The iliacus muscle is a triangle-shaped muscle in the pelvic bone that flexes and rotates the thigh bone. It works with the other muscles in the hip and thigh to help bend, run, walk, sit, and maintain correct posture. Injuries and common medical conditions can affect its function, causing pain and stiffness. Can physical therapy help?
The Iliacus Muscle
The iliacus is one of the body’s most important hip flexor muscles. The iliacus and surrounding muscles work together to produce the stability and range of motion required for bending, dancing, sitting, and walking.
Anatomy
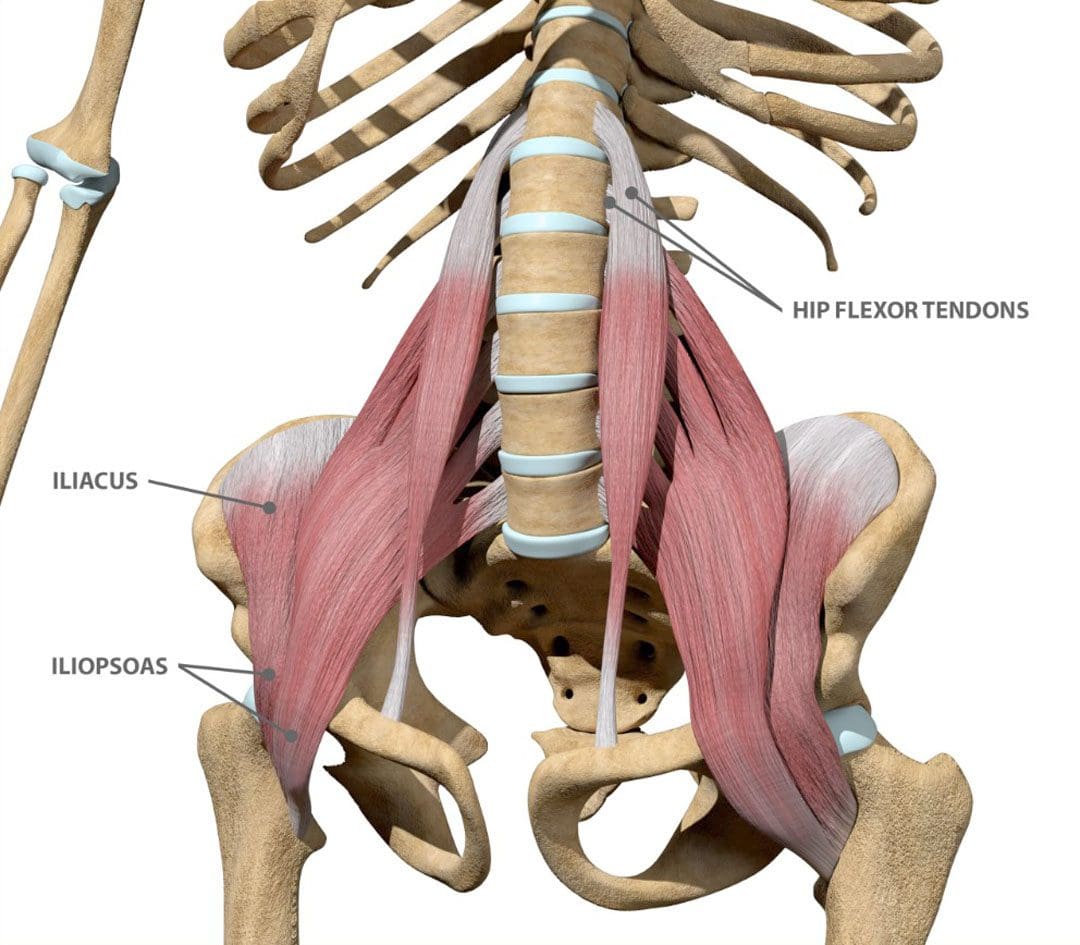
The iliacus muscle is part of a complex muscle system in the hip and pelvis. Two iliacus muscles on each side of the pelvic bone enable the thigh to flex and rotate. They are innervated by the femoral nerve, which provides movement and sensation to the lower limbs. (Bordoni B. and Varacallo M. 2023) The iliacus muscle sits on the wing-shaped ilium and fits into the curved surface of the ilium, called the iliac fossa. The top of the muscle is attached to the upper wings of the ilium or iliac crest. It extends past the hip joint, which connects to the upper thigh bone/femur at the lesser trochanter protrusion. The iliacus is part of a major trio of muscles called the iliopsoas, including the major psoas and minor psoas muscles. These muscles are also attached to the upper femur but extend upward, connecting to the lumbar/lower spine at several attachment points. The iliopsoas also interact with the quadratus lumborum muscle, the deepest muscle of the lower back that starts at the iliac crest and attaches to the lumbar spine at several points. The quadratus lumborum enables flexion and elevation of the spine, while the iliopsoas enable the flexion and rotation of the hip and thigh.
Functions
The iliacus muscle has many functions that include: (Physiopedia, 2024)
Flexing and rotating the femur.
Helps maintain proper body posture while standing and sitting.
Produces hip movement that enables walking, running, and climbing stairs.
Provides hip flexion – bringing the knee to the chest.
Enables the forward tilt of the pelvis and side-bending.
Conditions
Several conditions can affect the iliacus muscle, specifically from under and/or overuse injuries. These conditions, collectively known as Iliopsoas syndrome, are typically the result of overuse/repetitive strain or injuries. These include:
Iliopsoas tendinopathy – which affects tendons.
Iliopsoas bursitis – which affects cushioning sacs known as bursae.
Iliopsoas syndrome can affect anyone but is common in:
Individuals and athletes who repeatedly use movements that flex the hips.
Track-and-field athletes
Gymnasts
Dancers
Iliopsoas Bursitis
This is the inflammation of the cushioning sac or bursa under the iliacus muscle, which helps the muscle slide over the pelvic bone. Symptoms can range from mild discomfort to pain that radiates through parts of the leg and hips. Runners, skiers, and swimmers are commonly affected, and individuals who regularly have tight hips and individuals with different forms of arthritis can also be affected. Early treatment can prevent the symptoms from worsening. Mild cases can be treated with self-care and stretching to help relieve tightness, rest, ice application, and over-the-counter nonsteroidal anti-inflammatory drugs. In severe cases, treatment options that may be recommended include: (Physiopedia, 2024)
Physical therapy
Assistant walking devices to relieve pressure – for example, a cane.
Corticosteroid steroid injections
Prescription anti-inflammatory medications
Iliopsoas Tendinopathy
Another condition affecting the iliacus muscles is iliopsoas tendinopathy, sometimes called snapping hip syndrome, because individuals can hear an audible snapping sound (Davenport KL. 2019). The condition is often experienced by dancers who repeatedly flex and hyperextend their hips and can result in hip and groin pain that gets worse with kicking or rotation. Treatment of iliopsoas tendinopathy can include:
Retraining muscle imbalances with strengthening and stretching exercises.
If these fail to provide relief, corticosteroid injections may be used. A saline hydro dissection can relieve stress around the tendon by injecting fluids that cushion and release trapped tissues.
Tendon release surgery may be recommended when all other options have failed. The surgical release involves severing the tendon to reduce pain and improve the range of motion.
Rehabilitation
Core muscle strengthening is essential to the rehabilitation of iliacus muscle injuries. The iliopsoas is an integral component of the core group and can benefit from stretching and strengthening exercises (Yogateket, 2019)
Lunge stretches
Straight leg raises
Knee-to-chest stretches
Standing hip flexion with resistance bands
Certain yoga poses can also help and include variations on the bridge pose that encourage hip flexion. (Yoga International, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
Iliopsoas pain is often felt at the front of the hips, thigh, mid-back, and lower back. Chiropractic care can help with iliacus muscle injuries through:
Evaluation
A chiropractor can evaluate the condition and determine if the iliacus muscle is causing pain.
Treatment plan
A chiropractor can create a personalized treatment plan that may include exercise instructions, manipulation, and other therapies.
Rehabilitation
A chiropractor can create a rehabilitation program to expedite healing.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Hip Labral Tear and Chiropractic Care
References
Bordoni, B., & Varacallo, M. (2024). Anatomy, Bony Pelvis, and Lower Limb, Iliopsoas Muscle. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30285403
Davenport KL. (2019). The professional dancer’s hip. Performing Arts Medicine, 77-87. https://doi.org/https://doi.org/10.1016/B978-0-323-58182-0.00009-2
Yogateket. Lizette Pompa. (2019). Essential yoga body parts. Hip flexor/psoas and yoga. Yogateket. https://www.yogateket.com/blog/hip-flexor-psoas-and-yoga
For individuals who may need to take pain medications to manage an injury or condition, can knowing the potential side effects help in treatment?
Medications For Pain Side Effects
Over-the-counter and prescription pain medications can help relieve physical discomfort and distress but can also cause side effects. Patients may not manifest side effects when using certain meds or experience mild, limited, severe, or intolerable effects. Pain medication side effects can include:
Allergic reactions
Upset stomach
Bruising
Dizziness
However, medication side effects don’t affect everyone in the same way.
Pain Relief
The patient and their healthcare provider can decide whether they risk developing side effects and which effects they are more predisposed to. Individuals may be susceptible to side effects from certain medications but are likely to tolerate others. For example, individuals with a history of ulcers may be recommended to avoid anti-inflammatories. For those who have trouble sleeping, it is recommended to avoid pain meds that are known to interfere with sleep.
Reading Labels and Asking Questions
When taking over-the-counter medications, read the label for side effects, then weigh the possible risks against the medicine’s benefits for pain relief. Ask a pharmacist or healthcare provider about anything that is not understood. Some side effects are medical emergencies, such as allergic reactions. Recognizing the signs of an allergic reaction and being prepared to call for emergency help if symptoms present. (American Academy of Allergy, Asthma & Immunology, 2024) These can include:
Itching
Hives
Rash
Mouth or facial swelling
Shortness of breath
If a healthcare provider prescribes medication, discuss the anticipated risks and benefits. The prescription will come with a label that lists the side effects associated with the drug.
Opioid Risks
Opioids are powerful prescription meds, usually used for severe, short-term use, like post-surgery pain or after a severe traumatic injury. Some effects of opioids include: (Plein L. M. and Rittner H. L. 2018) Common side effects include sedation, constipation, and nausea. Chronic use can lead to depression and/or sexual dysfunction. With narcotics, there is the risk of addiction that can change an individual’s life, as addiction can be difficult to overcome. One of the reasons the CDC published a guideline on opioid prescriptions was because of the number of overdoses and deaths.
The CDC recommends that practitioners not prescribe opioids as a first-line treatment for chronic back pain.
The CDC recommends that healthcare providers initially treat patients with chronic back or neck pain using non-pharmacological therapies or medications other than opioids.
Opioids should only be used if the expected benefits for pain and function are anticipated to outweigh the risks to the patient.
With more than half of regular opioid users experiencing back pain, they aren’t proven to help return individuals to work or normal life faster, nor did they improve functioning when used for the treatment of an acute episode. (Deyo R. A. Von Korff M. and Duhrkoop D. 2015) The effectiveness of opioids is about 30% for short-term relief and did not improve physical functioning.
Examples and Comparisons
Examples of common medications used to treat back pain.
Advil
Active Ingredient – Ibuprofen
Drug Class – NSAID
Over-the-counter or Prescribed – Available over-the-counter
Side Effects – GI-related symptoms and Reye’s Syndrome in children
Aleve and Other Generic Brands
Active Ingredient – Naproxen
Drug Class – NSAID
Over-the-counter or Prescribed – Available as both depending on strength.
Side Effects – GI-related symptoms, headaches
Tylenol and Other Generic Brands
Active Ingredient – Acetaminophen
Drug Class Analgesic – pain reliever
Over-the-counter or Prescribed – Available as both and can be prescribed with codeine.
Side Effects – Potential liver damage
Lyrica
Active Ingredient – Pregabalin
Drug Class – Anticonvulsant
Over-the-counter or Prescribed – Prescribed FDA-approved for shingles pain and neuropathy in diabetes. Other uses off-label.
Side Effects – Dizziness, drowsiness, swelling, weight gain.
Neurontin
Active Ingredient – Gabapentin
Drug Class – Anticonvulsant
Over-the-counter or Prescribed – Prescribed FDA-approved for shingles pain
Side Effects – Dizziness, drowsiness, allergic reaction, withdrawal, and seizures.
Injury Medical Chiropractic and Functional Medicine Clinic
Chiropractic therapy is among the more conservative treatment options and may be tried first. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself.
Chronic Body Pain Recovery
References
American Academy of Allergy, Asthma & Immunology. (2024). Anaphylaxis Symptoms & Diagnosis. https://www.aaaai.org/conditions-treatments/allergies/anaphylaxis
Plein, L. M., & Rittner, H. L. (2018). Opioids and the immune system – friend or foe. British journal of pharmacology, 175(14), 2717–2725. https://doi.org/10.1111/bph.13750
Deyo, R. A., Von Korff, M., & Duhrkoop, D. (2015). Opioids for low back pain. BMJ (Clinical research ed.), 350, g6380. https://doi.org/10.1136/bmj.g6380
Are there blood tests for individuals with chronic and severe back pain symptoms that can help healthcare providers diagnose?
Blood Tests To Help Diagnose Back Pain
If a healthcare provider suspects an infection or inflammatory arthritis is the cause of back pain, blood tests may be used to diagnose. When trying to find the cause of back pain, a healthcare provider will examine the patient’s medical history, perform a physical examination, and, if necessary, order diagnostic tests. (Dansie E. J. and Turk D. C. 2013) For example, the National Institute of Arthritis and Musculoskeletal and Skin Diseases says that MRIs can reveal abnormalities in the spine. Still, a person may not feel pain or experience any other symptoms. The NIAMS also says healthy, pain-free individuals can have elevated SED levels. A high sedimentation rate or sed rate, also known as an erythrocyte sedimentation rate (ESR) test, can indicate inflammation in the body. (National Institute of Arthritis and Musculoskeletal and Skin Diseases, 2023)
Commonly Used Tests
Blood tests that can help diagnose back pain include:
Complete Blood Count – CBC
This test can indicate inflammation or infections.
Sed Rate or Erythrocyte Sedimentation Rate
This test measures inflammation by analyzing how red blood cells settle through plasma.
If the SED rate indicates that inflammation is present, the possibility of an underlying cause may be some form of arthritis or a tumor, which is rare.
A genetic marker in the blood that is more common in individuals with ankylosing spondylitis and reactive arthritis. (McMichael A. and Bowness P. 2002)
This marker may be tested if the healthcare provider suspects either disease.
Ankylosing spondylitis is an inflammatory arthritis affecting the sacroiliac joints, hips, and spine. (Sieper J. et al., 2002)
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you to relieve pain and restore function. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. Our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, severe sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness and nutrition, Functional Medicine Treatments, and in-scope care protocols. They can also work with other associated medical professionals to develop a personalized treatment plan to help relieve muscle pain, improve the body’s flexibility and mobility, resolve musculoskeletal issues, and prevent future pain symptoms from reoccurring.
Integrative Medicine Approach
References
Dansie, E. J., & Turk, D. C. (2013). Assessment of patients with chronic pain. British journal of anaesthesia, 111(1), 19–25. https://doi.org/10.1093/bja/aet124
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Back Pain. Retrieved from https://www.niams.nih.gov/health-topics/back-pain
Harrison M. (2015). Erythrocyte sedimentation rate and C-reactive protein. Australian prescriber, 38(3), 93–94. https://doi.org/10.18773/austprescr.2015.034
Sproston, N. R., & Ashworth, J. J. (2018). Role of C-Reactive Protein at Sites of Inflammation and Infection. Frontiers in immunology, 9, 754. https://doi.org/10.3389/fimmu.2018.00754
McMichael, A., & Bowness, P. (2002). HLA-B27: natural function and pathogenic role in spondyloarthritis. Arthritis research, 4 Suppl 3(Suppl 3), S153–S158. https://doi.org/10.1186/ar571
Sieper, J., Braun, J., Rudwaleit, M., Boonen, A., & Zink, A. (2002). Ankylosing spondylitis: an overview. Annals of the rheumatic diseases, 61 Suppl 3(Suppl 3), iii8–iii18. https://doi.org/10.1136/ard.61.suppl_3.iii8
Hamdulay, S. S., Glynne, S. J., & Keat, A. (2006). When is arthritis reactive?. Postgraduate medical journal, 82(969), 446–453. https://doi.org/10.1136/pgmj.2005.044057
Can healthcare professionals implement H.E.A.R.T. protocols for trafficked individuals while providing a safe space?
Introduction
Across the world, many local media and organizations are paying close attention to a phenomenon that many people should be aware of. This phenomenon is known as trafficking, and it can be associated with numerous activities, from forced labor to sex labor, and can affect a person’s sense of self-worth. While many people will correlate that trafficking affects many women and children, it can affect many individuals regardless of age, gender, and background. While many survivors of trafficking are dealing with the psychological and physical injuries that they obtain from their traffickers, many medical professionals can implement protocols and roles through the implementation of H.E.A.R.T. to provide a safe space for individuals suffering from trafficking. Today’s article focuses on the definition of trafficking, what H.E.A.R.T. is, and how it is used in a clinical setting. We discuss with certified associated medical providers who consolidate our patients’ information to assess and identify trafficking in a clinical approach while providing a safe space. We also inform and guide patients while asking their associated medical provider intricate questions to formulate customized treatment plans for their pain and provide them with a safe space and positive experience. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Definition Of Trafficking
When it comes to defining trafficking, it can be challenging as it is frequently associated with other issues. However, the main definition for trafficking is “recruiting, transporting, transferring, or harboring many individuals or a person that are threatened or forced to achieve the consent of a person having control of the individuals for exploitation.” With human trafficking being a pressing public concern that affects all races, social classes, demographics, and genders, it can impact society and the individual who is being trafficked. (Toney-Butler et al., 2024) Additionally, many people often mistake trafficking and smuggling as they are completely different. Smuggling requires a person to be transported into a nation through voluntary illicit means. While trafficking can come in two forms, which are labor and commercial sex, it can happen within the person’s own home. (Rambhatla et al., 2021) This is because many survivors who are going to get healthcare services will feel various emotions of fear or shame that can prevent them from asking for help due to what they have been through with their trafficker. However, when many individuals who are trafficking survivors are suffering from significant physical, mental, and social health problems and are seeking healthcare services, many healthcare professionals play an important role by creating a safe and responsive space for them. (The Lancet Regional Health-Western, 2022)
Beyond the Surface: Understanding the Effects of Personal Injury- Video
What is H.E.A.R.T In A Clinical Setting
When it comes to creating a safe and positive space in a clinical setting, many healthcare professionals often miss the signs of trafficking due to a lack of training or confidence to identify and treat patients who are trafficking victims. (Lee et al., 2021) However, healthcare protocols should be implemented, and H.E.A.R.T. should be incorporated into a clinical approach to assess and develop a customized treatment plan for the patient. Healthcare professionals can engage with the patient in a one-on-one discussion away from their trafficker and can offer important medical and psychological care resources. (Exeni McAmis et al., 2022) By incorporating H.E.A.R.T. protocols in a healthcare clinic, many doctors and medical professionals can help many patients be in a safe environment. Below is what H.E.A.R.T. stands for.
H-Hearing
The “H” in H.E.A.R.T. is for hearing as many medical professionals not only to hear but to see what is going on in the clinic and to establish environmental awareness. This is due to looking at the patient and who is accompanied by them. With healthcare providers being at the front, they interact with patients and may not know what health concerns are affecting them. This could be due to the following:
By incorporating the hearing aspect in H.E.A.R.T., many healthcare professionals can provide a safe, thoughtful, and engaging approach to the patient and know what to look for when a patient is coming in for treatment.
E-Evaluating
The “E“ in H.E.A.R.T. is used to evaluate its importance in enhancing patient interactions in a trauma-informed care facility. This is highly important because the individual is seeking health care. For the patients being trafficked, it is important to notice the red flags the individual is experiencing. Some of the red flags that many healthcare providers should look for are:
Physical health
Behavioral Health
The patient is with a controlling person
The patient does not have possession of their I.D.
Additionally, it is always important to show compassion, be sensitive to the individual while addressing their needs and concerns, and use a non-judgmental approach during the interview process. This helps the individual ensure they are in a safe environment when discussing sensitive topics. At the same time, it is important not to let the patient be re-traumatized while avoiding the impulse to rescue and overpromise the patient to mental health as we want them to have their self-worth. At the same time, it is best to remember the four “Rs“ when doing a trauma-informed approach; they are:
Realize: Understanding how trauma can affect people.
Recognize: Recognizing the signs of trauma.
Respond: Have all staff trained, use evidence-based practices, and provide a safe environment.
Resist Re-trauma: Recognizing how some practices may trigger painful memories while avoiding re-traumatizing the patient.
By implementing the four “Rs“ and the “E“ in H.E.A.R.T., many healthcare professionals can provide valuable resources to trafficking survivors with a strong support system.
A-Activating
The “A“ in H.E.A.R.T. stands for activating, where healthcare professionals must have proper protocols to engage all employees. This allows the healthcare providers to understand how beneficial it is to develop a protocol for a person who is being trafficked, understand their state and federal reporting laws, and list key elements of effective trauma-informed screening procedures when assessing the patient. This allows a foundational structure to support a response for suspected patients who are being trafficked. At the same time, by following HIPAA laws and organization policies, many healthcare providers must explain the reporting process to the right officials. Additionally, the benefits of developing a protocol for trafficking are by:
Clarifying procedures
Enhance staff training
Optimize the interactions with the trafficking patients
Improve staff confidence
Prepare for any threatening situations
Maximizing preparedness to aid trafficking patients
Optimize support for patients
Develop collaborative outside resources
R-Resourcing
The “R“ in H.E.A.R.T. stands for resourcing, as many healthcare providers must identify the referral systems. This allows healthcare professionals to understand the important message to convey when assessing trafficking victims and the importance of responding to safety, emergency, and reporting requirements. When assessing and interviewing the patient, many will have to recognize that their patient may be a possible victim of trafficking, what their immediate needs are, and what long-term resources can help.
T-Training
The “T” in H.E.A.R.T. stands for training, as it is important that many healthcare providers continuously train to spot trafficking; this provides confidence to many healthcare workers and can help save a person’s life. By implementing H.E.A.R.T. protocols, the “T” allows the doctor to respect the individual’s decision to want help, providing a positive support system while encouraging them to come back, offering to help with a safety plan, and building a resource network. This is because if the patient is accompanied by someone who is controlling and answering for the patient, handing out information discreetly can provide a bit of hope to the individual to make the move. At the same time, providing local and immediate assistance resources can help the individual in the long run. This allows healthcare providers to build a trusting relationship and even help individuals to have a safe and positive experience on their health and wellness journey.
References
Exeni McAmis, N. E., Mirabella, A. C., McCarthy, E. M., Cama, C. A., Fogarasi, M. C., Thomas, L. A., Feinn, R. S., & Rivera-Godreau, I. (2022). Assessing healthcare provider knowledge of human trafficking. PLOS ONE, 17(3), e0264338. https://doi.org/10.1371/journal.pone.0264338
Gutfraind, A., Yagci Sokat, K., Muscioni, G., Alahmadi, S., Hudlow, J., Hershow, R., & Norgeot, B. (2023). Victims of human trafficking and exploitation in the healthcare system: a retrospective study using a large multi-state dataset and ICD-10 codes. Front Public Health, 11, 1243413. https://doi.org/10.3389/fpubh.2023.1243413
Lee, H., Geynisman-Tan, J., Hofer, S., Anderson, E., Caravan, S., & Titchen, K. (2021). The Impact of Human Trafficking Training on Healthcare Professionals’ Knowledge and Attitudes. J Med Educ Curric Dev, 8, 23821205211016523. https://doi.org/10.1177/23821205211016523
Rambhatla, R., Jamgochian, M., Ricco, C., Shah, R., Ghani, H., Silence, C., Rao, B., & Kourosh, A. S. (2021). Identification of skin signs in human-trafficking survivors. Int J Womens Dermatol, 7(5Part B), 677-682. https://doi.org/10.1016/j.ijwd.2021.09.011
Individuals who have experienced spinal or back trauma, suffered fractures, are going through spinal degeneration, or are dealing with a spinal condition have an increased risk of anterolisthesis, where a vertebra slips forward relative to the vertebra below it. Can healthcare providers help prevent and treat the condition?
Anterolisthesis
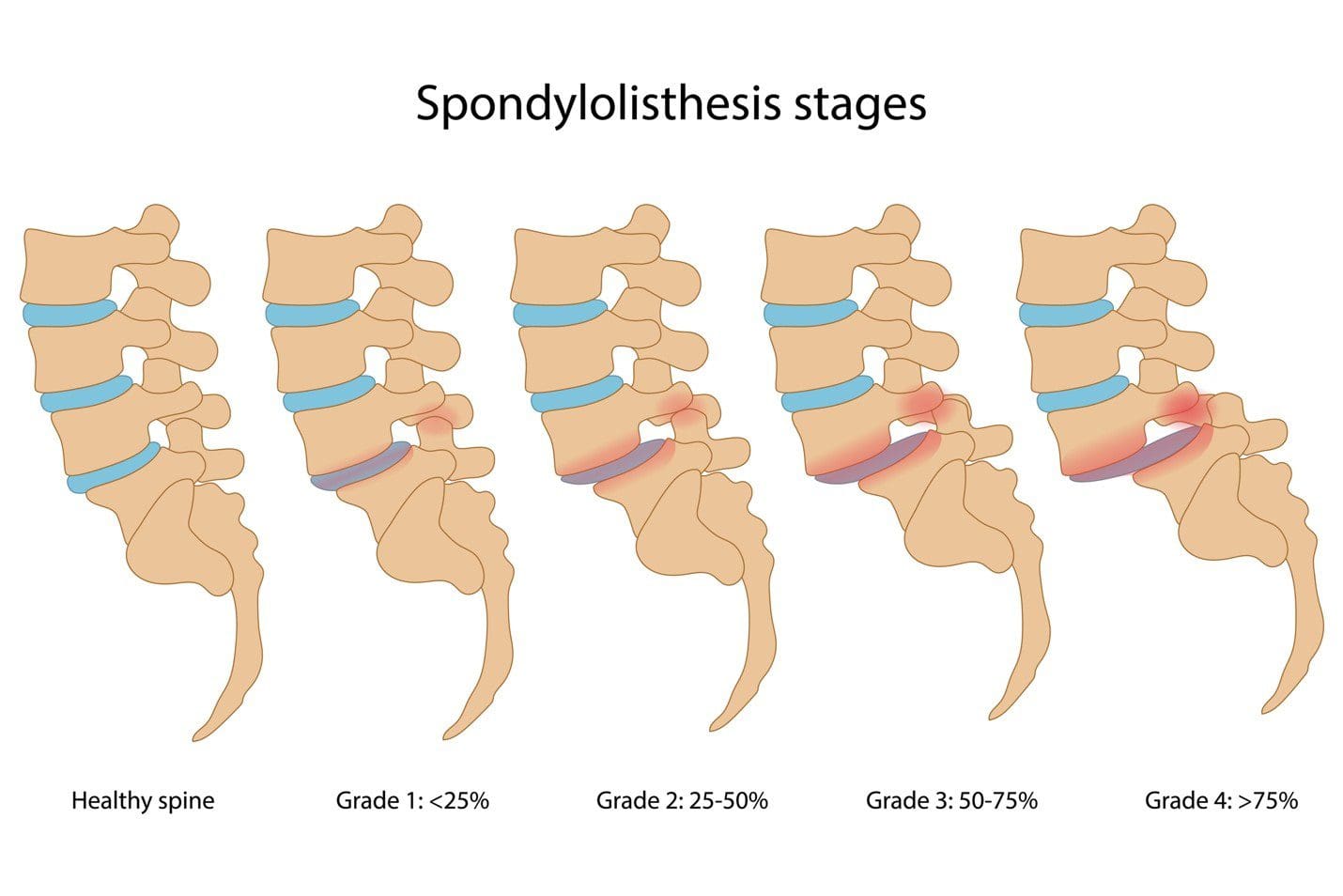
The spine consists of 33 individual bones or vertebrae stacked on one another. Anterolisthesis occurs when one vertebral segment slips forward over another. The condition can be mild, asymptomatic, or cause significant pain and neurological symptoms. Many different things, including osteoarthritis, osteoporosis, trauma, or a fracture, can cause this vertebral shifting. (Cedars Sinai, 2022) Spondylolisthesis is a general term for shifting a spinal vertebra over the one below it. It includes anterolisthesis, forward moving, and the less common retrolisthesis, or backward shifting.
Grades
Anterolisthesis is typically graded using the Meyerding scale, which assigns one of five grades according to how much slippage has occurred. These grades include:
Anterolisthesis can lead to various symptoms, depending on the severity and if the surrounding spinal nerves have been affected. The most common complaints include:
Diagnosis begins with a subjective evaluation and a physical examination. During these, the healthcare provider will assess sensation, strength, and reflexes and will order one of several diagnostic tests, including:
X-rays
Visualizes the vertebrae in the spine and their position relative to those above and below.
Also provides a clear picture of spinal arthritis or disc degeneration.
Magnetic Resonance Imaging – MRI
Allows the spinal cord, nerves, muscles, and discs to be assessed for compression or damage.
Several factors determine how the condition is treated, including:
The grade of the slippage.
The cause.
The symptoms.
The presence of instability on a diagnostic test such as an X-ray.
Stable and mildly symptomatic cases are usually treated with a combination that can involve:
Physical therapy
Activity modification
Bracing
Nonsteroidal anti-inflammatory medications/NSAIDs like ibuprofen.
Spinal injections
In more severe cases in which spinal instability or significant neurological symptoms are present, surgery may be recommended. This commonly involves a spinal decompression or fusion procedure. The technique varies based on the surgeon’s preferences and anatomy. (Koslosky E., and Gendelberg D. 2020)
Prognosis
Most individuals with this condition don’t know they have it until it is found accidentally on an X-ray or an MRI for something else. Mild cases can cause minimal symptoms and can be well-managed with conservative treatments. Cases of unstable anterolisthesis or those with neurological compression often require surgical intervention. These surgeries restore stability to the spine and alleviate any pressure on the nerves. More than 85% of individuals who need surgery have a successful outcome. (American Academy of Orthopaedic Surgeons, 2021)
Self-Care and Management
For individuals experiencing pain, numbness, or tingling from anterolisthesis, getting symptoms evaluated by a healthcare provider is an important first step. The healthcare provider may suggest one of several management strategies, which include:
Core Strengthening
To alleviate symptoms, exercises targeting the core muscles in the hips, pelvis, abdomen, and lower back are recommended.
Formal physical therapy may also be recommended.
Over-the-counter Meds
A healthcare provider may suggest pain-relieving medications like ibuprofen or naproxen to reduce soreness.
Activity Modification
Sticking to gentle, pain-free activities and avoiding excessive or repetitive extension of the spine can help prevent symptom aggravation. (American Academy of Orthopaedic Surgeons, 2021)
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for you to relieve pain and restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Koslosky, E., & Gendelberg, D. (2020). Classification in Brief: The Meyerding Classification System of Spondylolisthesis. Clinical orthopaedics and related research, 478(5), 1125–1130. https://doi.org/10.1097/CORR.0000000000001153
American Academy of Orthopaedic Surgeons. (2021). Adult spondylolisthesis in the low back. https://orthoinfo.aaos.org/en/diseases–conditions/adult-spondylolisthesis-in-the-low-back
Hospital for Special Surgery. (2023). Spondylolisthesis. https://www.hss.edu/condition-list_spondylolisthesis.asp
Can the Oswestry Low Back Pain Disability Questionnaire help assess how low back pain impacts individuals’ ability to perform everyday tasks and activities and help physical therapists incorporate the outcome measure into an effective treatment plan?
Oswestry Disability Questionnaire
The Oswestry Disability Questionnaire, also known as the Oswestry Disability Index, provides objective data about an individual’s lower back pain. It determines the severity of the pain and how much it limits their daily activities. The questionnaire is a validated measure backed by research that can be used to justify the need for medical treatment. It includes questions regarding the symptoms and severity of low back pain and how these symptoms interfere with regular activities. Lower back pain can result from various causes (National Institute of Neurological Disorders and Stroke, 2020)
Arthritis, including inflammatory types of arthritis like psoriatic arthritis and ankylosing spondylitis.
Lumbar vertebrae compression fractures – usually from trauma or osteoporosis.
Low back surgery – including spinal fusions, discectomies, and laminectomies.
Spinal stenosis
Spondylolisthesis
Scoliosis
How The Questionnaire Works
The Oswestry Disability Questionnaire consists of 10 questions about the impact of lower back pain on daily life. The questions are divided into the following categories: (American Academy of Orthopedic Surgeons, N.D.)
Pain Intensity
How intense is the pain?
If painkillers are used, how much symptom relief do they provide?
Personal Care
Can the patient perform self-care activities like bathing and dressing when experiencing significant pain or limitations?
Whether physical assistance from another person is needed?
Lifting
Can the patient lift objects like weights with or without pain?
Can lifting be performed from the floor or a higher surface like a table if the objects are light, moderate, or heavy?
Walking
If and to what extent does the pain limit the patient’s walking distance and independence?
If an assistive device like a cane or crutches are needed?
Sitting
If so, how much pain limits the patient’s sitting tolerance?
Standing
If so, how much pain limits the patient’s standing tolerance?
Sleeping
If so, how much pain limits a patient’s sleeping duration?
Whether pain medication is needed to help the patient sleep comfortably?
Social Life
If and to what extent a patient’s social activities are limited because of pain symptoms?
Traveling
If so, to what extent does pain limit a patient’s ability to travel?
Employment and/or Homemaking Duties
Does pain limit a patient’s ability to perform job-related and/or household activities, including physically demanding and light duties?
Patients self-report the information and complete it on their own based on their understanding of the extent of their lower back pain and disability.
Each question can be scored between 0 and 5, with 0 indicating no limitations and 5 indicating complete disability.
The scores from all the questions are added together for a cumulative total score of 50 points.
Scores
The Oswestry Disability Questionnaire assesses how much a patient’s lower back pain limits daily activities. This information is used in clinical documentation for medical services. A higher score indicates a greater level of disability, according to the following scoring criteria:
0–4: No disability
5–14: Mild disability
15–24: Moderate disability
25–34: Severe disability
35–50: Completely disabled
Physical therapists must create individualized goals for each patient to develop a treatment plan and receive authorization from insurance companies. One of the most important aspects of a physical therapy goal is that it must be measurable. The Oswestry Disability Questionnaire provides a numerical score to track functional limitations and monitor the range of motion and strength testing. A baseline measurement is taken at the beginning of treatment, and progress is tracked in follow-up visits. A new score is used as a treatment goal. According to a study, the minimal clinically important difference (MCID) for the Oswestry Disability Questionnaire is 12.88. The MCID is the minimum score healthcare providers need to confirm a patient’s progress in function due to treatment. (Johnsen, L. G. et al., 2013)
By tracking changes in the total score before, during, and after treatment, healthcare providers can better assess whether treatment improves symptoms. A decrease in total score by 13 points or more would indicate that treatment is helping to improve a patient’s lower back pain and level of disability. Along with physical examination results, the patient’s score and the severity of symptoms can help healthcare providers determine an appropriate treatment plan.
No Disability
Treatment is unnecessary other than providing advice for lifting mechanics and general physical activity to maintain health.
Mild Disability
Conservative measures, such as physical therapy, exercise, hot or cold therapy, pain medication, and rest, are needed to help alleviate symptoms.
Moderate Disability
More aggressive intervention is needed, which can include extensive physical therapy services and pain management.
Severe Disability
Significant medical intervention is needed, including surgery, pain management, equipment like wheelchairs, and help from a caretaker.
Completely Disabled
Patients are either bedbound or have worsening symptoms, and a caretaker is needed to complete daily activities and self-care tasks.
Injury Medical Chiropractic and Functional Medicine Clinic
Improvements in range of motion, strength, and quality of movement and a decrease in total score can help show the treatment’s positive impact in managing lower back pain. A thorough medical exam and diagnostic tests, such as X-ray, MRI, or EMG, can help determine the underlying causes, discover the cause of the problem, and develop an effective treatment plan. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. Using an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility and help individuals return to normal activities. Our providers use Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers.
Optimizing Your Wellness
References
National Institute of Neurological Disorders and Stroke. (2020). Low Back Pain Fact Sheet. Retrieved from https://www.ninds.nih.gov/sites/default/files/migrate-documents/low_back_pain_20-ns-5161_march_2020_508c.pdf
American Academy of Orthopedic Surgeons. (N.D.). Oswestry Low Back Pain Disability Questionnaire. https://www.aaos.org/globalassets/quality-and-practice-resources/patient-reported-outcome-measures/spine/oswestry-2.pdf
Johnsen, L. G., Hellum, C., Nygaard, O. P., Storheim, K., Brox, J. I., Rossvoll, I., Leivseth, G., & Grotle, M. (2013). Comparison of the SF6D, the EQ5D, and the oswestry disability index in patients with chronic low back pain and degenerative disc disease. BMC musculoskeletal disorders, 14, 148. https://doi.org/10.1186/1471-2474-14-148
Back pain is one of the most common reasons for seeking health care. Individuals dealing with back pain but don’t know the cause may have some inflammatory joint disease or autoimmune condition. Can seeing a rheumatologist help?
Rheumatologist
Depending on what’s causing the back pain, individuals may need to see their primary doctor for a referral. Individuals are recommended to see a rheumatologist if they have back pain that doesn’t come from an injury that doesn’t go away after a few weeks, pain that comes back after treatment, or symptoms that suggest a rheumatic condition. Rheumatologists treat severe or persistent back pain and are experts in autoimmune diseases, including lupus, Sjogren’s syndrome, rheumatoid arthritis, ankylosing spondylitis, axial spondylitis, Psoriatic arthritis, and other forms of inflammatory or autoimmune arthritis.
What Do They Do?
A rheumatologist is an internist or pediatrician who has completed special training in treating conditions that are:
Inflammatory
Autoimmune
Related to painful joint disease
The doctors diagnose, treat, and manage these conditions long-term. Depending on diagnosis and care needs, they may also lead or be part of a team that includes other healthcare providers.
Symptoms
When muscles ache, pain presents, or joints hurt, and especially if there are signs of inflammation that don’t go away, seeing a healthcare provider is recommended. Symptoms of inflammation include:
Redness
Swelling
Pain
Stiffness
Loss of joint function
Usually, to see a rheumatologist, individuals need a referral from their primary care provider and may be referred when:
There is no evidence of a back injury.
At-home therapies like heat application, prescription medications, or physical therapy are unsuccessful.
There is uncertainty about what’s causing the back pain, but I suspect it’s rheumatological.
Blood tests for inflammatory markers or certain antibodies yield abnormal results.
There is a diagnosis of a rheumatic condition and recommend a specialist to manage it.
There is a family history of a rheumatic or autoimmune condition that may cause back pain.
Some types of arthritis can cause permanent, progressive joint damage.
Conditions
Conditions that can affect the spine and cause back pain and are treated by a rheumatologist include: (Johns Hopkins Medicine, 2024)
Rheumatoid arthritis (RA)
This often starts in smaller joints of the hands and feet and later moves to the neck and/or back.
It can also affect different body organs and have systemic symptoms.
Ankylosing Spondylitis (AS)
Primarily a disease of the spine, it may also impact the shoulders, hips, knees, and ankles.
Systemic symptoms, including fever and fatigue, can manifest.
Axial Spondylitis
This primarily affects the spine, chest, and pelvis.
It may also cause problems with the connective tissue, eyes, bowel, and skin.
Psoriatic Arthritis (PsA)
Pain in the lower back is common, especially in severe cases.
It can affect other joints and cause psoriasis.
Reactive Arthritis
This is a reaction to infection.
It is more common in the limbs, hands, and feet joints but can involve the spine.
Enteropathic Arthritis
This mainly affects the spine but can include other joints.
It is associated with inflammatory bowel disease.
Autoimmune diseases that don’t specifically target the spine but can also cause back pain include:
Lupus
Sjögren’s syndrome
Hashimoto’s thyroiditis
Finding a Doctor
Individuals may be fine with their primary healthcare provider’s choice regarding which rheumatologist to see. However, they may want to research other options to ensure the right rheumatologist is chosen. Things to look at include:
Search online medical directories.
Visit the websites of the doctors being considered to learn more about their training, approach, and specialties.
Check online reviews.
Check on health insurance coverage.
Ask members of the healthcare team, friends, and family for recommendations.
Contact rheumatologists’ offices to see if they are accepting new patients.
Once decided, pass along the information to the primary care doctor so they can make the referral.
Preparing For The Initial Visit
Before seeing a new rheumatologist, take a few minutes to prepare so you can make the most of the appointment. Individuals will want to have:
A list of back-related symptoms, including frequency and severity.
A list of what makes symptoms better or worse.
A copy of recent test results and records from other doctors.
Individuals can ask their provider/s to send their medical information to the rheumatologist’s office in advance.
A list of treatments that have been tried and how well they worked.
A list of all medications, over-the-counter and prescription, supplements, and herbal products taken.
A list of medication allergies.
Complete medical history and family history of potentially related diseases.
A list of any questions regarding conditions, treatment, etc.
If possible, fill out any paperwork for the new office beforehand to save time on the appointment day.
Injury Medical Chiropractic and Functional Medicine Clinic
Talking with a healthcare provider is important. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. Using an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility and help individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers.
Quick Patient Initiation Process
References
Hospital for Special Surgery. (2023). What Is a Rheumatologist and What Conditions Do They Treat? https://www.hss.edu/conditions_what-is-a-rheumatologist.asp#when
Yale University School of Medicine. Dee, J. E. (2021). 5 reasons why a patient should see a rheumatologist. https://medicine.yale.edu/news-article/5-reasons-to-see-a-rheumatologist/
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Autoimmune diseases. Retrieved from https://www.niams.nih.gov/health-topics/autoimmune-diseases
Johns Hopkins Medicine. (2024). Spinal arthritis (arthritis in the back or neck). https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-arthritis
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine