Trying to understand what is causing back pain that comes out of nowhere, whether a spinal issue or a kidney issue can be quite challenging. Doing a self-examination, retracing steps, and constantly thinking about it is exhausting. The right healthcare professional that has experience in spinal issues, as well as, understanding various health conditions that can contribute to spine pain, and making the correct diagnosis can help in developing the proper treatment plan or refer the individual to the proper specialist.
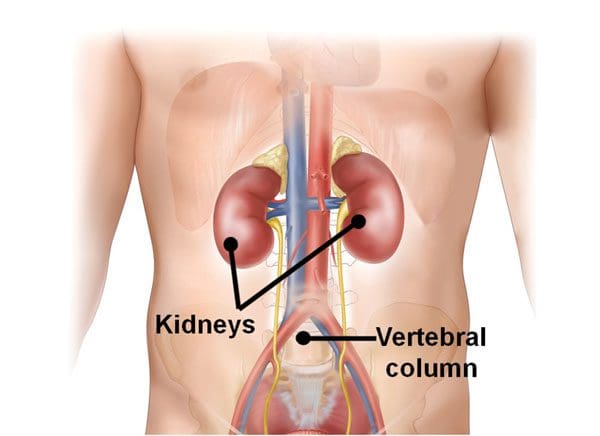
The Kidneys
The organs are located below the ribs, close to the middle/thoracic back. Healthy kidneys support and help with:
These can easily be mistaken for mid and upper back pain. However, if there is persistent soreness or irritation it could mean a more significant health issue associated with the kidneys could be present.
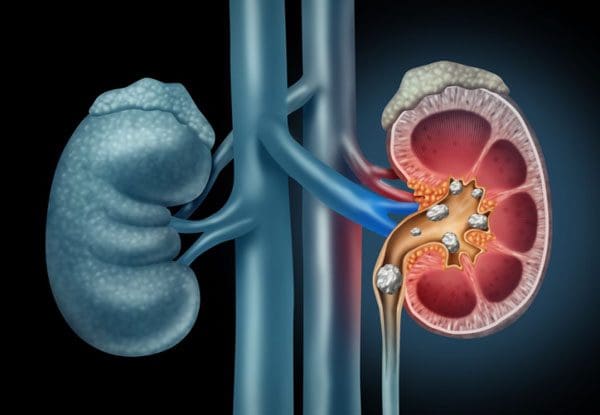
Spine Problem or Stone/s
If there is a feeling of kidney pain it is possible to come from one of two places and/or both. This could be distension/ballooning of the capsule called the ureter that surrounds the kidneys. The ureters are the tubes that are attached to each kidney and transport urine from the kidneys to the bladder. Urine contains salts and minerals. These minerals can clump together creating a kidney stone and block the ureters. The ureter contracts from the stone that is creating the blockage.
When there is a blockage from a stone, the urine can back up and cause the capsule to expand causing pain. The pain location is usually on one side and is categorized as a dull ache – meaning the pain is constantly present and causing discomfort. Chronic back pain caused by nerve compression is typically on one side like sciatica.
The pain from a stone can be only slight unless the stone is trying to move. Then the pain can be severe and last for several minutes before it passes. However, if the pain is excruciating and a kidney stone is suspected, go to the hospital and get an examination. Collecting the stone is crucial when it passes in order to be analyzed. A stone analysis will help in figuring the proper treatment to prevent another kidney stone/s from developing.
Spine Problem or Infection
A kidney infection could be another cause of back pain. Kidney infection/s are typically caused by bacteria. A dull throbbing could be sensed in the middle and/or upper back.
Symptoms
Signs and symptoms associated with infection often include back, side, and groin pain as well as a combination of symptoms like:
Chills
Fever
Burning sensation when urinating
Constant sensation of needing to use the bathroom
Nausea
Vomiting
Causes
Causes that can increase the chances of developing an infection.
Kidney stone/s
Nerve damage that affects the bladder
Spinal damage that does not allow the bladder to be emptied
Urinary tract infection
Older individuals can develop kidney infections without any underlying conditions. There are rare genetic diseases like polycystic kidney disease and Fabry disease that can cause kidney pain and be mistaken for back pain.
Telling the Difference
There is no quick and easy way to figure out if it is back or kidney pain. Especially, if a constant aching is present. Seeing an experienced doctor or chiropractor is the recommended option for getting a formal and accurate diagnosis. A physical exam, family, and personal medical history will be collected along with various tests. Tests can include:
Urine analysis
Culture
Abdominal X-ray
CT scan
MRI
Pain medications and specific fluids are usually prescribed along with time to pass the stone. Antibiotics can be prescribed for kidney infections, chiropractic treatment can be suggested for spinal alignment/myofascial tense muscle release, and home remedies can help treat any discomfort. These can include:
Using ice/heat on the area where there is discomfort
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Tozzi, P et al. �Low back pain and kidney mobility: local osteopathic fascial manipulation decreases pain perception and improves renal mobility.��Journal of bodywork and movement therapies�vol. 16,3 (2012): 381-391. doi:10.1016/j.jbmt.2012.02.001
Back discomfort and pain could be caused by hip issues and could be resolved with hip replacement. According to a recent study, a total hip replacement solved back pain in four out of five individuals dealing with spinal discomfort and pain. When the hip/s are stiff or cannot move normally, this places added pressure on the spine. Studies show that low back pain was resolved in 82% of individuals after a total hip replacement known as total hip arthroplasty or THA. The body is designed as a fluid chain with fluid motion connecting the neck all the way down to the toes.
When a region like the hip tightens/stiffens, it generates added stress/pressure on the other areas of the body, which in this case happens to be the lower spine. Individuals with mild arthritis of the spine are able to experience increased pain reduction than individuals with severe arthritis. An insight into the relationship between the hips and low back that can lead to accurate diagnoses and optimal treatment plans.
Hip Issues
The hip/s move with the lower back during activities like walking, sitting, bending, etc. Tight muscles, normal wear-and-tear, and osteoarthritis can reduce hip movement, forcing the lower back to make awkward and poor posture causing adjustments. Individuals usually relieve the painful position by increasing the curve of their lower back.
If an individual has severe arthritis of the hip, they put a lot of stress and pressure on the low back that often results in low back pain. Advanced hip osteoarthritis is the breakdown of joint cartilage and the most common type of arthritis. Individuals with this type experience low back pain 50% of the time, and even higher depending on the individual’s condition. 80% to 90% of individuals with hip or knee arthritis, unfortunately, develop low back arthritis.
There is not yet a clear reason as to why this occurs. It is theorized that some osteoarthritis risk factors like obesity and high-impact/force activities can be modified with lifestyle adjustments. Other risk factors that include injury, trauma, age, and congenital conditions like hip dysplasia, cannot be avoided. Hip osteoarthritis isn�t the only hip issue that can also cause lower back pain. Other hip issues.
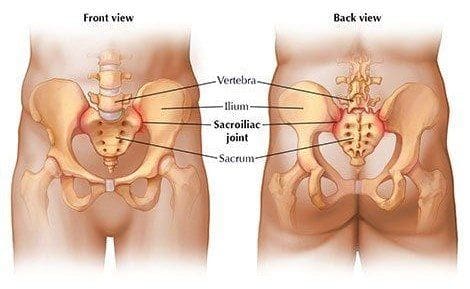
Sacroiliac joint dysfunction
The sacroiliac joint connects the sacrum to the pelvis. It is a shock absorber between the upper body, the pelvis and can stiffen with time. Sacroiliac joint pain affects around 15% to 25% of individuals with low back pain. It worsens when climbing stairs, getting up from a seated position or running. Symptoms include:
Low back pain
Pain in buttock/s
Groin pain
Stiffness
Instability
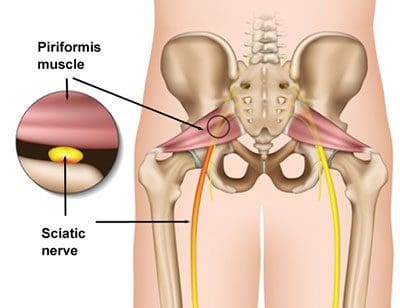
Piriformis syndrome
About 200,000 individuals each year are affected with piriformis syndrome and is often misdiagnosed as symptoms resemble sciatica. What happens is the piriformis muscle, which connects the sacrum to the top of the femur, tightens/irritates the sciatic nerve. Symptoms are often mistaken for sciatica with pain in the buttocks, numbness, and tingling that travels down the back of the leg and into the feet.
Diagnosis
A doctor or chiropractor will use a combination of diagnostic tools. This typically includes a physical exam, X-rays with other specific tests to help identify the source of pain. What typically happens is a patient will undergo a hip and lumbar spine X-ray, but the thoracic spine, pelvis, and hip areas are missed. Getting the middle segment is critical to see how the spine and hips are working together. It is critical to understand the hip-spine connection. All spine patients should have X-rays of the hips to make sure any problems don’t go undetected. The overlap of symptoms with these two areas could be overlooked.
If necessary a diagnostic injection into the hip joint can help precisely locate the pain source. This can be done at the clinic or doctor’s office using ultrasound or X-ray to guide the needle. If no pain relief results from the injection, hip replacement is still not considered because the pain could be coming from the spine. A critical part of the diagnosis is not just imaging. One of the most important parts is getting a thorough history of symptoms. X-rays and MRI show what the problem could be, however, the symptoms could coming from another area.
Treatment Options
Before total hip replacement is considered there are nonsurgical approaches to be considered. All diagnoses should start with conservative treatment. Physical therapy, chiropractic, gait training, and core strengthening can optimize the spine to better manage hip issues and arthritis. Conservative therapies could also include:
Weight loss
Activity modification like walking instead of running
Anti-inflammatory medication
Cortisone injections
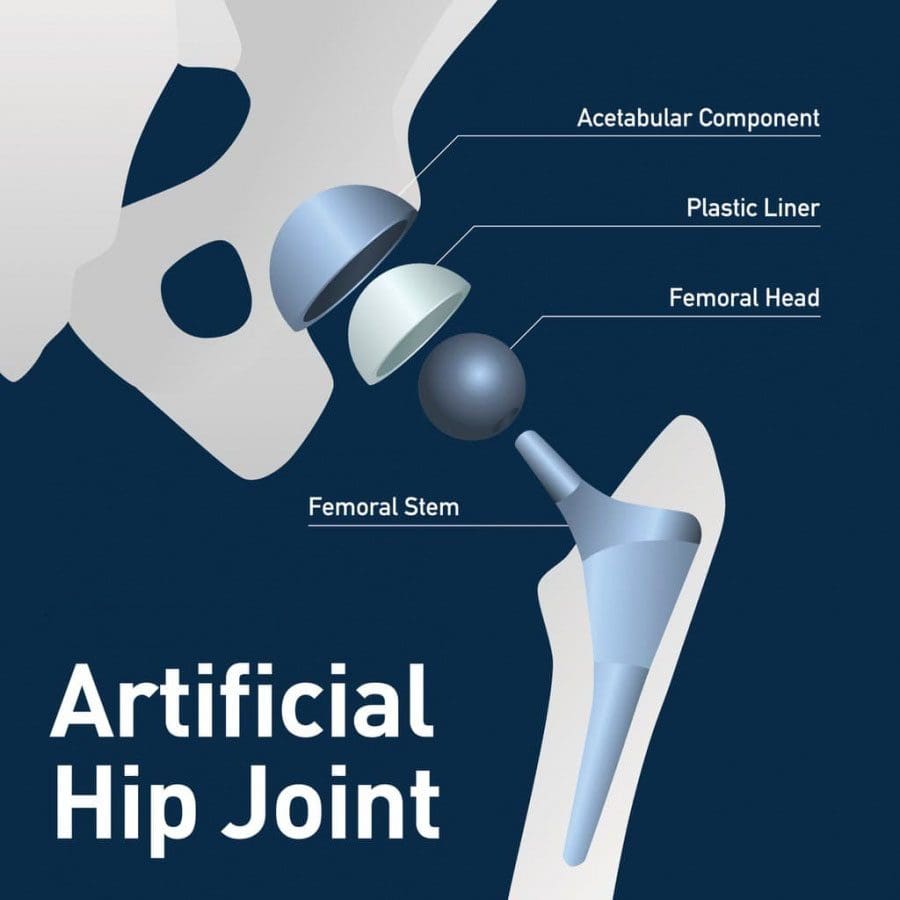
Total hip replacement is the last option for individuals experiencing pain, difficulty walking, and limited mobility. The procedure removes the damaged cartilage and bone from the hip joint. This includes the head of the thighbone along with the socket where it fits and replaces it with artificial parts.
Conclusion
Get a second opinion. Individuals are encouraged to educate themselves as much as possible on the condition. The hip and spine is a complex relationship. The most important information for patients is that they understand along with their doctor where the pain is coming from, the hip, spine, or both.
Reduce Plantar Fasciitis Foot Pain
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
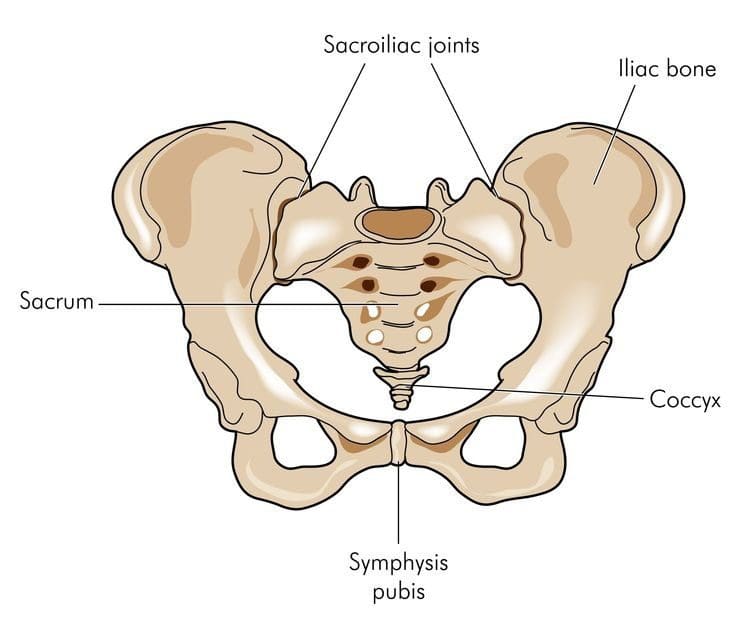
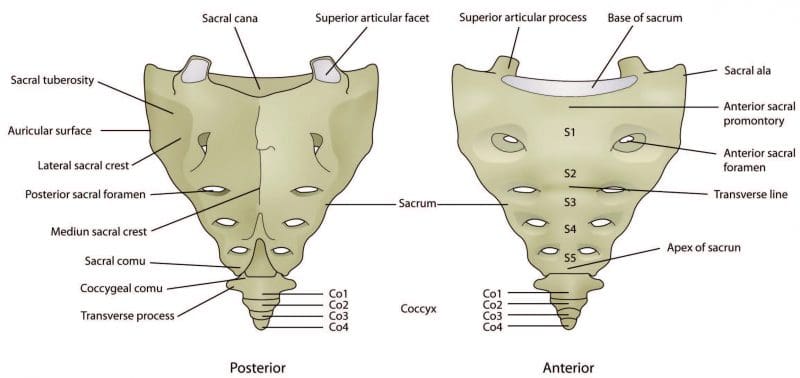
The sacrum and coccyx are part of the vertebral spinal column and could contribute to low back pain. They are not like the other bones in the spinal column. The sacrum, also known as the sacral vertebra, sacral spine, and S1 is a large, flat triangular-shaped bone that is between the hip bones and below the last lumbar vertebra known as L5. The coccyx, known as the tailbone, is positioned below the sacrum.
The sacrum and coccyx are made up of smaller bones that fuse and grow into a solid bone mass by the age of 30. The sacrum is composed of 5 fused vertebrae known as S1-S5 and 3 to 5 smaller bones that fuse creating the coccyx. Both are weight-bearing bones and are integral to walking, standing, and sitting functions.
Sacrum and the Lumbosacral Spine
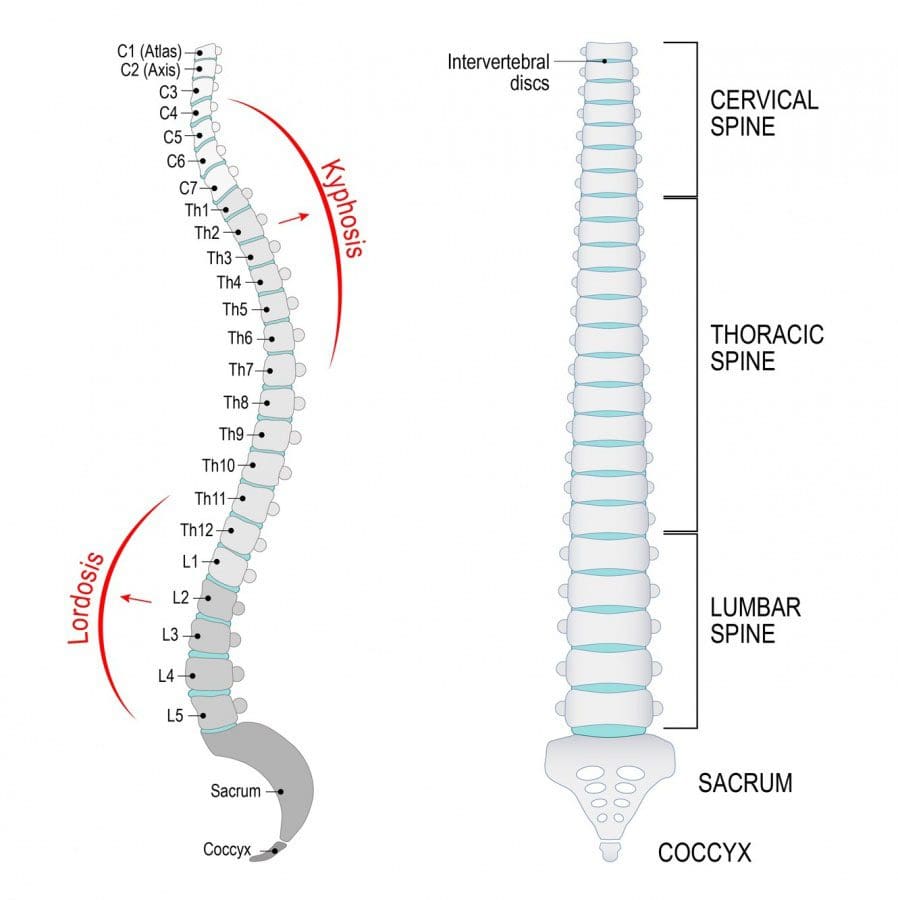
The sacrum forms the back of the pelvis. Along with the coccyx and the two sacroiliac joints make up the pelvic girdle. S1 is at the top of the sacrum and connects to the last lumbar vertebrae L5. Together they create the lumbosacral spine. Where they join forms the lumbosacral curves known as lumbar lordosis and lumbar kyphosis.
The curvature works to support the upper body, weight/force distribution maintains spinal balance and flexibility. Lordosis is the inward curve of the spine, but too much can cause swayback that can be associated with spondylolisthesis. Loss of this curve can cause spinal imbalance and can lead to Flatback syndrome.
Kyphosis is the outward curve of the spine. The location of the sacrum at the intersection of the spine and pelvis means it has an important role in the movement of the low back and hips. The sacrum�s joints help to bear weight and help stabilize the spinal column along with the ligaments, tendons, and muscles help support/stabilize joint movement.
Lumbosacral joint
Joint L5 and S1connect the lumbar spine to the sacrum. The pressure at this meeting point can be massive as the curve of the spine shifts from the lordotic forward curve to a kyphotic backward curve. The L5-S1 region bears weight, absorbs, and distributes the upper body�s weight when moving and resting. Disc herniation and spondylolisthesis are more common at L5-S1 for this reason.
Sacroiliac joints
The sacroiliac joints connect the sacrum to the left and right sides of the pelvis. The range of movement of the sacroiliac joints is minimal compared to other joints like the knees. However, the joints are essential for walking, standing, and stabilization of the hips. Sacroiliitis and sacroiliac joint dysfunction are two spinal disorders related to the joints. Other spinal disorders related to the sacral spine include:
The coccyx commonly known as the tailbone is just below the sacrum. It is smaller than the sacrum and has an important weight-bearing function. It helps supports weight while sitting.An example is leaning back while sitting. This motion and position increase the pressure/weight on the coccyx. An injury in this area can cause tailbone pain. Inflammation of the coccyx�s connective tissue that results in tailbone pain that gets worse when sitting is a common symptom. A traumatic event like a fall or auto accident that causes a tailbone fracture can also cause this pain.
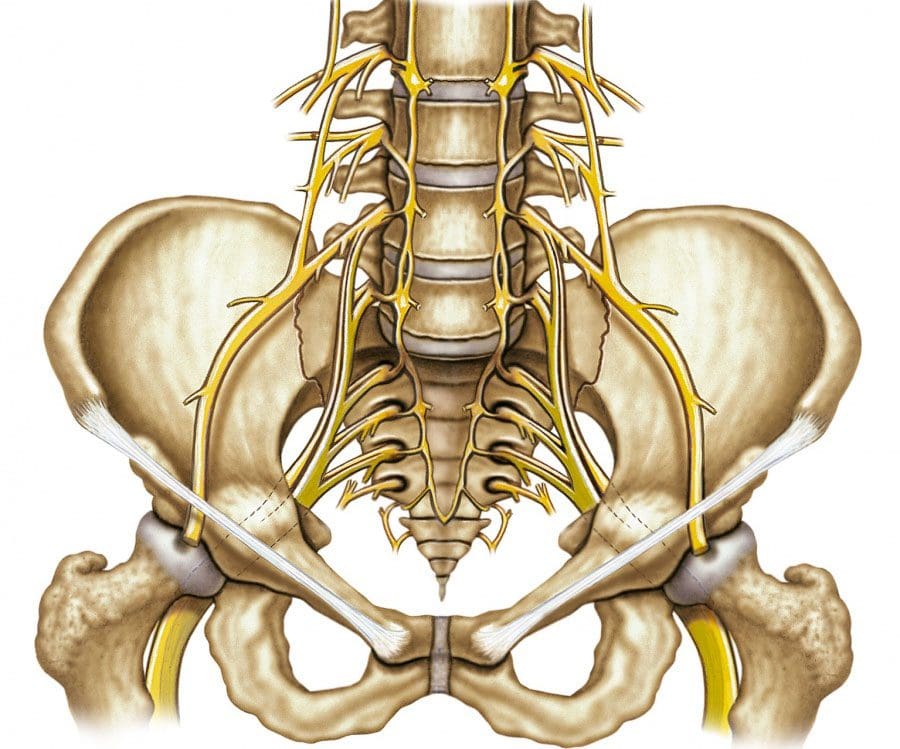
Sacral and Coccygeal Nerves
The spinal cord ends at L1-L2, which branches out into the cauda equina, which is a bundle of nerves that looks like a horse’s tail. In the sacrum, there are sacral nerves known as the sacral plexus. Plexus means a network of nerve structures. The sacral and lumbar plexus compose the lumbosacral plexus. This is where the sciatic nerve, which is the largest nerve in the sacral plexusconverges into the band. Sciatic nerve compression causes a combination of symptoms known as sciatica. It is very well known for causing low back and leg pain.
The coccygeal nerve serves the tailbone. There are five sacral nerves numbered S1 through S5 and are part of the spinal cord.
S1 supports groin and hip function
S2 the back of the thighs
S3 the middle of the buttock area
S4 and S5 the anus and vagina
Injury or trauma to the sacral spine can cause mild stress fractures to severe bone fractures. These fractures can cause sacral nerve compression and intense pain. Symptoms include:
A doctor or chiropractor, physical therapist are excellent sources for information to help prevent sacrum and coccyx pain. These medical professionals will utilize a patient’s medical history, recommend lifestyle changes and injury prevention guidelines.
If at risk of developing osteoporosis then a bone mineral density test could be recommended.
Proper posture must be maintained. Avoid slouching as this places added pressure on the lumbosacral spine and the sacroiliac joints.
Proper body mechanics when engaging in any activity needs to be observed.
Use legstrength to lift objects.
Avoid twisting while lifting or holding heavy objects, as this can cause sprain, strain, or serious injury of the lower spine.
Put on the seat belt. Auto accidents are a major cause of spine trauma. Exercise restraint when driving or riding in any vehicle even a golf cart.
Sciatica Pain Relief
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Acetaminophen, best known as Tylenol, is one of the most common medications for headaches and general pain. More than likely the most common back, neck, and overall pain medication around. However, it is only a pain reducer, and will not reduce inflammation.
Doctors often recommend this medicine before moving on to prescription medication. A member of the analgesic pain reliever class of medications. These can vary in strength along with side effects, but their purpose is to reduce pain. Acetaminophen can be found in over 600 prescriptions and over-the-counter medicines, including certain opioids. Other acetaminophen brand names include:
Tylophen
Tempra
FeverAll
Mapap
Pharbetol
Panadol
Strength and Weakness
When neck or back pain presents, over-the-counter medicines fall into two categories. These are acetaminophen or non-steroid anti-inflammatory drugs also known as NSAIDs. Acetaminophen and NSAIDs like Advil, aspirin both relieve pain. However, non-steroid anti-inflammatories also help in reducing inflammation. Although non-steroid anti-inflammatories have this added benefit, they can also present potential side effects like stomach and gastrointestinal problems.A spinal sprain or strain can cause acute back pain. Acetaminophen is typically recommended for acute back or neck pain and for pain that comes and goes quickly. Individuals that experience periodic pain usually take acetaminophen when the pain flares up. Individuals with chronic spinal pain report acetaminophen help to alleviate/reduce the pain. Many with chronic pain use acetaminophen regularly and not only when the pain presents. This helps manage before pain strikes.
Safety
Acetaminophen is gentle on the stomach, making some individuals preferring it over the non-steroid anti-inflammatories. But just like any other medication acetaminophen has its risks and can cause severe damage if used improperly.
Taking acetaminophen in large doses can cause severe liver damage. The Food and Drug Administration reports that acetaminophen overdoses send over fifty-thousand individuals to the emergency room every year. And over one-hundred Americans die yearly from accidental overdoses.
Using acetaminophen safely means taking no more than 3,000 milligrams a day and no more than 1,000 milligrams at a time. Take extra precautions when taking extra-strength. These can include as much as 650 mg per pill/capsule.Before taking acetaminophen for back and neck pain, talk to a doctor or pharmacist about the proper dosage. And tell the doctor about all the medications being taken including natural herbs and holistic. Another reason for telling the doctor is that many other medications have acetaminophen included without you knowing it. Part of the discussion should include alcohol consumption. This can elevate the risk of negative reactions.
Resources
If non-pharmacological treatments/therapies done for at least 4 months prove ineffective then an acetaminophen regimen could be a safe and effective part of a back and neck pain treatment plan. While this medicine is one of the most common treatments, it is not without risks and side effects. Talk to a doctor or pharmacist about all the medications and supplements to ensure the regimen supports health for the long-term. To learn more along with safety information go to Acetaminophen Patient Guide.
Severe Back Pain Chiropractic Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Women experiencing low back pain will find there are a variety of possible causes. Lower back pain can stem from the reproductive system or the spine itself. Finding the possible cause of low back pain can be difficult to diagnose. As well as, pinpointing the pain can be a very challenging task. Women wonder how it’s possible to mistake menstrual cramps for back pain and then it happens to them. There are certain conditions that make the low back and core region a central location of continual pain. And unfortunately, women could be more susceptible.
Most individuals will experience low back pain at some point during their life. However, there is a slight prevalence and is more common in females than males across all ages. Low back pain in women increases with age. A research comparison studying middle-aged individuals reported an increase of low back pain in females versus males post-menopause. Some possible low back pain causes include.
Menopause and Hormone Issues
Chronic lower back pain is one of the most reported musculoskeletal issues women face during menopause. About sixty-seventy percent of perimenopausal women present symptoms associated with estrogen deficiency. And over half in perimenopause report chronic musculoskeletal pain. Many of these studies show increasing menopausal symptoms and the correlation to chronic low back pain symptoms.
Menstruation and Uterine Dysfunction
Dysmenorrhea is a uterine dysfunction that involves frequent and severe cramping during menstruation, which often leads to low back pain. The condition is classified as primary or secondary. Both types include low back pain as a common symptom.Primary dysmenorrhea starts when a woman begins menstruation and continues throughout their life. Intense contractions can cause continual and severe menstrual cramping. Secondary dysmenorrhea usually starts later and is caused by another condition like endometriosis or pelvic inflammatory disease.
Endometriosis
Endometriosis is a condition that can contribute to back pain in women. Tissue that behaves like endometrial tissue begins to grow outside of the uterus, in the pelvic cavity or other areas. The new tissue responds to the body’s hormonal changes and can cause swelling, pain, spotting, and bleeding. Endometriosis growths bleed monthly as well. Without a place for the blood to go, the excess irritates and inflames the surrounding tissue.
The condition can cause heavy periods, chronic pain, and scar tissue build-up. Symptoms can present at any menstrual cycle stage. Pelvic pain that runs down the legs is common. Some women have also reported throbbing, shooting pain that can be mild to severe. Symptoms include:
Abdominal pain
Low back pain
Pain when walking or standing
Pain during ovulation
Pain when urinating
Urinary urgency
Pelvic inflammation
Constipation
Pain during intercourse
Bowel movement pain
Rectal pain that radiates
Pain caused by scar tissue build-up within the bladder, fallopian tubes, bowels, and ovaries
Chronic fatigue
Endometriosis can be diagnosed by a doctor during an initial pelvic exam. Further imaging tests to assist in the identification could be requested.
Spinal Issues
The reproductive organs can sometimes contribute to back pain. However, women can also be susceptible to degenerative conditions that affect the spine’s structure. Low back pain is common with an average patient experiencing one to two episodes a year. Low back pain can start in early adulthood and become a chronic problem that can be triggered by various events or activities. Most back pain issues are resolved within six weeks. This is known as acute low back pain. When the pain doesn’t stop for more than 12 weeks it is considered chronic lower back pain.
Postmenopausal Compression Fractures
Around twenty-five percent of women will go through a vertebral compression fracture of the middle or lower spine. The risks increase with age, with around a 40 percent chance at 80 years of age. Small cracks in the vertebrae can cause severe disability and limit function. Osteoporosis is the most common cause of vertebral compression fracture/s. Postmenopausal women are at an increase of developing osteoporosis. This comes from hormonal changes that decrease bone mineral density, leaving the bones open to fracture.
Spondylolisthesis
This is when one vertebral body, or the thick oval bone segment in front of the vertebra, slips against an adjacent body. The result is pain or mechanical symptoms. The pain can spread throughout the spine to the hip, buttocks, into the legs, and possibly the foot. The condition can be congenital, from an unknown cause, or acquired. There is some research on childbirth and hysterectomies putting women at risk for spondylolisthesis.
It is common in the lumbar spine/lower back, but can also present in the cervical spine/neck region. The thoracic/middle spine is extremely rare except in trauma cases. The thoracic spine is the longest region of the spine. It is between the cervical and lumbar regions. One cause of the increased pain is longer times spent sitting in chairs that are not ergonomic. A second is being confined to smaller workspaces. The key is to get up and move around or use a sit-stand desk to alternate sitting and standing. Irregular and localized low back pain is typical for low back spondylolisthesis. The pain usually worsens when the area/region is flexed or directly touched.
Piriformis Syndrome
Back pain sometimes isn�t back pain, but piriformis syndrome. The piriformis muscle is a small muscle that extends from the lower spine to the top of the femur. It can involuntarily contract and compress or irritate the sciatic nerve. The muscle helps rotate and turn the leg and foot outward. Symptoms are consistent with sciatica. It typically presents with buttock pain that shoots, aches, or throbs along the leg�s backside, thigh, calf, and foot. Tingling along the nerve along with numbness is common. Causes include:
Buttock injury
Hip injury
Weight training specifically the gluteal/buttock, hips, and hamstrings
Sitting for a long time – Examples include truck drivers, desk job workers, etc.
Damage to the piriformis muscle
Sciatic nerve wraps around the piriformis muscle
Sacroiliac Joint Dysfunction
Sacroiliac joint dysfunction involves inflammation of the joints, located at the connection of the pelvis and lower spine. It can present as low back or buttock pain that radiates down the leg/s. The pain worsens when climbing stairs or standing for an extended amount of time. Sacroiliac joint dysfunction can be tough to diagnose, as it is often mistaken for other low back pain causes.
SI joint dysfunction causes:
Pregnancy – the increased weight and altered movement/s can cause additional stress and wear.
Joint infection – in rare cases, the joints can be subject to infection.
Arthritis – the joints can develop arthritis from normal wear and tear.
Traumatic Injury – the joints can be injured from a forceful impact from a fall or auto accident.
Most cases do not end up requiring medication or surgery. It is when the pain lasts more than six weeks that there could be something more taking place like neurologic symptoms or other conditions, spinal or otherwise.
Personalized Chiropractic Spine Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
A doctor, chiropractor, or physical therapist could recommend therapeutic stretches along with exercises as part of a sacroiliitis or sacroiliac joint pain treatment plan. Sacroiliitis refers to inflammation in one or both of the sacroiliac joints. This could be caused by:
Pregnancy
Injury
Infection
Arthritis
Ankylosing spondylitis
Sacroiliac joint pain is a symptom related to sacroiliac joint dysfunction. The symptoms of sacroiliitis and sacroiliac joint pain can be felt in the lower back, buttocks, hips, and legs. These symptoms can be similar to sciatica and can mimic other lower back disorders.
Some of the stretches and exercises included are common for treatment plans for various low back conditions/problems. Talk with a chiropractor or doctor to get their recommendation prior to starting any exercise or stretching program.
Stretches
Piriformis stretch
The piriformis muscle extends over the hip and can aggravate the sacroiliac joint when it becomes tight. To help stretch the muscle:
Lie on back with knees bent
Feet flat on the floor
Slowly raise the right leg
Bring the right knee toward chest
Gently pull the leg in until there is a comfortable stretch in the buttock
Exhale during the stretch movement
Hold the stretch for 30 seconds
Lower leg
Repeat on the left leg
Repeat each side 3 times daily, as needed
The stretch helps the muscle fibers to lengthen/elongate and relax.
Trunk rotation
Trunk rotation increases flexibility in the low back and hips. This can help relieve pressure on the sacroiliac joints. To do this stretch:
Lie on back with knees bent
Feet flat on the floor
With knees together
Slowly rotate to one side
Feet, hips, and back should stay on the floor
Hold 3-5 seconds
Move knees to the opposite side
Repeat 5-10 times on each side
Bridge
This is a stretch that strengthens the muscles in the lower back, buttocks, and hips.
Lie on back with arms at side
Knees should be bent, and feet flat on the floor
Slowly raise hips while squeezing buttocks and hamstrings
Hold raised position for 5 seconds
Repeat 10 times
Water Therapy and Yoga Exercises
Aquatics and yoga are a gentle and natural form of exercise that is recommended for staying active. Talk to a doctor before starting any exercise program. Aquatic therapy, known now as hydrotherapy/water therapy, is one of the gentlest forms of exercise and is highly effective.
Exercising in water creates an almost weightless environment without gravity. Hydrotherapy uses the resistance from the water to improve strength and flexibility without straining the muscles. Regular exercise can cause pain by placing added pressure on the sacroiliac joints. Water therapy conditions the spine and hip muscles without generating muscle stress. Another option for individuals with back pain is yoga. The following poses are recommended and beneficial for the sacroiliac joints:
Child�s pose
This pose stretches the hips and thighs and is a great yoga pose for beginners.
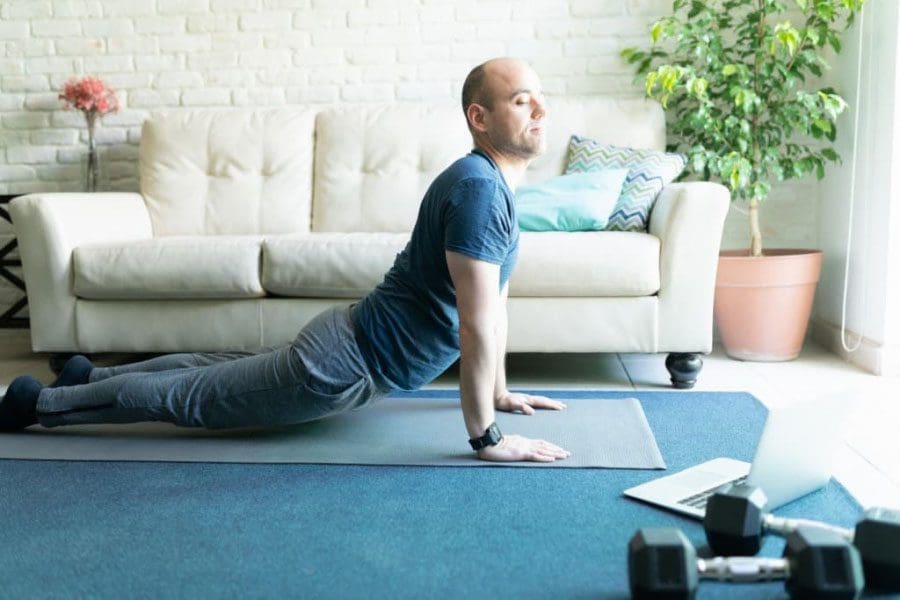
Cobra
Cobra pose can help strengthen and stabilize the sacroiliac joints.
Lie flat on the stomach
Hands beneath the shoulders
Slowly push up as far as the arms extend
Bring upper body off the ground
Keep the pelvis and legs on the floor
When extended, be sure low back and buttocks are relaxed
Hold for 15 to 30 seconds
Gently lower to the floor
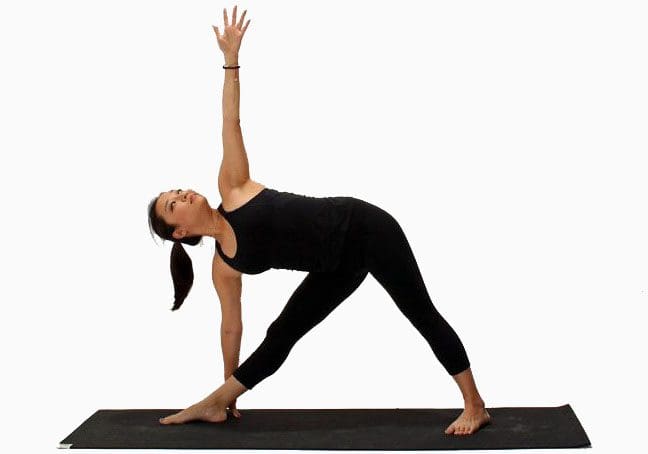
Triangle pose
Triangle pose helps to strengthen the sacroiliac joints and makes them less susceptible to pain. However, this pose involves twisting, so make sure to do this pose only when the joints are stable and pain-free.
Before stretching and exercise
Before starting any stretching or exercise program, check with a doctor or chiropractor, if the joints are able then the stretching/exercise could begin right away. However, in most cases, a doctor will refer the patient to a physical therapist or chiropractor to create a customized exercise and stretching plan. The therapist will show exactly what activities will strengthen the joints and how to do them properly and safely. These movements can help condition the spinal and abdominal muscles. This can help prevent future episodes of back pain.
If an individual just had surgery for sacroiliac joint pain, the surgeon more than likely prescribed a customized rehabilitation stretching/exercise program. Follow instructions, and get the surgeon�s approval before engaging in anything outside of the plan.
Staying fit safely
When dealing with sacroiliac joint dysfunction or sacroiliitis, physical activity may need to be redefined after treatment. As regular exercise could mean strenuous activity and could do more damage. Exercises like heavy weightlifting, contact sports, and intense biking could place excessive pressure on the joints. A doctor or chiropractor will offer the best stretching and exercises for every individual.
Physical activity combined with gentle stretching and conditioning exercises can effectively reduce low back and hip pain. Talk to a doctor, chiropractor, or physical therapist about incorporating healthy exercise into a daily regimen. For some, the workout might not feel like there’s anything going on, but the effects on the pain will be.
Chiropractic Hip Pain Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Self-care practice when back pain flares up is a way for individuals to give themselves self-therapy attention in the midst of crazy schedules. It�s never been more important than now to be able to take care of oneself when back or any type of pain presents. For a few minutes, daily physical and mental health activities can make a difference.
Self-care is the ability to self-manage pain and take care of our constantly changing needs daily. Regular self-care is essential to our families, and friends well being. Pain is emotionally and physically taxing on the body. It brings and encourages mental/emotional and physical balance, which helps, especially when there is a condition that causes pain.
There is a connection between self-care and chronic pain that is being studied currently. Studies are finding that individuals practicing self-care in addition to regular medical care have significant reductions in pain and reduction in disability. So, alleviate back pain with a few self-care tips.
Hot Bath
Hydrotherapy better known as a hot bath can provide pain relief. Adding Epsom salt for these baths contains magnesium which can help relax muscles and the body.
Music can be an effective way to ease back pain. Research has shown that music can be a complementary treatment when addressing chronic pain. It helps especially when an individual is experiencing back pain along with a low/negative mood.
More Sleep
Poor sleep has been proven to increased back pain. Getting the proper amount of sleep is essential in addressing pain. Healthy sleep hygiene and bedtime routines will significantly help with the body�s recovery, healing, and general health.
Yoga
Yoga stretching is highly effective in relieving and avoiding/preventing back pain completely. Poses like the cat, cow, triangle, and child�s pose will generate relief along with improving balance.
Healthy Diet
Diet and lifestyle changes have been proven to reduce inflammation, which can cause chronic pain. Go with whole foods that are minimally processed. This will help reduce inflammation. Healthy weight along with healthy body mass keeps the spine healthy and free of the added stress from the weight. Therefore a sensible diet is the single most important factor in weight loss.
Connection
Isolation can exacerbate pain. Loneliness can be a significant risk factor in the development of pain, and with time, depression, and fatigue. Simply reaching out and connecting with loved ones, friends, co-workers, etc, could help in soothing the pain away.
Mindfulness
Mind-body therapy as a method to treat pain has been proven in various studies. Individuals taking part have reported significantly lower pain than those who only received traditional medical care. What happens is you are training your mind senses to be present and focused on what you are doing, the surroundings, etc, and not focusing, and getting lost in the pain. However, sitting down and meditating is not for everybody.
Drink the Proper Amount of Water
Hypohydration, which is not enough water can increase pain. Therefore, drink up.
Stretching
Stretching will definitely decrease pain and allow for practicing mindfulness. It doesn’t matter when the stretching happens so long as, the individual sticks with it and continues development to further their ability and flexibility. Core abdominal exercises are very helpful for back pain and strengthening.
Go Outside
Many of us know that getting out in nature feels good mentally and physically, and it can actually relieve pain, too. Nature therapy or ecotherapy has shown to improve the psychological and physiological symptoms associated with chronic pain. Connecting to nature can have tremendous benefits for optimal health.
Heat Therapy
Heat, whether from a topical agent or heating pad can soothe the mind and spine. Check with a doctor before trying any type of heat treatment.
Frequent Breaks
Taking breaks is essential for the mind in keeping stress levels balanced. This can lessen back pain. Just a few minutes to stop whatever and take a few minutes for yourself and your health. Taking proper physical and mental rests throughout the day to stretch out, move around, and do something else. This will help keep things open and fresh, as opposed to going through the same thing over and over with less than optimal results. The mind needs to reflect.
Go Easy
Go easy on yourself, this is probably the most important form of self-care. If the pain is too intense, do not force yourself to work through it. Use the various techniques mentioned and go slowly, with the fundamentals of combating pain and chronic pain. Slow down whenever you feel the need.
Lower Back Pain Skating Boarding Injury Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine