For individuals experiencing musculoskeletal issues and pain symptoms, can learning about biomechanics and how it applies to movement, physical training, and performance, help in injury treatment and prevention?
Biomechanics
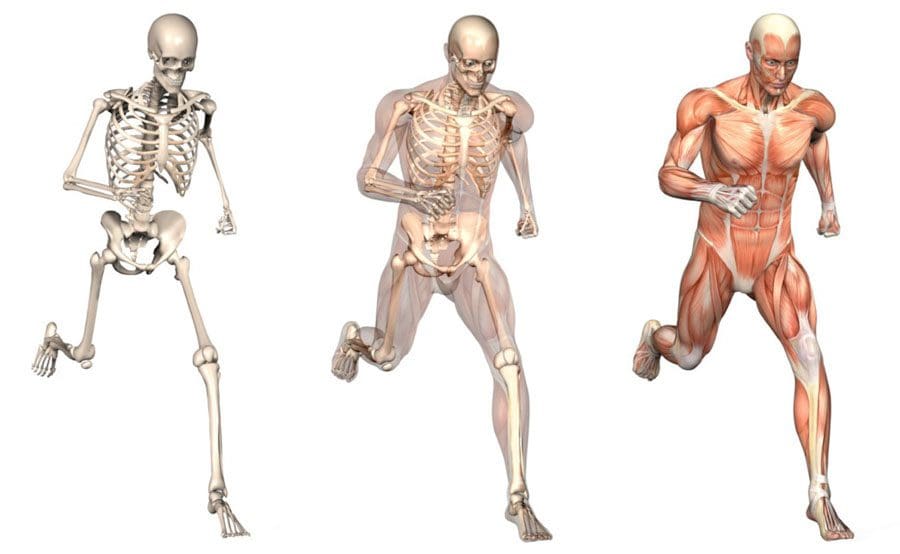
Biomechanics studies all life forms and their mechanical workings. Many think of biomechanics in sports and athletic performance, but biomechanics helps create and improve technologies, equipment, and injury rehabilitation techniques. (Tung-Wu Lu, Chu-Fen Chang 2012) Scientists, sports medicine doctors, physiotherapists, chiropractors, and conditioning specialists utilize biomechanics to help develop training protocols and techniques to improve therapy outcomes.
Body Movement
Biomechanics studies the movement of the body, including how muscles, bones, tendons, and ligaments work together, especially when movement is not optimal or correct. It is part of the larger field of kinesiology, specifically focusing on motion mechanics and analysis of how all the individual parts of the body work together to make up athletic and normal movements. (José M Vilar et al., 2013) Biomechanics includes:
Structure of bones and muscles.
Movement ability.
Mechanics of blood circulation, renal function, and other functions.
The study of forces and the effects of these forces on the tissues, fluid, or materials used for diagnosis, treatment, or research. (Jose I. Priego-Quesada 2021)
Sports
Sports biomechanics studies motion in exercising, training, and sports, which incorporates physics and the laws of mechanics. For example, the biomechanics of a specific exercise looks at:
Body position.
Movement of the feet, hips, knees, back, shoulders, and arms.
Knowing the correct movement patterns helps make the most of the exercise while preventing injuries, correcting form mistakes, informing training protocols, and increasing positive results. Understanding how the body moves and why it moves the way it does helps medical professionals prevent and treat injuries, alleviate pain symptoms, and improve performance.
Equipment
Biomechanics is used in the development of physical and sports equipment to improve performance. For example, a shoe can be designed for optimal performance for a skateboarder, long-distance runner, or soccer player. Playing surfaces are also studied for this purpose, such as how the surface stiffness of artificial turf affects athletic performance. (Jose I. Priego-Quesada 2021)
Individuals
Biomechanics can analyze an individual’s movements for more effective movement during training and games.
For example, an individual’s running gait or swing can be filmed with recommendations on what to change to improve.
Injuries
The science studies the causes, treatment, and prevention of neuromusculoskeletal injuries.
The research can analyze the forces that cause injuries and provide information for medical professionals on how to reduce the risk of injury.
Training
Biomechanics studies sports techniques and training systems to develop ways to improve efficiency.
This can include research on positioning, release, follow-through, etc.
It can analyze and help design new training techniques based on the mechanical demands of the sport, aimed at resulting in better performance.
For example, muscle activation is measured in cycling using electromyography and kinematics, which helps researchers analyze factors like posture, components, or exercise intensity that affect activation. (Jose I. Priego-Quesada 2021)
Motions
In biomechanics, the body’s motions are referred to from anatomical positioning:
Standing upright, with the gaze straight ahead
Arms at the sides
Palms facing forward
Feet spaced slightly apart, toes forward.
The three anatomical planes include:
Sagittal – median – Dividing the body into right and left halves is the sagittal/median plane. Flexion and extension occur in the sagittal plane.
Frontal – The frontal plane divides the body into front and back sides but also includes abduction, or moving a limb away from the center, and adduction, or moving a limb towards the center in the frontal plane.
Transverse – horizontal. – The upper and lower parts of the body are divided by the transverse/horizontal plane. Rotating movements occur here. (American Council on Exercise 2017)
Moving the body in all three planes occurs with daily activity. This is why performing exercises in each plane of motion to build strength, function, and stability is recommended.
Tools
Various tools are used to study biomechanics. Studies are usually performed using a device known as electromyography or EMG sensors. Sensors are placed on the skin and measure the amount and degree of muscle fiber activation in certain muscles during test exercises. EMGs can help:
Researchers understand which exercises are more effective than others.
Therapists know whether patients’ muscles are properly operating and functioning.
Dynamometers are another tool that helps measure muscle strength.
They measure the force output generated during muscle contractions to see if the muscles are sufficiently strong.
They are used to measure grip strength, which can be an indicator of overall strength, health, and longevity. (Li Huang et al., 2022)
Beyond Adjustments: Chiropractic and Integrative Healthcare
References
Lu, T. W., & Chang, C. F. (2012). Biomechanics of human movement and its clinical applications. The Kaohsiung journal of medical sciences, 28(2 Suppl), S13–S25. https://doi.org/10.1016/j.kjms.2011.08.004
Vilar, J. M., Miró, F., Rivero, M. A., & Spinella, G. (2013). Biomechanics. BioMed research international, 2013, 271543. https://doi.org/10.1155/2013/271543
Priego-Quesada J. I. (2021). Exercise Biomechanics and Physiology. Life (Basel, Switzerland), 11(2), 159. https://doi.org/10.3390/life11020159
American Council on Exercise. Makeba Edwards. (2017). Planes of Motion Explained (Exercise Science, Issue. https://www.acefitness.org/fitness-certifications/ace-answers/exam-preparation-blog/2863/the-planes-of-motion-explained/
Huang, L., Liu, Y., Lin, T., Hou, L., Song, Q., Ge, N., & Yue, J. (2022). Reliability and validity of two hand dynamometers when used by community-dwelling adults aged over 50 years. BMC geriatrics, 22(1), 580. https://doi.org/10.1186/s12877-022-03270-6
Individuals that have gone through a back injury may develop a synovial spinal cyst as a way to protect the spine that could cause pain symptoms and sensations. Can knowing the signs help healthcare providers develop a thorough treatment plan to relieve pain, prevent worsening of the condition and other spinal conditions?
Spinal Synovial Cysts
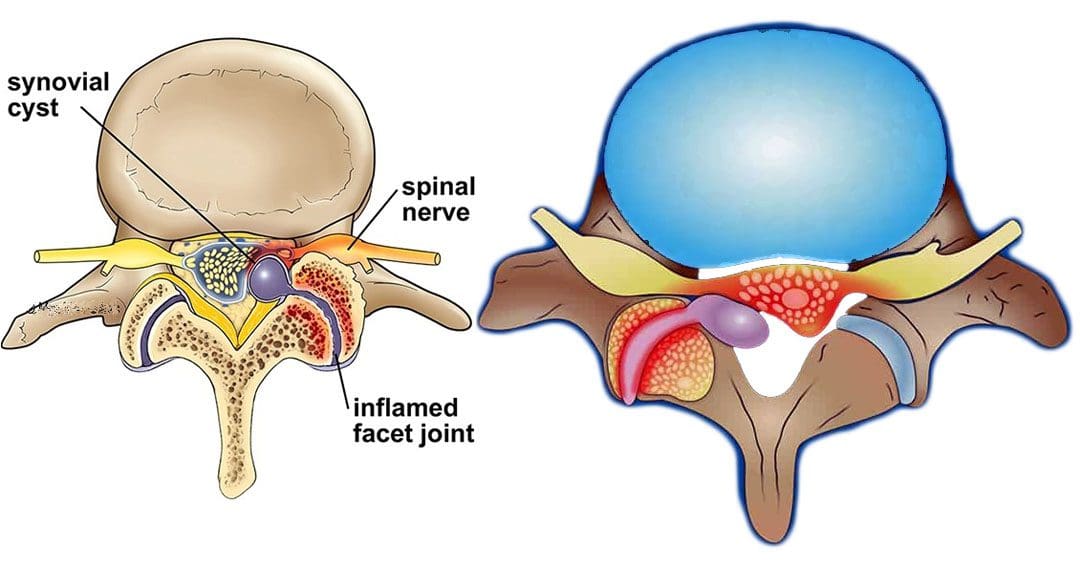
Spinal synovial cysts are benign fluid-filled sacs that develop in the spine’s joints. They form because of spinal degeneration or injury. The cysts can form anywhere in the spine, but most occur in the lumbar region/lower back. They typically develop in the facet joints or junctions that keep the vertebrae/spinal bones interlocked.
Symptoms
In most cases, synovial cysts don’t cause symptoms. However, the doctor or specialist will want to monitor for signs of degenerative disc disease, spinal stenosis, or cauda equina syndrome. When symptoms do present, they typically cause radiculopathy or nerve compression, which can cause back pain, weakness, numbness, and radiating pain caused by the irritation. The severity of symptoms depends on the size and location of the cyst. Synovial cysts can affect one side of the spine or both and can form at one spinal segment or at multiple levels.
Effects Can Include
Radiculopathy symptoms can develop if the cyst or inflammation caused by the cyst comes into contact with a spinal nerve root. This can cause sciatica, weakness, numbness, or difficulty controlling certain muscles.
Neurogenic claudication/impingement and inflammation of spinal nerves can cause cramping, pain, and/or tingling in the lower back, legs, hips, and buttocks. (Martin J. Wilby et al., 2009)
If the spinal cord is involved, it may cause myelopathy/severe spinal cord compression that can cause numbness, weakness, and balance problems. (Dong Shin Kim et al., 2014)
Symptoms related to cauda equina, including bowel and/or bladder problems, leg weakness, and saddle anesthesia/loss of sensation in the thighs, buttocks, and perineum, can present but are rare, as are synovial cysts in the middle back and neck. If thoracic and cervical synovial cysts develop, they can cause symptoms like numbness, tingling, pain, or weakness in the affected area.
Causes
Spinal synovial cysts are generally caused by degenerative changes like osteoarthritis that develop in a joint over time. With regular wear and tear, facet joint cartilage/the material in a joint that provides protection, a smooth surface, friction reduction, and shock absorption begins to waste away. As the process continues, the synovium can form a cyst.
Traumas, large and small, have inflammatory and degenerative effects on joints that can result in the formation of a cyst.
Around a third of individuals who have a spinal synovial cyst also have spondylolisthesis.
This condition is when a vertebrae slips out of place or out of alignment onto the vertebra underneath.
It is a sign of spinal instability.
Instability can occur in any spine area, but L4-5 are the most common levels.
This segment of the spine takes most of the upper body weight.
Epidural corticosteroid injections can reduce inflammation and could be an option to relieve pain.
Patients are recommended to receive no more than three injections per year.
Surgical Options
For severe or persistent cases, a doctor may recommend decompression surgery to remove the cyst and surrounding bone to relieve pressure on the nerve root. Surgical options range from minimally invasive endoscopic procedures to larger, open surgeries. The best surgical option varies based on the severity of the situation and whether associated disorders are present. Surgical options include:
Laminectomy – Removal of the bony structure that protects and covers the spinal canal/lamina.
Hemilaminectomy – A modified laminectomy where a smaller portion of the lamina is removed.
Facetectomy – The removal of part of the affected facet joint where the synovial cyst is located, usually following a laminectomy or hemilaminectomy.
Fusionof the facet joints and vertebra – Decreases vertebral mobility in the injured area.
Most individuals experience immediate pain relief following a laminectomy or hemilaminectomy.
Fusion can take six to nine months to heal completely.
If surgery is performed without fusion where the cyst originated, the pain could return, and another cyst could form within two years.
Surgery Complications include infection, bleeding, and injury to the spinal cord or nerve root.
How I Gained My Mobility Back With Chiropractic
References
Wilby, M. J., Fraser, R. D., Vernon-Roberts, B., & Moore, R. J. (2009). The prevalence and pathogenesis of synovial cysts within the ligamentum flavum in patients with lumbar spinal stenosis and radiculopathy. Spine, 34(23), 2518–2524. https://doi.org/10.1097/BRS.0b013e3181b22bd0
Kim, D. S., Yang, J. S., Cho, Y. J., & Kang, S. H. (2014). Acute myelopathy caused by a cervical synovial cyst. Journal of Korean Neurosurgical Society, 56(1), 55–57. https://doi.org/10.3340/jkns.2014.56.1.55
Epstein, N. E., & Baisden, J. (2012). The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surgical neurology international, 3(Suppl 3), S157–S166. https://doi.org/10.4103/2152-7806.98576
Individuals’ feet will heat up when walking or running; however, burning feet could be a symptom of medical conditions like athlete’s foot or a nerve injury or damage. Can awareness of these symptoms help identify solutions to relieve and heal the underlying condition?
Burning Feet
Walkers and runners often experience heat in their feet. This is natural from the increased circulation, heart rate, warm or hot sidewalks, and pavement. But the feet could experience an abnormal hot or burning sensation. Usually, the overheating is caused by socks and shoes and fatigue after a long workout. The first self-care steps include trying new or specialized footwear and workout adjustments. If burning feet persist or there are signs of infection, tingling, numbness, or pain, individuals should see their healthcare provider. (Mayo Clinic. 2018)
Footwear
The shoes and how they are worn may be the cause.
First, look at the material of the shoes. They could be shoes and/or insoles that don’t circulate air. They can get hot and sweaty without proper air circulation around the feet.
When choosing running shoes, consider a mesh material that allows airflow to keep the feet cool.
Consider getting fitted for shoes that are the right size, as the feet swell when running or walking.
If the shoes are too small, air can’t circulate, creating more friction between the foot and the shoe.
Shoes that are too large can also contribute to friction as the feet move around too much.
Insoles could also contribute.
Some insoles can make the feet hot, even if the shoes are breathable.
Swap the insoles from another pair of shoes to see if they are contributing, and if so, look into new insoles.
Tips to help prevent hot feet:
Topical Ointments
Use an anti-blister/chafing topical cream to lubricate and protect the feet.
This will reduce friction and prevent blisters.
Lace Properly
Individuals may be lacing the shoes too tight, constricting circulation, or irritating the nerves at the top of the foot.
Individuals should be able to slide one finger under the knot.
Remember that the feet will swell as walking or running commences
Individuals may need to loosen their laces after warming up.
Individuals are recommended to learn lacing techniques that will ensure they are not too tight over the sensitive areas.
Cushioning
Fatigue from long workouts or long days standing/moving can result in burning feet.
Individuals may need added cushioning in the shoes.
Look for work and athletic shoes that have added cushioning.
Shoe Allergies
Individuals may have an allergic reaction or a sensitivity to the fabric, adhesives, dyes, or other chemicals. (Cleveland Clinic. 2023) The chemicals used in production vary for leather compared to fabric and are different by brand and manufacturer.
A shoe material allergy may also result in burning, itching, and swelling.
It’s recommended to note whether symptoms only happen when wearing a specific pair of shoes.
Recommendations are to try different kinds and brands of shoes.
Socks
The sock fabric could be contributing to hot or burning feet. Steps to take can include:
Avoid cotton
Cotton is a natural fiber but is not recommended for walking and running as it holds sweat that can keep the feet wet.
It is recommended to use socks made of Cool-Max and other artificial fibers that wick sweat away and cool them down.
Wool
Wool socks can also cause itching and burning sensations.
Consider athletic socks made from itch-free wool.
Mindfulness
Individuals could be sensitive to other fabrics or dyes in socks.
Take note of which socks cause hot or burning feet symptoms.
Individuals could also be sensitive to laundry products and are recommended to try a different brand or type.
Medical Conditions
In addition to shoes and socks, medical conditions could cause and contribute to symptoms.
Athlete’s Foot
Athlete’s foot is a fungal infection.
Individuals may feel a burning sensation in the affected area.
Typically, it is itchy, red, scaling, or cracking.
Rotate shoes.
The fungus grows in damp places, therefore, it is recommended to rotate shoes to allow them to dry out between workouts.
Wash and dry the feet after walking or running.
Try home and over-the-counter solutions, powders, and remedies to treat athlete’s foot.
Peripheral Neuropathy
Individuals frequently experiencing burning feet apart from when they have been exercising could be due to nerve damage known as peripheral neuropathy. (National Institute of Neurological Disorders and Stroke. 2023) Peripheral neuropathy symptoms include pins and needles, numbness, tickling, tingling, and/or burning sensations.
Examination
Diabetes is one of the most common causes of peripheral neuropathy.
Diabetes can come on at any age.
Individuals need to learn how to protect their feet, as exercise is recommended for diabetes.
Other conditions that can produce peripheral neuropathy include:
Vitamin B-12 deficiency
Alcohol abuse
Circulatory disorders
AIDS
Heavy metal poisoning
Massage and Movement
Massaging the feet also increases circulation.
Exercise such as walking is recommended for peripheral neuropathy as it improves circulation to the feet.
Can musculoskeletal therapies treat individuals with upper crossed syndrome to relieve pain, improve posture, and strengthen the muscles in the neck, shoulders and chest?
Upper Crossed Syndrome
Upper crossed syndrome is a condition in which the muscles of the shoulders, neck, and chest become weak and tight, and is usually brought on from practicing unhealthy posture. Symptoms typically include:
Neck stiffness and pulling sensations.
Jaw tension and/or tightness
Upper back tension, lack of flexibility, stiffness, and aching soreness.
Neck, shoulder, and upper back pain.
Tension headaches
Rounded shoulders
Hunched spine
Upper Crossed Syndrome and Posture
The condition affects healthy posture by creating imbalanced muscles between the upper back and chest.
The tight short muscles in the upper chest get overly stretched and remain in a semi-contracted state pulling on the back muscles.
This causes the muscles in the upper back, shoulders, and neck to get pulled and weaken.
The result is a hunched back, forward shoulders, and protruded neck.
The specific muscles affected include the trapezius and the levator scapula/side of the neck muscles. (Hospital for Special Surgery. 2023)
Prescription anti-inflammatory medication for pain symptoms – short-term.
Individuals may be advised by the chiropractic therapy team to avoid too much bed rest and to limit or avoid activities that can cause pain or worsen symptoms. (Cedars-Sinai. 2022)
Studies have shown chiropractic spinal manipulation effectively reduces neck, spine, and low back pain symptoms. (Gevers-Montoro C, et al., 2021)
Increasing or decreasing physical activity as recommended by the therapy team.
Using ice or heat packs to relieve pain and increase circulation to promote muscle rehabilitation and healing.
Using topical pain creams or gels.
Over-the-counter nonsteroidal – NSAIDs, like Advil or Motrin and Aleve.
Muscle relaxants to relieve tension short-term.
Enhance Your Lifestyle
References
Hospital for Special Surgery. Move with the purpose to combat upper and lower crossed syndromes.
National Institute of Arthritis and Musculoskeletal and Skin Diseases. Back pain.
Seidi, F., Bayattork, M., Minoonejad, H., Andersen, L. L., & Page, P. (2020). Comprehensive corrective exercise program improves alignment, muscle activation, and movement pattern of men with upper crossed syndrome: a randomized controlled trial. Scientific reports, 10(1), 20688. https://doi.org/10.1038/s41598-020-77571-4
Bae, W. S., Lee, H. O., Shin, J. W., & Lee, K. C. (2016). The effect of middle and lower trapezius strength exercises and levator scapulae and upper trapezius stretching exercises in upper crossed syndrome. Journal of physical therapy science, 28(5), 1636–1639. https://doi.org/10.1589/jpts.28.1636
National Institute of Neurological Disorders and Stroke. Back pain.
Cedars-Sinai. Back and neck pain.
Gevers-Montoro, C., Provencher, B., Descarreaux, M., Ortega de Mues, A., & Piché, M. (2021). Clinical Effectiveness and Efficacy of Chiropractic Spinal Manipulation for Spine Pain. Frontiers in pain research (Lausanne, Switzerland), 2, 765921. https://doi.org/10.3389/fpain.2021.765921
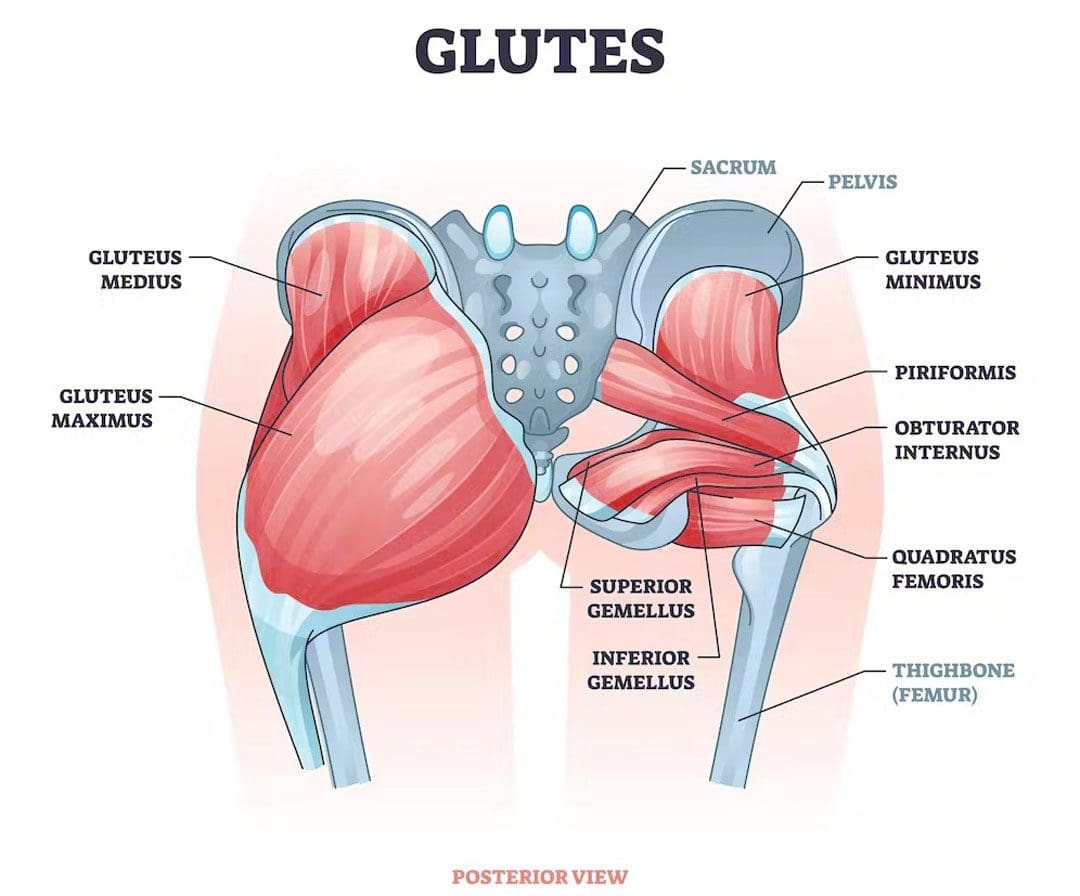
The gluteal muscles/glutes comprise the buttocks. They are a powerful muscle group that consists of three muscles. The gluteus maximus, gluteus medius, and gluteus minimus. The glute muscles help power physical performance and daily movements like walking, standing, and sitting and help to prevent injuries to the core, back, abdominal muscles, and other supporting muscles and tissues. Individuals can develop a glute imbalance where one side becomes more dominant and activates more or is higher than the other. An imbalance that is not addressed can lead to further muscle imbalance, posture problems, and pain issues. Injury Medical Chiropractic and Functional Medicine Clinic can develop a personalized treatment plan to relieve symptoms and restore alignment, balance, and health.
Glute Muscle Imbalance
Strong, healthy glutes promote lumbopelvic stability and rhythm, meaning they keep the low back and pelvis in correct alignment to prevent strains and injuries. Glute imbalance occurs when one side of the glutes is larger, stronger, or more dominant. Glute imbalances are common and part of normal human anatomy, as the body is not perfectly symmetrical. Shifting and utilizing the more dominant side when taking on weight or picking up objects is normal, so the one side gets bigger. Just as an individual prefers one hand, arm, and leg over another, one glute side can work harder and become stronger.
Causes
There are several causes of glute muscle imbalance, including:
Anatomical variations- Everyone has uniquely shaped muscles, attachment points, and nerve pathways. These variations can make one side of the glutes more dominant or stronger.
Unhealthy posture.
Back pain symptoms can cause individuals to take on unhealthy postures and positioning, like leaning on one side.
Pre-existing injuries.
Inadequate rehabilitation from a previous injury.
Nerve injuries.
Ankle sprains can lead to reduced glute activation.
Improper training
Leg length discrepancies
Atrophy
Spine condition
Job occupation
Sports factors may prioritize one side of the body over the other.
Shifting the Body
When pain presents in one body area, signals are sent to caution the other muscles to contract/tighten as a protective mechanism to prevent further injury. These changes alter movement patterns, leading to muscular imbalances in the glutes and other areas. Individuals who do not rehabilitate from an injury properly can be left with an imbalance.
Chiropractic Relief and Restoration
This condition needs to be addressed to prevent further injuries and issues with posture. Treatment varies depending on the individual and the extent of the problem. A treatment plan to prevent and improve some forms of glute imbalance may include the following.
Spinal decompression will stretch out the body and muscles to a workable position.
Therapeutic massage will relax the muscles and increase blood flow.
Chiropractic adjustments to realign the spine and body.
Targeted stretches and exercises will be provided to maintain alignment.
Unilateral training or training one side of the body at a time can help build and strengthen the weaker side.
Core strengthening can work out the differences on both sides of the body.
Chiropractic Approach for Pain Relief
References
Bini, Rodrigo Rico, and Alice Flores Bini. “Comparison of linea alba length and core-muscles engagement during core and lower back orientated exercises.” Journal of Bodywork and movement therapies vol. 28 (2021): 131-137. doi:10.1016/j.jbmt.2021.07.006
Buckthorpe, Matthew, et al. “ASSESSING AND TREATING GLUTEUS MAXIMUS WEAKNESS – A CLINICAL COMMENTARY.” International Journal of sports physical therapy vol. 14,4 (2019): 655-669.
Elzanie A, Borger J. Anatomy, Bony Pelvis and Lower Limb, Gluteus Maximus Muscle. [Updated 2023 Apr 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538193/
Liu R, Wen X, Tong Z, Wang K, Wang C. Changes of gluteus medius muscle in the adult patients with unilateral developmental hip dysplasia. BMC Musculoskelet Disord. 2012;13(1):101. doi:10.1186/1471-2474-13-101
Lin CI, Khajooei M, Engel T, et al. The effect of chronic ankle instability on muscle activations in lower extremities. Li Y, ed. PLoS ONE. 2021;16(2):e0247581. doi:10.1371/journal.pone.0247581
Pool-Goudzwaard, A. L. et al. “Insufficient lumbopelvic stability: a clinical, anatomical and biomechanical approach to ‘a-specific’ low back pain.” Manual therapy vol. 3,1 (1998): 12-20. doi:10.1054/math.1998.0311
Vazirian, Milad, et al. “Lumbopelvic rhythm during trunk motion in the sagittal plane: A review of the kinematic measurement methods and characterization approaches.” Physical Therapy and Rehabilitation vol. 3 (2016): 5. doi:10.7243/2055-2386-3-5
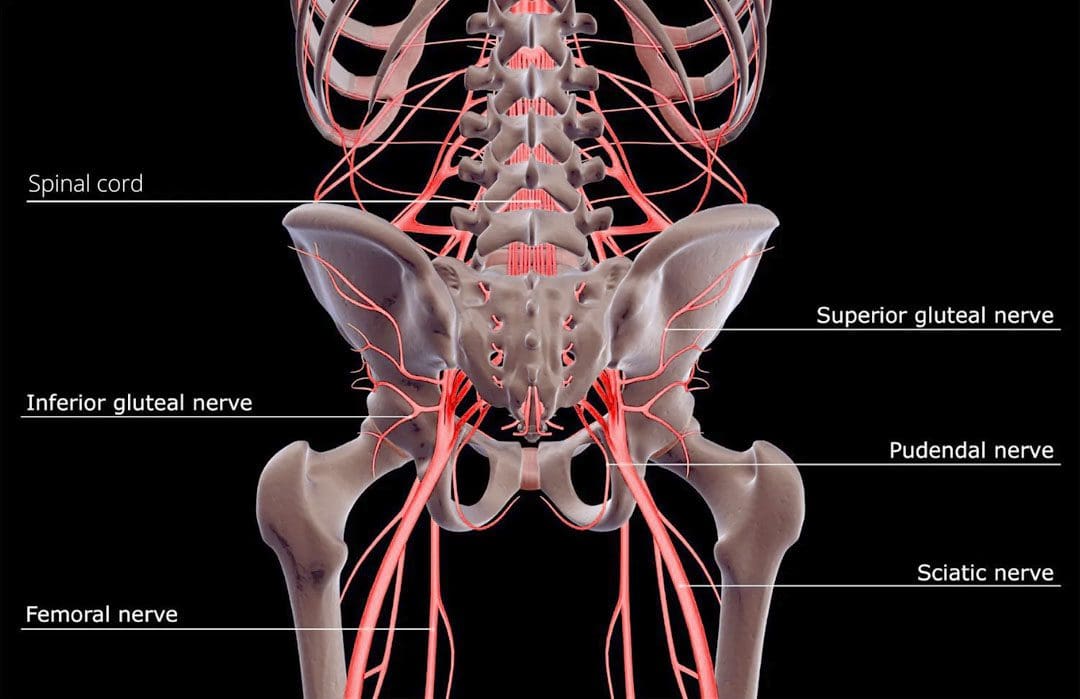
The nervous system communicates with the entire body and reacts to internal and external changes using electrical and chemical impulses to send and receive messages. Messages travel/synapse from one neuron to another using specialized chemicals known as neurotransmitters. Paresthesia refers to sensations of numbness, tingling, prickling, skin crawling, itching, or burning, usually in the arms, hands, legs, and/or feet, but can affect other areas of the body. Chiropractic care, massage therapy, decompression therapy, and functional medicine can relieve tissue and nerve compression, improve flexibility, range of motion, and mobility, and strengthen the muscles surrounding the affected nerve to maintain optimal health and prevent worsening or further injury.
Paresthesia
The sensation comes on without warning and is usually painless and described as tingling or numbness. There are different causes of paresthesia, including:
Some individuals have chronic or long-term paresthesia, which can be a sign of a more serious nerve injury or condition. Added physical stress can cause surrounding tissues to irritate or entangle the nerve leading to building pressure. This pressure causes paresthesia in the area interrupting circulation and function. A pinched nerve can happen anywhere in the body, like the neck, shoulder, wrist, back, and face.
A herniated disc in the lower spine can cause back pain and paresthesia in the leg or foot on the affected side.
Carpal tunnel syndrome is a pinched nerve in the wrist that causes numbness and tingling in the hand and fingers.
Pinched nerve symptoms can be intermittent or constant.
Usually, a temporary sensation is caused when pressure is placed on the affected nerve.
Once that pressure is relieved, the discomfort goes away.
Individuals with an Increased Risk
Overuse Injury
Individuals with jobs or hobbies requiring repetitive motions are at a higher risk for nerve compression, paresthesia, or injury.
Anyone can get a pinched nerve, and most individuals will experience paresthesia at some point.
Weight and water gain can cause swelling and increase pressure on nerves.
Thyroid Disease
This puts individuals at risk for carpal tunnel syndrome.
Rheumatoid arthritis
This causes inflammation, which can also compress nerves in the joints.
Diagnosis
To diagnose paresthesis, a doctor will look at the individual’s medical history and ask questions about the symptoms. They will perform a physical examination and, depending on the findings, may recommend tests that can include:
Nerve Conduction Study
This measures how fast nerve impulses travel in the muscles.
Electromyography – EMG
To look at the electrical activity of how nerves and muscles interact.
Magnetic Resonance Imaging – MRI
This looks at the different areas of the body in high definition.
Ultrasound
Used to produce images, this can be applied to the smaller areas to look for nerve compression or damage.
Chiropractic
Treatment options depend on the cause of the paresthesia. Body misalignments can cause nerve interference that can lead to health problems such as migraines, or can disrupt nerve communication and block proper circulation. Chiropractic care focuses on treating the nervous system and is a safe and effective method for treating nerve problems that cause discomfort and sensations. After a thorough examination of problem areas, massage, decompression, and chiropractic adjustments will:
Bova, Joseph, and Adam Sergent. “Chiropractic management of a 24-year-old woman with idiopathic, intermittent right-sided hemiparesthesia.” Journal of chiropractic medicine vol. 13,4 (2014): 282-6. doi:10.1016/j.jcm.2014.08.002
Christensen, Kim D, and Kirsten Buswell. “Chiropractic outcomes for managing radiculopathy in a hospital setting: a retrospective review of 162 patients.” Journal of chiropractic medicine vol. 7,3 (2008): 115-25. doi:10.1016/j.jcm.2008.05.001
Freihofer, H P Jr. “Parästhesien” [Paresthesia]. Schweizerische Monatsschrift fur Zahnheilkunde = Revue mensuelle suisse d’odonto-stomatologie vol. 89,2 (1979): 124-5.
Karne, Sampada Swapneel, and Nilima Sudhakar Bhalerao. “Carpal Tunnel Syndrome in Hypothyroidism.” Journal of Clinical and diagnostic research: JCDR vol. 10,2 (2016): OC36-8. doi:10.7860/JCDR/2016/16464.7316
A big part of sports is avoiding and preventing injuries, as injury prevention is far better than rehabilitation and recovery. This is where prehabilitation comes in. Prehabilitation is a personalized, constantly evolving, and developing strengthening exercise program. The program aims to provide sports-specific targeted exercises and activities to maintain athletes’ physical abilities and mental preparedness for their sport. The first step is for an athletic trainer, sports chiropractor, and physical therapist to examine the individual.
Prehabilitation
Everybody is different when it comes to developing an effective prehabilitation program. Every individual’s program should be progressive and re-evaluated to adapt and adjust to the athlete’s needs. The first step is learning to prevent injuries and following basic injury prevention protocols. Knowing what to do when the body sustains an injury, like home treatment and when it’s time to see a doctor.
Athletes
Athletes of all levels are recommended to incorporate a prehabilitation program into their training. As athletes engage in their sport, their bodies adjust to the physical demands of practicing, playing, and training. Imbalances can happen naturally with normal activity but become more pronounced with each practice, game, and training session and often are the cause of injury. The repetitive movements and regular stresses can cause neuromusculoskeletal symptoms to present. This includes:
Tightness of muscle groups.
Pain and discomfort symptoms.
Stabilization issues.
Strength imbalances.
Program
A chiropractic therapist will measure the individual’s range of motion and strength, biomechanics, evaluate medical history, and present health status. Individuals with an injury or a condition can also benefit from prehabilitation.
Each program is personalized and will address total body balance, sports-specific needs, and weaknesses.
The exercises will balance strength, coordination, range of motion, and stabilization.
The premise is looking at and comparing movements from left to right, front to back, and upper to lower body.
Activities can be subtle, focused exercises or a complex movement sequence to stabilize or improve a specific skill.
Programs focus on strengthening and stabilizing the core, abdominals, hips, and back.
Instability is common and often presents from a lack of core training, as athletes tend to focus on what parts of the body their specific sport utilizes, leaving the core without a regular training routine.
A prehabilitation program has to be constantly updated to adjust to the individual’s progress.
Tools like foam rollers, balance boards, weights, and exercise balls are used.
Training
Prehabilitation should start before any acute or chronic injury occurs, but often it takes a few injuries for individuals to decide to get into a prehabilitation program. Depending on an athlete’s training cycle, prehabilitation can be incorporated into practice or as an independent workout and become part of an athlete’s training routine. A session can include the following:
Warm-up and cool-down exercises.
Exercises to perform while resting or waiting during practice.
A targeted workout on specific weaknesses.
A complete workout for days off or active rest days.
Mini workouts for when traveling and recovery days.
For athletes, feeling challenged and motivated can be the difference between success and failure. Working with a trainer, sports chiropractor, and therapists who know sports, understand athletic needs, and communicate well, will contribute to a successful prehabilitation program.
Improving Athletic Performance
References
Durrand, James et al. “Prehabilitation.” Clinical medicine (London, England) vol. 19,6 (2019): 458-464. doi:10.7861/clinmed.2019-0257
Giesche, Florian, et al. “Evidence for the effects of prehabilitation before ACL-reconstruction on return to sport-related and self-reported knee function: A systematic review.” PloS one vol. 15,10 e0240192. 28 Oct. 2020, doi:10.1371/journal.pone.0240192
Halloway S, Buchholz SW, Wilbur J, Schoeny ME. Prehabilitation Interventions for Older Adults: An Integrative Review. Western Journal of Nursing Research. 2015;37(1):103-123. doi:10.1177/0193945914551006
Smith-Ryan, Abbie E et al. “Nutritional Considerations and Strategies to Facilitate Injury Recovery and Rehabilitation.” Journal of athletic training vol. 55,9 (2020): 918-930. doi:10.4085/1062-6050-550-19
Vincent, Heather K, and Kevin R Vincent. “Rehabilitation and Prehabilitation for Upper Extremity in Throwing Sports: Emphasis on Lacrosse.” Current sports medicine reports vol. 18,6 (2019): 229-238. doi:10.1249/JSR.0000000000000606
Vincent, Heather K et al. “Injury Prevention, Safe Training Techniques, Rehabilitation, and Return to Sport in Trail Runners.” Arthroscopy, sports medicine, and rehabilitation vol. 4,1 e151-e162. 28 Jan. 2022, doi:10.1016/j.asmr.2021.09.032
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine