and can often improve mobility and range of motion in the process.
What is it?
The term �carpal tunnel� refers to an actual tunnel created by ligaments and bones in the wrist. Tendons and median nerves travel from the forearm through the carpal tunnel in the wrist and into the hand. When the median nerve becomes compressed inside the carpal tunnel�usually due to injury or inflammation�it can lead to the symptoms associated with CTS.
The Causes
The exact cause of CTS is not always easy to identify, but there are many factors that can play a role. A family history of CTS makes it more likely that you will develop the condition. Repetitive work, such as a job on an assembly line, is known to increase the risk of CTS. Wrist injuries can also cause carpal tunnel. There are other contributing factors that are not as obvious, such as pregnancy, menopause, and dialysis.
Symptoms
The first signs of carpal tunnel often include a feeling of pins and needles in the wrist, hands, and fingers. You may notice some numbness from time to time, especially after using the wrist in a way that causes compression�like performing a task over and over at work.
Over time, the symptoms can become more severe. Eventually, carpal tunnel can lead to a loss of coordination with the thumb, then other digits. Pain may not be significant at first, but tends to get worse and the condition progresses.
Chiropractic Can Help
Standard medical treatments for carpal tunnel include using anti-inflammatory drugs, refraining from using the wrist/hand, wearing a splint and eventually surgery. While these treatments can sometimes be effective, the risks associated with surgery are significant. Carpal tunnel surgery may or may not fix the problem, and as with any surgery, can sometimes cause more issues than it helps.
Learning to Protect Yourself
Chiropractic care offers a safe alternative to standard medical care, one that is non-invasive and minimizes the need for medications and their potential side effects. Chiropractic treatments for carpal tunnel can help to reduce inflammation and minimize pain. But chiropractic goes further than just treating the symptoms�it can also help you avoid aggravating the condition so that it can heal.
Chiropractors are trained in proper movement and ergonomics. Your chiropractor can help you understand what you are doing that is causing the carpal tunnel to begin with. He or she can also advise you on ways to adjust your movements to protect your wrists moving forward. You may be able to learn new ways of doing things that will allow you to achieve your goals without risking injury.
Getting Stronger
One of the fundamentals of chiropractic care is improving strength and mobility to aid in healing and protect from further injury. Your chiropractor can guide you through exercises to make you stronger. Once you know how to do the exercises, you can do them at home to continue to gain strength.
Schedule An Appointment
Carpal tunnel sufferers, don’t wait any longer and contact us to schedule an appointment. We will get you the relief you need!
Fibromyalgia and sciatica are two well-known health issues which can commonly occur at seemingly the same time in people, however, these may also frequently require different treatment approaches to help manage their painful symptoms. Fibromyalgia is characterized by widespread pain throughout numerous regions of the human body. As complex as the diagnosis and treatment for fibromyalgia might be, it’s ultimately fundamental for patients to be aware of any other conditions which may subsequently develop due to the painful symptoms of these well-known health issues. �
Sciatica, also known as sciatic nerve pain, is a collection of symptoms rather than a single condition and it is one of the most common health issues to coexist together with fibromyalgia. In this instance, one condition doesn’t necessarily cause the other, however, they can basically be present together. Fibromyalgia�patients should understand how sciatica and its characteristic symptoms can affect their overall health and wellness. Many people with fibromyalgia may subsequently develop other health issues when these painful symptoms overlap with other conditions, such as piriformis syndrome. �
Piriformis Syndrome vs Sciatica and Fibromyalgia
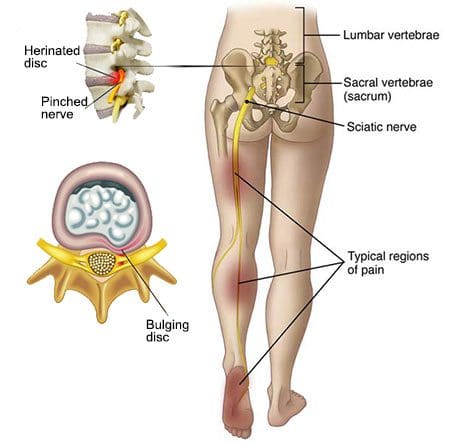
People with sciatic nerve pain, or sciatica, will often report experiencing pain and discomfort, tingling sensations, and numbness anywhere along the length of the sciatic nerve. The sciatic nerve is the longest and largest nerve in the human body, which travels from the lower back into the hip and buttocks, down into the thighs, knees, legs, and feet. Healthcare professionals may perform a variety of evaluations and tests to determine the source of a patient’s symptoms. People with fibromyalgia and sciatica may also experience another common health issue known as piriformis syndrome. �
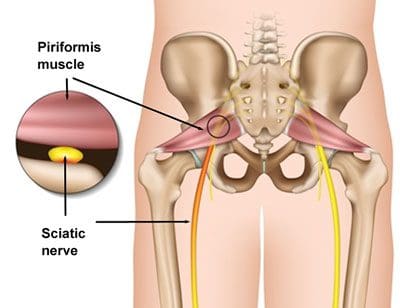
Sciatica is caused by the compression or impingement of the sciatic nerve, frequently due to a herniated disc. Piriformis syndrome can cause sciatica when a piriformis muscle spasm irritates the sciatic nerve. The piriformis is a muscle which extends from the front of the sacrum, or the triangle-shaped bone between the two hipbones in the pelvis, across the sciatic nerve and into the top of the femur, or the large bone in the upper leg.� The piriformis muscle is fundamental because it allows the thighs to move from side to side. When an injury or underlying condition causes the piriformis muscle to compress or impinge the sciatic nerve due to irritation and/or inflammation, the end result is typically piriformis syndrome. �
�
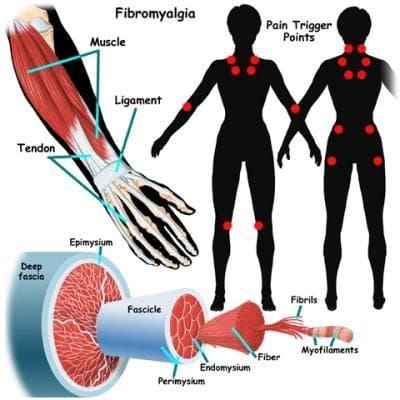
Sciatica is the most common symptom associated with piriformis syndrome. Other common symptoms associated with piriformis syndrome include tingling sensations and numbness, muscle tenderness, pain and discomfort while sitting or engaging in physical activities, and difficulty sitting comfortably. Because fibromyalgia causes widespread pain and inflammation, it’s also fundamental for people with fibromyalgia to seek immediate medical attention to diagnose all of their symptoms and rule out the possibility of their sciatica symptoms being due to piriformis syndrome or any other health issue. �
As previously mentioned above, sciatica, or sciatic nerve pain, is a medical condition or rather a collection of symptoms which causes pain and discomfort anywhere along the entire length of the sciatic nerve. For both fibromyalgia sufferers and people with the health issue alone, the pain and discomfort will generally manifest on one or both sides of the hips, buttocks, and thighs, where it will then radiate down the back of the leg, knees, and feet. In some instances, other common symptoms may manifest along the lower extremities, including tingling sensations, burning sensations, numbness, and weakness.
Sciatic nerve pain is most frequently caused by a slipped disc, a bulging disc, a herniated disc, or any other health issue which ultimately causes nerve pain and discomfort, such as fibromyalgia. When sciatica due to piriformis syndrome and/or another medical condition is experienced by fibromyalgia sufferers, it may be difficult for healthcare professionals to find the true source of their painful symptoms. Also, the symptoms associated with sciatic nerve pain and piriformis syndrome are generally the same for fibromyalgia sufferers, however, the most common causes may not be responsible for the symptoms.
Differential Diagnosis in Hip Pain
�
Fibromyalgia is characterized as widespread pain and discomfort throughout the human body. People with this painful health issue can experience a variety of symptoms, including sciatic nerve pain, or sciatica. Healthcare professionals believe that fibromyalgia can increase the way the human body experiences painful sensations by affecting the way the brain processes pain signals. Fibromyalgia and sciatica are two well-known conditions which can commonly coexist together. However, many fibromyalgia sufferers have reported piriformis syndrome, a condition caused when the piriformis muscle irritates the sciatic nerve. Because fibromyalgia can often be associated with increased pain and inflammation, these painful symptoms and health issues can ultimately occur. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Fibromyalgia Magazine
�
�
People with fibromyalgia experience widespread pain and discomfort as a result of their medical condition, however, healthcare professionals have demonstrated that fibromyalgia may also cause other symptoms and health issues to manifest, such as sciatica, or sciatic nerve pain, and piriformis syndrome. The purpose of the article above was to demonstrate and compare fibromyalgia and sciatica symptoms versus piriformis syndrome. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900�. �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Severe Sciatica
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of sciatica, or sciatic nerve pain. Sports injuries or automobile accident injuries are often the most frequent cause of painful symptoms, however, sometimes the simplest of movements can have these results. Fortunately, alternative treatment options, such as chiropractic care, can help ease sciatic nerve pain, or sciatica, through the utilization of spinal adjustments and manual manipulations, ultimately improving pain relief. �
�
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
*All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 �
� �
�



 �
� �
�
 �
� �
�
 �
� 


 �
�
 �
�





