We are familiar with neck stiffness or a crick. This can prevent us from comfortably moving the head all around. A crick can cause the spine, and shoulders to feel rigid and stressed from not being able to turn around and could cause an upper or low-back strain from having to turn the whole body to look back or even just to the side. Chiropractic treatment is available and will help, along with some self-care therapies that can be done at home.
Crick in the Neck vs. Neck Stiffness
A crick in the neck is the same as a stiff neck. It develops when the neck muscles, tendons, and ligaments become strained/sprained. Most strains and sprains are minor but do cause inflammation/swelling of the neck�s soft tissues, which results in stiffness and, at times muscle spasms.
The symptoms
Cricks in the neck are uncomfortable, but not necessarily painful. If there is a pre-existing neck condition or injuries like whiplash the crick and stiffness could increase the uncomfortableness and generate pain.
The most common symptoms include:
Neck stiffness
Muscle stiffness
Reduced mobility affecting the neck�s range of motion
A popping sensation when trying to turn or tilt the head
Causes of a stiff neck or crick
There are different causes of neck stiffness. It can be a combination of things you can control and some you can�t.
Possible causes that you can control:
Poor posture working either sitting or standing for several hours without breaks or stretching.
Sleeping in a position that puts the neck in an awkward position or using a pillow that does not support the neck when sleeping.
Constantly looking down at a cell phone or tablet.
Stress and emotional tension can cause involuntarily tightening of the neck muscles and shoulders.
Heavy labor along with incorrect lifting techniques.
Reaching or having to look up/overhead for several hours like when painting a ceiling.
Possible causes that are out of your control:
Whiplash injury
Sports-injuries like a football stinger
Aging muscles and bones
Around 13% of cases the stiffness, and pain are caused by separate cervical spinal conditions, like:
Cold therapy reduces the swelling of soft tissues, like muscles and ligaments, while heat soothes the tightness by boosting blood circulation to the affected area. There are different products available that can deliver cold or heat to the neck and upper back.
Apply ice for 15 minutes each hour.
Apply heat therapy like a heating pad for 15 minutes every 2 or 3 hours.
Over-the-counter anti-inflammation medicines
Non-steroidal anti-inflammatory medications like ibuprofen and naproxen can help relieve inflammation and pain.
Because neck stiffness can be linked to lifestyle choices, individuals may find that they occur repeatedly. Simple neck stretches, chiropractic treatment, using a supportive pillow, and taking frequent breaks at your job can help prevent neck stiffness and keep you moving. These professionals have undergone extensive training in their field and are capable of treating neck pain effectively. So if you or a loved one are experiencing neck pain, give us a call. We�re ready to help!
Neck pain prevention can go a long way as long as you take proper care of your body, exercise, and practice healthy habits. Here are a few tips to help prevent neck pain before it begins. Neck mobility is a marvelous thing. The neck can move the head in various directions:
90� of flexion forward motion
90� of extension backward motion
180� of rotation side to side
Almost 120� of tilt to each shoulder
A lot of us are very familiar with a stiff neck or a crick in the neck. This stiffness prevents us from moving comfortably. A crick in the neck can cause the neck part of the spine to feel stiff, rigid and immobile. Fortunately, prevention and various treatments can help.
Prevention:
Standing and sitting properly maintains proper posture and keeps muscles working/healthy. If you begin to hunch over, correct it immediately as it can quickly lead to pain in the neck. Pay attention to how you stand and sit and the more you do this it will become a healthy habit.
Do neck and body exercises regularly and try for a 30-minute cardio workout 3-5 times week.
Staying within a healthy weight-range will keep your spine in top form as it carries the weight of your body, and not overstrain it, which can lead to all kinds of pain.
With healthy weight comes a healthy meal plan, not just for proper weight but to strengthen muscles, bones, enriching the blood and getting to optimal health.
Smoking can affect the bones and muscles in your cervical/neck area of the spine, as well as all the other areas of the body. Therefore it is time to quit.
Sleep with correct head and neck posture. Sleeping with your head in an awkward position is an easy set-up for a strain and pain.
Stress and tension reduction.�Tense muscles in the neck and shoulder often lead to pain in the neck. A few effective ways to reduce stress can be writing, talking to friends, exercising, walking, listening/playing music, art/crafts, cooking, reading,� and turn to these when the stress begins to build.
Driving safely and wearing seat belts can help prevent whiplash.
Using the proper equipment to protect your neck while participating in sports that can lead to neck injuries like football, skateboarding, wrestling, soccer is a must.
Taking care of your body is a complex process. Lifestyle changes pave the way to wellness and making these changes will benefit more than just the neck.
Don’t worry about the list and try to check everything off. Look at the things that apply to you and try to implement a few of these tips one at a time. Keep the bigger changes like quitting smoking/losing weight in the foreseeable future. It takes time, patience and commitment. With a little hard work, it will pay off, and you should have a healthier life with less neck pain episodes and remember prevention is key.
Massage
This is a popular therapy that relieves:
Aches
Fluid retention
Inflammation
Muscle tension
Pain
Spasms
Stiffness
Other benefits include improved blood and lymph circulation, flexibility, range of motion, and increased tissue elasticity.While increasing circulation the muscles are warmed along with other soft tissues like tendons and ligaments.
Swedish
It is one of the most popular massage types in the US. Usually, therapeutic muscle lotion or oil is used to reduce friction and relax the area/muscles as the therapist performs light stroking in one direction with deep pressure in another to relax and loosen the muscles and surrounding ligaments/tissues.
This takes the blood flow and flushes lactic acid, uric acid, and other waste products from the muscles. The ligaments and tendons get stretched, which increases their soft but firm/strong feel. The nerves are stimulated and relaxed, with any stress in the muscles taken away. Relaxing the muscles is the overall goal.
Deep Tissue
This technique aims at chronic muscle tension. The strokes are slower, using more intense direct pressure to release the built-up stress, knots, and tightness. Depending on how deep the muscle and tissue stress maybe, the therapist will adjust their hand positions, strokes, and intensity periodically to work the tissues releasing tension.
Relaxing the Muscles
The therapist using their hands or tools to rhythmically knead, rub, and stroke muscles, circulation begins muscle stimulation. This blood flow brings needed oxygen and nutrients and helps the muscles eliminate waste products, like lactic acid, that can collect in the muscles brought on by spasms, which cause pain.
El Paso, TX Neck Pain Chiropractic Treatment
NCBI Resources
Individuals with chronic neck pain that don�t seem to have a cause, could be trigger points. A doctor will refer you to a�physical therapist, chiropractor or another spine specialist�to conduct an examination for trigger points.
There are different types of topical medications, different ways of delivery and are available for patients with back and neck pain. A physician may combine one or more types of medication for maximum relief or as a way of�limiting the side effects of larger doses of only one medication. Strong dose compounds and controlled drugs are�only�available with a doctor’s prescription.
Medicines with a low potency and low risk of side effects are available at stores and local pharmacies over-the-counter. But remember medications sold over the counter without a prescription doesn’t mean they are safe to use as much as possible. Please read the label and follow the instructions. Taking higher doses, even acetaminophen e.g. Tylenol can cause liver damage. Discussing these medications with a doctor or pharmacist before purchase would be wise. Your physician should know if you plan to continue using over-the-counter medications.
Medicines with a low potency and low risk of side effects are available at stores and local pharmacies over-the-counter. But remember medications sold over the counter without a prescription doesn’t mean they are safe to use as much as possible. Please read the label and follow the instructions. Taking higher doses, even acetaminophen e.g. Tylenol can cause liver damage. Discussing these medications with a doctor or pharmacist before purchase would be wise. Your physician should know if you plan to continue using over-the-counter medications.
Inform your physician about all the products you take including herbal remedies to decrease the risk of side effects or potential severe drug interactions. When acute pain is present, injections either intravenous or intramuscular injected into the muscles are used. For chronic pain, medications are used and are typically in pill form. Both methods have limitations and different�delivery�approaches may be considered. This includes inhalation or topical on top of the skin applications.
Topical Pain Alleviators
These type of medications come prepared and are applied to the skin via:
Topical medications aim to reduce inflammation and soothe nerve and muscle pain. Some are available with a doctor’s prescription and others are over-the-counter. Medication administered�through the skin is becoming more popular.
Skin Cells
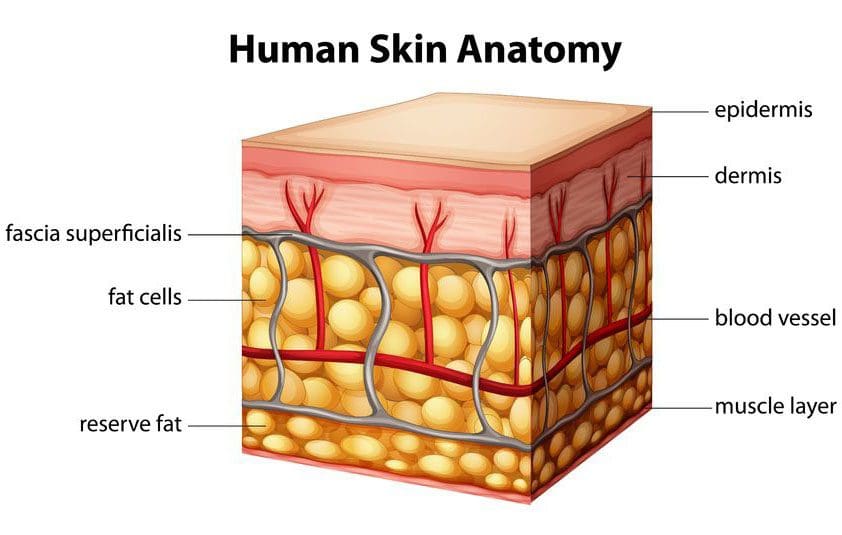
The skin is the largest organ of the body. It serves as�water barrier protection, it regulates body temperature, controls fluid loss, and is important to homeostasis/healthy internal balance.
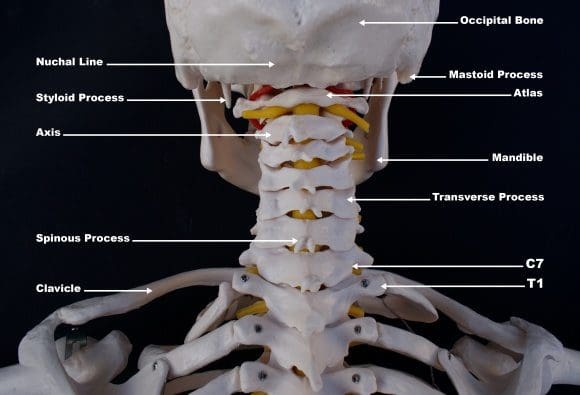
It is made up of many layers and is supported by a complex blood supply. The blood vessels are in a framework of connective tissue including fat and fascia that holds the tissues together. Below that layer is the bone and muscle. There are also nerve endings that relay touch, temperature, and pain signals from the skin to the spinal cord, to the brain.
Compounds�have been developed to safely carry the various medicines through the skin into the blood. These compound enhancers are able to penetrate the skin by opening normally closed channels for a quick time to help the skin absorb the medication/s and then close back up.
Spine Pain
Spine physicians and pain specialists often first recommend topical pain-relievers to help relieve the symptoms of back and neck pain/conditions.
Topical medicines may be used to treat the pain associated with:
Neck strain
Low back strain
Whiplash
Muscle inflammation
Spasms
Osteoarthritis
Rheumatoid arthritis
Certain types of nerve pain
Topical Advantages
Bases like creams, ointments, gels, and sprays make application easy.
Symptom relief is faster than oral medicines.
Symptoms reduce at a steady rate.
Relief can last longer.
Not as much medicine is needed when applied in topical form.
As the medication is diffused through the skin and enters the bloodstream, it bypasses the digestive system reducing any unwanted�side effects, like an irritated stomach.
Topical Disadvantages
Blood flows in different ways to different parts of the body. Education about the product is essential to know where to apply the product like the arm or abdomen and how often.
Blood flow to certain parts of the body can change over time. For example, when it’s cold the blood vessels in the skin contract which decreases the absorption of the medicine, while sweating can open the pores too much and allow too much medication to be absorbed too quickly or wash it away completely.
The skin could present a negative reaction. Therefore patients need to know what to do if an allergic or other reaction takes place.
The skin nerves are different from the spinal nerves, so certain types of neck/back pain may not respond well to topical treatment.
Spinal conditions/disorders deep in the body will not respond well to topical therapy.
Is it right
Are topical pain-alleviating medications the right for you? The best person to ask is your doctor or healthcare provider. Upon a final diagnosis and medical history, your doctor should offer various treatments/therapies for pain management.
Conclusion
Patches and creams can be used to deliver a wide variety of medications. These topicals are becoming popular because of their convenience and, reduction of negative side-effects.
For individuals with muscle or tendon inflammation, applying a topical to the affected area limits the amount of medication going to other areas of the body that do not need it.
For those that have stomach problems and find it difficult to digest anti-inflammatories, these topicals could be all they need to stay active.
Individuals with chronic neck or back pain should discuss these medications with their pain specialist, physician or chiropractor to see if one of these topicals might work for them.
El Paso, TX Neck Pain Chiropractic Treatment
NCBI Resources
Everyone needs to take care of their back/spine because it is what holds us up as long as we keep it straight and strong.�Strengthening the core�can help prevent�a weak and misaligned spine from getting worse�and helps to eliminate pain.
Back safety should be priority one, as it affects all aspects of your life. Not only are you protecting your back, but are preventing future injury. We all need to pay attention to proper body positioning and�body mechanics, as it will pay off in the long run.
More and more individuals are looking to add or try out complementary, alternative or integrative treatments for their back and neck pain. To help understand the differences as well as the similarities between the terms, try to remember:
If an alternative clinic which means not mainstream is combined with a conventional clinic this is mainstream medicine, then it is known as complementary or integrative health care.
If it is used instead of or replaces conventional medical care, it is known as alternative health care.
These terms complementary, alternative and integrative tend to get used interchangeably.
The acronym C.A.M is sometimes used, which means Complementary Alternative Medicine.
Choosing the right practitioner for your spine problem whether osteoarthritis, chronic back pain, or whiplash is just as important as choosing a medical physician or chiropractor.
You want to find an alternative or complementary/ integrative professional who is
Highly trained
Licensed
Experienced in treating your particular condition
Makes you feel comfortable
Takes time to answer all your questions
Finding a Complementary Alternative Specialist
A good place to start is to ask your primary care physician, chiropractor for a referral. Others include:
Credentialing, licensing and certifying are terms you will find when learning about a particular complementary alternative medicine clinic or practitioner. Credentials can include the practitioner�s education, where and what they are allowed to practice. Certification in a particular field of practice like acupuncture, for example, is typically needed before the state issues a license and allows the professional to begin treating patients.
You can check your state�s mandatory licensure process for the type of complementary, alternative or integrative practitioner or clinic you are looking into. Most states require the practitioner to register their education, graduation, training, and continuing education credits. Your state agency can provide this information explaining what services the practitioner is allowed to provide such as the ability to provide dietary supplements.
Review the education and qualifications of all potential practitioners
Questions to think about when doing your research.
Did they graduate from a certified program/school?
Did they complete advanced training?
Are they a member of professional societies or organizations?
Do they regularly continue their training with up to date and advanced education?
How long have they been practicing?
Are the treatments covered by insurance?
Are they ready to work with your insurance provider?
What’s the cost of treatment if not covered by insurance?
Your Appointment Plan
Treatment or therapy that the complementary, alternative or integrative practitioner/clinic provides is considered non-medical.
These practitioners need your medical history, that includes over-the-counter and prescription medications, allergies, prior treatment like surgery/spinal injections along with vitamins/supplements you take. Additional information that could be needed is the contact information of your primary care physician or the doctor who referred you. Keep your primary physician/chiropractor informed about all treatments or therapies you will be receiving.
El Paso, TX Neck Pain Chiropractic Treatment
NCBI Resources
The spine is the primary support for the body. When it breaks down, the body suffers.�Regular chiropractic treatment ensures that the spinal column remains in proper alignment which, in turn, keeps the body in proper alignment. It helps with joint health as well as the health of the related muscles and ligaments.
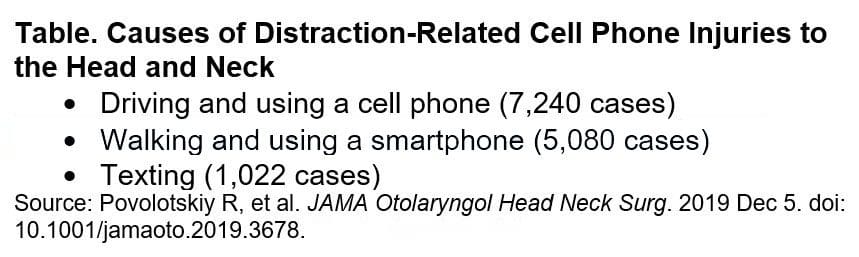
Head and neck injuries related to phone use are on the rise. Since the first iPhone was released, according to a study in JAMA Otolaryngology-Head & Neck Surgery.
Doctors are warning cell phone users to be especially careful when:
Walking around and texting
It is a distraction and one of the leading causes of head and neck injuries.
2,501 reported cases of phone-related head and neck injuries that lead to emergency room visits between January 1998 and December 2017 found in a nationwide database. Injuries in teens and young adults aged 13 to 29 years old were about 40%, in women (55%) and men (45%).
Common Phone Injuries
Common injuries include:
Cuts
Bruises
Abrasions
Internal injuries usually happen around the eyes and nose
Possible trauma to the brain
Over 41% of these injuries happened at home and were minor with little or no treatment needed. Around 50% of injuries were a result of distracted driving and 30% from distracted walking.
Any type of phone distraction in and out of the home puts you and others at risk for:
Falls
Slips
Trips
All of which can lead to injuries and other possible consequences (e.g. a busted phone).
More individuals are getting injured because of phone use while moving around and not paying attention to what’s around them.
Children
Children under the age of 13 were at higher risk to suffer a mechanical injury like parents accidentally dropping the phone on their child or children hitting themselves in the face. For example, ninety cases of injuries occurred while playing Pokemon Go.
Spending as little as two to four hours a day hunched over a smartphone is enough to make a serious impact on the body over time. And though two to four hours may not seem like a long time, it isn�t hard to arrive at two hours by adding several 15-minute or half-hour segments together.
For teenagers, specifically, two to four hours on a smartphone has changed as of now teenagers spend around seven to eight hours on their phones. Spending twice as much time on afternoons or the space between classes or lunch. Think about the impact of 1500 plus hours of bad posture throughout the year. There is no surprise that teenagers are at risk.
The lasting impact of text neck and distracted phone use on today�s young people will be costly. Therefore, the public needs to be educated about the risks of distracted phone use and reducing this distracted behavior.
*Neck* Pain Chiropractic Care El Paso, Texas
NCBI Resources
If you begin noticing pain, spasms, or irritation around the neck, shoulders, or back make an appointment with a professional chiropractor. Explain when the pain occurred, the severity, and the activity that started it. A simple adjustment may be all that is needed to get re-aligned and gain relief from pain caused by overuse. A chiropractor can also help decrease the chances of the injury worsening over time.
Here are some tips that you can use throughout the year but are especially useful during the holidays. So give yourself the gift of spending happy holidays with less stress, neck and back pain. Christmas is a time of excitement, growth, family, friends mixed with stress.
Now there is good stress that we all use when we need it, but when everything just starts to close in all around you, that’s the bad kind of stress that we want to prevent and avoid. For people with chronic back or neck pain, the strain of getting your to-do list done can take the joy of the season right out and replace it with pain and misery. �Therefore plan ahead so you can get your holiday chores done without pain.
Five tips for making the holidays more enjoyable and comfortable
Tip 1 – Shop Simple
Back and leg pain, along with sciatica, can make walking at a shopping mall almost impossible. Instead of doing a lot of walking maybe pick up gift cards or go online. This way the family and friends get to pick whatever they want and you avoid lifting and carrying shopping bags. But, if you do buy personalized gifts, go online. Everything gets shipped straight to wherever you want.
Tip 2 – Plan Before Cooking
If you’re expecting a large crowd, prepare all you can ahead of time. Example: pies can be baked the day before.
Before you start cooking, look at the kitchen. Is there room for everyone to fit while helping, conversing, etc? If not, set up the space so people can flow easily around each other and get things done.
Use your counter-top to lean on every now and then for a few minutes and take the pressure off your back. Do not stay in any one position for an extended period. To help you not forget, set a timer to remind you to sit, rest, or stand. Also, let your guests help with serving and clean up so any stress on the body is reduced.
Tip 3 – Make Decorating a Group Activity
Don�t decorate by yourself. Especially when moving heavy objects. Get help so everyone is involved. This will prevent repetitive injuries when reaching or twisting and reduce stress to you and your family’s backs.
Tip 4: Make Time for Yourself
During the holidays we can get tempted to forget about our regular eating and exercise routines.
Stay focused, as you need strength and flexibility to be able to accomplish these tasks. So stretch out and continue your exercise regimen no matter how hectic it gets.
Stretching will help keep you limber and reduce the risk of a sprain or strain.
If there is no time for your regular exercise routine, don�t just drop it. Adapt and break up the exercises into little segments throughout the day.
Continue to eat the regular healthy meals you’re used to. Gaining weight will make back pain worse. Staying on track isn�t easy during the holidays. Take a look online for healthy strategies before the holiday parties begin.
Here are some examples:
Eat breakfast to prevent overeating later in the day.
At the party, fill up with low-calorie foods like vegetables, leafy green salads, and lean proteins.
Try to stay out of easy reach of nuts, chips or candies, cookies, etc.
If you’re going to have some high-calorie food have some, but don’t overdo it.
And if you�re going to indulge try something that doesn’t come around all the time, like a piece of your aunt�s pie, cookies, cake, ham, tamales, that you only get once a year.
Tip 5 – Look to the Future
Look ahead to the future and look up some simple ways to improve your back or neck pain. Setting some goals like adding a 5-minute walk break to your day that you could gradually increase to ten, fifteen minutes and so on. Signing up for a yoga/fitness class could be another idea. This could also be the year to replace your mattress. Whatever the case, take it all in, look at the options and figure out what works for you.
How to eliminate Back Pain naturally | (2020) Foot Levelers |El Paso, Tx
NCBI Resources
There are 3 major categories of stress: bodily, environmental and emotional.
Bodily stress: Caused by lack of sleep, disease, trauma or injury, and improper nutrition.
Environmental stress:�Caused by loud noises (sudden or sustained), pollution and world events, such as war and politics.
Emotional stress:�Caused by a variety of life events, such as moving homes, starting a new job and regular personal interactions. In contrast to the other two categories of stress, however, people can have some control over their emotional stress. Such can depend on the individual�s own attitude.
A trigger point is a knot or bundle of stiff spine muscle tissue that you can’t move or relax, and when touched pain spreads to the neck, shoulders, and upper back.
Pretty much everyone can relate to this type of pain in the neck or what is known as myofascial pain syndrome when several of these trigger points are grouped.
How to ease the pain and prevent it
Trigger points can form in muscles all over the body. Myofascial pain syndrome in the neck happens when trigger points develop in the muscles of the shoulders, upper back, and neck.
A Trigger Point
Trigger points have a unique connection to America. They were first identified in the 1940s by Janet Travell, MD, who was John F. Kennedy’s doctor. JFK had severe chronic back pain and had trigger point injections to ease the pain.
A trigger point is a sensitive area within the muscles. They are typically described as knots and feel like a bundle of tense, contracted muscles that twitch and spread pain when touched. The spreading pain is known as referred pain. Example: Trigger points in the shoulder send pain into the neck.
Trigger points cause muscles to stress and to contract. This results in:
Muscle weakness
Numbness
Limited muscle movement
Formation of Points in The Neck
They are usually caused by mechanical factors (factors that strain or stress the muscles).� Spinal trauma, like whiplash from an automobile accident or sports-related injury, can create trigger points.
They also develop through repetitive actions and routine everyday chores that can hurt the spine over time.
Straining the neck muscles from poor posture for extended times like craning the neck while working on a computer, carrying a heavy bag that stresses the muscles of the neck, upper back, and shoulders.
Trigger Points vs Fibromyalgia Tender Points
Trigger points do get confused with tender points of fibromyalgia. Trigger points and tender points are both defined as local areas of pain but are not the same.
Tender points do not cause referred pain the way trigger points do.
Tender points are symmetrical meaning that they are on both sides of the body. Whereas trigger points do not follow a symmetrical pattern.
But it can become complicated because individuals with fibromyalgia can have both tender points and trigger points. People with fibromyalgia can also have myofascial pain syndrome.
Trigger Point Diagnosis
Trigger points are a regular cause of different types of spine pain, that can range from neck pain to low back pain. However, doctors are still trying to understand how trigger points produce referred pain. This is why diagnosing trigger points can be difficult for doctors.
They are complex because they are easy to pinpoint but difficult to diagnose. As they can directly cause muscle pain but they can mimic other pain making conditions exactly the way Myofascial pain and fibromyalgia get confused.
Jaw pain
Earaches
Toothaches
These types of pain that do not go away could be caused by trigger point/s in the neck.
Individuals with chronic neck pain that don’t seem to have a cause, could be trigger points. A doctor will refer you to a physical therapist, chiropractor or another spine specialist to conduct an examination for trigger points.
Treatment
Treatment can range from home remedies, chiropractic care, physical therapy and if severe muscle injections. There is no one treatment that works, as everyone and their injuries are different, meaning that various treatment options need to be looked into.
Home
Before starting any home therapy, discuss it with a trained professional like a doctor, chiropractor, massage therapist, or physical therapist to identify the location of the trigger point to effectively treat it.
Treated with massaging the area but can be tough with hard-to-reach places in the upper back. If unable to reach the point slowly and gently roll over a foam roller, golf or tennis ball for quick relief.
Massage
Massage therapists are trained in relieving muscle pain. Deep tissue massage can relieve an irritated area. Regular massage sessions can reduce pain and prevent the points from reemerging.
Physical therapy
Physical therapy treats trigger points in different ways, this includes:
Massage
Heat
Electrical stimulation
Ultrasound
A cooling spray is applied followed with stretches to relax and relieve the contracted muscle/s
Medications
Muscle relaxants can be used to reduce the symptoms and relieve pain. However, these meds can have all kinds of side effects, and become habit-forming, so use should be limited and in conjunction with a proper chiropractic/physical therapy treatment plan.
Injections
If the pain continues despite the non-surgical treatments or worsens, then your doctor could recommend trigger point injections. Injections are late-stage therapy. Doctors want to avoid patients becoming dependant on injections and will prescribe injections with an exercise, chiropractic/physical therapy program for maximum relief and effectiveness.
Overall Health
The majority of people have felt tight muscles around the neck. Utilizing proper posture and healthy spinal mechanics can prevent trigger points and myofascial pain syndrome.
Our services are specialized and focused on injuries and the complete recovery process.�Our areas of practice include�Wellness & Nutrition, Chronic Pain,�Personal Injury,�Auto Accident Care, Work Injuries, Back Injury, Low�Back Pain, Neck Pain, Migraine Headaches, Sports Injuries,�Severe Sciatica, Scoliosis, Complex Herniated Discs,�Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, and Functional Medicine Treatments.
�Neck Pain and Chiropractic Treatment El Paso, Texas
NCIB Resources
Many people who have trigger points or myofascial pain syndrome in their spine have knots and tightness throughout their back and neck. To prevent myofascial pain syndrome one needs to practice a healthy lifestyle that promotes good spine health. Stretching and exercising regularly can help keep stress under control and prevent tension from building up, which makes it harder for trigger points to activate and cause pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine