The body is held up by skeletal joints that keep the body upright and provide everyday movements for the body to go anywhere at any time. The musculoskeletal system provides the muscles, tissues, and ligaments that encase the skeletal joints protecting them from unknown factors that can cause harm to the body. The internal organs also have a purpose in the body as they help provide the nutrients and necessary hormones to the muscles and joints that need these nutrients to function. When environmental factors affect the body, either internal or external, it can cause the body to become dysfunctional and even cause unwanted symptoms that affect the internal organs that correspond to the muscles suffering. Today’s article looks at pelvic pain, how gut disorders are associated with pelvic pain, and how viscerosomatic pain affects the pelvis. We refer patients to certified, skilled providers specializing in osteopathic and gut treatments that help those with gut disorders and pelvic pain issues. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Pelvic Pain?
Have you been experiencing gut issues that are affecting your pelvic region? Has your gut been feeling inflammatory effects? Have you noticed that you need to go to the bathroom more frequently than usual? Many of these symptoms are some of the signs that are associated with pelvic pain. Research studies have defined pelvic pain as disabling, chronic, and persistent pain that commonly affects women. Pelvic pain can range from acute to chronic depending on how severe the pain affects the pelvic region of the body. Additional research studies have mentioned that pelvic pain in its chronic form can become a multifactorial disorder that can cause pain in the gastrointestinal, pelvic musculoskeletal, or nervous system, making the immune, neurological, and endocrine metabolism dysfunctional. When pelvic pain begins to affect the gastrointestinal system, it can lead to various gut disorders that can cause the pain to become worse if it is not treated.
How Do Gut Disorders Associate Pelvic Pain?
Research studies have mentioned that since pelvic pain is a multifactorial disorder, it can cause pain to arise in the internal organs in the gastrointestinal system. When pelvic pain starts to affect the gastrointestinal system, it can cause the development of gut disorders to affect the body further. When gut disorders co-exist with pelvic pain, it can cause an enhancement to the overall pain symptoms that are becoming the result of viscerosomatic dysfunction through the cross-organ sensitization mechanisms. Additional information studies have mentioned that gut disorders like IBS (irritable bowel syndrome) can cause changes in thermal/visceral pain sensitivity that overlap in the lower body’s pelvic region, further enhancing rectal/thermal pain. This can cause a person to become miserable and even affect their quality of life since they are suffering from so much pain.
Visceral Afferent Nerves Being Affected By Pelvic Pain-Video
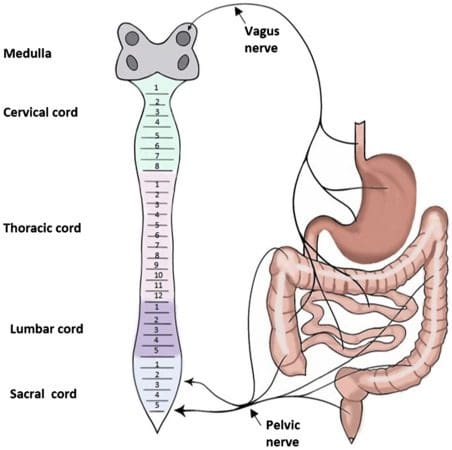
Have you experienced gut issues like IBS (irritable bowel syndrome), inflammation, or IBD (inflammatory bowel disease)? Have you felt pain in your pelvic region constantly? Has the pain-affected certain areas in your body, not just your pelvis? If you have these symptoms, it might be due to your visceral nerves being involved. The video above explains what the visceral afferent nerves from the pelvic region are doing to keep the body functioning in the lower extremities. The visceral afferent nerves become aggravated by environmental factors affecting the body, including the gut system. Symptoms of inflammation and gut disorders from persistent aspects of many forms of stress or trauma can cause visceral pain to affect the body, thus causing pelvic pain, gut issues, lower back pain, and other body pains.
How Viscerosomatic Pain Affects The Pelvis
The body’s viscerosomatic pain can be complex since the organs also affect the corresponding muscles. The way the pain is described in the body from viscerosomatic pain ranges from dull to excruciating pain. Research studies have mentioned that the burden of viscerosomatic pain emanates from the internal thoracic, pelvic, and abdominal organs associated with the muscles. For visceral pain to affect the pelvic region, research studies have shown that the nociceptive pain from the pelvic area is usually visceral from the results from the pelvic organs that are poorly localized and can overlap with the somatic sensory tracts that are located in the spinal cord. When this happens, it can cause significant discomfort to the pelvic organs in the body and affect the individual with excruciating painful symptoms.
Conclusion
The body provides everyday movements held by the skeletal joints that help the body go anywhere. While the musculoskeletal system and the internal organs help give the muscles, tissues, ligaments, and nutrients the body needs to function. When environmental factors affect the body, it can lead to various issues that cause gut disorders and even pain in the pelvic region, known as visceral pain. Visceral pain is a complex disorder since the affected organs also affect the corresponding muscles. For visceral pain to affect the pelvic area, it can lead to dull excruciating pain in the pelvic organs and affect the individual. Visceral pain can also overlap the sensory somatic tracts in the spinal cord, causing unbearable painful symptoms to the body while inflammatory issues in the gut system are developing. When people realize that the pain is affecting them, they can start to find treatments from their specialized providers to help alleviate their pain.
References
Dydyk, Alexander M, and Nishant Gupta. “Chronic Pelvic Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Nov. 2021, https://www.ncbi.nlm.nih.gov/books/NBK554585/.
Grinberg, Keren, et al. “New Insights about Chronic Pelvic Pain Syndrome (CPPS).” International Journal of Environmental Research and Public Health, MDPI, 26 Apr. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7246747/.
Origoni, Massimo, et al. “Neurobiological Mechanisms of Pelvic Pain.” BioMed Research International, Hindawi Publishing Corporation, 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4119661.
Udoji, Mercy A, and Timothy J Ness. “New Directions in the Treatment of Pelvic Pain.” Pain Management, U.S. National Library of Medicine, Sept. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3979473/.
Verne, G Nicholas, et al. “Viscerosomatic Facilitation in a Subset of IBS Patients, an Effect Mediated by N-Methyl-D-Aspartate Receptors.” The Journal of Pain, U.S. National Library of Medicine, Sept. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3489925/.
Yuan, Tian, and Beverley Greenwood-Van Meerveld. “Abdominal and Pelvic Pain: Current Challenges and Future Opportunities.” Frontiers in Pain Research (Lausanne, Switzerland), Frontiers Media S.A., 4 Feb. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8915637/.
The body is a marvelous functional machine that requires constantly moving worldwide. The body can do everyday movements from the head to the feet and be in weird positions without feeling pain. However, ordinary factors like natural aging, wear and tear, and issues affect the body over time. When these factors start to affect the body, they can cause unwanted symptoms that can inflict pain on specific areas around the body. Some areas that suffer pain include the hips, lower back, neck, the body’s internal systems, and the spine, causing the individual to be miserable. Luckily many treatments do relieve pain in the body and help dampen the effects of the unwanted symptoms that are hindering the individual. Today’s article focuses on hip pain, its symptoms, and how decompression therapy can help many individuals suffering from hip pain. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Hip Pain?
Are you feeling stiffness from your lower back and hips? Do your hips hurt after falling due to playing sports? How about pain from the lower back to the hips down to the feet? You might be experiencing hip pain. Research studies have stated that hip pain can be associated with many factors that can cause many individuals to be in distress, impair their daily activities, and affect their quality of life. Hip pain can be associated with simple movements that are damaged, like sitting and standing, which can be hard after a while. Other associations that hip pain can occur can be lower back pain, neuropathies, herniation, or chronic pain. According to research studies, hip pain is considered a musculoskeletal disorder. It shows that posterior hip pain in adults is caused by osteoarthritis or traumatic causes like sacral stress fractures that can affect the hips. This musculoskeletal disorder can become a problem for many older adults suffering from hip issues.
The Symptoms
Research studies have found that hip pain is a musculoskeletal complaint affecting young and old adults. Since hip pain is associated with various chronic issues, it can cause many individuals to be miserable and be in constant pain. For adults, hip pain can be one of the issues for those suffering from osteoarthritis in the anterior hip region. As research shows, in the posterior hip region, hip pain can be associated with chronic conditions like piriformis syndrome and lumbar radiculopathy that are centralized in the lower back. Other symptoms that hip pain cause on its own do associate with other chronic conditions, including:
Are you experiencing discomfort from your hips while sitting or standing? How about sharp, throbbing pain coming from your lower back and affecting your hips and legs? Do you feel tenderness and swelling on your joints? These symptoms are various forms of hip pain, and lumbar traction can help lower hip pain symptoms. The video above mentions how to prepare for lumbar traction therapy and how it can alleviate symptoms caused by hip pain. Lumbar traction helps compressed disc in the lumbar region of the spine to be restored to its original state and even takes the pressure off the sciatic nerve and other nerve roots that are causing hip pain to the body. Utilizing traction therapy increases the disc height and allows the lumbar spinal discs to be rehydrated again. Suppose you want to learn more about lumbar traction or decompression and how it can benefit you? In that case, this link will explain what decompression does for the lumbar area in the spine and provide relief from hip pain and its associates.
How Decompression Therapy Helps With Hip Pain
Since hip pain is associated with various other conditions that can affect the body, the most common condition that the body has suffered from is low back pain. There are ways to treat hip and low back pain; some individuals utilize heat and ice to neutralize the pain to go away, and others use chiropractic therapy to get the joints to realign themselves. One of the treatments used to relieve hip and low back pain is decompression therapy. Research studies have found that decompression therapy is safe and effective in helping to improve the blood circulation to the hips to provide relief to the hips. Since hip pain is associated with low back pain, decompression allows the herniated discs to be taken off the nerves surrounding the hips and provide pain relief. Other research studies show that traction is used to create negative gravity pressure to help reduce the pressure that is causing pain to the soft tissues and the nerve roots. This negative gravity allows the spine to separate and create more height for the disc to rehydrate while relieving the individual.
Conclusion
Overall the body is a marvelous machine that has the ability to move without pain. When issues start to affect the body, like the hips and lower back, it can cause the individual to suffer from various forms of pain. Since hip pain is associated with low back pain, it can lead to other chronic issues like sciatica or osteoarthritis, affecting the joints and causing them to swell. Treatments like decompression or traction therapy are used to alleviate the pain caused by the hips or lower back. When people incorporate decompression or traction into their wellness journey, they relax a bit as they are laid down and have their spine stretched slowly. This will cause them relief and take the pressure off the nerve roots that are sending pain signals to the brain. This ensures them that they can take back their lives pain-free.
References
Ahuja, Vanita, et al. “Chronic Hip Pain in Adults: Current Knowledge and Future Prospective.” Journal of Anaesthesiology, Clinical Pharmacology, Wolters Kluwer – Medknow, 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022067/.
Battaglia, Patrick J, et al. “Posterior, Lateral, and Anterior Hip Pain Due to Musculoskeletal Origin: A Narrative Literature Review of History, Physical Examination, and Diagnostic Imaging.” Journal of Chiropractic Medicine, Elsevier, Dec. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5106442/.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Lee, Yun Jong, et al. “Causes of Chronic Hip Pain Undiagnosed or Misdiagnosed by Primary Physicians in Young Adult Patients: A Retrospective Descriptive Study.” Journal of Korean Medical Science, The Korean Academy of Medical Sciences, 11 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6300658/.
Wilson, John J, and Masaru Furukawa. “Evaluation of the Patient with Hip Pain.” American Family Physician, U.S. National Library of Medicine, 1 Jan. 2014, https://pubmed.ncbi.nlm.nih.gov/24444505/.
Healthy hips are necessary for standing, sitting, walking, running, bending, twisting, lifting, etc. Hip problems can seriously interfere with everyday activities. Out of alignment hips don’t just cause pain and soreness in the hip area but can radiate to other body areas. When the hip joint is out of alignment, the rest of the body has to start compensating for the misalignment, which can cause chronic pain in the back and/or legs.
Out of Alignment Hips
Discomfort and soreness begin as occasional but can quickly become regular. Individuals may also begin to limp when they walk, have a reduced range of motion in the hips, and pain that escalates with physical activity and improves with immobility/rest. Out of alignment hips can be caused by:
Lifting incorrectly
Repetitively carrying heavy loads on one side of the body places uneven pressure on the pelvis, causing an imbalance.
Performing repetitive motions that begin to stress the joint
If the legs are different lengths, this can cause the hips to go out of alignment. Using a foot wedge/foot orthotic in the shoe can remedy the situation.
Functional Leg Length Discrepancy
Functional leg length discrepancy is a common cause of hip misalignment, meaning that leg length is equal, but the individual is doing something to cause the hips to go out of alignment. It usually involves posture, standing, walking, sitting, lifting, and carrying improperly or awkwardly and repetitively could create functional leg length discrepancy.
Scoliosis
Scoliosis is only one cause of hip misalignment. It is not likely that an individual has scoliosis if they are an adult and have not previously been diagnosed with the condition. If a child has what looks like a misaligned hip, it is recommended to take them to get tested for scoliosis. Most children with the disorder will outgrow it, but they need to be monitored by a medical professional.
One of the most prominent signs that it is a hip problem is the presence of groin pain. Groin pain can radiate downward toward the buttocks, front of the thighs, and knees. The hip joint is located behind the groin; pain usually means the hip is the root cause.
Chiropractic Decompression
A chiropractic examination can identify uneven hips. Chiropractic and motorized spinal decompression can reset the hips to their proper position. A chiropractor will be able to rebalance the hips and help avoid invasive surgical treatments and long-term rehabilitation.
DRX9000 90 Seconds Spinal Decompression
References
Battaglia, Patrick J et al. “Posterior, Lateral, and Anterior Hip Pain Due to Musculoskeletal Origin: A Narrative Literature Review of History, Physical Examination, and Diagnostic Imaging.” Journal of chiropractic medicine vol. 15,4 (2016): 281-293. doi:10.1016/j.jcm.2016.08.004
Jones HR, Burns TM, Aminoff MJ, Pomeroy SL. Pain. Chapter: Diagnosis of Low Back, Buttock, and Hip Pain. Netter Collection of Medical Illustrations: Spinal Cord and Peripheral Motor and Sensory Systems, Section 8, 201-224.
Khamis, Sam, and Eli Carmeli. “A new concept for measuring leg length discrepancy.” Journal of orthopedics vol. 14,2 276-280. 27 Mar. 2017, doi:10.1016/j.jor.2017.03.008
Miyagi, Masayuki, et al. “Hip-spine syndrome: cross-sectional-study of spinal alignment in patients with coxalgia.” Hip international: the journal of clinical and experimental research on hip pathology and therapy vol. 29,1 (2019): 21-25. doi:10.1177/1120700018803236
Nunes, Guilherme S et al. “Acute Effects of Hip Mobilization With Movement Technique on Pain and Biomechanics in Females With Patellofemoral Pain: A Randomized, Placebo-Controlled Trial.” Journal of sport rehabilitation vol. 29,6 707-715. 18 Oct. 2019, doi:10.1123/jsr.2018-0497
The hips are highly active joints. Hip sprains are rare but do occur. A hip sprain is caused by tearing or stretching the ligaments that surround the hip and join the bones to each other. This is different from a hip strain, which is an injury to the muscles and is generally caused by over-use of the hip flexor muscles and tendons, causing them to tear. Hip sprains usually happen after a fall or a sudden twisting motion, which can occur during sports or an accident.
Individuals involved in sports that require quick stops, body shifting, and sudden direction changes, like soccer, football, basketball, tennis, volleyball, etc., have an increased risk. Most hip sprains can be effectively treated with conservative treatments like self-massage, rest, ice, and nonsteroid anti-inflammatory medications. For more severe cases, physical therapy and chiropractic can treat the condition.
Hip Sprain Symptoms
Tenderness in the hip increases when lifting the thigh.
Cramping sensation/s in the muscles of the upper leg.
Swelling in the hip or thigh
Bruising in the hip or thigh.
Sudden pain in the hip or pelvis.
Sharp pain in the hip or pelvis.
Pain that worsens when walking, running, or stretching the hip muscles.
Loss of strength in the front of the groin.
Tugging or pulling sensation.
Limping.
Diagnosis
The doctor or chiropractor will:
Look into medical history.
Inquire about symptoms.
Inquire about activities that could cause symptoms.
Perform a physical examination.
Ask the individual to perform a variety of movements to determine what type of injury has been sustained.
Pain in one or both hips might not have anything to do with the hips but a pinched nerve root in the lower back.
Sciatica can develop when certain nerve roots in the lower back are irritated or compressed, causing symptoms to travel down the sciatic nerve and radiate around the pelvis and leg.
X-rays can help rule out hip stress fractures, which can have similar symptoms.
MRI or CT scans are used to see if any soft tissue damage has occurred.
Hip Sprain Treatment
Treatment usually begins with over-the-counter pain medications and anti-inflammatories to reduce swelling and relieve pain.
Resting the hip will help prevent further damage.
Applying ice will help prevent tissue damage and reduce swelling.
It is recommended to use an ice pack several times a day for the first 48 hours after an injury.
Once the swelling goes down, a chiropractor and physical therapy team will create a personalized treatment plan that includes:
Adjustments.
Exercise therapy.
Posture training.
Stretching.
Massage.
Treatment/Rehabilitation Objectives
Reduce inflammation.
Relax muscle spasms.
Strengthen weakened muscles.
Improve joint mobility.
Individuals will be shown how to prevent the risk of sprains in the future. This includes:
Avoiding exercising when the body is tired
Wearing proper footwear and protective equipment
Warming up properly before exercise/physical activities.
Depending on the severity of the sprain, surgery could be the last resort to repair the ruptured or torn ligaments.
Body Composition
Realistic Goals
Not seeing results after putting in the work through exercise and diet can be frustrating. Setting realistic goals can help when results are not showing.
Realistic Fat Loss
Do not expect actual fat loss without being in a caloric deficit.
The body needs to use more energy than the amount of food/energy taken in; otherwise, excess energy/food gets stored, primarily as adipose tissue.
There are caloric deficit variations, but most doctors, dieticians, trainers, and fitness experts agree that a caloric deficit of around 500 calories a day that equals to about 3,500 calories a week will result in a pound of fat loss per week.
One pound of fat a week lost might seem slow, but the one pound of fat is a real pound removed.
The long-term goal is not to fall back into unhealthy habits and develop and maintain new healthy ones.
References
Brantingham JW, Globe GA, Cassa TK, et al. A single-group pretest posttest design using full kinetic chain manipulative therapy with rehabilitation in the treatment of 18 patients with hip osteoarthritis. Journal of Manipulative and Physiological Therapy 2012; 33(6): 445-57.
Kamali, Fahimeh and Esmaeil Shokri. The effect of two manipulative therapy techniques and their outcome in patients with the sacroiliac joint syndrome. Journal of Bodywork and Movement Therapies. 2012; 16: 29-35.
McMorland G, Suter E, Casha S, du Plessis SJ, Hurlbert RJ. Manipulation or microdiscectomy for sciatica? A prospective randomized clinical study. Journal of Manipulative and Physiological Therapeutics. 2010; 33(8): 576-584.
Tibor, Lisa M, and Jon K Sekiya. “Differential diagnosis of pain around the hip joint.” Arthroscopy: the journal of arthroscopic & related surgery: official publication of the Arthroscopy Association of North America and the International Arthroscopy Association vol. 24,12 (2008): 1407-21. doi:10.1016/j.arthro.2008.06.019
Wedro, Benjamin. “Hip Pain: Causes, Symptoms, Treatment Information and Diagnosis-eMedicineHealth.” http://www.emedicinehealth.com/hip_pain/article_em.htm.
The body is a connected whole and more than just separate parts and regions. When back pain presents, it might not be the back muscles or spine but could be tense, tight hips, and hamstrings causing low back pain. How it happens, how to stretch and loosen up, and target these areas could help alleviate the pain.
The Hips and Hamstrings
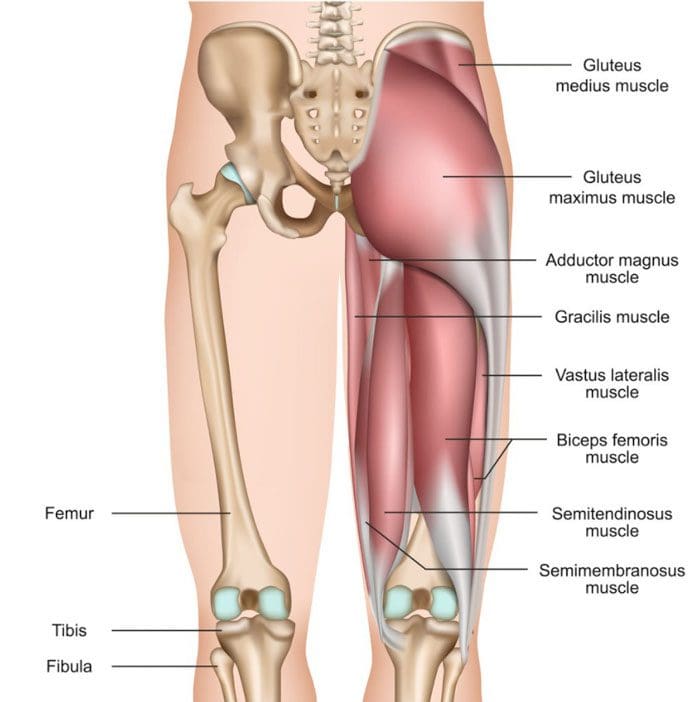
When the hip flexors and hamstrings become tense, the tightness can alter the pelvic alignment. This affects spinal alignment leading to discomfort and low back pain. The hip flexors are a group of muscles around the front of the hips, and they activate when moving the leg and knee upward. The hamstrings are the muscles in the back of the thighs that allow for flexion of the knees and hip extension. Muscle tightness in the hips and/or hip joint stiffness can also contribute to low back pain. Not being able to rotate, flex, or extend the hip forward or backward can affect:
Walking
Running
Swinging
Twisting movements
This increases mechanical strain on the lower back.
Losing the ability to function through the entire length of motion can also indicate muscle weakness and a lack of joint movement where the joint around the muscle becomes stiff. This can be caused by:
A lack of movement
Arthritis
Age-related changes
Stretching and Treatment
Stretching exercises can be the first line of treatment. It is recommended to start with gentle stretches targeting these areas. What works best for the individual is the stretch they are comfortable repeating enough to make a difference. Warming up the muscles first will generate the best results. An easy place to begin is a gentle forward fold stretch.
Stand up straight, or sit with the legs extended out in front.
Then, reach with the fingers toward the toes. Don’t worry if you can’t reach them.
If the stretching does not bring relief, it is recommended to progress to a personalized treatment and stretching program with a chiropractor or physical therapist. Chiropractic and physical therapy can relieve the problems without medication, injections, or surgery and provide lifelong techniques for maintaining optimal flexibility, mobility, and strength. The hands-on treatment loosens and relieves the tense tightness, reinforcing the flexibility and range of motion. Treatment includes:
Joint mobilization to the hips and spine.
Soft tissue mobilization.
A personalized strengthening program with stretches and exercises that target the specific muscles.
Health coaching.
Anti-inflammatory diet recommendations.
Body Composition
Monounsaturated Fats
Monounsaturated fat is considered healthy fat. This type of fat makes up a significant component of the Mediterranean diet. Studies have shown monounsaturated fats like extra-virgin olive oil can help prevent adverse events related to cardiovascular disease. A meta-analysis evaluating diets high in monounsaturated fats indicated a significant reduction in:
Triglycerides
Bodyweight
Systolic blood pressure in individuals with type II diabetes.
A significant increase in HDL or good cholesterol.
Another study showed the protective effects of monounsaturated fatty acids reduced the risk factors associated with metabolic syndrome and cardiovascular disease. Monounsaturated fats can have a positive impact on overall health. Monounsaturated fat sources include:
Olive, peanut, and canola oil
Avocados
Almonds
Pecans
Hazelnuts
Sesame and pumpkin seeds
References
Estruch, Ramón et al. “Retraction and Republication: Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N Engl J Med 2013;368:1279-90.” The New England journal of medicine vol. 378,25 (2018): 2441-2442. doi:10.1056/NEJMc1806491
Gillingham, Leah G et al. “Dietary monounsaturated fatty acids are protective against metabolic syndrome and cardiovascular disease risk factors.” Lipids vol. 46,3 (2011): 209-28. doi:10.1007/s11745-010-3524-y
American College of Physicians. (February 2017) “American College of Physicians issues guideline for treating non-radicular low back pain” https://www.acponline.org/acp-newsroom/american-college-of-physicians-issues-guideline-for-treating-nonradicular-low-back-pain
MedlinePlus. (2019) Hip flexor strain – aftercare https://medlineplus.gov/ency/patientinstructions/000682.htm
Scoliosis causes the spinal curvature to go sideways and can cause various symptoms. One of the most common symptoms is scoliosis hip pain. This happens because the spine’s curvature can pull the hips out of alignment, causing one side to be raised higher than the other. A result of this is one hip begins to take on more weight. This overloads the hip causing strain, soreness, aches, and pain, especially after standing or walking.
Scoliosis Hip Pain
Idiopathic scoliosis typically occurs in children, but often there are no pain symptoms. This type of scoliosis can go on unnoticed and undiagnosed for years even until adulthood. When the spine stops growing, even a small scoliosis curve can cause hip pain. The hip pain varies but generally presents with:
Sharp pain.
Throbbing pain.
Pain that increases with activity like walking, running, standing for a long time.
Stiffness with combined pain after sitting or lying down for a long time.
The type of scoliosis – degenerative or idiopathic.
Bodyweight. Individuals that are obese are more likely to have severe hip pain because of the added weight.
Activity level. Physical activity can cause the pain to worsen.
Lifestyle.
It varies from person to person.
The Higher Hip
When scoliosis has progressed enough, the curvature and uneven hips are pretty apparent. However, only around 10% of scoliosis cases get this far. If the curvature is minimal, which is usually the case, trying to determine which hip is higher usually requires medical assistance.
The hip that presents with pain is generally the one taking on more weight.
This causes the muscles to fatigue faster and places added stress on that hip joint.
A way to tell which hip is higher stand on bare feet in front of a mirror holding a piece of yarn, or string with both hands.
Place the heel of each hand on the corresponding hip bone.
The string will be tilted if the hips are uneven or will be straight if they are not.
Adult Scoliosis
Hip pain caused by scoliosis is most common in adults. However, it is not the only cause of hip pain. Unless diagnosed with scoliosis as a child, individuals may be suffering from de novo scoliosis or degenerative scoliosis.
De Novo/Degenerative Scoliosis
As the body ages, the spinal discs between the vertebrae begin to wear down. The worn-down discs can cause the spine to develop a sideways curve, that can pull the hips out of alignment. Studies are showing that this type of scoliosis is widespread. Loss of bone density can be a contributor to scoliosis in older adults. Bone density loss from menopause means women are more susceptible than men. Past the age of 70, both men and women lose on average, the same amount of bone density. There are effective integrative, natural treatment therapies that incorporate:
Exercises
Nutrition
Posture correction
Chiropractic
Physical therapy
Scoliosis Hip Exercises
For uneven hips, there are exercises to help relieve pain and strengthen weak muscles.
Hip Stretch
Lie on the back with both legs straight out.
Lift the right leg
Using the hands pull the knee toward you, keeping the foot pointed up.
Pull the knee to your chest as far as you can without causing discomfort or pain.
With the right hand, reach toward the left foot, touching if possible.
Return to the original position.
With the left hand, reach toward the right foot.
Repeat 6 to 8 times.
Chiropractic
If misaligned and uneven hips are causing pain, chiropractic care for scoliosis is recommended. Spine and hip realignments help relieve pain, stretch the muscles, and corrects posture. One study showed that multi-approach chiropractic for adult scoliosis was found to be beneficial even two years after treatment was finished. Injury Medical Chiropractic and Functional Medicine Clinic can help with recommending nutrition and lifestyle tips. Instead of just treating symptoms, our team helps manage the cause.
Body Composition
Body Analysis for Disease Prevention
Early identification of disease is imperative for developing the proper treatment plan. Testing can help improve long-term health outcomes. Testing is made easy with the data being easily implemented into patient management software. A comprehensive printout is ready for engaging and educating patients in understanding health risk management and reduction. In 60 seconds, an InBody Test will generate easy-to-understand, accurate, and objective measurements to evaluate potential disease risk. Medical providers can use the InBody to:
Monitor muscle, and visceral fat to provide an accurate measure of health risk.
Monitor muscle distribution to determine specific health risks related to diseases.
Identify fluid imbalances associated with certain diseases.
Track changes for effective long-term risk identification and reduction.
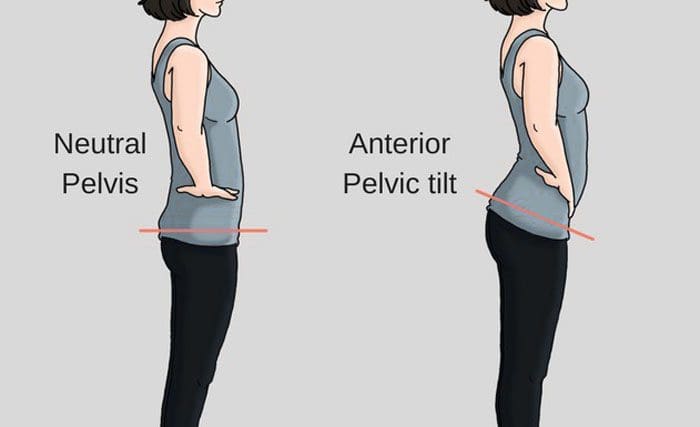
APT is short for anterior pelvic tilt. APT is when the pelvis tilts more down than forward, which can cause strain on the surrounding muscles and the spine to hold the torso up. The body’s own anatomical structure causing the condition and/or part of a bad habit that an individual has grown accustomed to. This can be from injury/s, back, and/or hip pain causing an individual to take on awkward postures to compensate for the discomfort and try and avoid it. However, these unhealthy postures cause their own set of musculoskeletal problems. Addressing this form of poor posture can help reduce and alleviate low back and hip pain and prevent further injuries. Chiropractic can pinpoint an anterior pelvic tilt and fix it.
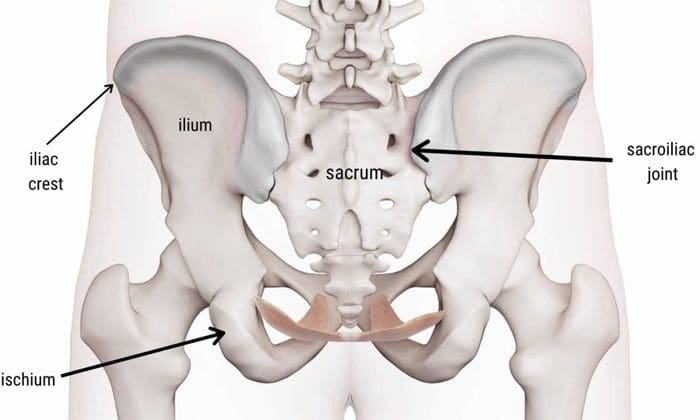
Anterior Pelvic Tilt
What happens is the pelvis becomes tilted or rotated forward. Place the hands, specifically the fingertips, on the hips. There are bone ridges. These are the iliac crests. If they’re facing more toward the ground than directly forward, this could be an anterior pelvic tilt. It usually happens when the hip flexors become tight and pull the pelvis down. Another contributor is the glute and hamstring muscles have weakened and are not strong enough to counteract the forward pulling. This can be caused by sitting for long periods, poor posture, and for women who wear high heels regularly. These contribute to tightening the hip flexors and the glutes, hamstrings, and core muscles.
An anterior pelvic tilt causes an increase in the curve of the lower back. It can feel like the hip flexors are tightening up. It typically affects the lower back at the lowest two levels, which are L4-5 and L5-S1. There can be long-term issues if an anterior pelvic tilt is left untreated. The spine becomes more vulnerable to disc issues that can include:
An anterior pelvic tilt is a repairable condition. Several exercises can help loosen/relax the hip flexors and strengthen the core and posterior muscle chain. This in addition to walking and reducing wearing high heels regularly. A few exercises for anterior pelvic tilt.
The Tail Tuck
This is literally trying to tilt the tailbone forward, like tucking in an imaginary tail. This can be done for 10-12 reps and up to 3 times.
Plank
Core-strengthening exercises can help with all types of back and hip problems. If possible, do the exercises in front of a mirror to ensure no arching of the back or the butt sticking out. If it is too difficult on the hands, go to the elbows. If there are wrist or shoulder issues, planks can be done on a raised surface, like a table or couch. Hold as long as possible, maintaining proper form. Start with 10-30 seconds and build up to minutes.
Strengthening the Glutes
It is recommended to strengthen the glute muscles. This can be done with exercises like clams or side-stepping with resistance bands. For clams, lie on the side and raise each leg up and down 10-12 times, up to 3 sets. For side-stepping, place resistance bands around the ankle/shin area and step to the side for 8-10 steps. Then go the other direction for the same number of steps. Repeat up to 3 sets.
Hip Flexor Stretch
Lunge forward while standing or lunge and kneel with the other leg on the ground. Then move the torso back a little and engage the core to stretch the hip flexors in the front of the thigh/pelvis area. Hold for 30 seconds, then release. Repeat 3-5 times per leg.
Lifestyle
These exercises can help, but if there is no progress around a month, contact a qualified chiropractor or physical therapist for further instruction and supervision. Also, if any neurological symptoms present like:
Sciatica
Shooting pain
Numbness
Tingling
Weakness
See a doctor as soon as possible.
Fixing posture-related problems require individuals to learn to be posture aware along with making some lifestyle adjustments. One way to do these exercises is to tack them onto a workout. Also, set reminders on a calendar to get up, stretch, and move around if sitting most of the day.
Body Composition Health
Difference between Processed sugar and Natural sugar
There are different types of sugar. There are natural sugars that are found in:
Fruits
Vegetables
Nuts
Whole grains
Beans
All sugar is broken down into glucose. However, foods that contain natural sugar are also rich in nutrients, including:
Vitamins
Minerals
Fiber
Protein
All which the body requires for optimal health.
Natural sugar does not lead to excess sugar intake; it happens with processed sugar. Processed sugar is extracted from sugarcane or sugar beet and is normally found as sucrose. This is present in cakes, cookies, cereal, and beverages. Processed sugar is also hidden in foods that are not sweet, like:
Microwave meals
Spaghetti sauce
Low-fat yogurt
Ketchup
Sports drinks
Foods that contain processed sugar are an energy source, but they contain little or no nutrients and can cause blood sugar levels to spike. In addition, consuming too much sugar is linked to an increased risk of:
Diabetes
Accelerated aging
Weight gain
Research has found that added sugar contributes to around 17% of the total calorie intake for adults. The recommended daily amount of calories from added sugar is 10%.
References
Azaïs-Braesco, Véronique et al. “A review of total & added sugar intakes and dietary sources in Europe.” Nutrition journal vol. 16,1 6. 21 Jan. 2017, doi:10.1186/s12937-016-0225-2
Centers for Disease Control and Prevention (CDC). (May 2020) “Acute Low Back Pain” https://www.cdc.gov/acute-pain/low-back-pain/index.html
National Institute of Neurological Disorders and Stroke. (March 2020) “Low Back Pain Fact Sheet” https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Low-Back-Pain-Fact-Sheet
Orlando Health. (2019) “Bad Posture Often to Blame for Chronic Pain and Health Issues, But Survey Finds Too Few Americans Are Concerned” https://www.orlandohealth.com/content-hub/bad-posture-often-to-blame-for-chronic-pain-and-health-issues
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine