Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Dr. Mario Ruja, a chiropractor in El Paso, TX, discuss how chiropractic care can help with personal injuries, especially automobile accidents. Personal injuries can also include work injuries and slip-and-fall injuries. Auto accidents can cause a variety of injuries and underlying conditions, including neck pain, whiplash, back pain, low back pain, and sciatica. Sports injuries can also cause a variety of health issues. Chiropractic care is a safe and effective alternative treatment option that focuses on the diagnosis, treatment, and prevention of health issues associated with the musculoskeletal and nervous system. Dr. Alex Jimenez and Dr. Mario Ruja discuss how spinal adjustments and manual manipulations are commonly utilized to treat neck pain and back pain associated with personal injuries. Whiplash-associated-disorders are the most common types of health issues resulting after an automobile accident. Chiropractic care can carefully restore the original alignment of the spine, treating neck pain and whiplash caused by personal injuries, especially an auto accident. Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Dr. Mario Ruja, a chiropractor in El Paso, TX further discuss how it’s fundamental for people who’ve been involved in a car crash to seek chiropractic care to treat soft tissue injuries that can cause neck pain and back pain. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
In the following podcast video article, Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Daniel (Danny) Alvarado, owner of PUSH Fitness Center in El Paso, TX, discuss the three points of weight loss. Excess weight and obesity are associated with metabolic syndrome and a variety of other health issues. Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing diabetes, stroke, and diabetes, among other complications. Dr. Alex Jimenez and Daniel Alvarado discuss how weight loss can be a safe and effective way to improve metabolic syndrome as well as overall health and wellness. Decreasing or eliminating sugar and carbohydrate consumption, increasing the consumption of proteins, �good� fats, and vegetables, as well as engaging and participating in exercise and physical activity can ultimately help promote weight loss to improve metabolic syndrome and a variety of other health issues. Furthermore, Dr. Alex Jimenez and Daniel Alvarado discuss how they can help people with excess weight and obesity achieve their weight loss goals by encouraging and motivating them through every step of the way. Weight loss is essential for people with metabolic syndrome to achieve overall health and wellness. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Daniel Alvarado & Dr. Alex Jimenez
Subscribe: http://bit.ly/drjyt
Facebook Fitness Center Page: https://www.facebook.com/PUSHftinessathletictraining/
Yelp: El Paso Rehabilitation Center: http://goo.gl/pwY2n2
Yelp: El Paso Clinical Center: Treatment: https://goo.gl/r2QPuZ
Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL or good cholesterol levels are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines, such as the ketogenic diet or the keto diet, as well as demonstrate the biochemical and chemical pathways that the body goes through during ketosis to help people with metabolic syndrome improve their overall health and wellness. From eating good fats and staying hydrated to exercise and better sleep, Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas discuss how diet and lifestyle modifications, such as the ketogenic diet or keto diet, can help improve the 5 risk factors associated with metabolic syndrome to prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Everybody has a backstory. It is not easy. We got to PUSH Hard. It is not EASY…Dr. Alex Jimenez, a chiropractor in El Paso, TX, talks to Daniel (Danny) Alvarado, owner of the PUSH Fitness Center, about the importance of nutrition, diet, and fitness. Stress is the body’s natural response to any physical, mental, and emotional response. Although too much stress can be harmful, getting the right amount of stress is essential for survival. Dr. Alex Jimenez and Daniel Alvarado discuss how stress is the fundamental basis for inspiration and motivation. The PUSH Fitness Center was first created by Danny to help people achieve their optimal health and wellness goals. Hard-work and pushing towards your goal are essential for every individual. Danny discusses how he chooses to inspire and believe in his athletes in order to help them become the best person they can be. Nutrition, diet, and fitness can help prevent a variety of health issues, including metabolic syndrome, diabetes, stroke, and heart disease. Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Daniel (Danny) Alvarado demonstrate how stress, inspiration, and motivation in people can support the hard work and the extra “push” they need to improve themselves, achieve their goals, and improve overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share with us.
Thank You & God Bless.
Daniel Alvarado
Dr. Alex Jimenez
Facebook Fitness Center Page: https://www.facebook.com/PUSHftinessathletictraining/
Metabolic syndrome is a collection of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez and Dr. Mario Ruja explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines to help people with metabolic syndrome improve their overall health and wellness. From eating fiber and staying hydrated to exercise and better sleep, Dr. Alex Jimenez and Dr. Mario Ruja discuss how diet and lifestyle modifications can help improve the 5 risk factors associated with metabolic syndrome to ultimately prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
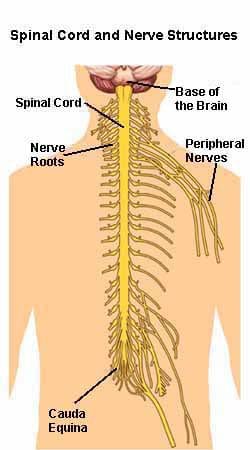
Understanding chronic pain and its alleviation requires an understanding of the anatomy of the nervous system. The nerves of the body are the carriers for the nervous system, as it sends messages to and from the brain. It is quite a complex system. The central nervous system consists of the spinal cord and the brain. The peripheral nervous system branches off the spinal cord.� Both the central and peripheral nervous systems can be affected by neuropathic pain, a type of chronic pain caused by nerve malfunction.
The peripheral nervous system contains 31 pairs of nerve roots that extend from the spinal cord to the rest of the body. There are the feeling nerves/sensory nerves and moving nerves/motor nerves. The chart shows how many pairs of spinal nerves are at each level of the spine.
Peripheral nervous system
The somatic nervous system is comprised of nerves that connect to the musculoskeletal system’s:
Bones
Ligaments
Tendons
Muscles
Skin
It’s what helps generate feeling and what generates the feeling of pain.
It makes sure the heart keeps pumping and the digestive system breaks down food correctly without thinking. Damage to any nerves can lead to the development of chronic pain. The nerves are responsible for sending pain messages, and if they get damaged, they can continually send a steady stream of pain messages.
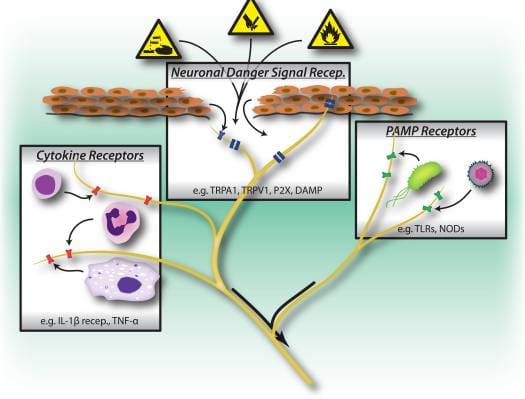
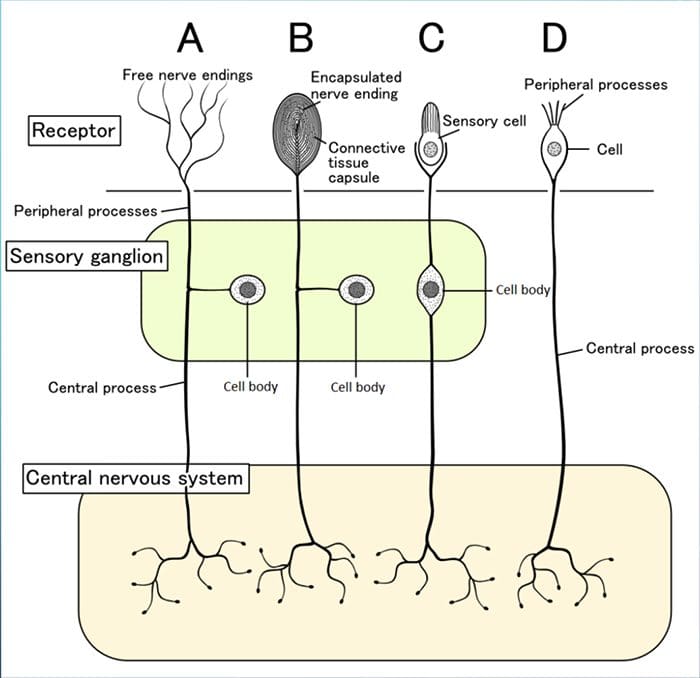
Nociceptorsare another important part of the nerve body. Nociceptors are receptors at the nerve endings, which are activated when something happens and triggers a pain message.
Example: Nociceptors�in the finger turn on and send a pain message through the peripheral nerve to the spinal cord, on to the brain when a finger gets smashed in the car door. Before the finger was smashed, the nociceptors were not on because there was nothing to make them respond.
One possible cause of chronic pain could be malfunctioning nociceptors. Even if there is not a direct or root cause, they could be continually sending pain messages. Using the same example of the finger smashed in the car door. The finger heals after the smashing but pain signals are still being sent. The�finger’s�nociceptor’s nerves could be malfunctioning, which is why they are still sending pain messages. The result is chronic pain.
Chronic pain symptoms
Chronic pain is pain that does not stop for more than 6 months. Pain is a subjective experience, it is different for everyone and takes on many forms. The pain could be:
Aching
Burning
Constant Soreness
Constant Stiffness
Electric
Sharp
Shooting
Throbbing
Tight
Chronic pain can lead to other problems, specifically social, psychological and emotional. It can:
Cause sleeplessness
Drain the body’s energy
Cause depression
Withdraw from activities/friends/family
Weaken the immune system because so much energy is spent dealing with the pain
These added conditions feed off each other. Example: Sleeping is impossible when the pain is active, the next day nothing gets done because of the tiredness. As a result of the inactiveness, a loss of self-esteem begins to set in causing withdrawal from family and social life.
Alleviation
To get the best treatment possible, take note of activities, diet, accidents, injuries, etc before the pain began. Depending on the diagnosis, chiropractic care could help. Research studies have shown that two weeks of regular adjustments/manipulation can bring significant improvement.
Physical therapy combined with stretching and strengthening exercises is part of the treatment for chronic pain. Physical therapy could consist of ice, heat, transcutaneous electrical nerve stimulation, ultrasound, and myofascial release. A chiropractor and other pain professionals can help bring alleviation, so you can fully live your life.
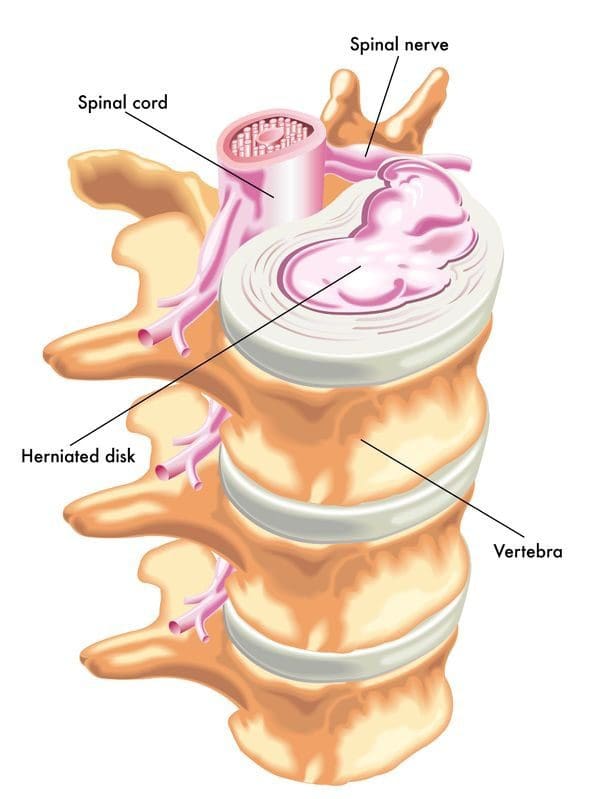
Individuals can develop a herniated, slipped or bulging disc in the neck or back.�Too much stress on the disc/s whether from poor posture, being overweight, injury, aging, and an unhealthy lifestyle can increase the risk for disc problems. Herniation can be caused by a combination of factors or physical injury. Several common questions about disc problems are answered.
Can Discs Slip
A slipped disc can mean a ruptured or herniated disc. We use the term slipped disc, however, the discs do not slip. Each disc is sandwiched between two vertebrae that are supported by a system of ligaments that hold the spine together. A bulging or herniated disc is the proper term.
Difference Between a Bulging and Herniated Disc
Disc disorders are categorized as contained or non-contained. Bulging disc is an example of a contained disc disorder.
Bulging
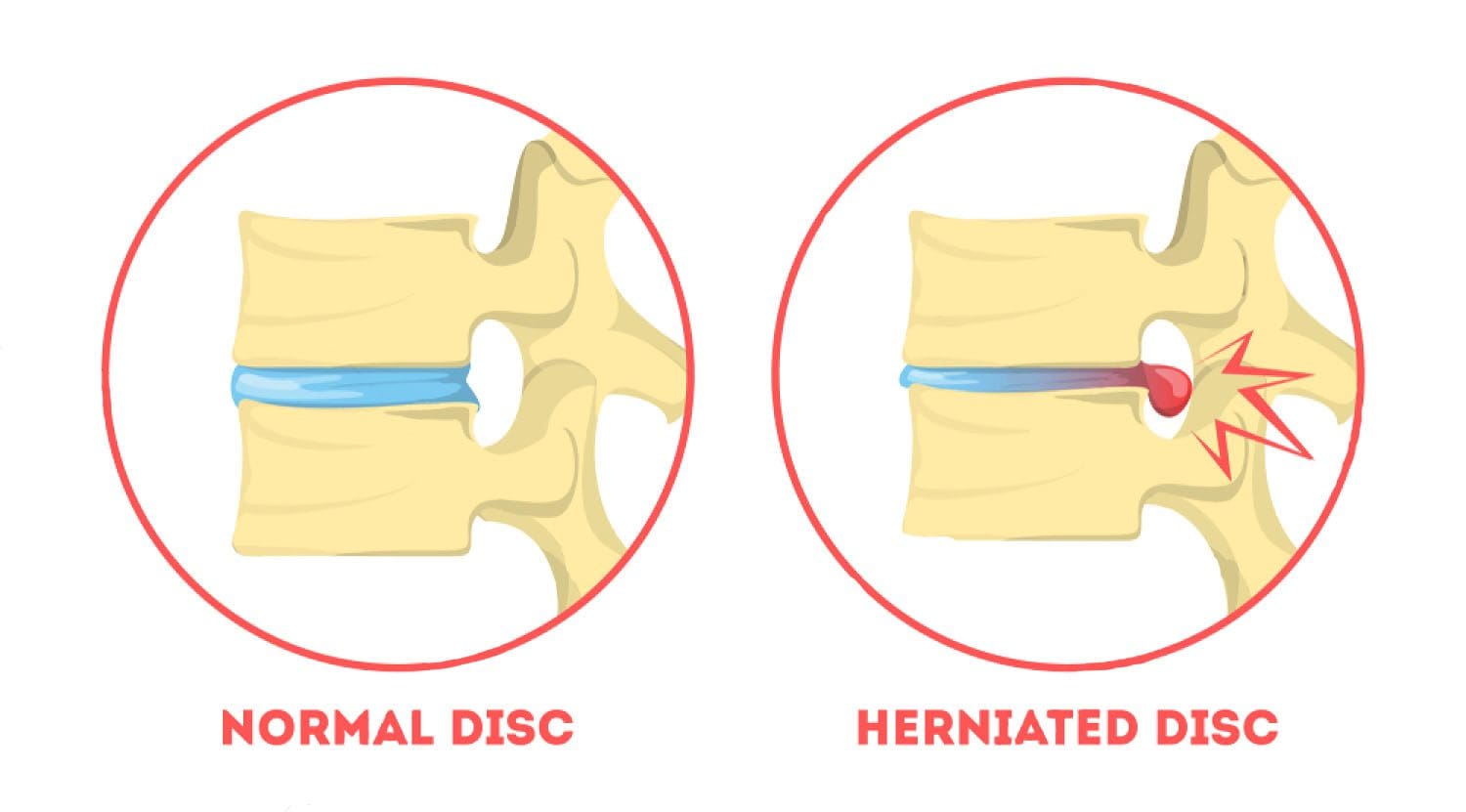
A bulging disc has not broken open meaning the nucleus is still contained inside the annulus fibrosus. The disc could protrude into the spinal canal without breaking open. The gel, the jelly interior does not leak out. The disc stays intact except a small bubble pops out.
Herniated/Ruptured
A non-contained disc has either partially or completely broken open, and that is a herniated/ruptured disc. Imagine a closed tube�being squeezed placed under pressure, which causes the contents to move wherever they can. If a portion of the tube is weak or there is too much pressure, the contents could leak or burst out. When a disc herniates the gel-like contents could spread out to the spinal cord and nerves.
Herniation Can Cause Pain
The disc’s gel-like nucleus has a chemical that irritates the nerves and causes them to become inflamed and swell. The chemical stays and continues to press on the irritated nerves. Sometimes fragments from the disc wall or the tube break off from the disc and drift into the spinal canal causing other nerves to inflame and swell. Based on the type of injury and condition of the discs, more than one disc could herniate, rupture, or bulge. Sometimes injury causes a combination of disc disorders.
Symptoms
Symptoms of a herniated disc can include:
Dull
Shooting pain
Muscle spasms
Cramping
Weakness
Tingling
Referred or radiating/traveling pain
Sometimes, however, a herniated disc does not cause any symptoms at all. When this happens it is called an asymptomatic herniated disc. Disc/s could be bulging or herniated, but if it or they are not applying pressure on the spinal nerve/sor the cord, symptoms like pain may not present. This makes a point about herniated disc symptoms that they are dependent on where you have a herniated disc.
Cervical Herniation Symptoms
With a herniated or bulging disc in the neck, then you could experience:
Neck soreness/pain
Muscle tightness
Cramping in the neck
Pain that travels down the arm/s
Tingling in the arm/s or hand/s
Weakness in the arm/s or hand/s
Lumbar Herniation Symptoms
With a herniated disc in the low back the following symptoms could happen:
Low back pain
Muscle tightness
Cramping in and around the low back
Radiating pain that travels down the leg/s
Tingling in your leg/s or foot/feet
Weakness in the leg/s or foot/feet
Referred Pain
Referred pain means that you have pain in another part of the body from the disc problem. An individual could have a bulging or herniated slipped disc in the low back and have pain in the leg. This is lumbar radiculopathy or sciatica. Usually, just one leg is affected. If you have a herniated disc in the neck, there could be referred pain going down the arm and into the hand.
Chiropractic Cares
A chiropractor can help relieve back pain and other herniated disc symptoms. A chiropractor will go through your medical history, do a physical exam, and perform orthopedic and neurological tests. They are looking at several things. Orthopedic and neurological exams can help the chiropractor figure out what’s going on.
Are reflexes functioning properly?�Meaning are your nerves sending messages correctly. An example is a reflex test is when a doctor taps the knee with a hammer and the leg kicks.
Is there a loss of muscle strength?
Signs of muscle/s wasting away?
Is there a loss of sensation, tingling or numbness along the nerve/s path?
They will carefully look at posture, and will probably order an X-ray or MRI to help with the diagnosis.
Chiropractors evaluate the entire spine. Even if you only have lower back pain, your chiropractor will examine your neck, too. They want to see how well your spine is functioning overall. Remember what happens to one area of your spine can influence another part of the spine and/or body.
Pain from a herniated disc can make it difficult to enjoy daily life. Walking, sitting, and sleeping normally/comfortably can become a nightmare. You should make an appointment with a doctor or chiropractor if your herniated slipped disc symptoms last for more than two weeks.
Herniated Disc Treatment
NCBI Resources
In the United States alone, acute cases of lower back pain are the fifth most frequent reason for doctor visits and cause 40% of missed days off work. What�s more, it is the leading cause of disability worldwide.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine