Maintaining healthy joints is crucial to preventing injuries from affecting the body. Incorporating physical activities, eating healthy foods, staying hydrated, and getting a routine check-up are ways to ensure that the body is functional, including the joints. The joints in the body act like shock absorbers that soften the impact of any injuries that the body has sustained. However, as the body ages, so do the joints, causing them to become hardened and cause problems in the body. In today’s article, we will look at sacroiliac dysfunction, what issues it affects besides back pain, and how chiropractic care manages sacroiliac dysfunction. We refer patients to certified providers specializing in musculoskeletal therapies to help those with sacroiliac dysfunction. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Sacroiliac Dysfunction?
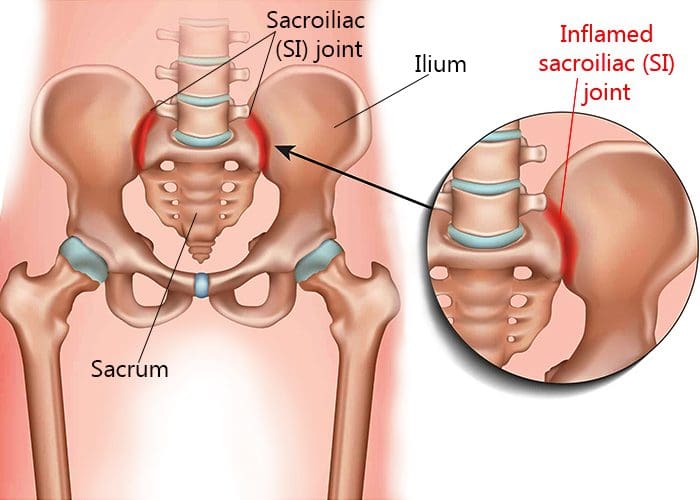
Are you experiencing pain in the pelvis? Do your hips seem tighter than usual? Do you feel muscle stiffness when you twist from side to side? Some of these issues are signs that you might be experiencing sacroiliac dysfunction. Around the pelvic region lies the sacroiliac joint, a weight-bearing solid joint connecting the pelvis to the sacrum. It is surrounded by tough ligaments that support the body as it distributes the weight from the upper body to the lower body. However, like all the other joints in the body, any injury or condition can cause this joint to be unstable and succumb to the pain, causing sacroiliac dysfunction. Sacroiliac dysfunction or sacroiliac joint pain is defined as one of the potential causes of axial low back pain. When there are issues affecting the sacroiliac joints, it’s associated with about a quarter of most low back pain cases. This is due to the problems that overlap with pain associated with the low back. Studies reveal that dysfunction in the sacroiliac joint can relate to leg or back pain, making diagnosing the problem difficult. Back pain associated with sacroiliac dysfunction causes the pelvis to be hypermobile, causing the risk of developing radiating groin pain. Leg pain associated with sacroiliac dysfunction causes muscle tension and stiffness to the low back, legs, or buttock region, mimicking sciatica-like symptoms.
What Other Issues Does It Affect?
Many individuals may not realize that when they are experiencing sacroiliac dysfunction, symptoms show that they overlap with lumbar spine pathologies. However, sacroiliac dysfunction can also affect the pelvic region of the body. Studies reveal that when the muscles around the body’s pelvic area become inflamed or irritated, it can cause stiffness in the sacroiliac joints, thus developing the risk of pelvic pain. Pelvic pain is usually defined as non-menstrual pain that causes functional disability to the lower extremities. Around the pelvic region, the lower sacral nerves provide extensive neurologic connections to the structures throughout the pelvic area that maintain normal pelvic organ function. When issues like sacroiliac dysfunction become the risk of pelvic pain, it may potentially involve pelvic symptoms like constipation. Studies reveal that constipation is significantly associated with a high prevalence of pelvic organ prolapse and low urinary tract symptoms. Other issues that sacroiliac dysfunction correlates with are:
Ankylosing spondylitis
Rheumatoid arthritis
Inflammatory issues
Hip pain
Pelvic pain
Low back pain
Piriformis syndrome
An Overview Of Sacroiliac Joint Pain- Video
Are you experiencing radiating from your lower back down to your leg? How about stiffness in your hips? Are you feeling constipated or have a sense of fullness in your bladder? You may suffer from sacroiliac dysfunction in your pelvic region if you notice these symptoms. The video above explains how to understand sacroiliac joint pain. The sacroiliac joint connects the pelvis and sacrum, surrounded by tough ligaments and muscles that help support the body by distributing weight from the upper body to the lower body. When issues affect the sacroiliac joints can overlap other risk profiles like low back pain, leg pain, and pelvic pain. This can make diagnosing sacroiliac dysfunction difficult because the symptoms are similar to other issues. For example, hip pain is associated with piriformis syndrome while potentially being involved with sciatica. How would hip pain be correlated with piriformis syndrome? The piriformis muscle can become overused and injured and can entrap the sciatic nerve (which runs from the lumbar spine, through the hips, and down to the leg), causing radiating, throbbing pain. Other times referred pain in the low back can affect different areas in the body due to sacroiliac dysfunction. Luckily, there are treatments available to manage sacroiliac dysfunction.
How Chiropractic Care Manages Sacroiliac Dysfunction
When issues of sacroiliac dysfunction become associated with leg or back pain, physicians often misdiagnose it as a soft tissue issue rather than a joint issue. Many doctors might rule out various medical conditions before including sacroiliac dysfunction as part of the diagnosis. Some treatments like massage therapy can help loosen up the tight muscles surrounding the joints relieving the pain and discomfort. At the same time, chiropractic care utilizes spinal manipulation and mobilization to the affected spinal area. Since the sacroiliac joint is an essential part of the musculoskeletal system, chiropractors specialize in this area. Through practical, non-invasive methods, chiropractic care has proven to not only relieve pain in the spine but can also help rehabilitate the spine. Chiropractors are specially trained to guide the individual through several phases of care that help loosen the stiff muscles and strengthen the joints. Chiropractic care will help decrease the pain from returning to the body and let the individual return to their health and wellness journey.
Conclusion
Maintaining healthy joints is crucial to prevent injuries from affecting the body. The sacroiliac joints are part of the musculoskeletal system that connects the pelvic bone to the sacrum. This joint is surrounded by tough ligaments and muscles that support the upper and lower half of the body through weight distribution. When the sacroiliac joint becomes unstable, it can succumb to pain, thus becoming sacroiliac dysfunction. Sacroiliac dysfunction sometimes mimics low back and leg pain, making it difficult to diagnose. Co-morbidities like pelvic pain correlate to sacroiliac dysfunction, causing somato-visceral pain in different body areas. Treatments like chiropractic care can help strengthen the stiff muscles and joints in the body through spinal manipulation and mobilization in practical, non-invasive treatment. Chiropractic care can help rehabilitate the spine while decreasing the pain from returning to the body.
References
Jonely, Holly, et al. “Chronic Sacroiliac Joint and Pelvic Girdle Dysfunction in a 35-Year-Old Nulliparous Woman Successfully Managed with Multimodal and Multidisciplinary Approach.” The Journal of Manual & Manipulative Therapy, Maney Publishing, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4459139/.
Raj, Marc A, et al. “Sacroiliac Joint Pain.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK470299/.
Singh, Prashant, et al. “Pelvic Floor Symptom Related Distress in Chronic Constipation Correlates with a Diagnosis of Irritable Bowel Syndrome with Constipation and Constipation Severity but Not Pelvic Floor Dyssynergia.” Journal of Neurogastroenterology and Motility, Korean Society of Neurogastroenterology and Motility, 31 Jan. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6326213/.
The muscles in our body help us be active when we want to be, rest and repair after activities, and continue to provide everyday movements that help keep the body functioning correctly. For athletes and the general population, physical training and eating healthy foods help deliver fuel to not only the internal organs but also help support the muscles, ligaments, and skeletal joints from injuries. As many individuals start to think about their health and wellness, many factors tend to pop up that can cause them to halt their health and wellness journey. Issues like stress, accidents, traumatic events, and lifestyle habits can affect the body and, over time, can become the risk of developing into chronic problems. An example would be where a person is experiencing hip pain associated with piriformis syndrome. Today’s article looks at piriformis syndrome, how it can cause more than hip pain, and how there are available treatments for piriformis syndrome. We refer patients to certified providers specializing in musculoskeletal therapies to help those with piriformis syndrome. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Piriformis Syndrome?
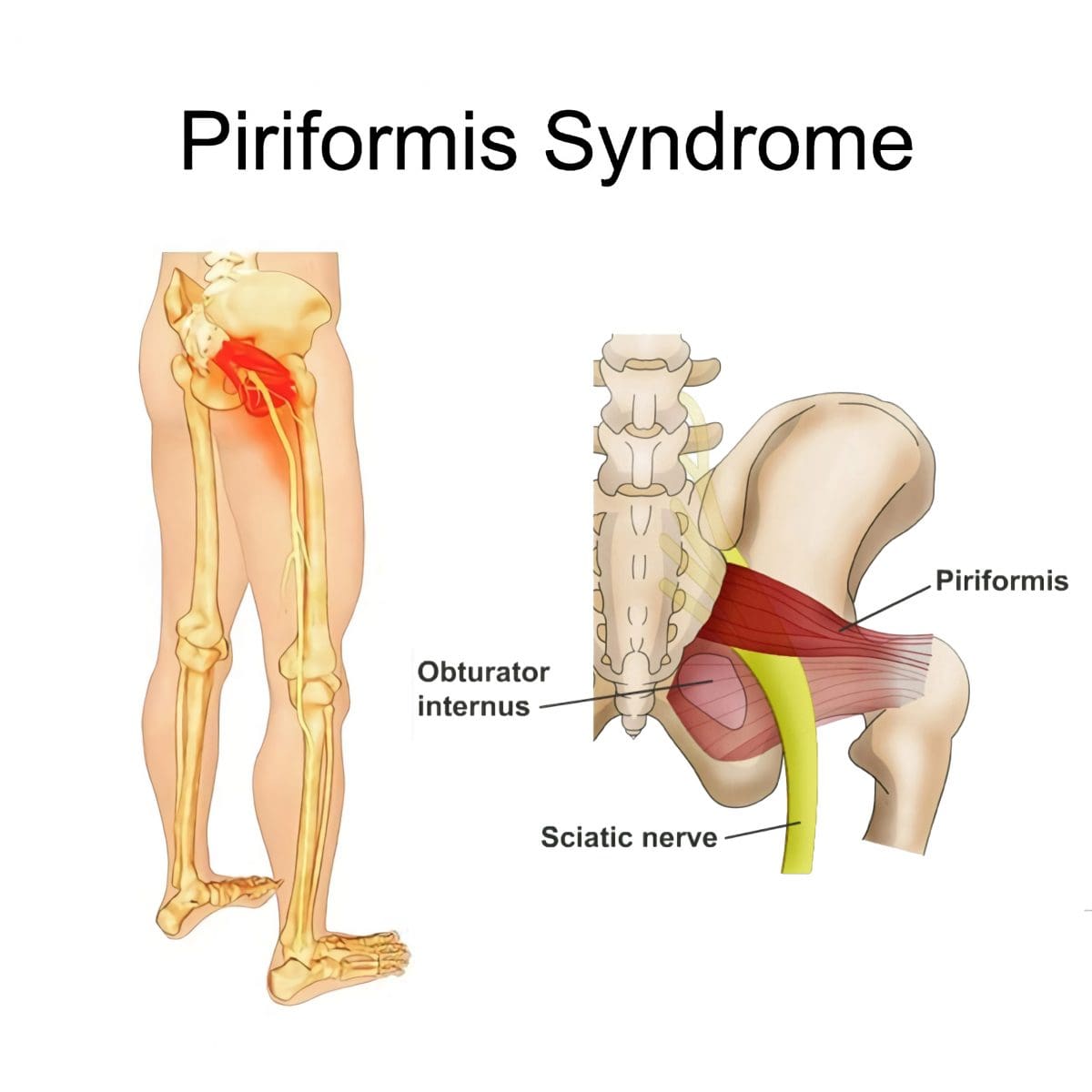
Have you been experiencing pain radiating from the buttock down to your legs? Does it hurt when you are sitting down? Or are you feeling tingling sensations and numbness on your butt and thighs? Some of these symptoms might be signs that you might be experiencing piriformis syndrome. Research studies have defined piriformis syndrome as a clinical condition where everyday stress affecting the body causes the piriformis muscle (the small muscle deep in the buttock region) to become tight and irritates the sciatic nerve. When that sciatic nerve becomes aggravated, it can become the risk of developing into sciatica. Many individuals don’t realize that the sciatic nerve also gets affected when their piriformis muscles in the buttock region become overused and tight through strenuous activities. This is due to the belief that any unusual traumatic abnormality in the piriformis muscle will be associated with sciatica symptoms. However, when a person is experiencing buttock pain that travels down the leg caused by the affected piriformis muscle, many will rule out some of the more common causes of sciatica like nerve root impingement triggered by disc herniation.
Surprisingly, three primary causing factors can be associated with piriformis syndrome. The first causing factor is myofascial trigger points may be the results of referred pain (pain or discomfort from another body location). The second causing factor is nerve entrapment against the greater sciatic foramen passing through the various piriformis muscles. And finally, the third causing factor is sacroiliac joint dysfunction due to piriformis muscle spasm. Studies reveal that the piriformis muscle helps stabilize the sacroiliac joint; when the small muscle starts to become irritated, it causes pain in the buttock region. But how does sacroiliac dysfunction relates to piriformis syndrome? Well, since low back pain is associated with sacroiliac dysfunction, the pain will often radiate down to the knee and the groin muscles while becoming a risk of developing piriformis syndrome.
Piriformis Syndrome Causes More Than Hip Pain?
Due to its broad size in the greater sciatic foramen, the piriformis muscle can become overused and tight, thus becoming piriformis syndrome. Piriformis syndrome can also become a risk to the numerous vessels and nerves that exit out in the pelvis region and may become compressed, causing more than just hip pain. Studies reveal that piriformis syndrome may be masquerading as ischiofemoral impingement triggering extra-articular hip pain by entrapping the quadratus femoris muscle causing groin pain. Another cause that piriformis syndrome is associated with is chronic pelvic pain. How does chronic pelvic pain correlate with piriformis syndrome? Chronic pelvic pain is a non-cyclic pain localized in the pelvis, potentially involving the surrounding muscles like the piriformis muscle supporting the irritated hip joint and pelvis region. Piriformis syndrome could also be an overlapping condition risk of developing other health issues like fibromyalgia in many people. Some conditions have common symptoms associated with piriformis syndrome, including:
Tingling sensations
Numbness
Muscle tenderness
Pain while sitting
Discomfort while exercising
The Difference Between Sciatica & Piriformis Syndrome-Video
Have you found it challenging to be comfortable while sitting down doing leisure activities? How about radiating pain that travels down your leg? Or do your hips feel tight and stiff? Experiencing these symptoms means that you might suffer from piriformis syndrome. The video above explains the difference between piriformis syndrome and sciatica. Studies reveal that piriformis syndrome is classically defined as sciatic pain; however, it is not sciatica. Sciatica is caused by compressed sciatic nerve due to herniated disc in the lumbar spine. In contrast, piriformis syndrome is caused when a traumatic injury or an underlying condition causes the piriformis muscle to spasm and aggravate the sciatic nerve. Various factors like prolonged sitting, repetitive movements that involve the legs, and even extensive stair climbing can cause the piriformis muscle to be easily damaged or injured, causing piriformis syndrome. Fortunately, there are ways to alleviate sciatic nerve pain and improve piriformis syndrome.
Treatments Available For Piriformis Syndrome
Many treatments are accessible to manage the pain and discomfort caused by piriformis syndrome for suffering individuals. Some people take over-the-counter medicine to decrease the pain, while others utilize a hot/cold pack on the affected area to relieve discomfort. The symptoms associated with piriformis syndrome usually go away without any additional treatment; however, if the pain or discomfort is still there, many people might benefit from alternative options for treatment, like chiropractic care, physical therapy, or even spinal decompression. Whether it is through gentle stretching, spinal manipulation, or decompression, these treatments are for anyone dealing with piriformis syndrome and its associated symptoms. Physical therapy can help decrease the painful symptoms associated with piriformis syndrome through gentle stretches that help return a person’s range of motion. Chiropractic care incorporates spinal adjustments and manual manipulations to treat various injuries or conditions. Spinal decompression uses traction to gently pull on the spine to release the aggravated nerve from causing pain. The relief can gradually restore a person’s natural health while managing its associated symptoms with various treatments available for individuals with piriformis syndrome.
Conclusion
Piriformis syndrome is a condition where everyday stress affects the piriformis muscle in the buttock region to become irritated and tight while aggravating the sciatic nerve. Many think traumatic abnormalities affecting their piriformis muscle will be associated with sciatica symptoms. However, sciatica is due to nerve root compression triggered by disc herniation. Piriformis syndrome is where that small muscle is overused from various factors that cause more than hip and butt pain. Some overlapping conditions associated with piriformis syndrome can become mediators for groin and pelvic pain. Fortunately, chiropractic care, physical therapy, and decompression can help restore the body gradually by managing piriformis syndrome and its associated symptoms.
References
Hicks, Brandon L., et al. “Piriformis Syndrome.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 21 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK448172/.
Newman, David P, and Liang Zhou. “Piriformis Syndrome Masquerading as an Ischiofemoral Impingement.” Cureus, Cureus, 16 Sept. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8520408/.
Professionals, Northwest Medical. “Piriformis Syndrome/Sacroiliac Dysfunction.” Northwest Medical Center, 2021, https://nw-mc.com/piriformis-syndromesacroiliac-dysfunction/.
Ro, Tae Hoon, and Lance Edmonds. “Diagnosis and Management of Piriformis Syndrome: A Rare Anatomic Variant Analyzed by Magnetic Resonance Imaging.” Journal of Clinical Imaging Science, Medknow Publications & Media Pvt Ltd, 21 Feb. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843966/.
Pain in different body areas can excruciate the host as it can affect other regions. In the body, pain can affect the muscles, tissues, organs, and skeletal joints through environmental factors that affect the body’s systems. For example, the gut system provides the body with overall health and wellness by regulating homeostasis and metabolism, which can be affected by common factors like stress or unhealthy eating habits that can cause joint inflammation due to overproducing harmful gut bacteria. Or how about poor posture affecting the organs in the pelvic region and causing the lower back and neck muscles to have a dull ache in the body. Today’s article looks at how pelvic pain affects the somato-visceral reflexes in the body and how there are treatments for relieving pelvic pain. We refer patients to certified providers specializing in chiropractic treatments that help those with pelvic pain. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
Somatovisceral Reflexes & Pelvic Pain
Have you experienced pain in your lower back or pelvic regions from sitting too long? Have you experienced bladder dysfunction that is causing you to urinate frequently? Or are you suffering from muscle cramps in the pelvic area? Studies have revealed that pelvic pain can be a chronic, persistent pain associated with co-morbidities like IBS (irritable bowel syndrome), neurological disorders, or low back pain. Pelvic pain is challenging to diagnose since it is multifactorial and shares various nerve roots that send signals to the brain. For example, individuals that suffer from pelvic pain will complain about the somatovisceral convergence affecting their reproductive organs and connective tissues. Other issues like prolonged sitting and poor posture can also affect the lumbosacral nerve root as it is being compressed, causing low back pain and pelvic organ dysfunction.
The somato-visceral reflexes of the pelvic muscles can become overstretched and compress the surrounding nerve roots like the sciatic nerve and the lumbosacral nerve, causing issues of sciatica or lower back pain. Studies have also revealed that individuals who suffer from spinal cord injuries can disrupt the somatic lumbosacral nerve pathway that is responsible for coordinating bladder function to the pelvic region. These pathways can also produce different autonomic reflex responses to the various organs and somatic afferents. For example, if a female is experiencing pain in her hips or thighs from hyper-sensitive nerve roots, the brain will register that as pain in her reproductive system. Or, if the pelvic muscles are hypersensitive to the touch, something might be affecting the genital regions.
An Overview Of Pelvic Pain- Video
Have you experienced muscle tenderness located in the pelvic region? Have stressful events caused changes in the reproductive system? Have you experienced pelvic pain that is associated with low back pain? You might be experiencing these systems due to pelvic pain and associated co-morbidities. The video above gives an overview of pelvic pain and how it affects the body. Research studies have revealed that the characteristic of mechanically induced pelvic pain and organic dysfunction that correlates to lower sacral nerve root compression results from low back disorders. The environmental factors that can cause low back conditions include:
Obesity
Heavy lifting
Muscle strain
Poor posture
Herniated disc
Treatments For Pelvic Pain
Various treatments can help relieve these overlapping risk profiles associated with pelvic pain and low back pain that are causing the issue and strengthen the weak muscle affected. Exercising can help support the hip and thigh muscles to prevent muscle strain on the low back and pelvic muscles with the combination of chiropractic therapy to provide beneficial pain relief. Chiropractic therapy on the lumbar spine can help alleviate pelvic pain and lumbosacral nerve root irritation affecting the pelvic region. The effects of chiropractic therapy help sustain the caudal flexion of the lumbar spine and release the muscle that aggravates the lumbosacral nerve root that is running along the pelvic region.
Conclusion
Pain affecting the pelvic region can be due to co-morbidities affecting different areas in the body. With pelvic pain being multifactoral, it can be a challenge to diagnose since it shares various nerve roots signaling to the brain. This causes many individuals to complain about somatovisceral convergence that can affect their reproductive organs and connective tissues in the pelvic region. Other issues like low back pain associated with prolonged sitting and poor posture can cause pelvic pain too. Treatments like chiropractic therapy and exercising can help strengthen the low back and pelvic muscles to alleviate painful symptoms that are causing underlying issues and discomfort in the body.
References
Browning, J E. “Mechanically Induced Pelvic Pain and Organic Dysfunction in a Patient without Low Back Pain.” Journal of Manipulative and Physiological Therapeutics, U.S. National Library of Medicine, Sept. 1990, https://pubmed.ncbi.nlm.nih.gov/2212886/.
Browning, J E. “Chiropractic distractive decompression in treating pelvic pain and multiple system pelvic organic dysfunction.” Journal of manipulative and physiological therapeutics vol. 12,4 (1989): 265-74. https://pubmed.ncbi.nlm.nih.gov/2527938/
CM;, Spitznagle TM;Robinson. “Myofascial Pelvic Pain.” Obstetrics and Gynecology Clinics of North America, U.S. National Library of Medicine, 9 June 2014, https://pubmed.ncbi.nlm.nih.gov/25155122/.
Craggs, Michael D. “Pelvic Somato-Visceral Reflexes after Spinal Cord Injury: Measures of Functional Loss and Partial Preservation.” Progress in Brain Research, U.S. National Library of Medicine, 2006, https://pubmed.ncbi.nlm.nih.gov/16198702/.
Dydyk, Alexander M, and Nishant Gupta. “Chronic Pelvic Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Nov. 2021, https://www.ncbi.nlm.nih.gov/books/NBK554585/.
The lower half helps stabilize the body and provides movement from the legs and rotation in the hips. The lower abdominal organs help control bowel movement while the muscles allow movement by regulating internal abdominal pressure. Combined with the back muscles, the lower abdomen can keep the body stable while protecting the lumbar section of the spine. When external factors begin to affect the lower back or disrupt the lower abdominal organs, it can trigger different symptoms that correspond to other sections of the body, like knee or leg pain being associated with menstrual cramping in the lower abdominals or even having pelvic pain that is an associated mediator to having constipation. Today’s article looks at pelvic pain, how it affects the lower abdominals, and ways to treat pelvic dysfunction in the body. We refer patients to certified, skilled providers specializing in chiropractic treatments that help those suffering from pelvic pain. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
How Does Pelvic Pain Occur?
Have you suffered from frequent urination or irregular periods? Have you felt excruciating pain when bending down? Or feeling muscle weakness in the lower extremities of the body? Many of these symptoms are correlated to pelvic pain and can trigger different symptoms affecting the body’s lower half. Research studies have mentioned that pelvic pain in its chronic form is a non-cyclic pain located in the pelvis, and the multiple causations can make it difficult to source where the pain is coming from. The overlapping profiles of pelvic pain can be traced through the numerous nerve pathways that are connected to the spine that can become aggravated and become the mediators for pelvic pain. For example, a person having low back pain might experience uncontrollable urinary discharge in their pelvic region. This could be due to the lower sacral nerve root being impaired and causing an overlap of the profiles resulting from mechanical legions to the lumbar spine, thus increasing the risk associated with the pelvis.
How Does It Affect The Lower Abdominals?
The pelvic region ensures that the body’s lower half is stable and protects the lower abdominal organs from disruptive factors like pelvic pain. Research studies have shown that pelvic pain is a relatively common pain associated with comorbidities affecting the body. Some of the various associated symptoms of pelvic pain can cause a correlation to disturbances of the bladder and sexual function in both sexes while also triggering abdominal and low back pain. Additional research studies have found that chronic pelvic pain can cause a correlated issue with PBS or painful bladder syndrome. What PBS does is that it can make a person have a frequent need to urinate and can cause the pelvic muscles to become tense and sensitive. This coincidentally causes the lower sacral nerves to be aggravated and become a mediator for the genital region to be hypersensitive.
Pelvic Pain Overview-Video
Are you feeling stiffness or tenderness in the groin region? How about going to the bathroom constantly? Or have you been experiencing low back pain? Many of these symptoms correlate to pelvic pain and other symptoms associated with the body. The video above overviews pelvic pain and how it affects the body’s lower extremities. The pelvic region consists of lower sacral nerve roots connected to several different nerve pathways that correspond to the primary nerves and provide an extensive neurological connection to the other areas in the pelvis. When mediators cause an increased risk in the pelvic region, the pelvic splanchnic nerves start to trigger muscle dysfunction in the lower abdominal organs. This causes numerous combinations of symptoms and disorders that causes overlapping of profiles in the body. The lower sacral nerve that is aggravated in the pelvic region could be the causation of pelvic and leg pain.
Treatments For Pelvic Dysfunction
Since the pelvic region has many nerve roots that are intertwined and connect to the major nerves in the spinal cord, it can become aggravated by accompanying the lower lumbar and upper sacral nerve roots to be impaired. Research studies have found that pelvic pain can cause an overlap in risk profiles that involves either the visceral or somatic system and the encompassed structures that help the nervous system form a causal relationship to the spine and lower extremities. When the nerve roots become irritated and affect the pelvic region, treatments like chiropractic therapy and physical therapy can help relieve the pelvic area and even help alleviate other symptoms. Physical therapy helps strengthen the hip and abdominal muscles from becoming weak and can reduce overlapping pathologies. Chiropractic therapy can help manipulate the L-1 through 5 vertebrae in the lumbar region of the spine, causing low back pain and bladder dysfunction. Research studies have mentioned that spinal manipulation can help reduce lower sacral nerve root compression triggering low back pain associated with leg pain. This overlap of risk profiles may cause pelvic pain affecting the body and causing organ dysfunction.
Conclusion
The lower half of the body consists of the lower abdominal organs and the pelvic region that allows bowel movement and keeps the body stable when in motion. When external factors begin to affect the lower back or the lower abdominal organs, it can cause a triggering effect on different sections of the body. Pelvic pain can affect the internal organs in the lower abdominal and pelvic region and cause comorbidities affecting the body’s lower back and bladder function. Treatments that help strengthen the hips and abdominal muscles or manipulate the spine to reduce the encased nerves trapped in the pelvic muscles will provide relief to the body’s lower extremities and improve functionality.
References
Browning, J E. “Chiropractic Distractive Decompression in Treating Pelvic Pain and Multiple System Pelvic Organic Dysfunction.” Journal of Manipulative and Physiological Therapeutics, U.S. National Library of Medicine, Aug. 1989, https://pubmed.ncbi.nlm.nih.gov/2527938/.
Dydyk, Alexander M, and Nishant Gupta. “Chronic Pelvic Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Nov. 2011, https://www.ncbi.nlm.nih.gov/books/NBK554585/.
Grinberg, Keren, et al. “New Insights about Chronic Pelvic Pain Syndrome (CPPS).” International Journal of Environmental Research and Public Health, MDPI, 26 Apr. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7246747/.
Hwang, Sarah K. “Advances in the Treatment of Chronic Pelvic Pain: A Multidisciplinary Approach to Treatment.” Missouri Medicine, Journal of the Missouri State Medical Association, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6143566/.
Lee, Dae Wook, et al. “Chronic Pelvic Pain Arising from Dysfunctional Stabilizing Muscles of the Hip Joint and Pelvis.” The Korean Journal of Pain, The Korean Pain Society, Oct. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5061646/.
The body is held up by skeletal joints that keep the body upright and provide everyday movements for the body to go anywhere at any time. The musculoskeletal system provides the muscles, tissues, and ligaments that encase the skeletal joints protecting them from unknown factors that can cause harm to the body. The internal organs also have a purpose in the body as they help provide the nutrients and necessary hormones to the muscles and joints that need these nutrients to function. When environmental factors affect the body, either internal or external, it can cause the body to become dysfunctional and even cause unwanted symptoms that affect the internal organs that correspond to the muscles suffering. Today’s article looks at pelvic pain, how gut disorders are associated with pelvic pain, and how viscerosomatic pain affects the pelvis. We refer patients to certified, skilled providers specializing in osteopathic and gut treatments that help those with gut disorders and pelvic pain issues. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Pelvic Pain?
Have you been experiencing gut issues that are affecting your pelvic region? Has your gut been feeling inflammatory effects? Have you noticed that you need to go to the bathroom more frequently than usual? Many of these symptoms are some of the signs that are associated with pelvic pain. Research studies have defined pelvic pain as disabling, chronic, and persistent pain that commonly affects women. Pelvic pain can range from acute to chronic depending on how severe the pain affects the pelvic region of the body. Additional research studies have mentioned that pelvic pain in its chronic form can become a multifactorial disorder that can cause pain in the gastrointestinal, pelvic musculoskeletal, or nervous system, making the immune, neurological, and endocrine metabolism dysfunctional. When pelvic pain begins to affect the gastrointestinal system, it can lead to various gut disorders that can cause the pain to become worse if it is not treated.
How Do Gut Disorders Associate Pelvic Pain?
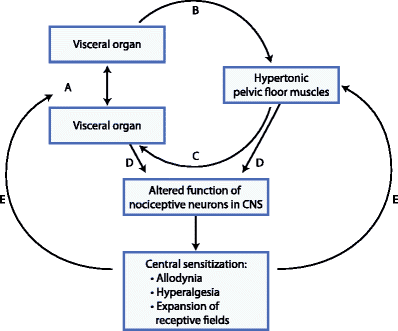
Research studies have mentioned that since pelvic pain is a multifactorial disorder, it can cause pain to arise in the internal organs in the gastrointestinal system. When pelvic pain starts to affect the gastrointestinal system, it can cause the development of gut disorders to affect the body further. When gut disorders co-exist with pelvic pain, it can cause an enhancement to the overall pain symptoms that are becoming the result of viscerosomatic dysfunction through the cross-organ sensitization mechanisms. Additional information studies have mentioned that gut disorders like IBS (irritable bowel syndrome) can cause changes in thermal/visceral pain sensitivity that overlap in the lower body’s pelvic region, further enhancing rectal/thermal pain. This can cause a person to become miserable and even affect their quality of life since they are suffering from so much pain.
Visceral Afferent Nerves Being Affected By Pelvic Pain-Video
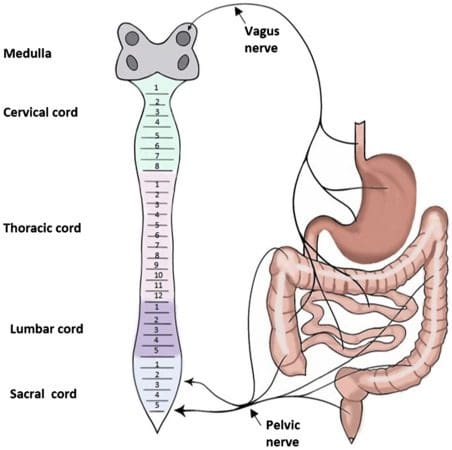
Have you experienced gut issues like IBS (irritable bowel syndrome), inflammation, or IBD (inflammatory bowel disease)? Have you felt pain in your pelvic region constantly? Has the pain-affected certain areas in your body, not just your pelvis? If you have these symptoms, it might be due to your visceral nerves being involved. The video above explains what the visceral afferent nerves from the pelvic region are doing to keep the body functioning in the lower extremities. The visceral afferent nerves become aggravated by environmental factors affecting the body, including the gut system. Symptoms of inflammation and gut disorders from persistent aspects of many forms of stress or trauma can cause visceral pain to affect the body, thus causing pelvic pain, gut issues, lower back pain, and other body pains.
How Viscerosomatic Pain Affects The Pelvis
The body’s viscerosomatic pain can be complex since the organs also affect the corresponding muscles. The way the pain is described in the body from viscerosomatic pain ranges from dull to excruciating pain. Research studies have mentioned that the burden of viscerosomatic pain emanates from the internal thoracic, pelvic, and abdominal organs associated with the muscles. For visceral pain to affect the pelvic region, research studies have shown that the nociceptive pain from the pelvic area is usually visceral from the results from the pelvic organs that are poorly localized and can overlap with the somatic sensory tracts that are located in the spinal cord. When this happens, it can cause significant discomfort to the pelvic organs in the body and affect the individual with excruciating painful symptoms.
Conclusion
The body provides everyday movements held by the skeletal joints that help the body go anywhere. While the musculoskeletal system and the internal organs help give the muscles, tissues, ligaments, and nutrients the body needs to function. When environmental factors affect the body, it can lead to various issues that cause gut disorders and even pain in the pelvic region, known as visceral pain. Visceral pain is a complex disorder since the affected organs also affect the corresponding muscles. For visceral pain to affect the pelvic area, it can lead to dull excruciating pain in the pelvic organs and affect the individual. Visceral pain can also overlap the sensory somatic tracts in the spinal cord, causing unbearable painful symptoms to the body while inflammatory issues in the gut system are developing. When people realize that the pain is affecting them, they can start to find treatments from their specialized providers to help alleviate their pain.
References
Dydyk, Alexander M, and Nishant Gupta. “Chronic Pelvic Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Nov. 2021, https://www.ncbi.nlm.nih.gov/books/NBK554585/.
Grinberg, Keren, et al. “New Insights about Chronic Pelvic Pain Syndrome (CPPS).” International Journal of Environmental Research and Public Health, MDPI, 26 Apr. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7246747/.
Origoni, Massimo, et al. “Neurobiological Mechanisms of Pelvic Pain.” BioMed Research International, Hindawi Publishing Corporation, 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4119661.
Udoji, Mercy A, and Timothy J Ness. “New Directions in the Treatment of Pelvic Pain.” Pain Management, U.S. National Library of Medicine, Sept. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3979473/.
Verne, G Nicholas, et al. “Viscerosomatic Facilitation in a Subset of IBS Patients, an Effect Mediated by N-Methyl-D-Aspartate Receptors.” The Journal of Pain, U.S. National Library of Medicine, Sept. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3489925/.
Yuan, Tian, and Beverley Greenwood-Van Meerveld. “Abdominal and Pelvic Pain: Current Challenges and Future Opportunities.” Frontiers in Pain Research (Lausanne, Switzerland), Frontiers Media S.A., 4 Feb. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8915637/.
The body is a marvelous functional machine that requires constantly moving worldwide. The body can do everyday movements from the head to the feet and be in weird positions without feeling pain. However, ordinary factors like natural aging, wear and tear, and issues affect the body over time. When these factors start to affect the body, they can cause unwanted symptoms that can inflict pain on specific areas around the body. Some areas that suffer pain include the hips, lower back, neck, the body’s internal systems, and the spine, causing the individual to be miserable. Luckily many treatments do relieve pain in the body and help dampen the effects of the unwanted symptoms that are hindering the individual. Today’s article focuses on hip pain, its symptoms, and how decompression therapy can help many individuals suffering from hip pain. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Hip Pain?
Are you feeling stiffness from your lower back and hips? Do your hips hurt after falling due to playing sports? How about pain from the lower back to the hips down to the feet? You might be experiencing hip pain. Research studies have stated that hip pain can be associated with many factors that can cause many individuals to be in distress, impair their daily activities, and affect their quality of life. Hip pain can be associated with simple movements that are damaged, like sitting and standing, which can be hard after a while. Other associations that hip pain can occur can be lower back pain, neuropathies, herniation, or chronic pain. According to research studies, hip pain is considered a musculoskeletal disorder. It shows that posterior hip pain in adults is caused by osteoarthritis or traumatic causes like sacral stress fractures that can affect the hips. This musculoskeletal disorder can become a problem for many older adults suffering from hip issues.
The Symptoms
Research studies have found that hip pain is a musculoskeletal complaint affecting young and old adults. Since hip pain is associated with various chronic issues, it can cause many individuals to be miserable and be in constant pain. For adults, hip pain can be one of the issues for those suffering from osteoarthritis in the anterior hip region. As research shows, in the posterior hip region, hip pain can be associated with chronic conditions like piriformis syndrome and lumbar radiculopathy that are centralized in the lower back. Other symptoms that hip pain cause on its own do associate with other chronic conditions, including:
Are you experiencing discomfort from your hips while sitting or standing? How about sharp, throbbing pain coming from your lower back and affecting your hips and legs? Do you feel tenderness and swelling on your joints? These symptoms are various forms of hip pain, and lumbar traction can help lower hip pain symptoms. The video above mentions how to prepare for lumbar traction therapy and how it can alleviate symptoms caused by hip pain. Lumbar traction helps compressed disc in the lumbar region of the spine to be restored to its original state and even takes the pressure off the sciatic nerve and other nerve roots that are causing hip pain to the body. Utilizing traction therapy increases the disc height and allows the lumbar spinal discs to be rehydrated again. Suppose you want to learn more about lumbar traction or decompression and how it can benefit you? In that case, this link will explain what decompression does for the lumbar area in the spine and provide relief from hip pain and its associates.
How Decompression Therapy Helps With Hip Pain
Since hip pain is associated with various other conditions that can affect the body, the most common condition that the body has suffered from is low back pain. There are ways to treat hip and low back pain; some individuals utilize heat and ice to neutralize the pain to go away, and others use chiropractic therapy to get the joints to realign themselves. One of the treatments used to relieve hip and low back pain is decompression therapy. Research studies have found that decompression therapy is safe and effective in helping to improve the blood circulation to the hips to provide relief to the hips. Since hip pain is associated with low back pain, decompression allows the herniated discs to be taken off the nerves surrounding the hips and provide pain relief. Other research studies show that traction is used to create negative gravity pressure to help reduce the pressure that is causing pain to the soft tissues and the nerve roots. This negative gravity allows the spine to separate and create more height for the disc to rehydrate while relieving the individual.
Conclusion
Overall the body is a marvelous machine that has the ability to move without pain. When issues start to affect the body, like the hips and lower back, it can cause the individual to suffer from various forms of pain. Since hip pain is associated with low back pain, it can lead to other chronic issues like sciatica or osteoarthritis, affecting the joints and causing them to swell. Treatments like decompression or traction therapy are used to alleviate the pain caused by the hips or lower back. When people incorporate decompression or traction into their wellness journey, they relax a bit as they are laid down and have their spine stretched slowly. This will cause them relief and take the pressure off the nerve roots that are sending pain signals to the brain. This ensures them that they can take back their lives pain-free.
References
Ahuja, Vanita, et al. “Chronic Hip Pain in Adults: Current Knowledge and Future Prospective.” Journal of Anaesthesiology, Clinical Pharmacology, Wolters Kluwer – Medknow, 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022067/.
Battaglia, Patrick J, et al. “Posterior, Lateral, and Anterior Hip Pain Due to Musculoskeletal Origin: A Narrative Literature Review of History, Physical Examination, and Diagnostic Imaging.” Journal of Chiropractic Medicine, Elsevier, Dec. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5106442/.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Lee, Yun Jong, et al. “Causes of Chronic Hip Pain Undiagnosed or Misdiagnosed by Primary Physicians in Young Adult Patients: A Retrospective Descriptive Study.” Journal of Korean Medical Science, The Korean Academy of Medical Sciences, 11 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6300658/.
Wilson, John J, and Masaru Furukawa. “Evaluation of the Patient with Hip Pain.” American Family Physician, U.S. National Library of Medicine, 1 Jan. 2014, https://pubmed.ncbi.nlm.nih.gov/24444505/.
Healthy hips are necessary for standing, sitting, walking, running, bending, twisting, lifting, etc. Hip problems can seriously interfere with everyday activities. Out of alignment hips don’t just cause pain and soreness in the hip area but can radiate to other body areas. When the hip joint is out of alignment, the rest of the body has to start compensating for the misalignment, which can cause chronic pain in the back and/or legs.
Out of Alignment Hips
Discomfort and soreness begin as occasional but can quickly become regular. Individuals may also begin to limp when they walk, have a reduced range of motion in the hips, and pain that escalates with physical activity and improves with immobility/rest. Out of alignment hips can be caused by:
Lifting incorrectly
Repetitively carrying heavy loads on one side of the body places uneven pressure on the pelvis, causing an imbalance.
Performing repetitive motions that begin to stress the joint
If the legs are different lengths, this can cause the hips to go out of alignment. Using a foot wedge/foot orthotic in the shoe can remedy the situation.
Functional Leg Length Discrepancy
Functional leg length discrepancy is a common cause of hip misalignment, meaning that leg length is equal, but the individual is doing something to cause the hips to go out of alignment. It usually involves posture, standing, walking, sitting, lifting, and carrying improperly or awkwardly and repetitively could create functional leg length discrepancy.
Scoliosis
Scoliosis is only one cause of hip misalignment. It is not likely that an individual has scoliosis if they are an adult and have not previously been diagnosed with the condition. If a child has what looks like a misaligned hip, it is recommended to take them to get tested for scoliosis. Most children with the disorder will outgrow it, but they need to be monitored by a medical professional.
One of the most prominent signs that it is a hip problem is the presence of groin pain. Groin pain can radiate downward toward the buttocks, front of the thighs, and knees. The hip joint is located behind the groin; pain usually means the hip is the root cause.
Chiropractic Decompression
A chiropractic examination can identify uneven hips. Chiropractic and motorized spinal decompression can reset the hips to their proper position. A chiropractor will be able to rebalance the hips and help avoid invasive surgical treatments and long-term rehabilitation.
DRX9000 90 Seconds Spinal Decompression
References
Battaglia, Patrick J et al. “Posterior, Lateral, and Anterior Hip Pain Due to Musculoskeletal Origin: A Narrative Literature Review of History, Physical Examination, and Diagnostic Imaging.” Journal of chiropractic medicine vol. 15,4 (2016): 281-293. doi:10.1016/j.jcm.2016.08.004
Jones HR, Burns TM, Aminoff MJ, Pomeroy SL. Pain. Chapter: Diagnosis of Low Back, Buttock, and Hip Pain. Netter Collection of Medical Illustrations: Spinal Cord and Peripheral Motor and Sensory Systems, Section 8, 201-224.
Khamis, Sam, and Eli Carmeli. “A new concept for measuring leg length discrepancy.” Journal of orthopedics vol. 14,2 276-280. 27 Mar. 2017, doi:10.1016/j.jor.2017.03.008
Miyagi, Masayuki, et al. “Hip-spine syndrome: cross-sectional-study of spinal alignment in patients with coxalgia.” Hip international: the journal of clinical and experimental research on hip pathology and therapy vol. 29,1 (2019): 21-25. doi:10.1177/1120700018803236
Nunes, Guilherme S et al. “Acute Effects of Hip Mobilization With Movement Technique on Pain and Biomechanics in Females With Patellofemoral Pain: A Randomized, Placebo-Controlled Trial.” Journal of sport rehabilitation vol. 29,6 707-715. 18 Oct. 2019, doi:10.1123/jsr.2018-0497
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine