El Paso Back Clinic Shockwave Therapy: A Non-Surgical Option for Chronic Pain
Why Real ESWT Matters for Deep Healing at an Integrative El Paso Back Clinic
When people hear the term shockwave therapy, they often assume every machine is the same. It is not.
Some devices are true medical Extracorporeal Shockwave Therapy (ESWT) systems. Other devices are weaker radial pressure wave tools that are sometimes marketed as shockwave devices, even though they work differently. That difference matters if your goal is real tissue healing, not just short-term soreness relief. Mayo Clinic explains that focused shockwave (FSW) and radial pressure wave (RPW) are distinct waveforms, and only FSW is considered a “true shockwave” in a strict physical sense.
For a clinic like El Paso Back Clinic, where patients often come in with chronic pain, sports injuries, auto injuries, soft-tissue damage, and complex back conditions, the type of device and the treatment plan can make a big difference. The clinic’s site emphasizes multidisciplinary care, non-surgical recovery, and an integrative model that includes chiropractic, rehab, and functional medicine support.
This article explains, in plain language, what “real” shockwave therapy is, why focused shockwave is different from weaker devices, and how it fits into a complete recovery program in an integrative chiropractic setting.
What Is Real Shockwave Therapy?
Extracorporeal Shockwave Therapy (ESWT) is a non-invasive treatment that sends acoustic energy (sound waves) into injured tissue from outside the body. It is used in musculoskeletal care to help reduce pain and support healing in stubborn injuries. UCHealth describes ESWT as a noninvasive option for people who have not responded well to more conventional treatments, noting that it delivers high-energy acoustic waves to injured areas.
Mayo Clinic also describes shockwave therapy as a growing tool in physical medicine and sports medicine, especially for tendon and fascia problems.
In simple terms
Shockwave therapy is used to help the body “restart” healing in tissue that has been painful or stuck for a long time, such as:
tendons
fascia
ligaments
some chronic soft-tissue injuries
certain bone healing problems (in selected cases)
Mayo Clinic lists many musculoskeletal uses, including plantar fasciitis, Achilles tendinopathy, patellar tendinopathy, and lateral epicondylitis (tennis elbow).
Not All “Shockwave” Machines Are the Same
This is the most important part of the topic.
Many clinics use the word shockwave, but there are two main categories of devices used in musculoskeletal care:
Focused Shockwave (FSW / F-ESWT)
Radial Pressure Wave (RPW / radial therapy)
Mayo Clinic clearly explains that these are different technologies and should not be treated as identical. In fact, Mayo states that only focused shockwave generates a true shockwave, while radial devices generate a radial pressure wave.
Why that matters
The difference is not just marketing. It affects:
how deep the energy goes
how precise the treatment is
how much energy reaches the target tissue
what conditions may respond best
If a patient has a deep tendon problem, scar tissue, or a stubborn chronic injury, the provider should know exactly what machine is being used and why.
Focused Shockwave vs. Radial Pressure Wave
Here is the practical difference in plain language.
Focused Shockwave (FSW)
Focused shockwave is designed to deliver energy to a specific target depth. It is more precise and is often the better choice when the provider wants to treat a deeper structure or a smaller, more exact area. Mayo Clinic notes that focused shockwave has different physical properties and can be used alone or in combination with radial treatment, depending on the condition.
Radial Pressure Wave (RPW)
Radial therapy spreads energy more broadly and is often more surface-level. Mayo Clinic explains that radial devices generate pressure waves and notes tissue penetration of about 4 to 5 cm in its 2022 discussion of radial ESWT.
That does not mean radial is “bad.” It means it is different. In many cases, radial therapy remains helpful. But if a clinic claims “shockwave” and the patient expects high-energy focused treatment, the patient should ask which device is being used.
Quick comparison
Focused shockwave
More precise targeting
True shockwave physics
Often used for deeper or more exact lesions
Better fit for some regenerative goals
Radial pressure wave
Broader spread
Pressure-wave technology
Often, more superficial or diffuse treatment
Can still be useful in the right case
Why Energy Dose Matters
Real ESWT is not just “machine on, machine off.” It is dosed.
One of the main ways clinicians describe ESWT dose is Energy Flux Density (EFD), and the standard unit is mJ/mm² (millijoules per square millimeter). A PubMed Central review explains that EFD is the professional parameter used to describe shockwave energy flow through tissue, and specifically notes the unit of measurement as mJ/mm².
This is important because:
stronger energy is not always better
tissue type matters
the diagnosis matters
different injuries need different treatment settings
A quality clinic should be able to explain the treatment plan in a way that matches your condition, rather than using the same approach for every patient.
Does Shockwave Therapy Create “Microtrauma”?
Many people explain shockwave therapy by saying it creates “microtrauma” that triggers healing. That is a common explanation, and Mayo Clinic Sports Medicine uses this language in a patient-friendly way, noting that acoustic waves can create microtrauma to help reinitiate a healing response in tendons.
That said, many experts also describe the process in a more modern way as mechanotransduction—meaning the waves create a mechanical signal that helps cells activate repair pathways. Mayo Clinic’s 2025 article also highlights mechanotransduction and regenerative effects like cellular signaling and neovascular changes.
A simple way to think about it
Shockwave therapy helps by:
stimulating local tissue response
improving healing signaling
reducing pain pathways over time
helping stubborn tissue become more “active” in repair
So the short answer is:
Yes, “microtrauma” is a common way to explain it.
But the bigger idea is that the shockwave creates a healing signal, not uncontrolled tissue damage.
FDA Regulation and Why It Matters
Another reason patients should ask questions is that regulatory status matters.
The FDA has approved/cleared specific extracorporeal shockwave devices for specific uses. For example, the FDA PMA listing for the OrthoSpec Extracorporeal Shock Wave Therapy device states that it is indicated for adults with proximal plantar fasciitis (with or without a heel spur) who have had symptoms for 6 months or more and have failed conservative treatment.
That helps patients understand two important points:
real ESWT is a recognized medical technology
device claims should match actual indications and training
If a clinic says “shockwave,” it is fair to ask:
What exact device is this?
Is it focused or radial?
Is it FDA-cleared/approved for a musculoskeletal indication?
These are smart questions, not rude questions.
Why Real ESWT Is Useful in an Integrative Chiropractic Clinic
Shockwave therapy can be very effective, but it works best when the diagnosis is correct, and the rest of the care plan supports healing.
That is where an integrative clinic model is helpful.
The El Paso Back Clinic describes on its website a multidisciplinary, non-surgical, and functional recovery approach that includes chiropractic care, rehab, and broader wellness support. It also describes care for back, auto, and sports injuries, tendinopathy-related issues, and chronic pain.
Why this pairing makes sense
Shockwave therapy targets soft tissue and the healing response.
Chiropractic and rehab help restore:
joint motion
spinal alignment
posture
movement control
load tolerance
When these are combined, the patient gets a more complete plan.
Example of an integrative recovery setup
A patient with chronic Achilles pain, plantar fasciitis, or post-accident scar tissue restriction may benefit from:
Focused shockwave or radial therapy (depending on the tissue depth and goal)
Chiropractic adjustments to improve joint mechanics
Mobility work to reduce compensation patterns
Strength training/rehab exercise to improve tissue tolerance
Lifestyle support (sleep, inflammation control, nutrition)
This is especially important for back and soft-tissue injuries, as pain often has multiple causes. The tissue may be irritated, but there may also be a movement issue, posture problem, or old compensation pattern keeping it from healing.
Clinical Observations in Dr. Alexander Jimenez’s Integrative Model
Public information on dralexjimenez.com and El Paso Back Clinic describes Dr. Alexander Jimenez as a Doctor of Chiropractic and board-certified Family Nurse Practitioner (DC, APRN, FNP-BC) who uses a multidisciplinary, integrative approach focused on non-surgical recovery, diagnostics, and personalized care.
His El Paso Back Clinic content also emphasizes:
advanced injury rehabilitation
chronic pain care
sports injury care
auto injury care
functional medicine support
team-based recovery planning
These clinic observations support the idea that shockwave therapy should not be used as a stand-alone “gadget” treatment. Instead, it fits best within a broader care plan that includes biomechanics, rehab, and whole-person recovery.
Why dual training matters in this setting
In a clinic model that blends chiropractic and nurse practitioner perspectives, the provider can often look at a case more completely, including:
musculoskeletal pain drivers
nerve irritation patterns
inflammation
healing delays
activity limitations
overall recovery readiness
That type of clinical reasoning is helpful when deciding whether a patient should receive:
focused shockwave
radial therapy
chiropractic and rehab only
imaging first
referral or co-management
What Conditions Often Respond to Shockwave Therapy?
Shockwave therapy is often used for chronic injuries that have not improved enough with standard care.
Mayo Clinic and UCHealth commonly describe these types of cases:
Plantar fasciitis
Tennis elbow (lateral epicondylitis)
Achilles tendinopathy
Patellar tendinopathy
Shoulder tendinopathy
Other chronic tendon or fascia pain problems
Mayo’s clinical articles also note that ESWT has roles in treating tendons, ligaments, fascia, and even in selected bone-healing situations.
It may be especially helpful when:
pain has lasted for months
the patient plateaued in regular therapy
surgery is being considered, but not yet desired
the injury is painful with loading (walking, running, lifting, gripping)
the provider wants a non-invasive option
How to Tell if a Clinic Is Offering “Real” Shockwave Therapy
Because the market uses confusing language, patients should ask direct questions before paying for treatment.
Ask these questions
Is this focused shockwave (FSW) or radial pressure wave (RPW)?
What condition are you treating, and why is this device the right choice?
How do you set the energy dose (EFD/mJ/mm2)?
How many sessions are usually recommended for my condition?
Will I also get rehab or movement treatment?
If my pain is deep, how will you target it?
Is the device FDA-cleared/approved for musculoskeletal use?
A strong clinic should be comfortable answering these questions in simple language.
Why Device Hype Alone Is Not Enough
Some clinics advertise shockwave therapy as a miracle treatment. That is not the best way to present it.
Shockwave therapy can be a powerful tool, but results depend on:
Even the best technology will not work well if the diagnosis is wrong or if the patient returns to the same harmful movement pattern right away.
This is one reason integrated care models, like the one described at El Paso Back Clinic and Dr. Jimenez’s clinical sites, can be so useful for complex injuries: patients receive more than one treatment option and more than one clinical lens.
Bottom Line: Focused ESWT Is the Better Choice for True Regenerative Shockwave Goals
If your goal is real regenerative shockwave therapy, focused shockwave (FSW/F-ESWT) is usually the benchmark because it is the true shockwave form and offers more precise targeting. Mayo Clinic makes this distinction very clearly.
Radial devices can still be helpful in many cases, but they are not the same technology. Patients should not be told they are identical.
For patients in El Paso dealing with:
chronic tendon pain
back-related soft tissue problems
sports injuries
accident-related soft tissue injury
stubborn pain that has not improved
An integrative clinic model like El Paso Back Clinic can be a strong fit because it combines:
non-invasive care
structural assessment
chiropractic and rehab
broader healing support
multidisciplinary planning
That is often what it takes to move from “temporary pain relief” to true recovery.
Sciatica Self-Massage at Home (The El Paso Back Clinic Approach to Safer Relief)
Sciatica is a nerve irritation pattern, not just a tight muscle. It often feels like burning, aching, tingling, or “electric” pain that can start in the low back or buttock and travel into the thigh, calf, and foot. Many people in El Paso experience sciatica after long hours of sitting, driving, or heavy lifting, or after an old injury that never fully healed. At El Paso Back Clinic, sciatica care is commonly described as integrative—meaning hands-on chiropractic care plus soft-tissue work, rehab, and (when appropriate) decompression strategies to reduce nerve pressure and help the body heal instead of just “chasing symptoms.”
Self-massage can be an effective home tool when done correctly. The goal is to relax the tissues around the irritated nerve pathway—especially the glutes, piriformis, low back muscles, hamstrings, and sometimes the calf—without smashing the nerve itself.
The safety rule that matters most: don’t “dig into” the sciatic nerve
If you press directly on the most “zappy” spot, you can flare symptoms. Instead, aim for gentle, targeted pressure that feels like a controlled release.
Use the “hurts good” rule:
Keep pressure 0–3 out of 10 (mild to moderate discomfort)
Avoid 4–10 out of 10 (too aggressive)
If symptoms worsen, stop right away and reduce pressure next time
Tools that work well at home
You do not need expensive equipment. These basic tools are enough for most people:
Tennis ball (beginner-friendly pressure)
Foam roller (great for slow myofascial release)
Two tennis balls taped together or in a sock (to work beside the spine more safely)
Heat pack (before or after)
Many sciatica massage guides recommend simple tools like tennis balls and foam rollers because they help you reach deep glute and hip muscles without overworking your hands.
Step-by-step: a simple self-massage routine for sciatica relief
Start with heat (optional, but helpful)
Apply heat to the lower back or glutes for 10–15 minutes. Heat can help muscles relax, so you do not need to apply as much pressure during a massage.
Tip: Heat should feel soothing, not scorching.
Trigger point release for the glutes and piriformis (tennis ball)
This is one of the most helpful self-massage steps because the piriformis and nearby glute muscles can tighten and irritate the sciatic nerve pathway.
How to do it:
Sit on the floor (or a firm bed) and place a tennis ball under one buttock.
Lean your weight into the ball until you find a tender “knot.”
Hold steady pressure for 20–45 seconds while breathing slowly.
Move the ball 1–2 inches and repeat on 2–4 spots.
Keep it safe:
If pain becomes sharp, numbness increases, or symptoms travel farther down the leg, stop immediately.
Low back muscle release (two tennis balls—NOT on the spine)
At El Paso Back Clinic, massage and soft-tissue work are considered a key part of sciatica treatment because relaxing tight tissues can reduce pressure on irritated structures. A safe home approach is to use two tennis balls so that pressure is applied beside the spine.
How to do it:
Tape two tennis balls together (or place them in a sock).
Lie on your back with knees bent.
Place the balls on either side of the spine, not on the bone.
Make tiny shifts and pauses—no fast rolling.
Work for 1–2 minutes, then rest.
Myofascial release for hamstrings (foam roller)
If your hamstrings are tight, they can “pull” on the pelvis and keep the low back and hip region tense. Slow foam rolling is often described as a form of self-myofascial release that warms and loosens tissue over time.
How to do it:
Sit with the roller under the back of your thigh.
Roll slowly and pause on tight spots for 20–30 seconds.
Don’t chase pain—stay in the 0–3/10 range.
Calf massage for referred pain (hands or roller)
Some sciatica patterns show up strongly in the calf or foot. Gentle calf work may help reduce guarding and improve comfort.
How to do it:
Use your hands to squeeze and glide from ankle toward knee.
Pause on a tender spot and breathe.
Keep pressure light to moderate.
What to avoid (so you don’t flare symptoms)
Heavy pressure on the “electric” pain spot
Fast rolling over the lower back or buttocks
Long sessions that leave you sore for 1–2 days
Pressing on the bone (spine, sacrum ridge, hip bone)
If you feel worse after self-massage, your body is telling you the dose was too high. Reduce pressure and shorten the next session.
Why chiropractic + massage often works better than either alone
Self-massage can help relieve muscle tension, but some cases of sciatica also involve spinal joint restriction, disc irritation, or nerve root pressure. That is why integrative chiropractic care is often paired with soft-tissue work.
On El Paso Back Clinic, sciatica care is described as focusing on addressing sources of pain (not only masking it), and the clinic also highlights combining chiropractic adjustments with therapeutic massage and non-surgical decompression options.
Common integrative components include:
Targeted chiropractic adjustments to improve motion and reduce irritation
Myofascial release/therapeutic massage to reduce spasms and improve circulation
Non-surgical spinal decompression (when appropriate) to reduce pressure on discs/nerve roots
Clinical observations from Dr. Alexander Jimenez
Across sciatica-focused education on the clinic’s site, the recurring theme is that lasting relief often improves when care addresses both sides of the problem:
tissue tension (glutes/piriformis/low back tightness), and
spinal mechanics (how joints/discs and nerve pathways are loading under stress).
When to stop home care and get evaluated quickly
Get urgent medical evaluation if you have:
New or worsening leg weakness
Loss of bowel or bladder control
Numbness in the saddle area
Severe pain with fever, unexplained weight loss, or major trauma
These may indicate a condition requiring immediate care beyond self-massage.
Neuropathy Pain: “What’s the Best Medication?” And How El Paso Back Clinic Uses a Team Approach
Neuropathy is a common reason people contact El Paso Back Clinic®. The most common question sounds simple: “What’s the best medication for this pain?” But neuropathy is not one single problem. It is a symptom pattern (burning, tingling, numbness, electric shocks, sensitivity) that can result from various causes, such as diabetes, vitamin deficiencies, nerve compression, medication side effects, or past injuries. Getting the “best” treatment usually means combining the right medical plan with the right hands-on and movement-based care, plus lifestyle steps that protect nerves over time.
At El Paso Back Clinic, the care model described in their neuropathy education includes integrative chiropractic care coordinated with nurse practitioner (NP) oversight, aiming to improve function and quality of life while also looking for root causes.
What Peripheral Neuropathy Really Means
Peripheral neuropathy means the nerves outside the brain and spinal cord are irritated or damaged. These nerves help with:
Feeling (touch, pain, temperature)
Movement (muscle control)
Automatic body functions (sweating, digestion, blood pressure)
When signals get disrupted, symptoms can include burning pain, numbness, tingling, cramps, and weakness—often starting in the feet or hands.
Why cause matters: Treatment works best when you address both the pain and the underlying cause of the nerve’s discomfort. Primary care guidance emphasizes a careful history, exam, and targeted lab testing to look for common causes (diabetes, alcohol use, nutritional issues, toxins, nerve compression, and more).
The “Best Medication” for Neuropathy Pain: What Most Guidelines Start With
There isn’t a single perfect medication for everyone. Most major guidance starts with a few first-line options because they can reduce abnormal nerve pain signaling:
Common first-line medication groups
Gabapentinoids:gabapentin or pregabalin
SNRIs (a type of antidepressant used for nerve pain):duloxetine
TCAs (older antidepressants used for nerve pain):amitriptyline (used more often at night due to sedation)
This is consistent across multiple evidence summaries and public clinical guidance.
What patients usually want to know (in plain language)
These medicines do not “fix” the nerve overnight.
They aim to reduce the volume of nerve pain messages reaching the brain.
Many people need dose adjustments or a different medication to get the best balance of relief and side effects.
Side Effects to Expect (And Why NPs Help So Much Here)
A big reason people stop neuropathy meds is side effects—especially in the first 1–3 weeks. The NHS lists these as commonly used neuropathic pain medicines, and side effects are a key part of safe prescribing decisions.
Typical side effects patients report
Gabapentin/pregabalin: sleepiness, dizziness, “brain fog,” swelling, weight gain (for some)
Amitriptyline: dry mouth, constipation, grogginess, dizziness (often taken at night)
How an NP helps (practical, real-world):
Reviews your full medication list to avoid risky combos
Adjusts timing (for example, shifting sedating doses toward evening)
Watches for issues like fall risk, daytime sleepiness, and mood changes
Checks labs or contributing problems (blood sugar, B12, thyroid, kidney function when relevant)
Plans step-by-step changes instead of guessing
NPs are also well-positioned to manage chronic pain patterns and medication decision-making over time, because neuropathy often requires follow-up and fine-tuning.
“Are There Non-Drug Treatments?” Yes—And They Matter
Most people with neuropathy want conservative options first, or at least options that let them use less medication. The El Paso Back Clinic neuropathy education highlights several non-surgical strategies commonly used in integrative care.
Integrative chiropractic care focused on movement, joint mechanics, and nerve irritation patterns
Footwear, balance support, and fall prevention
Sleep and stress strategies (very underrated for nerve pain)
Patient-facing education materials often encourage asking about topical options, TENS, and PT because neuropathy increases fall risk and balance issues.
A safety point that matters in real life
When numbness is present, people may not notice small injuries—especially on the feet. Major cancer center patient education emphasizes routine skin checks (hands/feet) and lifestyle habits that support nerve health and safety.
How Integrative Chiropractic Care Can Help Neuropathy Symptoms
Not all neuropathy pain is the same. Some nerve pain is driven by systemic issues (like diabetes). Other nerve pain can be worsened by biomechanics—for example, irritation at the spine, pelvis, or along nerve pathways that changes movement and increases sensitivity.
The El Paso Back Clinic neuropathy resource outlines an approach focused on non-invasive, whole-person strategies and coordination with NP oversight.
What integrative chiropractic care may focus on
Finding patterns of nerve compression/irritation linked to posture or movement
Improving joint motion to reduce “mechanical stress” on sensitive areas
Corrective exercises to support better balance and gait
Soft tissue work and mobility strategies to reduce protective tension
Coordinating with medical care when neuropathy is linked to diabetes, medication effects, or other systemic causes
Important note: Chiropractic and integrative therapies should be framed as part of a broader plan—not a stand-alone “cure.” A careful diagnostic workup is still key, especially if symptoms are new, worsening, one-sided, or include weakness.
“Why Is My Neuropathy Worse at Night?”
This is one of the most common questions. Nighttime can amplify nerve pain for several reasons:
Less distraction: your brain has fewer competing signals
Stress/emotions: the day catches up, and pain feels louder
Temperature changes: some people notice symptoms more when cooler
Cleveland Clinic’s patient education explains several of these factors and also notes that approaches like PT, mindfulness, and medication adjustments may help when pain spikes at night.
Nighttime tips that are often helpful
Keep a steady sleep schedule (even on weekends)
Avoid alcohol excess (it can worsen neuropathy for some people)
Review medication timing with your NP
Use foot/hand warmth if cold triggers symptoms (not hot enough to burn)
This is where a stepwise plan matters. Many people either give up too early or keep escalating one med until side effects take over.
Evidence-based reviews emphasize recognizing when treatment is not effective and switching earlier, and they also note that combination therapy can help some patients (using moderate doses instead of maxing out on a single drug).
Common next steps an NP may consider
Confirm the diagnosis (is it neuropathy, radiculopathy, vascular, or something else?)
Adjust dose timing or switch to a different first-line option
Consider combination therapy when appropriate and safe
Severe pain with fever, unexplained weight loss, or a cancer history
Primary care guidance recommends referral for electrodiagnostic studies when symptoms are concerning (e.g., rapid progression, asymmetry, motor/autonomic issues) or when the initial workup is normal but symptoms persist.
The “Two Lanes” of Neuropathy Care at El Paso Back Clinic: Medical + Mechanical
A practical way to think about neuropathy treatment is two lanes running together:
Support nerve health with lifestyle and risk-factor control
Coordinate referrals for testing if needed
Lane 2: Integrative chiropractic + rehab
Address movement patterns that keep pain “turned up”
Improve mobility, balance, and function
Reduce mechanical stress and improve daily tolerance
Build a home plan you can actually follow
This is the kind of “integrative” model described in El Paso Back Clinic’s neuropathy content—conservative, coordinated, and focused on quality of life.
Smart Questions to Ask at Your Neuropathy Visit
Patients often feel more confident when they come in with clear questions. These are consistent with neuropathy question guides and clinical evaluation principles:
Medication questions
“What is the first medicine you recommend, and what side effects should I expect?”
“If that doesn’t work, what’s next?”
“Are topical lidocaine patches or creams right for me?”
Diagnosis and cause questions
“What type of neuropathy do I have?”
“What do you think is the most likely cause for me?”
“Will we check for diabetes/prediabetes, vitamin levels, or thyroid issues?”
“Do my symptoms suggest inherited, toxic, inflammatory, or metabolic patterns?”
Function and safety questions
“What can I do to improve balance and prevent falls?”
“What should I do for foot care if I can’t feel injuries well?”
“Which exercises are safe for me right now?”
Bottom Line
The “best medication” for neuropathy pain is the one that reduces pain enough to help you function without side effects that wreck your day. For many people, that means starting with gabapentin, pregabalin, duloxetine, or amitriptyline, and then adjusting based on response and tolerability.
At El Paso Back Clinic, the integrative approach outlined in their neuropathy resources emphasizes coordinated care—NP oversight of medical management and integrative chiropractic strategies to support mobility, comfort, and daily life.
Sciatica Numbness in the Hamstring and Foot (Without Low Back Pain): An El Paso Back Clinic Guide to What It Means and What to Do
Patient with sciatica symptoms but no back pain, only leg and foot numbness and pain, lies supine on the examination table while the chiropractor/nurse practitioner lifts his extended leg with resistance.
If your hamstring feels numb or your foot feels tingly or “asleep,” it’s easy to think you pulled a muscle. But many people in El Paso are surprised to learn that sciatica can show up as leg numbness without much (or any) low back pain. That pattern is common—and it’s one reason sciatica can get missed at first. (Yale Medicine, n.d.; Penn Medicine, n.d.; AMA, 2024)
At El Paso Back Clinic, we often see this exact concern:
“My lower back doesn’t hurt… so how can this be sciatica?”
“Why is there numbness in my hamstring and foot?”
“Is this a hamstring strain or a nerve issue?”
“When should I worry and get checked?”
This article explains the “why,” helps you distinguish between muscle and nerve pain, and shows how an integrative chiropractic approach may reduce sciatica-related numbness by addressing the spine, hips, soft tissues, and movement habits that keep the nerve irritated. (HSS, 2024; Fletcher Family Chiropractic, 2025; Auburn Hills Chiropractic, n.d.)
Important: Numbness can have several causes. A careful evaluation matters—especially if symptoms persist or worsen.
What Sciatica Really Is (And Why It Can Feel Like a Hamstring/Foot Problem)
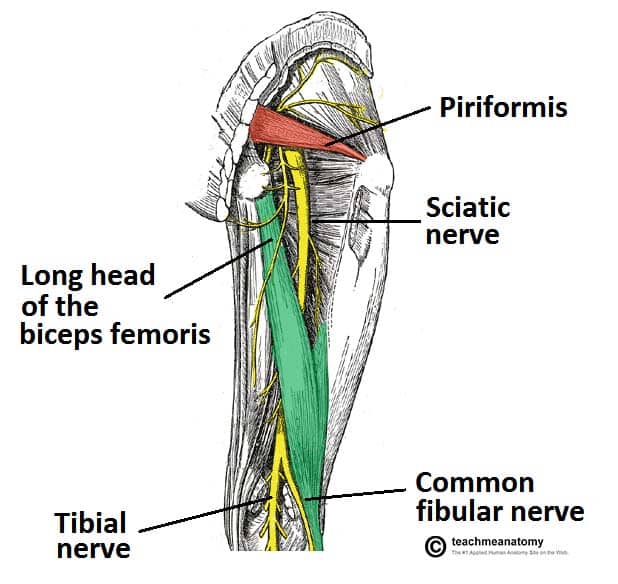
Sciatica is a set of symptoms caused by irritation or compression of nerve roots in the lower back or of the sciatic nerve pathway itself. The sciatic nerve is the largest nerve in the body. It starts in the lower back and travels through the buttocks, down the back of the thigh, and into the lower leg and foot. (Yale Medicine, n.d.; Penn Medicine, n.d.; HSS, 2024)
That pathway explains a big point:
You can feel the problem far away from where it starts. So even if your low back feels “fine,” the nerve signals going into your hamstring, calf, or foot can still be affected. (Yale Medicine, n.d.; Mayo Clinic, 2025)
Common sciatica symptoms include:
Pain that travels down the leg
Tingling (“pins and needles”)
Numbness in the thigh, leg, or foot
Burning or electric-like feelings
Weakness in the leg or foot (Mayo Clinic, 2025; Penn Medicine, n.d.)
Why Sciatica Can Cause Hamstring and Foot Numbness Without Back Pain
The nerve is irritated “upstream,” but you feel it “downstream”
A nerve can be irritated near the spine, but the symptoms often show up where the nerve travels—like the hamstring or foot. This is one reason people feel confused: the pain isn’t always in the back. (Yale Medicine, n.d.; Penn Medicine, n.d.)
Some sciatica patterns are leg-dominant
Some people mainly feel sciatica below the knee (calf/foot) with little low back pain. That’s still consistent with nerve involvement. (AMA, 2024; Mayo Clinic, 2025)
The irritation may be outside the spine (hip/buttock region)
Not every case is a disc issue. Sometimes the sciatic nerve becomes irritated where it passes through the buttocks. Tight, overworked muscles can compress or irritate the nerve, leading to numbness down the leg. (Total Ortho Sports Med, 2025; HSS, 2024)
Common Causes of Sciatica-Like Numbness (Even When the Low Back Doesn’t Hurt)
Think of these as the “usual suspects.” A proper exam helps pinpoint which one fits your pattern.
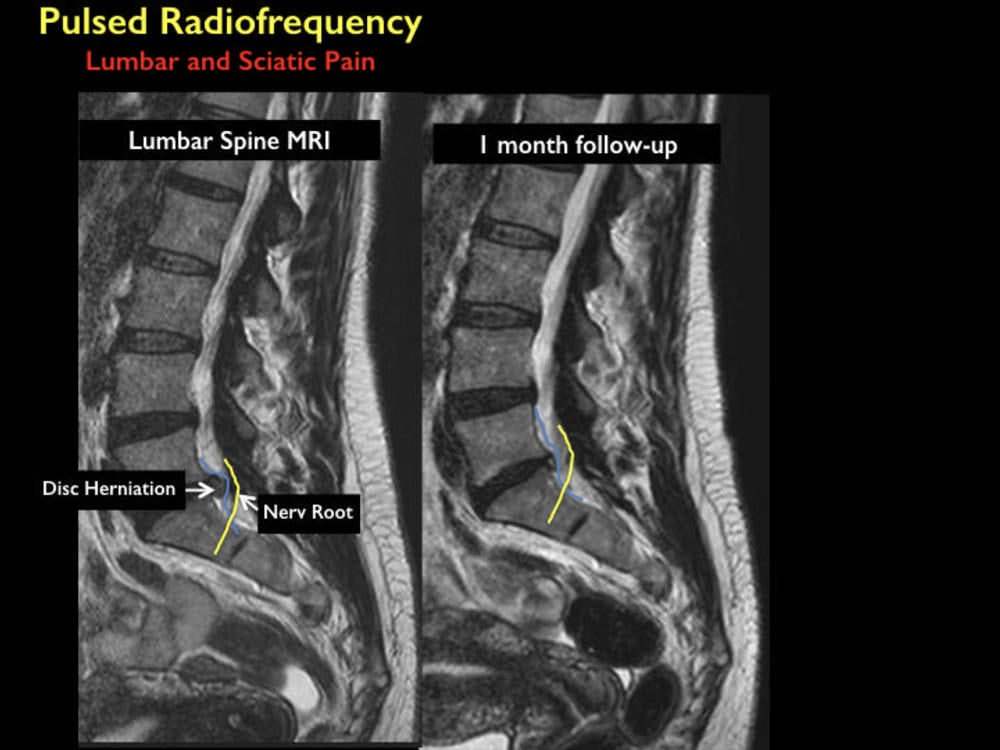
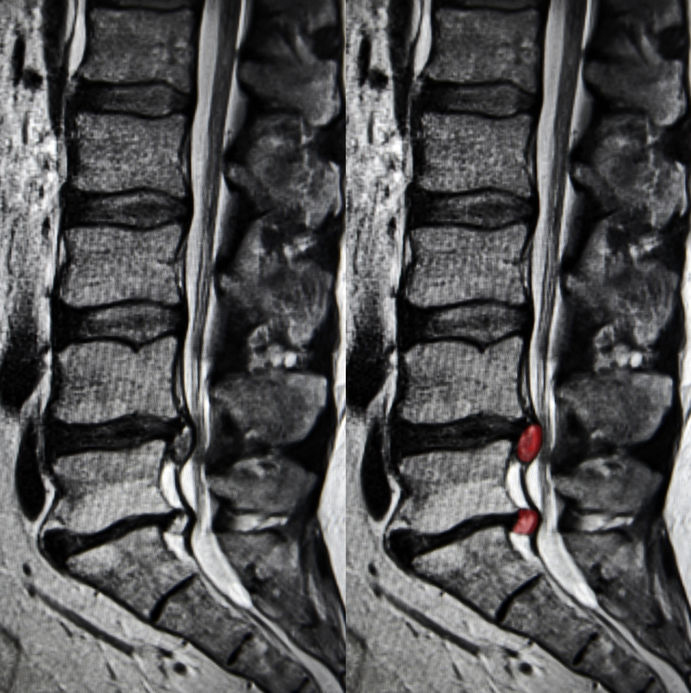
A) Lumbar nerve root irritation (radiculopathy)
A disc bulge/herniation, arthritic changes, or narrowing of the spaces in the spine can irritate nerve roots. You may feel numbness in the legs even if the back pain is mild. (Mayo Clinic, 2025; Penn Medicine, n.d.)
Clues that this may be happening:
Symptoms travel below the knee
Sitting makes it worse (especially long drives)
Coughing/sneezing increases symptoms
You notice weakness or heaviness in the foot (Mayo Clinic, 2025; Goodman Campbell, 2025)
B) Piriformis syndrome / deep buttock compression
When the buttock area is the main source of compression, you may feel:
Buttock tightness or a deep ache
Symptoms worsen with sitting
Numbness/tingling down the leg with minimal back pain (Total Ortho Sports Med, 2025)
C) Mobility and movement problems that keep the nerve irritated
Even when the “main” cause is a disc or nerve root, symptoms can stick around if:
The hips don’t move well
The pelvis is rotating during walking
The core and glutes aren’t supporting the spine
Work and driving keep you in nerve-irritating positions (HSS, 2022; Mayo Clinic, 2025)
In clinical settings like El Paso Back Clinic, we often see a pattern where spine mechanics + hip tension + repeated sitting/positioning team up to keep the nerve cranky. (Jimenez, n.d.)
D) Non-sciatica causes that mimic sciatica
Some issues look like sciatica but are different, such as:
Peripheral neuropathy
Other nerve entrapments lower in the leg
Vascular problems (circulation)
Rare but serious spinal conditions (AMA, 2024; Mayo Clinic, 2025)
That’s why ongoing numbness deserves a focused exam.
Sciatica vs. Hamstring Strain: How to Tell the Difference
This is one of the biggest “either/or” questions.
Hamstring strain is usually a muscle problem
Hamstring strains often occur during sprinting, sudden acceleration, or deep stretching. (Ducker Physio, 2025)
Typical hamstring strain signs:
Local pain in the back of the thigh
Tenderness to touch in the muscle
Pain with resisted knee bending or stretching the hamstrings
Usually no tingling or numbness in the foot (Ducker Physio, 2025)
Sciatica is a nerve problem
Sciatica symptoms often behave differently.
Typical sciatica signs:
Tingling, numbness, burning, or electric sensations
Symptoms can travel below the knee into the foot
Sitting, bending, or twisting can trigger it
The sensation may come and go with certain positions (Mayo Clinic, 2025; Yale Medicine, n.d.)
Quick comparison (simple and practical)
Hamstring strain: muscle pain, tender spot, worse with stretch/strength work, no foot numbness (Ducker Physio, 2025)
Sciatica: numbness/tingling, traveling symptoms, position-sensitive, may include weakness (Mayo Clinic, 2025)
Why You Can Have Foot Numbness and Not Much Pain
People often say, “It doesn’t hurt that badly, it’s just numb.” That can still be significant.
Numbness can happen when nerve signals are disrupted. Instead of sharp pain, your body gives you:
Reduced sensation
Tingling
A “sock-like” strange feeling
A foot that feels off when you walk (Mayo Clinic, 2025)
If numbness persists, spreads, or is accompanied by weakness, it’s a strong reason to get evaluated. (AMA, 2024; Mayo Clinic, 2025)
When to Get Help: Red Flags You Shouldn’t Ignore
Get urgent care if you have:
New or worsening leg weakness
Trouble lifting the foot (or frequent tripping)
Loss of bowel or bladder control
Numbness in the groin/saddle area
Severe symptoms after trauma (AMA, 2024; Mayo Clinic, 2025)
Schedule an evaluation soon if:
Numbness lasts more than 1–2 weeks
Symptoms keep returning
Numbness is moving farther down the leg
Pain/numbness is affecting sleep or walking
Home care isn’t working (Mayo Clinic, 2025; Goodman Campbell, 2025)
How El Paso Back Clinic Approaches Sciatica-Related Numbness (Integrative Chiropractic Perspective)
In Dr. Alexander Jimenez’s clinical observations, leg-dominant sciatica symptoms often improve best when care focuses on more than one area:
Spine mechanics (how the lumbar joints and discs are loading)
Hip and pelvis motion (how the leg is moving under the trunk)
Soft tissue tension (especially deep gluteal and posterior chain tightness)
Movement habits (sitting, driving posture, bending technique, sports training patterns) (Jimenez, n.d.)
This integrative approach aims to answer a simple question:
“Where is the nerve being stressed, and why is it staying stressed?” (Jimenez, n.d.)
Orthopedic tests (to reproduce or reduce symptoms)
Movement checks (hip hinge, gait, pelvic control)
Posture and work/drive habit review If findings suggest serious compression or a non-spine cause, referral or imaging may be appropriate. (Mayo Clinic, 2025; Penn Medicine, n.d.)
How Integrative Chiropractic Therapy May Help Reduce Hamstring and Foot Numbness
Sciatica-related numbness can improve when you reduce mechanical stress and calm irritation around the nerve.
Spinal and pelvic adjustments (when appropriate)
Chiropractic adjustments are often used to improve joint motion and reduce mechanical irritation patterns. Many chiropractic resources describe symptom improvement by addressing mobility restrictions and reducing stress on sensitive tissues. (Auburn Hills Chiropractic, n.d.; Alliance Ortho, 2024)
Soft tissue therapy for buttock/hip and posterior chain tension
Soft-tissue methods can help when muscle tension and fascial tightness contribute to irritation—especially in the deep gluteal region. (AFCadence, n.d.; Collective Chiro, 2024)
Common tools include:
Myofascial release
Trigger point work
Targeted stretching (symptom-guided)
Gentle mobilization
Rehab exercises that “retrain” movement, not just stretch
When numbness is linked to nerve irritation, the goal is often:
Better hip mobility without nerve flare-ups
Stronger glute support and core stability
Improved walking mechanics and posture
Gradual return to bending and lifting patterns (HSS, 2022; Mayo Clinic, 2025)
Technique options like flexion-distraction (case-by-case)
Some clinics use flexion-distraction approaches for certain disc-related patterns to reduce irritation and improve movement tolerance. (Fletcher Family Chiropractic, 2025; Spinal Recovery Center, n.d.)
The best plan depends on the pattern. If numbness is your main symptom, a clinician should check for weakness, reflex changes, and other signs that require faster escalation of care. (AMA, 2024; Mayo Clinic, 2025)
Practical Self-Care Tips for Sciatica Numbness (Simple, Safe, and Nerve-Friendly)
These are general strategies commonly recommended in conservative sciatica care.
Helpful basics
Take walking breaks if walking helps
Avoid long sitting without standing up
Use heat or ice based on what feels better
Don’t force stretches that shoot symptoms into the foot (Mayo Clinic, 2025; HSS, 2022)
If symptoms are not improving—or if weakness is appearing—get reassessed.
Key Takeaways
Sciatica can cause hamstring and foot numbness without back pain, because nerve irritation is often felt along the nerve’s path. (Yale Medicine, n.d.; Penn Medicine, n.d.)
It’s important to tell nerve symptoms apart from a hamstring strain, since numbness/tingling usually points to nerve involvement. (Ducker Physio, 2025)
An integrative chiropractic plan often combines mobility care, soft tissue work, and rehab exercises to reduce irritation and restore movement. (HSS, 2022; Alliance Ortho, 2024; Jimenez, n.d.)
Red flags like weakness or bowel/bladder changes require urgent evaluation. (AMA, 2024; Mayo Clinic, 2025)
If you’re dealing with hamstring or foot numbness—especially if it’s lingering—getting a focused evaluation can help you figure out whether it’s sciatica or something else and build a plan that fits your life in El Paso.
A physiotherapist works on a patient’s foot as part of their neuropathy treatment in the clinic
A Local, Integrative Approach from El Paso Back Clinic
Peripheral neuropathy is a common concern for many people in El Paso. Questions usually center on why symptoms are happening, how diabetes and spine health are connected, and what can be done beyond medication. At El Paso Back Clinic, care focuses on non-invasive, whole-person strategies that improve nerve function, movement, and daily quality of life.
This article answers the most common local questions in clear language and explains how integrative chiropractic care—coordinated with nurse practitioner (NP) oversight—addresses neuropathy by treating both symptoms and root causes. Clinical insights reflect the experience of Dr. Alexander Jimenez, DC, APRN, FNP-BC.
What Is Peripheral Neuropathy?
Peripheral neuropathy happens when nerves outside the brain and spinal cord are damaged or irritated. These nerves help you feel sensation, move muscles, and regulate automatic body functions like sweating and digestion. When nerve signals are disrupted, symptoms can feel burning, sharp, numb, or electric (West Texas Pain Institute, n.d.; Frontier Neurology, n.d.).
Most Common Neuropathy Symptoms We See in El Paso
People in El Paso often describe similar patterns:
Burning or throbbing pain (especially at night)
Tingling or “pins and needles”
Numbness in the feet or hands
Electric or shooting pain
Muscle weakness or cramping
Balance problems or frequent trips
Sensitivity to touch
In more advanced cases, symptoms can involve digestion, bladder control, or sweating (Frontier Neurology, n.d.).
Why Neuropathy Is So Common in This Region
A major driver locally is diabetes and prediabetes. High blood sugar can injure small blood vessels that feed nerves, leading to poor nerve signaling over time.
Other contributors include:
Spine and posture problems that stress nerve roots
Vitamin deficiencies (especially B vitamins)
Circulation issues
Prior injuries or repetitive strain
Certain medications or alcohol overuse
Inflammatory or autoimmune conditions
Many patients have multiple contributing factors, which is why a full evaluation is important (Medicos Family Clinic, n.d.; West Texas Pain Institute, 2023).
How Diabetic Neuropathy Affects Daily Life
Diabetic neuropathy often begins in the feet and slowly progresses upward. Common concerns include:
Burning feet at night
Loss of protective sensation
Higher risk of cuts, sores, and ulcers
Changes in walking or posture
Increased fall risk
Early integrative care can slow progression and reduce complications (El Paso Feet, n.d.; iVascular Center, n.d.).
How Neuropathy Is Evaluated at El Paso Back Clinic
Diagnosis is not based solely on symptoms. A complete assessment looks at the whole person.
Evaluation commonly includes:
Detailed health and symptom history
Review of blood sugar control and medications
Neurological and sensory testing
Posture and movement analysis
Spinal and joint evaluation
Imaging when nerve compression is suspected
Dr. Jimenez emphasizes that neuropathy symptoms often overlap with spinal nerve irritation or biomechanical stress, making dual-scope evaluation especially valuable (Jimenez, n.d.-a; Nonsurgical Spine Center, n.d.).
Can Neuropathy Improve Without Surgery?
For many people, yes. Most patients want conservative options before considering surgery or long-term medication use.
Non-surgical strategies may include:
Chiropractic care
Targeted exercise and physical therapy
Lifestyle and nutrition guidance
Laser therapy
Nerve stimulation techniques
Footwear and balance support
Stress and sleep optimization
Combining approaches is often more effective than relying on just one method (P3 Physical Therapy, n.d.; El Paso Feet, n.d.).
How Chiropractic Care Supports Nerve Health
Chiropractic care focuses on restoring healthy movement in the spine and joints, thereby reducing stress on nerves.
At El Paso Back Clinic, care may include:
Gentle spinal adjustments
Joint mobilization
Postural correction
Nerve decompression strategies
Soft tissue techniques
Guided movement and mobility work
Clinical observations show that improving spinal mechanics can enhance nerve signaling and reduce irritation—especially when neuropathy overlaps with back or neck problems (Jimenez, n.d.-b; El Paso Back Clinic, n.d.).
The Role of Nurse Practitioners in Neuropathy Care
Nurse practitioners (NPs) are essential for addressing medical and metabolic contributors to nerve damage.
NP-guided support may involve:
Lab testing and result interpretation
Diabetes and metabolic management
Identifying vitamin or nutrient deficiencies
Reviewing medication side effects
Monitoring nerve-related complications
Dr. Jimenez’s dual licensure allows structural findings and medical factors to be evaluated together, helping patients understand why symptoms are happening—not just where they hurt (Jimenez, n.d.-c).
Why an Integrative Approach Works Best
Neuropathy rarely has a single cause. Integrative care addresses multiple systems at once.
Benefits include:
More accurate diagnosis
Personalized care plans
Reduced dependence on pain medications
Improved balance, strength, and confidence
Better long-term nerve health
This approach is especially helpful for people with diabetes, chronic back pain, or long-standing symptoms (HealthCoach Clinic, n.d.; Pain and Wellness Institute, n.d.).
Physical Therapy and Movement for Nerve Recovery
Physical therapy complements chiropractic care by retraining safe movement and improving circulation.
Physical therapy may help by:
Strengthening supportive muscles
Improving balance and coordination
Reducing fall risk
Teaching nerve-friendly movement patterns
When coordinated with chiropractic and NP care, recovery is often faster and more sustainable (P3 Physical Therapy, n.d.).
Lifestyle Habits That Matter for Neuropathy
Daily habits can either protect or irritate nerves.
Helpful habits include:
Keeping blood sugar stable
Wearing supportive footwear
Limiting alcohol and avoiding smoking
Staying physically active
Managing stress
Prioritizing sleep
Small, consistent changes can reduce flare-ups and improve comfort over time (Modern Pain Houston, n.d.; Dr. Dennis Harris, n.d.).
Emotional and Community Support
Living with nerve pain can affect mood and sleep. Support makes a difference.
Education and coaching
Stress-management strategies
Peer or virtual support groups
Family involvement in care plans
Support resources help patients feel informed and empowered (Foundation for Peripheral Neuropathy, n.d.).
When to Seek Professional Help
Consider an evaluation if you notice:
Persistent tingling or numbness
Burning or electric pain
Muscle weakness
Balance problems or frequent falls
Foot wounds that heal slowly
Early care can help prevent progression and complications (West Texas Pain Institute, n.d.; Frontier Neurology, n.d.).
The El Paso Back Clinic Difference
At El Paso Back Clinic, neuropathy care is centered on conservative, patient-focused solutions. By combining chiropractic care with nurse practitioner oversight and lifestyle strategies, patients receive practical, non-invasive options designed to improve nerve function and daily life.
Innovations in Sciatica Treatment in 2026: A Shift Toward Targeted, Minimally Invasive, and Integrative Care
Sciatica is one of the most common causes of chronic lower back and leg pain. It occurs when the sciatic nerve—the longest nerve in the body—is irritated or compressed, often due to disc herniation, spinal degeneration, inflammation, or biomechanical imbalance. For years, treatment options focused mainly on pain medications, steroid injections, or surgery when symptoms became severe.
In 2026, sciatica care has entered a new phase. Treatment is no longer just about “blocking pain.” Instead, the focus is on precision diagnosis, nerve healing, inflammation reduction, and functional recovery, with fewer complications and faster healing times. These advances also emphasize integrated, interdisciplinary care, combining chiropractic treatment with the diagnostic and clinical oversight of nurse practitioners (NPs).
This article explains the most important innovations shaping sciatica treatment in 2026, using easy-to-understand language while staying grounded in current clinical research and real-world outcomes.
Understanding Sciatica: Why Better Solutions Were Needed
Sciatica is not a single disease. It is a symptom caused by pressure or irritation along the sciatic nerve, usually beginning in the lower spine and traveling into the buttock and leg. Pain can feel sharp, burning, electric, or aching and may include numbness or weakness.
Common contributors include:
Herniated or bulging lumbar discs
Spinal stenosis
Degenerative disc disease
Muscle imbalance or pelvic instability
Inflammation around nerve roots
Traditional treatments often relied on:
Long-term anti-inflammatory or pain medications
Opioids for severe cases
Epidural steroid injections
Surgery as a last resort
While these approaches helped some patients, they did not always address the underlying cause, and many carried risks such as dependency, complications, or prolonged recovery (Stanford Health Care, n.d.).
What Has Changed in 2026?
By 2026, sciatica treatment emphasizes early, targeted, and minimally invasive care. Research and clinical experience now show that addressing nerve irritation early and restoring healthy movement patterns can prevent chronic pain and disability (BioSpace, 2025).
Key changes include:
Improved imaging and diagnostics
Precision-guided nerve procedures
Regenerative medicine options
Advanced neuromodulation technologies
Integrated chiropractic and NP-led care models
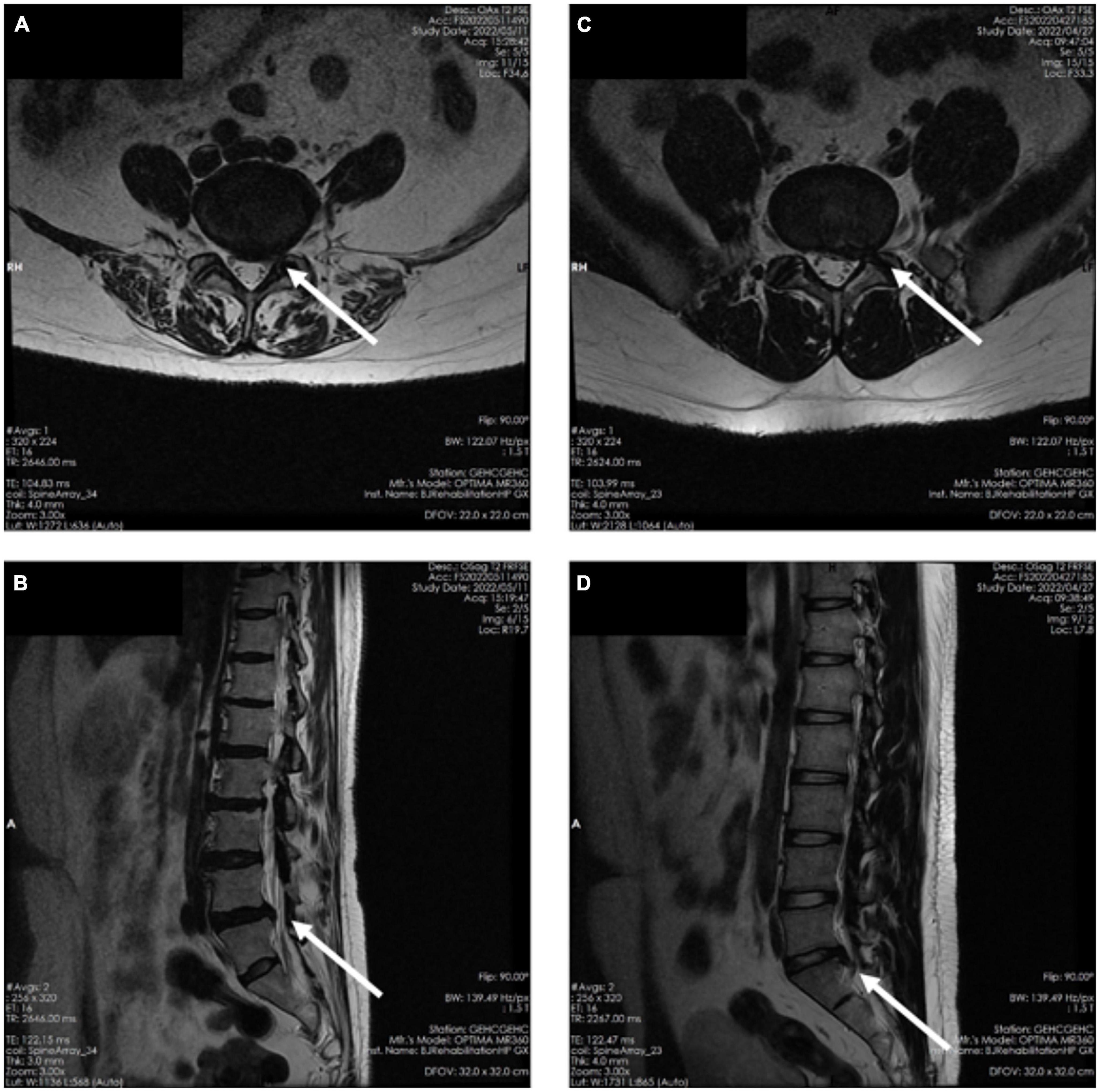
Advanced Diagnostic Imaging: Seeing the True Source of Pain
One of the biggest improvements in sciatica care is high-resolution MRI technology. Modern imaging allows clinicians to:
Identify the exact nerve root involvement
Distinguish disc-related pain from muscular or inflammatory causes
Detect subtle nerve inflammation missed in earlier imaging methods
Enhanced MRI protocols now guide treatment decisions more accurately, reducing unnecessary procedures and improving outcomes (Stanford Health Care, n.d.).
Nurse practitioners play a critical role here by:
Ordering and interpreting imaging
Correlating findings with physical symptoms
Coordinating referrals and follow-up care
Minimally Invasive Pain Procedures: Precision Without Surgery
Improved Nerve Blocks
Modern nerve blocks are no longer “blind injections.” In 2026, they are image-guided and highly targeted, delivering medication exactly where inflammation and irritation occur.
Benefits include:
Faster pain relief
Reduced medication dosage
Improved diagnostic clarity
Lower complication risk
Nerve blocks are now often used as diagnostic tools to help clinicians determine whether pain is mechanical, inflammatory, or neuropathic in origin (Apollo Spine & Pain, 2026a).
Radiofrequency Ablation (RFA)
Radiofrequency ablation uses controlled heat to disrupt pain signals traveling through irritated nerves. Newer RFA systems are more precise and selective than earlier versions.
Key advantages:
Long-lasting pain relief
Minimal tissue damage
Short recovery time
Reduced reliance on medications
RFA is especially helpful for chronic sciatica that does not respond to conservative care (Apollo Spine & Pain, 2026b).
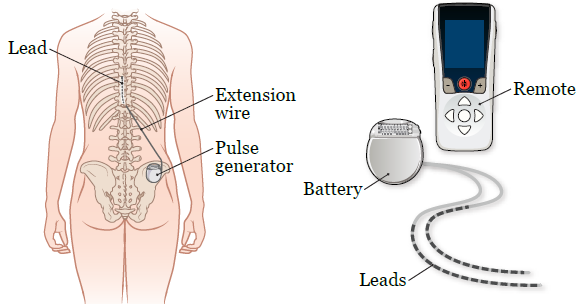
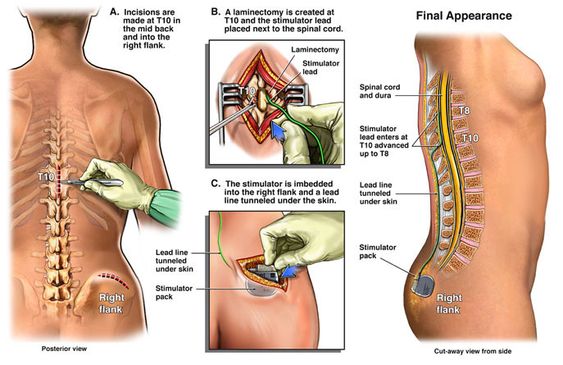
Spinal Cord Stimulation: Rewiring Pain Perception
Spinal cord stimulation (SCS) has evolved significantly. New devices are smaller, smarter, and more adaptive. They deliver gentle electrical signals that change how the brain interprets pain signals from the sciatic nerve.
Modern SCS systems offer:
Personalized stimulation patterns
Adjustable settings via external controllers
Reduced side effects compared to older models
SCS is now used earlier in care for select patients, helping many avoid surgery altogether (Pain and Spine Specialists, n.d.).
Regenerative Medicine: Supporting Nerve Healing
Platelet-Rich Plasma (PRP)
PRP therapy uses a patient’s own blood components to promote healing and reduce inflammation. In sciatica care, PRP is increasingly used around:
Inflamed nerve roots
Degenerative disc structures
Surrounding soft tissues
Research suggests PRP may:
Reduce inflammation
Support tissue repair
Improve long-term outcomes
While still evolving, regenerative therapies are driving growth in the global sciatica treatment market (Grand View Research, n.d.; PMC, 2024).
Therapeutic Exercise Innovations: Movement as Medicine
Nerve Flossing and Targeted Rehab
Exercise therapy in 2026 is more specific and personalized. One standout approach is nerve flossing, which involves controlled movements designed to improve nerve mobility and reduce irritation.
Benefits include:
Improved nerve glide
Reduced stiffness
Decreased pain during daily activities
Programs are now customized using imaging findings and functional testing, ensuring exercises match the patient’s specific condition (Goodman Campbell, 2026).
Chiropractic Care: A Drug-Free Foundation
Chiropractic care remains central to non-surgical sciatica treatment. Modern chiropractic approaches focus on restoring spinal alignment, reducing nerve compression, and improving movement patterns.
Common techniques include:
Spinal adjustments
Flexion-distraction therapy
Soft tissue mobilization
Low-level laser therapy
Research continues to associate chiropractic care with reduced opioid use and improved pain outcomes (ReachMD, 2024; UH Hospitals, 2025).
Integrated Care: Chiropractors and Nurse Practitioners Working Together
One of the most important shifts in 2026 is the collaborative care model. Instead of isolated treatment, patients benefit from coordinated care involving chiropractors and nurse practitioners.
This model allows for:
Accurate diagnosis and imaging oversight
Conservative, drug-free pain management
Monitoring of neurological symptoms
Reduced opioid exposure
Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, highlight that patients receiving coordinated chiropractic and NP care often experience:
Faster recovery
Better functional improvement
Fewer invasive interventions
Greater long-term pain control
His integrative approach emphasizes treating the cause of nerve irritation, not just the symptoms (Jimenez, n.d.).
Why These Innovations Matter
Together, these advances represent a major shift in sciatica care:
From surgery-first to conservative-first
From symptom masking to root-cause resolution
From isolated care to interdisciplinary teamwork
Patients now have more options, fewer risks, and better long-term outcomes.
Conclusion: The Future of Sciatica Care Is Personalized and Precise
By 2026, sciatica treatment has become more effective, safer, and patient-centered. Innovations in diagnostics, minimally invasive procedures, regenerative medicine, and integrative chiropractic-NP–NP care are reducing the need for surgery and long-term medication use.
The focus is no longer just pain relief—it is nerve health, mobility restoration, and sustainable recovery. As research and technology continue to evolve, patients suffering from sciatica can expect even more targeted, evidence-based solutions in the years ahead.
When You Don’t Stretch: Why Muscles Get Stiff, Movement Gets Harder, and Injuries Become More Likely
A patient with chronic back pain does targeted stretches.
If you rarely stretch, your body can start to feel “tight,” which can change how you move. Many people notice they can’t bend, twist, squat, reach overhead, or turn their head as easily as they used to. Over time, this can affect your flexibility, your range of motion (how far a joint can move), and how smooth and efficient your daily movements feel.
At El Paso Back Clinic, Dr. Alexander Jimenez, DC, APRN, FNP-BC, often explains this: when mobility decreases, the body starts to “compensate.” That means you move around a stiff area instead of through it, and those workarounds can build up stress in nearby joints and muscles (Jimenez, n.d.-a). This is one reason people can develop recurring back pain, neck stiffness, hip tightness, or shoulder irritation even without a single big injury.
What “Muscle Stiffness” Really Means
Muscle stiffness usually feels like tightness, soreness, or difficulty moving. It can happen after overuse, after you’ve been still for a long time, or when your muscles stay “stuck” in a more contracted state (Tarantino, 2025). Osmosis
Osmosis notes that stiffness can appear after a long period of minimal motion (such as bed rest or inactivity) or after new exercise that causes temporary muscle cell damage (Tarantino, 2025). Osmosis
Key idea: When your body doesn’t move a joint through its normal range often enough, the muscles and tissues around it can start to feel restricted. That restriction can make normal tasks think harder than they should.
Do Muscles Actually “Shorten” If You Don’t Stretch?
You’ll hear people say, “If you don’t stretch, your muscles will shorten.” That statement is partly true, but it needs context.
Adidas explains that the word “shorten” can be misleading: for most people, it feels like shortening because mobility and flexibility decrease when stretching is skipped, even if the muscle is not literally shrinking in everyday life (Adidas, 2025). adidas
Harvard Health adds an important clarification: without regular stretching, muscles can become tight, and when you need them for activity, they may not extend fully, increasing the risk of joint pain, strains, and muscle damage (Harvard Health Publishing, 2024). Harvard Health
So the practical takeaway is simple:
Skipping stretching often leads to less mobility and flexibility
Tight muscles can reduce how far joints can move
Tight muscles can make injuries more likely when you suddenly “ask more” of your body
How Tight Muscles Reduce Range of Motion
Range of motion (ROM) is the movement around a joint or body part. When ROM is limited, you can’t move that body part through its usual, healthy motion (Jimenez, n.d.-b). El Paso Back Clinic® • 915-850-0900
El Paso Back Clinic explains how tightness—especially in areas like the hips and ankles—can reduce ROM and limit potential for form and strength. When posture and form are compromised, pain and injury risk can rise (Jimenez, n.d.-b). El Paso Back Clinic® • 915-850-0900
What limited ROM can look like in real life
You might notice:
You can’t turn your head fully when driving
You bend from your lower back instead of your hips
You can’t squat without your heels lifting
Your shoulders feel “pinched” when reaching into a cabinet
Your hamstrings feel tight when you try to walk fast
And here’s the tricky part: your body still gets the job done—just with more strain.
Why Stiffness Can Raise Injury Risk
Harvard Health explains that tight muscles may be more easily damaged when they are suddenly stretched during strenuous activity (Harvard Health Publishing, 2024). Harvard Health
That’s why injuries often show up in moments like:
A weekend game after sitting all week
A sudden sprint to catch something
Lifting a heavy box with “cold” hips and hamstrings
A long drive followed by quick unloading or bending
Mayo Clinic also notes that better flexibility can help joints move through full ROM and may decrease injury risk, while emphasizing that stretching must be done correctly (Mayo Clinic Staff, n.d.). Mayo Clinic
Common Reasons People Stop Stretching (And How to Fix Them)
Most people don’t skip stretching because they don’t care. They skip it because it feels confusing, time-consuming, or uncomfortable.
Common barriers
“I don’t have time.”
“Stretching hurts.”
“I’m not flexible, so it doesn’t work for me.”
“I only need stretching if I work out.”
Better, more realistic reframes
You only need 5–10 minutes a few times a week to start seeing benefits (Mayo Clinic Staff, n.d.). Mayo Clinic
Stretching should create tension, not pain (Mayo Clinic Staff, n.d.). Mayo Clinic
Flexibility improves over weeks to months, not days (Harvard Health Publishing, 2024). Harvard Health
Stretching supports everyday movement, not just workouts (Harvard Health Publishing, 2024). Harvard Health
Safe Stretching Basics (So You Don’t Make Things Worse)
This matters: stretching done poorly can backfire.
Mayo Clinic recommends:
Don’t stretch cold muscles—warm up 5–10 minutes first
Don’t bounce
Hold stretches about 30 seconds (longer for problem areas)
Don’t stretch into pain (Mayo Clinic Staff, n.d.). Mayo Clinic
The American Heart Association adds:
Stretch when muscles are warm
Hold 10–30 seconds and repeat 3–5 times
Stretch slowly and smoothly (American Heart Association, 2024). www.heart.org
Quick safety checklist
Warm up first (easy walk, gentle movement)
Move slowly
Breathe
No bouncing
Stop if you feel sharp pain, numbness, or joint pain
A Simple 10-Minute Daily Stretch Routine for Real Life
This is designed for normal adults: busy schedules, stiff hips, tight neck, and lots of sitting.
Step 1: Warm up (1–2 minutes)
Walk around the house
March in place
Gentle arm circles
Step 2: Do these 6 stretches (about 8 minutes total)
1) Hip flexor stretch (1 minute each side) Helps if you sit a lot and feel tight in the front of your hips.
2) Hamstring stretch (1 minute each side) Harvard points out that tight hamstrings from sitting can limit how well you extend your leg and support walking mechanics (Harvard Health Publishing, 2024). Harvard Health
3) Calf stretch (45 seconds each side) Helpful for ankle mobility, walking, and squatting mechanics.
4) Chest opener (45 seconds) Stand in a doorway and gently open the chest to reduce rounded-shoulder posture.
5) Upper back reach (45 seconds) Hug yourself and gently pull your shoulder blades apart.
6) Neck side stretch (30 seconds each side) Gentle only—never crank your neck.
Step 3: Add “micro-mobility” during your day (optional but powerful)
Stand up every hour for 30–60 seconds
Do 5 bodyweight squats to a chair
Do 10 shoulder rolls
Take a 3-minute walk after meals
These small habits often matter as much as one long stretch session.
Stretching After Workouts: What You Should Know
Adidas explains the difference clearly:
Dynamic movement is best before workouts (prepares your body)
Static stretching is typically better after workouts, when you’re warm (Adidas, 2025). adidas
Mayo Clinic also cautions that stretching cold muscles can increase injury risk and notes that some intense activities may not benefit from heavy stretching right before performance (Mayo Clinic Staff, n.d.). Mayo Clinic
A balanced approach
Before exercise: warm up + dynamic mobility
After exercise: gentle static stretching + breathing
On rest days: short, consistent flexibility routine
When Stiffness Is a Sign You Need More Than Stretching
Sometimes the problem is not just “tight muscles.” You may have:
Joint restrictions that block movement
Spine or pelvis alignment issues affecting mechanics
Inflammation around a joint
Pain patterns that keep muscles “guarded”
A nerve-related problem (numbness, tingling, weakness)
El Paso Back Clinic notes that limited ROM in areas like the back, neck, or shoulders can be linked to the body being out of natural alignment, repetitive motions, or wear and tear (Jimenez, n.d.-b). El Paso Back Clinic® • 915-850-0900
If stretching doesn’t help—or makes symptoms worse—it’s smart to get assessed.
The El Paso Back Clinic Approach: Integrative Chiropractic + Nurse Practitioner Support
This is where integrative care can be a game-changer: you’re not only “stretching more,” you’re also finding out why you’re tight and building a plan that fits your body.
What chiropractic care can add
El Paso Back Clinic describes a “restoration” approach that may include:
Soft tissue work (to reduce tightness and improve circulation)
Adjustments (to address misalignments and support mobility)
Nurse practitioners are advanced practice clinicians who assess, diagnose, and treat illnesses and injuries and support chronic condition management (American Nurses Association, n.d.). ANA Healthgrades also describes NPs performing screenings and physical exams, ordering lab work, documenting care, and diagnosing certain conditions (Prosser, 2025). Healthgrades Resources
Why the combo helps stiffness and pain
Together, a chiropractor + NP team can:
Screen for red flags (nerve symptoms, systemic issues)
Decide when imaging or labs are appropriate
Build a movement plan that matches your pain level
Address sleep, stress, inflammation, and recovery habits
Track progress using measurable goals (like ROM improvements)
Dr. Jimenez’s Mobility & Flexibility materials emphasize that “great mobility” supports functional movement without ROM restrictions and that people who don’t stretch often may experience stiffened muscles that reduce effective movement (Jimenez, n.d.-a). El Paso Back Clinic® • 915-850-0900
Red Flags: When to Stop Stretching and Get Checked
Call a clinician promptly if you have:
Numbness, tingling, or weakness in an arm/leg
Loss of balance, clumsiness, or trouble walking
Severe pain that doesn’t improve
Pain after trauma (car accident, fall, sports collision)
Fever, unexplained swelling, or sudden intense stiffness
Muscle stiffness can sometimes be related to underlying medical issues, and diagnosis may require an exam and follow-up testing, depending on the cause (Tarantino, 2025). Osmosis
The Bottom Line
If you don’t stretch regularly, it’s common to feel tighter and less mobile over time. That stiffness can reduce range of motion, make daily tasks harder, and increase your risk of injury when you suddenly push your body. The good news is that you don’t need extreme flexibility. You need consistent, safe mobility work—and when required, professional support to restore movement and reduce pain.
A practical plan usually includes:
Small daily stretching habits
Better warm-ups and recovery routines
Strength + mobility (not stretching alone)
Integrative evaluation when pain, ROM loss, or repeated flare-ups keep returning
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine