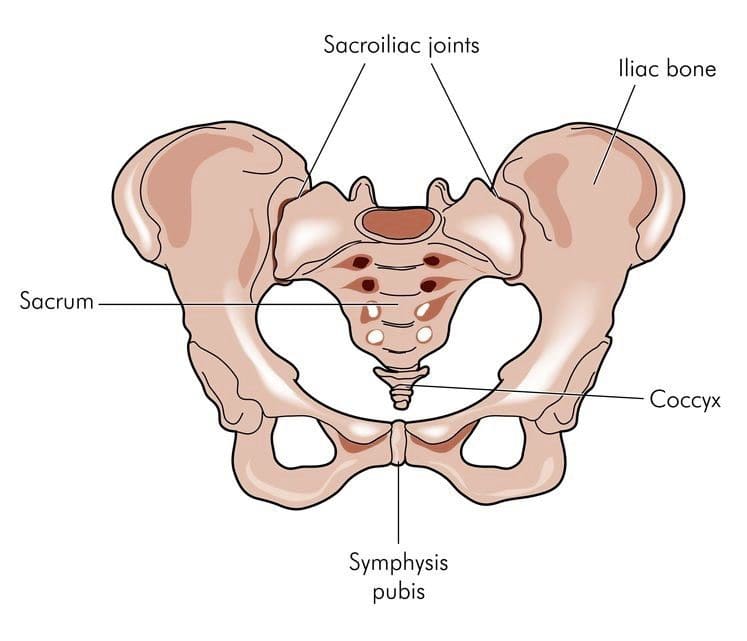
Sacroiliac joint dysfunction and its symptoms can also be a cause for low back pain conditions and disorders.
This condition is also known as:
Sacroiliitis
SI joint inflammation
SI joint syndrome
Sacroiliac joint dysfunction
SI joint strain
It can make regular activities like sitting, standing, walking, and sleeping frustrating, difficult and unbearable. It has been found in around 30-35% of individuals.�Many individuals can spend months or even years dealing with symptoms but are never aware that it’s not the correct diagnosis. Sacroiliac joint dysfunction can sometimes be difficult to diagnose. These joints are so close to the hip and low back, that it is common for sacroiliac joint dysfunction to be mistaken for other causes/conditions of low back pain, like a herniated, slipped or bulging disc.
Sacroiliac Joint Dysfunction Symptoms
When low back pain is present, it can be quite difficult for a doctor to figure out the exact source/cause of your pain.
These are a few recognizable symptoms of sacroiliac joint dysfunction.
Low back pain is the most common.
Pain could also present in the hips, buttocks, thighs, and possibly the groin area.
The pain can be so severe that just touching the area is unbearable.
Other activities that can cause symptoms:
Common movements like climbing stairs, sitting down/getting up out of a seat, can cause pain. Pain can also be aggravated from standing or walking for extended periods but improve when relaxed or lying down. Stiffness or a burning sensation in the pelvis can also present.
Causes of Joint Dysfunction
A variety of conditions can cause sacroiliac joint dysfunction. The most common:
Arthritis
Joint pain can be caused by spinal osteoarthritis because as the cartilage around the sacroiliac joint wears down, the bones can start to rub against each other. Ankylosing spondylitis is an inflammatory arthritis that affects the spine that can also cause joint dysfunction.
Pregnancy
Pregnant women can experience low back pain or pelvic pain from sacroiliac dysfunction because the joints get stretched and lose their elasticity during pregnancy. Hormone changes and added weight during pregnancy can place added stress on the sacroiliac joints.
Accident Trauma
High impact from an auto accident, slip and fall injury, or sports injury could damage the sacroiliac joint/s.
Viral Infection
Infections are extremely rare but could be another cause of joint pain.
There are a variety of treatment options that can help reduce and prevent low back pain.
Exercise/Physical Therapy
Exercise and physical therapy are therapies that doctors highly recommend before other treatments like pain medications or surgery. Exercise, chiropractic and physical therapy can help manage pain and other symptoms. Consult your doctor before starting any physical therapy or exercise program. Your doctor can recommend a chiropractor or therapist that can help get you started with the proper exercise treatment plan.
Physical Therapy
Physical therapy can help reduce stress on the joints, that are strained and tight. It also helps maintain joint flexibility. A physical therapist will perform passive and active treatment therapies to help manage joint pain.
Passive treatments – the physical therapist does the majority of the work. An example of passive treatment applying heat or ice along with massaging the area.
Active treatments – the patient participates in the treatment with at-home exercise routines is an example of active treatment.
A combination of passive and active treatment provides the best outcomes and offers the most benefits, as the patient has the know-how of proper posture, exercises that they can do and injury prevention. A chiropractor and physical therapist can build a physical therapy program to help address your symptoms.
Exercise
With sacroiliac joint dysfunction, you do not have to do hard intense exercise. The benefits come from a consistent gentle exercise routine with an emphasis on consistency. Exercising stretches and strengthens muscles of the low back muscles and helps maintain joint flexibility.
An overall exercise plan should incorporate the three main types:
Sacroiliac joint dysfunction is known to cause low back pain, but diagnosing can be hard for some doctors. Especially those that do not have a great deal of experience in sacroiliac joint pain. However,�chiropractors specialize in this area as the SI joint is an important part of the musculoskeletal system.
There are different types of topical medications, different ways of delivery and are available for patients with back and neck pain. A physician may combine one or more types of medication for maximum relief or as a way of�limiting the side effects of larger doses of only one medication. Strong dose compounds and controlled drugs are�only�available with a doctor’s prescription.
Medicines with a low potency and low risk of side effects are available at stores and local pharmacies over-the-counter. But remember medications sold over the counter without a prescription doesn’t mean they are safe to use as much as possible. Please read the label and follow the instructions. Taking higher doses, even acetaminophen e.g. Tylenol can cause liver damage. Discussing these medications with a doctor or pharmacist before purchase would be wise. Your physician should know if you plan to continue using over-the-counter medications.
Medicines with a low potency and low risk of side effects are available at stores and local pharmacies over-the-counter. But remember medications sold over the counter without a prescription doesn’t mean they are safe to use as much as possible. Please read the label and follow the instructions. Taking higher doses, even acetaminophen e.g. Tylenol can cause liver damage. Discussing these medications with a doctor or pharmacist before purchase would be wise. Your physician should know if you plan to continue using over-the-counter medications.
Inform your physician about all the products you take including herbal remedies to decrease the risk of side effects or potential severe drug interactions. When acute pain is present, injections either intravenous or intramuscular injected into the muscles are used. For chronic pain, medications are used and are typically in pill form. Both methods have limitations and different�delivery�approaches may be considered. This includes inhalation or topical on top of the skin applications.
Topical Pain Alleviators
These type of medications come prepared and are applied to the skin via:
Topical medications aim to reduce inflammation and soothe nerve and muscle pain. Some are available with a doctor’s prescription and others are over-the-counter. Medication administered�through the skin is becoming more popular.
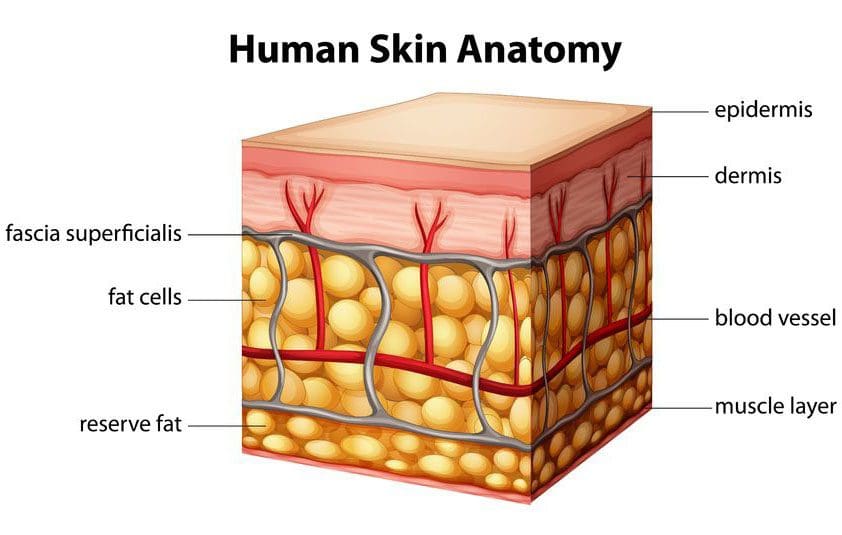
Skin Cells
The skin is the largest organ of the body. It serves as�water barrier protection, it regulates body temperature, controls fluid loss, and is important to homeostasis/healthy internal balance.
It is made up of many layers and is supported by a complex blood supply. The blood vessels are in a framework of connective tissue including fat and fascia that holds the tissues together. Below that layer is the bone and muscle. There are also nerve endings that relay touch, temperature, and pain signals from the skin to the spinal cord, to the brain.
Compounds�have been developed to safely carry the various medicines through the skin into the blood. These compound enhancers are able to penetrate the skin by opening normally closed channels for a quick time to help the skin absorb the medication/s and then close back up.
Spine Pain
Spine physicians and pain specialists often first recommend topical pain-relievers to help relieve the symptoms of back and neck pain/conditions.
Topical medicines may be used to treat the pain associated with:
Neck strain
Low back strain
Whiplash
Muscle inflammation
Spasms
Osteoarthritis
Rheumatoid arthritis
Certain types of nerve pain
Topical Advantages
Bases like creams, ointments, gels, and sprays make application easy.
Symptom relief is faster than oral medicines.
Symptoms reduce at a steady rate.
Relief can last longer.
Not as much medicine is needed when applied in topical form.
As the medication is diffused through the skin and enters the bloodstream, it bypasses the digestive system reducing any unwanted�side effects, like an irritated stomach.
Topical Disadvantages
Blood flows in different ways to different parts of the body. Education about the product is essential to know where to apply the product like the arm or abdomen and how often.
Blood flow to certain parts of the body can change over time. For example, when it’s cold the blood vessels in the skin contract which decreases the absorption of the medicine, while sweating can open the pores too much and allow too much medication to be absorbed too quickly or wash it away completely.
The skin could present a negative reaction. Therefore patients need to know what to do if an allergic or other reaction takes place.
The skin nerves are different from the spinal nerves, so certain types of neck/back pain may not respond well to topical treatment.
Spinal conditions/disorders deep in the body will not respond well to topical therapy.
Is it right
Are topical pain-alleviating medications the right for you? The best person to ask is your doctor or healthcare provider. Upon a final diagnosis and medical history, your doctor should offer various treatments/therapies for pain management.
Conclusion
Patches and creams can be used to deliver a wide variety of medications. These topicals are becoming popular because of their convenience and, reduction of negative side-effects.
For individuals with muscle or tendon inflammation, applying a topical to the affected area limits the amount of medication going to other areas of the body that do not need it.
For those that have stomach problems and find it difficult to digest anti-inflammatories, these topicals could be all they need to stay active.
Individuals with chronic neck or back pain should discuss these medications with their pain specialist, physician or chiropractor to see if one of these topicals might work for them.
El Paso, TX Neck Pain Chiropractic Treatment
NCBI Resources
Everyone needs to take care of their back/spine because it is what holds us up as long as we keep it straight and strong.�Strengthening the core�can help prevent�a weak and misaligned spine from getting worse�and helps to eliminate pain.
Back safety should be priority one, as it affects all aspects of your life. Not only are you protecting your back, but are preventing future injury. We all need to pay attention to proper body positioning and�body mechanics, as it will pay off in the long run.
Living in the desert means we don’t have to deal with digging/shoveling through snow and ice, but there are still proper techniques, tools, body mechanics, posture, and core strength that we should pay attention to and apply to guard our spines and general health. It is no surprise that when shoveling many individuals experience muscle fatigue, low back strain, vertebral disc damage (herniated disc), and even spinal fractures.
A great deal of these injuries come from excessive stress to spinal structures by slip and fall accidents. Shoveling is a frequent cause of back pain and injuries. Injuries are not only limited to the musculoskeletal system but excessive shoveling can also place added stress on the cardiovascular system.� Any hint of shortness of breath or chest pain, stop shoveling immediately but if symptoms continue, seek medical attention.
A study published indicated when handling heavy material with a shovel, the L5-S1 disc has been identified as the weakest link in the body. The most severe injuries along with pain are likely to occur in the back. Here are some tips to prevent injury.
Shoveling Basics
Shoveling can be compared to weight lifting and intense aerobic exercise. To help your body function correctly consider the following tips:
Eat long before shoveling so you have fuel but don’t cramp up.
Avoid caffeinated drinks/beverages. Stimulants can increase heart rate and cause blood vessels to constrict.
If you experience pain, stop immediately and get assistance.
Pace yourself when shoveling.
Take plenty of breaks.
Drink plenty of water to rehydrate your body.
For snow, if the ground is icy or slick, throw sand or salt to help create traction. But still be aware that some areas can still be uneven and cause you to slip, trip, or fall.
Proper Clothing
Consider the weather before beginning the job.
When it’s cold dress in layers, wear gloves, and a hat because a good amount of body heat is lost through the head. If icy cold, use a scarf.
Wear clothing that is easy to move around in.
Proper boots are essential for maintaining balance, traction and keeping feet warm/dry.
Choose specialized work/blister-free gloves or thicker gloves, that allow for a good grip on the handle.
The Shovel That’s Right for You and the Job
Shovels come in different materials, purposes, shapes, and sizes.
Choose an ergonomic shovel with a curved handle. These shovels help keep your back straight and reduce spinal stress.
Hardware stores stock ergonomically designed shovels of all types.
For snow maybe try a shovel with a plastic blade instead of metal as it’s lightweight.
Sometimes a smaller blade is the way to go. You don’t shovel as much per load, but it weighs less and puts less strain on the spine.
Don’t go for a cheap model if the job you are doing is heavy-duty. Your body will thank you.
Once you have your shovel take some time to learn the proper technique.
Technique is Key
Take some time to stretch and prepare your body as warm muscles work better.
Hand placement on the shovel is very important! Don�t grip with the hands close to each other.
Keep some distance between the hands. This will give you more leverage and make it easier to lift.
Think about proper posture and maintaining the natural curve of your spine.
Address the task directly.
Stand with your feet shoulder-width apart to stay balanced.
Try to keep the shovel close to your body. Holding a shovelful with arms outstretched puts added weight on your spine.
Bend at the knees and not the waist or back.
Tighten your stomach muscles as you lift.
Lift with your legs and not your back.
Dump the material in front of you. If you need to move the material to the side, move your feet.
Do not twist your body.
Scoop small amounts into the shovel
Walk to where you want to dump it.
Do not throw over your shoulder.
Go forward with the material.
Pace yourself. Take frequent breaks and stretch your back and body.
Power Equipment
Power equipment is terrific, but if it’s not used correctly, you can still strain or injure your back.
Example: Snowblowers are designed to remove snow at a certain speed but pushing or forcing the equipment to go faster is defeating the purpose of the machine doing the work for you.
You may not realize that you hurt your back. But that little twinge you felt could change your life forever. Getting back to 100% of where you were before the injury could take time and treatment. So, do not take this activity lightly and remember prevention is the best defense.
El Paso, TX Lower Back Pain Chiropractic Care
NCBI Resources
Injuries that are caused by repetitive movements often develop gradually.�It�s not until the symptoms get very painful and debilitating that the individual realizes that something is wrong. Don�t wait, as soon as you feel a tingle, slight pinch, or a little soreness and feel that it’s from your work, get in touch with a doctor or chiropractor.
Around 70% of America’s workforce sits in an office chair for most of the day. Then we spend extended time sitting down eating, studying, watching T.V., and driving. All of this time spent sitting is taking its toll on our bodies.
Effects of When We Sit Too Long
Sitting places added stress and pressure on the back because it transfers the body’s full weight onto the buttocks and thighs. Sitting for long periods can cause pressure to increase on the discs, which can lead to severe/chronic back pain. Sitting also takes a toll on the lower extremities. As the blood stays�in the legs and feet this creates a sluggish return of blood to the heart.
In addition to sitting proper body mechanics are not implemented. Most of us sit with an improper posture, which can not only cause physical discomfort but also contributes to other health problems, which include:
Abdominal pain
Back pain
Eyestrain
Leg pain
Neck pain
Repetitive movement/motion injuries
Using a well-made ergonomic chair can help reduce fatigue, discomfort, increase blood flow, reduce injury, and increase job productivity.
An Ergonomic Chair
If it is to be used at a computer station or on a factory�machine, it needs to be able to handle the tasks and fit the worker’s size. Here are some recommendations to help you pick a quality chair that will increase comfort and reduce injury.
Casters
Use a chair with casters either in the form of a pivoting roller/with wheels and a 5-point base to make movement easier. There are different types of casters, some for carpet use, and soft wheel casters for hard surfaces like tile and linoleum. Rubber locking casters can help prevent tipping. Also, choose a chair that swivels easily.
Seat Pan
The seat pan supports the majority of your weight. A chair with the cushion made from a dense, foam padding or spring coils is better than a basic cushion that loses its shape and compresses which causes discomfort, imbalance, and hip/back fatigue. The pan should be at least one inch wider than the hips and thighs on each side. The front part of the seat should slope down a little and allow a fist-sized space between the back of your knees and the front edge of the seat pan to reduce pressure on the back of the thighs.
Also, a chair with tilting adjustments allows the individual the ability to a forward working posture or a properly reclined posture. Some seat pans also have a sliding mechanism that can be beneficial. This means small and tall users are able to adjust the distance of the seat pan from the backrest.
The Backrest
Adequate back support is the most essential element of a backrest. Inadequate back support places added pressure on the spine. The backrest should be small enough to fit the small of the back, the pelvis, and back of the rib cage or be curved. Both provide adequate support. A lot of the chairs come with a built-in adjustment, that can be adjusted by turning a knob on one side or under the chair. Chairs with back supports that are large enough to provide mid-back and upper back support are an added bonus.
Armrests
Chairs with adjustable height and width are necessary with a chair with armrests. The armrest should be made of soft comfortable material and be 2 inches wide for adequate surface area.
Seat Height
Pretty much all chairs come with a seat height adjustment. A properly�adjusted�seat means that your feet can rest properly on the floor while the upper body is aligned with the computer, display, and keyboard. Hydraulic adjustments are standard on most chairs, but there are pneumatic adjustments that allow you to adjust the seat height while sitting on the chair. Keep in mind the mechanism to adjust the seat should be easy to reach.
Chair Reclining and Tilt Adjustment
The chair recline/tilt adjustment changes the angle of the entire seat. Like with the backrest angle adjustability, a reclined chair transfers upper body weight to the backrest of the chair. However, locking the backrest in one position is not recommended or beneficial for the back.
Considerations
Footrests
For most a footrest is not necessary. But if additional foot support is necessary, a floor-mounted rest will allow you to rest your feet in a comfortable position.
Fabric Types
Keep in mind the cleaning and maintenance that goes into the chair when choosing which. Upholstery is the most common covering but is not the easiest to keep clean. Vinyl and leather covers are easy to clean but don’t breathe well and can generate heat in the legs.
Safe Sitting
Other than using an ergonomic chair, here are some precautions to minimize discomfort and injury while sitting:
Do not stay in one position for a long time.
Change postures often.
Shift between sitting and standing, 20 minutes of standing then 20 of sitting.
Try to keep your feet flat on the floor.
Sit with proper posture upright with your back and shoulders against the backrest.
Do not use the armrests to slouch.
Elbows and arms should rest lightly to promote circulation.
Make sure the shoulders are relaxed and slightly dropped when on the keyboard.
�Stay In a Neutral Posture
With the back supported and straight
The hips slightly higher than the knees
Keep between 2-4 inches of the chair edge and behind the knees
Maintain an equal balance of weight on the seat
Most Important
Take frequent breaks
Stand up and move around
Stretch
Be aware of your posture while your sitting
Correct yourself if you are slouching or moving out of the proper posture
Take deep breaths
This will increase blood flow and reduce fatigue.�Small changes will go a long way and keep you comfortable and healthy.
Work smarter not harder
Because we spend so much time in a chair we need to have the right one that will protect our spines. Think of the chair as a piece of�work�equipment to optimize productivity. Ergonomics utilized to the fullest means less back pain and better focus.
When your body is truly healthy, you will arrive at your optimal health and proper physiological state. �We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing we have learned what works effectively at decreasing pain while increasing human vitality.
Reduce Back Pain With Custom Foot Orthotics El Paso, TX.
NCBI Resources
Ergonomic chairs have come a long way, and they do help reduce spine problems, pain, and improve movement.�Improving spinal health and hygiene at work�is as simple as�taking breaks for light stretching,walking around, and utilizing ergonomic office products to stay fit and injury-free. Whatever you choose, understand how your back and neck are moving/functioning during the workday/night by using ergonomic fundamentals that will keep your body/mind healthy and prevent office injuries.
Back/spine injuries now rank either second or third overall for workplace injury/s. According to the Bureau of Labor Statistics, every year there are over 900,000 cases of back injuries that account for 1 in 4 non-fatal job-related injuries that involve work days missed.�
Backcare & Standing Work
Back injuries can be painful, debilitating, and life-changing. 8 out of 10 people will experience a back/spine injury that can lead to chronic pain and health conditions. We all need to know, especially those of us that work standing up is firsthand knowledge of how important it is learning how to improve spine health and take steps to prevent back injury.
In order to prevent low back disorders means that there needs to be an understanding�of the spine when working along with knowledge of back injury risk factors.
Back/Spine Basics
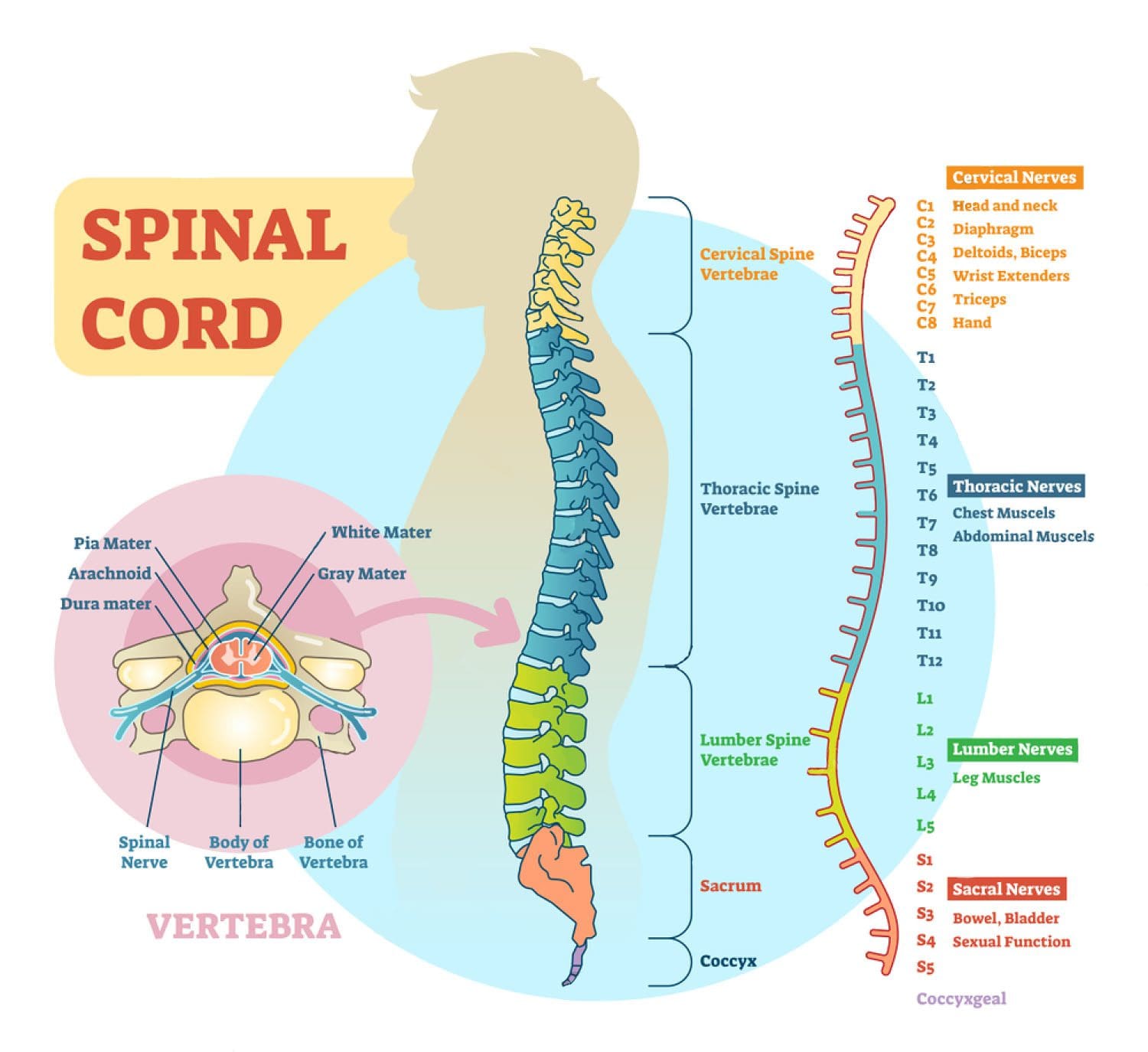
The spine is a flexible structure that consists of 24 bones that move, shift, and contort, called vertebrae. There are:
7 in the neck
12 in the chest
5 in the low back
These are connected by ligaments and separated by pads of cartilage, called intervertebral discs. These are the shock absorbers that allow the flexible movement of the spine, specifically at the neck and the low back.
When we stand, the spine naturally curves inwards and outwards. The inward curve is called lordosis, and curves towards the front of the body at the lower back and neck area. The outward curve is called kyphosis, and curves towards the back of the body around the chest area. When we bend over the vertebrae of the lower back change position and shift from being in lordosis to kyphosis when completely bent over and then back again when upright. With this information, it is easy to see how much we move around, bend, stretch and reach during a regular day. The lower back gets used the most, which is why low back pain and injury/s and disorders are the most common.
The National Institute of Occupational Safety and Health concluded: �muscle strain is the most common type of work or nonwork back pain� (Bernard, 1997). This is good news for chiropractors and ergonomists because it means that we can find ways to reduce/change the way we work and the effort involved to minimize injury risks.
Keeping the intervertebral discs healthy plays an extremely significant role in preventing back/spine injuries. If these discs get damaged and start to degenerate,�flexibility begins to fade away, stiffness and soreness sets in and the ability to absorb the daily pressure/forces that comes with standing, moving and working.
There is not a normal blood supply to the intervertebral discs. Instead, as the discs change shape when we move around, the nutrients that they need are absorbed into the discs as the waste products are pumped out. This is why moving the body and staying active is very important. Because as you move you are literally feeding your spine and expelling the bad stuff. Intermittently changing postures and positions helps change the force and weight on the discs so that not all one area is taking the brunt of the force. Remember to move around and keep your spine as healthy as possible.
Risk factors
Major risk factors for back injuries include:
Awkward postures
Bending
Twisting�
Heavy physical tasks
Lifting
Forceful movements
Whole-body vibration aka W.B.V.
Static or unmoving work postures
These risks can happen separately or could be a combination of them all, and if these risks are taking place at any one time the higher probability of an injury/s.
Standing Work
When we stand, the pressure on the�lower back discs is relatively low. Not that there is pressure but it is much lower than when seated with an unsupported backrest like bleachers for example. Standing up uses 20% more energy than sitting does. When we need to bend down to pick up objects or reach to get overhead objects there is an increase in the forces and pressure on the lower back, and this is when an injury is likely to happen.
Tips to Minimize Injury
Here are some tips to help minimize your risks of back/spine injury when you are doing standing work:
Moving around is important to keep the spine healthy. Moving will help improve circulation and reduce muscle fatigue.
Taking consistent short breaks will help reduce fatigue, discomfort and work other muscles.
Gentle stretching during some of these breaks helps to ease muscle tension and gets circulation pumping.
Pay attention to your posture and the way you stand as you work.
Lean on a solid support to help reduce fatigue when you are standing with a support that you can put your back up against, lean against sideways, lean forwards against and to hold on to will increase safety.
Keep your back strong and try to do exercises that will strengthen the back muscles. Activities, like Yoga, Crossfit, HITT or workouts focused on the spine for flexibility are the way to go.
Maintain a stable posture with your feet on a firm surface.
Avoid twisting the lower back around to reach for things.
Move your feet so that your whole body changes position.
Minimize bending, but when you have to, bend for objects in front of you and bend at the knees instead of the back. When bending for objects that are to the side of you change your stance so you are facing the object, and then bend down at the knees.
Don’t overreach but if you have to reach up to a high area to get something use a step-ladder.
Don’t reach over objects and move the obstruction or change your position before reaching for whatever it is.
Low Back Pain? Fix it with *FOOT ORTHOTICS* | El Paso, Tx
NCBI Resources
The one size fits all method just doesn�t cut it. A more focused approach for every individual leads to better results. Patients find that placing their bodies in certain positions and certain physical activities can:
Activate
Aggravate
Deactivate�their back pain.
Patients also find the pain being either better or worse. Understanding why sitting, standing, and walking can change the severity of low back pain can be helpful in diagnosis. These are important cues that help to diagnose and treat low back pain. People sit, stand, and walk all day. This is why so much research has been conducted on how these specific positions and activities contribute to low back pain.
Inversion tables and inversion treatment/therapy could help with low back/leg pain and sciatica. It�s non-surgical and an option your doctor, or chiropractor could recommend to you before looking into more invasive options. Individuals with low back pain, sciatica or both found inversion therapy with an inversion table provided relief from symptoms, and continued use has kept them and their spines healthy.
With an inversion table, you don�t have to use gravity boots or completely hanging upside down. There are inversion boots and hanging racks that also offer inversion therapy, this type is not for beginners. With experience, you can move on to this type but for now, leave it to individuals in top health and athletic condition. This type of inversion table therapy is an alternative that doesn’t require being completely upside down.
An Ancient Therapy Brought Back
Inversion therapy is nothing new. Hippocrates, the father of medicine, saw what inversion therapy could do and the benefits around 400 BC. The goal is to use gravity to release compression in the spine. The downward force pulls everything toward the earth’s center.
How It Works
Inversion therapy works in a way like spinal traction.
For example, when we stand and sit gravity pulls the spine downward and this is what compresses the discs, vertebral bodies, nerves, and other spinal structures. The physical dynamics along with gravity helps relieve spinal compression. As the spine is stretched out the pressure on your back is reduced.
The theory behind inversion therapy sounds like a fantastic non-surgical option to back pain. However, the research going into inversion therapy is a bit more mixed. One study found that almost 77% of patients that were candidates for surgery no longer needed the surgery after using inversion therapy. For patients that didn�t use inversion therapy, only 23% avoided surgery.
But like all back pain/sciatica treatment plans, it’s what works for you. Ask your doctor/chiropractor about the pros and cons of this type of treatment as it relates to your condition to make an informed decision.
Other Benefits
Many patients report that inversion therapy is a great way to:
Stretch the muscles and ligaments
Reduce muscle spasms
Improve circulation
Stretching stimulates the lymph glands which increases the flow of lymphatic fluids, that are part of the body’s waste disposal. Cellular health depends on healthy blood circulation to be delivered, to nourish and remove waste.
The therapy also helped to relieve motion sickness and stress. This is because the body is more aware of its spatial orientation along with balance as the inner ear gets stimulated while inverted. As stated earlier it is not necessary to be positioned completely upside down to benefit from this therapy. Inversion tables are adjustable and offer the flexibility to find the best angle.
Discuss Inversion Therapy with A Doctor
Before you start using an inversion table�talk to your doctor. Certain medications and health conditions could make using an inversion table unsafe.
It could be recommended against inversion table therapy if you have:
There could be other medical conditions that are not listed but could interfere with inversion therapy, so make sure your doctor knows all your medical history/conditions and current health state before beginning.
Starting Inversion Therapy
How to start an inversion therapy program? Take it very slow, easy, taking your time and have someone there to help and assist until you are comfortable doing it on your own.�The tables can be set at different angles and it is recommended you start at the first and work your way to the last. At the 15-degree angle, your body will feel a stretch along with the benefits of increased blood circulation.
Most people don’t have to go beyond 60-degrees, as the spine decompresses at this angle. But you might want to completely invert yourself as you work through the different degrees and go for the full inversion. But don’t overdo it and listen to what your body tells you.
The tables come in a variety of styles, so be sure to research the different brands. Some tables can include a sliding backrest and foot lock that lets you work in gentle stretching exercises during inversion. This could include head movements from side-to-side, stretching the arms overhead, and doing abdominal sit-ups or crunches.
But first, find out from your doctor how often you should invert and the kinds of movements that will help with your condition and enhance your inversion program. Inversion therapy is another option for a back, sciatic pain treatment plan. For the different forms of spine pain, a doctor will try several non-surgical treatment options before discussing surgery. Inversion therapy could be part of a conservative treatment plan and could help prevent the need for spine surgery.
*Effective Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
The spine is the primary support for the body. When it breaks down, the body suffers. Regular chiropractic treatment ensures that the spinal column remains in proper alignment which, in turn, keeps the body in proper alignment. It helps with joint health as well as the health of the related muscles and ligaments.
Your chiropractor can also recommend stretching and strength-building exercises to help keep your spine healthy and supple. Chiropractic helps to keep the back flexible which aids in preventing injury. A healthy spine is also less likely to become misaligned or experience pain. It can significantly improve your quality of life as you are more flexible and mobile.
Musculoskeletal health is one of the highest costs in healthcare today.
There are 1 in 2 Americans that have a musculoskeletal condition. And the need for support along with body alignment is at an all-time high.
In today’s world surveys found that Americans wear two to three pairs of shoes during the week.
However, these shoes are not made to support:
The body
Fit the feet
And can be dangerous to general musculoskeletal health
Health and freedom from pain are important factors in a healthy quality of life. But it starts with proper support for the body that begins from the ground up.
Many believe that to get proper support all you need is to buy top shoes that are optimized with athletic properties. While athletic shoes are definitely more comfortable they do not provide adequate support for the body and can affect posture and the body’s alignment.
The shoes out on the market today, whether athletic or dress are more about fashion than function. These shoes are designed based on sample sizes. Shoe companies use for men a size ten and for women a size eight for their sample. Then material is�added or subtracted to create the larger or smaller sizes.
The resultant shoes are designed to fit and provide optimum performance but are not customized to conform to each individual’s unique feet.�
Shoes are designed to protect feet from the elements and adapt to various activities.
They are not designed to handle the additional forces necessary to support the body.
Take a look at the extensive wear patterns on your shoes and see if there are imbalances in the feet. If there are areas that are really worn/flattened out then there can be severe pronation taking place. This is one serious reason to look into foot orthotics,
Not to worry, as excessive foot pronation affects everyone.
While at school, work or conducting daily chores is when individuals pronate and while wearing shoes with no arch/spine support.
Pronation in the feet combined with shoes that don’t fit with no support has a negative impact on posture and alignment.
With no sufficient support, the body reverts to the imbalanced state. With continued use and not addressed will cause pain in the:
Knees
Hips
Back
Neck
And unfortunately, most of us ignore and even power through the pain caused by the poor fit and lack of support from these shoes.
Reasons to Use Custom Orthotics
The feet make up the body�s foundation. Just like a house, problems with the foundation will create problems throughout the structure over time. Therefore if the foundation is remedied properly then the other issues remedy themselves or are easier to treat because the feet are already taken care of.
Feet problems/issues create back problems. Fixing foot problems will make a difference with the back pain treatment plan.
Individuals think their feet are just fine. However, they don’t know what problems are in the background waiting for the worst moment to present. Imbalance/dysfunction is a silent issue that can ripple into many problems along with pain in the spine.
Feet are as unique as fingerprints. Custom orthotics will make a vast difference between the right and left foot and accommodate the body to achieve its full potential.
Custom orthotics are built just for you. Based on a high-resolution 3D scan of your feet, that is sent to a Foot Levelers� team of technicians, who create your 100% unique, tailored foot orthotic/s.
Don�t be fooled by over-the-counter knock offs. These are mass-produced insoles that can worsen pain. And while most cases of back pain respond well with Chiropractic care, adding custom foot orthotics will enhance the effectiveness of the treatment with no need for surgery or side effects from medications.
Your feet and your body will thank you and will improve health by maintaining proper posture, combined with full-body support to achieve optimal quality of life.
How to eliminate Back Pain naturally | (2020) Foot Levelers |El Paso, Tx
NCBI Resources
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot�line up which extends through the tibia, or shin bone.
This can cause a condition called knock knees and it can change the way the entire body is aligned. This puts the body out of balance, destabilizing the spine, and can even cause the pelvis to tilt to one side or the other. When you are walking or standing, the stress caused by the misalignment can create a domino effect, causing or contributing to low back pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine