Neck injuries are more common than people realize and can lead to mobility issues, affecting the head and shoulders. This is caused by herniated or compressed cervical discs, which can irritate spinal nerve roots. Neck muscles can also be injured, resulting in shoulder pain, stiffness, or headaches. Neck pain is the second most common problem after back pain. Poor posture, phone usage, and computer work can all contribute to neck pain, which can worsen over time if left untreated. Fortunately, therapies are available to gently stretch affected muscles and realign cervical discs, providing relief. Our article discusses how neck pain affects the body, factors related to anterior cervical compression, and how spinal decompression can alleviate neck pain. We work with certified medical providers who use our patients’ valuable information to provide cervical disc treatments for individuals with neck pain affecting their cervical spine and causing mobility issues. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
How Does Neck Pain Affect The Body?
Are you experiencing muscle stiffness between your neck and shoulders? Do you feel discomfort when working for long periods in a hunched position? Or are you suffering from persistent headaches that won’t go away? These symptoms could be caused by neck pain associated with anterior cervical disc compression, a common issue affecting many people. Neck pain is the second most common pain-related problem after low back pain, and it carries corresponding risk profiles that can lead to its development. Research studies revealed that cervical disc herniation associated with neck pain can affect the upper body extremities, ranging from mild to severe symptoms. The spine has three regions: cervical, thoracic, and lumbar, which protect the spinal cord that branches out the nerve roots, allowing mobility and flexibility for the head, neck, and shoulders. When the cervical discs become herniated, they can aggravate the nerve roots, leading to numerous symptoms that can affect the surrounding muscles in the neck and shoulders. Further research studies have revealed that when the cervical intervertebral discs are compressed, they become a common source of neck pain, usually accompanied by neck stiffness and other overlapping risk profiles that can cause referred pain to the upper body extremities. Therefore, neck pain associated with anterior cervical disc compression can become an issue when multiple environmental factors are involved.
Factors Associated With Anterior Cervical Compression To The Neck
Neck pain caused by anterior cervical compression can be due to numerous factors such as poor posture, degenerative disc disease (DDD), spinal stenosis, constantly looking down at a cell phone, being in a hunched or slouched position at work, and repetitive lifting of heavy objects. When individuals engage in repetitive motions that strain the neck, it can result in cervical compression that affects the nerve roots, causing abnormal neuron signals and shoulder or neck pain, according to research studies. This can also lead to overlapping risk profiles, causing referred pain to the upper extremities and somato-visceral pain. Additionally, anterior cervical compression can affect the cardiovascular system, resulting in unwanted symptoms like headaches and neck stiffness, causing significant discomfort.
Chiropractic Recovery Testimony-Video
Are you experiencing frequent headaches or stiffness between your shoulders and neck? Do you feel pain when stretching your neck from side to side? These symptoms may be related to anterior cervical compression in your cervical spine, which can cause herniation of the spinal disc and affect the nerve roots within muscle and tissue fibers. This can lead to referred pain in the neck and shoulder regions. Fortunately, there are various ways to alleviate pain and stiffness in the neck and treat chronic conditions associated with cervical disc herniation. Non-surgical treatments like chiropractic care can relieve neck and shoulder pain caused by cervical disc herniation. Combining non-surgical treatments with other therapies can prevent neck pain from recurring and improve posture. Chiropractic care can also alleviate referred pain caused by neck pain through manual and mechanical manipulation. Check out the video above for more information on non-surgical treatments for cervical disc herniation.
How Spinal Decompression Can Alleviate Neck Pain
Neck pain can be confusing because it can affect the shoulders and chest, leading to referred visceral-somatic pain. Fortunately, many treatments are available to alleviate neck pain and its associated symptoms. According to “The Ultimate Spinal Decompression” by Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., unwanted pressure on the cervical spinal disc can cause damage and ongoing pain by pressing the nerve root. If this happens, some people choose anterior cervical discectomy, which involves a small incision in the neck to remove the damaged disc and relieve pressure on the nerve root. Others opt for spinal decompression if the disc is herniated and aggravates the nerve root in the cervical spine region.
Studies have shown that spinal decompression can help ease neck and shoulder pain by gently stretching the spine through traction. This allows the herniated disc to be pulled back to its original position, relieving pressure on the affected nerve root and muscles. Spinal decompression is a safe and non-invasive treatment option that can be combined with other non-surgical therapies. It is also cost-effective and can benefit individuals who incorporate it into their health and wellness plans.
Conclusion
Neck pain is commonly caused by cervical disc herniation, leading to discomfort in the upper extremities around the neck. Repetitive motions associated with normal activities, such as poor posture, phone usage, and desk work, can also contribute to neck pain. Fortunately, non-surgical treatments like spinal decompression are available. This gentle technique uses traction to stretch the spine and alleviate pain from disc herniation, making it a cost-efficient option. By combining spinal decompression with other therapies, individuals can prevent the recurrence of neck pain and enjoy a pain-free life.
References
Kaplan, E., & Bard, P. (2023). The Ultimate Spinal Decompression. JETLAUNCH.
Shoulder and neck discomfort, pain, and headaches could be caused by vision problems and eye strain that require corrective glasses, contact lenses, or an updated prescription. Spending long periods of activity involving eye usage, like driving, reading/writing reports, studying plans, instructions, reviewing charts, orders, etc., on mobile devices and computer screens fatigues the eyes. Individuals with tired eyes try to reduce eye strain by tilting their head or neck and hunching forward, which results in an unhealthy posture. And for individuals that need glasses squinting and straining the eyes also leads to unhealthy postures, directly contributing to neck and shoulder pain and headaches. Injury Medical Chiropractic and Functional Medicine Clinic can repair and heal musculoskeletal injuries and refer patients to the proper specialist, in this case, an eye care professional.
Vision Problems
Like any muscle, the eyes can be overworked, causing unconscious tensing of the neck, upper back, and shoulder muscles, leading to muscle tension in the back of the skull. The tense muscles can cause blood flow and circulation restriction. Individuals compensate by tilting the head towards one shoulder, craning the neck, or leaning/hunching. This can help for a little while but does not relieve muscle soreness, headaches, or migraines, as well as the throbbing around the temples or the fact that it will keep happening. Individuals learn to live with the pain and push through it. This is unhealthy and can lead to serious, chronic musculoskeletal conditions that can cascade into other health problems. For individuals, the symptoms they are experiencing are common in conditions they may have been previously or currently diagnosed with, including:
Neck Strain
The risk of neck strain or injury comes with the overuse of the neck muscles and tendons.
This results in neck pain, tenderness, and a decreased range of motion.
With vision problems, individuals have additional stress on their neck muscles as they tilt their heads to relieve the discomfort.
Neck Muscle Spasms
When the muscles in the neck involuntarily tighten, it can cause sharp or sudden pain; this is referred to as a muscle spasm.
Individuals can experience muscle spasms for minutes, hours, or even days.
Constantly tilting the head to one side to realign vision can cause overuse and strain on the neck muscles, resulting in muscle spasms.
Torticollis/Wry Neck
With torticollis, individuals will likely have a head tilt and experience neck muscle tenderness, stiffness, and pain.
Chiropractic Treatment
Chiropractors are experts in relieving discomfort symptoms and restoring the neuromusculoskeletal system to optimal function. They help reduce inflammation and muscle spasms through heat, cold, stretches and exercises, and electrical stimulation to expedite healing. They also retrain individuals on posture training eliminating the need to tilt the head and being more aware of body positioning.
As primary care doctors, chiropractors can refer their patients to specialists.
Chiropractors work with a wide range of medical professionals, depending on the needs of their patients.
When neck and shoulder discomfort and headaches become chronic and do not heal or improve, they could be vision problems.
By treating the vision misalignment, pressure can be relieved in the neck and shoulders, reducing and eliminating spasms.
Beyond Medicine
References
Bryans, Roland, et al. “Evidence-based guidelines for the chiropractic treatment of adults with headache.” Journal of manipulative and physiological therapeutics vol. 34,5 (2011): 274-89. doi:10.1016/j.jmpt.2011.04.008
Gowrisankaran, Sowjanya, and James E Sheedy. “Computer vision syndrome: A review.” Work (Reading, Mass.) vol. 52,2 (2015): 303-14. doi:10.3233/WOR-152162
Kaur, Kirandeep, et al. “Digital Eye Strain- A Comprehensive Review.” Ophthalmology and therapy vol. 11,5 (2022): 1655-1680. doi:10.1007/s40123-022-00540-9
Lodin, Camilla, et al. “Eye- and neck/shoulder-discomfort during visually demanding experimental near work.” Work (Reading, Mass.) vol. 41 Suppl 1 (2012): 3388-92. doi:10.3233/WOR-2012-0613-3388
Richter, Hans O. “Neck pain brought into focus.” Work (Reading, Mass.) vol. 47,3 (2014): 413-8. doi:10.3233/WOR-131776
Zetterberg, Camilla et al. “Neck/shoulder discomfort due to visually demanding experimental near work is influenced by previous neck pain, task duration, astigmatism, internal eye discomfort, and accommodation.” PloS one vol. 12,8 e0182439. 23 Aug. 2017, doi:10.1371/journal.pone.0182439
Many individuals are constantly in their vehicles and driving from one place to another in the quickest amount of time. When auto accidents occur, numerous effects can affect many individuals, especially their bodies and mentality. The emotional impact of an auto accident can change a person’s quality of life and take a toll on the person as they become miserable. Then there is the physical side, where the body lunges forward rapidly, causing excruciating pain in the upper and lower portions. The muscles, ligaments, and tissues become overstretched beyond their capacity causing pain-like symptoms to develop and overlap other risk profiles. Today’s article discusses the effects of an auto accident occurs on the body, the symptoms associated with auto accidents, and how treatment like chiropractic care utilizes techniques like the MET technique to assess the body. We provide information about our patients to certified medical providers that offer available therapy techniques like MET (muscle energy techniques) for individuals dealing with back and neck pain associated with auto accidents. We encourage each patient appropriately by referring them to our associated medical providers based on their diagnosis results. We accept that education is a spectacular way when asking our providers the most crucial questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., assesses this information as an educational service. Disclaimer
The Effects Of An Auto Accident On The Body
Have you been dealing with excruciating pain in your neck or back after an automobile collision? Have you noticed any of your muscles feeling stiffed or strained? Or have you been dealing with unwanted pain-like symptoms affecting your daily life? When a person has been through an auto accident, the spine, neck, and back along with their associated muscle groups, are affected by pain. When it comes to the effects of an auto accident on the body, we have to look at how the body reacts when the vehicles collide. Research studies have revealed neck pain is a common complaint to many adults involved in an auto accident. When a person collides with another car, their necks are lunged forward rapidly, causing a whiplash effect on the neck and shoulder muscles. Not only the neck is being affected, but also the back. Additional studies have mentioned that low back pain associated with vehicle collisions can cause the lumbar back muscles to be overstretched and develop non-fatal physical injuries over time, either during or the day after the accident. To that point, it can lead to unwanted symptoms associated with auto accidents and correlate with overlap risk profiles.
Symptoms Associated With Auto Accidents
The symptoms associated with auto accidents affecting neck and back muscles vary depending on the collision’s severity. According to “Clinical Application of Neuromuscular Techniques,” Leon Chaitow, N.D., D.O., and Judith Walker DeLany, L.M.T., stated that when someone suffers from an auto accident, the traumatic forces affect not only the cervical or temporomandibular muscles but also the lumbar muscles. This causes the muscle tissue fibers to be torn and damaged, which causes muscle pain. The book also mentioned that a person injured in a collision could develop nociceptive modulated neck, shoulders, and back muscle dysfunction. To that point, the flexor and extensor muscles are hyperextended, shortened, and strained, which is the result of causing muscle stiffness, pain, and limited range of motion to the neck, shoulder, and back.
Unlocking Pain Relief: How We Assess Motion To Alleviate Pain-Video
Have you been experiencing a limited range of motion to your shoulders, neck, and back? What about feeling muscle stiffness when stretching? Or do you feel muscle tenderness in certain body areas after an auto accident? Many of these pain-like symptoms are associated with auto accidents affecting the neck, shoulders, and back. This causes constant body pain, and many issues develop over time in the various muscle groups. Luckily there are ways to reduce the pain and help restore the body to function. The video above explains how chiropractic care is used to assess the body through spinal manipulation. Chiropractic care uses various techniques to help with spinal subluxation and loosen up stiff, tight muscles to help relax and restore each muscle group while relieving unwanted pain from the muscle tissues and ligaments.
Chiropractic Care & The MET Technique Assessing The Body
Studies reveal that auto accidents are a major cause of spinal and muscle injuries treated by chiropractic care. When a person suffers after an auto accident, they will experience pain all over their bodies and try to find ways to relieve the pain affecting their daily lives through treatment. One of the treatments that can help reduce pain and restore the body is chiropractic care. When chiropractors are treating the body to reduce pain, they use various techniques like the MET technique (muscle energy technique) to stretch and strengthen soft tissue and use manual manipulation to realign the spine, work out the tight muscles, nerves, and ligaments to prevent further damage on the body while getting the affected individuals back to shape. Chiropractic care also has a close relationship with other treatments like physical therapy to help strengthen the muscles in the body and help many people be aware of how their bodies function.
Conclusion
Overall, when a person has experience pain in their back, neck, and shoulder muscles from an auto accident, it can affect their emotional and physical well-being. The effects of an auto accident cause unwanted pain symptoms to develop and correlate with nociceptive modulated dysfunction. To that point, it can cause issues like muscle stiffness and tenderness in the affected areas. Fortunately, treatments like chiropractic care allow the body to be restored through manual manipulation and the MET technique to gently stretch the soft tissues and muscles and realign the body back to functioning. Incorporating chiropractic care with the MET technique, the body will experience relief, and the host can be pain-free.
References
Chaitow, Leon, and Judith Walker DeLany. Clinical Application of Neuromuscular Techniques. Churchill Livingstone, 2002.
Dies, Stephen, and J Walter Strapp. “Chiropractic Treatment of Patients in Motor Vehicle Accidents: A Statistical Analysis.” The Journal of the Canadian Chiropractic Association, U.S. National Library of Medicine, Sept. 1992, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2484939/.
Fewster, Kayla M, et al. “Low-Velocity Motor Vehicle Collision Characteristics Associated with Claimed Low Back Pain.” Traffic Injury Prevention, U.S. National Library of Medicine, 10 May 2019, https://pubmed.ncbi.nlm.nih.gov/31074647/.
Vos, Cees J, et al. “Impact of Motor Vehicle Accidents on Neck Pain and Disability in General Practice.” The British Journal of General Practice : the Journal of the Royal College of General Practitioners, U.S. National Library of Medicine, Sept. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2529200/.
Bruxism is an abnormal jaw clenching or grinding of the teeth, either while awake or during sleep. This can cause neck and shoulder tension caused by excess pressure on the neck and jaw muscles. Individuals may not realize they have bruxism until a dentist notices excess wear and tear or a chiropractor examines their symptoms. Bruxism can play a role in temporomandibular disorders. Doctors and dentists agree that factors like stress increase the likelihood of jaw clenching. Dentists usually recommend a mouth guard to prevent grinding. Chiropractic care, massage, and decompression therapy can relieve symptoms, release and relax the muscles, realign the spine, and restore function.
Bruxism
There is awake bruxism and sleep bruxism. A tight jaw generates tension extending to the neck, shoulder, and upper back muscles. Over time, that excess strain irritates the joints, causing inflammation. Jaw clenching and teeth grinding can lead to health issues like damaged teeth, neck, shoulder, and upper back pain symptoms, and tension headaches.
Symptoms
Signs and symptoms can include:
Face, jaw, neck, and upper back aches, tightness, and soreness.
Tired or tight jaw muscles.
Headaches that start in the temples.
What feels like earache pain symptoms.
Damage from clenching on the inside of the cheek.
Increased tooth sensitivity.
Teeth that are loose, flattened, chipped, or fractured.
Sleep problems.
Risk Factors
Emotional tension – Stress, anxiety, frustration, and anger.
An unhealthy lifestyle – smoking, excess drinking, caffeine, etc., disrupts brain and cardiovascular functions.
Medications
Chiropractic Care for Jaw Clenching
If there is a jaw clenching or grinding issue, it is recommended to see a dentist for a professional diagnosis. Then a chiropractor can develop a personalized treatment plan that utilizes massage and decompression therapy to re-position the jaw, stretch, release and relax the muscles. They will recommend exercises to strengthen and maintain the relaxed jaw muscles and awareness exercises to help identify triggers and prevent clenching.
Jaw Exercises
References
Capellini, Verena Kise, et al. “Massage therapy in managing myogenic TMD: a pilot study.” Journal of applied oral science: Revista FOB vol. 14,1 (2006): 21-6. doi:10.1590/s1678-77572006000100005
Kuhn, Monika, and Jens Christoph Türp. “Risk factors for bruxism.” Swiss dental journal vol. 128,2 (2018): 118-124.
Nishida, Norihiro et al. “Stress analysis of the cervical spinal cord: Impact of the morphology of spinal cord segments on stress.” The journal of spinal cord medicine vol. 39,3 (2016): 327-34. doi:10.1179/2045772315Y.0000000012
Ohayon, M M et al. “Risk factors for sleep bruxism in the general population.” Chest vol. 119,1 (2001): 53-61. doi:10.1378/chest.119.1.53
Santos Miotto Amorim, Cinthia, et al. “Effectiveness of two physical therapy interventions, relative to dental treatment in individuals with bruxism: study protocol of a randomized clinical trial.” Trials vol. 15 8. 7 Jan. 2014, doi:10.1186/1745-6215-15-8
Neck aches, soreness, and pain symptoms are not always neck-related. Tight thoracic or mid-back muscles can pull on the neck muscles causing various symptoms. Upper back tightness occurs anywhere from the neck’s base to the bottom of the rib cage. The bones in the upper area don’t move or flex as much as the neck and low back. This can lead individuals to believe there is nothing wrong with the mid-back, as there are no pain symptoms or signs of discomfort. However, individuals don’t realize how tight the muscles are, which can go on for years, causing neck issues. Injury Medical Chiropractic and Functional Medicine Clinic can relieve symptoms, release, and relax tight muscles, increase circulation, and restore optimal function.
Mid-Back Muscle Tightness
The upper and middle back is the thoracic spine. The thoracic spine has twelve small bones called vertebrae. Each vertebra on the thoracic spine is connected to a pair of ribs. The ribs wrap around the body and attach to a long, flat sternum bone. This forms the rib cage. The bones in the upper back work with the ribs to stabilize the back and protect vital organs, including the heart and lungs. The tightening and pulling eventually cause neck aches that can come out of nowhere; even when not moving and looking straight ahead, there can be persistent dull achiness or stinging sensations.
Causes
Unhealthy posture, disc problems, injuries, fractures, or other issues or conditions can cause mid-back muscle tightness.
Posture
Constant sitting or standing combined with unhealthy posture and being hunched over can cause the muscles to tighten, limiting mobility.
Holding Onto Stress
Chronic stress can cause muscle tightening, whether it is in the low back, mid-back, neck, or elsewhere.
Hereditary
Individual genetic makeup may make the body more susceptible to muscle tightness.
For example, individuals with a lot of muscle tone vs. individuals with less muscle tone may experience muscle tightness more often.
Adequate Hydration
Being properly hydrated is important for muscle and joint lubrication.
Water provides nutrients to contracting muscles.
This keeps the body loose and ready for movement.
Muscle Imbalance and Underlying Weakness
Individuals that tend to work one side of the body more than the other or have repeatedly been moving in a certain way for years can cause muscle imbalances and trigger points to develop.
If muscle tightness continues, even after stretching, it could be an underlying weakness.
The muscles can sometimes seize up and guard, so they feel tight when they have become chronically weak and not strong enough to meet the physical demands.
Chiropractic Care
Chiropractic care involves various therapies to address the root cause fully and relieve neck aches. These include:
Massage therapies to break up compacted muscle tissue.
Remove trigger points.
Relax the muscles to a pliable state.
Perform chiropractic adjustments to realign the spine.
Stretching and strengthening.
Posture training that includes stretches/exercises.
Nutritional plans to help strengthen muscles.
Thoracic Tension Release
References
Gatt, Adrianna, et al. “Anatomy, Fascia Layers.” StatPearls, StatPearls Publishing, Jul 25, 2022.
Liebsch, Christian, and Hans-Joachim Wilke. “How Does the Rib Cage Affect the Biomechanical Properties of the Thoracic Spine? A Systematic Literature Review.” Frontiers in bioengineering and biotechnology vol. 10 904539. Jun 15, 2022, doi:10.3389/fbioe.2022.904539
Maciejewska-Skrendo, Agnieszka et al. “Genetics of Muscle Stiffness, Muscle Elasticity and Explosive Strength.” Journal of human kinetics vol. 74 143-159. 31 Aug. 2020, doi:10.2478/hukin-2020-0027
Modes RJ, Lafci Fahrioglu S. Anatomy, Back. [Updated 2022 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539746/
Page, Phil. “Current concepts in muscle stretching for exercise and rehabilitation.” International journal of sports physical therapy vol. 7,1 (2012): 109-19.
Petrofsky, Jerrold et al. “The Efficacy of Sustained Heat Treatment on Delayed-Onset Muscle Soreness.” Clinical journal of sports medicine: official journal of the Canadian Academy of Sports Medicine vol. 27,4 (2017): 329-337. doi:10.1097/JSM.0000000000000375
The body is a functional machine that requires many muscles, organs, ligaments, joints, and tissues that provide everyday movements. In the upper extremities, the head, neck, and shoulders have many muscles, ligaments, and tissues that work together with the nerve roots from the nervous system that provides sensory-motor function to make the fingers move, the shoulders rotate, and the head turns from side to side. When injuries or common issues affect the muscles in the head, neck, or shoulders, it can cause small nodules to form along the muscle fibers of the affected muscle area and cause referred pain in different locations of the body. Today’s article looks at the scalene muscles, how trigger points affect the scalene muscles while mimicking shoulder pain, and how to manage chronic pain associated with trigger points. We refer patients to certified providers who specialize in musculoskeletal treatments to aid individuals suffering from trigger points related to the shoulders affecting the scalene muscles. We also guide our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure to find that education is the solution to asking our providers insightful questions. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
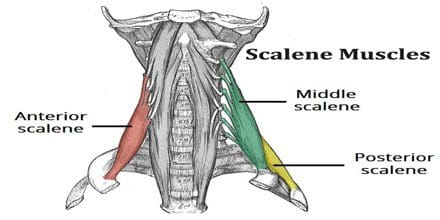
What Are The Scalene Muscles?
Have you been experiencing tingling sensations running down your fingertips? Do you feel stiffness when rotating your neck or shoulders? Or do you feel muscle soreness in your shoulders? Many individuals who are feeling any of these symptoms affecting their neck or shoulders could be dealing with trigger point pain along the scalene muscles. The scalene muscles play a crucial part in the head and neck as they are deep muscles positioned laterally on the cervical tract of the spine. These muscles have three different branches: the anterior, medius, and posterior, which play the role of being accessory breathing muscles while being an important contributor to head and neck movement. To that point, it allows stability to the cervical spine. The scalene muscles even help support and elevate the upper rib cage when a person is lifting, pulling, or carrying heavy objects. However, like most muscles in the body, the scalene muscles can be prone to injury and can develop issues that can affect the upper extremities of the body.
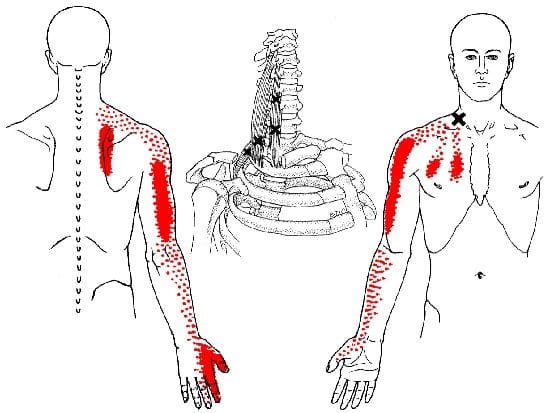
Trigger Points Affects The Scalene Muscles Mimicking Shoulder Pain
When common injuries like pulling a muscle when carrying a heavy object or even a traumatic injury like being involved in an auto accident can cause pain in the affected area, over time, if not treated, can cause various symptoms to overlap and affect the muscles. When the scalene muscles are affected by injuries, they can develop tiny nodules along the taut muscle fibers and become hyperirritable to the surrounding areas of the upper half of the body. This is known as trigger point pain and can mimic other chronic issues that affect different body areas. To that point, trigger points affecting the scalene muscles may mimic shoulder pain in the upper half of the body. Studies reveal that scalene myofascial pain is a regional pain syndrome that originates pain in the neck area and radiates pain down to the arm. Since trigger points mimic other chronic issues, it is often misdiagnosed as another neck pain associated with radiculopathy when the scalene muscles are affected. When this happens, the muscles become stiff and weak, causing a reduction in the range of movement.
Studies reveal that when individuals suffer from acute whiplash-associated disorders, the local and referred pain can be elicited from active trigger points to reproduce neck and shoulder pain. This causes a higher disability that exhibits widespread pressure causing the muscles to be hypersensitive and reducing the cervical range of motion. Many individuals often complain about shoulder pain while rubbing the upper parts of their arms. The scalene muscle is affected by active trigger points, thus mimicking shoulder pain.
Scalenes Trigger Points-Video
Have you been feeling muscle stiffness in your neck or shoulders? Have you been experiencing a numbing sensation along your arms? Have you felt tenderness along your shoulders when you touch them? Many of these pain symptoms are associated with trigger points along the scalene muscles. The video above explains where the trigger points are located along the scalene muscles and how they are causing referred pain in the neck and shoulder areas. Many factors can lead to the causation of trigger point pain and overlap with other chronic issues that can affect the upper extremities of the body, using sleep as an example. Studies reveal that poor sleeping posture can affect the neck and shoulders, leading to muscle stiffness along the scalene muscles and developing trigger points over time. Fortunately, various ways to manage referred shoulder pain are associated with trigger points.
Management Of Chronic Shoulder Pain Associated With Trigger Points
Many individuals are referred to pain specialists that can alleviate trigger points along the scalene muscle to reduce the effects of shoulder and neck pain. When referred pain along the scalene muscles causes chronic shoulder pain associated with trigger points, many people often do various movements to alleviate the pain. However, it can cause more pain in the affected area and prevent relief from the neck and shoulders. Studies reveal that various treatments like physiotherapy, trigger point injections, manipulation of the cervical spine, or acupuncture can help relax and lengthen the muscle fibers associated with the scalene muscle. To that point, this allows the neck to extend further without pain and reduces the overlapping symptoms that affect the upper extremities of the body.
Conclusion
The scalene muscles play a crucial part in the head and neck area as deep muscles are positioned laterally on the cervical tract of the spine. These muscles help elevate the upper chest and laterally bend the neck from side to side. When injuries affect the scalene muscles and form tiny nodules known as trigger points, it can cause referred pain to the shoulders and the neck. To that point, symptoms like numbing or tingling sensations can travel down the arms and fingers. Fortunately, available treatments can reduce the symptoms and manage myofascial trigger pain along the shoulders and neck associated with the scalene muscles. This allows a better range of motion to the neck and shoulder and prevents future trigger points from forming in the scalene muscles.
References
Abd Jalil, Nizar, et al. “Scalene Myofascial Pain Syndrome Mimicking Cervical Disc Prolapse: A Report of Two Cases.” The Malaysian Journal of Medical Sciences : MJMS, Penerbit Universiti Sains Malaysia, Jan. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3216145/.
Bordoni, Bruno, and Matthew Varacallo. “Anatomy, Head and Neck, Scalenus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 16 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK519058/.
Fernández-Pérez, Antonio Manuel, et al. “Muscle Trigger Points, Pressure Pain Threshold, and Cervical Range of Motion in Patients with High Level of Disability Related to Acute Whiplash Injury.” The Journal of Orthopaedic and Sports Physical Therapy, U.S. National Library of Medicine, July 2012, https://pubmed.ncbi.nlm.nih.gov/22677576/.
Lee, Won-Hwee, and Min-Seok Ko. “Effect of Sleep Posture on Neck Muscle Activity.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, June 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5468189/.
Thapa, Deepak, et al. “Management of Chronic Shoulder Pain with Restricted Mobility – a Case Series.” Indian Journal of Anaesthesia, Medknow Publications & Media Pvt Ltd, Nov. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5125193/.
The muscles in the body help provide motion and protect the skeletal joints from harm. Each muscle group has ligaments, tissues, and muscle fibers that retract, stretch, and contract the body while helping the host to do everyday movements, breath, digest food, stabilize, and even rest. When a person is dealing with pain from a traumatic event or making repetitive motions, it can affect the muscles over time. Factors like not drinking enough water, constantly looking down on the phones, and being hunched over can cause strain on the muscles, causing overlapping pain on top of other chronic issues that may develop. When the muscles begin to cause pain along the shoulders and neck, it can become a risk of developing trigger points in the levator scapulae muscles. Today’s article examines the levator scapulae muscles, how trigger points affect these muscles, and how treatments can help manage the trigger points on the levator scapulae muscles. We refer patients to certified providers who specialize in musculoskeletal treatments to aid individuals suffering from trigger points associated with the neck and shoulders affecting the levator scapulae muscles. We also guide our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure to find that education is the solution to asking our providers insightful questions. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
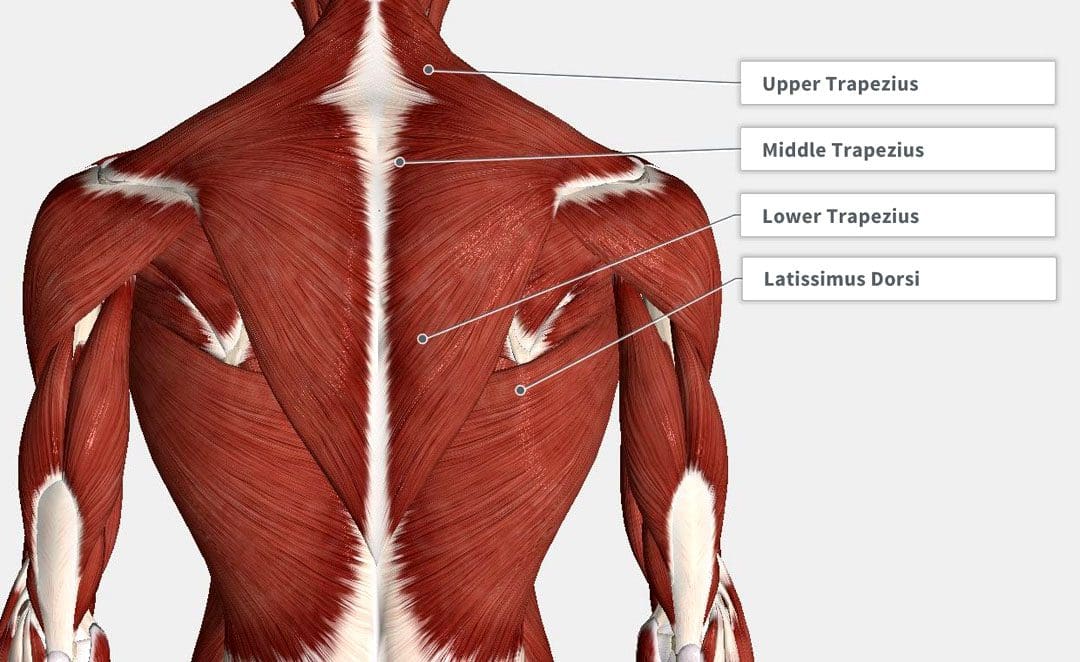
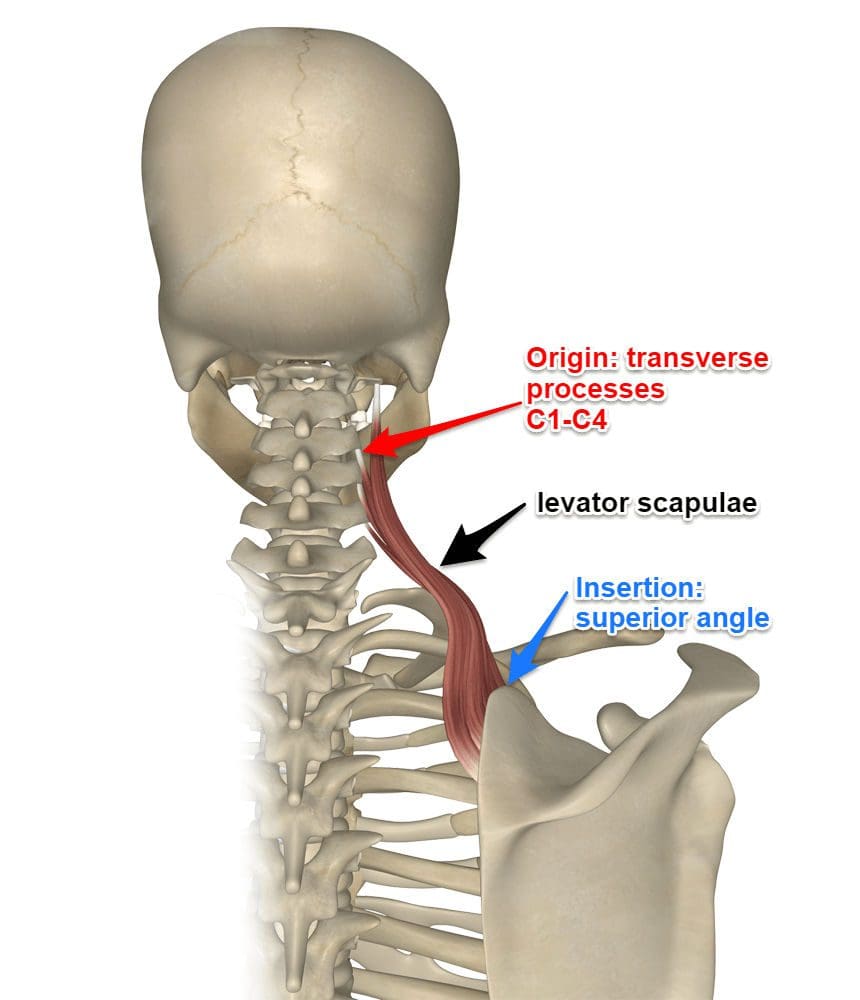
What Is The Levator Scapulae?
Have you been dealing with pain along the neck or shoulders? Do you feel stiffness when turning your head from side to side? Or do you feel tenderness in the base of your neck and shoulders? Many individuals with shoulder and neck pain risk developing trigger points along the levator scapulae. The levator scapulae muscles originate from the posterior tubercles of the C1 through C4 vertebrae in the neck that is between the superior angle and the root of the scapulae spine. This superficial muscle’s primary function is to elevate the scapulae or the shoulder blades while working together with the trapezius and rhomboid muscles to assist the movement. The levator scapulae muscles also assist in providing neck extension, ipsilateral rotation, and lateral flexion. When pathologies like fibromyalgia, levator scapulae syndrome, or cervical myofascial pain begin to affect the levator scapulae muscles, the symptoms can potentially involve the shoulders and neck to cause referred pain to the upper extremities.
How Trigger Points Affect The Levator Scapulae?
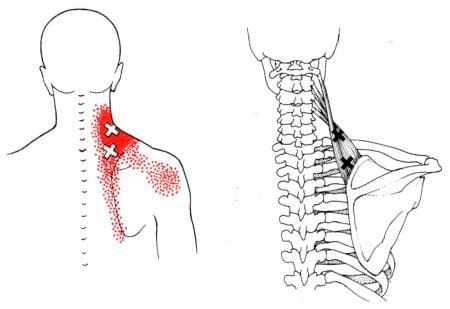
Many individuals with shoulder and neck pain have described radiating pain from their neck to their shoulders. Known as referred pain, the pain is located in one area of the body but in a different location. Studies reveal that when pain radiates from the neck and shoulders, any movements that are overstretching the levator scapulae can aggravate overlapping symptoms on the affected side. This allows small nodules to form along the levator scapulae muscle fibers, causing trigger points to affect the shoulder and neck muscles.
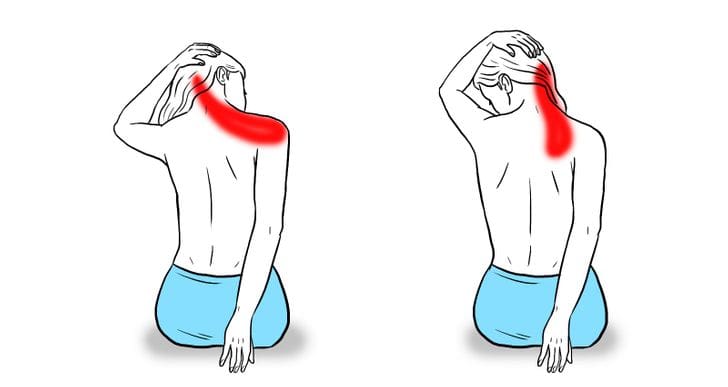
Trigger point associated with the levator scapulae muscles causes the individual to have pain-like symptoms in the neck that causes muscle stiffness. This causes an emphasis on referred pain symptoms from the levator scapulae, like neck tension and restriction of range of motion on the neck. Studies reveal that pain over the superior angle of the levator scapulae is a common musculoskeletal disorder that is often accompanied by radiating pain on the neck, head, and shoulders. Some of the ways that trigger points form along the levator scapulae muscle can be due to ordinary factors like:
Stress
Posture
Over-exercising
Upper respiratory infections
Some of these factors above can shorten the levator scapulae muscle and restrict muscle movement to provide a full range of motion for the head and neck to turn. To that point, treatments are available to help loosen up and stretch the levator scapulae muscles to allow rotation and flexion on the neck and shoulders.
Trigger Points Anatomy On The Levator Scapulae- Video
Have you been dealing with stress that is affecting your neck and shoulders? Have you been dealing with neck stiffness when turning your head? Or have you been feeling muscle tenderness between the neck and shoulders? Some of these symptoms are associated with trigger points affecting the levator scapulae muscles between the neck and shoulder. The video above overviews common trigger points and how they affect the levator scapulae, causing shoulder and neck pain. Since the levator scapulae muscles lay behind the trapezius muscle, studies reveal that trigger points or myofascial pain syndrome can cause hyperirritability in the muscle tissues and affect mobility functions in the nerve ends. Even though referred pain affects the neck and shoulder of the body, treatments are available to manage trigger points on the levator scapulae and relieve neck and shoulder pain.
Treatments To Manage Trigger Points On The Levator Scapulae
When there is trigger point pain affecting the levator scapulae, some common complaints that many individuals often complain about are neck and shoulder pain. However, various ways can alleviate the pain symptoms from the neck and shoulders while managing trigger points associated with the levator scapulae. Studies reveal that stretching the levator scapulae muscle in a seated position can improve muscle length along the levator scapulae and the cervical range of motion. Stretching the levator scapulae muscle can help reduce the pain along the levator muscle. To that point, it even helps reduce muscle imbalances and movement dysfunction along the cervical joints. Many individuals are referred to pain specialists like chiropractors by their doctors to reduce pain and functionality disability in the neck and realign the spine to loosen up the stiff muscles caused by subluxation. Realigning the cervical spine and stretching can reduce future trigger points and reduce pain symptoms from affecting the muscle.
Conclusion
The levator scapulae muscles in the body provide movement functionality to the neck and shoulders. The levator scapulae work together with the trapezius and rhomboid muscles to elevate the shoulder blades and assist with neck extension, ipsilateral rotation, and lateral flexion. When pathologies affect the levator scapulae muscles, they can develop trigger point pain along the muscle and cause neck and shoulder pain. The factors that cause trigger point pain can either be ordinary or traumatic and cause referred pain to the neck and shoulders. Fortunately, treatments like stretching and adjustments can help reduce the pain and loosen up stiff muscles along the levator scapulae. This will allow a cervical range of motion back to the neck and shoulder and elongate the levator scapulae.
References
Akamatsu, Flávia Emi, et al. “Trigger Points: An Anatomical Substratum.” BioMed Research International, Hindawi Publishing Corporation, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4355109/.
Henry, James P, and Sunil Munakomi. “Anatomy, Head and Neck, Levator Scapulae Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 13 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK553120/.
Jeong , Hyo-Jung, et al. “Stretching Position Can Affect Levator Scapular Muscle Activity, Length, and Cervical Range of Motion in People with a Shortened Levator Scapulae.” Physical Therapy in Sport : Official Journal of the Association of Chartered Physiotherapists in Sports Medicine, U.S. National Library of Medicine, 4 Apr. 2017, https://pubmed.ncbi.nlm.nih.gov/28578252/.
Kulow, Charlotte, et al. “Levator Scapulae and Rhomboid Minor Are United.” Annals of Anatomy = Anatomischer Anzeiger : Official Organ of the Anatomische Gesellschaft, U.S. National Library of Medicine, Aug. 2022, https://pubmed.ncbi.nlm.nih.gov/35367623/.
Menachen, A, et al. “Levator Scapulae Syndrome: An Anatomic-Clinical Study.” Bulletin (Hospital for Joint Diseases (New York, N.Y.)), U.S. National Library of Medicine, 1993, https://pubmed.ncbi.nlm.nih.gov/8374486/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine