High school football takes a toll on the body. The sport can cause all kinds of injuries that can range from mild – severe. Areas that are commonly injured include:
Head
Neck
Shoulder
Arms
Hands
Spine
Legs
Knees
Ankles
Feet
Chiropractic has become a medically recommended form of treatment and rehabilitation for these injuries but also injury prevention. Today all NFL teams utilize a chiropractic team for players and staff. College teams are also discovering the benefits that chiropractic offers. There are significant benefits that high school football players can attain from chiropractic care.
Enhanced Mobility
A chiropractic adjustment, technically known as chiropractic manipulative treatment/CMT, is a primary therapy in sports medicine. It helps to increase flexibility and minimize or eliminate pain during motion/movement. Adjustments have been shown to improve athletic performance.
Injury Prevention
Athletes who regularly use chiropractic experience a decline in sports-related injuries.
Treatment increases flexibility and mobility, allowing for optimal agility that has been linked to preventing injuries. This is because the body is relaxed and stays loose, even when tackled, instead of tensing up, which is a major contributor to strains and injuries.
Enhanced Strength
Chiropractic adjustments also help increase muscular strength, making the body stronger, and more resistant to injury. It has been shown to promote strength in the muscles after a few sessions effectively. The strengthened muscles also help avoid injury by being able to withstand the hits and recover faster. The strengthened body also helps to increase endurance and stamina.
Pain Relief
Many high school players use chiropractic to ease the general pain that comes from general practice and games. Adjustments and massage are highly effective for pain management and alleviate headaches, especially those that come from constant impact to the head and neck. It helps to alleviate soreness, stiffness, and pain from the entire body.
Sports Hernia
Athletes often experience athletic pubalgia. This is one of the most common causes of injury-related groin pain. Chiropractic can relieve the discomfort within 8 weeks in combination with rehabilitative stretches and exercises. Chiropractic plays a critical role in whole-body care, pain relief and keeps the body operating and performing at the highest level.
Body Composition
Water Intoxication
When an individual overwhelms their body’s ability to excrete water and waste products consumed, water intoxication can develop. Water intoxication causes disturbances in the body’s electrolyte balance. This can cause a life-threatening condition known as hyponatremia. With a rapid decrease in the sodium levels in the blood, relative to the amount of water, symptoms can develop rapidly:
If left untreated, later symptoms can develop into:
Seizures
Coma
Death
References
Hession, E F, and G D Donald. “Treatment of multiple lumbar disk herniations in an adolescent athlete utilizing flexion distraction and rotational manipulation.” Journal of manipulative and physiological therapeutics vol. 16,3 (1993): 185-92.
Pritchett, J W. “A statistical study of physician care patterns in high school football injuries.” The American journal of sports medicine vol. 10,2 (1982): 96-9. doi:10.1177/036354658201000206
Shane, Eric R et al. “Sports chiropractic management of concussions using the Sports Concussion Assessment Tool 2 symptom scoring, serial examinations, and graded return to play protocol: a retrospective case series.” Journal of chiropractic medicine vol. 12,4 (2013): 252-9. doi:10.1016/j.jcm.2013.08.001
Triathlon training involves running, biking, and swimming. This much fitness training takes a toll on the body. Pulled hamstrings, twisted ankles, and sore heels are common, but triathlon training can also cause or worsen back pain. Because the back muscles are connected to many other muscles, certain types of movement after a tough training session can present with back pain. There was an Ironman triathlete study that found that 90% of the athletes suffered some form of soft-tissue injury during training, with 70% reporting low back pain and/or sciatica. A 2020 study in BMC Musculoskeletal Disorders found that 14% of recreational half-marathon runners presented with low-back pain.
Triathlon Training Hard on the Back
High-impact activities/exercises, constant repetitive motion, places a heavy pounding on the body that impacts the joints and spine. Using improper techniques will aggravate any issues. The stresses applied from repetitive motions, and poor form can lead to the joints breaking down. If new to intense training the muscles might not be strong enough yet, which could also cause back pain and injury. The back stabilizer muscles tend to get neglected in the training, but these muscles support the structures in the midline, spine, and joints. Strengthening the:
Ensures stability of the spine and joints from all the wear and tear.
Training and Overtraining Errors
Even veteran athletes can make mistakes during their training that can lead to sore backs. The biggest mistake individuals make during triathlon training is that they only swim, bike, and run. Training for the specific sport/s is important; but weight lifting, core strengthening, and flexibility training are just as important. Proper rest can become neglected as the individual wants to get in as much training as possible that often gets overlooked, leading to overuse injuries. However, rest is a vital part of training to allow the body to fully recover and operate at full and optimal potential.
Preventing and Avoiding Back Pain When Training
How to sidestep back pain altogether during training includes:
Sleep
A healthy lifestyle includes proper sleep cycles and is even more important during training. The mental aspects a triathlon competition can create require proper rest. Fatigue can also lead to poor technique/form, placing excess stress on the joints and the spine, leading to injury.
Flexibility
Muscles need to maintain flexibility to preserve function and recovery ability. After a training session stretching and working on flexibility will help with overall performance. Stretching should be done after activity when the muscles are warm, and the fibers can be stretched/elongated for optimal recovery.
Proper nutrition
The body needs high-performance fuel to support high-calorie deficits that are associated with intense training and competition.
Strengthening the body
Having a solid body foundation is the objective. Everything is balanced with strong muscles supporting healthy bones. Specific exercises that target the multifidus muscles. These are the body’s back brace. Strengthening these muscles will help prevent spinal injury/s. Back-strengthening exercises include:
Plan rest days no matter what. Pushing through will not make the body stronger or able to perform better, and could cause performance to decrease leading to injury. This does not mean sleeping all day, but engaging in active recovery where the body gets the rest it needs while still maintaining fitness. Active recovery includes:
Allows for a thorough recovery and enhances training.
Technique Improvement
Proper form and technique can really make the difference between staying injury-free and injury/s. Using the right form promotes healthy function. It could help to have gait, swim stroke, and bike techniques evaluated by a professional to ensure that proper form is being utilized.
Body awareness
Stop if the body signals one to stop. This is why the body feels pain. It is the internal mechanism that tells the individual something is wrong. It is not recommended to follow the phrases train through the pain, and no pain, no gain. Individuals are recommended to:
Always pay attention if pain presents and does not go away after exercising or warming up.
Pain that limits function.
Pain that interferes with daily activities.
These could significantly exacerbate a spinal injury and should be checked by a doctor.
Body Composition
Rest and Recovery
During rest and recovery, the body goes back to normal or homeostasis. This is the body’s resting rate or normal phase. The body is always trying to go back to homeostasis. This is done by:
Maintaining core temperature
Blood pressure stable
Muscles refreshed
When exercising/training, the homeostasis phase is disturbed, meaning the body needs a period of rest to return to normal. The process of homeostasis uses a lot of energy, which results in an abundant amount of calories burned. After exercise, there is an increase in excess post-exercise oxygen consumption or EPOC. The body uses up more oxygen during recovery than it does before or during exercise. This increase results in burned calories and strong muscles. The most important part of recovery is the rebuilding of muscle. When working out, especially resistance training, tiny tears are made in the muscle fibers. For the tiny tears to turn into growing muscles, they need to repair themselves. This happens during rest. Apart from the physiological benefits, rest helps prevent injury caused by overuse and assists in healing when injuries do occur. Time off helps with mental health as well to refocus, reassess, and apply what has been learned. What rest and recovery can do for the body includes:
Burn massive calories
Build muscle
Refuels the muscles
Prevents injury
Improves mental health and motivation
References
American journal of physical medicine & rehabilitation/Association of Academic Physiatrists. (October 2014) “Efficacy of Aerobic Exercise for Treatment of Chronic Low Back Pain: A Meta-Analysis” https://www.researchgate.net/publication/266682158_Efficacy_of_Aerobic_Exercise_for_Treatment_of_Chronic_Low_Back_Pain_A_Meta-Analysis
Stretch Before and After Journal of Chiropractic Medicine. (Winter 2003) “Changes in low back pain in a long-distance runner after stretching the iliotibial band” https://www.sciencedirect.com/science/article/pii/S0899346707600718
Finding the right physical activity that elevates heart rate and maintains it for 30 minutes a day increases the amount of oxygen delivered to the heart, brain, and muscles. Some form of aerobic activity will keep individuals moving in a healthy direction. This benefits the:
Heart
Muscles
Mood
Self-esteem
Amount of energy
It helps to lower:
Blood pressure
Cholesterol
Blood sugar
Body fat
Anxiety
Depression
Fatigue
Finding What Works For You
Doctors and health experts agree that individuals need to perform normal/moderate activity balanced with vigorous/intense activity. Some ideas for both types include:
Sports – soccer, field hockey, tennis, basketball, flag football, volleyball
Hiking
Cycling
Mountain biking
Skating and skateboarding
Horseback riding
House and Yard Work/Chores
Moderate house and yard work exercises:
Sweeping
Vacuuming
Mopping
Washing the car by hand
Sweeping the garage, walkways, sidewalk, or patio
Mowing the lawn
Raking the lawn
Labor intense gardening
Vigorous house and yard work exercises:
Shoveling dirt, rocks, etc
Carrying groceries upstairs
Carrying boxes
Moving furniture
Cleaning and organizing the house
Mix it up
Finding the activities that work for you are important. But mix them up, so you don’t get bored and tired of them. For example, if getting bored with walking, try a light aerobics class, dancing, or something similar.
Try new routes for walking and biking.
Change the room for exercising or stretching.
Exercise at different times, so it doesn’t just become a chore.
Mix up the amount of time exercising. Do a full 30 minute or longer workout one day, then break the workout into smaller 15, 10, 5-minute workouts other days.
Having options allows you to pick and choose what suits your mood and schedule.
Job Physical Activity
If job occupation includes sitting for long periods, try adding short bursts of activity throughout the day:
If the commute permits, walk, jog, or bicycle to work.
Park several blocks away or the furthest in the parking lot to get some walking in.
Use the stairs instead of the elevator for a few floors.
Get coffee or use the bathroom on another floor using the stairs the farthest from the office.
Need to talk to a coworker, take a walk to their office or station instead of e-mail or phone.
Finding breaks to take quick walks and stretch out.
Get Involved In Competition
Competition can motivate individuals as it:
Requires specific and measurable goals to work toward. An example could be training to walk or run a race.
Learning the details of an event and preparing/training can generate or restore the excitement and challenge of the activity.
Instead of entering a competition, an individual can help with organizing and planning. This can provide friendship with other individuals interested in the same activity that can lead to working out together and staying motivated.
CrossFit Training
CrossFit training is a combination of various exercises to work out various muscle groups. CrossFit can be beneficial because:
It prevents boredom by providing a variety of workouts.
It helps maintain balance among various muscle groups.
For example, runners that have powerful leg muscles cross-train to strengthen the upper body.
It reduces the risk of injuries because the combination of exercises allows muscles to recover while working out a different set of muscles.
Whatever the case, it’s all about finding what works for you. But the objective is to keep the body moving to maintain overall health.
Body Composition
Why the brain needs sugar?
The brain needs half of the body’s energy supply because of its complex system. The brain needs glucose for brain cell energy. As neurons cannot store energy, they need a constant fuel supply to function properly. The ability to think, learn and recall information is connected with the body’s glucose levels. When blood glucose levels are low, the ability to think clearly is slowed down as the production of neurotransmitters is reduced, leading to communication disruption. Natural sugars can increase brain health for optimal functioning. When consuming naturally occurring sugar like apples and bananas, sugar is released incrementally into the bloodstream. This maintains energy levels at a steady pace, and the body does not crave more sugar.
References
Berg JM, Tymoczko JL, Stryer L. Biochemistry. 5th edition. New York: W H Freeman; 2002. Section 30.2, Each Organ Has a Unique Metabolic Profile. Available from: https://www.ncbi.nlm.nih.gov/books/NBK22436/
Ainsworth BE, et al. (2011). Compendium of Physical Activities Tracking Guide. Columbia, SC: Prevention Research Center, Norman J. Arnold School of Public Health, University of South Carolina. Available online: http://prevention.sph.sc.edu/tools/compendium.htm.
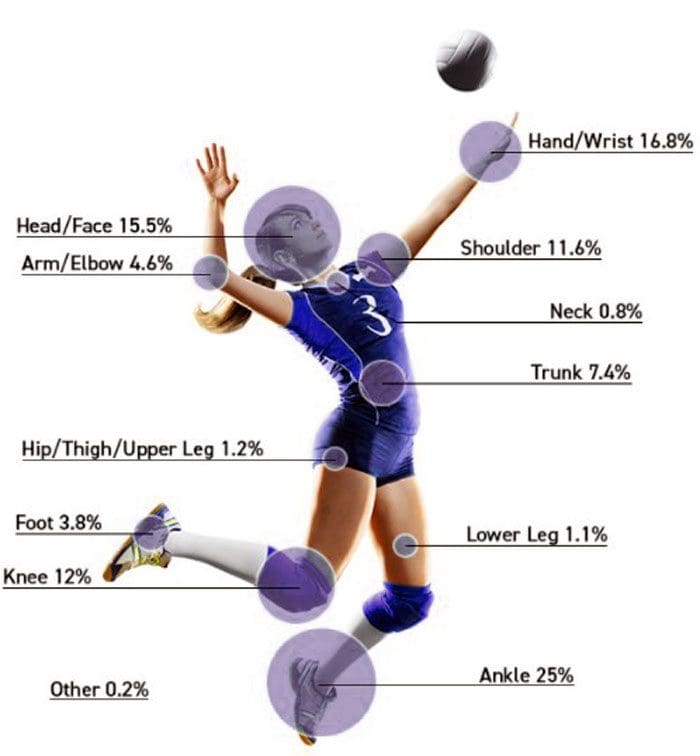
Around a half-million high school students in the U.S. play volleyball. Whether the parent of a volleyball player or part of a recreational league, the goal is to be ready for the season, which means preventing and addressing volleyball injuries. It is a highly demanding sport with quick movements, jumping, twisting, diving, spiking, etc. Despite being fit and healthy, extensive training along with match play takes a toll on the body. Chiropractic can benefit volleyball players.
Common Volleyball Injuries
Why Chiropractic Works
Chiropractic treatment and rehabilitation, especially by a sports chiropractor, is recommended for volleyball injuries because it addresses acute and chronic injuries to all areas of the body. Chiropractic treats the entire musculoskeletal system. Proper joint alignment from chiropractic adjustments in the spine and throughout the body maintains the biomechanic integrity. This reduces high-impact forces in the joints. Soft tissue treatments like instrument-assisted soft tissue mobilization can help resolve injuries by providing the tissues with more blood flow into the affected area allowing for faster healing. Most volleyball injuries result from overuse to the joints and muscles, resulting in repetitive strain. In volleyball, repetitive/overuse injuries are common in the knees, ankles, and shoulders. This comes from all the jumping, serving, and spiking.
Player Benefits
Body Soreness Is Reduced/Alleviated
Many athletes, including volleyball players, do not get the proper recovery time from training or playing.
Reduced recovery periods cause body soreness and stiffness that can overlap into an injury.
Chiropractic can reduce and alleviate body soreness.
Chiropractic promotes faster recovery.
Optimal Performance
Studies show that athletes that receive regular chiropractic care found speed and mobility performance enhanced.
Athletes require fast reflexes and optimal hand-eye coordination.
Speed, mobility, reflexes, and coordination depend on a healthy nervous system.
90% of the central nervous system travels through the spine.
Spinal alignment can either allow for proper nerve flow or disrupt nerve flow.
Even when just one spinal segment is misaligned and out of place, the nervous system can impact reflexes, speed, mobility, and hand-eye coordination.
A properly functioning spine and nervous system will ensure the player is at their best.
Faster Injury Recovery Time
Healing the body properly takes time. Just like the body needs sleep/rest to function properly, so it is with injuries.
The issue for athletes is how much time healing takes.
Individual athletes receiving chiropractic care have been shown to heal faster.
Mobility and Strength
A chiropractic doctor can reduce the pressure around the nerve roots that exit the spine, which will help improve player performance. This includes:
Range of motion
Mobility and flexibility
Strength
Endurance
To find out how chiropractic can help, contact Injury Medical Chiropractic and Functional Medicine Clinic. We will perform a thorough musculoskeletal and nervous system examination.
Ankle Sprain Treatment
How Many Calories Over 24 hours
Myths that offer strategies that avoid the hard work and commitment that diet and exercise demand should be avoided. Individuals cannot expect to experience healthy body composition changes by increasing/decreasing meal frequency if they are living a sedentary lifestyle. It is not important how often or what time an individual takes in calories (has a meal). What is important is how many calories an individual has over a 24-hour period. A study looked at healthy individuals that ate one large meal a day for two weeks and then later ate the same meal but spread out over five smaller meals for another two weeks. It was concluded that there was no statistical difference in body weight gain or loss between the two eating methods. 2000 calories over 3 meals is the same 2000 calories consumed over 5 meals. There is no substitute for proper diet and exercise. The focus should be on what and how much you eat.
References
Eerkes, Kevin. “Volleyball injuries.” Current sports medicine reports vol. 11,5 (2012): 251-6. doi:10.1249/JSR.0b013e3182699037
Gouttebarge, Vincent et al. “Preventing musculoskeletal injuries among recreational adult volleyball players: design of a randomized prospective controlled trial.” BMC musculoskeletal disorders vol. 18,1 333. 2 Aug. 2017, doi:10.1186/s12891-017-1699-6
Kilic, O et al. “Incidence, etiology, and prevention of musculoskeletal injuries in volleyball: A systematic review of the literature.” European journal of sports science vol. 17,6 (2017): 765-793. doi:10.1080/17461391.2017.1306114
Seminati, Elena, and Alberto Enrico Minetti. “Overuse in volleyball training/practice: A review on the shoulder and spine-related injuries.” European journal of sports science vol. 13,6 (2013): 732-43. doi:10.1080/17461391.2013.773090
Wolfram, G et al. “Thermogenese des menschen bei unterschiedlicher mahlzeitenhäufigkeit” [Thermogenesis in humans after varying meal time frequency]. Annals of nutrition & metabolism vol. 31,2 (1987): 88-97. doi:10.1159/000177255
When back pain presents for a prolonged period, the back muscles reduce in mass but increase fat content, resulting in more stiffness. This leads to chronic muscle fatigue and results in chronic pain symptoms. Adding resistance to a workout routine in weight machines, free weights, and/or resistance bands helps reduce back pain. Studies have shown that specific therapeutic back muscle weight training is safe and can help relieve pain. A sports chiropractic specialist can recommend appropriate exercises for individuals and their specific condition/s to safely participate in strength training.
Back muscles development
With time, back pain and increased fatigue can lead to a fear of moving the body and engaging in physical activity. This results in spinal deconditioning and instability. Weight training works on incrementally/progressively increasing the load that the back muscles can tolerate. This technique gradually improves the body’s ability and strength to perform regular daily activities without strain and in optimal fashion. Weight training improves whole-body health because:
Back muscles and core muscles increase in function and performance.
Muscles are strengthened.
Lean muscle mass increases.
The range of motion of the spine increases.
Body fat decreases.
Guidelines while using weights
When weight training, it is important to understand safety guidelines to help relieve back pain and not worsen or cause further injury. Weighted treatment exercises are for individuals that have been cleared by their physician or chiropractor and are specific to their injury and /or condition. Depending on the underlying pain source, weight training may not be suitable for individuals that have:
Severe pain.
Back pain that originates from:
Previous spinal surgery
Tumor
Nerve root compression
Neurological symptoms
Sciatica
Spinal fracture/s
Spinal infection/s
Medical professionals and chiropractors can accurately diagnose and determine if weight training is safe and which specific exercises to perform. Guidance from a trained therapist or therapeutic trainer is recommended for optimal results.
Weight training techniques to alleviate back pain are different from regular weight or resistance exercises.
Trained physical/occupational therapists and sports chiropractors can educate an individual on:
Correct techniques
Frequency
Type of training that will help an individual’s condition.
Therapeutic training can significantly reduce the risk of further injury and damage to the spine.
After initial training, individuals are encouraged to exercise to maintain back muscles and total body health.
Smaller weights build strength progressively
Effective ways to strengthen the spine.
Begin with small/light weights and exercise slowly.
Fast rapid movements or incorrect lifting and pulling techniques can cause additional damage to the tissues.
It is recommended to start with:
Low-load motor control exercises without weights activate and stretch the muscles and improve balance.
Simple stretches
Exercise machines can be recommended instead of free weights.
Exercise machines can provide safe, effective, and progressive resistance to the exercises.
The machines can help reduce/prevent injury compared to free weights.
The machines can maintain proper support on the back and spine.
It is recommended to combine regular walking activity with a weight training program.
Low impact aerobic exercises increase blood circulation along with essential nutrients to the muscles and soft tissues.
This promotes healing and reduces stiffness.
Training program and benefits
Gaining the most benefits from strength training, tips to keep in mind:
Warm up for a few minutes using heat therapy and simple stretches.
Try for 2 or 3 times a week for 30 minutes.
Focus on building strength in the core muscles – back, abdominals, obliques, buttocks, and pelvic leg muscles.
There is no need to join a gym or buy expensive equipment.
Work out at home with small hand weights, resistance bands, and body weight.
The therapist or chiropractor will inform the individual on which exercises to avoid, which require extreme or quick moves.
Slow, steady resistance training takes advantage of muscle lengthening exercises and muscle shortening exercises for strengthening.
If back pain presents with a sustained increase, take time off or modify the strength training exercises.
Some soreness is to be expected, but sharp pain is not. If any sharp, sudden pain presents while exercising, stop immediately.
Ice therapy can be beneficial after exercising to decrease inflammation and alleviate pain.
Record the amount of weight when beginning the training and note when progressing to a heavier weight. Consistent improvements in pain, flexibility, strength, and function will help maintain motivation. Consult with a professional sports injury chiropractor today to see if weight training is a suitable and safe treatment.
Body Composition
Carbohydrates and Muscle Growth
Simple carbs are a quick, periodic source of energy. Complex carbs are a recommended source of steady energy. Complex carbs are not as readily available for immediate energy as simple carbs are but are more efficient and healthier. Complex carbs offer sustainable energy, meaning the energy is constant with no crash like simple carbs. Because complex carbs have slow-release properties, they should be the largest component of daily energy consumption.
Carbs prevent muscle weakness.
Some glycogen is stored in the muscles. When those muscles are used during exercise, the body taps into the glycogen stores in that specific muscle. Lifting weights with the arms, for example, access the glycogen in the biceps. Athletes take advantage of glycogen by loading up on carbs by consuming a day or more before a workout. This maximizes the muscle glycogen stores. This delays muscle fatigue, making for a better workout and stronger muscles, and can improve athletic performance.
Carbs help muscles recover after exercise.
Recovery goes back to the glycogen stores. Right after exercising, the body needs to replenish its glycogen stores to prevent glycogen depletion. Glycogen depletion, when the stores run out, causes gluconeogenesis. What happens is the body forms glucose from new sources. This is to compensate for the lack of glucose from carbohydrates. This is when the body turns to sources like fat and protein to fill the need. Protein is the last line of defense when energy is required, meaning that energy is running low. When the body breaks down protein for glucose production, it takes what it needs from the muscle/s, causing them to shrink and break down.
References
Dreisinger TE. Exercise in the management of chronic back pain. Ochsner J. 2014;14(1):101–107.
Lee JS, Kang SJ. Strength exercise and walking effects on lumbar function, pain level, and body composition in chronic back pain patients. J Exerc Rehabil. 2016;12(5):463–470. Published 2016 Oct 31. doi:10.12965/jer.1632650.325
Michaelson P, Holmberg D, Aasa B, Aasa U. High load lifting exercise and low load motor control exercises as interventions for patients with mechanical low back pain: A randomized controlled trial with 24-month follow-up. J Rehabil Med. 2016;48(5):456-63.
Welch N, Moran K, Antony J, et al. The effects of a free-weight-based resistance training intervention on pain, squat biomechanics, and MRI-defined lumbar fat infiltration and functional cross-sectional area in those with chronic low back. BMJ Open Sport Exerc Med. 2015;1(1):e000050. Published 2015 Nov 9. doi:10.1136/bmjsem-2015-000050
Poor spinal health in adolescence can lead to chronic pain in adulthood. Teenagers, just like adults, can experience back pain from accidents, sports injuries, a sedentary lifestyle, part-time jobs, chores, etc. However, sitting too long in school along with heavy backpacks can also contribute to compromised spinal health. Chiropractic professionals can help these young individuals address and prevent spinal issues/injuries to maintain a healthy spine.
Teenagers Spine Issues
If discomfort or pain is present, much push through, as they and their spines are young. There are common spinal dysfunctions that teens and parents should be aware of. These include:
Disc injuries
Teenagers can put a serious strain on the spine from various forms of physical activity, jumping, dancing, and playing. This pressure gets transmitted through the spine. During a teenager’s development, this can result in permanent disc damage.
Scoliosis
A spinal deformity or exaggerated curvature of the spine is common and affects young children and teens. It usually happens during the growth spurt just before puberty. This is why it is important to have a teenager’s spine checked regularly and analyzed for signs/symptoms of scoliosis.
Spondylolysis
This condition is often associated with sports injuries. It happens when teenagers overextend/overreach their backs. It’s most common in gymnastics, weight lifting, tennis, football, diving, and other similar sports.
Protection and Prevention
There are several ways that parents and healthcare providers can help teenagers make healthy decisions to achieve and maintain optimal spinal health.
Sitting less, moving more.
Children are taught to sit from a very young age. In school, watching t.v., or doing homework, teenagers spend more time sitting than their bodies should. Teenagers need to stand, walk and move around just like adults to protect their spines from degeneration and injury.
Playing sports is healthy. However, there is a risk associated with teen sports. Although they are taught to play safely, encourage them to continue to educate themselves about sports injuries and know how to address them.
Chiropractic Support
At Injury Medical Chiropractic and Functional Medicine Clinic, we’re committed to helping young adults and adolescents overcome and prevent spinal injuries that could turn into chronic pain conditions. We are continually developing our chiropractic, and physical therapy treatment approaches to achieve optimal results.
Body Composition
Sleep and Growth Hormone In Children
Growth hormones primarily control growth. The hypothalamus and the pituitary gland regulate this hormone. Sleep plays an important role in the proper function of these glands. A review showed that:
Growth hormone levels rise and peak at the onset of deep sleep
Multiple but smaller peaks were seen during other sleep stages
Individuals that have a delay in the onset of deep sleep have delayed peaks in growth hormone levels
For children to grow properly, they need to have adequate levels of growth hormone. This means they need to have a sufficient amount of sleep. The proper amount of sleep is vital for healthy body composition. A study measured the body composition of preschool-aged children. The study found that children who had proper sleep levels had less overall fat mass and reduced body fat. Children and teenagers need to get the proper amounts of sleep for their bodies to grow healthily.
References
Clement, R Carter et al. “What are normal radiographic spine and shoulder balance parameters among adolescent patients?.” Spine deformity vol. 8,4 (2020): 621-627. doi:10.1007/s43390-020-00074-9
Driehuis, Femke et al. “Spinal manual therapy in infants, children and adolescents: A systematic review and meta-analysis on treatment indication, technique, and outcomes.” PloS one vol. 14,6 e0218940. 25 Jun. 2019, doi:10.1371/journal.pone.0218940
Manansala, Christian et al. “Change in young people’s spine pain following chiropractic care at a publicly funded healthcare facility in Canada.” Complementary therapies in clinical practice vol. 35 (2019): 301-307. doi:10.1016/j.ctcp.2019.03.013
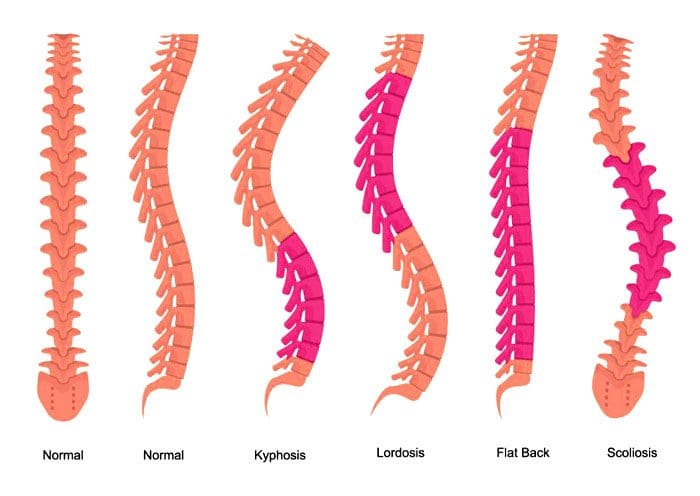
A non-invasive method of treating scoliosis. Yoga Has Been Shown To Help Reverse Scoliosis. Scoliosis is the lateral curvature of the spine. The spine bends inward toward the front of the body at the neck region and lower back region. This curve is known as lordosis and bows outward in the middle-back region. This is known as kyphosis. If the spine curves to the side, this could indicate curvature that could be scoliosis. It can be painful and often can affect an individual’s appearance once the measurement goes beyond 25 – 30 degrees. One shoulder is usually higher than the other, and clothing cannot fit properly. If the curve goes beyond 60 degrees, it can affect breathing and cardiac function.
Idiopathic Causes Unknown
This condition can consist of various components, especially with more intense curves. The ribs can shift backward on the side where the curve bulges. Most cases consist of adolescent idiopathic (without a known cause) scoliosis. Because the cause is unknown, there are not a variety of effective treatment besides surgery. Physicians carefully keep an eye for:
Curves under 25 degrees.
Bracing between 25 and 45 degrees.
Consider surgery for intense curvature.
Curves in individuals typically appear between 12 and 20 years old.
Yoga Shown To Reverse Scoliosis
Individuals are recommended to do just one yoga pose daily. However, depending on the type and severity of the curves, it could be more than one. They are asked to perform the pose for 5 minutes or less, depending on the condition. A yoga therapist, chiropractor, and physical therapist can generate significant spinal improvement. This could mean that a curve of 30 degrees could be reduced to around 18 degrees in 10-12 months. Individuals that do the poses at least 4 times a week have shown 80-90% improvement. The pose can be done at work during breaks, etc.
The biggest advantage of this technique is that it is non-invasive; it can help individuals with developing curves, reversing the curvature early. Most curves do not reach the point of surgery. In late adolescence and teen years, the spine is still quite flexible. This can help accelerate the effectiveness of the yoga pose to straighten the spine. The technique reduces the curve from worsening. X-rays will show if the curvature has improved or not. Patients could be asked to do the pose/s twice or more daily depending on the direction the condition is taking.
Body Composition
Gluten Effects
Gluten causes digestive issues for individuals that have celiac disease or autoimmune thyroid disease. Individuals with these conditions could experience a variety of uncomfortable and/or painful effects. These symptoms can vary based on their presentation. They fall into classifications.
Classical Celiac Disease
With classical celiac disease, symptoms include:
Diarrhea
Discolored stools
Constipation
Abdominal bloating and pain
Weight loss
However, these symptoms are more common in children than adults. In adults, symptoms are more similar to non-classical celiac disease.
Non-Classical Celiac Disease
With non-classical celiac disease, severe digestive symptoms may not present as classic celiac disease symptoms but develop other symptoms. These include:
Silent celiac disease is less visible. Individuals might not see any symptoms. However, damage to the intestines is still happening from gluten consumption.
Autoimmune Thyroid Disease
Autoimmune Thyroid Disease or ATD. Autoimmune thyroid disease includes conditions like Hashimoto’s disease. This affects the thyroid gland and causes:
Extreme fatigue
Sensitivity to cold
Hair loss
Body aches
Joint aches
Negative health effects
Studies have shown that gluten-free helps alleviate symptoms.
References
Loren M. Fishman, M.D., B.Phil. (oxon). Healing Yoga. (New York: W.W. Norton, 2014).
Loren M. Fishman, M.D., B.Phil. (oxon). “Isometric Yoga-Like Maneuvers Improve Adolescent Idiopathic Scoliosis—A Nonrandomized Control Trial.” Global Advances in Health and Medicine. February 24, 2021. https://journals.sagepub.com/doi/full/10.1177/2164956120988259
Fishman LM, Groessl EJ, Sherman KJ, “Serial Case Reporting Yoga for Idiopathic and Degenerative Scoliosis.” Global Advances in Health and Medicine. September 1, 2014. https://journals.sagepub.com/doi/10.7453/gahmj.2013.064
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine