Federal employees that are injured at work do not get benefits through workers’ comp insurance or their nation’s workers’ comp program.
Instead, federal employees receive workers’ compensation benefits through the Federal Employees Compensation Act, abbreviated as FECA, except for railroad workers, longshoremen, black lung coal miners, and refuge workers (that are insured under their own national laws for workers’ compensation). Members of the USA armed forces are also not considered federal employees for purposes of FECA.
FECA provides benefits and injury compensation for workers injured on the job, or even if their injury happened during the course and scope of their employment offsite. FECA covers both injuries and occupational diseases that arise over time work conditions. The United States Department of Labor, through the Office of Worker Compensation Programs, administers the workers’ comp benefits provided by the Federal Employees Compensation Act.
Qualifications
Coverage under FECA, or the Federal Employees Compensation Act, is supplied to all national government employees regardless of the number of years of service, nature of the position, or kind of job they perform. In order to be covered by FECA, you must be employed by the federal government, not a private government contractor. If you are currently working for a private business, the workers’ compensation laws in the state will cover you.
For the injury or illness to qualify under FECA, then you must have become injured while performing duties of your job or you developed a disease because of the conditions and hazards inherent in your job. This may consist of accidents occurring while working or traveling offsite as well.
FECA does not cover injuries and diseases that arise because of activities beyond the “course and scope of your employment.” Activities beyond the course and scope of employment include commuting to and from work, recreational excursions, and activities for private reasons. Injuries sustained while intoxicated or under the influence of non-prescription drugs will not be covered by the Federal Employees Compensation Act. FECA also provides benefits to surviving family members for employees that die on the job while performing work-related pursuits.
Back Pain in Federal Employees
As with anyone experiencing symptoms of back pain after being involved in a work accident, due to aggravated conditions or illness, or simply from wear-and-tear injuries, it’s essential for federal employees to seek the proper care and benefits for their symptoms to receive immediate medical attention. Spine issues resulting in sciatica can be debilitating and may affect an employee’s capability to work. Programs for federal employees like FECA may help substantially improve an individual’s overall health and wellness, allowing them to return to work as soon as possible.
FECA Workers’ Compensation Benefits
If your FECA workers’ compensation claim is permitted, you will start to receive workers’ compensation benefits to compensate you for your injury or illness and help you with the recovery. First, FECA will cover all necessary and appropriate claim-related medical therapy. This includes prescriptions, surgery and rehabilitation.
The Federal Employees Compensation Act provides compensation if a worker is disabled and unable to work as a result of industrial injury or occupational disease. You will be compensated by your service directly for your lost wages and more. Should your inability to work exceed 45 days, FECA will cover your wages that are lost.
If your workers’ compensation claim is based on an occupational disease, you’re entitled to compensation for lost salary from FECA after an initial three-day waiting period.
If your injury or illness results in permanent partial disability or permanent total disability, FECA will provide advantages and additional benefits. The total amount of the compensation is based on the severity of your permanent disability and the effect it has on your earning capacity. And if you have dependents, you will probably receive increased permanent disability compensation to account for your own requirement to supply for those dependents.
In the event that you need job retraining to return to the workforce after your injury or illness FECA provides compensation. Dependents are eligible to receive survivor’s benefits. For further details regarding the benefits of the Federal Employees Compansation Act, visit the�Division of Federal Employees’ Compensation (DFEC).
Speak to an Attorney
If your FECA employees’ compensation claim is refused, your claim may be more complicated, or your injury may have been considered more severe. You should carefully consider speaking to a lawyer in your area experienced in FECA employees’ compensation law. Although an attorney isn’t necessary to obtain workers’ compensation benefits, an attorney can help in ensuring you get all of the benefits you’re entitled to get, guiding you through the procedure.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Back pain is one of the most common symptoms reported among the general population. While back pain can occur due to a variety of injuries and/or underlying conditions, a work accident has often been associated as a frequent origin of back pain issues. Back pain can affect an individual at least once throughout their lifetime. Fortunately, federal employees who experience back pain, such as symptoms of sciatica, can benefit from programs like FECA.
After ruling out a herniated disc is not causing your sciatic nerve problems, you should look to the pelvis and many times the culprit is the piriformis muscle.
When the piriformis becomes tight or inflamed, it can put pressure on the sciatic nerve and you can get the sensations going down the leg. �Symptoms such as numbness, tingling, and sharp shooting pain.
A common mistake I�ve seen on YouTube videos and at different gyms and clinics, is people using a tennis ball, lacrosse ball, or foam rollers to apply pressure to the piriformis muscle in order to relax it.
If your sciatica is caused by piriformis syndrome, applying pressure to an area that�s already compressed will only add more pressure to the sciatic nerve and cause more pain.
What you should do instead, is stretch the muscle causing the problem so that it relaxes and takes pressure off the sciatic nerve. In this video you�ll learn an easy stretch you can do on the floor.
You simply lay on your back with both legs bent. Then cross the painful leg over the good one. And pull the affected leg towards the opposite shoulder and hold that stretch for 30 seconds.
Repeat the stretch as needed.
This will help to relieve the sciatic pain associated with piriformis syndrome.
As with any conditions, there is no quick fix. You have to consistently perform sciatica stretches and exercises to achieve the best results.
Thomas M Kosloff1*�, David Elton1�, Jiang Tao2� and Wade M Bannister2�
CHIROPRACTIC & MANUAL THERAPIES
Abstract
Background: There is controversy surrounding the risk of manipulation, which is often used by chiropractors, with respect to its association with vertebrobasilar artery system (VBA) stroke. The objective of this study was to compare the associations between chiropractic care and VBA stroke with recent primary care physician (PCP) care and VBA stroke.
Methods: The study design was a case�control study of commercially insured and Medicare Advantage (MA) health plan members in the U.S. population between January 1, 2011 and December 31, 2013. Administrative data were used to identify exposures to chiropractic and PCP care. Separate analyses using conditional logistic regression were conducted for the commercially insured and the MA populations. The analysis of the commercial population was further stratified by age (<45 years; ?45 years). Odds ratios were calculated to measure associations for different hazard periods. A secondary descriptive analysis was conducted to determine the relevance of using chiropractic visits as a proxy for exposure to manipulative treatment.
Results: There were a total of 1,829 VBA stroke cases (1,159 � commercial; 670 � MA). The findings showed no significant association between chiropractic visits and VBA stroke for either population or for samples stratified by age. In both commercial and MA populations, there was a significant association between PCP visits and VBA stroke incidence regardless of length of hazard period. The results were similar for age-stratified samples. The findings of the secondary analysis showed that chiropractic visits did not report the inclusion of manipulation in almost one third of stroke cases in the commercial population and in only 1 of 2 cases of the MA cohort.
Conclusions: We found no significant association between exposure to chiropractic care and the risk of VBA stroke. We conclude that manipulation is an unlikely cause of VBA stroke. The positive association between PCP visits and VBA stroke is most likely due to patient decisions to seek care for the symptoms (headache and neck pain) of arterial dissection. We further conclude that using chiropractic visits as a measure of exposure to manipulation may result in unreliable estimates of the strength of association with the occurrence of VBA stroke.
Keywords: Chiropractic, Primary care, Cervical manipulation, Vertebrobasilar stroke, Adverse events
Background
The burden of neck pain and headache or migraine among adults in the United States is significant. Survey data indicate 13% of adults reported neck pain in the past 3 months [1]. In any given year, neck pain affects 30% to 50% of adults in the general population [2]. Prevalence rates were reportedly greater in more eco- nomically advantaged countries, such as the USA, with a higher incidence of neck pain noted in office and com- puter workers [3]. Similar to neck pain, the prevalence of headache is substantial. During any 3-month time- frame, severe headaches or migraines reportedly affect one in eight adults [1].
Neck pain is a very common reason for seeking health care services. �In 2004, 16.4 million patient visits or 1.5% of all health care visits to hospitals and physician offices, were for neck pain� [4]. Eighty percent (80%) of visits occurred as outpatient care in a physician�s office [4]. The utilization of health care resources for the treatment of headache is also significant. �In 2006, adults made nearly 11 million physician visits with a headache diagno- sis, over 1 million outpatient hospital visits, 3.3 million emergency department visits, and 445 thousand inpatient hospitalizations� [1].
In the United States, chiropractic care is frequently utilized by individuals with neck and/or headache com- plaints. A national survey of chiropractors in 2003 re- ported that neck conditions and headache/facial pain accounted respectively for 18.7% and 12% of the patient chief complaints [5]. Chiropractors routinely employ spinal manipulative treatment (SMT) in the management of patients presenting with neck and/or headache [6], either alone or combined with other treatment approaches [7-10].
While evidence syntheses suggest the benefits of SMT for neck pain [7-9,11-13] and various types of headaches [10,12,14-16], the potential for rare but serious adverse events (AE) following cervical SMT is a concern for researchers [17,18], practitioners [19,20], professional organizations [21-23], policymakers [24,25] and the public [26,27]. In particular, the occurrence of stroke affecting the vertebrobasilar artery system (VBA stroke) has been associated with cervical manipulation. A recent publication [28] assessing the safety of chiropractic care reported, �…the frequency of serious adverse events varied between 5 strokes/ 100,000 manipulations to 1.46 serious adverse events/ 10,000,000 manipulations and 2.68 deaths/10,000,000 manipulations�. These estimates were, however, derived from retrospective anecdotal reports and liability claims data, and do not permit confident conclusions about the actual frequency of neurological complications following spinal manipulation.
Several systematic reviews investigating the association between stroke and chiropractic cervical manipulation�have reported the data are insufficient to produce definitive conclusions about its safety [28-31]. Two case�control studies [32,33] used visits to a chiropractor as a proxy for SMT in their analyses of standardized health system databases for the population of Ontario (Canada). The more recent of these studies [32] also included a case-crossover methodology, which reduced the risk of bias from confounding variables. Both case�control studies reported an increased risk of VBA stroke in association with chiropractic visits for the population under age 45 years old. Cassidy, et al. [32] found, how- ever, the association was similar to visits to a primary care physician (PCP). Consequently, the results of this study suggested the association between chiropractic care and stroke was non-causal. In contrast to these studies, which found a significant association between chiropractic visits and VBA stroke in younger patients (<45 yrs.), the analysis of a population-based case-series suggested that VBA stroke patients who consulted a chiropractor the year before their stroke were older (mean age 57.6 yrs.) than previously documented [34].
The work by Cassidy, et al. [32] has been qualitatively appraised as one of the most robustly designed investigations of the association between chiropractic manipulative treatment and VBA stroke [31]. To the best of our knowledge, this work has not been reproduced in the U.S. population. Thus, the main purpose of this study is to replicate the case�control epidemiological design published by Cassidy, et al. [32] to investigate the association between chiropractic care and VBA stroke; and compare it to the association between recent PCP care and VBA stroke in samples of the U.S. commercial and Medicare Advantage (MA) populations. A secondary aim of this study is to assess the utility of employing chiropractic visits as a proxy measure for exposure to spinal manipulation.
Methods
Study design and population
We developed a case�control study based on the experience of commercially insured and MA health plan members between January 1, 2011 and December 31, 2013. General criteria for membership in a commercial or MA health plan included either residing or working in a region where health care coverage was offered by the in- surer. Individuals must have Medicare Part A and Part B to join a MA plan. The data set included health plan members located in 49 of 50 states. North Dakota was the only State not represented.
Both case and control data were extracted from the same source population, which encompassed national health plan data for 35,726,224 unique commercial and 3,188,825 unique MA members. Since members might be enrolled for more than one year, the average�annual commercial membership was 14.7 million members and the average annual MA membership was 1.4 million members over the three year study period, which is comparable to ~5% of the total US population based on the data available from US Census Bureau [35]. Administrative claims data were used to identify cases, as well as patient characteristics and health service utilization.
The stroke cases included all patients admitted to an acute care hospital with vertebrobasilar (VBA) occlusion and stenosis strokes as defined by ICD-9 codes of 433.0, 433.01, 433.20, and 433.21 during the study period. Pa- tients with more than one admission for a VBA stroke were excluded from the study. For each stroke case, four age and gender matched controls were randomly se- lected from sampled qualified members. Both cases and controls were randomly sorted prior to the matching using a greedy matching algorithm [36].
Exposures
The index date was defined as the date of admission for the VBA stroke. Any encounters with a chiropractor or a primary care physician (PCP) prior to the index date were considered as exposures. To evaluate the impact of chiropractic and PCP treatment, the designated hazard period in this study was zero to 30 days prior to the index date. For the PCP analysis, the index date was excluded from the hazard period since patients might consult PCPs after having a stroke. The standard health plan coverage included a limit of 20 chiropractic visits. In rare circumstances a small employer may have selected a 12-visit limit. An internal analysis (data not shown) revealed that 5% of the combined (commercial and MA) populations reached their chiropractic visit limits. Instances of an employer not covering chiropractic care were estimated to be so rare that it would have had no measurable impact on the analysis. There were no limits on the number of reimbursed PCP visits per year.
Analyses
Two sets of similar analyses were performed, one for the commercially insured population and one for the MA population. In each set of analyses, conditional logistic regression models were used to examine the association between the exposures and VBA strokes. To measure the association, we estimated the odds ratio of having the VBA stroke and the effect of total number of chiropractic visits and PCP visits within the hazard period. The analyses were applied to different hazard periods, including one day, three days, seven days, 14 days and 30 days for both chiropractic and PCP visits. The results of the chiropractic and PCP visit analyses were then compared to find evidence of excess risk of having stroke for patients with chiropractic visits during the
hazard period. Previous research has indicated that most patients who experience a vertebral artery dissection are under the age of 45. Therefore, in order to investigate the impact of exposure on the population at different ages, separate analyses were performed on patients stratified by age (under 45 years and 45 years and up) for the study of the commercial population. The number of visits within the hazard period was entered as a con- tinuous variable in the logistic model. The chi square test was used to analyze the proportion of co-morbidities in cases as compared to controls.
A secondary analysis was performed to evaluate the relevance of using chiropractic visits as a proxy for spinal manipulation. The commercial and MA databases were queried to identify the proportions of cases of VBA stroke and matched controls for which at least one chiropractic spinal manipulative treatment procedural code (CPT 98940 � 98942) was or was not recorded. The analysis also calculated the use of another manual therapy code (CPT 97140), which may be employed by chiropractors as an alternative means of reporting spinal manipulation.
Ethics
The New England Institutional Review Board (NEIRB) determined that this study was exempt from ethics review.
Results
The commercial study sample included 1,159 VBA stroke cases over the three year period and 4,633 age and gender matched controls. The average age of the patients was 65.1 years and 64.8% of the patients were male (Table 1). The prevalence rate of VBA stroke in the commercial population was 0.0032%.
There were a total of 670 stroke cases and 2,680 matched controls included in the MA study. The aver- age patient age was 76.1 years and 58.6% of the patients were male (Table 2). For the MA population, the prevalence rate of VBA stroke was 0.021%.
Claims during a one year period prior to the index date were extracted to identify comorbid disorders. Both the commercial and MA cases had a high percentage of comorbidities, with 71.5% of cases in the commercial study and 88.5% of the cases in the MA study reporting at least one of the comorbid conditions (Table 3). Six comorbid conditions of particular interest were identified, including hypertensive disease (ICD-9 401�404), ischemic�heart disease (ICD-9 410�414), disease of pulmonary circulation (ICD-9 415�417), other forms of heart disease (ICD-9 420�429), pure hypercholesterolemia (ICD-9 272.0) and diseases of other endocrine glands (ICD-9 249�250). There were statistically significant differences (p = <0.05) between groups for most comorbidities. Greater proportions of comorbid disorders (p = <0.0001) were reported in the commercial and MA cases for hyper- tensive disease, heart disease and endocrine disorders (Table 3). The commercial cases also showed a larger proportion of diseases of pulmonary circulation, which was statistically significant (p = 0.0008). There were no significance differences in pure hypercholesterolemia for either the commercial or MA populations. Overall, cases in both the commercial and MA populations were more likely (p = <0.0001) to have at least one co- morbid condition.
Among the commercially insured, 1.6% of stroke cases had visited chiropractors within 30 days of being admit- ted to the hospital, as compared to 1.3% of controls visit- ing chiropractors within 30 days prior to their index date. Of the stroke cases, 18.9% had visited a PCP within 30 days prior to their index date, while only 6.8% of controls had visited a PCP (Table 4). The proportion of exposures for chiropractic visits was lower in the MA sample within the 30-day hazard period (cases = 0.3%; controls = 0.9%). However, the proportion of exposures for PCP visits was higher, with 21.3% of cases having PCP visits as compared to12.9% for controls (Table 5).
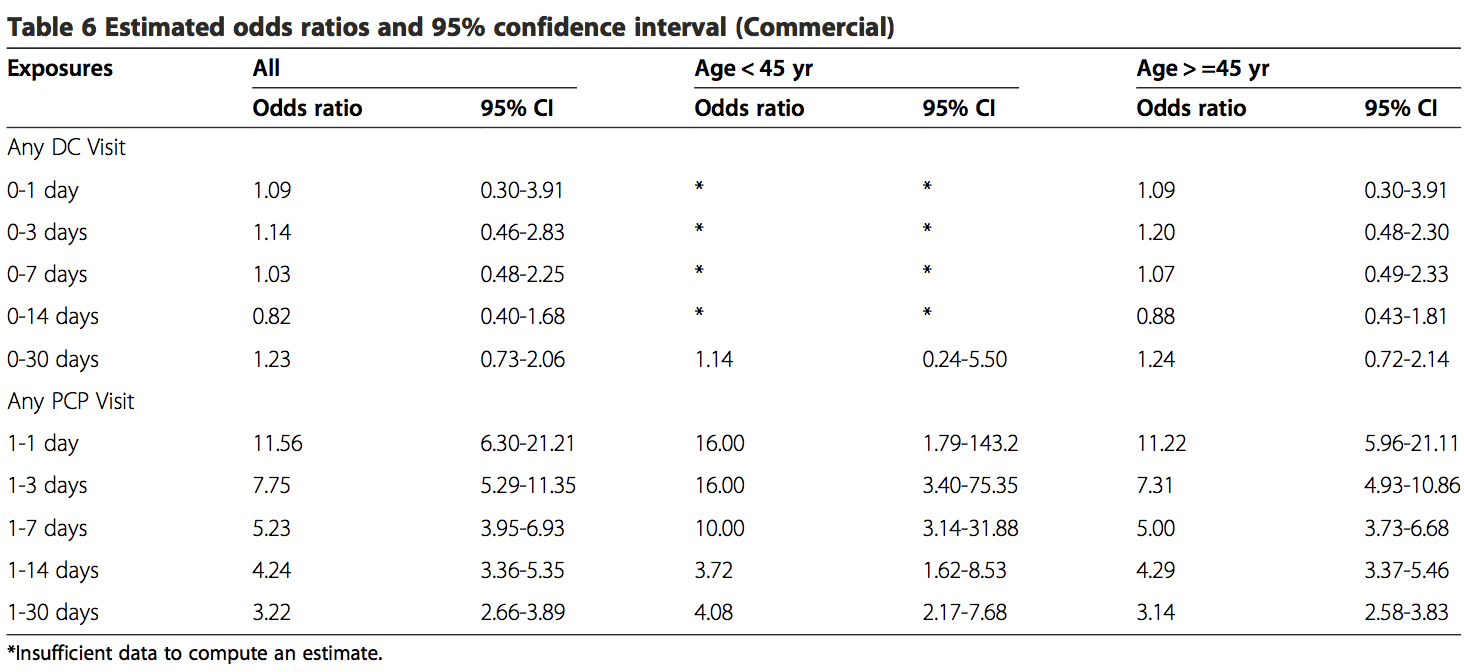
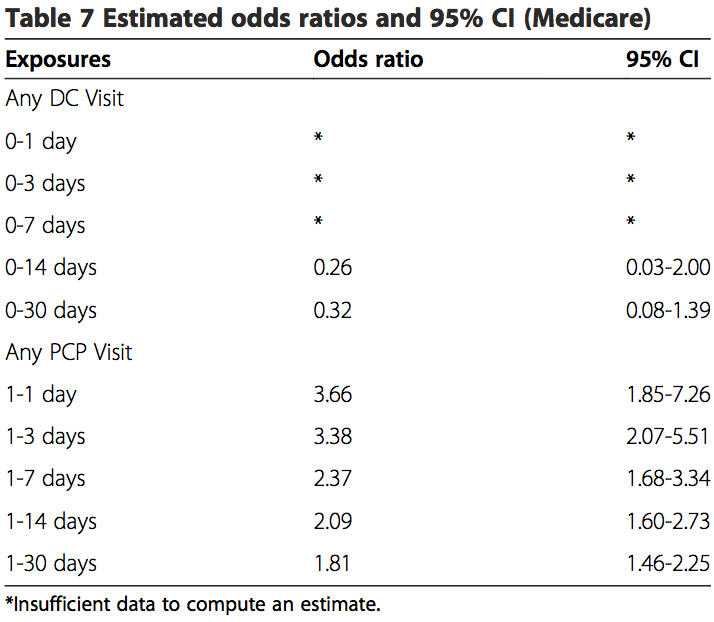
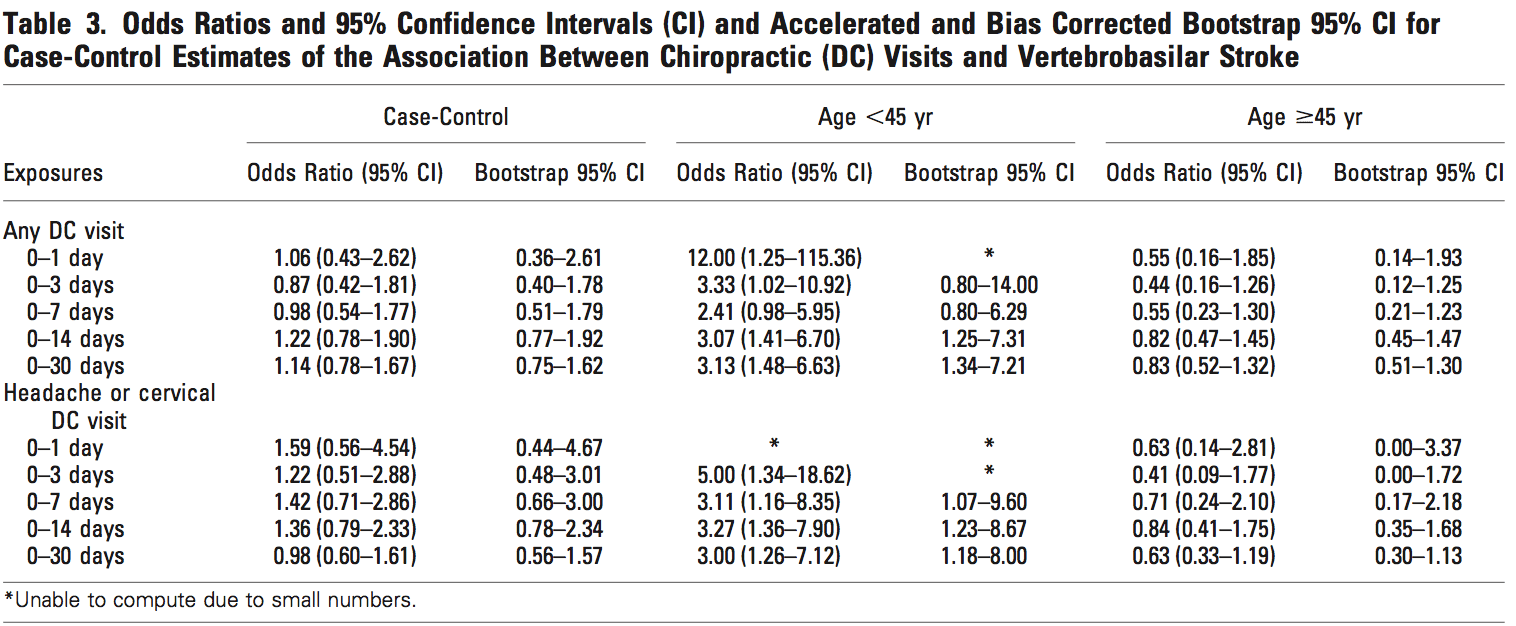
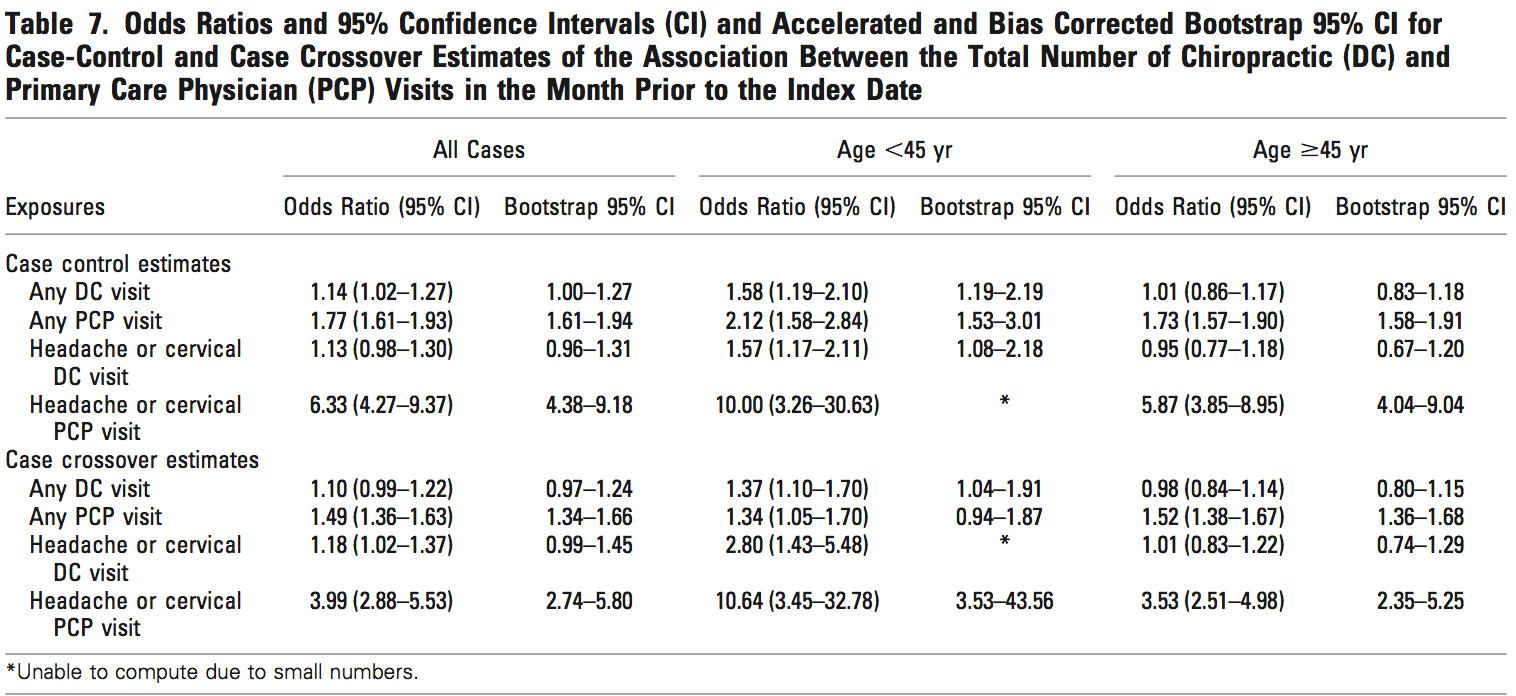
The results from the analyses of both the commercial population and the MA population were similar (Tables 6, 7 and 8). There was no association between chiropractic visits and VBA stroke found for the�overall sample, or for samples stratified by age. No estimated odds ratio was significant at the 95% confidence level. MA data were insufficient to calculate statistical measures of association for hazard periods less than 0�14 days for chiropractic visits. When stratified by age, the data were too sparse to calculate measures of association for hazard periods less than 0�30 days in the commercial population. The data were too few to analyze associative risk by headache and/or neck pain diagnoses (data not shown).
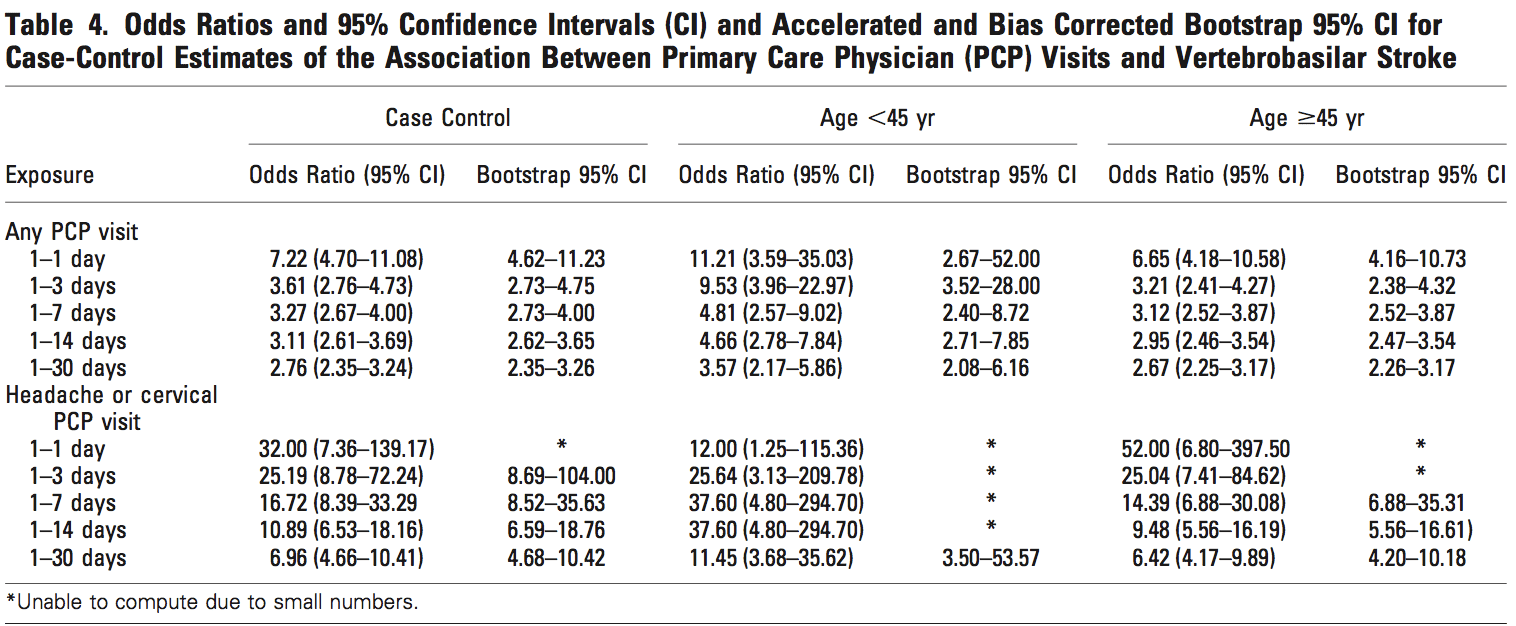
These results showed there is an association existing between PCP visits and VBA stroke incidence regardless of age or length of hazard period. A strong association was found for those visits close to the index date (OR 11.56; 95% CI 6.32-21.21) for all patients with a PCP visit within 0�1 day hazard period in the commercial sample. There was an increased risk of VBA stroke associated with each PCP visit within 30-days prior to the index date for MA patients (OR 1.51; 95% CI 1.32-1.73) and commercial patients (OR 2.01; 95% CI 1.77-2.29).
The findings of the secondary analysis showed � that of 1159 stroke cases from commercial population � there were a total of 19 stroke cases associated with chiropractic visits for which 13 (68%) had claims documentation indicating chiropractic SMT was performed. For the control group of the commercial cohort, 62 of 4633 controls had claims of any kind of chiropractic visits and 47 of 4633 controls had claims of SMT. In the commercial control group, 47 of 62 DC visits (76%) included SMT in the claims data. Only 1 of 2 stroke cases in the MA population included SMT in the claims data. For the MA cohort, 21 of 24 control chiropractic visits (88%) included SMT in the claims data (Table 9).
None of the stroke cases in either population included CPT 97140 as a substitute for the more conventionally re- ported chiropractic manipulative treatment procedural codes (98940 � 98942). For the control groups, there were three instances where CPT 97140 was reported without CPT 98940 � 98942 in the commercial population. The CPT code 97140 was not reported in MA control cohort.
Discussion
The primary aim of the present study was to investigate the association between chiropractic manipulative treatment and VBA stroke in a sample of the U.S. population. This study was modeled after a case�control design previously conducted for a Canadian population [32]. Administrative data for enrollees in a large national health care insurer were analyzed to explore the occurrence of VBA stroke across different time periods of exposure to chiropractic care in comparison with PCP care.
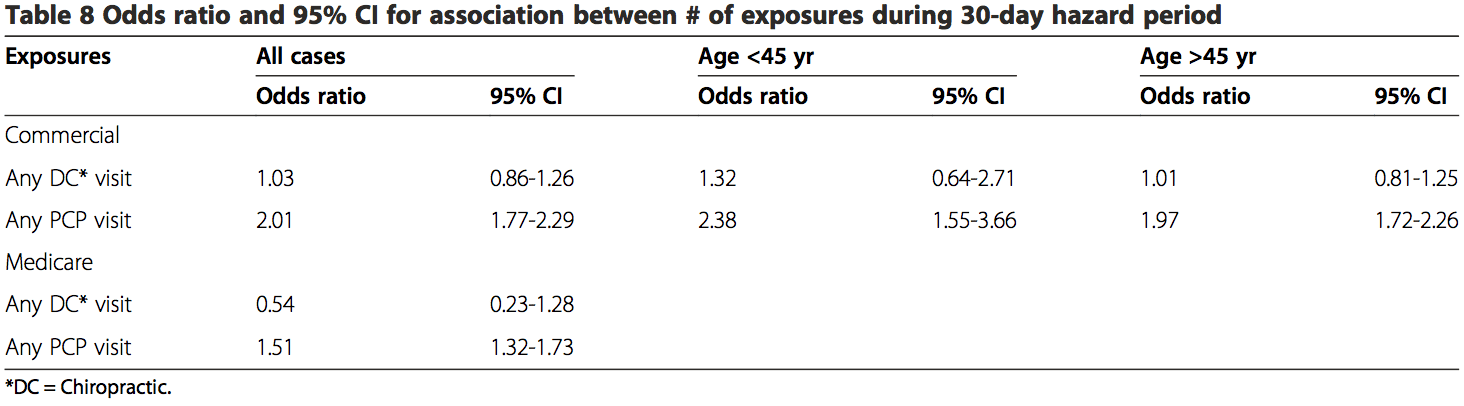
Unlike Cassidy et al. [32] and most other case�control studies [33,37,38], our results showed there was no significant association between VBA stroke and chiropractic visits. This was the case for both the commercial and MA populations. In contrast to two earlier case�control studies [32,33], this lack of association was found to be irrespective of age. Although, our results (Table 8) did lend credence to previous reports that VBA stroke occurs more frequently in patients under the age of 45 years. Additionally, the results from the present study did not identify a relevant temporal impact. There was no significant association, when the data were sufficient to calculate estimates, between chiropractic visits and stroke regardless of the hazard period (timing of most recent visit to a chiropractor and the occurrence of stroke).
There are several possible reasons for the variation in results with previous similar case�control studies. The younger (<45 yrs.) commercial cohort that received chiropractic care in our study had noticeably fewer cases. The 0�30 days hazard period included only 2 VBA stroke cases. There were no stroke cases for other hazard periods in this population. In contrast, earlier studies reported sufficient cases to calculate risk estimates for most hazard periods [32,33].
Another factor that potentially influenced the difference in results concerns the accuracy of hospital claims data in the U.S. vs. Ontario, Canada. The source population in the Province of Ontario was identified, in part, from the Discharge Abstract Database (DAD). The DAD includes hospital discharge and emergency visit diagnoses that have undergone a standardized assessment by a medical records coder [39]. To the best of our know- ledge, similar quality management practices were not routinely applied to hospital claims data used in sourcing the population for our study.
An additional reason for the disparity in results may be due to differences in the proportions of chiropractic visits where SMT was reportedly performed. Our study showed that SMT was not reported by chiropractors in more than 30% of commercial cases. It is plausible that a number of the cases in earlier studies also did not�include SMT as an intervention. Differences between studies in the proportion of cases reporting SMT may have affected the calculation of risk estimates.
Also, there were an insufficient number of cases having cervical and/or headache diagnoses in our study. Therefore, our sample population may have included proportionally less cases where cervical manipulation was performed.
Our results were consistent with previous findings [32,33] in showing a significant association between PCP visits and VBA stroke. The odds ratios for any PCP visit increase dramatically from 1�30 days to 1�1 day (Tables 6 and 7). This finding is consistent with the hypothesis that patients are more likely to see a PCP for symptoms related to vertebral artery dissection closer to the index date of their actual stroke. Since it is unlikely that the services provided by PCPs cause VBA strokes, the association�between recent PCP visits and VBA stroke is more likely attributable to the background risk related to the natural history of the condition [32].
A secondary goal of our study was to assess the utility of employing chiropractic visits as a surrogate for SMT. Our findings indicate there is a high risk of bias associated with using this approach, which likely overestimated the strength of association. Less than 70% of stroke cases (commercial and MA) associated with chiropractic care included SMT. A somewhat higher proportion of chiropractic visits included SMT for the control groups (commercial = 76%; MA = 88%).
There are plausible reasons that support these findings. Internal analyses of claims data (not shown) consistently demonstrate that one visit is the most common number associated with a chiropractic episode of care. The single visit may consist of an evaluation without treatment such as SMT. Further; SMT may have been viewed as contraindicated due to signs and symptoms of vertebral artery dissection (VAD) and/or stroke. This might explain the greater proportion of SMT provided to control groups in both the commercial and MA populations.
Overall, our results increase confidence in the findings of a previous study [32], which concluded there was no excess risk of VBA stroke associated chiropractic care compared to primary care. Further, our results indicate there is no significant risk of VBA stroke associated with chiropractic care. Additionally, our findings highlight the potential flaws in using a surrogate variable (chiropractic visits) to estimate the risk of VBA stroke in association with a specific intervention (manipulation).
Our study had a number of strengths and limitations. Both case and control data were extracted from the same source population, which encompassed national health plan data for approximately 36 million�commercial and 3 million MA members. A total of 1,829 cases were identified, making this the largest case� control study to investigate the association between chiropractic manipulation and VBA stroke. Due to the nationwide setting and large sample size, our study likely reduced the risk of bias related to geographic factors. However, there was a risk of selection bias � owing to the data set being from a single health insurer � including income status, workforce participation, and links to health care providers and hospitals.
Our study closely followed a methodological approach that had previously been described [32], thus allowing for more confident comparisons.
The current investigation analyzed data for a number of comorbid conditions that have been identified as potentially modifiable risk factors for a first ischemic stroke [40]. The differences between groups were statistically significant for most comorbidities. Information was not obtainable about behavioral comorbid factors e.g., smoking and body mass. With the exception of hypertensive disease, there are reasons to question the clinical significance of these conditions in the occurrence of ischemic stroke due to vertebral artery dissection. A large multinational case-referent study investigated the association between vascular risk factors (history of vascular disease, hypertension, smoking, hypercholesterolemia, diabetes mellitus, and obesity/overweight) for ischemic stroke and the occurrence of cervical artery dissection [41]. Only hypertension had a positive association (odds ratio 1.67; 95% confidence interval, 1.32 to 2.1; P <0.0001) with cervical artery dissection.
While the effect of other unmeasured confounders cannot be discounted, there is reason to suspect the absence of these data was not deleterious to the results. Cassidy, et al. found no significant differences in the results their case-crossover design, which affords better control of unknown confounding variables, and the findings of their case�control study [32].
Our results highlight just how unusual VBA stroke is in the MA cohort (prevalence = 0.021%) and � even more so � for the commercial population (prevalence = 0.0032%). As a result, some limitations of this study re- lated to the rarity of reporting VBA stroke events. Despite the larger number of cases, data were insufficient to calculate estimates and confidence intervals for seven measures of exposure (4 commercial and 3 MA) for chiropractic visits. Additionally, we were not able to compute estimates specifically for headache and neck pain diagnoses due to small numbers. Confidence intervals associated with estimates tended to be wide making the results imprecise [42].
There were limitations related to the use of administrative claims data. �Disadvantages of using secondary data for research purposes include: variations in coding from hospital to hospital or from department to department, errors in coding and incomplete coding, for example in the presence of comorbidities. Random errors in coding and registration of discharge diagnoses may dilute and attenuate estimates of statistical association� [43]. The recordings of unvalidated hospital discharge diagnostic codes for stroke have been shown to be less precise when compared to chart review [44,45] and validated patient registries�[43,46]. Cassidy, et al. [32] conducted a sensitivity analysis to determine the effect of diagnostic misclassification bias. Their conclusions did not change when the effects of misclassification were assumed to be similarly distributed between chiropractic and PCP cases.
A particular limitation in using administrative claims data is the paucity of contextual information surround- ing the clinical encounters between chiropractors/PCPs and their patients. Historical elements describing the occurrence/absence of recent trauma or activities reported in case studies [47-51] as potential risk factors for VBA stroke were not available in claims data. Confidence was low concerning the ability of claims data to provide accurate and complete reporting of other health disorders, which have been described in case�control designs as being associated with the occurrence of VBA stroke e.g., migraine [52] or recent infection [53]. Symptoms and physical examination findings that would have permitted further stratification of cases were not reported in the claims data.
The reporting of clinical procedures using current pro- cedural terminology (CPT) codes presented additional shortcomings concerning the accuracy and interpretation of administrative data. One inherent constraint was the lack of anatomic specificity associated with the use of standardized procedural codes in claims data. Chiropractic manipulative treatment codes (CPT 98940 � 98942) have been formatted to describe the number of spinal regions receiving manipulation. They do not identify the particular spinal regions manipulated.
Also, treatment information describing the type(s) of manipulation was not available. When SMT was re- ported, claims data could not discriminate among the range of techniques including thrust or rotational manipulation, various non-thrust interventions e.g., mechanical instruments, soft tissue mobilizations, muscle energy techniques, manual cervical traction, etc. Many of these techniques do not incorporate the same bio- mechanical stressors associated with the type of manipulation (high velocity low amplitude) that has been investigated as a putative risk factor for VBA stroke [54-56]. It seems plausible that the utility of future VBA stroke research would benefit from explicit descriptions of the particular type of manipulation performed.
Moreover, patient responses to care � including any adverse events suggestive of vertebral artery dissection or stroke-like symptoms � were not obtainable in the data set used for the current study.
In the absence of performing comprehensive clinical chart audits, it is not possible to know from claims data what actually transpired in the clinical encounter. Further, chart notes may themselves be incomplete or otherwise fail to precisely describe the nature of interventions [57]. Therefore, manipulation codes represent surrogate
measures, albeit more direct surrogate measures, than simply using the exposure to chiropractic visits.
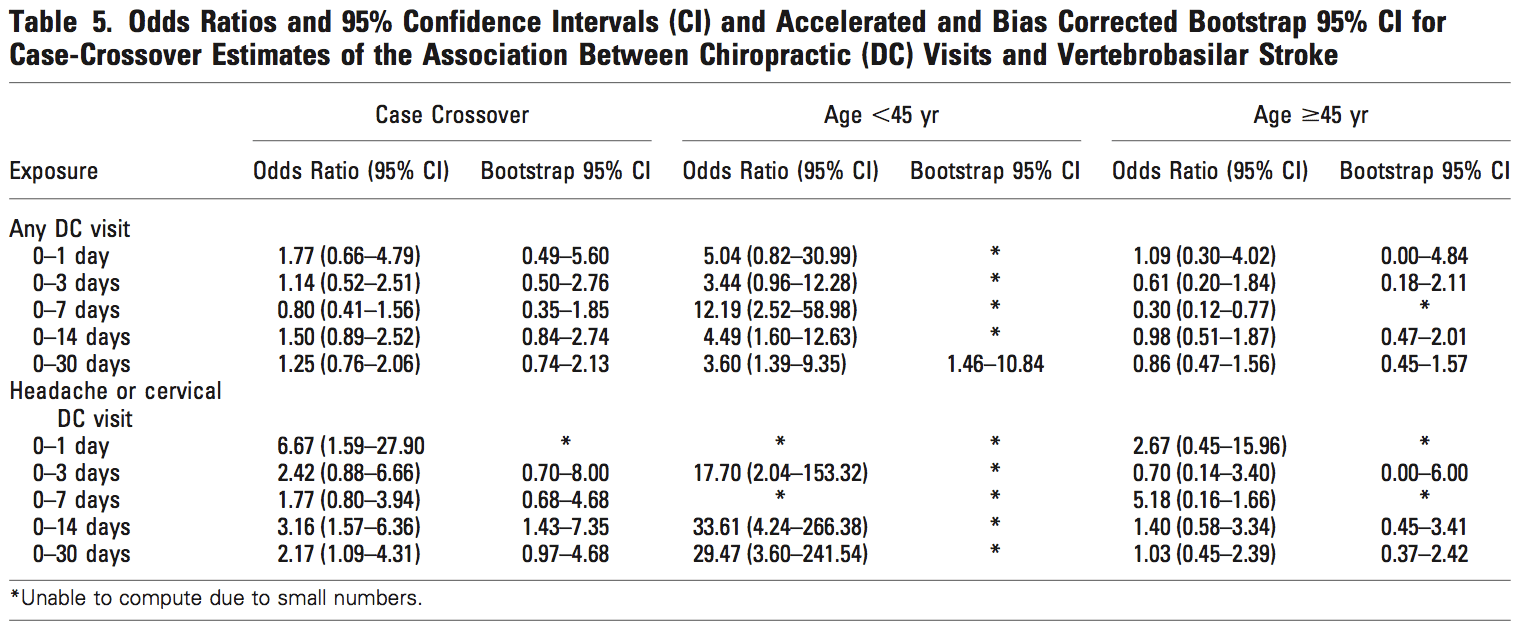
Our study was also limited to replication of the case� control design described by Cassidy, et al. [32]. For pragmatic reasons, we did not attempt to conduct a case-crossover design. While the addition of a case- crossover design would have provided better control of confounding variables, Cassidy, et al. [32] showed the results were similar for both the case control and case crossover studies.
The findings of this case�control study and previous retrospective research underscore the need to rethink how to better conduct future investigations. Researchers should seek to avoid the use of surrogate measures or use the least indirect measures available. Instead, the focus should be on capturing data about the types of services and not the type of health care provider.
In alignment with this approach, it is also important for investigators to access contextual data (e.g., from electronic health records), which can be enabled by qualitative data analysis computer programs [58]. The acquisition of the elements of clinical encounters � including history, diagnosis, intervention, and adverse events � can provide the infrastructure for more action- able research. Because of the rarity of VBA stroke, large data sets (e.g., registries) containing these elements will be necessary to achieve adequate statistical power for making confident conclusions.
Until research efforts produce more definitive results, health care policy and clinical practice judgments are best informed by the evidence about the effectiveness of manipulation, plausible treatment options (including non-thrust manual techniques) and individual patient values [20].
Conclusions
Our findings should be viewed in the context of the body of knowledge concerning the risk of VBA stroke. In contrast to several other case�control studies, we found no significant association between exposure to chiropractic care and the risk of VBA stroke. Our secondary analysis clearly showed that manipulation may or may not have been reported at every chiropractic visit. Therefore, the use of chiropractic visits as a proxy for manipulation may not be reliable. Our results add weight to the view that chiropractic care is an unlikely cause of VBA strokes. However, the current study does not exclude cervical manipulation as a possible cause or contributory factor in the occurrence of VBA stroke.
Authors’ Contributions
DE conceived of the study, and participated in its design and coordination. JT participated in the design of the study, performed the statistical analysis and helped to draft the manuscript. TMK participated in the design and coordination of the study, and wrote the initial draft and revisions of the manuscript. WMB participated in the coordination of the study and the statistical analysis, and helped to draft the manuscript. All authors contributed to the interpretation of the data. All authors read and approved the final manuscript.
Author Details
1Optum Health � Clinical Programs at United Health Group, 11000 Optum Circle, Eden Prairie MN 55344, USA. 2Optum Health � Clinical Analytics at United Health Group, 11000 Optum Circle, Eden Prairie MN 55344, USA.
Received: 14 October 2014 Accepted: 28 April 2015
Published Online: 16 June 2015
References
1. Paulose R, Hertz R. The burden of pain among adults in the United States. In Pfizer Facts. Edited by Pfizer Inc. 2008. [http://www.pfizer.com/files/products/PF_Pain.pdf] Accessed May 14, 2014.
2. Carroll L, Hogg-Johnson S, van der Velde G, Haldeman S, Holm L, Carragee E, et al. Bone and Joint Decade 2000�2010 Task Force on Neck Pain and Its Associated Disorders: Course and prognostic factors for neck pain in the
general population: results of the Bone and Joint Decade 2000�2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976).2008;33(4 Suppl):S75�82.
3. Hoy D, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24(6):783�92.
4. Jacobs J, Andersson G, Bell J, Weinstein S, Dormans J, Gnatz S, et al. Spine: low back and neck pain. In The Burden of Musculoskeletal Diseases in the United States. Chapter 2. Edited by Bone and Joint Decade USA
2002�2011. Rosemont, IL: The American Academy of Orthopaedic Surgeons; 2008:21�56.
5. Christensen M, Kollasch M, Hyland J, Rosner A. Chapter 8 � Patient Conditions. In Practice Analysis of Chiropractic: A Project Report, Survey Analysis, and Summary of the Practice of Chiropractic Within the United States. Greeley, CO: The National Board of Chiropractic Examiners. 2010:95�120.
6. Christensen M, Kollasch M, Hyland J, Rosner A. Chapter 9 � Professional functions and treatment procedures. In Practice Analysis of Chiropractic: A Project Report, Survey Analysis, and Summary of the Practice of
Chiropractic Within the United States. Greeley, CO: The National Board of Chiropractic Examiners. 2010:121�136.
7. D�Sylva J, Miller J, Gross A, Burnie S, Goldsmith G, Graham N, et al. Manual therapy with or without physical medicine modalities for neck pain: a systematic review. Man Ther. 2010;15(4):415�33.
8. Gross A, Miller J, D�Sylva J, Burnie S, Goldsmith G, Graham N, et al. Manipulation or mobilisation for neck pain: A Cochrane review. Man Ther. 2010;15(4):315�33.
9. Bryans R, Decina P, Descarreaux M, Duranleau M, Marcoux H, Potter B, et al. Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J Manipulative Physiol Ther. 2014;37(1):42�63.
10. Bryans R, Descarreaux M, Duranleau M, Marcoux H, Potter B, Ruegg R, et al. Evidence-based guidelines for the chiropractic treatment of adults withheadache. J Manipulative Physiol Ther. 2011;34(5):274�89.
11. Childs J, Cleland J, Elliott J, Teyhen D, Wainner R, Whitman J, et al. Neck pain: clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic
Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9):A1�A34.
12. Clar C, Tsertsvadze A, Court R, Hundt G, Clarke A, Sutcliffe P. Clinical effectiveness of manual therapy for the management of musculoskeletal and non-musculoskeletal conditions: systematic review and update of UK
evidence report. Chiropr Man Therap. 2014;22(1):12.
13. Vincent K, Maigne J, Fischhoff C, Lanlo O, Dagenais S. Systematic review of manual therapies for nonspecific neck pain. Joint Bone Spine. 2013;80(5):508�15.
14. Bronfort G, Assendelft W, Evans R, Haas M, Bouter L. Efficacy of spinal manipulation for chronic headache: a systematic review. J Manipulative Physiol Ther. 2001;24(7):457�66.
15. Chaibi A, Tuchin P, Russell M. Manual therapies for migraine: a systematic review. J Headache Pain. 2011;12(2):127�33.
16. Racicki S, Gerwin S, Diclaudio S, Reinmann S, Donaldson M. Conservative physical therapy management for the treatment of cervicogenic headache: a systematic review. J Man Manip Ther. 2013;21(2):113�24.
17. Cassidy J, Bronfort G, Hartvigsen J. Should we abandon cervical spine manipulation for mechanical neck pain? No BMJ. 2012;344, e3680.
18. Wand B, Heine P, O�Connell N. Should we abandon cervical spine manipulation for mechanical neck pain? Yes BMJ. 2012;344, e3679.
19. Moloo J. What’s the Best Approach for Managing Neck Pain? NEJM Journal Watch 2012. [http://www.jwatch.org/jw201202090000004/2012/02/09/whats-best-approach-managing-neck-pain] Accessed May 14, 2014.
20. Schneider M, Weinstein S, Chimes G. Cervical manipulation for neck pain. PM&R. 2012;4(8):606�12.
21. Biller J, Sacco R, Albuquerque F, Demaerschalk B, Fayad P, Long P, et al. Cervical arterial dissections and association with cervical manipulative therapy:a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, Epub ahead of print.
22. American Chiropractic Association: ACA Response to AHA Statement on Neck Manipulation. 2014 (Aug 7). [http://www.acatoday.org/press_css.cfm? CID=5534] Accessed August 15, 2014.
23. American Physical Therapy Association: APTA responds to American Heart Association cervical manipulation paper. 2014 (Aug 7). [http://www.apta.org/Media/Releases/Consumer/2014/8/7/] Accessed August 15, 2014.
24. Kardys JA. Declaratory ruling regarding informed consent. Connecticut State Board of Chiropractic Examiners � State of Connecticut Department of Public Health. 2010. [http://www.ctchiro.com/upload/news/44_0.pdf]
Accessed May 14, 2014.
25. Wangler M, Fujikawa R, Hestb�k L, Michielsen T, Raven T, Thiel H, et al. Creating European guidelines for Chiropractic Incident Reportingand Learning Systems (CIRLS): relevance and structure. Chiropr Man
Therap. 2011;19:9.
26. Berger S: How safe are the vigorous neck manipulations done by chiropractors? Washington Post 2014 (Jan. 6). [http://www.washingtonpost.com/national/health-science/how-safe-are-the-vigorous-neck-manipulationsdone-by-chiropractors/2014/01/06/26870726-5cf7-11e3-bc56-c6ca94801fac_story.html] Accessed January 10, 2014.
27. Group wants provincial ban on some neck manipulation by chiropractors. Winnipeg Free Press 2012 (Oct 4). [http://www.winnipegfreepress.com/local/Group-wants-provincial-ban-on-some-neck-manipulation-bychiropractors-172692471.htm] Accessed May 14, 2014.
28. Gouveia L, Castanho P, Ferreira J. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34(11):E405�13.
29. Carlesso L, Gross A, Santaguida P, Burnie S, Voth S, Sadi J. Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neckpain in adults: a systematic review. Man Ther. 2010;15(5):434 44.
30. Chung C, C�t� P, Stern P, L’Esp�rance G. The association between cervical spine manipulation and carotid artery dissection: a systematic review of the literature. J Manipulative Physiol Ther 2014, [Epub ahead of print].
31. Haynes M, Vincent K, Fischhoff C, Bremner A, Lanlo O, Hankey G. Assessing the risk of stroke from neck manipulation: a systematic review. Int J Clin Pract. 2012;66(10):940�7.
32. Cassidy J, Boyle E, Cote P, He Y, Hogg-Johnson S, Silver F, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case�control and case-crossover study. Spine (Phila Pa 1976).
2008;33 Suppl 4:S176�83.
33. Rothwell D, Bondy S, Williams J. Chiropractic manipulation and stroke: a population-based case�control study. Stroke. 2001;32(5):1054�60.
34. Choi S, Boyle E, C�t� P, Cassidy JD. A population-based case-series of Ontario patients who develop a vertebrobasilar artery stroke after seeing a chiropractor. J Manipulative Physiol Ther. 2011;34(1):15�22.
35. U.S. Census Bureau: State and County QuickFacts. Data derived from Population Estimates, American Community Survey, Census of Population and Housing, State and County Housing Unit Estimates, County Business
Patterns, Nonemployer Statistics, Economic Census, Survey of Business Owners, Building Permits. 2014 (rev July 8). [http://quickfacts.census.gov/qfd/states/00000.html] Accessed August 19, 2014.
36. Kosanke J, Bergstralh E. GMatch Macro (SAS program): Mayo Clinic College of Medicine. 2004. [http://www.mayo.edu/research/departments-divisions/department-health-sciences-research/division-biomedical-statisticsinformatics/software/locally-written-sas-macros]Accessed June 6, 2014.
37. Smith W, Johnston S, Skalabrin E, Weaver M, Azari P, Albers G, et al. Spinal manipulative therapy is an independent risk factor for vertebral artery dissection. Neurology. 2003;60(9):1424�8.
38. Engelter S, Grond-Ginsbach C, Metso T, Metso A, Kloss M, Debette S, et al. Cervical Artery Dissection and Ischemic Stroke Patients Study Group: Cervical artery dissection: trauma and other potential mechanical trigger
events. Neurology. 2013;80(21):1950�7.
39. Ardal S, Baigent L, Bains N, Hay C, Lee P, Loomer S: The health analyst�s toolkit. Ministry of Health and Long-Term Care Health Results Team – Information Management. Ontario (CA) 2006 (January) [http://www.health.gov.on.ca/transformation/providers/information/resources/analyst_toolkit.pdf]
Accessed January 12, 2015.
40. Sacco RL, Benjamin EJ, Broderick JP, Dyken M, Easton JD, Feinberg WM, et al. American Heart Association Prevention Conference. IV. Prevention and rehabilitation of stroke. Risk factors. Stroke. 1997;28(7):1507�17.
41. Debette S, Metso T, Pezzini A, Abboud S, Metso A, Leys D, et al. Cervical Artery Dissection and Ischemic Stroke Patients (CADISP) Group: Association of vascular risk factors with cervical artery dissection and ischemic stroke in
young adults. Circulation. 2011;123(14):1537�44.
42. Guyatt G, Oxman A, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence � imprecision. J Clin Epidemiol. 2011;64(12):1283�93.
43. Krarup L, Boysen G, Janjua H, Prescott E, Truelsen T. Validity of stroke diagnoses in a National Register of Patients. Neuroepidemiology. 2007;28(3):150�4.
44. Goldstein L. Accuracy of ICD-9-CM coding for the identification of patients with acute ischemic stroke: effect of modifier codes. Stroke. 1998;29(8):1602�4.
45. Liu L, Reeder B, Shuaib A, Mazagri R. Validity of stroke diagnosis on hospital discharge records in Saskatchewan, Canada: implications for stroke surveillance. Cerebrovasc Dis. 1999;9(4):224�30.
46. Ellekjaer H, Holmen J, Kr�ger O, Terent A. Identification of incident stroke in Norway: hospital discharge data compared with a population-based stroke register. Stroke. 1999;30(1):56�60.
47. Braksiak R, Roberts D. Amusement park injuries and deaths. An Emerg Med. 2002;39(1):65�72.
48. Dittrich R, Rohsbach D, Heidbreder A, Heuschmann P, Nassenstein I, Bachmann R, et al. Mild mechanical traumas are possible risk factors for cervical artery dissection. Cerebrovasc Dis. 2007;23(4):275�81.
49. Mas J, Bousser M, Hasboun D, Laplane D. Extracranial vertebral artery dissection: a review of 13 cases. Stroke. 1987;18(6):1037�47.
50. Slankamenac P, Jesic A, Avramov P, Zivanovic Z, Covic S, Till V. Multiple cervical artery dissection in a volleyball player. Arch Neuro. 2010;67(8):1024�5.
51. Weintraub M. Beauty parlor stroke syndrome: report of five cases. JAMA. 1993;269(16):2085�6.
52. Tzourio C, Benslamia L, Guilllon B, A�di S, Bertrand M, Berthet K, et al. Migraine and the risk of cervical artery dissection: a case control study. Neurology. 2002;59(3):435�7.
53. Guillon B, Berthet K, Benslamia L, Bertrand M, Bousser M, Tzourio C. Infection and the risk of cervical artery dissection: a case�control study. Stroke. 2003;34(7):e79�81.
54. Symons B, Leonard TR, Herzog W. Internal forces sustained by the vertebral artery during spinal manipulative therapy. J Manip Physiol Ther.2002;25(8):504�10.
55. Wuest S, Symons B, Leonard T, Herzog W. Preliminary report: biomechanics of vertebral artery segments C1-C6 during cervical spinal manipulation. J Manip Physiol Ther. 2010;33(4):273�8.
56. Herzog W, Leonard TR, Symons B, Tang C, Wuest S. Vertebral artery strains during high-speed, low amplitude cervical spinal manipulation. J Electromyogr Kinesiol. 2012;22(5):747�51.
57. Centers for Medicare & Medicaid: Comprehensive error rate testing (CERT). 2015 (Jan. 15). [http://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Medicare-FFS-Compliance-Programs/CERT/index.html?redirect=/cert] Accessed February 4, 2015.
58. Welsh E: Dealing with data: using NVivo in the qualitative data analysis process. Forum: Qualitative Social Research 2002, 3(2): Art. 26 [http://nbnresolving.de/urn:nbn:de:0114-fqs0202260] Accessed February 4, 2015.
Disclosures can be found in Additional Information at the end of the article
Background
Case reports and case control studies have suggested an association between chiropractic neck manipulation and cervical artery dissection (CAD), but a causal relationship has not been established. We evaluated the evidence related to this topic by performing a systematic review and meta-analysis of published data on chiropractic manipulation and CAD.
Methods
Search terms were entered into standard search engines in a systematic fashion. The articles were reviewed by study authors, graded independently for class of evidence, and combined in a meta-analysis. The total body of evidence was evaluated according to GRADE criteria.
Results
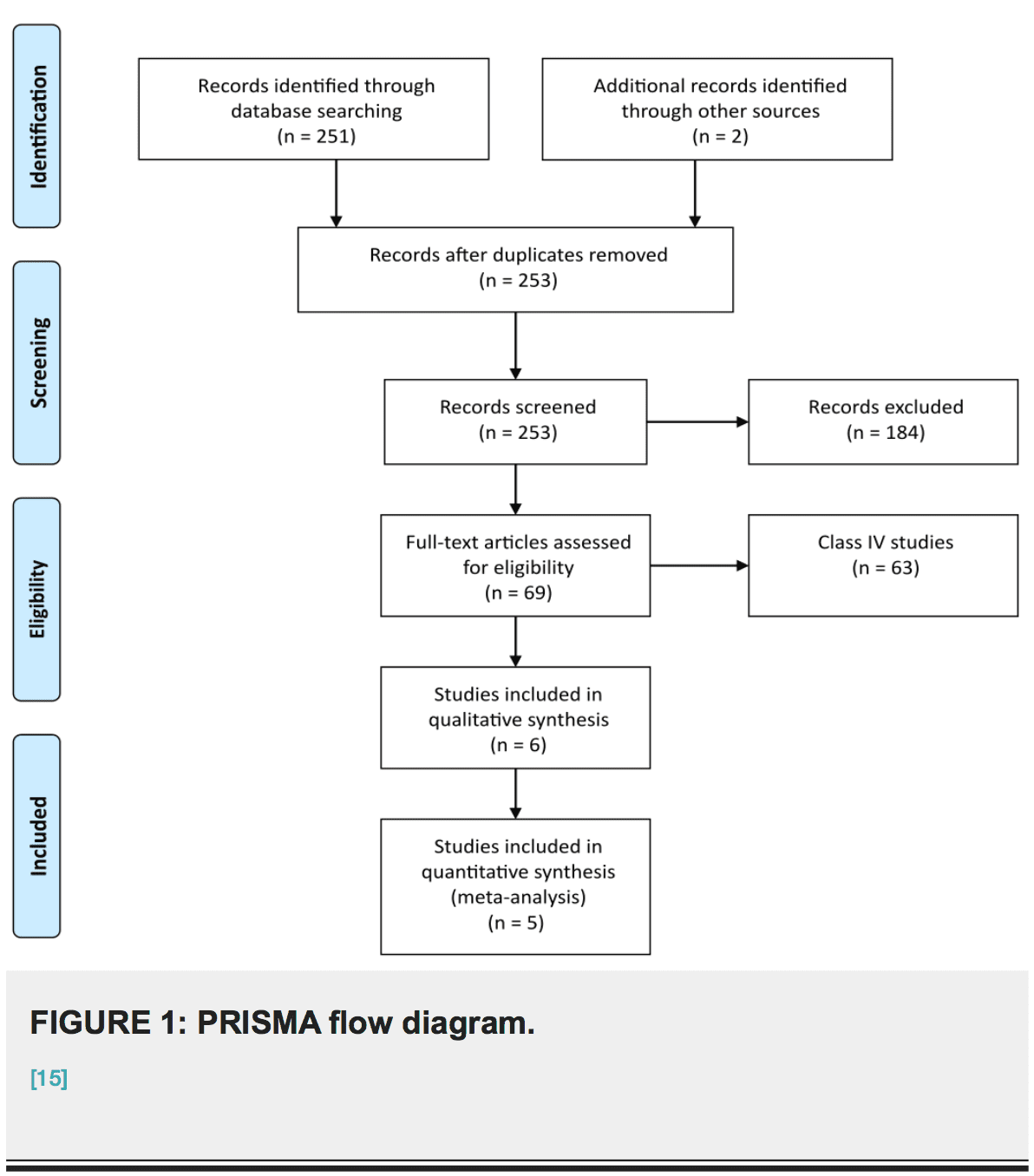
Our search yielded 253 articles. We identified two class II and four class III studies. There were no discrepancies among article ratings (i.e., kappa=1). The meta-analysis revealed a small association between chiropractic care and dissection (OR 1.74, 95% CI 1.26-2.41). The quality of the body of evidence according to GRADE criteria was “very low.”
Conclusions
The quality of the published literature on the relationship between chiropractic manipulation and CAD is very low. Our analysis shows a small association between chiropractic neck manipulation and cervical artery dissection. This relationship may be explained by the high risk of bias and confounding in the available studies, and in particular by the known association of neck pain with CAD and with chiropractic manipulation. There is no convincing evidence to support a causal link between chiropractic manipulation and CAD. Belief in a causal link may have significant negative consequences such as numerous episodes of litigation.
� Copyright 2016
Church et al. This is an open access article distributed under the terms of the Creative Commons Attribution License CC-BY 3.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
How to cite this article
Church E W, Sieg E P, Zalatimo O, et al. (February 16, 2016) Systematic Review and Meta-analysis of Chiropractic Care and Cervical Artery Dissection: No Evidence for Causation. Cureus 8(2): e498. DOI 10.7759/cureus.498
Neck pain is a common complaint in physicians� and chiropractors� offices. Data from the Centers for Disease Control and from national surveys document 10.2 million ambulatory care visits for a neck problem in 2001 and 2002. By comparison, there were 11 million office-based visits for ischemic heart disease [1]. Many patients with neck pain seek chiropractic care and undergo cervical manipulation. As many as 12% of North Americans receive chiropractic care every year, and a majority of these are treated with spinal manipulation [2].
In contrast to the frequency of neck pain and chiropractic treatments, spontaneous cervical artery dissection (CAD) is rare. The annual incidence of internal carotid artery dissection has been estimated at 2.5�3 per 100,000 patients and that of vertebral artery dissection at 1�1.5 per 100,000 [3]. Stroke occurs in a small proportion of those with CAD, and its true incidence is difficult to estimate. Overall, dissection accounts for two percent of all ischemic strokes [4].
Case reports and case series of cervical dissection following manipulation have been published. Despite their rarity, these cases are frequently publicized for several reasons. Patients are often young and otherwise in good health. Dissection accounts for 10�25% of ischemic strokes in young and middle aged patients [4]. If dissection is caused by cervical manipulation it is potentially a preventable condition. Recent reports, including case control studies, have suggested an association between chiropractic neck manipulation and cervical dissection [5- 10]. Notably, a recent study from the American Heart Association evaluated the available evidence and concluded such an association exists [11]. This report did not include a meta- analysis, nor did it seek to classify studies and grade the body of evidence. We sought to examine the strength of evidence related to this question by performing a systematic review, meta-analysis, and evaluation of the body of evidence as a whole.
Materials & Methods
Search terms �chiropract*,� �spinal manipulation,� �carotid artery dissection,� �vertebral artery dissection,� and �stroke� were included in the search. We used the Medline and Cochrane databases. We additionally reviewed references of key articles for completeness. A librarian with expertise in systematic review was consulted throughout the search process.
Two study authors independently reviewed all articles (EC, ES). They selected any applicable studies for evaluation based on pre-specified inclusion and exclusion criteria. We included only human trials examining patients with carotid or vertebrobasilar artery dissection and recent chiropractic neck manipulation. We excluded non-English language studies. The articles were independently graded using the classification of evidence scheme adopted by the American Academy of Neurology [12-14]. A third author (MG) arbitrated any discrepancies in the class- of-evidence ratings for the included studies.
Data from all class II and III studies were included in a meta-analysis. A second meta-analysis excluding class III studies was also performed. The inverse variance method and a fixed effects model were employed. Additionally, we report results using a variable effects model. The analyses were performed using RevMan 5.3 software from the Cochrane Informatics and Knowledge Management Department. We did not compose a protocol for our review, although PRISMA and MOOSE methodologies were used throughout [15-16].
We evaluated the total body of evidence for quality using the GRADE system [17-20]. A final GRADE designation was achieved by consensus after discussions involving all study authors as recommended by GRADE guidelines. This system is designed to assess the total body of evidence rather than individual studies. The criteria include study design, risk of bias, inconsistency, indirectness, imprecision, publication bias, effect size, dose response, and all plausible residual confounding. Four possible final designations are specified: high, moderate,�low, and very low quality.
Results
Results of the systematic review
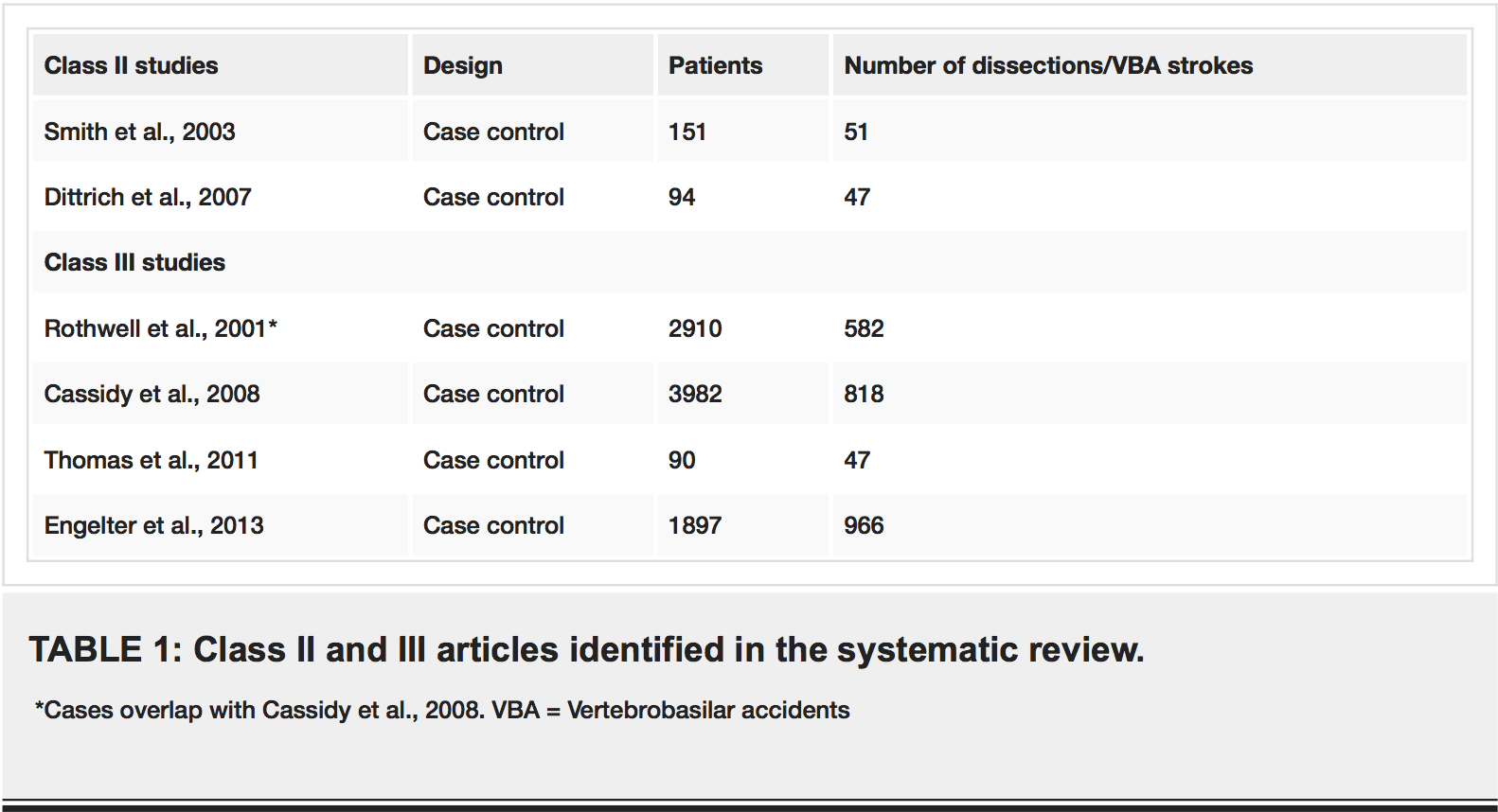
Our search strategy yielded 253 articles. Seventy-seven were judged by all reviewers to be non- relevant. Four articles were judged to be class III studies, and two were rated class II. There were no discrepancies between the independent ratings (i.e., kappa=1). Studies rated class III or higher are listed in Table 1. Figure 1 outlines our process of selecting studies for inclusion in the meta-analysis.
Meta-Analysis
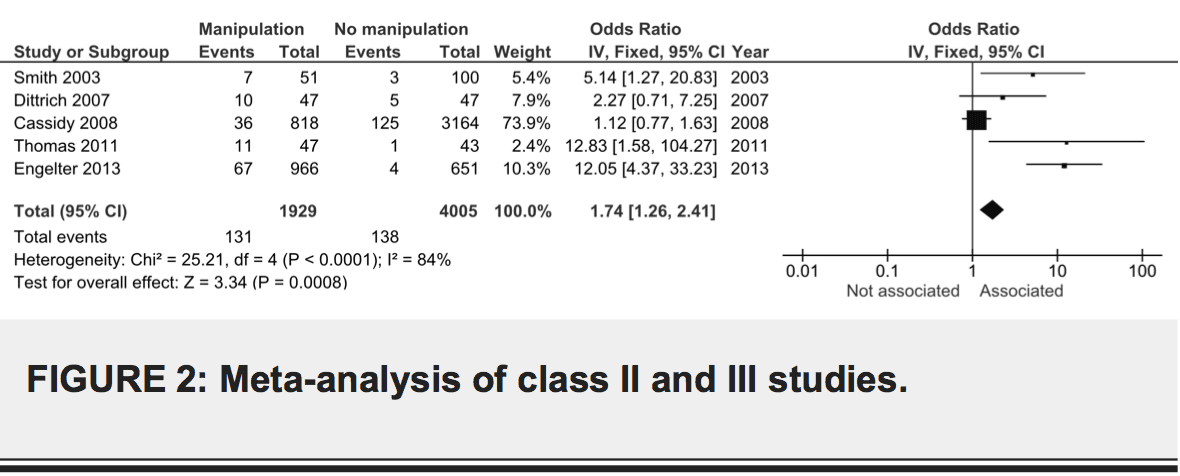
Combined data from class II and III studies suggests an association between dissection and chiropractic care, OR 1.74, 95% CI 1.26-2.41 (Figure 2). The result was similar using a random effects model, OR 4.05, 95% CI 1.27-12.91. We did not include the study by Rothwell et al. because it describes a subset of patients in the study by Cassidy et al. [5,8]. There was considerable heterogeneity among the studies (I2=84%).
We repeated the meta-analysis excluding class III studies. The combined effect size was again indicative of a small association between dissection and chiropractic care, OR 3.17, 95% CI 1.30-7.74). The result was identical when using a random effects model.
Class II Studies
Smith et al. used a retrospective case control design, combining databases from two academic stroke centers to identify cases of arterial dissection [9]. They found 51 cases and 100 controls. Exposure to spinal manipulative therapy (SMT) was assessed by mail survey. The authors reported an association between SMT and VBA (P = .032). In multivariate analysis, chiropractor care within 30 days was associated with VBA, even when adjusting for neck pain or headache (OR 6.6, 95% CI 1.4-30). While this study controlled for possible confounders such as neck pain, there were several limitations. Head and neck pain as well as chiropractor visit were assessed in a retrospective fashion by mail survey, very possibly introducing both recall and survivor bias. The reason for reporting to the chiropractor (e.g., trauma) was not assessed. Further, there was significant variability among diagnostic procedures, which may reflect increased motivation by physicians to rule out dissection in patients with a history of SMT. Such motivation could result in interviewer bias.
Dittrich et al. compared 47 patients with CAD to a control group with stroke due to etiologies other than dissection [6]. They assessed for risk factors using a face-to-face interview with blinding. These authors found no association between any individual risk factor and CAD, including cervical manipulative therapy. They blame the small sample size for the negative result, and they point out that cumulative analysis of all mechanical risk factors <24 hours prior to symptom onset showed an association (P = .01). This study is subject to recall bias.
Class III Studies
Rothwell et al. used a retrospective case control design to test for an association between chiropractic manipulation and vertebrobasilar accidents (VBA) [8]. They reviewed Ontario hospital records for admissions for VBA from 1993�1998. There were 582 cases and 2328 matching controls. The authors report an association between VBA and visit to a chiropractor within one week (OR 5.03, 95% CI 1.32-43.87), but this was only true for young patients (<45 years). This study represented the first attempt to delineate the association between chiropractic manipulation and extremely rare VBA with controls. Limitations included requisite use of ICD-9 codes to identify cases and associated classification bias, as well as potential unmeasured confounders (e.g., neck pain).
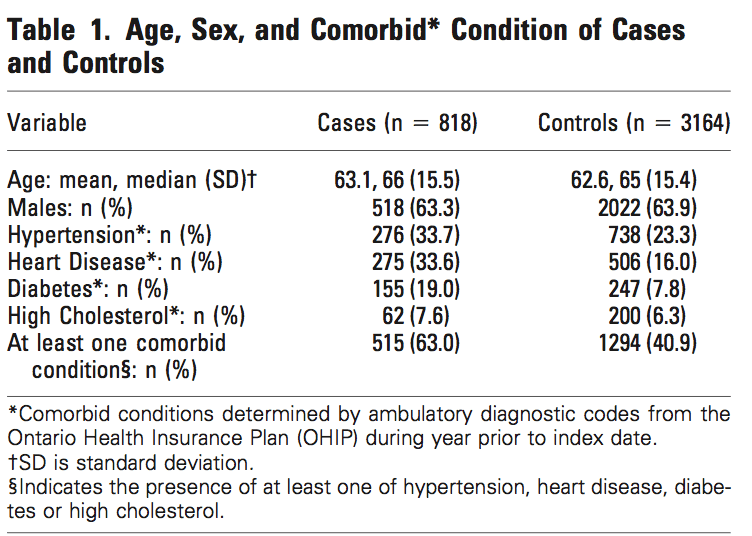
In 2008, Cassidy et al. set out to address the problem of neck pain possibly confounding the association between chiropractic care and VBA [5]. Again using a retrospective case control design, they included all residents of Ontario over a period of 9 years (1993�2002, 109,020,875 person years of observation). They identified 818 VBA strokes resulting in hospitalization and randomly selected age and sex matched controls. Next, they examined ambulatory encounters with chiropractors and primary care physicians (PCPs) in the one year preceding the stroke, limited to cervical manipulation, neck pain, and headache. Associations between chiropractor visit and VBA versus PCP visits and VBA were compared. Indeed, there were associations between both chiropractor visit and VBA (<45yrs OR 1.37, 95% CI 1.04-1.91), and PCP visit and VBA (<45 yrs OR 1.34, 95% CI .94-1.87; >45 yrs and OR 1.53, 95% CI 1.36-1.67). The association for chiropractor visit was not greater than for PCP visit. This data was interpreted as evidence that a confounder such as neck pain may account for the association between chiropractor visit and VBA. This study was subject to many of the same limitations as previous efforts. Canadian health records would not reveal whether a patient with cervical complaints underwent cervical manipulation, and the researchers could not review each chart for imaging confirming dissection. Additionally, the incidence of comorbidities (e.g., hypertension, heart disease,�diabetes) was significantly higher among cases as compared to controls, and we are concerned that these differences were non-random.
In another case control study, Thomas et al. compared the records of 47 patients with confirmed or suspected vertebral or internal carotid artery dissection with 43 controls [10]. They limited their analysis to young patients defined as <55 years. These authors report a significant association between dissection and recent head or neck trauma (OR 23.51, 95% CI 5.71-96.89) as well as neck manual therapy (OR 1.67, 95% CI 1.43-112.0). An inconsistent standard for case ascertainment (a significant number of patients lacked radiographic confirmation of dissection) and lack of blinding weaken this study.
Engelter et al. evaluated data from the Cervical Artery Dissection and Ischemic Stroke Patients (CADISP) consortium, identifying 966 patients with CAD, 651 with stroke attributable to another cause, and 280 healthy controls [7]. The CADISP study involved both prospectively and retrospectively collected data at multiple centers in several countries. They assessed for prior cervical trauma within one month using questionnaires administered during clinic visits. Cervical manipulation therapy was more common for CAD versus stroke from another cause (OR 12.1, CI 4.37-33.2). The report notes that an association between any trauma and CAD was present even when restricting the analysis to prospectively recruited patients. However, in patients to whom the questionnaire was administered after dissection, recall bias may have been at work whether or not the patient was enrolled prospectively. Indeed, the frequency of prior cervical trauma in this study was substantially higher than previous reports (40% versus 12-34%). Additional weaknesses include a highly heterogeneous standard for case definition and no clear masking procedures.
Body Of Evidence Quality (GRADE Rating)
Having performed a systematic review and rated articles according to their individual strengths and weaknesses, we graded the overall body of evidence using the system proposed by Guyatt et al. [17-20]. The GRADE approach to rating quality of evidence proposes four categories that are applied to a body of evidence: high, moderate, low, and very low. In the setting of systematic review, a particular rating reflects the extent of confidence that the estimates of effect are correct. The GRADE approach begins with study design and sequentially examines features with the potential to enhance or diminish confidence in the meta-analytic estimate of effect size.
Our final assessment of the quality of the body of evidence using these criteria was very low. The initial rating based on study design was low (observational studies). Given the controversial nature of this topic and the legal ramifications of results, there is certainly potential for bias (-1 serious). However, blinding in the Class II studies mitigated this risk to some extent. Inconsistency and imprecision did not lower our rating. Because the body of evidence is derived from measures of association, the rating was lowered for indirectness (-1 serious). Publication bias is less likely because of the impact of a negative result in this case. The funnel plot from our meta-analysis was inconclusive with regard to possible publication bias because of the small number of studies included but suggested a deficit in the publication of small negative trials. There was not a large effect size, and currently there is no evidence for a dose response gradient. Moreover, the most worrisome potential confounder (neck pain) would increase rather than reduce the hypothesized effect.
Discussion
The results of our systematic review and meta-analysis suggest a small association between chiropractic care and CAD. There are no class I studies addressing this issue, and this conclusion is based on five class II and III studies. Scrutiny of the quality of the body of data�using the GRADE criteria revealed that it fell within the �very low� category. We found no evidence for a causal link between chiropractic care and CAD. This is a significant finding because belief in a causal link is not uncommon, and such a belief may have significant adverse effects such as numerous episodes of litigation.
The studies included in our meta-analysis share several common weaknesses. Two of the five studies used health administrative databases, and since conclusions depend on accurate ICD coding, this technique for case ascertainment may introduce misclassification bias. It is not possible to account for the type of spinal manipulation that may have been used. Retrospective collection of data is also a potential weakness and may introduce recall bias when a survey or interview was used. Moreover, patients arriving at a hospital complaining of neck pain and describing a recent visit to a chiropractor may be subject to a more rigorous evaluation for CAD (interviewer bias). Another potential source of interviewer bias was lack of blinding in the class III studies. Further, we noted substantial variability among diagnostic procedures performed. All of these weaknesses affect the reliability of the available evidence and are not �corrected� by performing a meta-analysis.
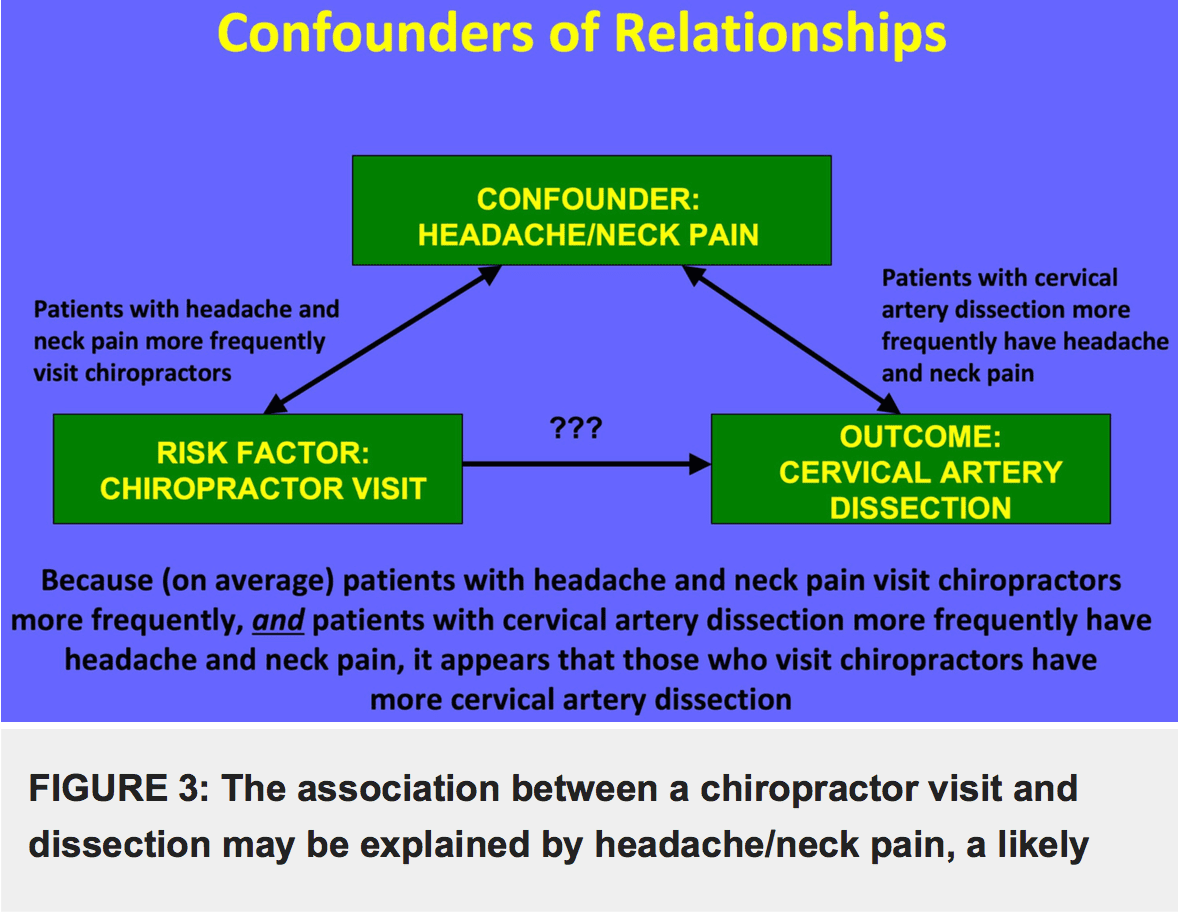
Perhaps the greatest threat to the reliability of any conclusions drawn from these data is that together they describe a correlation but not a causal relationship, and any unmeasured variable is a potential confounder. The most likely potential confounder in this case is neck pain. Patients with neck pain are more likely to have CAD (80% of patients with CAD report neck pain or headache) [21], and they are more likely to visit a chiropractor than patients without neck pain (Figure 3). Several of the studies identified in our systematic review provide suggestive evidence that neck pain is a confounder of the apparent association between chiropractic neck manipulation and CAD. For example, in Engelter et al. patients with CAD and prior cervical trauma (e.g., cervical manipulation therapy) were more likely to present with neck pain but less often with stroke than those with CAD and no prior cervical trauma (58% vs. 43% for trauma and 61% vs. 69% for stroke) [7]. If patients with CAD without neurological symptoms came to medical attention, it was probably because of pain. Patients with neck pain would also be more likely to visit a chiropractor than those without neck pain.
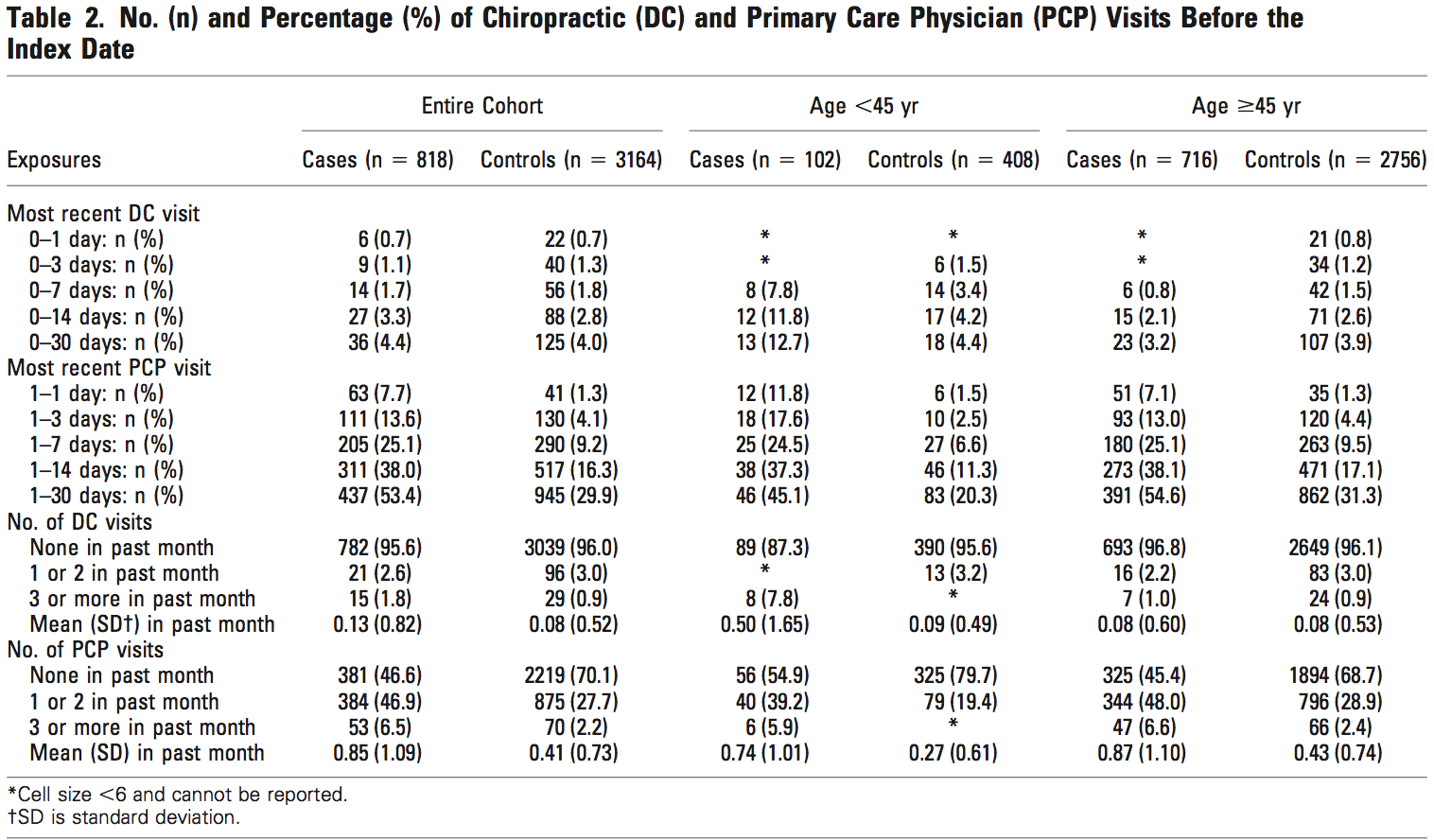
Cassidy et al. hypothesized that, although an association between chiropractor visits and vertebrobasilar artery stroke is present, it may be fully explained by neck pain and headache [5]. These authors reviewed 818 patients with vertebrobasilar artery strokes hospitalized in a population of 100 million person-years. They compared chiropractor and PCP visits in this population and reported no significant difference between these associations. For patients under 45 years of age, each chiropractor visit in the previous month increased the risk of stroke (OR 1.37, 95% CI 1.04-1.91), but each PCP visit in the previous month increased the risk in a nearly identical manner (<45 yrs OR 1.34, 95% CI .94-1.87; >45 yrs and OR 1.53, 95% CI 1.36- 1.67). The authors conclude that, since patients with vertebrobasilar stroke were as likely to visit a PCP as they were to visit a chiropractor, these visits were likely due to pain from an existing dissection.
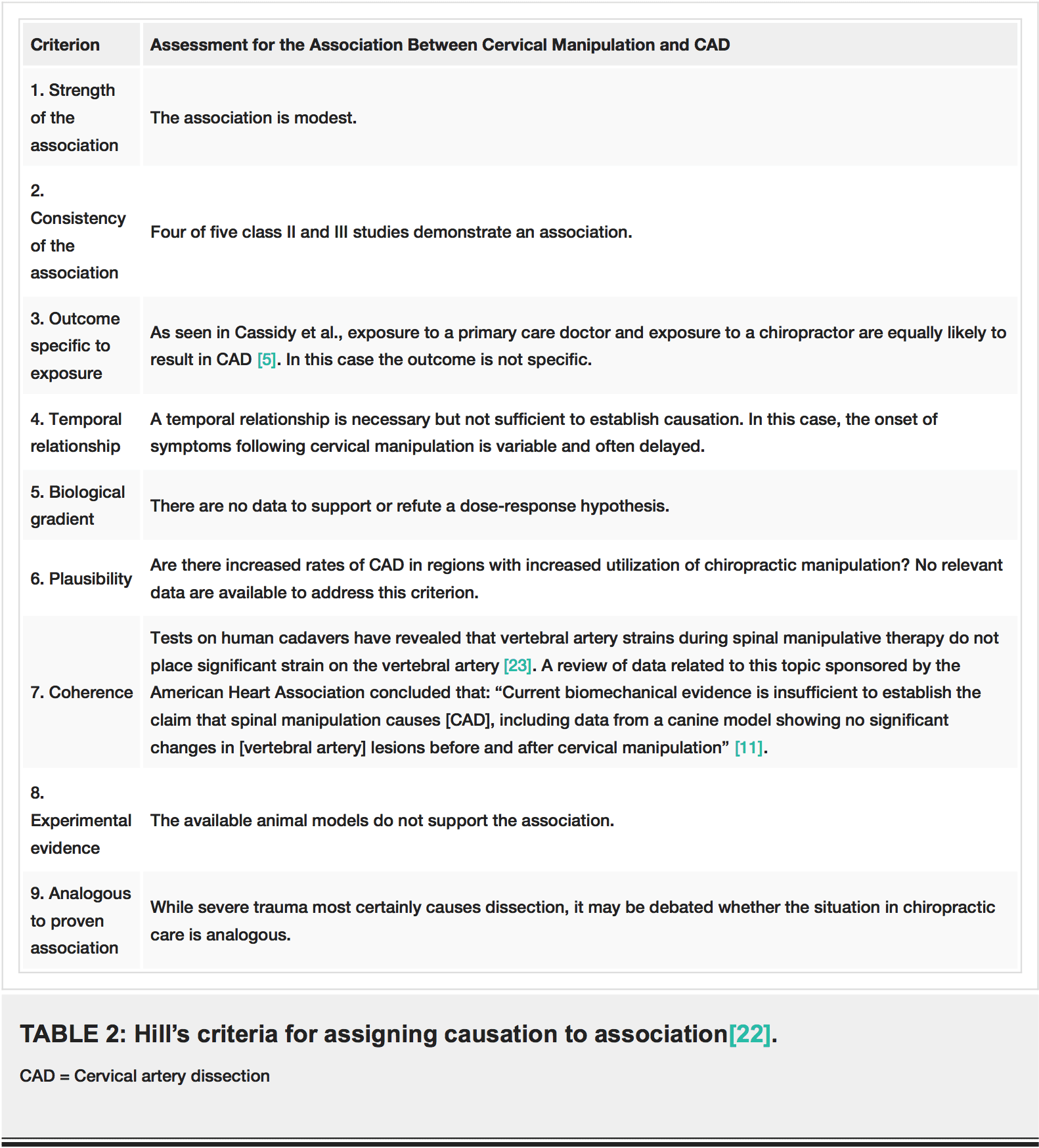
Cervical artery dissection is a rare event, creating a significant challenge for those who wish to understand it. A prospective, randomized study design is best suited to control for confounders, but given the infrequency of dissection, performing such a study would be logistically and also ethically challenging. Sir Austin Bradford Hill famously addressed the problem of assigning causation to an association with the application of nine tests [22]. These criteria include strength, consistency, specificity, temporality, biological gradient, plausibility, coherence, experimental evidence, and analogy. The specific tests and our assessment for the association between cervical manipulation and CAD are summarized in Table 2. In our appraisal, this association clearly passes only one test, it fails four, and the remaining four are equivocal due to absence of relevant data [23]. Further, a 2013 assessment of the quality of reports of cervical arterial dissection following cervical spinal manipulation similarly found lacking data to support a causal relationship [24].
In spite of the very weak data supporting an association between chiropractic neck manipulation and CAD, and even more modest data supporting a causal association, such a relationship is assumed by many clinicians. In fact, this idea seems to enjoy the status of medical dogma. Excellent peer reviewed publications frequently contain statements asserting a causal relationship between cervical manipulation and CAD [4,25,26]. We suggest that physicians should exercise caution in ascribing causation to associations in the absence of adequate and reliable data. Medical history offers many examples of relationships that were initially falsely assumed to be causal [27], and the relationship between CAD and chiropractic neck manipulation may need to be added to this list.
Conclusions
Our systematic review revealed that the quality of the published literature on the relationship between chiropractic manipulation and CAD is very low. A meta-analysis of available data shows a small association between chiropractic neck manipulation and CAD. We uncovered evidence for considerable risk of bias and confounding in the available studies. In particular, the known association of neck pain both with cervical artery dissection and with chiropractic manipulation may explain the relationship between manipulation and CAD. There is no convincing evidence to support a causal link, and unfounded belief in causation may have dire consequences.
Additional Information
Disclosures
Conflicts of interest: The authors have declared that no conflicts of interest exist.
Acknowledgements
The authors wish to thank Elaine Dean, MLS, of the Penn State Hershey Medical Center George T. Harrell Health Sciences Library, for her assistance with the systematic review.
References
1. Riddle DL, Schappert SM: Volume and characteristics of inpatient and ambulatory medical care for neck pain in the United States: data from three national surveys. Spine. 2007, 32:132�140.
2. Hurwitz EL, Chiang LM: A comparative analysis of chiropractic and general practitioner patients in North America: findings from the joint Canada/United States survey of health, 2002-03. BMC Health Serv Res. 2006, 6:49. 10.1186/1472-6963-6-49
3. Micheli S, Paciaroni M, Corea F, et al.: Cervical artery dissection: emerging risk factors . Open Neurol J. 2010, 4:50�55. 10.2174/1874205X01004010050
4. Schievink WI: Spontaneous dissection of the carotid and vertebral arteries . N Engl J Med. 2001, 344:898�906. 10.1056/NEJM200103223441206
5. Cassidy JD, Boyle E, C�t� PDC, et al.: Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine. 2008, 33:176�183.10.1097/BRS.0b013e3181644600
6. Dittrich R, Rohsbach D, Heidbreder A, et al.: Mild mechanical traumas are possible risk factors for cervical artery dissection. Cerebrovasc Dis. 2007, 23:275�281. 10.1159/000098327
7. Engelter ST, Grond-Ginsbach C, Metso TM, et al.: Cervical artery dissection: trauma and other potential mechanical trigger events. Neurology. 2013, 80:1950�1957.10.1212/WNL.0b013e318293e2eb
8. Rothwell DM, Bondy SJ, Williams JI: Chiropractic manipulation and stroke: a population based case-control study. Stroke. 2001, 32:1054-1060.
9. Smith WS, Johnston SC, Skalabrin EJ, et al.: Spinal manipulative therapy is an independent risk factor for vertebral artery dissection. Neurology. 2003, 60:1424-1428.10. Thomas LC, Rivett DA, Attia JR, et al.: Risk factors and clinical features of craniocervical arterial dissection. Man Ther. 2011, 16:351�356. 10.1016/j.math.2010.12.008
11. Biller J, Sacco RL, Albuquerque FC, et al.: Cervical arterial dissections and association with cervical manipulative therapy: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014, 45:3155�3174.10.1161/STR.0000000000000016
12. AAN (American Academy of Neurology): Clinical Practice Guideline Process Manual. Gronseth GS, Woodroffe LM, Getchius TSD (ed): AAN (American Academy of Neurology), St Paul, MN; 2011.
13. French J, Gronseth G: Lost in a jungle of evidence: we need a compass . Neurology. 2008, 71:1634�1638. 10.1212/01.wnl.0000336533.19610.1b 2016 Church et al. Cureus 8(2): e498. DOI 10.7759/cureus.498 10 of 11
14. Gross RA, Johnston KC: Levels of evidence: taking Neurology� to the next level . Neurology. 2009, 72:8�10. 10.1212/01.wnl.0000342200.58823.6a
15. Moher D, Liberati A, Tetzlaff J, et al.: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009, 6:e1000097. Accessed: January 23, 2016: http://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000097. 10.1371/journal.pmed.1000097
16. Stroup DF, Berlin JA, Morton SC, et al.: Meta-analysis of observational studies inepidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000, 283:2008-2012.
17. Guyatt G, Oxman AD, Akl EA, et al.: GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011, 64:383�394. 10.1016/j.jclinepi.2010.04.026
18. Guyatt GH, Oxman AD, Kunz R, et al.: GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol. 2011, 64:395�400. 10.1016/j.jclinepi.2010.09.012
19. Balshem H, Helfand M, Sch�nemann HJ, et al.: GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011, 64:401�406. 10.1016/j.jclinepi.2010.07.015
20. The Cochrane Collaboration: Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0). Higgins JPT, Green S (ed): The Cochrane Collaboration, 2011.
21. Lee VH, Brown RD Jr, Mandrekar JN, et al.: Incidence and outcome of cervical artery dissection: a population-based study. Neurology. 2006, 67:1809-1812.
22. Hill AB: The environment and disease: association or causation?. Proc R Soc Med. 1965, 58:295�300.
23. Herzog W, Leonard TR, Symons B, et al.: Vertebral artery strains during high-speed, low amplitude cervical spinal manipulation. J Electromyogr Kinesiol. 2012, 22:740�746. 10.1016/j.jelekin.2012.03.005
24. Wynd S, Estaway M, Vohra S, Kawchuk G: The quality of reports on cervical arterial dissection following cervical spinal manipulation. PLOS ONE. 2013, 8:e59170. Accessed: February 8, 2016: http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0059170. 10.1371/journal.pone.0059170
25. Albuquerque FC, Hu YC, Dashti SR, et al.: Craniocervical arterial dissections as sequelae of chiropractic manipulation: patterns of injury and management. J Neurosurg. 2011, 115:1197�1205. 10.3171/2011.8.JNS111212
26. Debette S, Leys D: Cervical-artery dissections: predisposing factors, diagnosis, and outcome . Lancet Neurol. 2009, 8:668�678. 10.1016/S1474-4422(09)70084-5
27. Artenstein AW: The discovery of viruses: advancing science and medicine by challenging dogma. Int J Infect Dis. 2012, 16:e470�e473. 10.1016/j.ijid.2012.03.005
Ephraim W. Church 1 , Emily P. Sieg 1 , Omar Zalatimo 1 , Namath S. Hussain 1 , Michael Glantz 1 , Robert E. Harbaugh 1
1. Department of Neurosurgery, Penn State Hershey Medical Center
Corresponding author: Ephraim W. Church, [email protected]
Results Of A Population-Based Case-Control & Case-Crossover Study
J. David Cassidy, DC, PhD, DrMedSc,*�� Eleanor Boyle, PhD,* Pierre Co�te ?, DC, PhD,*��� Yaohua He, MD, PhD,* Sheilah Hogg-Johnson, PhD,�� Frank L. Silver, MD, FRCPC, and Susan J. Bondy, PhD�
SPINE Volume 33, Number 4S, pp S176 �S183 �2008, Lippincott Williams & Wilkins
Neck pain is a common problem associated with consid- erable comorbidity, disability, and cost to society.1�5 In North America, the clinical management of back pain is provided mainly by medical physicians, physi- cal therapists and chiropractors.6 Approximately 12% of American and Canadian adults seek chiropractic care annually and 80% of these visits result in spinal manipulation.7,8 When compared to those seeking medical care for back pain, Canadian chiropractic pa- tients tend to be younger and have higher socioeco- nomic status and fewer health problems.6,8 In On- tario, the average number of chiropractic visits per episode of care was 10 (median 6) in 1985 through 1991.7 Several systematic reviews and our best- evidence synthesis suggest that manual therapy can benefit neck pain, but the trials are too small to eval- uate the risk of rare complications.9 �13
Two deaths in Canada from vertebral artery dissection and stroke following chiropractic care in the 1990s attracted much media attention and a call by some neurologists to avoid neck manipulation for acute neck pain.14 There have been many published case reports linking neck manipulation to vertebral artery dissection15�and stroke.�The prevailing theory is that extension�and/or rotation of the neck can damage the vertebral artery, particularly within the foramen transversarium at the C1�C2 level. Activities leading to sudden or sustained rotation and extension of the neck have been implicated, included motor vehicle collision, shoulder checking while driving, sports, lifting, working over- head, falls, sneezing, and coughing.16 However, most cases of extracranial vertebral arterial dissection are thought to occur spontaneously, and other factors such as connective tissue disorders, migraine, hyper- tension, infection, levels of plasma homocysteine, vessel abnormalities, atherosclerosis, central venous�catherization, cervical spine surgery, cervical percutaneous nerve blocks, radiation therapy and diagnostic cerebral angiography have been identified as possible risk factors.17�21
The true incidence of vertebrobasilar dissection is un- known, since many cases are probably asymptomatic, or the dissection produces mild symptoms.22 Confirming the diagnosis requires a high index of suspicion and good vascular imaging. The cases that are most likely to be diagnosed are those that result in stroke.19,22 Ischemic stroke occurs when a thrombus develops intraluminally and embolizes to more distal arteries, or less commonly, when the dissection extends distally into the intracranial vertebral artery, obliterating branching vessels.22 The best incidence estimate comes from Olmstead county, where vertebral artery dissection causing stroke affected 0.97 residents per 100,000 population between 1987 and 2003.23
To date there have been two case-control studies of stroke following neck manipulation. Rothwell et al used Ontario health data to compare 582 cases of VBA stroke to 2328 age and sex-matched controls.24 For those aged 45 years, cases were five times more likely than con- trols to have visited a chiropractor within 1 week of VBA stroke. Smith et al studied 51 patients with cervical ar- tery dissection and ischemic stroke or transient ischemic attack (TIA) and compared them to 100 control patients suffering from other strokes not caused by dissections.25 Cases and controls came from two academic stroke cen- ters in the United States and were matched on age and sex. They found no significant association between neck manipulation and ischemic stroke or TIA. However, a subgroup analysis showed that the 25 cases with verte- bral artery dissection were six times more likely to have consulted a chiropractor within 30 days before their stroke than the controls.
Finally, because patients with vertebrobasilar artery dissection commonly present with headache and neck pain,23 it is possible that patients seek chiropractic care for these symptoms and that the subsequent VBA stroke occurs spontaneously, implying that the associ- ation between chiropractic care and VBA stroke is not causal.23,26 Since patients also seek medical care for headache and neck pain, any association between pri- mary care physician (PCP) visits and VBA stroke could be attributed to seeking care for the symptoms of verte- bral artery dissection.
The purpose of this study is to investigate the association between chiropractic care and VBA stroke and compare it to the association between recent PCP care and VBA stroke using two epidemiological designs. Evidence that chiropractic care increases the risk of VBA stroke would be present if the measured association between chiropractic visits and VBA stroke exceeds the association between PCP visits and VBA strokes.
Study Design
We undertook population-based case-control and case- crossover studies. Both designs use the same cases. In the case- control design, we sampled independent control subjects from the same source population as the cases. In the case-crossover design, cases served as their own controls, by sampling control periods before the study exposures.27 This design is most appropriate when a brief exposure (e.g., chiropractic care) causes a transient change in risk (i.e., hazard period) of a rare-onset disease (e.g., VBA stroke). It is well suited to our research questions, since within person comparisons control for unmeasured risk factors by design, rather than by statistical modeling.28 �30 Thus the advantage over the case control design is better control of confounding.
Source Population
The source population included all residents of Ontario (109,020,875 person-years of observation over 9 years) covered by the publicly funded Ontario Health Insurance Plan (OHIP). Available utilization data included hospitalizations with diagnostic coding, and practitioner (physician and chiropractic) utilization as documented by fee-for-service billings accompanied by diagnostic coding. We used two data sources: (1) the Discharge Abstract Database (DAD) from the Canadian Institute for Health Information, which captures hospital separations and ICD codes, and (2) the OHIP Databases for services provided by physicians and chiropractors. These data- bases can be linked from April 1992 onward.
Cases
We included all incident vertebrobasilar occlusion and stenosis strokes (ICD-9433.0 and 433.2) resulting in an acute care hospital admission from April 1, 1993 to March 31, 2002. Codes were chosen in consultation with stroke experts and an epidemiologist who participated in a similar past study (SB).24 Cases that had an acute care hospital admission for any type of stroke (ICD-9433.0, 433.2, 434, 436, 433.1, 433.3, 433.8, 433.9, 430, 431, 432, and 437.1), transient cerebral ischemia (ICD- 9435) or late effects of cerebrovascular diseases (ICD-9438) before their VBA stroke admission or since April 1, 1991 were excluded. Cases residing in long-term care facilities were also excluded. The index date was defined as the hospital admission date for the VBA stroke.
Controls
For the case-control study, four age and sex-matched controls were randomly selected from the Registered Persons Database, which contains a listing of all health card numbers for Ontario. Controls were excluded if they previously had a stroke or were residing in a long-term care facility.
For the case crossover study, four control periods were randomly chosen from the year before the VBA stroke date, using a time-stratified approach.31 The year was divided into disjoint strata with 2 week periods between the strata. For the 1 month hazard period, the disjoint strata were separated by 1 month periods and the five remaining control periods were used in the analyses. We randomly sampled disjoint strata because chiropractic care is often delivered in episodes, and this strategy eliminates overlap bias and bias associated with time trends in the exposure.32
Exposures
All reimbursed ambulatory encounters with chiropractors and PCPs were extracted for the one-year period before the index date from the OHIP database. Neck-related chiropractic visits were identified using diagnostic codes: C01�C06, cervical and cervicothoracic subluxation; C13�C15, multiple site subluxation; C30, cervical sprain/strain; C40, cervical neuritis/ neuralgia; C44, arm neuritis/neuralgia; C50, brachial radiculitis; C51, cervical radiculitis; and C60, headache. For PCP visits, we included community medicine physicians if they submitted ambulatory fee codes to OHIP. Fee codes for group therapy and signing forms were excluded. Headache or neck pain- related PCP visits were identified using the diagnostic codes: ICD-9307, tension headaches; 346, migraine headaches; 722, intervertebral disc disorders; 780, headache, except tension headache and migraine; 729, fibrositis, myositis and muscular rheumatism; and 847, whiplash, sprain/strain and other traumas associated with neck (These codes include other diagnoses, and we list only those relevant to neck pain or headache). There is no limit on the number of reimbursed PCP visits per year. However, there are limits chiropractors, but less than 15% of patients surpass them.24
Statistical Analysis
Conditional logistic regression was used to estimate the asso- ciation between VBA stroke after chiropractor and PCP visits. Separate models were built using different a priori specified hazard periods, stratified by age ( 45 years and 45 years) and by visits with or without head and neck pain related diag- nostic codes. For the chiropractic analysis, the index date was included in the hazard period, since chiropractic treatment might cause immediate stroke and patients would not normally consult a chiropractor after having a stroke. However, the in- dex day was excluded from the PCP analysis, since patients might consult these physicians after experiencing a stroke. We tested different hazard periods, including 1 day, 3 days, 1 week, 2 weeks, and 1 month before the index date. Exposure occurred if any chiropractic or PCP visits were recorded during the des- ignated hazard periods.
We also measured the effect of cumulative numbers of chiropractic and PCP visits in the month before the index date by computing the odds ratio for each incremental visit. These estimates were similarly stratified by age and by diagnostic codes related to headache and/or neck pain. Finally, we conducted analyses to determine if our results were sensitive to chiropractic and PCP visits related to neck complaints and headaches. We report our results as odds ratios (OR) and 95% confidence intervals. Confidence intervals were estimated by accelerated bias corrected bootstraps with 2000 replications using the variance co-variance method.33 All statistical analyses were per- formed using STATA/SE version 9.2.34
Results
A total of 818 VBA strokes met our inclusion/exclusion criteria over the 9 year inception period. Of the 3272 matched control subjects, 31 were excluded because of prior stroke, one had died before the index date and 76 were receiving long-term care. Thus, 3164 control subjects were matched to the cases. The mean age of cases and controls was 63 years at the index date and 63% were male. Cases had a higher proportion of comorbid conditions (Table 1). Of the 818 stroke cases, 337�(41.2%) were coded as basilar occlusion and stenosis, 443 (54.2%) as vertebral occlusion and stenosis and 38 (4.7%) had both codes.
Overall, 4% of cases and controls had visited a chiropractor within 30 days of the index date, while 53% of cases and 30% of controls had visited a PCP within that time (Table 2). For those under 45 years of age, 8 cases (7.8%) had consulted a chiropractor within 7 days of the index date, compared to 14 (3.4%) of controls. For PCPs, 25 cases (24.5%) under 45 years of age had a consultation within 7 days of the index date, com- pared to 27 (6.6%) of controls. With respect to the number of visits within 1 month of the index date, 7.8% of cases under the age of 45 years had three or more chiropractic visits, whereas 5.9% had three or more PCP visits (Table 2).
The case control and case crossover analyses gave similar results. (Tables 3�7) Age modified the effect of chiropractic visits on the risk of VBA stroke. For those under 45 years of age, there was an increased association between chiropractic visits and VBA stroke regardless of the hazard period. For those 45 years of age and older, there was no association. Each chiropractic visit in the month before the index date was associated with an in- creased risk of VBA stroke in those under 45 years of age (OR 1.37; 95% CI 1.04�1.91 from the case crossover analysis) (Table 7). We were not able to estimate boot- strap confidence intervals in some cases because of sparse data.
Similarly, we found that visiting a PCP in the month before the index date was associated with an increased risk of VBA stroke regardless of the hazard period, or the age of the subject. Each PCP visit in the month before the stroke was associated with an increased risk of VBA stroke both in those under 45 years of age (OR 1.34; 95% CI 0.94 �1.87 from the case crossover analysis) and 45 years and older (OR 1.52; 95% CI 1.36�1.67 from the case crossover analysis) (Table 7).
Our results were sensitive to chiropractic and PCP visits related to neck complaints and headaches, and we observed sharp increases in the associations when restricting the analyses to these visits (Tables 3�7). Overall,�these associations were more pronounced in the PCP analyses. However, the data are sparse, and we were unable to compute bootstrap confidence intervals in many cases.
Discussion
Our study advances knowledge about the association between chiropractic care and VBA stroke in two respects. First, our case control results agree with past case control studies that found an association between chiropractic care and vertebral artery dissection and VBA stroke.24,25 Second, our case crossover results confirm these findings using a stronger research design with better control of confounding variables. The case-crossover design controls for time independent confounding factors, both known and unknown, which could affect the risk of VBA stroke. This is important since smoking, obesity, undiagnosed hypertension, some connective tis- sue disorders and other important risk factors for dissection and VBA stroke are unlikely to be recorded in ad- ministrative databases.
We also found strong associations between PCP visits and subsequent VBA stroke. A plausible explanation for this is that patients with head and neck pain due to vertebral artery dissection seek care for these symptoms, which precede more than 80% of VBA strokes.23 Since it�is unlikely that PCPs cause stroke while caring for these patients, we can assume that the observed association between recent PCP care and VBA stroke represents the background risk associated with patients seeking care for dissection-related symptoms leading to VBA stroke. Be- cause the association between chiropractic visits and VBA stroke is not greater than the association between PCP visits and VBA stroke, there is no excess risk of VBA stroke from chiropractic care.
Our study has several strengths and limitations. The study base includes an entire population over a 9-year period representing 109,020,875 person-years of observation. Despite this, we found only 818 VBA strokes, which limited our ability to compute some estimates and bootstrap confidence intervals. In particular, our age stratified analyses are based on small numbers of ex- posed cases and controls (Table 2). Further stratification by diagnostic codes for headache and neck pain related visits imposed even greater difficulty with these estimates. However, there are few databases that can link�incident VBA strokes with chiropractic and PCP visits in a large enough population to undertake a study of such a rare event.
A major limitation of using health administrative data are misclassification bias, and the possibility of bias in assignment of VBA-related diagnoses, which has previously been raised in this context.24 Liu et al have shown that ICD-9 hospital discharge codes for stroke have a poor positive predictive value when compared to chart review.35 Furthermore, not all VBA strokes are secondary to vertebral artery dissection and administrative databases do not provide the clinical detail to determine the specific cause. To investigate this bias, we did a sensitivity analysis using different positive predictive values for stroke diagnosis (ranging from 0.2 to 0.8). Assuming non differential misclassification of chiropractic and PCP cases, our analysis showed attenuation of the estimates towards the null with lower positive predictive values, but the conclusions did not change (i.e., associations remained positive and significant�data not shown). The�reliability and validity of the codes to classify headache and cervical visits to chiropractors and PCPs is not known.
It is also possible that patients presenting to hospital with neurologic symptoms who have recently seen a chiropractor might be subjected to a more vigorous diagnostic workup focused on VBA stroke (i.e., differential misclassification).36 In this case, the predictive values of the stroke codes would be greater for cases that had seen a chiropractor and our results would underestimate the association between PCP care and VBA stroke.
A major strength of our study is that exposures were measured independently of case definition and handled identically across cases and controls. However, there was some overlap between chiropractic care and PCP care. In the month before their stroke, only 16 (2.0%) of our cases had seen only a chiropractor, while 20 (2.4%) had seen both a chiropractor and PCP, and 417 (51.0%) had�just seen only a PCP. We were not able to run a subgroup analysis on the small number of cases that just saw a chiropractor. However, subgroup analysis on the PCP cases (n 782) that did not visit a chiropractors during the 1 month before their stroke did not change the conclusions (data not shown).
Our results should be interpreted cautiously and placed into clinical perspective. We have not ruled out neck manipulation as a potential cause of some VBA strokes. On the other hand, it is unlikely to be a major cause of these rare events. Our results suggest that the association between chiropractic care and VBA stroke found in previous studies is likely explained by present- ing symptoms attributable to vertebral artery dissection. It might also be possible that chiropractic manipulation, or even simple range of motion examination by any practitioner, could result in a thromboembolic event in a patient with a pre-existing vertebral dissection. Unfortunately, there is no acceptable screening procedure to identify patients with neck pain at risk of VBA stroke.37 These events are so rare and difficult to diagnose that future studies would need to be multi-centered and have unbiased ascertainment of all potential exposures. Given our current state of knowledge, the decision of how to treat patients with neck pain and/or headache should be driven by effectiveness and patient preference.38
Conclusion
Our population-based case-control and case-crossover study shows an association between chiropractic visits and VBA strokes. However, we found a similar association between primary care physician visits and VBA stroke. This suggests that patients with undiagnosed vertebral artery dissection are seeking clinical care for head- ache and neck pain before having a VBA stroke.
Acknowledgments
The authors acknowledge the members of the Decade of the Bone and Joint 2000 �2010 Task Force on Neck Pain and its Associate Disorders for advice about de- signing this study. In particular, they acknowledge the help of Drs. Hal Morgenstern, Eric Hurwitz, Scott Haldeman, Linda Carroll, Gabrielle van der Velde, Lena Holm, Paul Peloso, Margareta Nordin, Jaime Guzman, Eugene Carragee, Rachid Salmi, Alexander Grier, and Mr. Jon Schubert.
References
1. Borghouts JA, Koes BW, Vondeling H, et al. Cost-of-illness of neck pain in The Netherlands in 1996. Pain 1999;80:629�36.
2. Co�te� P, Cassidy JD, Carroll L. The Saskatchewan Health and Back PainSurvey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine 1998;23:1689�98.
3. Co�te� P, Cassidy JD, Carroll L. The factors associated with neck pain and its related disability in the Saskatchewan population. Spine 2000;25:1109�17.
4. Co�te� P, Cassidy JD, Carroll L. Is a lifetime history of neck injury in a trafficcollision associated with prevalent neck pain, headache and depressive symptomatology? Accid Anal Prev 2000;32:151�9.
5. Co�te� P, Cassidy JD, Carroll LJ, et al. The annual incidence and course of neck pain in the general population: a population-based cohort study. Pain 2004; 112:267�73.
6. Co�te� P, Cassidy JD, Carroll L. The treatment of neck and low back pain: who seeks care? who goes where? Med Care 2001;39:956�67.
7. Hurwitz EL, Coulter ID, Adams AH, et al. Use of chiropractic services from 1985 through 1991 in the United States and Canada. Am J Public Health1998;88:771�6.
8. Hurwitz EL, Chiang LM. A comparative analysis of chiropractic and general practitioner patients in North America: findings from the jointCanada/United States Survey of Health, 2002�03. BMC Health Serv Res 2006;6:49.
9. Aker PD, Gross AR, Goldsmith CH, et al. Conservative management of mechanical neck pain: systematic overview and meta-analysis. BMJ 1996; 313:1291�6.
10. Gross AR, Kay T, Hondras M, et al. Manual therapy for mechanical neckdisorders: a systematic review. Man Ther 2002;7:131�49.
11. Hurwitz EL, Aker PD, Adams AH, et al. Manipulation and mobilization of the cervical spine. A systematic review of the literature. Spine 1996;21:1746�59.
12. McClune T, Burton AK, Waddell G. Whiplash associated disorders: a review of the literature to guide patient information and advice. Emerg Med J 2002;19:499�506.
13. Peeters GG, Verhagen AP, de Bie RA, et al. The efficacy of conservative treatment in patients with whiplash injury: a systematic review of clinical trials. Spine 2001;26:E64�E73.
14. Norris JW, Beletsky V, Nadareishvili ZG. Sudden neck movement and cervical artery dissection. The Canadian Stroke Consortium. CMAJ 2000;163:38�40.
15. Ernst E. Manipulation of the cervical spine: a systematic review of case reports of serious adverse events, 1995�2001. Med J Aust 2002;176:376�80.
16. Haldeman S, Kohlbeck FJ, McGregor M. Risk factors and precipitating neckmovements causing vertebrobasilar artery dissection after cervical trauma and spinal manipulation. Spine 1999;24:785�94.
17. Rubinstein SM, Peerdeman SM, van Tulder MW, et al. A systematic reviewof the risk factors for cervical artery dissection. Stroke 2005;36:1575�80.
18. Inamasu J, Guiot BH. Iatrogenic vertebral artery injury. Acta Neurol Scand 2005;112:349�57.
19. Schievink WI. Spontaneous dissection of the carotid and vertebral arteries. N Engl J Med 2001;344:898�906.
20. D�Anglejan-Chatillon J, Ribeiro V, Mas JL, et al. Migraine�a risk factor for dissection of cervical arteries. Headache 1989;29:560�1.
21. Pezzini A, Caso V, Zanferrari C, et al. Arterial hypertension as risk factor for spontaneous cervical artery dissection. A case-control study. J Neurol Neurosurg Psychiatry 2006;77:95�7.
22. Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl J Med 2005;352: 2618�26.
23. Lee VH, Brown RD Jr, Mandrekar JN, et al. Incidence and outcome of cervical artery dissection: a population-based study. Neurology 2006;67: 1809�12.
24. Rothwell DM, Bondy SJ, Williams JI. Chiropractic manipulation and stroke: a population-based case-control study. Stroke 2001;32:1054�60.
25. Smith WS, Johnston SC, Skalabrin EJ, et al. Spinal manipulative therapy is an independent risk factor for vertebral artery dissection. Neurology 2003;60: 1424�8.
26. Arnold M, Bousser MG, Fahrni G, et al. Vertebral artery dissection: presenting findings and predictors of outcome. Stroke 2006;37:2499�503.
27. Maclure M. The case-crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol 1991;133:144�53.
28. Kelman CW, Kortt MA, Becker NG, et al. Deep vein thrombosis and air travel: record linkage study. BMJ 2003;327:1072.
29. Mittleman MA, Maclure M, Tofler GH, et al. Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators.
N Engl J Med 1993;329:1677�83.
30. Redelmeier DA, Tibshirani RJ. Association between cellular-telephone calls and motor vehicle collisions. N Engl J Med 1997;336:453�8.
31. Janes H, Sheppard L, Lumley T. Overlap bias in the case-crossover design, with application to air pollution exposures. Stat Med 2005;24:285�300.
32. Janes H, Sheppard L, Lumley T. Case-crossover analyses of air pollution exposure data: referent selection strategies and their implications for bias. Epidemiology 2005;16:717�26.
33. Efron B, Tibshirani RJ. An Introduction to the Bootstrap. New York: Chapmanand Hall/CRC, 1993.
34. STATA/SE [computer program]. College Station, Tex: Stata Corp, 2006.
35. Liu L, Reeder B, Shuaib A, et al. Validity of stroke diagnosis on hospital discharge records in Saskatchewan, Canada: implications for stroke surveillance. Cerebrovasc Dis 1999;9:224�30.
36. Boyle E, Co�te� P, Grier AR, et al. Examining vertebrobasilar artery stroke in two Canadian provinces. Spine, in press.
37. Co�te� P, Kreitz BG, Cassidy JD, et al. The validity of the extension-rotation test as a clinical screening procedure before neck manipulation: a secondary analysis. J Manip Physiol Therap 1996;159�64.
38. van der Velde G, Hogg-Johnson S, Bayoumi A, et al. Identifying the best treatment among common non-surgical neck pain treatments: a decision analysis. Spine 2008;33(Suppl):S184�S191.
Key words: vertebrobasilar stroke, case control stud- ies, case crossover studies, chiropractic, primary care, complications, neck pain. Spine 2008;33:S176�S183
From the *Centre of Research Expertise for Improved Disability Outcomes (CREIDO), University Health Network Rehabilitation Solutions, Toronto Western Hospital, and the Division of Heath Care and Outcomes Research, Toronto Western Research Institute, Toronto, ON, Canada; �Department of Public Health Sciences, Management and Evaluation, University of Toronto, Toronto, ON, Canada; �Department of Health Policy, Management and Evalua- tion, University of Toronto, Toronto, ON, Canada; �Institute for Work & Health, Toronto, ON, Canada; �University Health Net- work Stroke Program, Toronto Western Hospital, Toronto, ON, Canada; and Division of Neurology, Department of Medicine, Fac- ulty of Medicine, University of Toronto, Toronto, ON, Canada. Supported by Ontario Ministry of Health and Long-term Care. P.C. is supported by the Canadian Institute of Health Research through a New Investigator Award. S.H.-J. is supported by the Institute for Work & Health and the Workplace Safety and Insurance Board of Ontario. The opinions, results, and conclusions are those of the authors and no endorsement by the Ministry is intended or should be inferred.
The manuscript submitted does not contain information about medical device(s)/drug(s).
University Health Network Research Ethics Board Approval number 05-0533-AE.
Address correspondence and reprint requests to J. David Cassidy, DC, PhD, DrMedSc, Toronto Western Hospital, Fell 4-114, 399 Bathurst Street, Toronto, ON, Canada M5T 2S8; E-mail: [email protected]
A chiropractor is a doctor who specializes in musculoskeletal and nervous system problems. It is the belief of the chiropractic community that problems in these areas can cause adverse health issues, including lowered resistance to disease, illness, and injury.
Chiropractors manipulate the spine to realign spinal joints in their patients. By doing so, patients are expected to experience optimum health without the assistance of drugs or surgery. Instead, chiropractors expect the body will heal itself once the spine and spinal joints are in proper alignment. Additionally, chiropractors consider and address other lifestyle factors which are commonly recognized as significantly affecting health such as diet, rest, exercise, heredity, and environmental factors. They also make other recommendations for changes which are expected to improve the patient�s overall health.
Chiropractors perform many of the same tasks as other general and specialty doctors. Patient health histories are gathered, physical, neurological, and orthopedic examinations are performed, and various laboratory tests, x-rays, and diagnostic imaging tools are used to diagnose and analyze the patient�s condition. Other forms of treatment may be used or recommended by the chiropractor including ultrasound, massage, heat, water, acupuncture, or electric currents. Prescription drugs and surgery are not part of the services provided by chiropractors. Chiropractors may recommend patients to see other doctors or specialists to address health issues or concerns outside of their area of expertise. Some chiropractors choose to specialize in a certain type of practice, such as orthopedics, neurology, sports injuries, internal disorders, diagnostic imaging, or pediatrics.
The Bureau of Labor Statistics predicts a job growth increase of 17% in the chiropractic field over the next seven years. An increasing public interest in alternative healthcare methods is beneficial to the chiropractic field. The public is seeking healthy living options which do not include prescription medicines or surgery; instead, a substantial number of people are searching for solutions which emphasize healthy lifestyles. The non-invasive procedures provided by chiropractors in answer to their patients health issues and concerns appeals to the segment of the public looking for these types of answers.
SELECTING THE RIGHT CHIROPRACTIC COLLEGE
Chiropractor students should select a college which offers a strong science degree or pre-medical program. Some colleges may have an affiliation with chiropractic training schools, which all future chiropractors must successfully complete. Research chiropractic schools to determine which one you are most interested in attending; this will help you to determine if the school is linked to any of the colleges you are considering. Courses in biology, chemistry, and physics will be important to individuals looking to work in a medical field. Electives may be concentrated in health, fitness, and nutrition. Students should, if given the opportunity, study topics and courses related to kinesiology and sports medicine. Courses in psychology and sociology will also help students to gain a more comprehensive understanding of people and society, better preparing them to serve the public. Additionally, business courses ensure that future professionals understand how to successfully manage a business in the complex healthcare field, as medical professionals must understand finances, medical insurance processing, business laws, business practices, business ethics, and medical records maintenance.
CHIROPRACTIC SCHOOLS
Students must attend chiropractic college in order to enter the profession. Upon completion of the program, students will have earned a doctorate in chiropractic medicine. The Council on Chiropractic Education, or CCE, is the nationally recognized accrediting agency by the United States Secretary of Education which regulates the quality of the curriculum offered at chiropractic colleges. Currently there are 15 CCE accredited chiropractic institutions in the United States. These include, as listed on the CCE website:
Students attend chiropractic college for four years. During this time, students are taught the scientific and academic skills and knowledge required to become experts in the field of chiropractic medicine. The final year is spent in practice, performing the functions of a chiropractic doctor under the supervision of an experienced professional. The curriculum includes intensive study of neuromusculoskeletal conditions, nutritional and holistic health, specialized and focused curriculum in areas of acupuncture and oriental medicine, applied nutrition, and various other disciplines. Students will complete extensive course hours in diagnosis, biochemistry, anatomy, chiropractic technique, and philosophy and ancillary therapeutic procedures.
TAKING THE NATIONAL BOARD EXAM
The National Board Exam for chiropractors is administered by the NBCE. The test is given twice each year. The exam consists of three parts. Part one is 110 multiple choice questions relating to general anatomy, spinal anatomy, physiology, chemistry, pathology, microbiology, and public health. The second part also consists of 110 multiple choice questions, but in the areas of general diagnosis, neuromusculoskeletal diagnosis, diagnostic imaging, and principles of chiropractic, chiropractic practice, and associated clinical sciences. Part three of the test consists of another 110 multiple choice questions and 10 case vignettes covering the areas of diagnosis or clinical impression, clinical laboratory and special studies examination, chiropractic techniques, case management, physical examination, case history, and roentgenologic examination. Each part of the test is timed. Additional specialized testing is offered for applicants who choose to pursue an area of specialization.
LICENSING FOR CHIROPRACTORS
After successful completion of an accredited chiropractic program, graduates will need to obtain a license to practice in their resident state or the state in which they intend to practice. State licensure regulations may vary from state to state. It is important to research your state�s regulations prior to completion of the doctor of chiropractic program to ensure all conditions are met. The Federation of Chiropractic Licensing Boards is a nonprofit organization which provides a link to the licensure information in all states. Locate information for each state through this directory.
The information provided includes licensing fees, renewal requirements, national board testing requirements, security and criminal check requirements, additional certification requirements, continuing education, and malpractice insurance requirements. A link to each state licensing board is also provided.
CONTINUING EDUCATION FOR CHIROPRACTORS
The chiropractic field is experiencing an increase in advancements in technology and knowledge through research and academic exploration. Changing regulations are also an area in which chiropractic doctors will need to remain current. Each state maintains their own continuing education requirements upon which licensing will be contingent. Twenty-four credit hours of continuing education every two years is a common requirement. All programs must be board approved and conducted by approved colleges or chiropractic associations or organizations. Check with your state licensing board to determine if the program has been approved prior to enrollment.
PRACTICING AS A CHIROPRACTOR
After obtaining a doctorate and passing the licensing examination, a new chiropractor has many options ahead of them. Most chiropractors will end up working solo or in a group practice, with about one in three being self-employed. A small group will work in hospitals or physicians� offices. The median pay for Chiropractors in 2016 was $67,520, with the lowest 10 percent earning less than $32,380, and the highest earning more than $141,030. Chiropractors can further increase their salary by building up a strong client base and developing their own practice. Many times, chiropractors will work in the evening or on weekends to accommodate their patients.
DAY TO DAY PRACTICE
Chiropractors will spend a lot of time on their feet as they examine and treat patients. Some of the most important qualities that a chiropractor can have include decision-making, detail-oriented, dexterity, empathy, and interpersonal skills. If the chiropractor is operating his or her own practice, the ability to manage a staff of employees like secretaries and nurses is vital to the success of the practice. An understanding of the current healthcare system is also important, as that will determine what kind of payments a chiropractor may be able to receive, unless they work in a cash-only system. More information can be found in the Occupational Outlook Handbook provided by the BLS.
CHIROPRACTIC SPECIALTIES AND CERTIFICATIONS
Another way for chiropractors to increase their annual earnings or skills would be to specialize in one or more areas. Specializations can help a chiropractor better diagnose and treat chronic illnesses, sports injuries, and/or complex occupational injuries. The American Chiropractic Association and American Board of Chiropractic Specialties (ABCS) lists 14 specialties and provides guidance to maintain standards of chiropractic certification. These include, as listed on the American Chiropractic Association website:
Chiropractic Physiotherapy and Rehabilitation (DACRB) Specialist
Has had extensive postgraduate training in physiologic therapeutics and rehabilitation to better treat injuries that may have resulted from an accident or a sports injury.
Treats a wide variety of health conditions that include all body systems and tissues, and focuses special attention on the relationship between the spine, nervous system, and the meridian system.
Is trained to encourage and promote a more advanced knowledge and use of nutrition in the practice of chiropractic for the maintenance of health and the prevention of disease.
Has special knowledge of both the normal function and diseases of the bones, joints, capsules, discs, muscles, ligaments, and tendons, as well as their complete neurological components, referred organ systems and contiguous tissues, and is able to diagnose and treat the conditions related to them.
Diplomate of the American Board of Forensic Professionals (DABFP)
Performs an orderly analysis, investigation, inquiry, test, inspection, and examination in an attempt to obtain the facts of a case, from which to form an expert opinion.
Is trained in chiropractic sports medicine and exercise science in order to treat sports injuries, enhance athletic performance, and promote physical fitness.
Chiropractic Occupational Health (DACBOH) Specialist
A DC trained in health care diagnosis and treatment choices for workplace neuromusculoskeletal injuries who is able to provide a broad range of work-related injury and illness prevention services for employee populations.
Diplomate in Clinical Chiropractic Pediatrics (DICCP)
Support members who take care of children in their chiropractic practices, and to promote the acceptance and advancement of pediatric chiropractic care.
These specialty �degrees� are given by their corresponding boards, which also maintain the level of expected qualifications and standards of excellency.
New studies in neuroscience suggest chiropractic care affects much more than back and neck pain. Celeste McGovern investigates an emerging body of evidence that spinal manipulation also improves your brain.
Imagine a convention that mixes cutting-edge natural health seminars with a surfer dude�s attitude, a revivalist�s enthusiasm and a good measure of live rock-�n-roll. That�s the California Jam, which took place in Costa Mesa in January. Billed as �the biggest health, wellness and chiropractic event on the planet�, it�s an annual meeting of thousands of unapologetically alternative practitioners who mill about three floors of exhibitions, sampling detox juices, protein snacks, �bulletproof� coffee and vitamins.
There�s a buzz about urine tests for metabolites; people are talking cellular detoxification and energy-balancing therapies, and they�re trading spinal adjustments on a row of tables. Inside the auditorium, a roster of headliner speakers takes the stage for two days, but one of the biggest ticket draws this year was a relatively unknown figure: neurophysiologist and chiropractor Heidi Haavik, who is pioneering a whole new field of research into what happens to a person�s brain when a chiropractor adjusts their spine.
�There is so much more to chiropractic care than back and neck pain, and headaches,� enthuses Haavik, who studied neuroscience after graduating from the New Zealand College of Chiropractic and is now focusing on research.
Up to now, there�s been a gulf between the available published research and the practice. A handful of studies have shown that chiropractic works only modestly�yet substantially better than drugs�at nipping neck and back pain,1 and may help with migraine,2 and even mysteriously lower blood pressure3 which, for 40 years, has been linked to joint dysfunction in the neck.
But the research is hardly enough to support its position as the most popular alternative medical treatment for more than a century, used by 30 million people in the US alone each year.
�Haavik�s research may finally explain scientifically the amazing results chiropractors have in clinical practice,� says Ross McDonald, a practising chiropractor and President of the Scottish Chiropractic Association.
The neuroscience studies explore the underlying mechanism of those results�how the spine and central nervous system (CNS) are interconnected and �talk� to each other, and how dysfunction in the spine can affect health and well-being.
One of Haavik�s studies, published this year in the journal Brain Sciences, looked at the effect of chiropractic adjustments in 28 patients with �subclinical� pain�those with a history of intermittent back or neck ache or stiffness for which they were never treated�but who were in pain the day of the experiment. On examination, all had tender spots and restricted joint movement in their spines.
Compared with �sham� adjustments, chiropractic spinal adjustments of these people induced significantly greater brain activity, or �cortical excitability� (which has to do with neuro-electrical signals produced when brain or peripheral muscles are stimulated), as measured by transcranial magnetic stimulation (TMS), which uses magnetic fields to stimulate nerve cells in the brain, as well as arm and leg muscle strength.
Increases in muscle strength have proved to be driven by brain activity resulting from spinal manipulation, and not by any changes made to the spinal cord itself. This offers a host of possibilities for, say, recovering muscle strength after nervous-system injuries. As the study concluded, �spinal manipulation may therefore be indicated� for patients who have lost muscle tone, or are recovering from a stroke or from orthopedic surgery that affects the muscles. It may even be of interest to athletes who participate in sports.4
These findings have confirmed a 2015 study which showed that, following a full-spine chiropractic adjustment session, voluntary leg muscle strength in study participants increased by 16 per cent, while electrical activity readings from the measured muscle increased by nearly 60 per cent. But most spectacularly, the researchers (from the Centre for Chiropractic Research in New Zealand) discovered a 45 per cent increase in the reflex pathway �drive� from the brain to muscle (an indicator of the ability of the brain to activate it). By contrast, the control participants who underwent the sham adjustment actually lost strength and brain drive to the measured muscle.5
This same Auckland-based team, led by Haavik and two colleagues are now embarking on some groundbreaking research involving brain-body communication in stroke patients.6 A preliminary study had tested the effect of a single chiropractic adjustment on 12 stroke patients, and found that it increased leg muscle strength by an average of 64 per cent and brain drive to the limb by more than 50 per cent. In contrast, both measurements fell after the sham adjustments in the controls.
Ordinarily, you wouldn�t expect to see muscles gain in strength after being asked to repeatedly resist something because muscles become fatigued. Now, that we have the technology to objectively measure an increase in muscle strength after an intervention, Haavik says, these results suggest that�chiropractic care is not only preventing fatigue, but making [muscles] even more efficient at producing force�.
The potential results of the new study could have a significant impact on the role of chiropractic care in people who have reduced muscle function as a result of stroke, she says.
Injury Risk
One interesting recent study by Haavik and her colleagues looked specifically at the impact of chiropractic on the risk of falls among older people.7
Falling is a significant cause of death, injury and health decline in the elderly, with about 30-40 per cent of older adults who still live independently suffering from at least one fall each year or more as they age.
In this randomized controlled trial, half of the group of 60 community-dwelling people, aged over 65 and living in Auckland, received 12 weeks of chiropractic care (two visits per week), while the other half received the �usual care�, which didn�t include seeing a chiropractor.
The patients were tested on their proprioception (in this case, their awareness of where their ankle joint was positioned), postural stability and ability to process �multi-sensory� information�a sound-induced flash illusion test, using flashing lights and beeps. This test is used to screen for fall risk, as it measures how well people can process two different kinds of stimuli at a time.8 The participants were also given a sensorimotor function test, which measured their ability to move their feet in response to a panel that suddenly lit up on the floor, plus a questionnaire based on their self-perceived health-related quality of life.
Over the 12 weeks of the study, the group receiving chiropractic care showed significant improvement in ankle joint position sense, meaning their brains may have become more accurately aware of what was going on in their feet; they were also able to react and move their foot onto the illuminated panel on the floor more quickly than before the chiropractic care. These improvements were not seen in the control group.
The chiropractic patients were 13 per cent better able to accurately report the correct number of flashes with the corresponding number of beeps�meaning they had lowered their risk for falls.
What�s more, at the end of the study, the participants who had received the chiropractic care reported a 2.4-fold increased improvement in the quality-of-life questionnaire compared with the controls.7
Your Plastic Brain
Haavik is now trying to explain how chiropractic achieves all this, and why restoration of proper movement is able to so profoundly affect the brain and overall health.
The CNS�the brain and spinal cord�and all the nerves beyond the CNS (the peripheral nervous system, or PNS) is a complex network comprising as many as 10 billion nerve cells (also called �neurons�) and 60 trillion synapses�tiny little junctions between neurons that mediate the �talk� across highly specialized neural circuits via chemicals called �neurotransmitters�. Indeed, nerves feed out of each segment of the spine like strands of spaghetti, and facilitate communication back and forth with various regions of the body.
Everything we do�from our basic motor reflexes to our capacity to experience abstract thoughts and feelings�relies on the precision of the computational processes performed by these CNS and PNS neural circuits. They, in turn, depend on having healthy excitatory and inhibitory systems.
A neuron gets �excited� when it�s �talked to� loudly enough, or stimulated, and this sends an electrical message down one of the neuron�s extensions (called �axons�), so allowing it to talk to another nerve cell by releasing more neurotransmitters at the synapses.
Such talk happens all the time as input comes in from our external senses (eyes, ears, mouth, nose and touch), as well as through an inner �map� of the location of our muscles and joints in three-dimensional space relative to each other (proprioception), as the brain carries out its decisions and functions.
Contrary to decades of scientific dogma, a recent wave of research has shown that the brain is actually highly adaptable to its ever-changing environment throughout life. It does this by keeping an up-to-date tab on its sensory inputs and its internal map of the self. This ability to adapt is known as �neural plasticity�.
Haavik likens the plasticity of the CNS to the subtle changes in the bed in a flowing stream. �You can never really step into the same river twice; the water, stones and silt of the riverbed are constantly changing,� she says. Likewise, your brain is changing with every thought and every execution, and is in a constant state of flux.
In fact, she believes her research demonstrates that vertebral subluxations (dysfunctional spinal segments; see box, page 33) lead to a breakdown in the way the brain perceives and controls the movement of the spine. And this spinal dysfunction doesn�t just affect how the brain then perceives and controls the spine, but also how it perceives and controls other parts of the body as well.
When the brain gets even slightly wrong information, it builds a faulty map that can impede neural signaling as effectively as damped sensory input�like wearing a blindfold or losing the sense of taste. And that translates to faulty functioning.
Chronic pain and neurodegenerative disorders have been linked to these faulty perceptions by the plastic brain.9 �Pain and conditions with other symptoms don�t necessarily happen all of a sudden for no reason. They can slowly develop without your awareness, a bit like a thousand straws on a camel�s back before it breaks,� says Haavik. �Only when the last straw is added do you feel the effect.�
Haavik�s team hypothesizes that spinal adjustments that restore normal movement also restore more normal data input from the spine to the brain. This, in turn, allows the spinal cord, brain stem and brain to process any incoming information more coherently.
�We believe this to be the mechanisms by which adjustments of vertebral subluxations can improve nervous system function, as observed daily in chiropractic practices all around the world.�
While the New Zealand researchers are reluctant to speculate on immunity, an emerging body of research is demonstrating the interconnectedness of both the nervous and immune systems too. An entirely new lymphatic system in the brain was only discovered in 2015 by a team of researchers at the University of Virginia,10 which highlights how limited our understanding of the brain, and the effect of the nervous system on global health, still is. It also raises further questions about how improving one system can lead to improvement in the other�and so perhaps why some people experience benefits to their immune-mediated disease with chiropractic manipulations.
�What is becoming clear is that chiropractic care seems to impact our brain�s inner reality by restoring the proper processing and integration of sensory information, which alters the way our brain controls our body,� says Haavik.
�It�s so exciting to see that there are other possible ways now to explain the effects of chiropractic that are actually congruent with current neuroscience,� she adds. �It�s actually more profound and powerful than we could have ever thought.�
The Many Faces Of Chiropractic
There are two schools of thought in chiropractic: the �mechanics�, who claim it should be absorbed into mainstream medicine as a standardized treatment for back and neck pain; and the �vitalists�, who believe that the treatment is much more far-reaching, as they�ve seen it help cases of fatigue, joint pain, migraines, allergies, asthma, bedwetting and even infertility.
The latter philosophy is radically different from the current medical paradigm. �The body has an innate ability to heal, provided there is no interference,� says Gilles LaMarche, vice president of professional relations at Life University in Atlanta, Georgia, the world�s largest chiropractic college. �It is self-developing, self-maintaining and self-healing.�
In this vitalistic view of chiropractic, when you get an infection or scrape your knee, the best practitioner merely assists the body in getting on with its own spontaneous and spectacular business of healing itself.
The chiropractor�s job, as vitalists see it, is to remove any interference in the body at the level of the spine, which they consider central.
�Conventional medicine doesn�t interpret symptoms as we interpret symptoms,� explains LaMarche from his end of chiropractic.
He sees fever, for instance, as one of the body�s natural mechanisms to fight infection: raising the body�s temperature kills bacteria and viruses, and facilitates other immune functions.
�Many doctors see fever as bad, as something to reduce,� he says, �and they give Tylenol [paracetamol], not considering it as a toxin that is actually going to stay in the liver and therefore interfere with healing and health.�
How Chiropractic Changes The Brain
So what�s going on in the brain after a chiropractic adjustment that could be increasing muscle strength in stroke patients? As a 2016 study from Aalborg University Hospital in Denmark demonstrated, a single chiropractic adjustment helps to improve something called �somatosensory integration� (when the brain receives accurate sensory input, so allowing it to properly organize and execute subsequent behaviors).1
Such a change mostly happens in the prefrontal cortex, that part of the brain known to be a key player in executive functions. It�s a sort of command control centre, integrating and coordinating the multiple neural inputs from a constantly changing environment to solve problems and achieve goals.
�Chiropractic care, by treating the joint dysfunction, appears to change processing by the prefrontal cortex,� the authors conclude.
So, while some chiropractors (and their patients) may have thought their adjustments were making changes locally and directly from the spine, in fact, the change is apparently effected indirectly by being sent to �central command� (the brain), then redirected back down neuronal chains to give the perception of reduced pain as well as other benefits.
�This suggests that chiropractic care may, as well, have benefits that exceed simply reducing pain or improving muscle function and may explain some claims regarding this made by chiropractors,� the study researchers say.
These claims include the ability of adjustments to increase muscle strength and core stability, improve reaction time and proprioception (your awareness of your body�s position in space), and so reduce the risk of injury.
What Is A Subluxation?
In 1895 in Iowa, the founder of chiropractic, Daniel David Palmer, claimed to have restored the hearing of deaf janitor Harvey Lillard by adjusting the part of his spine that Palmer could feel was �out of alignment�.
From this, he devised a theory that �misaligned� or �out-of-place� spinal segments interfere with proper nerve function, and that �adjusting� these segments back to their normal position relieves pressure on the nerves and restores neural function.
Chiropractors assess spines for areas where some of the small muscles that attach to the individual vertebrae have become tight due to injury, hunching over mobile phones and computers, or simply overuse. When these tight muscles cause the vertebrae�the small bones that make up the spine�to twist, certain parts of the bones can protrude and feel �misaligned� or �stuck�. Chiropractors call it a vertebral �subluxation� or �joint restriction�.
�It is more that a bone is functioning or moving in a less than ideal way�in a manner that is not �normal� for the body,� says Heidi Haavik.
And chiropractors counter this abnormality by �adjusting� it. �We don�t really put bones back in place when we adjust the spine,� she explains. The aim of the short, quick movements of chiropractic adjustments to the spine are to restore its natural range of movement.
How To Find A Good Chiropractor
All chiropractors must attend a licensed chiropractic college or university, and undergo at least four years of training in anatomy, neurology, physiology, radiology, pathology, clinical diagnostics and clinical nutrition, as well as physiotherapy and chiropractic techniques.
In the UK, chiropractors must pass a national exam to ensure competency. It is illegal to practice without first registering with the General Chiropractic Council.
Apart from these legal requirements, chiropractors have a broad range of approaches, specialities and techniques. Make sure to choose a chiropractor who:
��Meets your particular needs. Some chiropractors take a biomechanical approach, or treat a narrow range of conditions and only see people when they have a problem, like pain, while others take a �wellness� approach and treat people to prevent problems. Many chiropractors have special areas of focus: sports injuries, pregnancy, children, or even functional medicine, testing for metabolic deficiencies such as low vitamin D levels and prescribing supplements.
� Has a good reputation. It�s worth considering if other people have had good results.
� Talks with you at no cost to discuss your needs and their skills and services, and employs techniques that suit you. Some chiropractors use manual adjustments only, while others use devices like drop-tables�examination tables that move when the chiropractor adjusts so the impulse is delivered by the release-action of the table�and activators�hand-held tools that resemble a tire-pressure gauge and are spring-activated to deliver small and precisely controlled impulses to areas like the cervical (neck) spine. Some may also be trained in techniques like acupuncture, dry needling (acupuncture needles are inserted in muscle tissue to stimulate the release of �trigger points�, where muscles have gone into spasm) and active release technique (ART), which also targets contractions of muscles, ligaments and tendons to reduce joint stress.
� Carries out a thorough assessment before beginning treatment. A medical history and physical exam should be done to rule out conditions that need further referral or should not be treated by chiropractic. A chiropractor is trained to perform and read X-rays, which are sometimes required, but only if they meet standardized criteria.
� Gives you clear outcome measures to gauge improvement, such as less pain or an overall improved sense of wellbeing.
� Gives you enough time and attention. The best practitioner is also a coach or partner who can help you achieve your best state of health. Only choose someone who truly supports you.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




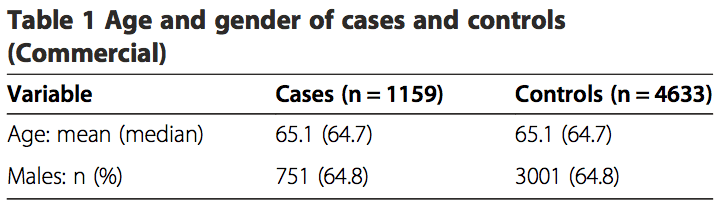
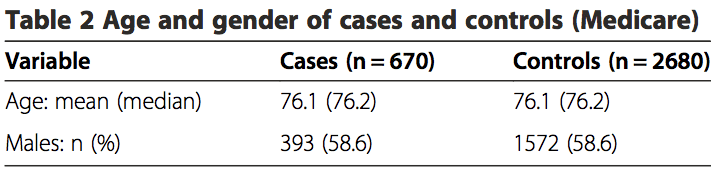
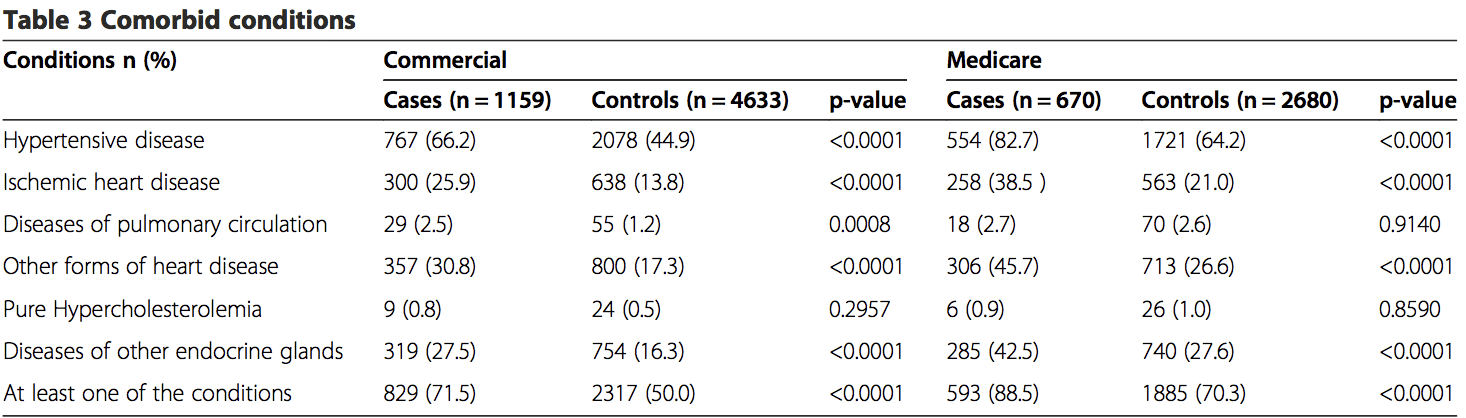 Among the commercially insured, 1.6% of stroke cases had visited chiropractors within 30 days of being admit- ted to the hospital, as compared to 1.3% of controls visit- ing chiropractors within 30 days prior to their index date. Of the stroke cases, 18.9% had visited a PCP within 30 days prior to their index date, while only 6.8% of controls had visited a PCP (Table 4). The proportion of exposures for chiropractic visits was lower in the MA sample within the 30-day hazard period (cases = 0.3%; controls = 0.9%). However, the proportion of exposures for PCP visits was higher, with 21.3% of cases having PCP visits as compared to12.9% for controls (Table 5).
Among the commercially insured, 1.6% of stroke cases had visited chiropractors within 30 days of being admit- ted to the hospital, as compared to 1.3% of controls visit- ing chiropractors within 30 days prior to their index date. Of the stroke cases, 18.9% had visited a PCP within 30 days prior to their index date, while only 6.8% of controls had visited a PCP (Table 4). The proportion of exposures for chiropractic visits was lower in the MA sample within the 30-day hazard period (cases = 0.3%; controls = 0.9%). However, the proportion of exposures for PCP visits was higher, with 21.3% of cases having PCP visits as compared to12.9% for controls (Table 5).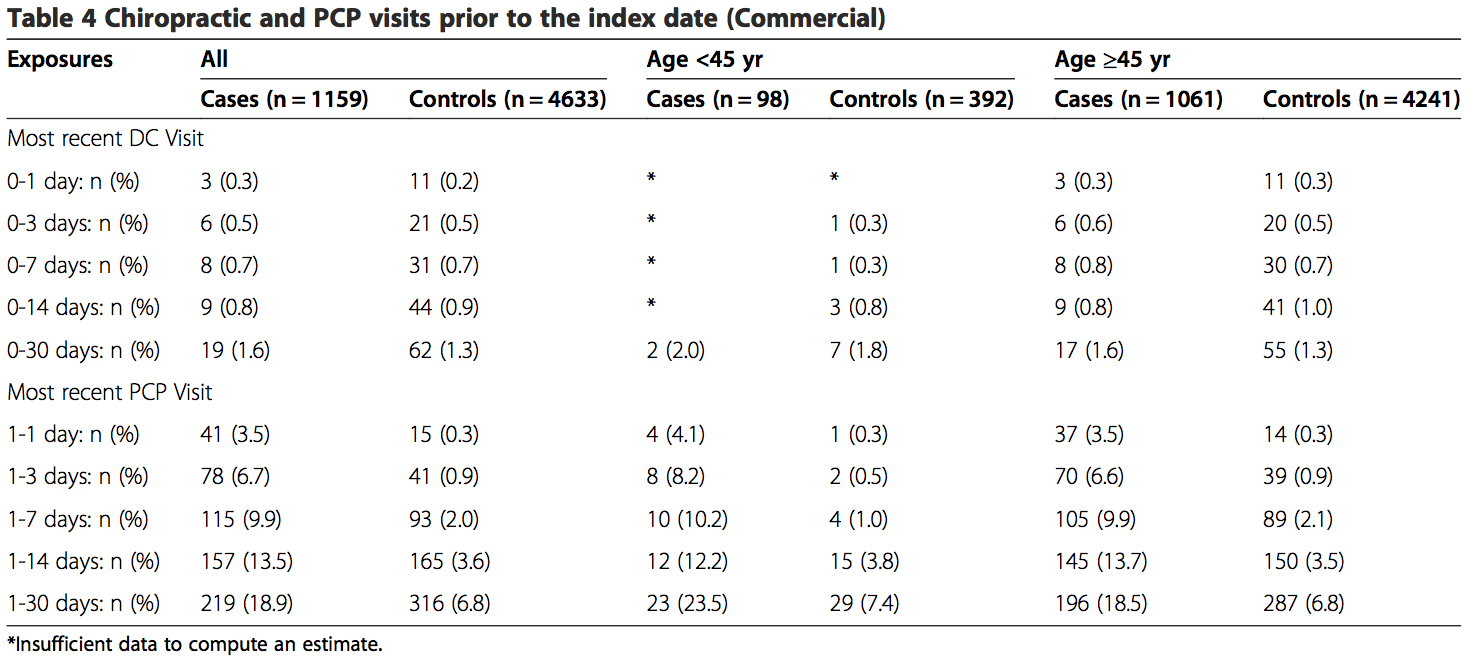
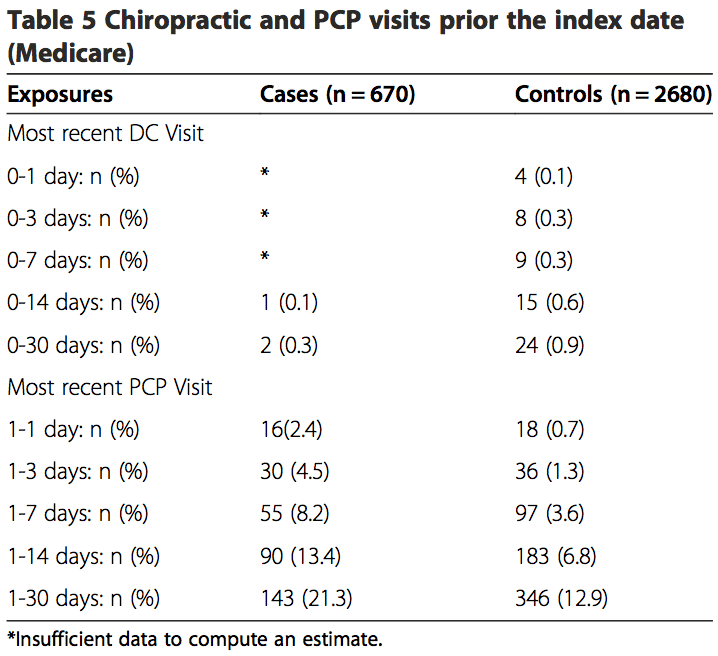 The results from the analyses of both the commercial population and the MA population were similar (Tables 6, 7 and 8). There was no association between chiropractic visits and VBA stroke found for the�
The results from the analyses of both the commercial population and the MA population were similar (Tables 6, 7 and 8). There was no association between chiropractic visits and VBA stroke found for the�