After all of these years, I am happy to announce that the Texas Supreme Court has finally made a decision regarding the Texas Board of Chiropractic Examiners et al v. Texas Medical Association case on January 29th, 2021. With great honor and gratitude, I’d like to continue to extend sincere thanks to everyone who worked hard on this case and whose tremendous efforts resulted in the decision. Thanks to the Supreme Court’s decision, chiropractors in Texas can now carry on their jobs accordingly. Below, I have provided a letter from Board President, Mark R. Bronson, D.C., F.I.A.N.M. on behalf of the Texas Board of Chiropractic Examiners stating the Texas Supreme Court’s decision in the Texas Board of Chiropractic Examiners et al v. Texas Medical Association case on January 29th, 2021. – Dr. Alex Jimenez D.C., C.C.S.T.
February 1, 2021
On behalf of the Texas Board of Chiropractic Examiners, I extend our sincere thanks and appreciation to everyone whose efforts resulted in the Texas Supreme Court’s decision in Texas Board of Chiropractic Examiners et al v. Texas Medical Association on January 29, 2021. Special thanks are due to all the attorneys at the Office of the Attorney General who worked on this case over these years.
The decision properly affirmed the validity of the Board’s scope of practice rule, which the court clearly said does not exceed our statutory scope of chiropractic practice. The court unequivocally held that the Board�s rules do not violate Occupations Code Chapter 201 or run counter to the chapter’s objectives set by the Texas Legislature, and in fact, carefully observe the statutory boundary between the medical and chiropractic professions. This decision, which recognizes the common sense and long-standing inclusion of associated nerves in chiropractic diagnosis and treatment, preserves and strengthens the essence of chiropractic.
Thanks to the court’s decision, our licensees can now fulfill their duties as vital portal-of-entry healthcare providers in Texas without fear. The court’s decision reaffirms the principles of economic freedom that have made Texas the best state in the nation to be a chiropractor.
Sincerely,
Mark R. Bronson, D.C., F.I.A.N.M. Board President
Texas Board of Chiropractic Examiners
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas & New Mexico*
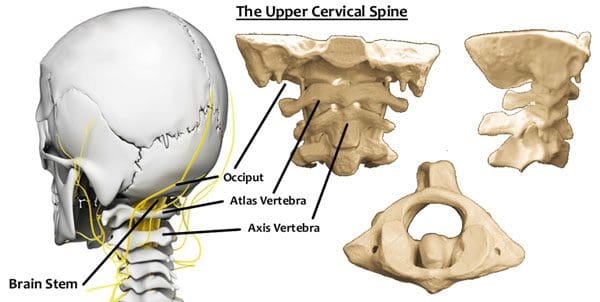
The Atlas vertebra is named for the mythological figure who held the world on their back/neck. The vertebrae are located at the top of the spine, where the cranium and spine connect. More than just a foundation for support, the vertebrae could be the most important vertebrae of the body. It consists of a complex bundle of nerves, vertebral arteries, and is the point where the entire weight of the cranium makes contact.
The myth requires Atlas to be careful while holding the world carefully and confidently at all times, otherwise it will come crashing down. The key is being able to balance it perfectly. The vertebra has the same job to hold the head up properly and maintain posture. If not problems with balance and alignment will begin to develop, and affect the entire spine.
The Atlas Vertebra
Balance
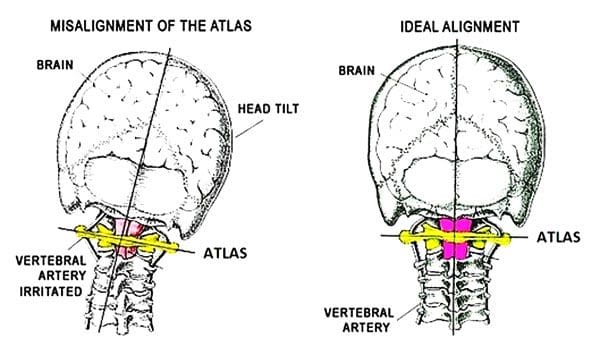
The Atlas vertebrae’s role in maintaining balance is based on its ability to adjust to the weight of the head. The actual vertebra is wider than the other cervical vertebrae. This creates a center of gravity that is reinforced through proper posture. It distributes the weight of the head (10-12lb) evenly to centralize the weight and is supported by the natural curvature of the spine.
If the center of gravity shifts, the Atlas vertebra will tilt in that direction as well. This creates instability in the cervical spine and can increase the amount of weight the spine is taking and trying to redistribute. This creates spinal issues and leads to everything from poor posture, overcompensation that leads to injury.
Shifting Causes
Disruption to the vertebra and its ability to balance can come from a variety of causes and can occur as a result of chronic and acute conditions. Some include:
Auto accidents, sports, work injuries can cause cervical soft tissue damage
Dislocation of cervical vertebrae below the Atlas results in instability
Poor posture/s make individuals overcompensate to one side of the body straining muscles, ligaments, tendons causing pain and other issues
Herniated, bulging, and slipped discs
Unbalanced effects
Spinal issues range from simple neck pain and soreness to full-on chronic pain. Because the Atlas can alter the balance of the entire spine, combined with cranium support, issues can be localized and referred creating further complications. Addressing the root problems requires a comprehensive chiropractic approach. Chiropractic will assess the position of the spine and determine the degree to which Atlas has shifted out of place. An adjustment treatment plan makes it possible to undo the widespread damage.
Body Composition
Muscle Loss
Individuals do not realize that muscle loss occurs throughout their lifetime. This is because muscles, like other tissues in the body, must go through cell turnover and protein synthesis. This means that the body is constantly breaking down protein in the muscles and rebuilding them.
Skeletal muscle can be developed with proper nutrition and includes consuming a proper amount of protein to provide the necessary amino acids and from physical activity. The reverse is also true, if an individual becomes less physically active and/or their diet no longer supports the development of increased muscle tissue, the body enters a catabolic/tissue-reducing state known as muscle atrophy.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Woodfield, H Charles 3rd et al. �Craniocervical chiropractic procedures – a pr�cis of upper cervical chiropractic.��The Journal of the Canadian Chiropractic Association�vol. 59,2 (2015): 173-92.
Spinal traction, both mechanical and manual are treatment options that are based on the application of force to the axis of the spinal column. A region of the spinal column is pulled in opposite directions to stabilize or change the position of herniated, slipped, bulging, discs, and/or nerve injury/damage to the spine. Traction treatment is crucial to spinal adjustments, especially with disc or nerve compression.
It allows the chiropractor to alleviate any stress that could lead to disc problems like herniation, rupture, or displacement. However, traction is a general term. The concepts can apply to all forms of traction, but the application itself can be drastically different in terms of static positioning and inverse force.
Mechanical vs. Manual Cervical Traction
Mechanical force is typically applied through a series of weights or a fixation device and requires the patient to stay in bed or is placed in a halo vest. The techniques and methodologies can vary, but the objectives/results are the same.
The utilization is developed on a case-by-case basis and the chiropractor’s diagnosis/recommendations. Many chiropractors implement both mechanical and manual traction approaches. Choosing the right traction plan comes from a thorough examination, medical history, and understanding of each method’s strengths.
Traction approach
The difference between mechanical and manual traction is simple. Mechanical traction is directed by the use of machines, weights, and pulleys, while manual traction is performed by a professional chiropractor. With mechanical traction, an individual’s head is cradled into a sling, then positioned at the optimal position for the adjustment. The sling is counterweighted to hold the head/neck in that position, leveraging mechanical pressure and affecting change.
Manual traction has the individual lie down on a table, with the chiropractor pulling the head away from the neck to decompress the cervical spine. The adjustment/s can be a continuous pull, or a series of low-force pulls in different directions. Again these depend on the individual’s condition and nature of the adjustment.
Techniques and methodologies
Mechanical and manual traction can have similar results, but both offer different benefits based on the individual. Mechanical traction is a hands-free technique for decompression that allows chiropractors to focus on the patient’s needs when working on complex cases. This method is more applicable for severe cases, where the traction could last for 20-30 minutes.
Mechanical traction is helpful when teaching healthy posturing. Manual traction benefits come from the control that a chiropractor has over the technique. With the manual pulling, the chiropractor can increase or decrease the countering force. A hands-on approach enables chiropractors to feel the spinal adjustments, and understand the effects of the traction.
The proper form of traction
The overall ability of traction to decompress the spine makes it a valuable approach to treat various conditions. The exact nature of the condition determines whether mechanical or manual traction will be used along with the recommendation/treatment plan of the chiropractor. Injury Medical Chiropractic Clinic is committed to implementing the best approach for spinal correction for every patient. Mechanical and manual traction are just two adjustment modalities.
Body Composition Health
Resistance Training For Everyone
Even if not an athlete resistance training is important for functional fitness. Functional strength training attempts to emulate the physiological demands of real day-to-day activities. Traditional strength training focuses on specific muscle groups during the exercise, while functional training focuses on whole muscle groups to train the body for daily responsibilities.
Individuals might believe they are too old for resistance training. But research shows the benefits of improving an individual’s functional fitness level, specifically for older adults. Functional training resistance exercises and bodyweight movements can help the body become stronger, more flexible, more agile, and better equipped to handle day-to-day responsibilities. Plus, it can help with injury prevention.
Reference
Afzal, Rabia et al. �Comparison between Manual Traction, Manual Opening technique, and Combination in Patients with cervical radiculopathy: Randomized Control Trial.� JPMA. The Journal of the Pakistan Medical Association�vol. 69,9 (2019): 1237-1241.
Individuals with neck and back pain should consider adding a few pain-relieving therapeutic tools to the holiday wish list. Spine specialists/experts have some tools for their patients and others who are dealing with back and neck pain. Looking at various points, these therapeutic tools offer the gift of helping to reduce neck and back pain, when unable to see a chiropractor or physical therapist.
Foam Rollers
Foam rolling is effective for different types of aches and pains, especially backaches. Foam rolling benefits include:
Releasing muscle knots and tension
Reduces inflammation
Decreases pain
Improves range of motion
Returns flexibility
Wedge Pillow
A wedge pillow for the back is a necessity. A wedge pillow removes the stress from the spine and neck when lying down. Flipped around will take the tension off the legs also bringing back pain relief.
Deep Percussive Massager
Percussive massagers can provide a deep massage to various areas of the body especially the lower back. There are a variety of brands available with different levels of technology. However, careful use of these instruments must be exercised. This is because the massage can be intense and can exacerbate or cause further injury, and individuals can develop a tolerance making the massage no longer effective.
Seat Cushion
If sitting at a desk throughout the day or working from home a proper seat cushion is mandatory. Many individuals who sit the majority of their day utilize a combination cushion that includes the seat cushion with lower back support. Individual cushions are great because they can be moved easily and adjusted to fit where needed. Therapeutic seat cushions come with various features available, here are a few to keep in mind. Memory foam and air cells offer the most pressure relief. If there is tailbone pain, focus on a seat cushion with the tailbone cut out for extra relief. An office chair with these features should also be considered.
Inversion Table
Inversion tables are available at reasonable prices, starting around $100. Used correctly this therapeutic tool can successfully help relieve back pain. Inversion tables and cervical traction provide decompression and postural alignment for the spine helping with pain relief. These devices offer gentle decompression through the angle used. Wider angles or full inversion provides more decompression on the back. Individual spinal needs should be discussed with a chiropractor, physical therapist, or physician before using this therapeutic tool.
Pain Patches and Topical Agents
Pain-relieving patches like Lidocaine, IcyHot, and Salonpas patches are widely recommended for tight and sore areas of the body.
Sitting Standing Desk
A sitting and standing desk can be highly beneficial to back pain. In addition to burning off bonus calories throughout the day, Changing positions and postures throughout the day are recommended. This is to keep the muscles, ligaments, tendons moving, and not in a static position for too long. Changing every 20 to 30 minutes is the recommended time. Sitting and standing desks can provide positional changes that will help with posture, core stability, and circulation. This will help reduce and alleviate pain in the low back, neck, and shoulders. However, the desk needs to be stable and adjusted to the proper height.
Lower Back Sitting Support
These therapeutic tools help reinforce the low back region when seated. Most of us start to slouch forward with the head and shoulders hunched forward after some time at the computer. This strains the whole body, specifically the low back. Lower back supports can help maintain proper alignment of the spine when seated.
Knee, Thigh, Pelvis Pillow
These pillows have different names but are used in the same way. This is a pillow that can be placed between the legs while sleeping takes the pressure off the pelvis and spine. These types of pillows are great for individuals that sleep on their side. This is because the top leg often shifts down, leading to increased stress on the hips and low back. These pillows help keep the legs aligned during sleep relieving pressure on the low back.
How To Self-Care for Back Pain Books
There are a variety of books that offer tips, and therapies for self-care. These products are not a cure-all. They are intended to help in combination with proper treatment, especially for certain spinal conditions. If pain is limiting daily function, consult a chiropractor, physical therapist, or physician about using the above therapeutic tools.
Doctor of Chiropractic Near Me
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Furlan, Andrea D et al. �Massage for low-back pain.��The Cochrane database of systematic reviews,9 CD001929. 1 Sep. 2015, doi:10.1002/14651858.CD001929.pub3
We all have our hobbies that we are passionate about, love doing, and could see turning into a second career. However, certain hobbies can generate stress on the spine. This often leads to a decrease in being able to participate in these activities, which can lead to various health issues. Maintaining the body’s physical fitness and keeping the spine healthy is key to being able to continue without neck or back pain. Hobbies are an important part of life. Individuals need to enjoy what they love from sports activities to music to arts and craft projects. Having activities/hobbies help:
Boost mental health
Relieve stress
Lower blood pressure
Promotes weight loss
Meditative qualities
Here�s how to make sure the hobbies/activities are fun and safe.
Protecting the Neck
Poor posture is one of the leading causes of neck and back pain. Looking down or being in a standing/sitting hunched position regularly increases the load/stress on the neck increasing the chances for strain, injury, headaches, and chronic pain. In the neutral position, the skull weighs around 10-12 pounds.
When leaning the head forward weight increases from let’s say 27 pounds at a 15-degree angle to 60 pounds at a 60-degree angle. The strain on the cervical vertebrae, joints, and muscles can be immense. A good example is text-neck. This has become a normal thing when using a smartphone, gaming, or other similar activities.
Studies suggest that the average individual spends three to five hours a day on a smartphone or tablet. This means three to five hours of extra weight on the cervical spine. Engaging in a hobby that requires an individual to look down constantly in a similar fashion can lead to serious and chronic neck pain along with other cervical issues.
Individuals are spending more time at home and getting more serious about their hobbies. This is fantastic, however, these individuals need to take time to stretch out, and get some physical activity into their hobby routine. Just like taking frequent walk-around, stretch out at work breaks, so to do hobbyists need to step back from their projects to keep a healthy balance. The position of the neck and the way it is held for activities like:
Sewing
Carpentry
Gardening
Painting
Pottery
Knitting
Music
Hobbies like this can increase the risk of neck pain, so the key is prevention, paying attention to head posture every now and again, and taking stretching breaks.
Proper Posture Makes a Difference
Many individuals stand and sit when working on their hobbies. This is quite common and is encouraged when doing these absorbing activities. But being immersed in these activities, most forget to check their posture when doing so. This is what leads to problems that at first are shrugged off as just soreness.
Eventually, the individual begins to engage in bad/awkward posture habits that avoid the pain and think this will help. This worsens the problems and promotes further strain/injury. Leaning, bending, reaching, and twisting curves the spine increasing the load and stress. Performing these actions over and over for extended periods means:
Strain
Low back pain
Muscle spasms
Sciatica
Leg pain
Foot pain
Slouching is another posture problem that increases the likelihood of lower back pain. Slouching causes gaps between the lower back vertebrae. This stresses the facet joints or the connections between the vertebrae. The soft tissues elongate/stretch and lengthen like muscles and connective tissue. What elongation does is:
Cause the tissues to attempt to snap back to the original shape. This can cause painful spasms.
Muscles that are constantly elongated become weaker with time.
The longer an individual sits, stands, and slouches impacts the body’s health negatively, leading to a chain of health problems. Maintaining proper posture and keeping the spine straight minimizes the strain on muscles and the vertebrae. Prevent pain and discomfort.
Ergonomics at the House
Ergonomic stressors include:
The force/s required to perform and complete a physical chore/task.
Adopted static and awkward working postures to complete task/s
The repetitiveness of the task/s
Any of these factors or combination places a higher risk for discomfort, pain, and injury. The immediate surroundings like the bench, work area, craft room, etc. and how the individual moves or does not move, and interacts in these areas is the focus of ergonomics. Proper ergonomics will help protect the spine, as well as the rest of the body. Improper ergonomics can cause damage like muscle strain, repetitive movements, and incorrect posture. Taking a look at the hobby workspace the ergonomics, and making any necessary adjustments can help prevent strain/injury.
Proper seating
Make sure the right type of chair, stool, bench, etc is being utilized. Adjustable types that have neck and lower back support are the way to go. Make sure the base is stable, the seat is comfortable and adjustable. Backrests and armrests can help maintain proper posture.
Correct table/desk/workstation height
Various drafting tables and lap desks have adjustable surfaces to adjust the height for working with a proper ergonomic posture. If the work surface is not adjustable adjust the chair or make adjustments as needed. The hips should be higher than the knees to take the strain off the sacrum and lower back. The upper back should be straight, with the shoulder blades together creating a supportive platform for the neck and head.
Tools
Using the best tools for working and organization will help avoid injuries and constant awkward positions like leaning/reaching over and around the workspace. Look for tools that can be adjusted to different heights, resistance levels, etc. depending on what is needed and what will reduce any strain.
Vision
If an individual needs to lean in to get a closer look then vision could be the problem. If an individual wears glasses it could be time for a check-up. Or if an individual does not wear glasses, it could be time to see an optometrist. Non-prescription magnifiers could be the answer.
Stretching Regularly
Working too long in one position can be detrimental to overall health.
It is very understandable when individuals get into the zone, working on something creative, and not wanting to stop the flow. However, frequent breaks are vital. Stretching regularly and getting up to move around is key to staying healthy.
Neck Stretch
Stretch the neck by turning the head from side to side in a gentle fashion.
Tip the head to each side so the ear almost touches the shoulder.
Lower the head so that the chin almost touches the chest.
Turn the to look diagonally down at the armpit. This stretches the trapezius and levator scapulae muscles.
Hold the stretches for 10-15 seconds.
Always perform slowly and gently.
Lower Back Stretch
15 minutes a day of stretches will maintain the health of the spine. If pain or discomfort becomes frequent or unmanageable, seek professional help. Physical therapists and chiropractors are trained in orthopedic issues and ergonomics without prescription. Call a doctor or physical therapist to find out if treatment is necessary. Following these guidelines can help keep hobbies fun and without pain.
Lower Back Pain Skate Boarding Injury Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Acetaminophen, best known as Tylenol, is one of the most common medications for headaches and general pain. More than likely the most common back, neck, and overall pain medication around. However, it is only a pain reducer, and will not reduce inflammation.
Doctors often recommend this medicine before moving on to prescription medication. A member of the analgesic pain reliever class of medications. These can vary in strength along with side effects, but their purpose is to reduce pain. Acetaminophen can be found in over 600 prescriptions and over-the-counter medicines, including certain opioids. Other acetaminophen brand names include:
Tylophen
Tempra
FeverAll
Mapap
Pharbetol
Panadol
Strength and Weakness
When neck or back pain presents, over-the-counter medicines fall into two categories. These are acetaminophen or non-steroid anti-inflammatory drugs also known as NSAIDs. Acetaminophen and NSAIDs like Advil, aspirin both relieve pain. However, non-steroid anti-inflammatories also help in reducing inflammation. Although non-steroid anti-inflammatories have this added benefit, they can also present potential side effects like stomach and gastrointestinal problems.A spinal sprain or strain can cause acute back pain. Acetaminophen is typically recommended for acute back or neck pain and for pain that comes and goes quickly. Individuals that experience periodic pain usually take acetaminophen when the pain flares up. Individuals with chronic spinal pain report acetaminophen help to alleviate/reduce the pain. Many with chronic pain use acetaminophen regularly and not only when the pain presents. This helps manage before pain strikes.
Safety
Acetaminophen is gentle on the stomach, making some individuals preferring it over the non-steroid anti-inflammatories. But just like any other medication acetaminophen has its risks and can cause severe damage if used improperly.
Taking acetaminophen in large doses can cause severe liver damage. The Food and Drug Administration reports that acetaminophen overdoses send over fifty-thousand individuals to the emergency room every year. And over one-hundred Americans die yearly from accidental overdoses.
Using acetaminophen safely means taking no more than 3,000 milligrams a day and no more than 1,000 milligrams at a time. Take extra precautions when taking extra-strength. These can include as much as 650 mg per pill/capsule.Before taking acetaminophen for back and neck pain, talk to a doctor or pharmacist about the proper dosage. And tell the doctor about all the medications being taken including natural herbs and holistic. Another reason for telling the doctor is that many other medications have acetaminophen included without you knowing it. Part of the discussion should include alcohol consumption. This can elevate the risk of negative reactions.
Resources
If non-pharmacological treatments/therapies done for at least 4 months prove ineffective then an acetaminophen regimen could be a safe and effective part of a back and neck pain treatment plan. While this medicine is one of the most common treatments, it is not without risks and side effects. Talk to a doctor or pharmacist about all the medications and supplements to ensure the regimen supports health for the long-term. To learn more along with safety information go to Acetaminophen Patient Guide.
Severe Back Pain Chiropractic Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
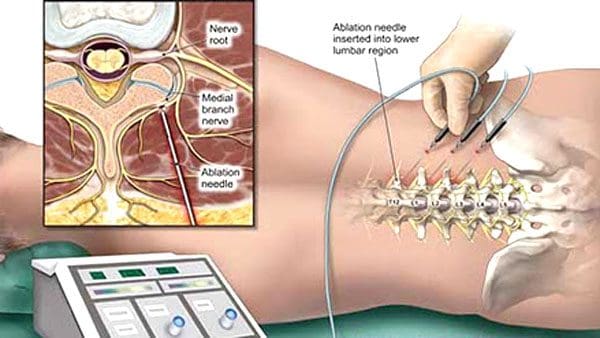
Radiofrequency ablation, also known as RFA is a minimally invasive procedure performed in an outpatient clinic to treat neck, back, facet joints, and sacroiliac joint pain. It involves the use of radio waves pulsing at a high frequency that temporarily disable the nerves from transmitting pain signals to the brain. Relief can last three to six months. Radiofrequency ablation treatment could be an option to manage chronic back and neck pain. There are other names, but the radio frequency concept is the same. They are:
Chronic neck, back, and hip pain take a significant toll on the body. Finding the right treatment can make all the difference. However, it does not work for everyone. For those that might have tried other non-surgical treatments to manage the pain, including physical therapy and steroid injections, that did not bring relief then radiofrequency ablation could be another treatment option.
Radiofrequency Ablation Benefits
Pain relief compared to steroid injections lasts longer
Relief exceeds that of injections
It is a non-surgical procedure
Complication risks are low
Opioid or other analgesic medication is reduced
Quick recovery
Improved quality of life
Relief can last six months to a year, and longer
Pain Reduction
Before undergoing radiofrequency ablation, a doctor must pinpoint the nerves causing the neck, back, or sacroiliac joint pain. They will perform a nerve block injection to determine if there is temporary relief from the pain. If there is temporary relief it means that the origin of the pain was found. This could qualify to become a candidate for radiofrequency ablation.
A Medial branch block is performed to diagnose the facet joint/s that are causing the pain.
Asacroiliac joint block is performed to determine if and which sacroiliac joint is causing the pain.
Preparation
The doctor will give instructions on how to prepare for the procedure. Instructions can vary from those listed, as every patient’s case is unique.
Do not eat 6 hours prior to your procedure
Wear loose, comfortable clothing
Easy to put on shoes
Have a designated driver for after the procedure
Make sure the doctor knows about all medications, vitamins, supplements, and herbs being taken
Follow the doctor�s instructions when taking prescribed and over-the-counter medications. This includes vitamins, supplements, and herbs
Bring all medications on the day of the procedure to be taken with minimal interruption
Radiofrequency ablation usually takes an hour or longer depending on the extent of the treatment. One example could be the number of facet joints being treated.
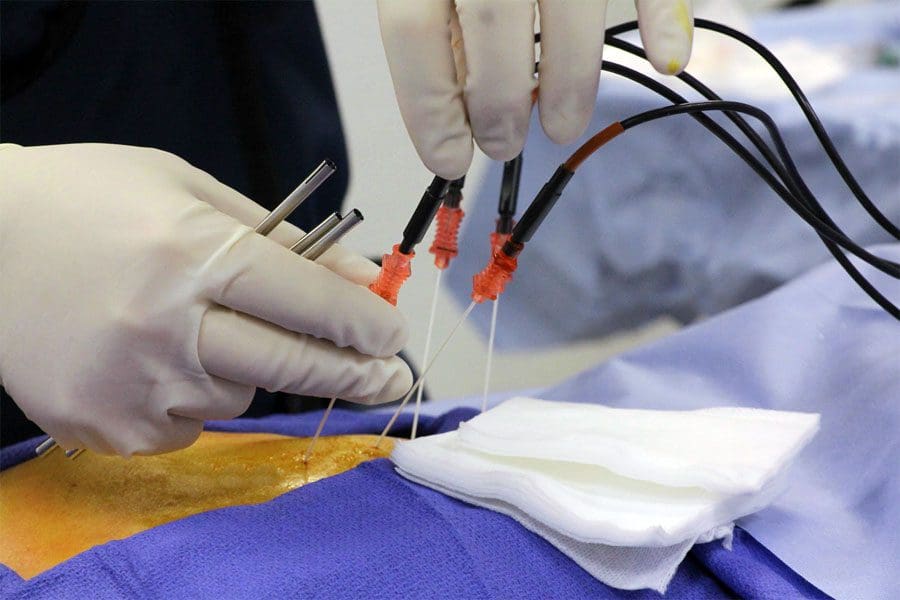
The Procedure
The patient will be positioned face down on the treatment table. Pillows are offered and positioned for optimal comfort. The area where the treatment will be administered is sterilized. The areas of the body not undergoing the treatment are covered with a sterile covering. Sedation could be utilized but not heavy sedation. More than likely it will be what is known as twilight sedation.
A local anesthetic is injected into and around the area/s being treated. Because radiofrequency ablation involves electricity a grounding pad is attached to the calf of one of the legs. The treatment table is adjusted for the precise placement of the needles and electrodes. The doctor will use fluoroscopy or a real-time x-ray as a guide.
Once the needle/s and electrode/s placement is confirmed, a low electrical current is sent through the electrodes. This creates waves of pulsating energy that stimulate and change the nerve/s sensory tissue so it does not send pain signals. Some individuals report a warm or mild pulsing sensation. When finished, the electrodes and needles are removed. The treated area is cleaned up, sterilized and bandages are applied.
After the Procedure
After the procedure, the patient is sent home with a set of recovery instructions. An example could be:
Keep the bandages in place
Don’t take a bath or shower
A shower can be taken the following day and the bandages removed
Do not perform any strenuous activity for up to two days
When the anesthetic wears off, the individual will have soreness and some mild pain around the treatment area. As long as everything is fine individuals can return to work and normal routine within three days. Full recovery can take up to two weeks for the treated/ablated nerves to stop sending pain signals. Although the nerves no longer conduct pain, it is temporary and not a permanent fix. This is because the nerves grow back. If the cycle starts over, talk with the doctor about another session.
Peripheral Neuropathy Relief & Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine