Can individuals with thoracic outlet syndrome incorporate electroacupuncture to reduce neck pain and restore proper posture?
Introduction
More times throughout the world, many individuals have experienced pain around their necks, which can lead to pain and discomfort. Many environmental factors, like being in a hunched position while looking at the computer or phone, traumatic injuries, poor posture, or spinal issues, can cause pain-like symptoms and complications to the body. Since neck pain is a common complaint many people suffer, symptoms like tingling, numbness, or muscle weakness in the upper extremities can lead to comorbidities. When this happens, it can lead to the development of a complex condition known as thoracic outlet syndrome or TOS. Today’s article looks at the link between thoracic outlet syndrome and neck pain, how to manage TOS while alleviating neck pain, and how electroacupuncture can help with TOS. We talk with certified medical providers who consolidate our patients’ information to assess how to minimize the effects of TOS while reducing neck pain. We also inform and guide patients on how electroacupuncture can help manage TOS. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating electroacupuncture to alleviate TOS associated with the neck. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Link Between Thoracic Outlet Syndrome & Neck Pain
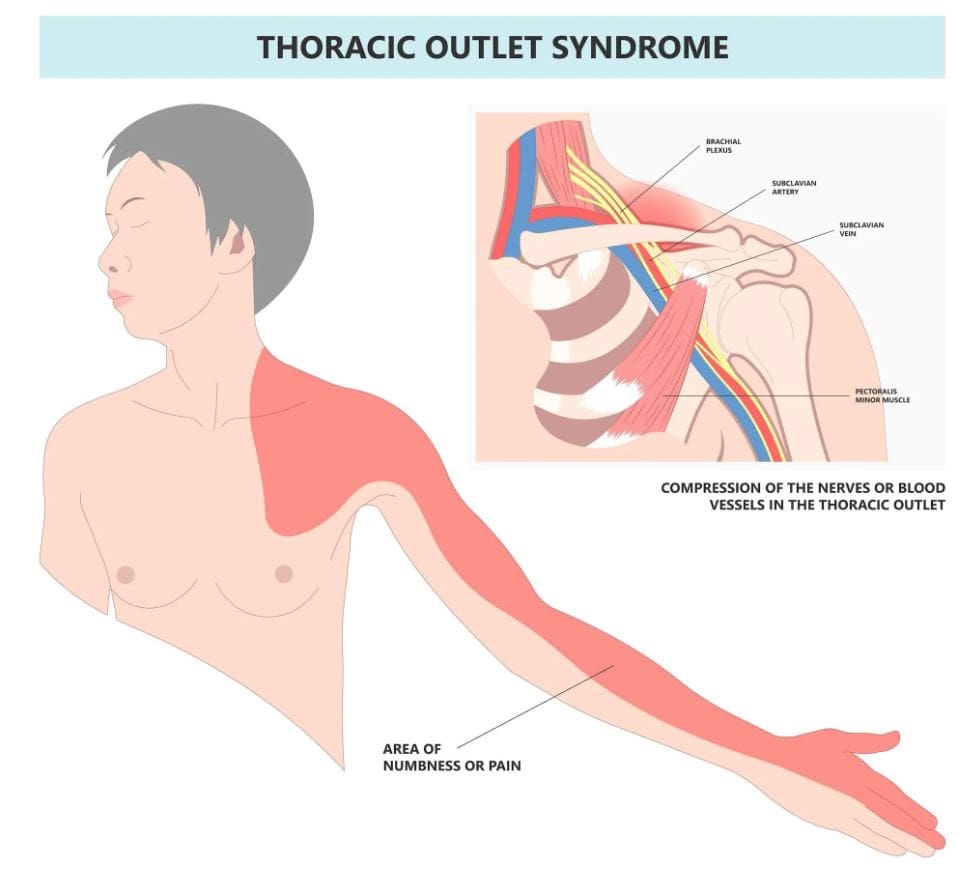
Have you been noticing how you are hunched over more than usual? Do you experience symptoms of tingling or numbness down from your arms to your hands? Or do you feel muscle tension in your neck? Thoracic outlet syndrome, or TOS, is a challenging condition resulting in the compression of neurovascular structures between the clavicle and the first rib. (Masocatto et al., 2019) These neurovascular structures are near the neck and shoulders. When environmental structures affect the upper extremities, it can lead to referred neck pain, which can cause overlapping risk profiles. Some of the factors that TOS can contribute to neck pain include:
Atomical variations
Poor posture
Repetitive motions
Traumatic injuries
At the same time, people with neck pain can develop TOS, as neck pain is a multifactorial musculoskeletal condition that can be associated with overlapping risk profiles that contribute to TOS. (Kazeminasab et al., 2022) As stated earlier, factors like poor posture can overstretch the neck muscles and the neurovascular structures, leading to neuropathic pain symptoms that can cause deep aching referred pain to the neck and muscle weakness. (Childress & Stuek, 2020) When this happens, many people will begin to feel miserable and start to seek treatment to not only reduce TOS but also alleviate neck pain.
What Is Thoracic Outlet Syndrome- Video
Managing TOS & Alleviating Neck Pain
When it comes to treating TOS, especially when neck pain is a significant component, many individuals will try to seek out non-surgical treatments to reduce the symptoms. Many individuals may try physical therapy to stretch and strengthen their shoulder, chest, and neck muscles to relieve compression. Others might try a manual treatment that is joint-oriented for the neck while neural-tissue-oriented for TOS to improve mobilization on the upper extremities and even improve poor posture. (Kuligowski et al., 2021) Additionally, non-surgical treatments can be combined with other therapies to reduce the chances of TOS from returning as they can further increase sensory-motor function back to the neck and upper extremities. (Borrella-Andres et al., 2021)
How Electroacupuncture Can Help With TOS
Electroacupuncture is a modern form of traditional acupuncture that is part of the non-surgical treatments that can help manage TOS while alleviating neck pain. Electroacupuncture is a modification of inserting needles into the body’s acupoints while incorporating electric stimulation to deliver a pulsed electrical current to the affected area gently. (Zhang et al., 2022) Some of the beneficial properties that electrostimulation can provide for TOS include:
Pain reduction by stimulating the release of endorphins to decrease inflammation.
Help relax the affected muscles in the chest and neck to alleviate the pressure on the nerves of the thoracic outlet.
Help enhance the blood flow to reduce vascular compression of TOS.
Help stimulate the nerve pathway to promote healthy nerve function and reduce pain-like symptoms.
By incorporating electroacupuncture and non-surgical treatments to reduce TOS, many individuals can make modifications to their lifestyle habits and prevent issues from affecting their upper body extremities. By utilizing these treatments, many people can listen to their bodies and focus on their health and well-being by addressing the pain-like symptoms they are experiencing from TOS correlating with neck pain. At the same time, they have a positive relationship with their primary doctors to develop a personalized treatment plan that can manage their TOS symptoms to the best outcomes.
References
Borrella-Andres, S., Marques-Garcia, I., Lucha-Lopez, M. O., Fanlo-Mazas, P., Hernandez-Secorun, M., Perez-Bellmunt, A., Tricas-Moreno, J. M., & Hidalgo-Garcia, C. (2021). Manual Therapy as a Management of Cervical Radiculopathy: A Systematic Review. Biomed Res Int, 2021, 9936981. https://doi.org/10.1155/2021/9936981
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Kuligowski, T., Skrzek, A., & Cieslik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health, 18(11). https://doi.org/10.3390/ijerph18116176
Masocatto, N. O., Da-Matta, T., Prozzo, T. G., Couto, W. J., & Porfirio, G. (2019). Thoracic outlet syndrome: a narrative review. Rev Col Bras Cir, 46(5), e20192243. https://doi.org/10.1590/0100-6991e-20192243 (Sindrome do desfiladeiro toracico: uma revisao narrativa.)
Zhang, B., Shi, H., Cao, S., Xie, L., Ren, P., Wang, J., & Shi, B. (2022). Revealing the magic of acupuncture based on biological mechanisms: A literature review. Biosci Trends, 16(1), 73-90. https://doi.org/10.5582/bst.2022.01039
For individuals dealing with musculoskeletal pain, can incorporating acupuncture and electroacupuncture therapy provide beneficial results?
Introduction
The upper and lower body quadrants are surrounded by muscles, soft tissues, and ligaments that allow the body to be mobile with feelings of pain or discomfort. Each muscle group has an important job providing sensory-motor functions like grasping objects, moving extremities, supporting the body in a correct posture, and stabilizing vertical axial weight. However, many people have adopted various habits from environmental factors or have been through traumatic injuries that can cause referred muscle pain in the upper and lower body quadrants. When this happens, it can lead to a life of disability, pain, and discomfort over time if it is not treated right away. To that point, musculoskeletal pain can also cause overlapping risk profiles with other comorbidities that can be pre-existing in the body. Fortunately, numerous treatments can help reduce musculoskeletal pain and benefit the body. Today’s article looks at two different non-surgical therapies, how each is beneficial to reducing musculoskeletal pain, and how effective they can help many people with musculoskeletal pain. We talk with certified medical providers who consolidate our patients’ information to assess how to reduce the pain-like effects of musculoskeletal pain with non-surgical treatments. We also guide patients on how these non-surgical treatments can help lessen the referred pain caused by various environmental factors affecting their musculoskeletal system. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating non-surgical treatments into their health and wellness treatments. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Traditional Touch Of Acupuncture
After a long workday, do you feel soreness in your arms, legs, or feet? Have you experienced any symptoms of numbness or stiffness in the upper or lower portions of your body? Or do you feel muscle aches and pains after waking up in the morning? Around the world, many individuals have dealt with musculoskeletal pain at some point, which causes many people to miss out on numerous activities. Musculoskeletal pain is a multifactorial condition that any individual can develop over time. Some biological mechanisms contributing to the development of musculoskeletal pain can be heterogeneous, cardiometabolic, and systemic inflammation that can affect the body. (Dzakpasu et al., 2021) When many people are doing repetitive motions or have dealt with injuries, it can cause the various muscles to be overstretched, tightened, or weak, which can cause individuals to feel miserable and seek treatment. When people go to get treatment for their musculoskeletal pain, many people will tell their doctors about their pain experience and how it impacts their daily social well-being. By gaining information about how musculoskeletal pain negatively affects their lives, a multidisciplinary approach to pain management that emphasizes rehabilitation and non-surgical treatments can be the first step in effectively managing musculoskeletal pain. (Welsh et al., 2020)
Now, non-surgical treatments vary depending on the severity of musculoskeletal pain the person is experiencing. Since musculoskeletal pain is a multifactorial condition, many people could experience comorbidities that cause overlapping risk profiles that correlate with musculoskeletal pain, hence why many people incorporate non-surgical treatments since it is affordable and can be combined with other treatments. One of the oldest therapies that is still practiced today is acupuncture. Now, acupuncture involves the insertion of thin, solid needles into the body’s acupoints to restore the normal flow of energy through the body’s pathways. Highly trained professionals do acupuncture, and it is safe and effective for the person dealing with musculoskeletal pain. Additionally, acupuncture can positively affect the body as it can help change the pain perception of the affected muscle. (Kelly & Willis, 2019)
How Acupuncture Benefits Muscle Pain
Acupuncture can also provide beneficial results to individuals by emphasizing the mobilization of self-healing mechanisms to restore the body’s homeostasis to normal. (Wang et al., 2023) Some of the beneficial properties that people can experience with acupuncture include:
Provides natural pain relief by stimulating the release of endorphins in the affected muscle.
Reducing muscle inflammation in the affected muscle group area.
Improving blood flow circulation to decrease muscle stiffness and soreness.
Reducing stress and muscle tension in the affected area.
At the same time, acupuncture therapy for muscle pain can help reduce the inhibitory effects and modulate the feeling of pain, which then modifies central sensitization. (Zhu et al., 2021)
The Modern Twist Of Electroacupuncture
Now, electroacupuncture is a different form of acupuncture that uses the application of acupuncture needles and electric stimulation on the affected muscle. At the same time, when people are getting treated with electroacupuncture, their somatosensory afferent nerves provide pain relief. They are blocked to stop the pain signals from reaching the central nervous system. (Chen et al., 2021) This is because adding electric stimulation can enhance the therapeutic effects of the acupuncture points in the body.
How Electroacupuncture Benefits Muscle Pain
Regarding reducing muscle pain, electroacupuncture is more effective as acupuncturists can help adjust the intensity of the electric currents on the affected muscle to ensure comfort. Some of the benefits that electroacupuncture provides include:
Enhanced pain relief as the electric current can stimulate endorphin release.
Muscle relaxation from spasms in the affected muscle group.
Increased the healing rate by stimulating deeper muscles.
Help enhance muscle strength and flexibility to improve functionality.
Electroacupuncture can relieve pain and even adjust the biomechanical properties of the extensor-flexor muscles to improve abnormal joint loading caused by musculoskeletal pain. (Shi et al., 2020)
How These Two Treatments Help With Musculoskeletal Pain?
When it comes to acupuncture and electroacupuncture, it all depends on the severity of musculoskeletal pain affecting the body. Many people prefer traditional acupuncture for acute musculoskeletal pain in a more holistic approach. In comparison, others might prefer electroacupuncture to reduce the chronic pain effects of musculoskeletal pain. However, both of these treatments are non-surgical. They can be combined with other therapies like physical therapy or chiropractic care to help stimulate the body’s natural healing factor and relieve musculoskeletal pain. When these two treatments are combined with other therapies, the affected muscles are strengthened and provide mobility function back into the extremities. When people start thinking about their well-being, they can utilize these treatments to reduce the comorbidities associated with musculoskeletal pain that is affecting them. Thus allowing them to make small, healthy changes to their routine and live pain-free lives.
Beyond Adjustments: Chiropractic and Integrative Healthcare- Video
References
Chen, L., Wang, X., Zhang, X., Wan, H., Su, Y., He, W., Xie, Y., & Jing, X. (2021). Electroacupuncture and Moxibustion-Like Stimulation Relieves Inflammatory Muscle Pain by Activating Local Distinct Layer Somatosensory Afferent Fibers. Front Neurosci, 15, 695152. https://doi.org/10.3389/fnins.2021.695152
Dzakpasu, F. Q. S., Carver, A., Brakenridge, C. J., Cicuttini, F., Urquhart, D. M., Owen, N., & Dunstan, D. W. (2021). Musculoskeletal pain and sedentary behaviour in occupational and non-occupational settings: a systematic review with meta-analysis. Int J Behav Nutr Phys Act, 18(1), 159. https://doi.org/10.1186/s12966-021-01191-y
Shi, X., Yu, W., Wang, T., Battulga, O., Wang, C., Shu, Q., Yang, X., Liu, C., & Guo, C. (2020). Electroacupuncture alleviates cartilage degradation: Improvement in cartilage biomechanics via pain relief and potentiation of muscle function in a rabbit model of knee osteoarthritis. Biomed Pharmacother, 123, 109724. https://doi.org/10.1016/j.biopha.2019.109724
Wang, M., Liu, W., Ge, J., & Liu, S. (2023). The immunomodulatory mechanisms for acupuncture practice. Front Immunol, 14, 1147718. https://doi.org/10.3389/fimmu.2023.1147718
Welsh, T. P., Yang, A. E., & Makris, U. E. (2020). Musculoskeletal Pain in Older Adults: A Clinical Review. Med Clin North Am, 104(5), 855-872. https://doi.org/10.1016/j.mcna.2020.05.002
Zhu, J., Li, J., Yang, L., & Liu, S. (2021). Acupuncture, from the ancient to the current. Anat Rec (Hoboken), 304(11), 2365-2371. https://doi.org/10.1002/ar.24625
Can the effects of electroacupuncture reduce sciatica in individuals dealing with low back pain to restore their mobility?
Introduction
When many people start to overuse their muscles in the lower quadrants, it can lead to numerous issues that cause pain and discomfort. One of the most common pain issues in the lower quadrants of the musculoskeletal system is sciatica, which is associated with low back pain. This pain duo can affect a person’s daily routine and lead them to pain and discomfort. This musculoskeletal condition is common, and when it affects one of the legs and lower back, many people state that it’s a radiating shooting pain that doesn’t go away for a while. Luckily, there are treatments like electroacupuncture to reduce sciatica associated with low back pain. Today’s article looks at the sciatica-low-back connection, how electroacupuncture reduces this pain connection, and how electroacupuncture can restore mobility to the individual. We talk with certified medical providers who consolidate our patients’ information to assess how to reduce the sciatica-low-back connection with electroacupuncture. We also inform and guide patients on how electroacupuncture therapy can be combined with other therapies to restore mobility to the body. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating electroacupuncture therapy as part of their routine to reduce sciatica associated with low back pain. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Sciatica & Low Back Connection
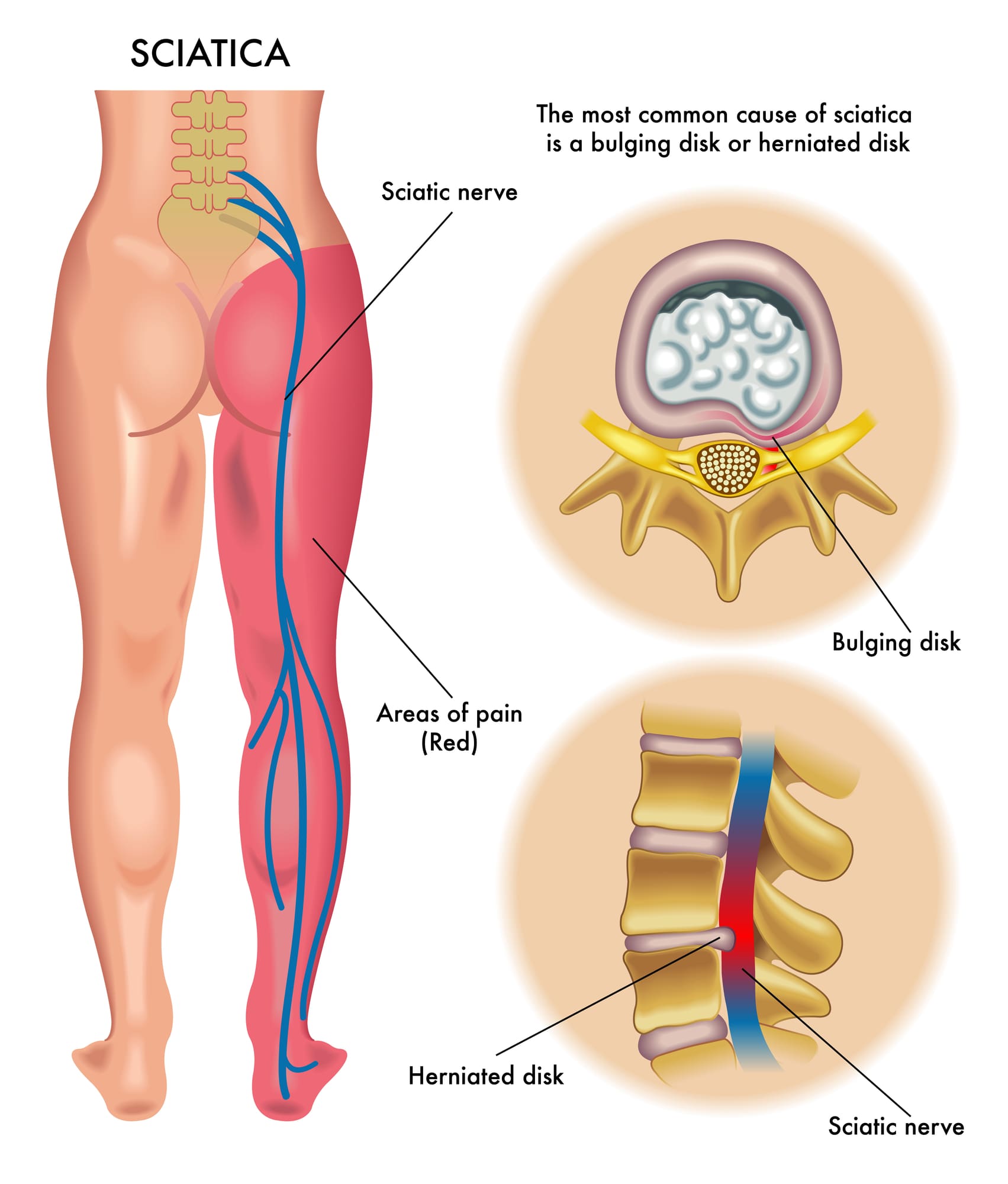
Do you feel muscle aches or pain in your lower back or your legs? Do you experience radiating, throbbing pain in your legs that affects your walking ability? Or have you noticed that your legs and lower back ache more when carrying a heavy object? Many of these scenarios are associated with sciatica, which correlates with lower back pain. Now, sciatica is often characterized by aggravating pain traveling along the sciatic nerve from the lower back region, impairing a person’s quality of life. In the musculoskeletal system, the sciatic nerve plays an important role by providing motor function to the legs. (Davis et al., 2024) Now, when the sciatic nerve, the lumbar region also has a pivotal role. The lumbar region in the musculoskeletal region also has a crucial role in providing support, strength, and flexibility to the body. However, both the sciatic nerve and lumbar spinal region are more prone to stress and injuries from traumatic injuries and environmental factors that can impact the lumbar spinal discs and the sciatic nerve.
Repetitive motions, obesity, improper lifting, degenerative spinal issues, and musculoskeletal conditions are a few causes and risk factors contributing to the development of sciatica associated with the lower back. What eventually happens is that the water content and the progressive loss of the proteoglycans of the spinal discs break down between the vertebrae and protrude out to press on the sciatic nerve, which then can become irritated and cause referred radiating pain in the legs and lower back. (Zhou et al., 2021) The combination of sciatica and lower back pain can become a socio-economic issue depending on the severity of the pain that the sciatic nerve is causing and can make individuals miss out on any activities they are participating in. (Siddiq et al., 2020) While sciatica pain-like symptoms often correlate with the lumbar region, many individuals can find the relief they are looking for through various treatments.
Sciatica Causes- Video
Electroacupuncture Reducing The Sciatica-Low Back Connection
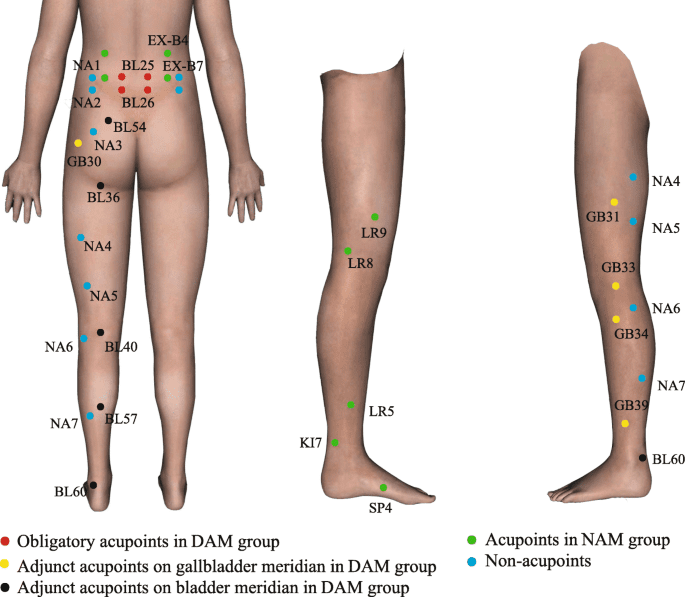
When it comes to reducing the sciatic-low-back connection, many individuals seek out treatment that is affordable and effective in decreasing pain-like issues. Non-surgical treatments like electroacupuncture can be beneficial to many individuals who are experiencing sciatica pain correlated with the lower back. Electroacupuncture is another form of traditional acupuncture therapy that originates in China. Highly trained acupuncturists follow the same acupuncture principles by placing solid thin needles at different acupoints in the body to restore qui or chi (energy flow). Electroacupuncture combines needles and electrostimulation to reduce the central pain-regulatory mechanisms causing low back pain and sciatica by blocking the pain signals and providing pain relief. (Kong, 2020) At the same time, electroacupuncture offers analgesic properties to stimulate endorphins and reduce pain medication for low back pain safely. (Sung et al., 2021)
Electroacupuncture Restoring Mobility
When the lower extremities are experiencing limited mobility due to sciatica associated with low back pain, electroacupuncture can help relax the muscles that are aggravating the sciatic nerve and even help improve blood flow to the lumbar muscles. That is because electroacupuncture can stimulate specific body regions to reduce the somato-vagal-adrenal reflexes to relieve and restore mobility to the lower extremities. (Liu et al., 2021) Additionally, electroacupuncture can be combined with other non-surgical therapies to help strengthen the core and lower back muscles, allowing people to be more mindful of what factors are causing sciatica and lower back pain. By doing this, many people struggling with sciatica associated with low back pain can incorporate electroacupuncture as part of their treatment program combined with holistic approaches to improving their quality of life and providing a pathway to improving their mobility.
Kong, J. T. (2020). Electroacupuncture for Treating Chronic Low-Back Pain: Preliminary Research Results. Med Acupunct, 32(6), 396-397. https://doi.org/10.1089/acu.2020.1495
Liu, S., Wang, Z., Su, Y., Qi, L., Yang, W., Fu, M., Jing, X., Wang, Y., & Ma, Q. (2021). A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis. Nature, 598(7882), 641-645. https://doi.org/10.1038/s41586-021-04001-4
Siddiq, M. A. B., Clegg, D., Hasan, S. A., & Rasker, J. J. (2020). Extra-spinal sciatica and sciatica mimics: a scoping review. Korean J Pain, 33(4), 305-317. https://doi.org/10.3344/kjp.2020.33.4.305
Sung, W. S., Park, J. R., Park, K., Youn, I., Yeum, H. W., Kim, S., Choi, J., Cho, Y., Hong, Y., Park, Y., Kim, E. J., & Nam, D. (2021). The effectiveness and safety of electroacupuncture for nonspecific chronic low back pain: A protocol for systematic review and/or meta-analysis. Medicine (Baltimore), 100(4), e24281. https://doi.org/10.1097/MD.0000000000024281
Zhou, J., Mi, J., Peng, Y., Han, H., & Liu, Z. (2021). Causal Associations of Obesity With the Intervertebral Degeneration, Low Back Pain, and Sciatica: A Two-Sample Mendelian Randomization Study. Front Endocrinol (Lausanne), 12, 740200. https://doi.org/10.3389/fendo.2021.740200
Can individuals dealing with gut inflammation be relieved with electroacupuncture to reduce low back pain symptoms & improve gut function?
Introduction
When it comes to the body, the gut system has a very interesting relationship to the various body groups. The gut system works with the central nervous, immune, and musculoskeletal systems as it helps protect the body from harmful bacteria while regulating inflammation. However, when environmental factors start to affect the body and cause the gut system to go haywire, it can cause numerous issues of pain and discomfort to the body. One of the issues that the gut can affect is the musculoskeletal system, causing back pain issues associated with gut inflammation. However, numerous treatments can help reduce the effects of gut inflammation that is causing back pain. Today’s article looks at the gut-back pain connection, how electroacupuncture can be integrated as a treatment, and how it can reduce inflammation. We talk with certified medical providers who consolidate our patients’ information to assess how gut inflammation impacts their bodies, causing back pain. We also inform and guide patients on how electroacupuncture therapy can help reduce the inflammatory effects causing gut and back issues and restore gut function. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating various non-surgical treatments to reduce gut inflammation correlated with back pain. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Gut-Back Pain Connection
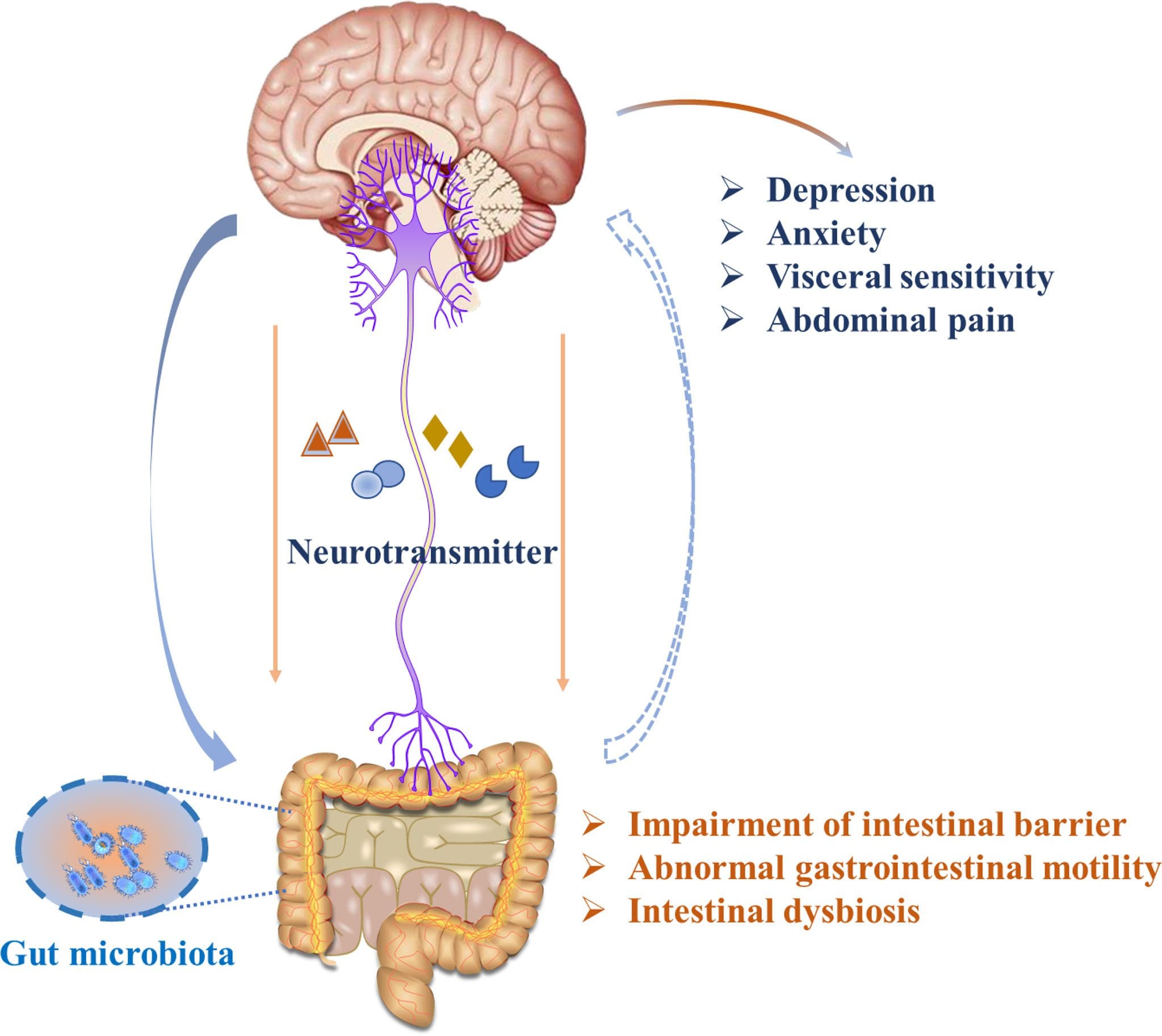
Do you feel muscle aches or pains in your gut or lower back? What about radiating heat in various areas of your body? Or have you experienced any low-energy moments throughout your day? While the gut is known as the second brain since it works with the immune system, one of its crucial roles is regulating the body’s immune system. This is because the gut microbiome houses trillions of bacteria to digest food and protect the body from bad bacteria. When environmental factors start to affect the gut’s delicate ecosystem, it can lead the immune system to be hyperactive, causing the inflammatory cytokines to mass produce, and this effect can ripple throughout the body, thus manifesting into various pain-like symptoms and conditions, including back pain. Since inflammation is the body’s defense response to injuries or infections, it removes the harmful issue in the affected area and helps heal. So when the inflammatory cytokines start to mass produce due to gut inflammation, it can compromise the gut system, allowing toxins and bacteria to enter the bloodstream and travel to different body areas, causing pain. Now, this is due to various environmental factors that lead to back pain development. When the harmful bacteria from inflammation start to cause back pain, they can attach themselves and affect the intervertebral disc homeostasis, causing the immune system to attack the intervertebral disc and cause back pain. (Yao et al., 2023) This is due to the connection of the gut and back through complex nerve pathways that send information from the gut to the back and up to the brain.
So, when inflammation starts to cause issues in the body, it can lead to musculoskeletal problems like back pain. Gut inflammation can cause an imbalance between the composition of the symbiont and pathobiont to decrease the integrity and function of the intestinal gut barriers, induce pain, and increase the inflammatory molecules. (Ratna et al., 2023) The inflammatory molecules can exacerbate pain receptors and muscle tension, leading to discomfort and pain in the lower back. Coincidentally, environmental factors like poor posture, physical inactivity, and poor dietary habits can cause the gut system to induce inflammation of the back muscles. When there is dysbiosis in the gut microbiota, the inflammatory effects can be indirectly associated with visceral pain and central nervous systemic functioning to alter the body and cause it to be in a persistent state of chronic systemic inflammation to induce back pain. (Dekker Nitert et al., 2020). However, there are numerous non-surgical treatments and holistic approaches to reduce gut inflammation and relieve back pain.
Integrating Electroacupuncture As Treatment
When people are experiencing back pain associated with gut inflammation, they will go to their primary healthcare doctor and explain the situation. Given the connection between gut inflammation and back pain, by addressing the environmental factors that cause these overlapping risk profiles, many doctors can work with pain specialists to reduce both gut inflammation and back pain. Pain specialists like chiropractors, acupuncturists, and massage therapists can help strengthen the affected muscles that are causing back pain and provide holistic approaches like anti-inflammatory vitamins and supplements to reduce gut inflammation. One of the oldest non-surgical treatments that can do both is electroacupuncture. Electroacupuncture combines traditional Chinese therapy and modern technology that uses electric stimulation and thin solid needles to be inserted into the body’s acupoint to obtain qi or energy. What this does is that it provides electric stimulation and anti-inflammatory effects to induce cholinergic reflexes in the gut and HPA axis. (Yang et al., 2024) Electroacupuncture can also be combined with other therapies to reduce the inflammatory effects associated with back pain.
How Does Electroacupuncture Reduce Gut Inflammation
Since electroacupuncture can reduce gut inflammation causing back pain, it can help regulate the intestinal flora by promoting intestinal motility and blocking the pain signals from affecting the back muscles. (An et al., 2022) This is because electroacupuncture can help relax the tense muscles causing back pain. Additionally, when people approach this treatment, it is under the guidance of highly trained acupuncturists who can insert the needles correctly while tailoring electroacupuncture therapy to the person’s specific needs and pain. Since electroacupuncture can be combined with other therapies, it can effectively reduce body weight and restore digestion and absorption to shape the gut microbiota. (Xia et al., 2022) This allows individuals to make small changes to their routine and prevent gut inflammation from affecting the body and causing back pain. They can improve their quality of life by incorporating electroacupuncture as part of their health and wellness treatment.
Unlocking The Secrets Of Inflammation-Video
References
An, J., Wang, L., Song, S., Tian, L., Liu, Q., Mei, M., Li, W., & Liu, S. (2022). Electroacupuncture reduces blood glucose by regulating intestinal flora in type 2 diabetic mice. J Diabetes, 14(10), 695-710. https://doi.org/10.1111/1753-0407.13323
Dekker Nitert, M., Mousa, A., Barrett, H. L., Naderpoor, N., & de Courten, B. (2020). Altered Gut Microbiota Composition Is Associated With Back Pain in Overweight and Obese Individuals. Front Endocrinol (Lausanne), 11, 605. https://doi.org/10.3389/fendo.2020.00605
Ratna, H. V. K., Jeyaraman, M., Yadav, S., Jeyaraman, N., & Nallakumarasamy, A. (2023). Is Dysbiotic Gut the Cause of Low Back Pain? Cureus, 15(7), e42496. https://doi.org/10.7759/cureus.42496
Xia, X., Xie, Y., Gong, Y., Zhan, M., He, Y., Liang, X., Jin, Y., Yang, Y., & Ding, W. (2022). Electroacupuncture promoted intestinal defensins and rescued the dysbiotic cecal microbiota of high-fat diet-induced obese mice. Life Sci, 309, 120961. https://doi.org/10.1016/j.lfs.2022.120961
Yang, Y., Pang, F., Zhou, M., Guo, X., Yang, Y., Qiu, W., Liao, C., Chen, Y., & Tang, C. (2024). Electroacupuncture Reduces Inflammatory Bowel Disease in Obese Mice by Activating the Nrf2/HO-1 Signaling Pathways and Repairing the Intestinal Barrier. Diabetes Metab Syndr Obes, 17, 435-452. https://doi.org/10.2147/DMSO.S449112
Yao, B., Cai, Y., Wang, W., Deng, J., Zhao, L., Han, Z., & Wan, L. (2023). The Effect of Gut Microbiota on the Progression of Intervertebral Disc Degeneration. Orthopaedic Surgery, 15(3), 858-867. https://doi.org/10.1111/os.13626
Can individuals with shoulder pain, find pain relief from electroacupuncture therapy to reduce stiffness associated with the neck?
Introduction
When many individuals are dealing with pain-like symptoms that are caused by environmental factors, it can affect their daily performance or their routines. Some of the most common pain areas that people usually get are from the neck, shoulder, or back. Since the musculoskeletal system has various upper and lower quadrant muscles, they have an outstanding relationship with the nerve roots that spread out to the muscles to provide sensory-motor functions. When environmental factors or traumatic injuries start to affect the musculoskeletal system, it can lead to a life of disability, pain, and discomfort. So, when individuals are dealing with shoulder pain that is causing issues with their neck, it can lead to various pain-like symptoms in the upper quadrants and searching for treatments to reduce their pain. Treatments like electroacupuncture can provide a positive outlook on reducing shoulder pain associated with the neck. Today’s article focuses on how shoulder pain correlates with the neck, how electroacupuncture positively reduces shoulder pain, and how it can reduce neck and shoulder stiffness. We talk with certified medical providers who consolidate our patients’ information to assess how shoulder pain is correlated with neck issues. We also inform and guide patients on how non-surgical treatments like electroacupuncture can help reduce shoulder pain and relieve the neck. We encourage our patients to ask their associated medical providers intricate and important questions about how their neck and shoulder pain affects their daily routine. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Does Shoulder Pain Correlate With The Neck?
Have you been dealing with stiffness in your neck or shoulders that is causing your hands to feel numb? Do you feel muscle strain from the sides of your neck that rotating your shoulders causes temporary relief? Or do you feel muscle soreness in your shoulders after laying on one side for too long? Many of these pain-like issues are correlated with shoulder pain, which can become a frequent musculoskeletal condition that can evolve into chronic problems over time. (Suzuki et al., 2022) This can cause the upper body extremities that work with the shoulders to deal with muscular issues that cause the shoulder and neck muscles to become hypersensitive. Since shoulder pain can often correlate with neck issues or the cervical spine, various environmental and traumatic factors can cause musculoskeletal conditions like muscular tightness in the neck, disc degeneration, or even cervical spondylosis, which can cause referred pain to the shoulders.
Additionally, many working individuals at a desk job can experience shoulder pain associated with the neck as they are in a forward hunched position that causes significant stress on the soft tissues surrounding and supporting the cervical spine, which can risk the development of neck and shoulder pain. (Moon & Kim, 2023) This is due to the numerous nerve roots that run through the neck and shoulder region, causing the pain signals to invoke referred pain in the soft muscle tissues. At the same time, when people dealing with shoulder pain correlating with the neck are doing repetitive motions, compression, or staying in a fixed position for an extended period, it can become overlapping risk profiles, thus increasing the spread of neck and shoulder pain. (Elsiddig et al., 2022) To that point, when people are dealing with neck problems, it can influence the shoulders, leading to discomfort, reduced mobility, pain, stiffness, and decreased quality of life that can impact a person. (Onda et al., 2022) However, when the shoulder pain associated with the neck becomes too much, many people will seek treatment to reduce the pain.
The Science Of Motion- Video
The Positive Effects Of Electroacupuncture Reducing Shoulder Pain
When many people are looking for alternative and complementary non-surgical therapies, electroacupuncture is the answer for individuals suffering from shoulder pain correlating with the neck. Like traditional acupuncture, electroacupuncture involves electric stimulation and needle insertion into specific points or acupoints on the body by highly trained professionals to enhance therapeutic effects on the affected muscle area. For shoulder pain, electroacupuncture controls pain by activating the central nervous system and inducing the body’s natural biochemicals to promote healing. (Heo et al., 2022) While shoulder pain associated with the neck can arise from a variety of causes, electroacupuncture can target these issues by:
Additionally, electroacupuncture can be combined with physical therapy to reduce neck and shoulder stiffness. When people incorporate exercises that target the neck and shoulders while combining electroacupuncture, they can see a long-term positive effect on pain reduction. (Duenas et al., 2021) The neck and shoulders will have improved flexibility and mobility from the exercises. At the same time, blood flow can help speed up the healing process, and the pain signals are blocked by electroacupuncture. For many individuals dealing with shoulder pain correlating with the neck, electroacupuncture can be an effective treatment to promote healing on the affected muscles and reduce pain.
References
Duenas, L., Aguilar-Rodriguez, M., Voogt, L., Lluch, E., Struyf, F., Mertens, M., Meulemeester, K., & Meeus, M. (2021). Specific versus Non-Specific Exercises for Chronic Neck or Shoulder Pain: A Systematic Review. J Clin Med, 10(24). https://doi.org/10.3390/jcm10245946
Elsiddig, A. I., Altalhi, I. A., Althobaiti, M. E., Alwethainani, M. T., & Alzahrani, A. M. (2022). Prevalence of neck and shoulder pain among Saudi universities’ students who are using smartphones and computers. J Family Med Prim Care, 11(1), 194-200. https://doi.org/10.4103/jfmpc.jfmpc_1138_21
Heo, J. W., Jo, J. H., Lee, J. J., Kang, H., Choi, T. Y., Lee, M. S., & Kim, J. I. (2022). Electroacupuncture for the treatment of frozen shoulder: A systematic review and meta-analysis. Front Med (Lausanne), 9, 928823. https://doi.org/10.3389/fmed.2022.928823
Moon, S. E., & Kim, Y. K. (2023). Neck and Shoulder Pain with Scapular Dyskinesis in Computer Office Workers. Medicina (Kaunas, Lithuania), 59(12). https://doi.org/10.3390/medicina59122159
Onda, A., Onozato, K., & Kimura, M. (2022). Clinical features of neck and shoulder pain (Katakori) in Japanese hospital workers. Fukushima J Med Sci, 68(2), 79-87. https://doi.org/10.5387/fms.2022-02
Suzuki, H., Tahara, S., Mitsuda, M., Izumi, H., Ikeda, S., Seki, K., Nishida, N., Funaba, M., Imajo, Y., Yukata, K., & Sakai, T. (2022). Current Concept of Quantitative Sensory Testing and Pressure Pain Threshold in Neck/Shoulder and Low Back Pain. Healthcare (Basel), 10(8). https://doi.org/10.3390/healthcare10081485
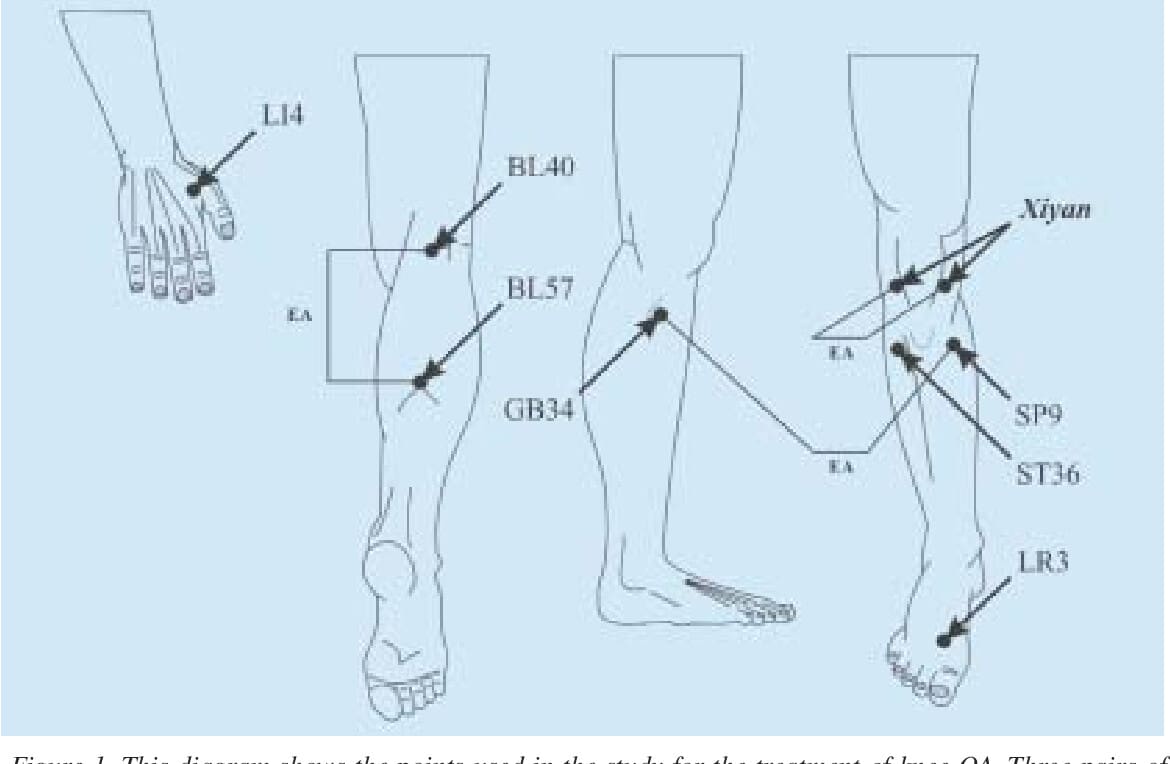
Can individuals with osteoarthritis find the relief they deserve through electroacupuncture to restore knee and hip mobility?
Introduction
The lower extremities provide movement and stability to the body, allowing people to be in motion. The hips, lower back, knees, and feet each have a function to do, and when traumatic issues start to affect the spinal structures, it can cause numerous symptoms to pop up and cause pain-like symptoms. Additionally, degenerative factors are natural to the joints of the lower extremities as many people make repetitive motions to their bodies that lead to the degenerative process. One of the most common degenerative issues that affect the lower extremities is osteoarthritis, which can make many people feel miserable. Today’s article looks at how osteoarthritis affects the lower extremities and how treatments like electroacupuncture reduce inflammation associated with osteoarthritis and restore knee and hip mobility. We talk with certified medical providers who consolidate our patients’ information to understand better how osteoarthritis affects their lower extremities. We also inform and guide patients on how electroacupuncture therapy can help reduce the inflammatory effects of osteoarthritis affecting the hips and knees. We encourage our patients to ask their associated medical providers intricate and important questions about reducing the progression of osteoarthritis through non-surgical treatments. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
Osteoarthritis Affecting The Lower Extremities
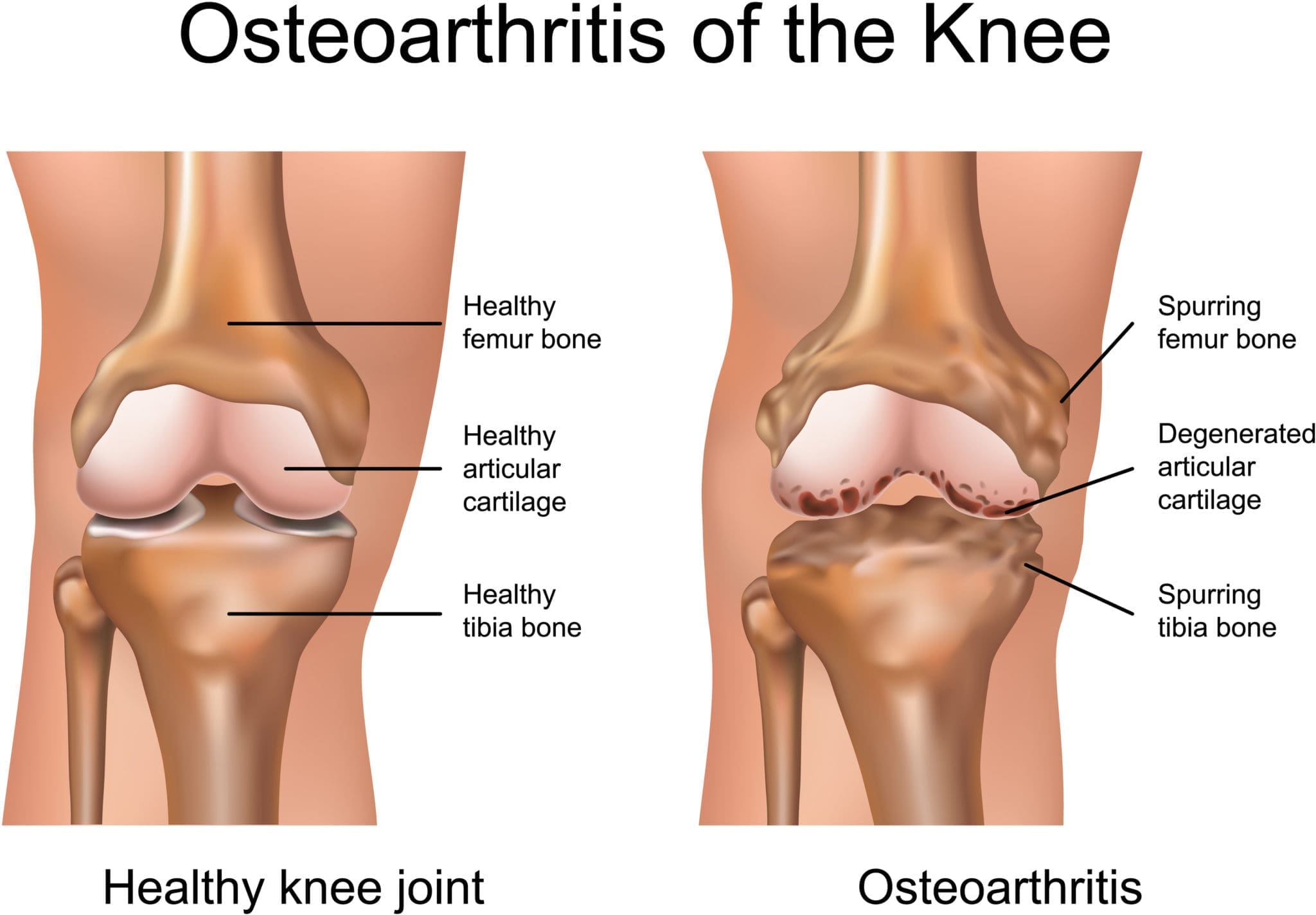
Have you been dealing with stiffness in your knees, hips, and lower back in the mornings? Do you feel like you are wobbling a bit too much when walking? Or do you think radiating heat and swelling in your knees? When people experience these inflammatory pain issues in their joints, it is due to osteoarthritis, a degenerative joint disorder affecting the cartilage between the bones and the tissue components surrounding the joint. Osteoarthritis is multifactorial, meaning it can be idiopathic or secondary while influenced by heredity factors. (Bliddal, 2020) The most common places where people experience osteoarthritis are the lower back, hand, hips, and, most commonly, the knees. Some of the major environmental factors that contribute to the development of osteoarthritis include:
Obesity
Age
Repetitive motions
Family history
Injuries
When people are dealing with osteoarthritis, environmental factors can lead to weight overloading on the joints, which results in compression and inflammation. (Nedunchezhiyan et al., 2022)
When inflammation is associated with osteoarthritis, it can cause the joints and surrounding muscle tissues to swell and feel hot to the touch. At the same time, osteoarthritis is one of the leading causes of disability that can become a socio-economic issue for many people. (Yao et al., 2023) This is because many individuals with osteoarthritis have comorbidities that are associated with the effects of inflammatory cytokines, which can cause them to be physically inactive and miserable. (Katz et al., 2021) However, there are various ways to reduce the progression of osteoarthritis and reduce the inflammatory effects on the joints.
Electroacupuncture Reducing Inflammation Associated With Osteoarthritis
When it comes to inflammation reduction associated with osteoarthritis, many people seek out surgical and non-surgical treatments that can help decrease the progression of this degenerative joint disease. Many people will do aqua therapy to relieve pressure off the joints and improve their mobility. At the same time, others use spinal decompression to create negative pressure on the joint space. However, many people have found that electroacupuncture can help reduce the inflammatory effects of osteoarthritis. Electroacupuncture combines electrical nerve stimulation and acupuncture by highly trained professionals that can help decrease the pain intensity in the joints and provide functionality. (Wu et al., 2020) Additionally, since osteoarthritis is associated with inflammation, electroacupuncture can promote blood circulation and adjustment of muscle tension on the joints, and improve mobility. (Zhang et al., 2023)
Electroacupuncture Restoring Knee & Hip Mobility
Electroacupuncture can help with hip and knee mobility as this non-surgical treatment helps promote pain limitations and muscular atrophy from biomechanical overloading, thus improving cartilage viscoelasticity. (Shi et al., 2020) This allows the joints to retain mobility in the hips, knees, and lower back. When people go through consecutive treatment for osteoporosis, they can recover their muscle strength over time to restore their mobility and reduce the progression of osteoarthritis. (Xu et al., 2020) By doing so, many people can find the relief they are looking for with electroacupuncture, which can enable them to make small changes in their daily routine to ensure they can function throughout the day.
Katz, J. N., Arant, K. R., & Loeser, R. F. (2021). Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. JAMA, 325(6), 568-578. https://doi.org/10.1001/jama.2020.22171
Nedunchezhiyan, U., Varughese, I., Sun, A. R., Wu, X., Crawford, R., & Prasadam, I. (2022). Obesity, Inflammation, and Immune System in Osteoarthritis. Front Immunol, 13, 907750. https://doi.org/10.3389/fimmu.2022.907750
Shi, X., Yu, W., Wang, T., Battulga, O., Wang, C., Shu, Q., Yang, X., Liu, C., & Guo, C. (2020). Electroacupuncture alleviates cartilage degradation: Improvement in cartilage biomechanics via pain relief and potentiation of muscle function in a rabbit model of knee osteoarthritis. Biomed Pharmacother, 123, 109724. https://doi.org/10.1016/j.biopha.2019.109724
Wu, S. Y., Lin, C. H., Chang, N. J., Hu, W. L., Hung, Y. C., Tsao, Y., & Kuo, C. A. (2020). Combined effect of laser acupuncture and electroacupuncture in knee osteoarthritis patients: A protocol for a randomized controlled trial. Medicine (Baltimore), 99(12), e19541. https://doi.org/10.1097/MD.0000000000019541
Xu, H., Kang, B., Li, Y., Xie, J., Sun, S., Zhong, S., Gao, C., Xu, X., Zhao, C., Qiu, G., & Xiao, L. (2020). Using electroacupuncture to recover muscle strength in patients with knee osteoarthritis after total knee arthroplasty: a study protocol for a double-blinded, randomized, and placebo-controlled trial. Trials, 21(1), 705. https://doi.org/10.1186/s13063-020-04601-x
Yao, Q., Wu, X., Tao, C., Gong, W., Chen, M., Qu, M., Zhong, Y., He, T., Chen, S., & Xiao, G. (2023). Osteoarthritis: pathogenic signaling pathways and therapeutic targets. Signal Transduct Target Ther, 8(1), 56. https://doi.org/10.1038/s41392-023-01330-w
Zhang, W., Zhang, L., Yang, S., Wen, B., Chen, J., & Chang, J. (2023). Electroacupuncture ameliorates knee osteoarthritis in rats via inhibiting NLRP3 inflammasome and reducing pyroptosis. Mol Pain, 19, 17448069221147792. https://doi.org/10.1177/17448069221147792
Can individuals dealing with neck pain find relief with electroacupuncture therapy while reducing pain symptoms to restore neck function?
Introduction
The cervical region of the body consists of the neck region, which allows the head to be mobile and stabilized from discomfort or pain. The neck has numerous muscles, ligaments, and tendons surrounding the cervical facet joints and spinal discs. However, when the neck muscles are overstretched or ached from environmental factors or traumatic injuries that cause the head and the neck muscles to whip back and forth rapidly, it can force individuals to deal with not only pain and discomfort from the neck but also the head and shoulders are affected as well. When this happens, many individuals try to find various relief methods to reduce the pain and its associated symptoms. Today’s articles look at how the pain symptoms are associated with the neck, how there are non-surgical treatments for neck pain, and how electroacupuncture can help restore neck function. We talk with certified medical providers who consolidate our patients’ information to understand better why they are experiencing neck pain. We also inform and guide patients on how non-surgical treatments like electroacupuncture can help restore neck function to the body. We encourage our patients to ask their associated medical providers intricate and important questions about reducing the impact of neck pain while trying to incorporate various therapeutic reliefs into their bodies. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Are Pain Symptoms Associated with the Neck?
Do you experience stiffness or pain on your neck’s left or right side? Do you constantly get headaches that you have to lie in a dark room to reduce the pain? Or do you experience numbness or tingling sensations on your shoulders and arms? Many of these pain-like scenarios are associated with neck pain. Now similar to back pain, neck pain is a multifactorial musculoskeletal condition that can lead to a socio-economic burden that causes many people to have reduced productivity and job-related problems that can be an issue. (Kazeminasab et al., 2022) Neck pain can be in acute or chronic stages as multiple factors can play the developmental part of neck pain. Some of the environmental factors and traumatic injuries associated with neck pain include:
Poor posture
Whiplash
Degenerative issues
Slouching/hunching position
Sprains or strains
Spinal fractures
When these environmental and traumatic injury factors start to cause issues in the neck region of the body, they can cause pain-like symptoms.
So, how is pain associated with the neck? Well, many individuals dealing with neck pain can either have specific or non-specific neck pain with various symptoms depending on the severity of the pain. While specific neck pain deals with the cervical spine, non-specific neck pain deals with the surrounding muscles and ligaments. To that point, many individuals who are dealing with neck pain are also experiencing somatic referred pain and radicular pain that is associated with neurological signs that make a diagnosis difficult to classify. (Misailidou et al., 2010) This can cause many individuals to experience referred pain in their shoulders and arms or have neurological issues like headaches and tension within their upper body regions, which then causes personal discomfort, disability, and impaired quality of life. (Ben Ayed et al., 2019) But all is not lost, as many individuals seek treatment to reduce the effects of neck pain.
Movement As Medicine- Video
Non-Surgical Treatments For Neck Pain
When it comes to reducing neck pain from environmental factors or traumatic injuries, many people will seek treatments that are affordable and effective in not only decreasing neck pain but also its associated pain-like symptoms. Non-surgical treatments are an excellent way to reduce the effects of neck pain, and they can be combined with other therapies. Some of the non-surgical treatments that are suitable for neck pain include:
Chiropractic care
Acupuncture
Electroacupuncture
Spinal decompression
Massage therapy
Physical therapy
Many individuals dealing with acute neck pain can incorporate non-surgical treatments since they are not only effective through consecutive treatment but are affordable as well. (Chou et al., 2020) This allows many individuals to be more mindful of what factors affect the neck and make small changes to prevent them from returning.
Electroacupuncture Restoring Neck Function
One of the oldest forms of non-surgical treatment is through acupuncture, which originates from China and is performed by highly trained professionals. Depending on how severe the pain is in the neck, many individuals seek out acupuncture therapy or electroacupuncture to reduce the pain. The difference between the two is that acupuncture incorporates thin, solid needles to the specific acupoints in the body that involve the central nervous system. In contrast, electroacupuncture incorporates electric stimulation to become a transformation of energy to block the pain signals that are causing pain in the neck region. (Liu et al., 2022)
Additionally, when the cervical area of the spine has been affected by traumatic forces, it can cause the neck to lose functionality. So, when people incorporate electroacupuncture to restore neck functionality, it has analgesic and anti-inflammatory properties that regulate the endocannabinoid system. (Wang et al., 2021) This means that the pain receptors from the nerve roots are blocked, and relief forms in the neck. Depending on the severity, many people with neck pain can utilize electroacupuncture consecutively to regain neck mobility and reduce the pain-like effects that are causing them to be miserable. When people think about their health and wellness, they can make small changes to reduce their environmental factors and start living life to the fullest extent possible.
References
Ben Ayed, H., Yaich, S., Trigui, M., Ben Hmida, M., Ben Jemaa, M., Ammar, A., Jedidi, J., Karray, R., Feki, H., Mejdoub, Y., Kassis, M., & Damak, J. (2019). Prevalence, Risk Factors and Outcomes of Neck, Shoulders and Low-Back Pain in Secondary-School Children. J Res Health Sci, 19(1), e00440. https://www.ncbi.nlm.nih.gov/pubmed/31133629
Chou, R., Wagner, J., Ahmed, A. Y., Blazina, I., Brodt, E., Buckley, D. I., Cheney, T. P., Choo, E., Dana, T., Gordon, D., Khandelwal, S., Kantner, S., McDonagh, M. S., Sedgley, C., & Skelly, A. C. (2020). In Treatments for Acute Pain: A Systematic Review. https://www.ncbi.nlm.nih.gov/pubmed/33411426
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Liu, R., Li, S., Liu, Y., He, M., Cao, J., Sun, M., Duan, C., & Li, T. (2022). Acupuncture Analgesia in Patients with Postoperative Neck Pain: A Protocol for Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med, 2022, 1226702. https://doi.org/10.1155/2022/1226702
Misailidou, V., Malliou, P., Beneka, A., Karagiannidis, A., & Godolias, G. (2010). Assessment of patients with neck pain: a review of definitions, selection criteria, and measurement tools. J Chiropr Med, 9(2), 49-59. https://doi.org/10.1016/j.jcm.2010.03.002
Wang, J., Zhang, J., Gao, Y., Chen, Y., Duanmu, C., & Liu, J. (2021). Electroacupuncture Alleviates Hyperalgesia by Regulating CB1 Receptor of Spinal Cord in Incisional Neck Pain Rats. Evid Based Complement Alternat Med, 2021, 5880690. https://doi.org/10.1155/2021/5880690
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine