Back pain is one of the most common reasons for seeking health care. Individuals dealing with back pain but don’t know the cause may have some inflammatory joint disease or autoimmune condition. Can seeing a rheumatologist help?
Rheumatologist
Depending on what’s causing the back pain, individuals may need to see their primary doctor for a referral. Individuals are recommended to see a rheumatologist if they have back pain that doesn’t come from an injury that doesn’t go away after a few weeks, pain that comes back after treatment, or symptoms that suggest a rheumatic condition. Rheumatologists treat severe or persistent back pain and are experts in autoimmune diseases, including lupus, Sjogren’s syndrome, rheumatoid arthritis, ankylosing spondylitis, axial spondylitis, Psoriatic arthritis, and other forms of inflammatory or autoimmune arthritis.
What Do They Do?
A rheumatologist is an internist or pediatrician who has completed special training in treating conditions that are:
Inflammatory
Autoimmune
Related to painful joint disease
The doctors diagnose, treat, and manage these conditions long-term. Depending on diagnosis and care needs, they may also lead or be part of a team that includes other healthcare providers.
Symptoms
When muscles ache, pain presents, or joints hurt, and especially if there are signs of inflammation that don’t go away, seeing a healthcare provider is recommended. Symptoms of inflammation include:
Redness
Swelling
Pain
Stiffness
Loss of joint function
Usually, to see a rheumatologist, individuals need a referral from their primary care provider and may be referred when:
There is no evidence of a back injury.
At-home therapies like heat application, prescription medications, or physical therapy are unsuccessful.
There is uncertainty about what’s causing the back pain, but I suspect it’s rheumatological.
Blood tests for inflammatory markers or certain antibodies yield abnormal results.
There is a diagnosis of a rheumatic condition and recommend a specialist to manage it.
There is a family history of a rheumatic or autoimmune condition that may cause back pain.
Some types of arthritis can cause permanent, progressive joint damage.
Conditions
Conditions that can affect the spine and cause back pain and are treated by a rheumatologist include: (Johns Hopkins Medicine, 2024)
Rheumatoid arthritis (RA)
This often starts in smaller joints of the hands and feet and later moves to the neck and/or back.
It can also affect different body organs and have systemic symptoms.
Ankylosing Spondylitis (AS)
Primarily a disease of the spine, it may also impact the shoulders, hips, knees, and ankles.
Systemic symptoms, including fever and fatigue, can manifest.
Axial Spondylitis
This primarily affects the spine, chest, and pelvis.
It may also cause problems with the connective tissue, eyes, bowel, and skin.
Psoriatic Arthritis (PsA)
Pain in the lower back is common, especially in severe cases.
It can affect other joints and cause psoriasis.
Reactive Arthritis
This is a reaction to infection.
It is more common in the limbs, hands, and feet joints but can involve the spine.
Enteropathic Arthritis
This mainly affects the spine but can include other joints.
It is associated with inflammatory bowel disease.
Autoimmune diseases that don’t specifically target the spine but can also cause back pain include:
Lupus
Sjögren’s syndrome
Hashimoto’s thyroiditis
Finding a Doctor
Individuals may be fine with their primary healthcare provider’s choice regarding which rheumatologist to see. However, they may want to research other options to ensure the right rheumatologist is chosen. Things to look at include:
Search online medical directories.
Visit the websites of the doctors being considered to learn more about their training, approach, and specialties.
Check online reviews.
Check on health insurance coverage.
Ask members of the healthcare team, friends, and family for recommendations.
Contact rheumatologists’ offices to see if they are accepting new patients.
Once decided, pass along the information to the primary care doctor so they can make the referral.
Preparing For The Initial Visit
Before seeing a new rheumatologist, take a few minutes to prepare so you can make the most of the appointment. Individuals will want to have:
A list of back-related symptoms, including frequency and severity.
A list of what makes symptoms better or worse.
A copy of recent test results and records from other doctors.
Individuals can ask their provider/s to send their medical information to the rheumatologist’s office in advance.
A list of treatments that have been tried and how well they worked.
A list of all medications, over-the-counter and prescription, supplements, and herbal products taken.
A list of medication allergies.
Complete medical history and family history of potentially related diseases.
A list of any questions regarding conditions, treatment, etc.
If possible, fill out any paperwork for the new office beforehand to save time on the appointment day.
Injury Medical Chiropractic and Functional Medicine Clinic
Talking with a healthcare provider is important. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. Using an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility and help individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers.
Quick Patient Initiation Process
References
Hospital for Special Surgery. (2023). What Is a Rheumatologist and What Conditions Do They Treat? https://www.hss.edu/conditions_what-is-a-rheumatologist.asp#when
Yale University School of Medicine. Dee, J. E. (2021). 5 reasons why a patient should see a rheumatologist. https://medicine.yale.edu/news-article/5-reasons-to-see-a-rheumatologist/
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Autoimmune diseases. Retrieved from https://www.niams.nih.gov/health-topics/autoimmune-diseases
Johns Hopkins Medicine. (2024). Spinal arthritis (arthritis in the back or neck). https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-arthritis
For individuals experiencing piriformis syndrome. Can knowing the causes and what it feels like help in diagnosis and treatment?
Managing Piriformis Syndrome
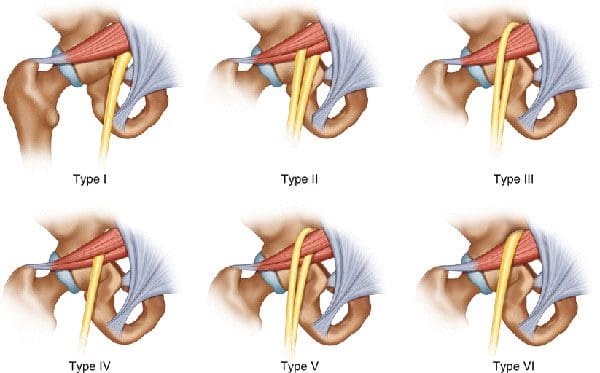
Piriformis syndrome is where spasms occur in the piriformis muscle located in the buttocks. These muscle spasms can cause pain and numbness in the buttocks and the back of the leg. (Cedars Sinai, 2022)
What Is It?
Piriformis syndrome is an irritation of the sciatic nerve from the piriformis muscle. Although the piriformis muscle is small compared to other muscles around the hip and thigh, it supports the hip joint’s external rotation or turning out. The sciatic nerve supplies the lower extremities with motor and sensory functions. The piriformis tendon and sciatic nerve cross each other behind the hip joint in the deep buttock. Both are about one centimeter in diameter. The piriformis muscle spasms can irritate the sciatic nerve, causing sciatica symptoms. (Cedars Sinai, 2022)
Triggers
A piriformis syndrome diagnosis means the piriformis tendon binds or spasms around the sciatic nerve, causing irritation and symptoms. Many doctors and specialists support the theory that when the piriformis muscle and its tendon tighten, this can cause compression and pinch the nerve. This can decrease blood circulation and irritate the nerve due to pressure. (Cass S. P. 2015) Many doctors also believe that piriformis syndrome occurs from anatomic variation of the muscle and tendon. It is thought this muscle-tendon variation irritates the nerve in some, leading to sciatica symptoms.
How It Feels
Common signs and symptoms experienced include (Cass S. P. 2015)
Pain in the buttocks.
Pain behind the hip.
Electric shock pains traveling down the back of the lower extremity.
Numbness in the lower extremity.
Tenderness with pressure that often causes pain when sitting.
Some develop symptoms abruptly, while others gradually increase in symptoms in the back of their thighs.
Most who are diagnosed with piriformis syndrome are generally active individuals who experience increasing difficulty with certain types of physical activity.
Testing
There are no specific tests that accurately diagnose piriformis syndrome. Doctors will order tests, including MRI and nerve conduction studies. Because it can be difficult to diagnose, there are likely many misdiagnosis cases. This means that some with the condition don’t have a piriformis diagnosis. In addition, some with vague hip pain may receive this diagnosis even if they don’t have the condition. (Cass S. P. 2015) An injection is often administered into the piriformis muscle when the diagnosis is uncertain. (Jankovic D. et al., 2013) Performing an injection can help determine the specific location of the discomfort. When an injection is given into the piriformis muscle or tendon, it is administered by ultrasound guidance to ensure the needle delivers medication to the correct location. (Bardowski E. A., and Byrd J. W. T. 2019)
Differential Diagnosis
Some other conditions with buttock pain can have similar symptoms. Other causes can include:
Radiculopathy/Sciatica
Herniated discs
Hip bursitis
Spinal stenosis
The diagnosis of piriformis syndrome is given when these diagnoses are eliminated as possible causes of pain.
Treatment
Managing piriformis syndrome is quite general, and it is often difficult to recover from. Common treatment and management suggestions include the following. (Jankovic D. et al., 2013)
Rest
Avoiding activities that cause symptoms for at least a few weeks.
Physical Therapy
Focuses on stretching and strengthening the hip rotator muscles.
Anti-inflammatory Medication
To decrease inflammation around the tendon.
Deep Massage
Used to relax the piriformis muscle and help release the compressed nerve.
Cortisone Injections
It can help decrease inflammation and swelling.
Botulinum Toxin Injection
It can paralyze the piriformis muscle to reduce pain and discomfort.
In severe cases, surgery can be performed to loosen the piriformis tendon, known as a piriformis release (Cass S. P. 2015). This surgical procedure is recommended when conservative treatments have been tried for at least six months and other causes of pain have been evaluated and ruled out. Recovery takes several months.
The goal of managing piriformis syndrome is to improve the range of motion and flexibility around the hip and diminish inflammation around the sciatic nerve. Working with a professional chiropractic team can help relieve pain, return individuals to normal function, and expedite healing. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a customized treatment program through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Piriformis Syndrome Treatment Chiropractor
References
Cedars Sinai. Sinai, C. (2022). Piriformis syndrome. https://www.cedars-sinai.org/health-library/diseases-and-conditions/p/piriformis-syndrome.html
Cass S. P. (2015). Piriformis syndrome: a cause of nondiscogenic sciatica. Current sports medicine reports, 14(1), 41–44. https://doi.org/10.1249/JSR.0000000000000110
Jankovic, D., Peng, P., & van Zundert, A. (2013). Brief review: piriformis syndrome: etiology, diagnosis, and management. Canadian journal of anaesthesia = Journal canadien d’anesthesie, 60(10), 1003–1012. https://doi.org/10.1007/s12630-013-0009-5
Bardowski, E. A., & Byrd, J. W. T. (2019). Piriformis Injection: An Ultrasound-Guided Technique. Arthroscopy techniques, 8(12), e1457–e1461. https://doi.org/10.1016/j.eats.2019.07.033
For individuals who sit at work for long hours, can years of practicing unhealthy posture be corrected through a step-by-step approach to ensure optimal body position while sitting?
Sitting Posture
Sitting up straight with a healthy posture requires the conscious alignment of the hips, pelvis, lower back, upper back, shoulders, neck, and head. Learning or retraining oneself to maintain correct sitting posture can relieve lower back pain, improve respiration and digestion, and reduce tension in the neck and shoulders. (Albarrati, A. et al., 2018) It starts by paying attention to posture throughout the day and correcting it whenever forward head posture, leaning, or slouching develops. Targeted exercises can also help build upper-body strength, and stretching can stabilize and strengthen the core muscles, lower back, and pelvic joints. (Albarrati, A. et al., 2018)
Sit Up Straight Guide
Sitting up straight can be uncomfortable because it is not a natural position for the body to be in for an extended time. Nowadays, work, school, appointments, and other activities require us to sit much longer than intended. The muscles also have to work against gravity, leading to muscle exhaustion, slouching, and slumping, which can cause chronic back, leg, neck, and/or shoulder pain. (Jung, K. S. et al., 2020)
Sitting up straight may seem simple, but the focus tends to be on straightening just the lower/lumbar spine. This posture is unsustainable and exhausts and stresses the upper and lower back. (Jung, K. S. et al., 2020) The whole body needs to be considered when protecting the stability and balance of the spine. Learning and maintaining the ability to sit up straight is a process that requires practice. Find a comfortable chair to sit in, and follow these steps to achieve the optimal postural alignment (Canadian Centre for Occupational Health and Safety, 2022)
Knee Spacing
The hips should be at a roughly 90-degree angle.
Knee Position
The knees should be at a 90-degree angle level with the hips.
Use a pillow to achieve the right knee position if the seat is too low.
Keep the Feet Flat on the Floor
If feet don’t reach the floor, place a footstool, box, book, or other flat object underneath them.
Sitting Bones
Also known as the ischial tuberosities, these are two knobby bones on the underside of the pelvis.
Feel around to find them.
Pelvis Adjustment
Shift the body so that the sitting bones are directly under the pelvis rather than situated too far back, stressing the lower back or too far forward, leading to slumping.
Spine Check
There should be a slight spinal curve, and one should be able to slip a hand between the lower back and the back of the chair.
Shoulder Check
The shoulders should be level and vertically aligned with the hips.
If the shoulder blades are pulled back or the shoulders are lifted or curled forward, relax them into a neutral position.
Head Positioning
The head tends to tilt too far forward while sitting as work and the day progresses.
Adjust the head position to align the neck with the upper spine.
The head should be slightly tilted forward, with the ears aligned with the shoulders.
Check for Pain and Discomfort
Pain may be due to structural imbalances of the spine, pelvis, or hips.
Use a lumbar chair support or place a rolled-up towel or cushion at the lower back to keep the back straight.
Added Tips
Tools and tricks to help prevent and avoid back, hip, and neck pain.
Chairs
All the bells and whistles for an ergonomic desk chair are unnecessary.
Focus on features like adjustable seat height and lumbar support. The correct seat depth recommendations are deeper if tall and shallower if short. (van Niekerk, S. M. et al., 2012)
Cushions
If sitting on a cushion or using one to bolster the back or hips, recommendations are not to go too soft.
Cushions that are too soft allow the ability to shift from one hip to the next, often without realizing it.
They usually eventually flatten and lose support.
Monitor Position
There is no point in sitting straight if the monitor is too high or too low.
The monitor should be at eye level to maintain the proper head and shoulder alignment.
If the monitor is too low, place a box or book underneath it.
If it is too high, raise the chair’s height and place a footrest under the feet to keep them flat.
Avoid Crossing Legs or Feet
Crossing the legs or feet places stress on the opposite hip, thigh, and knee and wears the body out faster.
If the hips or legs are tiring prematurely, the individual is not sitting correctly or in the wrong chair.
Use Comfortable Footwear
Maintaining flat feet on the floor while sitting is imperative.
This is not possible in high heels or platform shoes.
Change into a comfortable pair of flat shoes while sitting.
Take Regular breaks
Even with an ergonomic desk chair, the body is not meant to be sitting for hours and hours.
Get up at least every hour, walking and stretching to reactivate the muscles and circulation.
Sitting up straight requires body alignment awareness, stable core muscles, and balanced pelvis, hips, spine, shoulders, neck, and head positioning. It may take some time before these steps become normal, but they will become second nature with perseverance and practice. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution that fully benefits the individual to get back to normal. Using an integrated approach to treat injuries and chronic pain syndromes to improve ability through flexibility, mobility, and agility programs to relieve pain. Our providers create personalized care plans for each patient, including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. If other treatment is needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Posture and Mobility
References
Albarrati, A., Zafar, H., Alghadir, A. H., & Anwer, S. (2018). Effect of Upright and Slouched Sitting Postures on the Respiratory Muscle Strength in Healthy Young Males. BioMed research international, 2018, 3058970. https://doi.org/10.1155/2018/3058970
Jung, K. S., Jung, J. H., In, T. S., & Cho, H. Y. (2020). Effects of Prolonged Sitting with Slumped Posture on Trunk Muscular Fatigue in Adolescents with and without Chronic Lower Back Pain. Medicina (Kaunas, Lithuania), 57(1), 3. https://doi.org/10.3390/medicina57010003
Canadian Centre for Occupational Health and Safety. (2022). Working in a sitting position – good body position. Retrieved from https://www.ccohs.ca/oshanswers/ergonomics/sitting/sitting_position.html
van Niekerk, S. M., Louw, Q. A., & Hillier, S. (2012). The effectiveness of a chair intervention in the workplace to reduce musculoskeletal symptoms. A systematic review. BMC musculoskeletal disorders, 13, 145. https://doi.org/10.1186/1471-2474-13-145
How do healthcare professionals in a chiropractic clinic provide a clinical approach to recognizing impairment for individuals in pain?
Introduction
Any article you read about substance abuse among nurses will almost certainly repeat the claims made by the American Nurses Association, which states that, in line with the general public, 10% of nurses, or one in ten or about 300,000 Registered Nurses in the United States, are dependent on drugs of some kind. Impairment of any kind at work, particularly if it stems from substance misuse or usage, can have serious repercussions for the nurse and the nursing profession for several reasons. Preciseness, correctness, the capacity for critical thought, and observation are essential in the nursing profession. Because errors or accidents may occur, any inability to deliver these abilities puts patients, coworkers, and the nurse at risk. Additionally, people view nurses as trustworthy, dependable, and honest. Impairment can damage that perception, particularly if it is brought on by alcohol or drugs. In the following sections, we’ll examine impairment, its reasons, and your ethical and legal obligations if you believe a coworker is impaired. Today’s article focuses on the clinical approach to recognizing impairment in a clinical setting. We discuss with certified associated medical providers who consolidate our patients’ information to assess pain-like issues they are experiencing. We also inform and guide patients on various treatments and ask intricate questions to their associated medical providers to integrate a customized treatment plan. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
A Definition of Impairment
The fundamental definition of impairment is “The state of being decreased, weakened or harmed, especially mentally or physically” (“Impairment,” n.d.”) You’ll see that this is merely a description of a state of being and that no reason is given. This is a result of the abundance of possible reasons. While some causes might be simple to prove, others might not. Consequently, it is important to identify and consider the context and cause, if known, while talking about impairment. The impaired populace that surrounds us as nurses is: They are patients of ours. They are in a reduced, weakened, or damaged state, albeit they may be compromised by disease or injury. Similarly, you are compromised by illness if you have worked a shift with a bad cold. Symptoms of feeling slower, impaired thinking, andreviewing your work more frequently are examples of impairment in a clinical setting.
A disease or injury may have different consequences and affect how well you execute your job to varied degrees, but as the degree of impairment increases, so does the chance that you will make a mistake. The safety of both you and those around you, including your patients and coworkers, is inversely correlated with your degree of impairment. You, your patients, and your coworkers are less safe the more your performance is negatively impacted. Even though nurses know that the patients are vulnerable because they are compromised in some way. We also know that impairments can make it more likely for you to make mistakes. You are a responsible person and would never work if your impairment was severe enough to put your patients in danger. However, what if a coworker has a disability? Even worse, what if you think it was somehow self-inflicted? How do you proceed? Do you talk to them? Do you inform someone else about it? Do you hope nothing bad happens and ignore it?
Preserving patient safety is a top priority for nurses in their line of work. It is your responsibility to know what to do and how to do it if a colleague appears to be affected. But to achieve that, you must be able to spot potential impairment in both you and other people. Administrative and required reporting requirements must be known to you. You also need to be aware of the possible consequences for yourself if you do nothing.
Causes of Impairment
You might assume that we are discussing drug usage the moment you hear or read the phrase impairment in the workplace. However, there are other potential causes besides alcohol or drug abuse, and drawing the wrong conclusions can frequently have unanticipated results. You are not required to look into or determine what’s causing your colleague’s apparent disability. That is the task of others. You must identify impairment indicators and take the proper action. One of the things you should consider before reporting a coworker for drug addiction is whether or not you are witnessing real impairment. Everyone has occasional feelings of illness, irritability, or tension. Even if we might not be as effective as usual, nothing about our performance puts anyone at risk, and it doesn’t happen often. “Impairment in the healthcare system is defined as the inability or impending inability to practice, which is divided into two categories that can affect both the professional and the patient” (Baldisseri, 2007). This statement dismisses the previous scenario in which you might move more slowly than usual due to a severe cold.
Functional Medicine Influence Beyond Joints- Video
The Difference Between Impairment & A Bad Day
“Impairment is characterized by the inability to carry out the professional duties and responsibilities reasonably consistent with nursing standards.” Having a bad day can affect the individual’s mood and workflow. Sometimes, a faint impression that someone is not quite themselves leads to this discovery. Colleagues could experience unease or feel intimidated. Supervisors may notice a rise in the number of grievances lodged against an employee or by coworkers against that individual. Behavioral patterns suggest issues exist and can lead to the development of causing medical errors. Medical errors in healthcare organizations can create a serious health problem that can substantially threaten the patient’s safety. (Rodziewicz et al., 2024). Before examining these patterns, let’s consider some of the potential reasons other than drug or substance misuse that could be contributing to the decline in risky practices in nursing tasks.
Training & Education Deficits
A coworker’s risky activities could result from inadequate training, knowledge, or orientation to the current workplace. This is particularly valid for recently licensed nurses and nurses transitioning from one practice area to another. Nurses in refresher training may need to be more confident in how things have traditionally been done or need to be taught suggested modifications to policy or procedures. Refresher training may also encounter opposition or change and need to be successful. If the nurse is unwilling to acknowledge that their knowledge or abilities are not up to par, these educational deficiencies may appear as impairment. They might take much longer than other nurses to do jobs, among other indicators. Erroneous assumptions about which process is the most reasonable or accurate way to complete a task might lead to mistakes on the part of the nurse. Alternatively, they could be overly sensitive to criticism and try to maintain their composure by insisting they are competent.
Physical Illness
We have already discussed the issue of trying to work when you have a bad cold. For most of us, the experience of having a little illness or infection holding us back is probably known. Yet, increased chronic conditions could also lead to compromised performance days. Like many other ailments, diabetes, and arthritis can cause someone to feel less than 100% of themselves on certain days. It’s important to remember that you might not even be aware that your coworker has these ailments. For want of a better or more appropriate title to put this under, be sure the person you are about to accuse of abusing drugs is not pregnant before moving forward. Naturally, this is a partial list of all potential physical explanations. It’s merely a friendly reminder to consider the chance the incompetent nurse could be physically unwell.
Physical Injury
Like medical conditions, injuries can also hinder one’s ability to perform at work. Although it is more likely that there may be some overt signs of an injury—such as a limp or other unnatural movement, bandaged regions, or the use of a walking stick or other mechanical aid—this isn’t always the case. A person with a back strain or some different type of nerve entrapment could try to disguise their discomfort and their limits.
Stress & Fatigue
Since it is common for these causes to occur together or for one to manifest as a symptom of the other, they might be seen as a collective cause. They may also be the outcome of events outside the workplace, inside the workplace, or both. Someone who has recently gone through a divorce or someone who is the primary caregiver for a critically ill relative at home are two examples. Both scenarios are unpleasant, but what if these factors were secondary to financial difficulties? Both worrying about this and attempting to work more shifts due to their economic challenges may hurt their ability to sleep. Someone in these situations can easily get psychologically and physically fatigued very fast. Depending on their personality, it would also be unheard of for their colleagues to be unconscious of these difficulties. Alternatively, the cause might be as straightforward as stress at work, resulting in burnout and decreased motivation. Burnout and work dissatisfaction are, in fact, “common within the nursing profession” (Van Bogaert et al., 2017)
Mental Illness
Even though nurses like to think of themselves as resilient and unaffected by situations that others would see as weakness, the truth is that we are vulnerable to mental health issues like anxiety and depression, as well as drug use disorders, for many of the same reasons. In certain nursing specialties, we work with patients who are dying all the time—possibly even infant deaths—or we witness horrifying results from violent or accidental incidents. Circumstances like these may serve as antecedents to illnesses like Post Traumatic Stress Disorder (PTSD). Nurses are not superwomen or supermen—again, these are only a few examples. Healthcare professionals may be impacted if it impacts the broader public.
Substance Use
Substance addiction is perhaps the most chronic and damaging to the individual, the facility, and even the profession, even if it isn’t necessarily more common than the previously described causes of impairment. Substance abuse is not likely to go away on its own over time without assistance from coworkers and superiors, unlike medical conditions or injuries. This does not imply that interventions for other impairment causes are unnecessary or should be avoided. If you don’t act when something like low back pain is the cause of the impairment, you can end up addicted to painkillers in the first place. Included in the collection under this subject is disability brought on by the misuse or overuse of pharmaceuticals that have been prescribed to them or others. The impairment is frequently associated with the side effects of overuse or acute overdose. At the same time, it can also occasionally arise from adverse events associated with normal doses, such as nausea, sleepiness, or dizziness. The usage or misuse of “street drugs” or non-prescription substances like methamphetamine, ecstasy, or cannabis. The acute or chronic misuse or overuse of alcohol. The nurse may be severely intoxicated or experiencing a severe hangover, but both conditions would impede her abilities. Chronic use can also result in physical ailments or cognitive impairments that make it difficult for a nurse to perform at a high enough level. Since a nurse’s whole self-definition frequently centers around their work as a nurse, the entry of their abuse or addiction into their place of employment is often a sign of how far along their illness has evolved.
Because health workers identify with their line of work, evidence of disease sometimes points to a late stage of illness. Workplace issues are typically the last stage of a downhill spiral, and when a disease is discovered, coworkers are frequently astonished “(Washington State Department of Health, 2016, p.6). When the impairment is initially seen at work, coworkers and bosses may even deny or minimize the issue, offering justifications or avoiding confrontation in the hopes that the issue will magically disappear.
Unique Risk Factors For Nurses
The likelihood of having a drug use disorder is influenced by a variety of factors, including heredity, upbringing, parental and peer pressure, and so on. However, working as a nurse presents a few unique risk factors that are not present in other occupations. The main hour risk factors that nurses deal with in a healthcare facility are:
Drugs that are lawful to obtain by prescription are more likely to be used by nurses than by the general public, even though substance use disorders do not affect nurses more frequently than the general population. The explanation is that nurses handle these medications daily, even without a prescription. To this, we add our knowledge of medicine administration, usage, and dosage and work in a setting where the benefits of medication use are evident. This indicates that we are self-assured in our capacity to diagnose and treat ourselves and in our ability to handle these medications.
Stress
Some of the indications that all nurses are sometimes a part of the stress factors that have caused them to be impaired include:
Extended shifts
Heavy workload
Absence of personnel
Extremely urgent patients while retaining composure under intensely sentimental circumstances.
These are presumably well-known to all nurses and can occasionally be attributed to role strain. They are all a necessary component of a very demanding line of work. Work schedules alone have demonstrated a beneficial relationship with substance usage. Pain or insomnia following a demanding shift are common and often serve as the primary justification for taking medication to help with aches and pains, promote relaxation, or fall asleep.
Lack of Education
Here, the term “lack of education” does not mean ignorance of drugs. As we’ve already mentioned, there is no shortage of schooling there. No. In this context, ignorance of substance use problems and associated warning signs and symptoms is meant. Many times, healthcare professionals are unable to identify these symptoms and indicators in both themselves and other people. Even if they do identify them, stigmatization results from a lack of information about these disorders—especially if the sufferer is a fellow healthcare worker—because we tend to hold healthcare professionals—including ourselves—to higher standards than we do non-healthcare workers.
Recognizing The Signs
When a nurse is caught using drugs or alcohol at work, the ideal course of action these days is assistance and therapy rather than immediate termination. The idea is that the nurse will eventually be able to go back to work following treatment and rehabilitation. However, early intervention is a key component of this strategy. As we’ve already mentioned, substance use may need to continue for a while before signs of impairment at work become apparent. Therefore, in pursuing a successful result, time itself becomes a threat. It is appropriate to remind ourselves that substance abuse may not be the only explanation for the impairment as we examine some of the indicators that substance use may cause. For the sake of the patients’ and the staff’s safety, intervention is required regardless of the cause. Searching for behavioral changes or changes from a baseline rather than specific activities is perhaps more beneficial. After all, we all know that a nurse who is not incompetent but has always appeared messy or moves a little more slowly than others when completing tasks. Perhaps it’s just a personal preference, but if a nurse who used to appear well-groomed and productive suddenly starts to act sluggish and careless, there may be a deeper issue at hand.
On the other hand, it is also noteworthy if the nurse, who has always been sluggish and sloppy but has always stayed within acceptable parameters, suddenly became unacceptable or extremely slow and messy. However, the noticeable shift might be outside the condition of their attire. Even someone who is usually upbeat can seem depressed, nervous, or afraid. A typically quiet individual can appear animated, talkative, and gregarious. It’s also possible that the shy person isolates themselves more than usual, or the ordinarily talkative and active person becomes even more talkative and active than normal. Recall that the behavior is less important in many cases than the change in pointing out a problem. It is similar to checking for deviations from normal blood pressure or temperature as a sign of an issue. Additional indicators of a change to watch out for include:
Mood swings
Irritability
Drowsiness
Crying or inappropriate laughing
Suspicion or being extremely sensitive to criticism.
Inflexibility or excessive adherence to procedures when they are not required.
Bewilderment, or bad memory
When it comes to work performance, you could observe the following:
A rise in tardiness and absences, particularly when they follow a pattern.
Strange explanations for absences
Longer or more regular pauses
Uncharacteristic absences from the workplace,
Previously, ordinary tasks required more time.
Unusual or dubious “shortcuts” used in operations do not uphold the anticipated level of care.
When the quality or content of the charting becomes shoddy or unique, there are greater inaccuracies and negligence.
A rise in the nurse’s complaints or grievances.
Each of them points to a possible issue. They could be overtly apparent or strange enough to give you the impression that something is off. You may notice that they are using breath fresheners, mints, or chewing gum more frequently than they used to. They may mumble more than usual or exhibit more subtly stopped speech with longer silence while considering their response. “Were their pupils constricted (or dilated)?” or “Was that alcohol I smelled?” are some questions to ask yourself as you leave. As nurses, we may acquire hunches or intuition. Our innate ability to observe results from our extensive training and these instincts are frequently founded on observations we make unconsciously. Thus, please don’t ignore them. While you shouldn’t ignore them, you shouldn’t accept them as gospel.
Drug Diversion
Access to the drug of choice may be restricted for a nurse with a substance use disorder when they are not working. This could be for various reasons, such as the fact that their family is no longer prescribed that particular drug, their doctor or pharmacist becoming suspicious, or other reasons. They frequently attempt to supplement that access from the job in this kind of circumstance. And the nurse will need to be creative in hiding this behavior due to the precautions in place, particularly when it comes to banned substances.
Among the warning indicators to look out for are:
Regularly or eagerly offering to be a pharmaceutical nurse.
Patients continue to complain about discomfort even after receiving painkillers.
Documents reveal that the patient was given more painkillers than necessary for their condition.
There are more and more reports of drug spills and waste.
When this nurse performs medication rounds relative to other nurses, an abnormally high number of controlled drugs are administered.
Drug counts are inaccurate; If you have yet to witness a drug given or dispensed, the nurse may ask you to co-sign for it. This is a partial list, just like the others. As with the other lists, nurses are very wise due to our education, training, and experiences, so sometimes it’s just a gut instinct that warns you of a possible issue. However, as a general guideline, anything that feels off should be looked into further. Your obligations to your patients and your coworkers require this.
Interventions
The Florida Nurse Practice Act is broken when a nurse practices while intoxicated. Both illness and substance use are listed as potential causes of this impairment in the paragraph that defines this as a violation and could result in disciplinary action. It would also be illegal to fail to disclose a nurse’s impairment or to put a patient’s safety in peril by permitting them to work while impaired. It is preferable for everyone if there is no attempt to cover for the nurse or if the issue is ignored in the hopes that it will go away. As an employee, you should be fully conversant with the regulations and procedures each facility has likely designed for just these scenarios. These will have been created to guarantee compliance with all legal and regulatory obligations. It is never appropriate for you to approach a coworker who is impaired. Always ask a supervisor or nursing manager for assistance. The manager or supervisor will probably contact the impaired nurse first; however, having multiple people present during the intervention will:
Give the evidence given to the nurse more weight because she is likely to dispute impairment.
Present witnesses for incidents that might be needed in hearings or meetings later.
Provide strength to the message, emotional support, and uphold safety if the nurse exhibits agitation or aggression when contacted.
Never should the initial intervention be accusatory or involve attempting to identify the nurse’s issue.
It should be fact-based and provide written evidence of observations and concerns to make the nurse realize why you are requesting them to stop working now. The impairment and any subsequent intervention might be reported in one of two ways. The Florida State Board of Nursing is the first of them. More precisely, the Department of Health would receive the report, investigate the complaints, and take appropriate action. The second action would be to send the report to the Intervention Project for Nurses (IPN). The IPN was created in 1983 by legislative action to protect the public’s health and safety (Chan et al., 2019). It does this by offering close supervision to nurses who are deemed unsafe to practice because of impairments brought on by drug or alcohol abuse, misuse, or both, or because of a physical or mental illness that may impair the licensee’s capacity to practice safely and skillfully.
These alternative-to-discipline programs have been developed across the nation, and in Florida, they are part of the Integrated Patient Network (IPN) because of the recognition that a nurse with a substance use disorder should receive the same care and treatment as anyone else. Through its programs, nurses can obtain non-punitive treatment and rehabilitation. The IPN will assist the nurse’s successful return to practice if she consents to step away from the profession and finish the program while maintaining confidentiality—even from the Board of Nursing. The IPN will send the file to the Department of Health if a nurse accepts these terms but then changes their mind. Certain cases might be reported to the Department of Health and the IPN, where treatment AND disciplinary action might be started. The Department of Health’s participation might lead to the nurse’s license being suspended or revoked, making it more difficult for her to return to work. It is envisaged that by offering non-punitive routes, nurses will be encouraged to seek assistance before facing disciplinary action and may eventually be able to return to practice.
Conclusion
Because of the unique circumstances surrounding our education and training, the way we are perceived, and the fact that we perceive ourselves as somehow stronger than others, the issue of disability in the workplace for nurses is particularly complicated. In the past, if an employee was impaired at work, disciplinary action might have been taken because of the impairment itself or the mistakes made. This was particularly valid in cases where it was discovered that the nurse was intoxicated or impaired by another substance. You were out the door and never came back after that. You would also lose your license, preventing you from ever returning to work as a nurse. Thankfully, non-disciplinary initiatives have been sparked by recognizing that we are not immune to the same stressors as others. The idea behind these initiatives is to identify problems, including substance use disorders, early on so that the best possible outcome may be achieved for all parties.
Chan, C. W. H., Ng, N. H. Y., Chan, H. Y. L., Wong, M. M. H., & Chow, K. M. (2019). A systematic review of the effects of advance care planning facilitators training programs. BMC Health Serv Res, 19(1), 362. https://doi.org/10.1186/s12913-019-4192-0
Hakim, A. (2023). Investigating the challenges of clinical education from the viewpoint of nursing educators and students: A cross-sectional study. SAGE Open Med, 11, 20503121221143578. https://doi.org/10.1177/20503121221143578
Van Bogaert, P., Peremans, L., Van Heusden, D., Verspuy, M., Kureckova, V., Van de Cruys, Z., & Franck, E. (2017). Predictors of burnout, work engagement and nurse reported job outcomes and quality of care: a mixed method study. BMC Nurs, 16, 5. https://doi.org/10.1186/s12912-016-0200-4
For individuals who are getting older, can increasing bone strength help prevent fractures and optimize bone health?
Bone Strength
Bone strength is important, as a fractured hip can be serious for older individuals. A study found that for individuals in their 60s who had a hip fracture, 6.5% of women and 9.4% of men died within a year. Among individuals in their 80s, 13.1% of women and 19.6% of men died within a year. (Dimet-Wiley, et al., 2022)
Increasing bone strength can help prevent various issues. A small increase in bone mineral density has been shown to help reduce the risk of fractures, especially hip fractures. A decades-long study found that just a 3% increase in bone strength helps lower the chance of breaking a hip. Researchers enrolled two groups of individuals aged 60 and older, one in 1989 and the second in 1999.
The bone mineral density of each subject’s femoral neck joint at the top of the thigh bone near the hip was measured.
They then followed the subjects for years to see who experienced hip fractures.
While the bone mineral density of the second group was only 3% higher than the first group, these subjects experienced a 46% reduction in hip fractures. (Tran, T. et al., 2023)
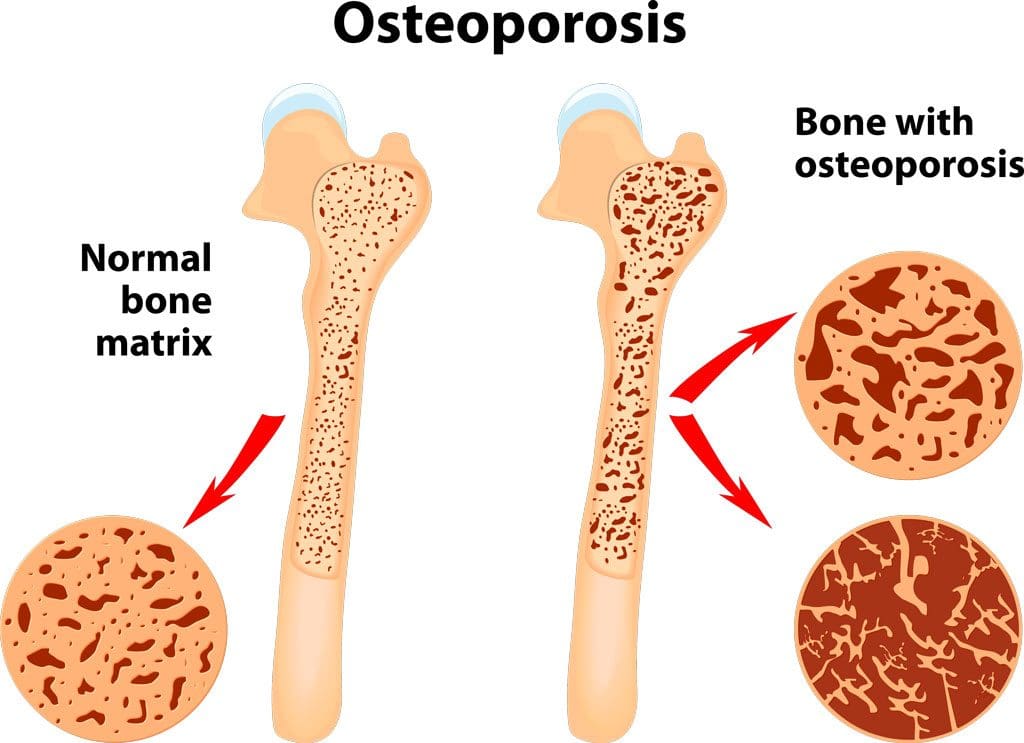
Bone Loss
Bone loss is progressive in men and women and increases as the body ages. Osteoporosis is a condition in which bone tissue deteriorates. (Department of Health and Human Services Office of Disease Prevention and Health Promotion. 2020) Bones constantly break down and reform as a normal remodeling process. If the balance of this process is impaired, osteoporosis develops, resulting in more bone breakdown than formation. While men and women experience bone loss, it’s more common in females. (National Institute of Arthritis and Musculoskeletal Diseases. 2022) Menopause is a risk factor because of the decline of estrogen (National Library of Medicine, Medline Plus, 2022). Estrogen reinforces bone strength by protecting against bone breakdown; with estrogen loss, bone breakdown increases. However, anyone of any age or background can experience bone loss due to the following:
While some loss of bone strength is common, several strategies exist to maintain bone health. Exercise, specifically weight-bearing activities, can increase bone strength. When bones and muscles are used to hold a position against gravity, this mechanically stresses the bone, causing it to reform stronger. Movement and physical exercise as medicine and the forces transmitted through the bones generate mechanical signals that tell the cells to increase bone formation relative to breakdown. Exercises focusing on posture, balance, gait, and coordination are recommended for individuals with osteoporosis to strengthen the core, quadriceps, and hip flexors. Different types of exercises can include:
Walking to strengthen the spine and hips.
Walking outside or on a treadmill provides more loading force to the bone.
Planks and push-ups can strengthen the forearm and wrist bones.
Holding a water bottle in each hand and lifting up and down 10 times together or alternating a few times a day.
Side leg lifts can strengthen the hip and forearm bones simultaneously.
Weight training provides the bones with a workout by having them support a weight load.
Any exercise therapy program should be designed by a healthcare provider, physical therapist, and trainer according to the individual’s condition and appropriate for them.
Diet
What goes into the body definitely affects bone health. Calcium and vitamin D are key to bone building, but both are needed as vitamin D is needed to absorb the calcium ingested. Calcium can be found in:
Dairy
Dairy products and non-dairy alternatives are fortified with calcium.
Leafy greens.
Beans.
Almonds.
The recommended daily calcium intake for adults over 50 is 1,200 milligrams.
Vitamin D can come from:
Sunlight
Fish.
Mushrooms.
Fortified milk.
Supplements.
The recommended daily vitamin D intake for adults aged 70 is 15 micrograms and 20 micrograms for individuals over 70.
Studies have found that increasing calcium and vitamin D intake with supplements can help maintain bone health. Talk to a healthcare provider about whether supplements could be beneficial.
Hormone Therapy
Females also naturally produce testosterone, which promotes bone formation. As levels drop with age and negatively impact bone strength, hormone therapy could be recommended. Declining testosterone levels start with women in their 20s and men in their 30s. The typical drop in women is 1% to 3% yearly before menopause and stabilizes somewhat afterward. Female patients at risk of bone loss may be prescribed testosterone in various forms that continuously emit the hormone. The dosage is low, so patients do not experience unwanted hair growth or skin changes. Combined with estrogen, testosterone effectively increases bone growth in female patients. Not everyone is a candidate for hormone therapy, like individuals with a history of breast cancer, heart disease, blood clots, or liver disease. (National Library of Medicine. Medline Plus, 2019)
Making small adjustments can optimize bone health and overall well-being
At Injury Medical Chiropractic and Functional Medicine Clinic, we passionately focus on treating patients’ injuries and chronic pain syndromes to create personalized care plans that improve ability through flexibility, mobility, and agility programs tailored to the individual. Using an integrated approach, our goal is to relieve pain naturally by restoring health and function to the body through Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine protocols. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them, as Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective clinical treatments. We focus on what works for you and strive to better the body through researched methods and total wellness programs.
Chiropractic Care: Movement Medicine
References
Dimet-Wiley, A., Golovko, G., & Watowich, S. J. (2022). One-Year Postfracture Mortality Rate in Older Adults With Hip Fractures Relative to Other Lower Extremity Fractures: Retrospective Cohort Study. JMIR aging, 5(1), e32683. https://doi.org/10.2196/32683
Tran, T. S., Ho-Le, T. P., Bliuc, D., Center, J. R., Blank, R. D., & Nguyen, T. V. (2023). Prevention of Hip Fractures: Trade-off between Minor Benefits to Individuals and Large Benefits to the Community. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research, 38(11), 1594–1602. https://doi.org/10.1002/jbmr.4907
Department of Health and Human Services Office of Disease Prevention and Health Promotion. (2020). Osteoporosis Workgroup. Retrieved from https://health.gov/healthypeople/about/workgroups/osteoporosis-workgroup
National Institute of Arthritis and Musculoskeletal Diseases. (2022). Osteoporosis. Retrieved from https://www.niams.nih.gov/health-topics/osteoporosis
National Library of Medicine. MedlinePlus. (2022). What causes bone loss? Retrieved from https://medlineplus.gov/ency/patientinstructions/000506.htm
National Library of Medicine. MedlinePlus. (2019). Hormone replacement therapy. Retrieved from https://medlineplus.gov/hormonereplacementtherapy.html
How do healthcare professionals in a chiropractic clinic provide a clinical approach to preventing medical errors for individuals in pain?
Introduction
Medical errors resulted in 44,000–98,000 hospitalized American deaths annually, and many more caused catastrophic injuries. (Kohn et al., 2000) This was more than the number of people who died annually from AIDS, breast cancer, and auto accidents at the time. According to later research, the actual number of deaths may be closer to 400,000, placing medical errors as the third most common cause of death in the US. Frequently, these mistakes are not the product of medical professionals who are inherently bad; rather, they are the outcome of systemic issues with the health care system, such as inconsistent provider practice patterns, disjointed insurance networks, underutilization or absence of safety protocols, and uncoordinated care. Today’s article looks at the clinical approach to preventing a medical error in a clinical setting. We discuss associated medical providers specializing in various pretreatments to aid individuals suffering from chronic issues. We also guide our patients by allowing them to ask their associated medical providers very important and intricate questions. Dr. Alex Jimenez, DC, only utilizes this information as an educational service. Disclaimer
Defining Medical Errors
Determining what medical error is the most crucial step in any conversation about preventing medical errors. You might assume this is a very easy chore, but that is only until you delve into the vast array of terminology utilized. Many terms are used synonymously (sometimes mistakenly) since some terminology is interchangeable, and occasionally, the meaning of a term depends on the specialty being discussed.
Even though the healthcare sector stated that patient safety and eliminating or reducing medical errors were priorities, Grober and Bohnen noted as recently as 2005 that they had fallen short in one crucial area: determining the definition of “perhaps the most fundamental question… What is a medical error? A medical error is a failure to complete a planned action in a medical setting. (Grober & Bohnen, 2005) However, none of the terms that one would often identify expressly with a medical error—patients, healthcare, or any other element—are mentioned in this description. Despite this, the definition offers a solid framework for further development. As you can see, that specific definition consists of two parts:
An execution error: A failure to complete a planned action as intended.
A planning error: is a technique that, even with perfect execution, does not produce the desired results.
The concepts of faults of execution and planning errors are insufficient if we are to define a medical error adequately. These may occur anywhere, not only at a medical establishment. The component of medical management must be added. This brings up the idea of unfavorable occurrences, known as adverse events. The most common definition of an adverse event is unintentional harm to patients brought about by medical therapy rather than their underlying disease. This definition has gained international acceptance in one way or another. For example, in Australia, the term incidents are defined as in which harm resulted in a person receiving health care. These consist of infections, injury-causing falls, and issues with prescription drugs and medical equipment. Certain unfavorable occurrences might be avoidable.
Common Types of Medical Errors
The only issue with this notion is that not all negative things happen accidentally or intentionally. Because the patient may ultimately benefit, an expected but tolerated adverse event may occur. During chemotherapy, nausea and hair loss are two examples. In this instance, refusing the recommended treatment would be the only sensible approach to prevent the unpleasant consequence. We thus arrive at the concept of preventable and non-preventable adverse occurrences as we further refine our definition. It isn’t easy to categorize a choice to tolerate one impact when it is determined that a favorable effect will occur simultaneously. But purpose alone isn’t necessarily an excuse. (Patient Safety Network, 2016, para.3) Another example of a planned mistake would be a right foot amputation due to a tumor on the left hand, which would be accepting a known and predicted unfavorable event in the hopes of a beneficial consequence where none has ever arisen before. There is no evidence to support the anticipation of a positive outcome.
Medical errors that cause harm to the patient are typically the focus of our research. Nonetheless, medical mistakes can and do occur when a patient is not harmed. The occurrence of near misses could provide invaluable data when planning how to reduce medical errors in a healthcare facility. Still, the frequency of these events compared to the frequency clinicians report them needs to be investigated. Near misses are medical errors that could have caused harm but did not to the patient, even if the patient is doing well. (Martinez et al., 2017) Why would you acknowledge something that could potentially result in legal action? Consider the scenario where a nurse, for whatever reason, had just been looking at photographs of different medications and was about to provide a medication. Maybe something lingers in her memory, and she decides that’s not how a specific medication looks. Upon checking, she found that the incorrect medicines had been administered. After checking all the paperwork, she fixes the mistake and gives the patient the right prescription. Would it be possible to avoid an error in the future if the administration record included photographs of the proper medication? It is easy to forget that there was a mistake and a chance for harm. That fact remains true regardless of whether we were fortunate enough to find it in time or suffer any negative consequences.
Errors of Outcomes & Process
We need complete data to develop solutions that improve patient safety and decrease medical errors. At the very least, when the patient is in a medical facility, everything that can be done to prevent harm and put them in danger should be reported. Many doctors have determined that using the phrases errors and adverse events was more comprehensive and suitable after reviewing mistakes and adverse events in health care and discussing their strengths and weaknesses in 2003. This combined definition would increase data gathering, including mistakes, close calls, near misses, andactive and latent errors. Additionally, the term adverse events includes terms that usually imply patient harm, such as medical injury and iatrogenic injury. The only thing that remains is determining whether a review board is a suitable body to handle the separation of preventable and non-preventable adverse events.
A sentinel event is an occurrence where reporting to the Joint Commission is required. The Joint Commission states that a sentinel event is an unexpected occurrence involving a serious physical or psychological injury. (“Sentinel Events,” 2004, p.35) There isn’t a choice, as it needs to be documented. Most healthcare facilities, however, do keep their records outlining sentinel incidents and what to do in the event of one to guarantee that the Joint Commission standards are met. This is one of those situations when it’s better to be safe than sorry. Since “serious” is a relative concept, there may be some wriggle room when defending a coworker or an employer. On the other hand, reporting a sentinel event incorrectly is better than failing to report a sentinel event. Failing to disclose can have serious consequences, including career termination.
When considering medical errors, people frequently make the mistake of focusing just on prescription errors. Medication errors are undoubtedly frequent and involve many of the same procedural flaws as other medical errors. Breakdowns in communication, mistakes made during prescription or dispensing, and many other things are possible. But we would be gravely misjudging the issue if we assumed that drug errors are the only cause of harm to a patient. One major challenge in classifying the different medical errors is determining whether to classify the error based on the procedure involved or the consequence. It is acceptable to examine those classifications here, given numerous attempts have been made to develop working definitions that incorporate both the process and the outcome, many of which are based on Lucian Leape’s work from the 1990s.
Enhance Your Lifestyle Today- Video
Analyzing & Preventing Medical Errors
Operative and nonoperative were the two main categories of adverse events that Leape and his colleagues distinguished in this study. (Leape et al., 1991) Operative problems included wound infections, surgical failures, non-technical issues, late complications, and technical difficulties. Nonoperative: headings such as medication-related, misdiagnosed, mistreated, procedure-related, fall, fracture, postpartum, anesthesia-related, neonatal, and a catch-all heading of the system were included under this category of adverse occurrences. Leape also classified errors by pointing out the point of process breakdown. He also categorized these into five headings, which include:
System
Performance
Drug Treatment
Diagnostic
Preventative
Many process faults fall under more than one topic, yet they all help to pinpoint the exact cause of the issue. If more than one physician was engaged in determining the precise areas that need improvement, then additional questioning might be required.
Technically, a medical error can be made by any staff member at a hospital. It is not limited to medical professionals like physicians and nurses. An administrator may unlatch a door, or a cleaning crew member could leave a chemical within a child’s grasp. What matters more than the identity of the perpetrator of the mistake is the reason behind it. What before it? And how can we make sure that doesn’t occur again? After gathering all the above data and much more, it’s time to figure out how to prevent similar errors. As for sentinel events, the Joint Commission has mandated since 1997 that all of these incidents undergo a procedure called Root Cause Analysis (RCA). However, using this procedure for incidents that need to be reported to outside parties would need to be corrected.
What Is A Root Cause Analysis?
RCAs “captured the details as well as the big picture perspective.” They make evaluating systems easier, analyzing whether remedial action is necessary, and tracking trends. (Williams, 2001) What precisely is an RCA, though? By examining the events that led to the error, an RCA can focus on events and processes rather than reviewing or placing blame on specific people. (AHRQ,2017) This is why it is so crucial. An RCA frequently makes use of a tool called the Five Whys. This is the process of continuously asking yourself “why” after you believe you have determined the cause of an issue.
The reason it’s called the “five whys” is because, while five is an excellent starting point, you should always question why until you identify the underlying cause of the problem. Asking why repeatedly could reveal many process faults at different stages, but you should keep asking why about every aspect of the issue until you run out of other things that could be adjusted to provide a desirable result. However, different tools besides this one can be utilized in a root cause investigation. Numerous others exist. RCAs must be multidisciplinary and consistent and involve all parties involved in the error to avoid misunderstandings or inaccurate reporting of occurrences.
Conclusion
Medical errors in healthcare institutions are frequent and mostly unreported events that seriously threaten patients’ health. Up to a quarter of a million individuals are thought to pass away each year as a result of medical blunders. These statistics are unacceptable in a time when patient safety is supposedly the top priority, but not much is being done to alter practices. If medical errors are accurately defined and the root cause of the problem is found without assigning blame to specific staff members, this is unnecessary. Essential changes can be made when fundamental causes of system or process faults are correctly identified. A consistent, multidisciplinary approach to root cause analysis that uses frameworks like the five whys to delve down until all issues and defects are revealed is a helpful tool. Although it is now necessary for the wake of sentinel events, the Root Cause Analysis may and should be applied to all mistake causes, including near misses.
Kohn, L. T., Corrigan, J., Donaldson, M. S., & Institute of Medicine (U.S.). Committee on Quality of Health Care in America. (2000). To err is human : building a safer health system. National Academy Press. http://books.nap.edu/books/0309068371/html/index.html
Leape, L. L., Brennan, T. A., Laird, N., Lawthers, A. G., Localio, A. R., Barnes, B. A., Hebert, L., Newhouse, J. P., Weiler, P. C., & Hiatt, H. (1991). The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med, 324(6), 377-384. https://doi.org/10.1056/NEJM199102073240605
Martinez, W., Lehmann, L. S., Hu, Y. Y., Desai, S. P., & Shapiro, J. (2017). Processes for Identifying and Reviewing Adverse Events and Near Misses at an Academic Medical Center. Jt Comm J Qual Patient Saf, 43(1), 5-15. https://doi.org/10.1016/j.jcjq.2016.11.001
For individuals who are dealing with back pain and problems, could knowing how to improve and maintain intervertebral disc health help alleviate symptoms?
Intervertebral Disc Health
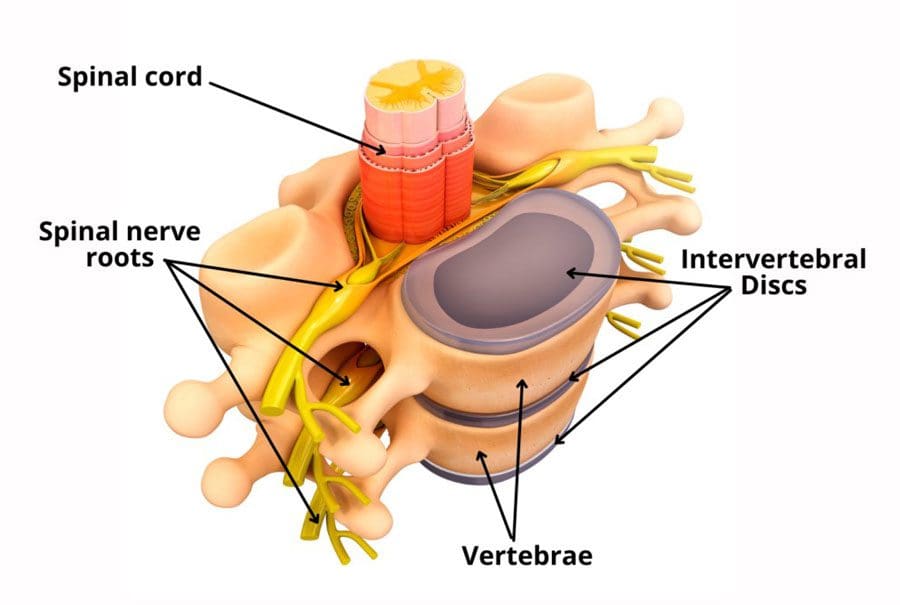
The spinal column comprises 24 movable bones and 33 bones called vertebrae. The vertebral bones are stacked on top of each other. The intervertebral disc is the cushioning substance between the adjacent bones. (Dartmouth. 2008)
Bones
The vertebral bones are small and round in an area called the vertebral body. In the back is a bony ring from which protrusions extend and arches and pathways are formed. Each structure has one or more purposes and includes: (Waxenbaum JA, Reddy V, Williams C, et al., 2023)
Stabilizing the spine.
Providing a space for the connective tissue and back muscles to attach.
Providing a tunnel for the spinal cord to pass through cleanly.
Providing a space where nerves exit and branch out to all areas of the body.
Structure
The intervertebral disc is the cushioning that sits between the vertebrae. The design of the spine allows it to move in various directions:
Flexion or bending
Extension or arching
Tilting and rotation or twisting.
Powerful forces act upon and influence the spinal column to produce these movements. The intervertebral disc absorbs shock during movement and protects the vertebrae and spinal cord from injury and/or trauma.
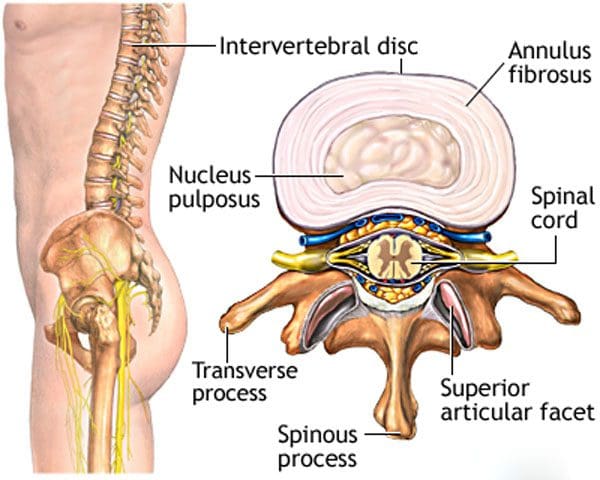
Ability
On the outside, strong woven fiber tissues form an area called the annulus fibrosis. The annulus fibrosis contains and protects the softer gel substance in the center, the nucleus pulposus. (Y.S. Nosikova et al., 2012) The nucleus pulposis provides shock absorption, flexibility, and pliability, especially under pressure during spinal movement.
Mechanics
The nucleus pulposus is a soft gel substance located in the center of the disc that allows elasticity and flexibility under stress forces to absorb compression. (Nedresky D, Reddy V, Singh G. 2024) The swivel action alters the tilt and rotation of the vertebra above and below, buffering the effects of spinal motion. The discs swivel in response to the direction the spine moves. The nucleus pulposus is made mostly of water, which moves in and out through small pores, acting as byways between the vertebra and disc bone. Body positions that load the spine, like sitting and standing, push the water out of the disc. Lying down on the back or in a supine position facilitates water restoration into the disc. As the body ages, the discs lose water/dehydrate, leading to disc degeneration. The intervertebral disc has no blood supply, which means that for a disc to receive necessary nutrition and for waste removal, it must rely on water circulation to stay healthy.
Care
Some ways of maintaining intervertebral disc health include:
Paying attention to posture.
Changing positions frequently throughout the day.
Exercising and moving around.
Applying correct body mechanics to physical activities.
Sleeping on a supportive mattress.
Drinking plenty of water.
Eating healthy.
Maintaining a healthy weight.
Drinking alcohol in moderation.
Quitting smoking.
At Injury Medical Chiropractic and Functional Medicine Clinic, we treat injuries and chronic pain syndromes by improving an individual’s ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. Our chiropractic team, care plans, and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Acupuncture, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Beyond the Surface: Understanding the Effects of Personal Injury
References
Dartmouth Ronan O’Rahilly, MD. (2008). Basic Human Anatomy. Chapter 39: The vertebral column. In D. Rand Swenson, MD, PhD (Ed.), BASIC HUMAN ANATOMY A Regional Study of Human Structure. W.B. Saunders. https://humananatomy.host.dartmouth.edu/BHA/public_html/part_7/chapter_39.html
Waxenbaum, J. A., Reddy, V., Williams, C., & Futterman, B. (2024). Anatomy, Back, Lumbar Vertebrae. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/29083618
Nosikova, Y. S., Santerre, J. P., Grynpas, M., Gibson, G., & Kandel, R. A. (2012). Characterization of the annulus fibrosus-vertebral body interface: identification of new structural features. Journal of anatomy, 221(6), 577–589. https://doi.org/10.1111/j.1469-7580.2012.01537.x
Nedresky D, Reddy V, Singh G. (2024). Anatomy, Back, Nucleus Pulposus. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30570994
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine













 Ability
Ability





