Recognizing clinical and experimental evidence, physiotherapy is a healthcare profession that helps restore and maintain function to individuals affected by injury, disease or disability by using mechanical force and movements, manual therapy, exercise and electrotherapy, as well as through patient education and advice. The terms physiotherapy and physical therapy are used interchangeably to describe the same healthcare profession. Physiotherapy is recommended for a variety of injuries and conditions, and it can help support overall health and wellness for people of all ages.
For further notice,�physiotherapy services may be offered alongside chiropractic care, to provide a cautious and gentle manipulation and/or mobilization of the cervical and thoracic spine in the instance of a large cervical disc herniation. Cervical disc herniations can cause pain and discomfort, numbness and weakness in the neck, shoulders, chest, arms and hands.
Contents
Abstract
A 34-year-old woman was seen in a physiotherapy department with signs and symptoms of cervical radiculopathy. Loss of cervical lordosis and a large paracentral to intraforaminal disc prolapse (8?mm) at C5�C6 level was reported on MRI. She was taking diclofenac sodium, tramadol HCl, diazepam and pregabalin for the preceding 2?months and no significant improvement, except temporary relief, was reported. She was referred to physiotherapy while awaiting a surgical opinion from a neurosurgeon. In physiotherapy she was treated with mobilisation of the upper thoracic spine from C7 to T6 level. A cervical extension exercise was performed with prior voluntary extension of the thoracic spine and elevated shoulders. She was advised to continue the same at home. General posture advice was given. Signs and symptoms resolved within the following four sessions of treatment over 3?weeks. Surgical intervention was subsequently deemed unnecessary.
Background
Surgical interventions are commonly recommended in large cervical prolapsed discs and the importance of non-aggressive physiotherapy interventions is less recognised and poorly understood. We present interventions that were associated with resolution of symptoms of radiculopathy resulting from a larger cervical herniated disc. These interventions, if applied correctly, may help to reduce the number of surgeries required for cervical prolapsed discs.
Case Presentation
The patient was a 34-year-old woman. She was seen in the physiotherapy department with a complaint of left-sided neck and shoulder pain. The pain was radiating to her left arm and there was associated numbness. The duration of symptoms was more than 2?months with no history of trauma. The pain was present on waking in the morning and gradually increased during the day. She was otherwise a healthy woman. Neck movements were aggravating the symptoms. She was seen in the acute hospital accident and emergency department (A&E) twice since onset and had been taking diclofenac sodium, tramadol HCl, diazepam and pregabalin. An MRI was planned and a request was sent for physiotherapy during the MRI waiting period. A neurosurgical review was requested by the A&E consultant upon receipt of the MRI report 7?weeks later.
Patient examination in the physiotherapy department revealed a normal gait pattern, her left arm held in front of her chest with the left shoulder slightly elevated. Her active range of neck motion was restricted and was painful on the left side. Flexion and rotation to the left were aggravating her arm and shoulder pain. Strength deficits were noted in the left elbow flexors and wrist extensors (4/5) when compared with the right side. There was paraesthesia along the radial border of the forearm and thumb regions. The brachioradialis reflex was diminished and biceps reflex was sluggish. Triceps and plantar reflexes were normal. Passive intervertebral movements were tender at C5�C6 level and were reproducing the pain. Sustained pressure at C7 and below was easing the pain and also improving the neck range of motion. The patient was deemed to have C6 radiculopathy. The MRI report, available 2?weeks after the commencement of physiotherapy, confirmed the diagnosis.
Investigations
The findings from the plain cervical x-ray were unremarkable. MRI showed (Figure 1) loss of cervical spine lordosis, a left paracentral to intraforaminal lesion with 8?mm hernia, which indented the cord and obstructed the left paracentral recess and neural foramen.
Figure 1: Loss of cervical spine lordosis and large disc herniation at C5 and C6 on MRI.
Differential Diagnosis
Cervical myelopathy.
Treatment
The patient received pharmacological treatment for the initial two symptomatic months, which included diclofenic sodium, tramadol, diazepam and pregabalin (lyrica) tablet. Physiotherapy was started after 2?months. Physiotherapy intervention consisted of mobilisation of the thoracic spine, resisted cervical extension exercises, a home programme of exercises and advice regarding the posture.
Mobilisation of the thoracic spine was administered in the prone lying position from C7 toT6 level. Mild intensity oscillations (15?reps) in an anterosuperior direction were directly applied to each of the spinal segments, through the thumb over the spinous processes, during the first visit. The applied force was enough to appreciate intervertebral movement in each segment and without significant pain. High-intensity oscillations (10�20) were applied during the subsequent treatment sessions. The patient was asked for symptom feedback during treatment.
Cervical spine extension exercises were carried out in a sitting position. The patient was asked to extend her thoracic spine with lungs fully inflated and shoulders elevated followed by extension of her cervical spine. Head extension was moderately resisted by the therapist near the end range of extension for 5�10?s and brought back to neutral after each resisted movement. The resisted movement was repeated at least three times with intervals of 30?s. The patient was asked to perform the same exercise at home every hour during the day.
The patient was educated regarding the rationale of extension exercises, sitting and lying posture and their effects on the spine. The duration of each session was approximately 20�25?min.
Dr. Alex Jimenez’s Insight
Surgical interventions are generally recommended and widely considered for large cervical disc herniations. Although less recognized and often misunderstood, however, physiotherapy can be just as effective towards improving herniated discs in the cervical spine, excluding the need for surgery, according to the research study. Pharmacological treatments are also commonly used to help temporarily reduce symptoms alongside physiotherapy interventions. Cautious and gentle, spinal manipulation and mobilization of the cervical spine should be performed in the case of large cervical disc herniations to avoid aggravating the injury and/or condition. As recommended by a physiotherapist, or other healthcare professional experienced in physiotherapy, proper exercise can restore the function of the cervical spine and prevent regression of large prolapsed discs along the spine. Through appropriate physiotherapy intervention as well as through patient safety and compliance, the retraction of the cervical herniated discs is possible.
Outcome and Follow-Up
Pharmacological interventions were helpful to reduce the patient’s pain on a temporary basis. Symptoms were recurring and resolution was not sustainable. The symptoms started improving after the first physiotherapy session and continued to improve during the subsequent sessions. It fully resolved in four sessions extended over 3?weeks. The patient was reviewed 4?months after the resolution of symptoms and there was no recurrence of symptoms. She was reviewed by a neurosurgeon and the surgical option was withdrawn.
Discussion
Stiffness of the thoracic spine has been linked to the painful pathologies of the cervical spine, and manipulation of the thoracic spine has been shown to improve painful symptoms and mobility of the cervical spine. However, cervical disc herniations of greater than 4?mm are considered inappropriate for physiotherapy interventions such as traction and manipulation. Spinal manipulation refers to a passive movement thrust of high velocity and low amplitude, usually applied at the end range of movement and is beyond the patient’s control. Manipulation of the cervical spine is an aggressive procedure, which carries various risks and is often associated with worsening of symptoms. Manipulation was not considered in the treatment options for this patient because of the risks associated with it, and also because of patient’s anxiety and lack of MRI-confirmed diagnosis.
Active extension of the thoracic spine increases the range of motion of the cervical spine and, in these authors� clinical experience, relieves minor neck symptoms. Conversely, thoracic spine kyphosis, such as slouch sitting, restricts the mobility of the cervical spine and aggravates the painful symptoms. A good sitting posture is constituted by a slightly extended thoracic spine. Therefore, active extension of the thoracic spine prior to cervical extension may improve cervical movements and restore cervical curvature.
It is believed that excessive pressure during flexion on the anterior aspect of the intervertebral discs pushes the nucleus pulposus posteriorly and causes herniations. Conversely, cervical lordosis might have the reverse effect�that is, decreases pressure on the anterior aspect of the discs and may create a suction effect which retracts the herniated contents. Therefore, a combination of short duration and repeated movements at the end of extension may serve as a suction pump and possibly retract the extruded content of the disc. Active cervical extension exercises, with an extended thoracic spine posture, may have been the key element in a home exercise programme to restore lordosis of the cervical spine and relieve radiculopathy symptoms in the current case. This may possibly have been due to the retraction of the herniated discs.
Spinal mobilisation refers to a gentle, oscillatory, passive movement of a spinal segment. These are applied to a spinal segment to gently increase the passive range of motion. It allows the patient to report aggravation of pain and to resist any unwanted movements. No mobilisation treatment was administered at C5�C6 level as palpation at this level was aggravating the symptoms. Segments below this level were mobilised with emphasis at C7�T1 level. Any treatment at the affected segment was likely to irritate the nerve root and thereby increase the inflammatory process.
Various interventions are reported for the treatment of prolapsed discs. Saal et al reported the use of traction, specific physical therapy exercise, oral anti-inflammatory medication and patient education in the treatment of 26 patients with herniated cervical discs (<4?mm) and reported significant improvement in outcomes for 24 patients. They observed that surgery for disc herniations occurs when a patient has significant myotomal weakness, severe pain or pain that persists beyond an arbitrary conservative treatment period of 2�8?weeks.
Spontaneous regressions of cervical disc protrusions are reported in the literature. However, spontaneous regressions of herniated cervical discs are speculated to be rare. Various factors related to regression are hypothesised and theorised. Pan et al summarised the factors related to the resorption of herniated disc as: the age of the patients; dehydration of the expanded nucleus pulposus; resorption of haematoma; revascularisation; penetration of herniated cervical disc fragments through the posterior longitudinal ligament; size of disc herniations; and existence of cartilage and annulus fibrosus tissue in the herniated material. Some studies on spontaneous regressions of discs reported that the patients were receiving physiotherapy. Physiotherapy interventions are not defined in any of these studies, however. Therefore, it is possible that disc regressions in these studies may be due to similar physiotherapy interventions as described here, or the patients were practising techniques and adopting postures as reported in the current case.
Learning Points
Thoracic spine mobilisation improves cervical spine biomechanics and can be considered in conjunction with other interventions in all painful conditions of the cervical spine.
Active extension of the thoracic spine facilitates movements of the cervical spine and may help regression of large prolapsed discs.
There is a possibility of retraction of herniated cervical discs through appropriate physiotherapy intervention.
Patient education ensures safety and compliance to therapist advice.
Meticulous assessment and patient feedback guides the therapist in selection of intensity of mobilisation.
Footnotes
Competing interests: None.
Patient consent: Obtained.
In conclusion,�physiotherapy, or physical therapy, is used to treat various injuries, diseases and disabilities, through the use of mechanical force and movements, manual therapy, exercise, electrotherapy, and through patient education and advice to restore and maintain function. As in the case above, physiotherapy can be recommended and considered as treatment before referring to surgical interventions of large cervical disc herniations. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1.�Norlander S, Gustavsson BA, Lindell J, et al.�Reduced mobility in the cervico-thoracic motion segment�a risk factor for musculoskeletal neck-shoulder pain: a two-year prospective follow-up study.�Scand J Rehabil Med�1997;29:167�74.�[PubMed]
2.�Walser RF, Meserve BB, Boucher TR.�The effectiveness of thoracic spine manipulation for the management of musculoskeletal conditions: a systematic review and meta-analysis of randomized clinical trials.�J Man Manipulative Ther�2009;17:237�46.�[PMC free article]�[PubMed]
3.�Krauss J, Creighton D, Ely JD, et al.�The immediate effects of upper thoracic translatoric spinal manipulation on cervical pain and range of motion: a randomized clinical trial.�J Man Manipulative Ther2008;16:93�9.�[PMC free article]�[PubMed]
4.�Saal JS, Saal JA, Yurth EF.�Nonoperative management of herniated cervical intervertebral disc with radiculopathy.�Spine (Phila Pa 1976)�1996;21:1877�83.�[PubMed]
5.�Murphy DR, Beres JL.�Cervical myelopathy: a case report of a �near-miss� complication to cervical manipulation.�J Manipulative Physiol Ther�2008;31:553�7.�[PubMed]
6.�Leon-Sanchez A, Cuetter A, Ferrer G.�Cervical spine manipulation: an alternative medical procedure with potentially fatal complications.�South Med J�2007;100:201�3.�[PubMed]
7.�Scannell JP, McGill SM.�Disc prolapse: evidence of reversal with repeated extension.�Spine (Phila Pa 1976)�2009;34:344�50.�[PubMed]
8.�Gurkanlar D, Yucel E, Er U, et al.�Spontaneous regression of cervical disc herniations.�Minim Invasive Neurosurg�2006;49:179�83.�[PubMed]
9.�Mochida K, Komori H, Okawa A, et al.�Regression of cervical disc herniation observed on magnetic resonance images.�Spine (Phila Pa 1976)�1998;23:990�5; discussion 6�7.�[PubMed]
10.�Song JH, Park HK, Shin KM.�Spontaneous regression of a herniated cervical disc in a patient with myelopathy. Case report.�J Neurosurg�1999;90(1 Suppl):138�40.�[PubMed]
12.�Pan H, Xiao LW, Hu QF.�Spontaneous regression of herniated cervical disc fragments and its clinical significance.�Orthop Surg�2010;2:77�9.�[PubMed]
13.�Teplick JG, Haskin ME.�Spontaneous regression of herniated nucleus pulposus.�AJR Am J Roentgenol1985;145:371�5.�[PubMed]
Stay Hydrated: Summer fun means outside activities in the warm sun, from strenuous pursuits like biking, hiking, and volleyball-playing, to more leisurely enjoyments like sunbathing on a float. No matter how you plan to enjoy the steamy summer months, maintaining hydration should be right up there with sunscreen on your list of important hot weather priorities.
Dehydration is a condition that ranges from mild to serious, and can happen quicker than you think. Right Diagnosis defines dehydration as “an abnormal condition in which the body’s cells are deprived of an adequate amount of water.” One of the main situations factoring into a person becoming dehydrated is heat.
Think you drink enough water and don’t need to worry about dehydration? Consider these points:
The ability to recognize thirst diminishes in individuals in their late 30’s or older.
A person’s body is made up of roughly 70% water.
When you lose 2% of the body’s water content, you are considered dehydrated.
Dehydration symptoms range from unpleasant confusion, muscle weakness, and fatigue to extremely dangerous ones like seizures, kidney failure, and death. The good news is that if you stay hydrated in the first place is relatively easy if you take a few precautions up front.
Contents
#1: Drink Plenty Of Water
Make it a habit of carrying water with you during the summer months, and sipping on it throughout the day, especially if you are planning on outside activities. Invest in a couple of BPA-free water bottles for yourself and your family to tote with them on their summer adventures.
Not a big fan of plain water? Try adding lemon, cucumber, and mint sprigs to liven it up! Mix up in a big pitcher the night before so the flavor has time to penetrate. Another option is flavor packets, which are individual packets of flavors like green tea, watermelon, and peach.
#2: Eat The Right Foods
Liquids aren’t the only way your body gets water. Avoid dehydration by eating foods with a high water content.
Choices like celery, watermelon, cucumbers, carrots, and citrus fruits all offer exceptional hydrating ability. Pack these as snacks for the pool or beach, or to enjoy before and after an outdoor workout.
#3: Steer Clear Of Certain Drinks
As yummy and refreshing as an icy beer or frosty margarita tastes, alcohol can contribute to dehydration. If you decide to indulge, limit yourself to one or two, and drink a large glass of water along with your beverage to counteract the alcohol’s effects.
#4: Avoid Overexertion
Exercise is a wonderfully healthy pursuit; however, keep an eye on the temperature. If it is going to be exceptionally hot and humid, choose to exercise either early in the morning, or after sunset, when temperatures are lower and the sun isn’t beaming.
#5: Wear Proper Attire
Dress in light, airy clothing in fabrics that breathe. Protect your head with a cap or hat that shades your face. Avoid black clothing, which tends to absorb the sun and make you hotter.
#6: Stay Hydrated & Be Prepared
Extreme heat makes everyday issues like a flat tire or dead battery life-threatening. Visit a mechanic to confirm your vehicle is in good shape to lessen the chances of getting stranded. Carry extra water or sports drinks in your vehicle, and keep your cell phone charged. If your car breaks down, either stay in your car to wait for help, or stand in the grass instead of on the sizzling pavement.
When you stay hydrated is essential for good health all the time, and during the summer in particular. Implement these easy tips into your daily routine so you and your family maintain hydration and enjoy hot weather outdoor fun.
Chiropractic Treatment For Concussions
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Cause Of Sciatica: Several lumbar spine (lower back) disorders can cause sciatica. Sciatica is often described as mild to intense pain in the left or right leg. Sciatica is caused by compression of one or more of the 5 sets of nerve roots in the lower back. Sometimes doctors call sciatica a radiculopathy. Radiculopathy is a medical term used to describe pain, numbness, tingling, and weakness in the arms or legs caused by a nerve root problem. If the nerve problem is in the neck, it is called a cervical radiculopathy. However, since sciatica affects the low back, it is called a lumbar radiculopathy.
Contents
Pathways To Sciatic Nerve Pain
Five sets of paired nerve roots in the lumbar spine combine to create the sciatic nerve. Starting at the back of the pelvis (sacrum), the sciatic nerve runs from the back, under the buttock, and downward through the hip area into each leg. Nerve roots are not “solitary” structures but are part of the body’s entire nervous system capable of transmitting pain and sensation to other parts of the body. Radiculopathy occurs when compression of a nerve root from a disc rupture (herniated disc) or bone spur (osteophyte) occurs in the lumbar spine prior to it joining the sciatic nerve.
What Causes Sciatic Nerve Compression?
Several spinal disorders can cause spinal nerve compression and sciatica or lumbar radiculopathy. The 6 most common are:
a bulging or herniated disc
lumbar spinal stenosis
spondylolisthesis
trauma
piriformis syndrome
spinal tumors
Sciatica�Cause:�6 Leading Sources
Several lumbar spine (lower back) disorders can cause sciatica. Sciatica is often described as mild to intense pain in the left or right leg. Sciatica is caused by compression of one or more of the 5 sets of nerve roots in the lower back. Sometimes doctors call sciatica a radiculopathy. Radiculopathy is a medical term used to describe pain, numbness, tingling, and weakness in the arms or legs caused by a nerve root problem. If the nerve problem is in the neck, it is called a cervical radiculopathy. However, since sciatica affects the low back, it is called a lumbar radiculopathy.
Sciatica Cause #1: Lumbar Bulging Disc Or Herniated Disc
A bulging disc is also known as a contained disc disorder. This means the gel-like center (nucleus pulposus) remains “contained” within the tire-like outer wall (annulus fibrosus) of the disc.
A herniated disc occurs when the nucleus breaks through the annulus fibrosus. It is called a “non-contained” disc disorder. Whether a disc bulges or herniates, disc material can press against an adjacent nerve root and compress delicate nerve tissue and cause sciatica.
The consequences of a herniated disc are worse. Not only does the herniated disc cause direct compression of the nerve root against the interior of the bony spinal canal, but the disc material itself also contains an acidic, chemical irritant (hyaluronic acid) that causes nerve inflammation. In both cases, nerve compression and irritation cause inflammation and pain, often leading to extremity numbness, tingling, and muscle weakness.
Herniated disc is a relatively common condition that can occur anywhere along the spine, but most often affects the lower back or neck region. Also known as a slipped disc or ruptured disc, a herniated disc develops when one of the cushion-like pads between the vertebrae moves out of position and presses on adjacent nerves.
Herniated discs are typically caused by overuse injuries or trauma to the spine; however, disc conditions can also develop as a result of the normal aging process. It is also known that there is a genetic factor that contributes to the development of disc degeneration and herniated disc. In most cases, a herniated disc in the lower back will heal within six months, as the size of herniation shrinks with time via resorption. Surgery may be needed if medication, physical therapy and other treatments fail.
What Is A Disc?
Spinal discs are cushion-like pads located between the vertebrae. Without these �shock absorbers,� the bones in the spine would grind against one another. In addition to giving the spine flexibility and making movements such as twisting and bending possible, discs protect the spine by absorbing the impact of trauma and body weight. Each disc has a strong outer layer called annulus fibrosus and a soft, gel-like center, called nucleus pulposus. There are fibers on the outside of each disc that attach to adjacent vertebrae and hold the disc in place. A herniated disc occurs when the outer layer tears or ruptures and the gel-like center leaks into the spinal canal.
The spinal canal has just enough space to house the spinal cord and spinal fluid. When a disc herniates and spills into the spinal canal, it can cause compression of the nerves or spinal cord. Intense, debilitating pain and alterations in sensation often occur. In addition, the gel-like substance inside the disc releases chemical irritants that contribute to nerve inflammation and pain.
What Causes A Herniated Disc?
As we age, the spinal discs gradually lose fluid volume. This process starts at about age 30 and progresses slowly, over time. As the discs dry out, microscopic cracks or tears can form on the outer surface, causing it to become brittle, weak and more susceptible to injury. The most common causes of herniated disc are:
Wear and tear: Discs dry out and aren�t as flexible as they once were.
Repetitive movements: Work, lifestyle, and certain sports activities that put stress on the spine, especially the lower back, further weaken an already vulnerable area.
Lifting the wrong way: Never lift while bent at the waist. Proper lifting entails lifting with your legs and a straight back.
Injury: High-impact trauma can cause the disc to bulge, tear or rupture.
Obesity: Carrying excess weight puts an undue amount of strain on the spine.
Genetics: There are some genes that are more commonly present in individuals with disc degeneration. More research is needed to investigate the role of these genes�they could be targets of biological treatment in the future.
What Are The Symptoms Of A Herniated Disc?
Pain from a herniated disc can vary, depending on the location and severity of the injury. It is typically felt on one side of the body.
If the injury is minimal, little or no pain may be felt. If the disc ruptures, pain can be severe and unrelenting. Pain may radiate to an extremity in a specific nerve root distribution if significant nerve impingement has occurred. For example, sciatica is frequently caused by a herniated disc in the lower back. Herniated disc can manifest itself with a range of symptoms, including:
Dull ache to severe pain
Numbness, tingling, burning
Muscle weakness; spasm; altered reflexes
Loss of bowel or bladder control (Note: These symptoms constitute a medical emergency. If they occur, seek medical attention immediately).
How Is A Herniated Disc Diagnosed?
History and physical examination point to a diagnosis of herniated disc. A herniated disc is likely if low back pain is accompanied by radiating leg pain in a nerve root distribution with positive straight leg raising test (ie, elevating the leg while lying down causes radiating pain down the leg), and other neurologic deficits such as numbness, weakness, and altered reflexes.
Imaging studies are usually ordered to confirm a diagnosis of herniated disc. X-rays are not the imaging medium of choice because soft tissues (eg, discs, nerves) are hard to capture with this technology. However, they may be used as an initial tool to rule out other disorders such as a growth or fracture. Confirmation of the suspicion of herniated disc is generally accomplished with:
Magnetic Resonance Imaging (MRI): This technology reveals the spinal cord, surrounding soft tissue and nerves. It is the best imaging study to support the diagnosis of a herniated disc.
Nerve Conduction Studies (NCS) and Electromyogram (EMG): These studies use electrical impulses to measure the degree of damage to the nerve/s caused by compression from a herniated disc and other conditions that cause nerve impingement can be ruled out. NCS and EMG are not routine tests to diagnose herniated disc.
Herniated discs sometimes heal on their own through a process called resorption. This means that the disc fragments are absorbed by the body. Most people suffering from herniated disc respond well to conservative treatment and do not require surgery.
Sciatica Cause #2: Lumbar Spinal Stenosis
Spinal stenosis is a nerve compression disorder most often affecting older adults. Leg pain similar to sciatica may occur as a result of lumbar spinal stenosis. The pain is usually positional, often brought on by activities such as standing or walking and relieved by sitting down.
Spinal nerve roots branch outward from the spinal cord through passageways called neural foramina comprised of bone and ligaments. Between each set of vertebral bodies, located on the left and right sides, is a foramen. Nerve roots pass through these openings and extend outward beyond the spinal column to innervate other parts of the body. When these passageways become narrow or clogged causing nerve compression, the term foraminal stenosis is used.
What Is Spinal Stenosis?
A clue to answering this question is found in the meaning of each word. Spinal refers to the spine. Stenosis is a medical term used to describe a condition where a normal-size opening has become narrow. Spinal stenosis may affect the cervical (neck), thoracic (chest), or lumbar (lower back) spines.
The most commonly area affected is the lumbar spine followed by the cervical spine.
Visualize Spinal Stenosis?
Consider a water pipe. Over time, rust and debris builds up on the walls of the pipe, thereby narrowing the passageway that normally allows water to freely flow. In the spine, the passageways are the spinal canal and the neuroforamen. The spinal canal is a hollow vertical hole that contains the spinal cord. The neuroforamen are the passageways that are naturally created between the vertebrae through which spinal nerve roots exit the spinal canal.
The neuroforamen are the passageways that are naturally created between the vertebrae through which spinal nerve roots exit the spinal canal.
Illustration above: The spine’s bony structures encase and protect the spinal cord. Small nerve roots shoot off from the spinal cord and exit the spinal canal through passageways called neuroforamen.
Lumbar (low back) spinal stenosis is illustrated below. Notice the narrowed areas in the spinal canal (reddish-colored areas). As the canal space narrows, the spinal cord and nearby nerve roots are squeezed causing different types of symptoms. The medical term is nerve compression.
Anatomy Overview Can Help You Understand Spinal Stenosis
The spine is a column of connected bones called vertebrae. There are 24 vertebrae in the spine, plus the sacrum and tailbone (coccyx). Most adults have 7 vertebrae in the neck (the cervical vertebrae), 12 from the shoulders to the waist (the thoracic vertebrae), and 5 in the lower back (the lumbar vertebrae). The sacrum is made up of 5 vertebrae between the hipbones that are fused into one bone. The coccyx is made up of small fused bones at the tail end of the spine.
Lamina and Spinous Processes: At the back (posterior) of each vertebra, you have the lamina, a bony plate that protects your spinal canal and spinal cord. Your vertebrae also have several bony tabs that are called spinous processes; those processes are attachment points for muscles and ligaments.
Ligaments, Especially the Ligamentum Flavum: Vertebrae are connected by ligaments, which keep the vertebrae in their proper place. The ligamentum flavum is a particularly important ligament. Not only does it help stabilize your spine, it also protects your spinal cord and nerve roots. Plus, the ligamentum flavum is the strongest ligament in your spine.
The ligamentum flavum is a dynamic structure, which means that it adapts its shape as you move your body. When you’re sitting down and leaning forward, the ligamentum flavum is stretched out; that gives your spinal canal more room for the spinal nerves. When you stand up and lean back, though, the ligamentum flavum becomes shorter and thicker; that means there’s less room for the spinal nerves. (This dynamic capability helps explain why people with spinal stenosis find that sitting down feels better than standing or walking.)
Discs: In between each vertebra are tough fibrous shock-absorbing pads called the intervertebral discs. Each disc is made up of a tire-like outer band (annulus fibrosus) and a gel-like inner substance (nucleus pulposus).
Spinal Nerves and the Spinal Cord: Nerves are also an important part of your spinal anatomy�after all, they’re what sends messages from your brain to the rest of your body. The spinal cord, the thick bundle of nerves that extends downward from the brain, passes through a ring in each vertebra. Those rings line up into a channel called the spinal canal.
Between each vertebra, two nerves branch out of the spinal cord (one to the right and one to the left). Those nerves exit the spine through openings called the foramen and travel to all parts of your body.
Normally, the spinal channel is wide enough for the spinal cord, and the foramen are wide enough for the nerve roots. But either or both can become narrowed, and cause spinal stenosis.
Sciatica Cause #3: Spondylolisthesis
Spondylolisthesis is a disorder that most often affects the lumbar spine. It is characterized by one vertebra slipping forward over an adjacent vertebra. When a vertebra slips and is displaced, spinal nerve root compression occurs and often causes sciatic leg pain. Spondylolisthesis is categorized as developmental (found at birth, develops during childhood) or acquired from spinal degeneration, trauma or physical stress (eg, lifting weights).
Spondylolisthesis occurs when one vertebra slips forward over the vertebra below it. The term is pronounced spondy-low-lis-thesis and is derived from the Greek language: spondylo means vertebra and listhesis means to slip. There are several types or causes of spondylolisthesis; a few are listed below.
Congenital spondylolisthesis means the disorder is present at birth.
Isthmic spondylolisthesis occurs when a defect, such as a fracture occurs in a bony supporting vertebral structure at the back of the spine.
Degenerative spondylolisthesis is more common and is often associated with degenerative disc disease, wherein the discs (eg, due to the effects of growing older) lose hydration and resilency.
How Spondylolisthesis May Develop
The lumbar spine is exposed to directional pressures while it carries, absorbs, and distributes most of your body’s weight at rest and during activity. In other words, while your lumbar spine is carrying and absorbing body weight, it also moves in different directions (eg, rotate, bend forward). Sometimes, this combination causes excessive stress to the vertebra and/or its supporting structures, and may lead to a vertebral body slipping forward over the vertebrae beneath.
Who May Be At Risk
If a family member (eg, mother, father) has spondylolisthesis, your risk for developing the disorder may be greater. Some activities make you more susceptible to spondylolisthesis. Gymnasts, linemen in football, and weight lifters all put significant pressure and weight on their low backs. Think about gymnasts and the positions they put their body in: They practically bend in half backwards�that’s an extreme arched back. They also twist through the air quickly when doing flips and then land, absorbing the impact through their legs and low back. Those movements put substantial stress on the spine, and spondylolisthesis can develop as a result of repeated excessive strains and stress.
X-Ray View Of Spondylolisthesis
The x-ray below shows you a good example of a lumbar spondylolisthesis. Look at the area the arrow is pointing to: You can see that the vertebra above the arrow isn’t in line with the vertebra below it. It’s slipped forward; it’s spondylolisthesis.
Arrow Points To A Lumbar Spondylolisthesis
Grading Spondylolisthesis
Doctors “grade” the severity of a spondylolisthesis using five descriptive categories. Although there are several factors your doctor considers when evaluating your spondylolisthesis, the grading scale (below) is based on the far forward a vertebral body has slid forward over the vertera beneath. Often, the doctor uses a lateral (side view) x-ray to examine and grade a spondyloisthesis. Grade I is a smaller slip than Grade IV or V.
Grade I: Less than 25% slip
Grade II: 25% to 49% slip.
Grade III: 50% to 74% slip.
Grade IV: 75% to 99% slip.
Grade V: The vertebra that has fallen forward off the vertebra below it. This is the most severe type of spondylolisthesis and is termed spondyloptosis.
Sciatica Cause #4: Trauma
Sciatica can result from direct nerve compression caused by external forces to the lumbar or sacral spinal nerve roots. Examples include motor vehicle accidents, falling down, football and other sports. The impact may injure the nerves or, occasionally, fragments of broken bone may compress the nerves.
Sciatica Cause #5: Piriformis Syndrome
Piriformis syndrome is named for the piriformis muscle and the pain caused when the muscle irritates the sciatic nerve. The piriformis muscle is located in the lower part of the spine, connects to the thighbone, and assists in hip rotation. The sciatic nerve runs beneath the piriformis muscle. Piriformis syndrome develops when muscle spasms develop in the piriformis muscle thereby compressing the sciatic nerve. It may be difficult to diagnose and treat due to the lack of x-ray or magnetic resonance imaging (MRI) findings.
If you�ve ever felt pain in the hip, pain in the center of the butt, or pain down the back of the leg, you are likely suffering, at least partially, with piriformis syndrome. The piriformis is a muscle which runs from your sacrum (mid-line base of spine) to the outer hip bone (trochanter). This muscle truly works overtime on anyone who runs at all.
The muscles in and around the gluteal region help with three areas
rotation of the hip and leg;
balance while one foot is off the ground; and
stability for the pelvic region.
Needless to say, all of these characteristics are highly needed by runners (and everyone else, when you come to think of it).
Injuries To The Piriformis
This muscle is a prime candidate for repetitive motion injury (RMI). RMI occurs when a muscle is asked to perform beyond it�s level of capability, not given enough time to recover, and asked to perform again. The typical response from a muscle in this situation is to tighten, which is a defensive response of the muscle. This tightness, however, manifests itself in several ways to a runner.
The first symptom suggesting piriformis syndrome would be pain in and around the outer hip bone. The tightness of the muscle produces increased tension between the tendon and the bone which produces either direct discomfort and pain or an increased tension in the joint producing a bursitis. Again, a bursitis is an inflammation of the fluid filled sac in a joint caused by an elevation of stress and tension within that joint.
The second symptom suggesting piriformis syndrome would be pain directly in the center of the buttocks. Although this is not as common as the other two symtpoms, this pain can be elicited with direct compression over the belly of the buttocks area. A tight muscle is a sore muscle upon compression due to a reduced blood flow to that muscle.
The third symptom suggesting piriformis syndrome would be a sciatic neuralgia, or pain from the buttocks down the back of the leg and sometimes into different portions of the lower leg. We have an article that can teach you more about how piriformis syndrome and sciatica are related.
The sciatic nerve runs right through the belly of the piriformis muscle and if the piriformis muscle contracts from being overused, the sciatic nerve now becomes strangled, producing pain, tingling and numbness.
Simple Physiology
Any muscle repetitively used needs to have an opportunity to recover. This recovery can either be on Nature�s clock, or can be facilitated and sped up with proper knowledge and treatment. Since the muscle is tightening due to overuse, continued use will only make it worse. This injured muscle needs to relax and have increased blood flow encouraged to it for more rapid healing. This tightness that exists also reduces the normal blood flow going to the muscle reducing the speed with which the muscle can recover. To encourage fresh, oxygen-rich blood to the muscle is the most powerful means of getting the muscle to begin to relax and function normally. Multiple massages per day to this area is greatly encouraged.
The next step in this “recovery” process is to use a tennis ball under the butt and hip area. While sitting down on the floor, roll away from the side of involvement and place a tennis ball just inside the outer hip bone under the butt area. As you begin to allow your weight onto the tennis ball, note areas of increased pain and soreness. Trigger points will tend to accumulate in a repetitively used muscle, and until these toxins are manually broken up and eliminated, the muscle will have an artificial ceiling with regard to flexibility potential and recovery potential. So, if it�s sore and hurts while your sitting on it, you�re doing a good job. Let the ball work under each spot for 15-20 seconds before moving it to another area. Once you�ve been on the ball for 4-5 minutes, now put the ankle of the involved leg over the knee of the non-involved leg (crossing your legs). Now place the tennis ball just inside the outer hip bone again and work the tendon of the piriformis muscle. While this pain is typically excruciating and takes some time to effectively reduce, the benefits here are huge. Be patient, be consistent and good things will happen.
Additional Treatments
Due to the fact that the sciatic neuralgia and the hip bursitis or tendonitis are both inflammatory in nature, ice, or cryotherapy, over the involved area 15-20 minutes at a time will be beneficial. This should be done multiple times per day.
Stretching of the hip muscles should not be done until the acute pain is gone. At that point in time, begin with gentle stretching, such as the cross-legged stretch while pulling up on the knee. The muscle should have increased flexibility before an active return to running.
Finally, I�m always discouraging the use of pharmaceutical anti-inflammatories. Not only do they greatly aggravate the intestines, but they also suggest an artificial wellness that can lead to bigger problems. Proteolytic enzymes, such as bromelain, are both natural and extremely beneficial with no side effects.
Conclusion: The piriformis muscle is pretty important for all of us.
Sciatica Cause #6: Spinal Tumors
Spinal tumors are abnormal growths that are either benign or cancerous (malignant). Fortunately, spinal tumors are rare. However, when a spinal tumor develops in the lumbar region, there is a risk for sciatica to develop as a result of nerve compression.
If you think you have sciatica, call your doctor or chiropractor. The first step toward relieving pain is a proper diagnosis.
Written by Jean-Jacques Abitbol, MD; Reviewed by Brian R. Subach, MD
Howard S. An, MD, Stewart G. Eidelson, MD; Reviewed by Howard S. An, MD, Jason M. Highsmith, MD
Timothy J. Maggs, D.C.; Reviewed by Edward C. Benzel, MD
Understanding the following, traditional Chinese medicine utilizes herbal medicines as well as various mind and body practices, such as acupuncture and tai chi, in order to treat or prevent numerous health issues. Traditional Chinese medicine, or TCM, originated in ancient China and has evolved over thousands of years. TCM has been primarily used as a complementary health approach along with other alternative treatment options like chiropractic care. Like TCM, chiropractic care is an alternative healthcare approach focused on the diagnosis, treatment and prevention of a variety of injuries and conditions of the musculoskeletal and nervous system, with an emphasis on manual manipulations and adjustments of the spine. As a doctor of chiropractic, or DC, TCM can also be offered to treat various types of injuries and conditions.
On a personal note, integrative TCM conservative therapies have been utilized to help treat symptoms of low back pain due to lumbar disc herniation, or LDH. Disc material from a ruptured or herniated disc in the lumbar spine can irritate or compress one or several of the nerves found in the lower spine. Pressure along the sciatic nerve can cause symptoms of sciatica, such as pain and discomfort, burning and tingling sensations, and numbness which may radiate from the buttocks into the leg and occasionally, down to the foot.�A randomized controlled trial was conducted in order to measure the outcomes of traditional Chinese medicine for low back pain due to LDH. The results have been recorded below.
Contents
Abstract
Low back pain due to lumbar disc herniation (LDH) is very common in clinic. This randomized controlled trial was designed to investigate the effects of integrative TCM conservative therapy for low back pain due to LDH. A total of 408 patients with low back pain due to LDH were randomly assigned to an experimental group with integrative TCM therapy and a control group with normal conservative treatment by the ratio of 3?:?1. The primary outcome was the pain by the visual analogue scale (VAS). The secondary outcome was the low back functional activities by Chinese Short Form Oswestry Disability Index (C-SFODI). Immediately after treatment, patients in the experimental group experienced significant improvements in VAS and C-SFODI compared with the control group (between-group difference in mean change from baseline, ?16.62 points, P < 0.001 in VAS; ?15.55 points, P < 0.001 in C-SFODI). The difference remained at one-month followup, but it is only significant in C-SFODI at six-month followup (?7.68 points, P < 0.001). No serious adverse events were observed. These findings suggest that integrative TCM therapy may be a beneficial complementary and alternative therapy for patients with low back pain due to LDH.
Introduction
Lumbar disc herniation (LDH) is a common disease and a major contributing factor of low back pain. Although many studies have confirmed that surgery is more effective for LDH, conservative therapies have also been recognized for their therapeutic efficacy. Considering the fact that 20% of patients still have pain after surgery, 7% to 15% of surgical patients may have failed back surgery syndrome, and some patients are scared of surgery, conservative treatment is still one of the primary means for LDH.
In China, TCM is one of the main conservative treatments for LDH. Previous studies have confirmed that some TCM therapies have certain effects on low back pain due to LDH. These include acupuncture, oral administration of Chinese medicine, external application of Chinese medicine, Chinese Tuina (massage), and TCM-characteristic functional exercise. Clinically, these therapeutic methods are not used alone but often in combination. Recently, the clinical pathway of treating LDH with integrative TCM therapy has attracted attention. The Shi’s Traumatology Medical Center of Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine is well recognized for its long-term commitment to the research on conservative treatment for LDH, coupled with a package protocol for LDH. However, high-quality research evidence is needed to support the effectiveness of the protocol.
This clinical trial aims to study the efficacy and safety of integrative TCM therapy for LDH and thus confirm its clinical effect.
Materials and Methods
Design
We conducted a multicenter, randomized controlled trial to evaluate the effectiveness of integrative TCM conservative treatment for patients with low back pain due to LDH. Patients were randomly assigned to an experimental group and a control group by the ratio of 3?:?1 using computer-generated numbers. The randomized treatment assignments were sealed in opaque envelopes and opened individually for each patient who agreed to be in the study. The nurse, who had no role in the design and conduct of the study, prepared the envelopes. Patients in the experimental group were treated with integrative TCM therapy once a day, for two weeks, whereas patients in the control group were treated with a two-week normal conservative intervention. At baseline, immediately after treatment, one and six months after treatment, visual analogue scale (VAS) and the Chinese Short Form Oswestry Disability Index (C-SFODI) were used as outcome assessment. This trial is registered in Chinese Clinical Trial Registry (No. ChiCTR-TRC-11001343).
Subjects
Patients were recruited from Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Ruijin Hospital Affiliated to Shanghai Jiaotong University, and Yueyang Integrative Traditional Chinese and Western Medicine Hospital Affiliated to Shanghai University of Traditional Chinese Medicine between January 2011 and August 2012.
Inclusion criteria: (1) aging 20�60 years; (2) having low back pain due to LDH (MRI scan confirmed lumbar disk herniation) and ruling out other relevant ongoing pathologies such as fractures, lumbar spondylolisthesis, tumor, osteoporosis, or infection; (3) willing to participate in this study and signing the informed consent.
Exclusion criteria: (1) having other pain syndromes; (2) experiencing a history of spinal surgery; (3) having neurological disease; (4) having psychiatric disease; (5) having serious chronic diseases that could interfere with the outcomes (e.g., cardiovascular disease, rheumatoid arthritis, epilepsy, or other disqualifying conditions); (6) scared of acupuncture; (7) pregnant or planning to become pregnant during the study; (8) having other diseases that the researchers believe is not suitable for the study.
Treatment
Experimental Group
Patients in the experimental group receive a two-week integrative TCM treatment. They were further divided into three subgroups (according to the duration from initial low back pain to getting treatment) for different treatment methods: acute stage (0�14 days), subacute stage (15�30 days), and chronic stage (>30 days).
Acute stage: (1) Electroacupuncture + (2) Chinese herbal injection (Salvia miltiorrhiza injection) + (3) external plaster (Compound Redbud Injury-healing Cataplasms); Subacute stag: (1) Chinese Tuina (massage) + (2) hot compress using Chinese medicine + (3) external plaster (Compound Redbud Injury-healing Cataplasms); Chronic stage: (1) TCM functional exercise + (2) external plaster (Compound Redbud Injury-healing Cataplasms).
Treatment Parameters
Electroacupuncture. Points: bilateral Dachangshu (BL 25) and Baihuanshu (BL 30).
Method: Insert the needles (the sterile, disposable needles, 0.3 � 75?mm, manufactured by Suzhou Medical Supplies Factory Co., Ltd.) 2.5 to 2.8?cun. Upon De Qi (needling sensation), connect the needles with the electroacupuncture device (Model: G6805-II, manufactured by Guangzhou KangMai Medical Devices Co., Ltd.), using a continuous wave, an electrical stimulation pulse wave of approximately 0.6?ms and a frequency of 20?Hz. The treatment was conducted once every day, 30?min for each treatment.
Main ingredients: Zi Jing Pi (Cortex Cercis Chinensis), Huang Jing Zi (Negundo Chastetree Fruit), Da Huang (Radix et Rhizoma Rhei), Chuan Xiong (Rhizoma Chuanxiong), Tian Nan Xing (Rhizoma Arisaematis), and Ma Qian Zi (Semen Strychni).
Functions: Circulates blood, resolves stasis, eliminates swelling, and alleviates pain.
Method: Apply the cataplasms to the most painful area, one plaster each time, once a day.
Chinese Herbal Injection. Salvia miltiorrhiza injection (Approval no. Z51021303, manufactured by Sichuan ShengHe Pharmaceutical Co., Ltd.).
The main ingredient of the injection is Salvia root P.E. It acts to circulate blood and resolve stasis.
Method: Intravenous dripping of 20?mL salvia miltiorrhiza injection and 250 mL 5% glucose, once a day.
Hot Compress Using Chinese Medicine. Ingredients: 20?g of Cang Zhu (Rhizoma Atractylodis), Qin Jiao (Radix Gentianae Macrophyllae), Sang Zhi (Ramulus Mori), Mu Gua (Fructus Chaenomelis), Hong Hua (Flos Carthami), Chuan Xiong (Rhizoma Chuanxiong), Hai Feng Teng (Caulis Piperis Kadsurae) and Lei Gong Teng (Radix Tripterygii Wilfordii), respectively. All herbs were provided by Shanghai Hongqiao Pharmaceutical Co., Ltd. and have been tested and qualified.
Method: Place the previous medicinal into a gauze bag, decoct with water for 20?mins and take it out. After the temperature cooled to 40~45�C, apply the back to the affected low back area for 30�40 minutes, once a day. The hot compress can help circulate blood and resolve stasis.
TCM Functional Exercise. The exercise is known as �Fei Yan Shi� (literally meaning �the flying swallow style�) in Chinese.
Method: Ask the patient to take a prone position, extend both hands backwards, lift the chest and lower limbs off the bed using the abdomen as a pivot, and then relax. Conduct this exercise once a day and repeat 4-5 times each time.
Functions: Strengthens the power of back muscles, increases the stability of the spine, and thus prevents relapses.
Chinese Tuina (Massage). Ask the patient to take a prone position and find the tenderness spots on the low back. Then apply gun-rolling (10?min), Anrou-pressing and kneading (10?min), and Tanbo-plucking (5?min) manipulation to the tenderness spots and surrounding areas. Conclude with oblique pulling manipulation of the low back. Conduct the treatment once a day.
Functions: Relaxes spasm of the low back muscles and adjusts lumbar subluxation.
After one week TCM treatment, if the patient’s lower back pain without any relief or even aggravated, the prescription of pain medication was adjusted according to clinical guidelines, detailed records the type and dose of pain medication taken by patients, and the patient was identified as no effect.
Control Group
Patients in the control group receive a two-week normal conservative treatment. Intervention measures include three sections, (1) health education. The patients were invited to receive LDH health education twice a week in outpatient; the health education was designed exclusively to inform patients about the natural course of their illness and the expectation of successful recovery, irrespective of the initial intensity of their pain, educate patients to avoid some bad habits that aggravate the disease, such as a sitting position for a long time and carrying heavy loads, and encourage patients to participate in social activities. (2) Rest: in addition to the normal sleep, the patients need to rest in bed for at least 1-2 hours a day. (3) Pain medication or physical therapy: after one week health education, if the patient’s lower back pain without any relief or even aggravated, the prescription of pain medication was adjusted according to clinical guidelines, detailed records the type and dose of pain medication taken by patients. And if the patients do not want to take pain medication, then the patients were referred to a physiotherapist.
Measurements
All outcomes were assessed by observers unaware of the grouping, at baseline (M1), immediately after the last intervention (M2). The followup included the assessments at one month (M3) and six months (M4) after the last intervention.
The primary outcome measure was the change in pain by the visual analogue scale (VAS), scores range 0 to 100, and a higher score indicates a greater pain, 0 means no pain, and 100 means intolerable pain.
The secondary outcome measure was the change in the Chinese Short Form Oswestry Disability Index (C-SFODI), range 0 to 100%. The C-SFODI consists of nine questions, which come from Oswestry Disability Index (ODI); omit the sex life question in Section??8, because this question is always unacceptable by Chinese. The C-SFODI calculation formula is actual cumulative score/45 � 100%, with higher percentage indicating more severe functional disability. And the study has shown that the C-SFODI has good reliability and validity.
Statistical Analysis
Our pretrial power calculation indicated that 81 patients in experimental group were required to detect a difference in pain relief based on the preliminary experiment data at a significant level of 5% (a two-sided t-test) with 80% power. In anticipation of a 20% attrition rate, we sought 102 patients at least in experimental group. Taking into account the poor effect of control therapy, 102 patients were included in the control group.
Between-group difference at baseline was analyzed using independent-samples t-test or Chi-square test. Changes in continuous measures were analyzed by analysis of variance (ANOVA). Effects were evaluated on an intention-to-treat basis (ITT), and participants who did not complete the followup period were considered not having any changes in scores. A two-sided P value of less than 0.05 indicated statistical significance. Results are presented as mean and standard deviation (SD) at M1 and as between-group difference with 95% confidence intervals (CI) at M2, M3, and M4.
Quality Control
Before the beginning of the study, all researchers have to receive protocol training. A clinic research coordinator (CRC) was employed to assist researchers in each center. A monitor was also appointed to ensure the quality of the research.
Dr. Alex Jimenez’s Insight
The above clinical trial focused on investigating the safety and effectiveness of TCM, or traditional Chinese medicine, for low back pain due to lumbar disc herniation as well as to confirm its clinical result. The participants of the research study with low back pain due to LDH were divided into two groups: the experimental group, which was treated with integrative TCM conservative therapy; and the control group, which was treated normal conservative treatment. The experimental group was then further divided into three subgroups. The details of each TCM treatment method used in the subgroups, including the name, ingredients, method and function of each, are described above. The outcomes were measured accordingly by observers unaware of the specific group divisions. The statistic results were properly analyzed by researchers who received protocol training before the start of the study.
Results
Between January 2011 and August 2012, a total of 480 patients with low back pain due to LDH were recruited, 72 were rejected due to exclusion criterions, and 408 eligible patients were randomly assigned in accordance with the ratio of 3?:?1 to the experimental group and the control group, 306 in the experimental group and 102 in the control group. Patients in the experimental group all completed a two-week treatment. In the control group, at the second week one patient in the control group was unwilling to continue to participate and withdrew his informed consent, and two patients took Fenbid (500?mg for each dose, 2 doses a day) since the pain worsened during treatment (Figure 1).
Figure 1: Screening, randomization, and completion evaluations from the baseline to six-month followup, LDH = lumbar disc herniation.
Baseline Characteristics of the Patients
Table 1 shows the baseline data for the 408 participants. The mean age of all patients is 45 years, and 51% were women. In terms of disease staging, experimental group and control group were comparable. And the baseline outcome including VAS scores and C-SFODI were also reasonably well balanced between experimental group and control group.
Table 1: Baseline characteristics of the study participants.
Improvement in the Primary Outcome
The changes in the primary outcomes from baseline to six-month followup are shown in Table 2 and Figure 2. Immediately after the intervention, two groups showed significant decrease in VAS than the baseline. And the experimental group showed a more significant decrease than the control group (?16.62 points [95% confidence interval {CI}, ?20.25 to ?12.98]; P < 0.001).
Figure 2: Mean changes of the primary and secondary outcomes. The means of outcomes are shown for the experimental group (diamond) and the control group (squares). Measurements were obtained at baseline (M1), immediately after the last intervention (M2).
Table 2: Changes in primary and secondary outcomes.
One month after intervention, two groups also had significantly greater reduction in VAS than the baseline. And again, the experimental group showed a more significant decrease than the control group (?6.37 points [95% CI, ?10.20 to ?2.54]; P = 0.001).
Six months after intervention, compared with the baseline, the changes in VAS remained significant in the experimental group and control group, but between-group difference was not significant (P = 0.091).
Improvement in the Secondary Outcome
Immediately after intervention, two groups had significant improvement in C-SFODI than the baseline, and the experimental group showed a more significant improvement than the control group (?15.55 points [95% CI, ?18.92 to ?12.18]; P < 0.001).
One month after intervention, two groups also had significant improvement in C-SFODI than the baseline. And again, the experimental group improved more (?11.37 points [95% CI, ?14.62 to ?8.11]; P < 0.001).
Six months after intervention, two groups also maintained significant improvement, and the experimental group showed superiority (?7.68 points [95% CI, ?11.42 to ?3.94]; P < 0.001).
Adverse Events
One patient in the experiment group had mild fainting during acupuncture, remission by bed rest, and then completed the remaining treatment. Two patients in the control group were given Fenbid orally due to aggravated low back pain. No other adverse events were noted in either experimental group or control group.
Discussion
Although the mechanism of low back pain caused by lumbar disc herniation (LDH) is still not very clear, the prevailing view is that low back pain due to LDH was found to occur not only in response to mechanical stimuli but also to chemical irritation around the nerve root sheath and sinuvertebral nerve.
Different TCM therapies have different advantages in the treatment of LDH. Pain is the main symptom in the acute stage of LDH; acupuncture has good analgesic effect on low back pain due to LDH. Lumbar dysfunction is the main symptom in the remission stage; Chinese massage has good effect on improving dysfunction. Oral Chinese herbal formulae, external use of Chinese medicine, and Chinese herbal injection also showed good effect in relieving pain and improving dysfunction caused by LDH. And one study also found that Salvia miltiorrhiza injection especially works better and faster for the acute stage when compared with mannitol. Although the mechanism of acupuncture, Chinese massage, and traditional Chinese herbs in the treatment of LDH remains unclear, it is generally agreed that these treatment methods play a role by increasing local blood circulation, relieving nerve root edema, and speeding up the metabolism of the local inflammatory mediators. In recovery stage of the disease, the major task is to strengthen the muscles of the waist and abdomen to prevent relapse, and TCM functional exercise has advantages in this regard and can subsequently increase the lumbar stability to prevent recurrence.
Treating LDH according to different stages has been more and more accepted. In China, LDH is mainly divided into three stages, including acute stage, subacute stage (or remission stage), and chronic stage (or recovery stage). Studies have proven that treating LDH according to different stages has obtained a good clinical effect. In addition, studies have also suggested that it can obtain a better effect than treatment without differentiating different stages.
The past 20 years of clinical practice have witnessed the safety of the treatment regimens used in this study. At the same time, its efficacy has been preliminarily confirmed; however, high quality research evidence is still needed. In the treatment regimens, different TCM therapies were selected according to the characteristics of different stages. Specifically, acupuncture and Chinese herbal injections were used in the acute stage for fast pain relief, Chinese Tuina (massage) and external application of Chinese medicine were used in the subacute stage for improvement of the lumbar functions, and low back muscle exercise was used in the chronic stage to increase the stability of the spine and prevent relapses.
In China, nonsurgical treatment of lumbar disc herniation mainly uses drugs, physical therapy, or TCM treatment. TCM treatment used in the experimental group has been used in clinical routine and is considered to have good clinical efficacy; the efficacy of conservative treatment used in the control group is considered very weak, usually as auxiliary treatment of other therapies. Ethics Committee considers that in order to maximize the protection of the interests of the patients, it is necessary to let the patients have more opportunity to receive TCM treatment, so in this research the sample size of the experimental group and the control group is 3?:?1.
The findings of this study have shown that immediately and one month after intervention, integrative TCM conservative treatment can significantly reduce the VAS scores and C-SFODI, and at six month after intervention, integrative TCM conservative treatment can also significantly reduce the C-SFODI, but two groups have no significant difference in reducing VAS score. VAS is an international general pain visual analog scale, and C-SFODI is the improved version of the ODI (Oswestry Disability Index), and it consists of 9 questions, a higher percentage indicating a more severe functional disability.
Regarding adverse events, one patient had mild fainting in the experiment group, two patients in the control group were given Fenbid oral due to low back pain aggravation, and no other adverse events were noted in either experimental group or control group. The mechanism of integrative TCM conservative treatment for LDH remains unclear, and it will be our future research orientation.
The main limitation of this study is the short followup time. As a result, we failed to conduct comprehensive evaluation regarding the long-term efficacy of integrative TCM conservative treatment for LDH.
Conclusions
This randomized controlled clinical trial provides reliable evidence regarding the effectiveness of integrative TCM conservative treatment for patients with low back pain due to lumbar disc herniation. A large sample of long-term followup is further needed for future research.
Conflict of Interests
No potential conflict of interests relevant to this study was reported.
Acknowledgments
This work is supported by the Key Discipline of TCM Orthopaedic and Traumatic of the Ministry of Education of the People’s Republic of China (100508); the Medical Key Project of Shanghai Science and Technology Commission (09411953400); the project of Shanghai Medical leading talent (041); the National Natural Science Foundation of China (81073114, 81001528); the National Key New Drugs Creation Project, innovative drug research and development technology platform (no. 2012ZX09303009-001); Shanghai University Innovation Team Construction Project of the Spine Disease of Traditional Chinese Medicine (2009-26).
In conclusion, with the measured outcomes and final results of the two groups of participants with low back pain due to lumbar disc herniation, the randomized controlled trial helped contribute valuable information regarding the safety and effectiveness, as well as the clinical effect of integrative TCM conservative therapy. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1.�Cypress BK. Characteristics of physician visits for back symptoms: a national perspective.�American Journal of Public Health.�1983;73(4):389�395.�[PMC free article]�[PubMed]
2.�Heliovaara M, Sievers K, Impivaara O, et al. Descriptive epidemiology and public health aspects of low back pain.�Annals of Medicine.�1989;21(5):327�333.�[PubMed]
3.�Peul WC, van Houwelingen HC, van Den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica.�New England Journal of Medicine.�2007;356(22):2245�2256.�[PubMed]
4.�Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the spine patient outcomes research trial.�Spine.�2010;35(14):1329�1338.[PMC free article]�[PubMed]
5.�Jacobs WCH, van Tulder M, Arts M, et al. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review.�European Spine Journal.�2011;20(4):513�522.[PMC free article]�[PubMed]
6.�Kosteljanetz M, Espersen JO, Halaburt H, Miletic T. Predictive value of clinical and surgical findings in patients with lumbago-sciatica. A prospective study (Part I)�Acta Neurochirurgica.�1984;73(1-2):67�76.[PubMed]
7.�Markwalder TM, Battaglia M. Failed back surgery syndrome. Part II: surgical techniques, implant choice, and operative results in 171 patients with instability of the lumbar spine.�Acta Neurochirurgica.�1993;123(3-4):129�134.�[PubMed]
8.�Lee JH, Choi TY, Lee MS, et al. Acupuncture for acute low back pain: a systematic review.�The Clinical Journal of Pain.�2013;29(2):172�185.�[PubMed]
9.�Xu M, Yan S, Yin X, et al. Acupuncture for chronic low back pain in long-term follow-up: a meta-analysis of 13 randomized controlled trials.�The American Journal of Chinese Medicine.�2013;41(1):1�19.[PubMed]
10.�Li D, Dong XJ, Li SB. Clinical observation on lumbar disc Herniation using method of clearing away heat and toxin.�Liaoning Journal of Traditional Chinese Medicine.�2012;39(9):1750�1751.
11.�Zhao CW, Li JX, Leng XY, et al. Clinical analysis on the curative effect of external application of traditional Chinese medicine on lumbar disc herniation.�The Journal of Traditional Chinese Orthopedics and Traumatology.�2010;22(12):21�22.
12.�Kong LJ, Fang M, Zhan HS, et al. Tuina-focused integrative chinese medical therapies for inpatients with low back pain: a systematic review and meta-analysis.�Evidence-Based Complementary and Alternative Medicine.�2012;2012:17 pages.578305�[PMC free article]�[PubMed]
13.�Qiu JW, Wei RQ, Zhang FG. The function of low back muscle exercise in the evaluation of long-term curative effect of patients with lumbar disc herniation.�Chinese Journal of Gerontology.�2010;31(3):413�414.
14.�Li ZH, Liu LJ, Han YQ. Evaluation of clinical pathway Chinese medicine treatment of lumbar disc herniation.�Chinese Journal of Gerontology.�2010;31(2):322�323.
15.�Peul WC, van Houwelingen HC, van der Hout WB, et al. Prolonged conservative treatment or �early� surgery in sciatica caused by a lumbar disc herniation: rationale and design of a randomized trial.�BMC Musculoskeletal Disorders.�2005;6(article 8)�[PMC free article]�[PubMed]
16.�Zheng GX, Zhao XO, Liu GL. Reliability of the modified oswestry disability index for evaluating patients with low back pain.�Chinese Journal of Spine and Spinal Cord.�2010;12(1):13�15.
17.�Anderson SR, Racz GB, Heavner J. Evolution of epidural lysis of adhesions.�Pain Physician.�2000;3(3):262�270.�[PubMed]
18.�Liu J, Fang L, Xu WD, et al. Effects of intravenous drip of compound Danshen injection on plasma NO and SOD levels in patients with lumbar intervertebral disc prolapse.�Chinese Journal of Clinical Health Care.�2004;7(4):272�274.
19.�Pan LH.�?-aescin sodium combined with Danshen injection in the treatment of lumbar disc herniation.�China Modern Doctor.�2010;48(23):117�121.
20.�Rhee HS, Kim YH, Sung PS. A randomized controlled trial to determine the effect of spinal stabilization exercise intervention based on pain level and standing balance differences in patients with low back pain.�Medical Science Monitor.�2012;18(3):CR174�CR181.�[PMC free article]�[PubMed]
21.�Wu K, Li YY, He YF, et al. Overview on clinical staging method of protrusion of lumbar intervertebral disc.�Journal of Liaoning University of Traditional Chinese Medicine.�2010;11(12):44�45.
22.�Li CH, Cai SH, Chen SQ, et al. The investigation of staging comprehensive program treatment for lumbar disc herniation.�Journal of Fujian University of Traditional Chinese Medicine.�2010;20(6):7�9.
23.�Li L, Zhan HS, Chen B, et al. Clinical observation of stage Treatment on 110 cases of lumbar disc herniation.�Chinese Journal of Traditional Medical Traumatology & Orthopedics.�2011;19(1):11�15.
24.�Li CH, Zheng QK, Zhang KM, et al. Phased comprehensive treatment for lumbar disc herniation in 60 cases.�Journal of Beijing University of Traditional Chinese Medicine(Clinical Medicine)�2011;18(6):10�12.
Electroacupuncture: Before reviewing the data below, it is important as a practicing doctor of chiropractic to inform that�sciatica and discogenic lower back pain are two closely related health issues which collectively, can be a source of painful symptoms and discomfort as well as a cause of limited mobility among affected individuals. Discogenic disease, also known as degenerative disc disease, is characterized as the naturally-occurring deterioration of the spinal intervertebral discs. While discogenic disease commonly develops with age, other factors, such as injury can also lead to degenerative disc disease. In addition, degenerative disc disease may cause other complications including bulging or herniated discs
Furthermore, from years of experience caring for patients with this health issue, bulging or herniated discs are not necessarily the cause of the individual’s pain and discomfort. Symptoms are instead the result of compression or irritation from displaced disc material against the spinal cord or an exiting nerve root. Sciatica occurs if the nerve being compressed or irritated is the sciatic nerve, the largest nerve in the human body which branches off the lower spine, down into the legs. Two methods of treatment, electroacupuncture and medium-frequency electrotherapy were used in the following research study to determine whether symptoms of sciatica would improve with one treatment therapy over the other.
Contents
Abstract
Objective. To investigate the short- and long-term effects of electroacupuncture (EA) compared with medium-frequency electrotherapy (MFE) on chronic discogenic sciatica. Methods. One hundred participants were randomized into two groups to receive EA (n = 50) or MFE (n = 50) for 4 weeks. A 28-week follow-up of the two groups was performed. The primary outcome measure was the average leg pain intensity. The secondary outcome measures were the low back pain intensity, Oswestry Disability Index (ODI), patient global impression (PGI), drug use frequency, and�electroacupuncture acceptance. Results. The mean changes in the average leg pain numerical rating scale (NRS) scores were 2.30 (1.86�2.57) and 1.06 (0.62�1.51) in the EA and MFE groups at week 4, respectively. The difference was significant (P < 0.001). The long-term follow-up resulted in significant differences. The average leg pain NRS scores decreased by 2.12 (1.70�2.53) and 0.36 (?0.05�0.78) from baseline in the EA and MFE groups, respectively, at week 28. However, low back pain intensity and PGI did not differ significantly at week 4. No serious adverse events occurred. Conclusions. EA showed greater short-term and long-term benefits for chronic discogenic sciatica than MFE, and the effect of EA was superior to that of MFE. The study findings warrant verification. This trial was registered under identifier ChiCTR-IPR-15006370.
Introduction: Electroacupuncture
Sciatica is defined as radicular leg pain localized to the dermatological distribution of a pathologically affected nerve root. Almost all discogenic sciatica is induced by lumbar disc herniation (LDH) and may be accompanied by neurological deficits, such as leg pain, leg paresthesia, disability, and low back pain. The estimated prevalence of sciatica ranges from 1.2 to 43% in various regions. Discogenic sciatica, which accounts for nearly 90% of sciatica, is a major cause of morbidity; moreover, it has a considerable impact on the economy due to both loss of work and the high costs of health care and societal support for the affected individual and his/her family. Current treatments for discogenic sciatica primarily include surgical and conservative treatments. Although discectomy is a more effective treatment than other treatments for patients with severe discogenic sciatica, in patients with less severe symptoms, surgery or conservative treatments appear to be equally effective. Discectomy should be avoided during initial treatment due to its high cost and its association with a higher incidence of postoperative complications, such as the loss of spine stability and extensive peridural fibrosis. Conservative measures comprise the first-line treatment strategy for managing radicular pain due to disc herniation. Regarding cost-effectiveness, the regimes that employ stepped approaches based on an initial treatment with conservative management have been recommended. However, many conservative treatments have no explicit curative effect, such as benzodiazepines, corticosteroids, traction, and spinal manipulation, which may be ineffective or less effective. Moreover, the long-term efficacy of analgesic drugs is not enduring, and intolerable side-effects, such as addiction, stomach ulcers, and constipation, occur frequently in patients with discogenic sciatica. Thus, based on recent information, the short- and long-term efficacy of conservative treatment should be evaluated.
Electroacupuncture (EA) has been used to treat sciatica for many decades in China. Several studies have reported that electroacupuncture EA may effectively treat neuropathic pain and relieve sciatica symptoms. However, no clear clinical evidence exists to support the application of acupuncture or�electroacupuncture in the treatment of discogenic sciatica according to the guideline for the diagnosis and treatment of lumbar disc herniation. Recently, two meta-analyses concerning sciatica treatment with acupuncture showed that previous studies on acupuncture were flawed and that the strength of the evidence was suboptimal; thus, studies of higher quality with longer-term follow-up are needed to clarify the long-term effect of acupuncture in sciatica patients.
Compared with manual acupuncture,�electroacupuncture treatment is capable of increasing the stimulation frequency and intensity in a controlled and quantifiable manner; moreover, its effect is superior to manual acupuncture for alleviating pain and improving paresthesia and dysfunction. Medium-frequency electrotherapy (MFE) is similar to transcutaneous electrical nerve stimulation (TENS) and may relieve pain and related symptoms. MFE works through electrostimulation of an electrode placed on the skin, and a battery powered device provided a small current to produce a tingling sensation. Several studies found that the effects obtained with 50?Hz EA were superior to those using 2?Hz EA. EA and MFE using the same frequency (50?Hz) at the same location were employed in another trial. The major difference between the two trial groups was the specific impact of needle penetration, with�electroacupuncture using needle penetration and MFE administered via nonpenetrating electrostimulation.
This study was a comparative trial that evaluated the effectiveness of electroacupuncture versus MFE for the treatment of chronic discogenic sciatica; these treatments are the most frequently used treatments for this disease in China. We explored the ability of�electroacupuncture to alleviate leg pain, low back pain, and dysfunction at various evaluation time points, which included an assessment of the long-term efficacy of electroacupuncture. We also assessed the patient global impression (PGI) and acceptance of�electroacupuncture compared with MFE and reports of adverse events.
Methods
Participants
The study commenced on May 28, 2015, and was completed by July 30, 2016, at the South Area of Guang’anmen Hospital, China Academy of Chinese Medical Sciences. Discogenic sciatica was diagnosed according to the criteria of the North American Spine Society. The inclusion criteria were as follows: (1) individuals aged 18 to 70 years; (2) participants whose sciatica symptoms correlated with magnetic resonance imaging (MRI) or computed tomography (CT) findings of lumbar disc herniation; (3) participants whose symptoms of leg pain lasted more than 3 months; (4) participants who agreed to follow the trial protocol; and (5) participants who could complete the study treatment and assessments. The exclusion criteria were as follows: (1) participants with severe progressive neurological symptoms (e.g., cauda equina syndrome and progressive muscle weakness); (2) participants who had undergone surgery for lumbar disc herniation within 6 months; (3) participants with symptoms caused by conditions other than lumbar disc herniation that might lead to radiating pain in the leg; (4) participants with pain in both legs; (5) participants with cardiovascular, liver, kidney, or hematopoietic system diseases, mental health disorders, or cancer for whom EA might be inappropriate or unsafe; (6) participants who had received EA or electrotherapy within the past week; (7) women who were pregnant or lactating; (8) participants who were participating in other clinical trials; and (9) participants with a pacemaker, metal allergy, or severe fear of needles.
Study Design
This was a single-center, prospective, controlled, randomized trial conducted in patients with chronic discogenic sciatica. This trial was approved by the Ethics Committee of Guang’anmen Hospital of China Academy of Chinese Medical Sciences (approval number 2015EC042) on May 26, 2015, and was registered on May 7, 2015, at http://www.chictr.org.cn/ (ref. ChiCTR-IPR-15006370). Written informed consent was obtained from each participant or their legal representative. All participants were required to be able to understand written instructions and able to complete the pain assessment forms.
Randomization and Allocation Concealment
The randomization was performed by the Drug Clinical Trial Office affiliated with Guang’anmen Hospital using a computerized random number generator. Opaque, sealed envelopes were numbered consecutively, and all the sealed envelopes were maintained by a researcher who was not involved in the treatment procedure or data analysis. After informed consent was obtained, an envelope was opened by the researcher according to the patient’s order of entry into the trial, and the assigned treatment was offered to the participant. The outcome assessors and statisticians were blinded to the allocation. Two copies of the envelopes were maintained to prevent the researchers from deviating from the randomization.
Intervention
The treatments were initiated one week after participant randomization. All participants received health education on sciatica, such as using a hard bed and losing weight. During the trial, the use of analgesic drugs or other treatments was not permitted. The details of prior drug use (including dose and time) were recorded in the medication record form. Huatuo Brand stainless steel needles (0.3 � 100?mm, Suzhou Medical Appliance Factory in China, CL) and a G6805-2 electric stimulator (Shanghai Huayi Medical Instrument in China Co., Ltd.) were used in the EA group, and the Quanrikang type J48A computerized intermediate-frequency therapy apparatus (Beijing Huayi New Technical Institute in China) was used in the MFE (control) group. The acupuncture procedures were performed in accordance with the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines. EA was performed by a trained clinician with more than 2 years of experience with acupuncture manipulation. The acupuncture regimen was based on our own pilot trial and specialist consensus. The acupoints of the affected side (DaChangShu, BL25) and the bilateral JiaJi (Ex-B2) corresponding to LDH were included in the EA group. The DaChangShu (BL25) acupoint was located according to the World Health Organization Standardized Acupuncture Point Location; JiaJi (Ex-B2) is located in the lumbar region 0.5 inches lateral to the posterior median line. After the participants assumed a prone position, the needle was vertically inserted rapidly into the JiaJi (Ex-B2) points. Then, the needle was inserted to a depth of approximately 1.5 inches. The participants were expected to experience soreness and distension transmitted to the leg. The needle was inserted straight into the DaChangShu on the BL25 point to a depth of 3 inches; then, the acupuncturist manipulated the needle with a lifting, thrusting, and twirling maneuver until feelings of soreness and distension were felt and radiated to the hips and lower limbs. The electric apparatus was applied to the JiaJi (Ex-B2) and DaChangShu (BL25) acupoints with a dilatational wave using a 50?Hz frequency and a comfortably tolerated maximum current intensity.
Participants assigned to the control group received MFE, which was administered by an experienced therapist different from the one delivering the EA. The acupoints and frequencies used in the MFE group were the same as those used in the EA group. After two pairs of 107 � 72?mm electrodes were placed on the acupoints, the MFE apparatus was turned on and muscle contractions were observed under the energizing electrode. The intensity was adjusted to the maximum current intensity tolerable at a comfortable level. The treatments in both groups were performed once daily for 5 sessions/week for the first 2 weeks and followed by 3 sessions/week for the following 2 weeks, with each session lasting 20 minutes.
Data Collection
The data in the trial were obtained from the case report forms recorded by the investigator. The participants’ demographic, clinical, and radiological characteristics were recorded. The diagnosis of lumbar disc herniation was confirmed after a review of the patient’s MRI or CT scan by two experienced musculoskeletal radiologists. Additionally, the diagnosis of discogenic sciatica was confirmed after a clinical examination by a consultant orthopedic physician. Investigators entered the collected data into the case report forms. At baseline and during the treatment period, the forms were completed by the participants under the guidance of a full-time staff member. During the follow-up period (16th and 28th weeks), the participants answered the questionnaire by phone.
Clinical Assessments
The primary outcome was the change from baseline in the average leg pain numerical rating scale (NRS) score at week 4. The secondary outcomes included average leg pain intensity at weeks 1, 2, 3, 16, and 28; low back pain intensity at weeks 2, 4, 16, and 28; Oswestry Disability Index (ODI) questionnaire results at weeks 2, 4, 16, and 28; PGI of improvement at weeks 2 and 4; drug use frequency at weeks 2 and 4; and EA acceptance evaluation at week 4. Adverse events were monitored and documented during the treatment and follow-up periods based on the investigator’s inquiry and reports by the participants themselves.
Primary Outcome Measure: The change from baseline in the average leg pain NRS score was measured using an 11-point numerical rating scale assessing leg pain, with 0 representing no pain and 10 representing the most severe pain. Participants were asked to rate their average leg pain intensity over the prior 24 hours. The average leg pain NRS score at week 4 was equal to the mean value of the NRS scores obtained at the three treatment sessions during the 4th week.
Secondary Outcome Measures: The following secondary outcome measures were determined. (1) The average leg pain intensity at other time points was measured by the NRS. The methods used to measure the secondary outcomes were the same as those used to measure the primary outcome except for the evaluation point. (2) Low back pain intensity was measured using an 11-point NRS. Participants rated their low back pain over the prior 24 hours with a pain NRS. The low back pain NRS score at the time of evaluation was equal to the mean value of the NRS scores in the previous 24 hours. (3) The ODI comprises 10 questions concerning the intensity of pain and daily activities. Each item contains 6 options. A higher score change in the ODI from baseline indicated more serious dysfunction. (4) The PGI improvement score was used to evaluate the improvement in pain and functional disability, and the improvement reported by patients was assessed using a 7-point scale (1 represents greatly improved and 7 represents marked worsening). (5) The frequency of drug use was recorded. The patients’ use of medications or nonprescription drugs during the trial was evaluated using a questionnaire to assess the influence of drugs. (6) To investigate which treatment was preferred, EA or MFE acceptance was assessed at week 4. A 4-point scale was used, with 1 representing �very difficult to accept� and 4 representing �very easy to accept.� (7) Adverse events were assessed using a questionnaire at the end of treatment and active reporting by the participants during treatment.
Sample Size and Statistical Analysis
The sample size calculation was based on the mean value of the leg pain intensity NRS score. According to our pilot trial, the decreases in the mean value of the leg pain intensity NRS scores in the EA and MFE groups at week 4 were 3.41 � 3.46 and 1.57 � 1.24, respectively. Our pilot study was an independent study conducted by our research team before this study, with no crossover participants between the previous study and the current study. We used PASS Version 11.0 (International Business Machines Corporation, China) software to calculate a sample size of 50 for each group to provide 90% power to detect a difference of 1.8 between the groups with a two-sided 5% level of significance, allowing for a 20% dropout rate and with the participants receiving the treatments and completing the follow-up.
The statistical analysis was performed using SPSS Version 22.0 (International Business Machines Corporation, China) software. Two-sided tests were used for all statistical analyses. The level of significance was established at 0.05. All patients who accepted randomization were included in the analysis. All data collected from the participants were included in the statistical analysis, and missing data were replaced by the last observed value. However, the outcomes for which no data except for the baseline assessment data were available were not included in the final analysis. The 100 participants included at least 1 treatment session. Thus, we analyzed the data of all the participants as the primary outcome, which was measured after the first treatment session. However, the secondary outcomes were evaluated at week 2, and 13 participants dropped out before week 2 without any data after treatment except for leg pain NRS scores. So the 13 participants were not included in the statistical analysis of secondary outcomes. Continuous data were represented by means and standard deviations (SD) if the data were normally distributed or by the medians and interquartile ranges if the data were skewed, or by means and 95% confidence intervals (CIs); categorical data were represented by percentages or 95% CIs. For comparisons with baseline data, a paired t-test was used for continuous data and a nonparametric test was used for categorical data. To compare the two independent samples, T tests or Mann�Whitney U tests were used to compare continuous variables, and chi-square tests or Fisher’s exact tests were used to compare categorical variables, as appropriate. A repeated measures analysis of variance or nonparametric test was used to compare differences in data between the groups at multiple time points.
Results
Dr. Alex Jimenez’s Insight
The short- and long-term effects of electroacupuncture (EA) versus medium-frequency electrotherapy (MFE) were evaluated to determine which of the two treatments, if not both, could most effectively be used to help improve symptoms of sciatica associated with degenerative disc disease. The research study was conducted with the participation of a variety of patients with symptoms of discogenic sciatica, over several types of interventions. Clinical assessments and data was collected throughout two different research study outcomes in order to gather the most valuable results. Sample size and statistical analysis were also considered before analyzing the data of all the participants and recording the results. The final outcome of the research study has been described in detail below.
Recruitment
A total of 138 participants with chronic sciatica due to lumbar disc protrusion were screened, among whom 36 were rejected due to the exclusion criteria and 2 withdrew from the study. Therefore, 100 eligible patients were randomly assigned to the experimental (EA) group (n = 50) or the control (MFE) group (n = 50) at a ratio of 1?:?1. Eight participants withdrew from the study during the course of treatment due to the presence of aggravating symptoms, 1 participant exited the study due to travel, 1 participant withdrew due to an unsatisfactory curative effect, and 3 participants were lost to follow-up. In the dropout participants, no additional data except for the leg pain NRS scores were available because the evaluation period was not reached. According to the principle of ITT analysis, we analyzed the data of all 100 subjects for the leg pain NRS scores and then performed a sensitivity analysis of these 13 subjects to verify the reliability of the results. Details are provided in Figures ?1 and ?2.
Figure 1: Time frame of each period. Figure 1 shows the time frame of baseline period, treatment period, and follow-up period.
Figure 2: Study flow diagram.
Characteristics of the Participants
Table 1 shows the baseline data of the 100 participants. The mean age of all patients was 52.67 � 12.72 years. The mean duration was 48 (12�120) months. The duration of 2 participants in the electroacupuncture group was one month, and the duration of 1 participant was one month in the MFE group. The baseline demographics, body measurement data, and baseline outcomes are listed in Table 1. No significant differences in baseline demographics and clinical characteristics were observed (Table 1).
Table 1: Baseline demographic and clinical characteristics of the study population.
Primary Outcome
The decrease in the leg pain NRS scores from baseline to week 4 differed significantly between the EA group (n = 50) and the MFE group (n = 50) (P < 0.001). As shown in Table 2, the mean change from baseline to the 4th week in the average leg pain intensity NRS score was 2.30 (1.86�2.75) in the EA group and 1.06 (0.62�1.51) in the MFE group. At four weeks, the two groups both exhibited significantly greater reductions in NRS scores compared with baseline; however, the EA group showed a more significant decrease than the MFE group (Table 2).
Table 2: Changes from baseline in primary outcomes.
Secondary Outcomes
EA showed a more significant improvement in the leg pain scores at all the evaluation points compared with that observed in the MFE group (P < 0.001) (Figure 3 and Table 2). The EA group showed a significant decrease compared to the baseline in the leg pain, low back pain, and ODI scores at weeks 2, 4, 16, and 28 (all P < 0.05). Conversely, the MFE group did not show a significant improvement compared to the baseline in the low back pain score at weeks 16 and 28 (all P = 0.096). Significant reductions in the leg pain and ODI questionnaire scores were detected in the EA group at multiple time points compared with the MFE group (all P < 0.05). The EA group exhibited greater improvement. However, a negligible change was detected at multiple time points in the low back pain score and PGI between the two groups (all P > 0.05). Furthermore, no significant difference was detected in the frequency of drug use between the two groups at weeks 2 and 4 (all P > 0.05) in our trial. Consequently, an EA or MFE acceptance assessment administered after 4 weeks of intervention showed that EA was accepted as readily as MFE with no significant differences between the two groups (P = 0.055). The corresponding data are shown in Tables ?2 and ?3.
Figure 3: Change of leg pain score in two groups.
Table 3: Secondary outcomes of the interventions.
A sensitivity analysis was performed based on the leg pain NRS score. We excluded 13 participants who received fewer treatment sessions (less than 10) and analyzed the data of the remaining 87 participants. This sensitivity analysis result showed that our original results were stable and reliable.
Adverse Events
No serious adverse events occurred in either group. One participant (2%) in the experimental group developed a subcutaneous hematoma. Two participants (4%) in the MFE group reported skin redness and itching. All adverse events disappeared without additional intervention.
Discussion
The results of this trial showed significant differences in the change in the leg pain NRS and ODI questionnaire scores in the EA group compared with those in the MFE group in the short-term treatment period and long-term follow-up. However, the EA group did not show a greater decrease in low back pain scores and PGI compared with the MFE group. These changes indicated that the effect of EA was superior to the effect of MFE in improving leg pain and dysfunction, whereas the effect of EA was not superior to that of MFE in relieving low back pain and systemic symptoms.
The leg pain NRS score showed a significant difference compared with the MFE group at week 4: a mean difference of 1.24 points was detected between the two groups. On average, a reduction of approximately 2�3.5 points in the NRS score represents a minimal clinically important difference (MCID) for acute and chronic pain. The change in the leg pain NRS score in the EA group at week 4 did not show a clinically important significant difference compared with the MFE group. However, our control group was not a placebo but a positive treatment. An effect size of 1.24 is generally considered as the large effect. The MCID of the ODI score ranged from 4 to 16 points, and the decline of the ODI score in the EA group reached the MCID criterion with a mean reduction of 5.69 compared with the MFE group. The results implied that the clinical effect of EA appears superior to the effect of MFE in improving dysfunction caused by sciatica. However, low back pain did not show a significant and clinically important difference, with a mean reduction in the NRS score of 0.58 at week 4 compared with the MFE group. It may be associated with a better response to pain around the electrodes by MFE. In our study, a long-term follow-up was performed. At week 28, the MFE group did not show significantly decreased leg pain compared to the baseline, whereas the EA group showed significantly decreased leg pain compared to the baseline. The difference between the two groups was significant. The results implied that the effect of EA but not MFE lasted at least 28 weeks. The low back pain and ODI scores also indicated that the long-term effects of EA were superior to those of MFE because the effects of EA persisted after the discontinuation of treatment.
In our trial, the leg pain NRS score was reduced by 49% compared with the baseline in the EA group at week 4; however, a greater increase in the response rate (69%) was reported in a trial comparing EA with TENS for sciatica during the treatment period. Another trial conducted in China demonstrated that the decrease in the mean value of the leg pain intensity NRS score in the EA group was 4.65 � 6.37 at week 4, which was higher than the value of 2.30 (1.86�2.75) obtained in our trial at the same time point. In a pilot trial comparing EA with physical therapy for symptomatic lumbar spinal stenosis (LSS), pain in the back and leg showed small improvements at 3 months. However, the ODI scores were different from the scores obtained in our study. No significant differences between the ODI scores of the two groups were observed at the 3-month follow-up time point in the study. The differences between the results of the two studies might be explained by the use of different acupoints, needling depth, manipulation methods, EA parameters, number and frequency, training and clinical experience level of the practitioners, missing data, and sample size.
Very few participants in either group took analgesics during the trial, and only anti-inflammatory drugs were used. This result might indicate that most of the participants believed that the analgesics would not alleviate pain and were concerned about adverse events. Most participants expected that EA or MFE would be beneficial and were aware that these techniques are relatively safe. According to the PGI, the participants perceived no difference between EA and MFE. Approximately 87.2% of the participants in the EA group reported that they were aided by EA at the 4th week, which was similar to the 83.5% of participants in the MFE group. The treatment acceptance assessment showed that none of the participants considered either treatment difficult to accept. Furthermore, 70.2% of the participants in the EA group reported that EA was easy or very easy to accept, similar to 72.5% of the participants in the MFE group. These results indicated that EA and MFE were both easy to accept and popular in China.
Leg pain is a typical symptom in sciatica patients, and the leg pain intensity NRS score reflects the improvement in this symptom in these patients. The leg pain NRS score may reasonably be used for the primary measurement of the therapeutic effect. Because studies have shown that most acupuncture therapy for sciatica lasts 1 to 4 weeks, we selected the change in the average leg pain intensity NRS score from baseline to the 4th week as the main measurement. In the previous literature, although primary outcome was generally measured at a certain time point, the average score reflected the average level of pain during the last week, which was thus more meaningful than other methods of measuring single time point due to recurrence of sciatica. The control group underwent MFE, which exerts its effect via the stimulation or activation of physiological events by applying energy, thereby producing therapeutic benefits that facilitate pain relief. Mechanisms leading to pain relief may be due to a variety of peripheral effects of control activity, on the spinal and spinal nervous system. The comparison between EA and MFE may reveal differences in response to needle penetration using the same electrostimulation. Because the stimulation parameters, particularly the frequency, are important factors that affect the outcome and because the effect of medium-frequency electrotherapy is better than the effect of low frequency electrotherapy, we used the same medium frequency and location in the study to ensure that the two groups were comparable.
Many studies have investigated the mechanism of EA. EA has been reported to relieve the symptoms of sciatica and increase the pain threshold in humans. Several previous studies showed that EA inhibited the primary afferent transmission of neuropathic pain and that deep EA stimulation improved the pathological changes and function of the injured sciatic nerve in rats. Other studies have suggested that descending inhibitory control, changes in nerve blood flow, or the inhibition of activity by nerve endings may be involved in the mechanism associated with the efficacy of EA. Long-lasting alleviation of pain has been suggested to be closely related to the muscle tension improvement provided by EA. A meta-analysis of patients with chronic pain showed that approximately 90% of the benefit of acupuncture was sustained at 12 months. The reason for the cumulative and sustained effects of acupuncture may be associated with the brain response and the cumulative duration of acupuncture stimulation.
This trial has several limitations. First, the participants and acupuncturists could not be blinded due to the significant difference between the two treatments. However, we followed rigorous quality control procedures in other aspects of the methodology. For example, a strict randomization and allocation concealment protocol was adopted. The outcome assessors and statisticians were blinded to the allocation. Second, some of the outcome measures of the trial were subjective. To address subjectivity, a short training session for the patients on the outcome reporting was held before they began the trial, and all subjective outcomes were based on the patient self-report forms. Third, we did not include a placebo control in the present preliminary study because several sham acupuncture randomized controlled trials (RCTs) have been performed to study acupuncture therapy in patients with sciatica. We considered that the use of a placebo did not provide sufficient sensitivity and may not have met ethical guidelines. Fourth, because we did not explore the effect of electroacupuncture EA on various degrees of pain severity, which degree of sciatica was most sensitive to EA was unclear. Subgroup analyses based on sciatica severity should be performed in a future multicenter, large-sample, randomized controlled study.
Conclusions: Electroacupuncture
This randomized controlled clinical trial demonstrated that the short-term and long-term effectiveness of electroacupuncture were superior to those of MFE in improving the symptoms of leg pain and dysfunction caused by chronic discogenic sciatica; moreover, the long-term effect of electroacupuncture was superior to that of MFE in improving low back pain. The results also suggested that the effect of electroacupuncture but not MFE lasted at least 28 weeks. No serious adverse events occurred in either group. Further studies are needed to examine the effectiveness of electroacupuncture relative to various physical therapy methods for patients with discogenic sciatica.
Acknowledgments
This trial was supported by the South Area of Guang’anmen Hospital science fund (Funding no. Y2015-07).
Conflicts of Interest
The authors have no conflicts of interest to declare.
In conclusion,�the effectiveness of electroacupuncture was superior to MFE towards improving the symptoms of discogenic sciatica. Although the research study concluded that electroacupuncture was superior to medium-frequency electrotherapy when treating for sciatica caused by degenerative disc disease, both types of treatments should still be used accordingly, depending on the patient’s condition and whether the specific treatment is best recommended by a healthcare professional. Electroacupuncture and medium-frequency electrotherapy are the most common types of treatment options for symptoms of sciatica associated with the deterioration of the spinal intervertebral discs. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Konstantinou K., Dunn K. M. Sciatica: review of epidemiological studies and prevalence estimates. Spine. 2008;33(22):2464�2472. doi: 10.1097/brs.0b013e318183a4a2. [PubMed] [Cross Ref]
2. Ergun T., Lakadamyali H. CT and MRI in the evaluation of extraspinal sciatica. British Journal of Radiology. 2010;83(993):791�803. doi: 10.1259/bjr/76002141. [PMC free article] [PubMed] [Cross Ref]
3. Dagenais S., Caro J., Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine Journal. 2008;8(1):8�20. doi: 10.1016/j.spinee.2007.10.005. [PubMed] [Cross Ref]
4. Asche C. V., Kirkness C. S., McAdam-Marx C., Fritz J. M. The societal costs of low back pain: data published between 2001 and 2007. Journal of Pain and Palliative Care Pharmacotherapy. 2007;21(4):25�33. doi: 10.1300/j354v21n04_06. [PubMed] [Cross Ref]
5. Saal J. A., Saal J. S. Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. An outcome study. Spine. 1989;14(4):431�437. doi: 10.1097/00007632-198904000-00018. [PubMed] [Cross Ref]
6. Kreiner D. S., Hwang S. W., Easa J. E., et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine Journal. 2014;14(1):180�191. doi: 10.1016/j.spinee.2013.08.003. [PubMed] [Cross Ref]
7. Alexandre A., Cor� L., Azuelos A., Pellone M. Percutaneous nucleoplasty for discoradicular conflict. Acta Neurochirurgica. Supplement. 2005;92:83�86. [PubMed]
8. Zhu R. S., Ren Y. M., Yuan J. J., et al. Does local lavage influence functional recovery during lumber discectomy of disc herniation? One year’s systematic follow-up of 410 patients. Medicine. 2016;95(42) doi: 10.1097/md.0000000000005022.e5022 [PMC free article] [PubMed] [Cross Ref]
9. Nguyen C., Palazzo C., Grabar S., et al. Tumor necrosis factor-a? blockade in recurrent and disabling chronic sciatica associated with post-operative peridural lumbar fibrosis: results of a double-blind, placebo randomized controlled study. Arthritis Research and Therapy. 2015;17(1, article 330) doi: 10.1186/s13075-015-0838-4. [PMC free article] [PubMed] [Cross Ref]
10. Haghnegahdar A., Sedighi M. An outcome study of anterior cervical discectomy and fusion among Iranian population. Neuroscience Journal. 2016;2016:7. doi: 10.1155/2016/4654109.4654109 [PMC free article] [PubMed] [Cross Ref]
11. Lewis R., Williams N., Matar H. E., et al. The clinical effectiveness and cost-effectiveness of management strategies for sciatica: systematic review and economic model. Health Technology Assessment. 2011;15(39):1�578. doi: 10.3310/hta15390. [PMC free article] [PubMed] [Cross Ref]
12. Chou R., Deyo R., Friedly J., et al. Noninvasive Treatments for Low Back Pain. Rockville, Md, USA: Agency for Healthcare Research and Quality; 2016. AHRQ comparative effectiveness reviews.
13. Robaina-Padr�n F. J. Controversies of instrumented surgery and pain relief in degenerative lumbar spine. Results of scientific evidence. Neurocirugia. 2007;18(5):406�413. doi: 10.1016/S1130-1473(07)70266-X. [PubMed] [Cross Ref]
14. Qin Z., Liu X., Wu J., Zhai Y., Liu Z. Effectiveness of acupuncture for treating sciatica: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine. 2015;2015 doi: 10.1155/2015/425108.425108 [PMC free article] [PubMed] [Cross Ref]
15. Ji M., Wang X., Chen M., Shen Y., Zhang X., Yang J. The efficacy of acupuncture for the treatment of sciatica: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine. 2015;2015:12. doi: 10.1155/2015/192808.192808 [PMC free article] [PubMed] [Cross Ref]
16. Pang T., Lu C., Wang K., et al. Electroacupuncture at ST25 inhibits cisapride-induced gastric motility in an intensity-dependent manner. Evidence-based Complementary and Alternative Medicine. 2016;2016:7. doi: 10.1155/2016/3457025.3457025 [PMC free article] [PubMed] [Cross Ref]
17. MacPherson H., Vertosick E., Foster N., et al. The persistence of the effects of acupuncture after a course of treatment: a meta-analysis of patients with chronic pain. Pain. 2016 doi: 10.1097/j.pain.0000000000000747. [PMC free article] [PubMed] [Cross Ref]
18. MacPherson H., Altman D. G., Hammerschlag R., et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. Journal of Evidence-Based Medicine. 2010;3(3):140�155. doi: 10.1111/j.1756-5391.2010.01086.x. [PubMed] [Cross Ref]
19. Qiu T., Li L. Discussion on the Chinese edition of the WHO standard acupuncture point locations in the western Pacific region. Chinese Acupuncture and Moxibustion. 2011;31(9):827�830. [PubMed]
20. Selim A. J., Ren X. S., Fincke G., et al. The importance of radiating leg pain in assessing health outcomes among patients with low back pain: results from the veterans health study. Spine. 1998;23(4):470�474. doi: 10.1097/00007632-199802150-00013. [PubMed] [Cross Ref]
21. Fairbank J. C. T., Pynsent P. B. The oswestry disability index. Spine. 2000;25(22):2940�2953. doi: 10.1097/00007632-200011150-00017. [PubMed] [Cross Ref]
22. Lee J., Shin J.-S., Lee Y. J., et al. Effects of Shinbaro pharmacopuncture in sciatic pain patients with lumbar disc herniation: study protocol for a randomized controlled trial. Trials. 2015;16(1, article 455) doi: 10.1186/s13063-015-0993-6. [PMC free article] [PubMed] [Cross Ref]
23. Ostelo R. W. J. G., de Vet H. C. W. Clinically important outcomes in low back pain. Best Practice and Research. Clinical Rheumatology. 2005;19(4):593�607. doi: 10.1016/j.berh.2005.03.003. [PubMed] [Cross Ref]
24. Farrar J. T., Young J. P., Jr., LaMoreaux L., Werth J. L., Poole R. M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149�158. doi: 10.1016/S0304-3959(01)00349-9. [PubMed] [Cross Ref]
25. Wang Z.-X. Clinical observation on electroacupuncture at acupoints for treatment of senile radical sciatica. Chinese Acupuncture & Moxibustion. 2009;29(2):126�128. [PubMed]
26. Yuan W. A., Huang S. R., Guo K., et al. Integrative TCM conservative therapy for low back pain due to lumbar disc herniation: a randomized controlled clinical trial. Evidence-Based Complementary and Alternative Medicine. 2013;2013:8. doi: 10.1155/2013/309831.309831 [PMC free article] [PubMed] [Cross Ref]
27. Kim K. H., Kim Y. R., Baik S. K., et al. Acupuncture for patients with lumbar spinal stenosis: a randomised pilot trial. Acupuncture in Medicine. 2016;34(4):267�274. doi: 10.1136/acupmed-2015-010962. [PubMed] [Cross Ref]
28. Tiktinsky R., Chen L., Narayan P. Electrotherapy: yesterday, today and tomorrow. Haemophilia. 2010;16, supplement 5:126�131. doi: 10.1111/j.1365-2516.2010.02310.x. [PubMed] [Cross Ref]
29. Zhao X.-Y., Zhang Q.-S., Yang J., et al. The role of arginine vasopressin in electroacupuncture treatment of primary sciatica in human. Neuropeptides. 2015;52:61�65. doi: 10.1016/j.npep.2015.06.002. [PubMed] [Cross Ref]
30. Wang W.-S., Tu W.-Z., Cheng R.-D., et al. Electroacupuncture and A-317491 depress the transmission of pain on primary afferent mediated by the P2X3 receptor in rats with chronic neuropathic pain states. Journal of Neuroscience Research. 2014;92(12):1703�1713. doi: 10.1002/jnr.23451. [PubMed] [Cross Ref]
31. Liu Y.-L., Li Y., Ren L., et al. Effect of deep electroacupuncture stimulation of �Huantiao� (GB 30) on changes of function and nerve growth factor expression of the injured sciatic nerve in rats. Zhongguo Yi Xue Ke Xue Yuan Yi Xue Qing Bao Yan Jiu Suo Bian Ji. 2014;39(2):93�99. [PubMed]
32. Inoue M., Hojo T., Yano T., Katsumi Y. Electroacupuncture direct to spinal nerves as an alternative to selective spinal nerve block in patients with radicular sciatica�a cohort study. Acupuncture in Medicine. 2005;23(1):27�30. doi: 10.1136/aim.23.1.27. [PubMed] [Cross Ref]
33. Fan Y., Wu Y. Effect of electroacupuncture on muscle state and infrared thermogram changes in patients with acute lumbar muscle sprain. Journal of Traditional Chinese Medicine. 2015;35(5):499�506. [PubMed]
34. Li C., Yang J., Park K., et al. Prolonged repeated acupuncture stimulation induces habituation effects in pain-related brain areas: an fMRI study. PLoS ONE. 2014;9(5) doi: 10.1371/journal.pone.0097502.e97502 [PMC free article] [PubMed] [Cross Ref]
35. Khadilkar A., Odebiyi D. O., Brosseau L., Wells G. A. Transcutaneous electrical nerve stimulation (TENS) versus placebo for chronic low-back pain. Cochrane Database of Systematic Reviews. 2008;4(4)CD003008 [PubMed]
Acknowledging the subsequent information below,�approximately more than 2 million people are injured in automobile accidents each year and among those incidents, the majority of the people involved are diagnosed with whiplash and/or neck injury by a healthcare professional. When the complex structure of the neck is subjected to trauma, tissue damage and other medical complications may occur. Vertebral artery dissection, or VAD, is characterized by a flap-like tear on the inner lining of the vertebral artery in charge of supplying blood to the brain. After the tear, blood can then enter the arterial wall and form a blood clot, thickening the artery wall and often impeding blood flow.
Through years of experience practicing chiropractic care,�VAD may often follow after trauma to the neck, such as that which occurs in an automobile accident, or whiplash injury. The symptoms of vertebral artery dissection include head and neck pain as well as intermittent or permanent stroke symptoms, such as difficulty speaking, impaired coordination and loss of vision. VAD, or vertebral artery dissection, is generally diagnosed with a contrast-enhanced CT or MRI scan.
Contents
Abstract
A 30-year-old woman presented to an emergency department with sudden onset of transient loss of left peripheral vision. Owing to a history of migraine headaches, she was released with a diagnosis of ocular migraine. Two days later, she sought chiropractic care for the chief symptom of severe neck pain. The chiropractor suspected the possibility of vertebral artery dissection (VAD). No manipulation was performed; instead, MR angiography (MRA) of the neck was obtained, which revealed an acute left VAD with early thrombus formation. The patient was placed on aspirin therapy. Repeat MRA of the neck 3?months later revealed resolution of the thrombus, without progression to stroke. This case illustrates the importance for all healthcare providers who see patients with neck pain and headache to be attentive to the symptomatic presentation of possible VAD in progress.
Background
Vertebral artery dissection (VAD) leading to stroke is an uncommon but potentially serious disorder. The incidence of stroke related to the vertebrobasilar system varies from 0.75 to 1.12/100?000 person-years. The pathological process in VAD typically involves dissection of the wall of the artery followed sometime later by thrombus formation, which may cause arterial occlusion or may lead to embolisation, causing occlusion of one or more of the distal branches off the vertebral artery, including the basilar artery, which can be catastrophic. VAD typically occurs in patients who have an inherent, transitory weakness in the arterial wall. In at least 80% of cases, the initial symptoms include neck pain with or without headache.
Many patients with VAD may in the early stages present to chiropractors seeking relief from neck pain and headache, without realising they are experiencing VAD. In many of these cases, the patient later develops a stroke. Until recently, it was assumed that the dissection (and subsequent stroke) was caused by cervical manipulative therapy (CMT). However, while early studies found an association between visits to a chiropractor and subsequent stroke related to VAD, recent data suggest that this relationship is not causal.
This case report is illustrative of the scenario in which a patient with an undiagnosed VAD in evolution consulted a chiropractor for neck pain and headache. After thorough history and examination, the chiropractor suspected VAD and did not perform CMT. Instead, the patient was referred for further evaluation, which detected a VAD in progress. Prompt diagnosis and anticoagulant treatment were thought to have averted progression to a stroke.
Case Presentation
A 30-year-old otherwise healthy woman consulted a chiropractor (DBF), reporting of right-sided neck pain in the suboccipital region. The patient reported that, 3?days previously, she had gone to the local hospital emergency department (ED) because of the sudden onset of loss of left peripheral vision. The visual symptoms interfered with her ability to see through her left eye; this was accompanied by �numbness� in her left eyelid. About 2?weeks prior to this ED visit, she had experienced an episode of acute left-sided neck pain with severe left-sided headache. She also related a history of migraine headache without prodrome. She was released from the ED with a tentative diagnosis of ocular migraine. She had never been previously diagnosed with ocular migraine, nor had she ever experienced any visual disturbances with her previous migraines.
Shortly after the left-sided ocular symptoms resolved, she suddenly developed right-sided neck pain without provocation, for which she sought chiropractic treatment. She also reported a transient episode of right-sided visual disturbance occurring that same day as well. This was described as sudden blurriness that was of short duration and resolved spontaneously earlier in the day of her presentation for chiropractic examination. When she presented for the initial chiropractic examination, she denied current visual disturbance. She said that she was not experiencing any numbness, paraesthesia or motor loss in the upper or lower extremities. She denied ataxia or difficulty with balance. Medical history was remarkable for childbirth 2� months prior to initial presentation. She stated that her migraine headaches were associated with her menstrual cycle. Family history was remarkable for a spontaneous ascending thoracic aortic aneurysm in her older sister, who was about 30?years of age when her aneurysm had occurred.
Investigations
Based on the history of sudden onset of severe upper cervical pain and headache with visual disturbance and ocular numbness, the DC was concerned about the possibility of early VAD. Urgent MR angiography (MRA) of the neck and head, along with MRI of the head, was ordered. No cervical spine examination or manipulation was performed because of the suspicion that the neck pain was related to VAD rather than to a �mechanical� cervical disorder.
MRA of the neck demonstrated that the left vertebral artery was small and irregular in calibre, extending from the C7 level cephalad to C2, consistent with dissection. There was a patent true lumen with a surrounding cuff of T1 hyper-intensity, consistent with dissection with subintimal thrombus within the false lumen (Figures 1 and ?2). MRI of the head with and without contrast, and MRA of the head without contrast, were both unremarkable. Specifically, there was no intracranial extension of dissection or evidence of infarction. MR perfusion of the brain revealed no focal perfusion abnormalities.
Figure 1: Axial proton density image demonstrates circumferential hyper-intensity surrounding the left cervical vertebral artery (representing the false lumen). Note decreased calibre of true lumen (black flow void) with respect to the right vertebral artery.
Figure 2: Axial image from three-dimensional time-of-flight MRA demonstrates T1 hypointense dissection flap separating the true lumen (lateral) from the false lumen (medial). MRA, MR angiography.
Differential Diagnosis
The ED released the patient with a tentative diagnosis of ocular migraine, due to her history of migraine headaches. However, the patient stated that the left-sided headache was atypical��like nothing I’ve ever experienced before.� Her previous migraines were associated with her menstrual cycle, but not with any vision changes. She had never been previously diagnosed with ocular migraine. MRA of the cervical region revealed that the patient actually had an acute dissection with thrombus formation in the left vertebral artery.
Treatment
Owing to the potential of impending stroke associated with an acute VAD with thrombus formation, the patient was admitted to the neurology stroke service for close neurological monitoring. During her admission, the patient did not experience any recurrence of neurological deficits and her headaches improved. She was discharged the following day with a diagnosis of left VAD and transient ischaemic attack. She was instructed to avoid vigorous exercise and trauma to the neck. Daily aspirin (325?mg) was prescribed, to be continued for 3�6?months after discharge.
Outcome and Follow-Up
After discharge from the stroke service, the patient had no recurrence of headache or visual disturbances, and her posterior neck pain symptoms resolved. Repeat imaging was performed 3?months after presentation, which demonstrated improved calibre of the cervical left vertebral artery with resolution of the thrombus within the false lumen (Figure 3). Imaging of the intracranial compartment remained normal, without evidence of interval infarction or perfusion asymmetry.
Figure 3: Maximum intensity projection (MIP) images from three-dimensional time-of-flight MRA (left image is at time of presentation and right image is at 3-month follow-up). The initial imaging demonstrates markedly diminutive calibre of the left vertebral artery
Discussion
The pathophysiological process of VAD is thought to start with degeneration of the tissues at the medial-adventitial border of the vertebral artery, leading to the development of microhaematomata within the wall of the artery and, eventually, arterial tear. This can lead to leakage of blood into the arterial wall, causing occlusion of the lumen with subsequent thrombus formation and embolisation, resulting in stroke related to one of the branches of the vertebral artery. This pathological process is similar to that of spontaneous carotid artery dissection, spontaneous thoracic aortic dissection and spontaneous coronary artery dissection. All these conditions tend to occur in younger adults and some have speculated that they may be part of a common inherited pathophysiological process. Notable in this case is the fact that the patient’s older sister had experienced a spontaneous thoracic aortic aneurysm (probably a dissection) at around the same age (30?years) as this patient was when she experienced her VAD.
While the dissection is often sudden, the luminal compromise and complications of VAD can develop gradually leading to variable symptoms and presentation, depending on the stage of the disease. The dissection itself, which develops some time before the onset of neural ischaemia, can cause stimulation of nociceptive receptors within the artery, producing pain that is most commonly felt in the upper cervical spine or head. Only after the pathophysiological process progresses to the point of complete arterial occlusion or thrombus formation with distal embolisation does the full manifestation of infarction occur. However, as illustrated in this case, neurological symptoms can develop early in the process, particularly in cases in which the true lumen demonstrates significant calibre decrease secondary to compression.
There are several interesting aspects to this case. First, it highlights the importance of spine clinicians being alert to the possibility that what may appear to be typical �mechanical� neck pain could be something potentially more sinister, such as VAD. The sudden onset of severe suboccipital pain, with or without headache, and accompanying brainstem related neurological symptoms, should alert the clinician to the possibility of VAD. As in the case reported here, patients with a history of migraine will typically describe the headache as different from their usual migraine. A careful neurological examination should be performed, looking for possible subtle neurological deficits, although the neurological examination will often be negative in the early stages of VAD.
Second, a triad of symptoms raised concern that the patient might be experiencing a VAD in progress. The symptom triad included: (1) spontaneous onset of severe upper cervical pain; (2) severe headache that was distinctly different from the patient’s usual migraine headaches; and (3) brainstem-related neurological symptoms (in the form of transient visual disturbance). Notably, careful neurological examination was negative. Nonetheless, the history was of sufficient concern to prompt immediate investigation.
When VAD is suspected but no frank signs of stroke are present, immediate vascular imaging is indicated. While the optimal imaging evaluation of VAD remains controversial, MRA or CTA are the diagnostic studies of choice given their excellent anatomic delineation and ability to evaluate for complications (including infarction and changes in brain perfusion). Some advocate the use of Doppler ultrasound; however, it has limited utility given the course of the vertebral artery in the neck and limited evaluation of the vertebral arteries cephalad to the origin. Additionally, ultrasound imaging is unlikely to allow visualisation of the dissection itself and thus can be negative in the absence of significant arterial occlusion.
Third, this case is interesting in light of the controversy about cervical manipulation as a potential �cause� of VAD. While case reports have presented patients who have experienced stroke related to VAD after cervical manipulation, and case�control studies have found a statistical association between visits to chiropractors and stroke related to VAD, further investigation has indicated that the association is not causal. Cassidy et al found that a patient who experiences stroke related to VAD is just as likely to have visited a primary care practitioner as to have visited a chiropractor prior to having the stroke. The authors suggested that the most likely explanation for the statistical association between visits to chiropractors and subsequent VAD is that a patient who experiences the initial symptoms of VAD (neck pain with or without headache) seeks medical attention for these symptoms (from a chiropractor, primary care practitioner, or another type of practitioner), then subsequently experiences the stroke, independent of any action taken by the practitioner.
It is important to note that, while there have been reported cases of carotid artery dissection after cervical manipulation, case�control studies have not found this association. The initial symptoms of carotid dissection (neurological symptoms, with neck and head pain less common than VAD), aortic dissection (sudden onset of severe, �tearing� pain) and coronary artery dissection (acute severe chest pain, ventricular fibrillation) are likely to cause the individual to immediately seek ED care, rather than seek chiropractic care. However, VAD has seemingly benign initial symptoms�neck pain and headache�which are symptoms that commonly cause patients to seek out chiropractic care. This may explain why only VAD is associated with visits to chiropractors, while these other types of dissections are not; patients with these other conditions, which have much more alarming symptoms, simply do not present to chiropractors.
This case is a good example of a patient with VAD in progress presenting to a chiropractor for the purpose of seeking relief from neck pain. Fortunately, the chiropractor was astute enough to ascertain that the patient’s symptoms were not suggestive of a �mechanical� cervical spine disorder, and appropriate diagnostic investigation was performed. However, if manipulation had been performed, the VAD that was already in progress from natural history may have been blamed on manipulation, after being detected on MRA imaging. Fortunately, in this case, the chiropractor was able to assist with early detection and treatment, and subsequently a stroke was likely averted.
Learning Points
A case is presented in which a patient saw a chiropractor, while seeking treatment for neck pain, and the history raised concern for possible vertebral artery dissection (VAD).
Rather than providing manipulative treatment, the chiropractor referred the patient for advanced imaging, which confirmed the diagnosis of VAD.
The case illustrates the importance of paying attention to subtle historical factors in patients with VAD.
It also serves as an example of a patient with a VAD in progress seeking the services of a chiropractor for the initial symptoms of the disorder.
In this case, early detection of the dissection occurred and the patient had a full recovery without any subsequent stroke.
Acknowledgments
The authors would like to acknowledge the assistance of Pierre Cote, DC, PhD, for his assistance with reviewing this manuscript.
Footnotes
Contributors: All the authors acknowledge that they have contributed the following to the submission of this manuscript: conception and design, drafting of the manuscript, critical revisions of the manuscript, literature review and references, and proof reading of the final manuscript.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Cited by Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
2.�Boyle E, Cote P, Grier AR et al.�Examining vertebrobasilar artery stroke in two Canadian provinces.�Spine�2008;33(4 Suppl):S170�5.�doi:10.1097/BRS.0b013e31816454e0�[PubMed]
3.�Lee VH, Brown RD Jr, Mandrekar JN et al.�Incidence and outcome of cervical artery dissection: a population-based study.�Neurology�2006;67:1809�12.�doi:10.1212/01.wnl.0000244486.30455.71[PubMed]
4.�Schievink WI.�Spontaneous dissection of the cartoid and vertebral arteries.�N Engl J Med�2001;344:898�906.�doi:10.1056/NEJM200103223441206�[PubMed]
5.�Volker W, Dittrich R, Grewe S et al.�The outer arterial wall layers are primarily affected in spontaneous cervical artery dissection.�Neurology�2011;76:1463�71.�doi:10.1212/WNL.0b013e318217e71c�[PubMed]
6.�Gottesman RF, Sharma P, Robinson KA et al.�Clinical characteristics of symptomatic vertebral artery dissection: a systematic review.�Neurologist�2012;18:245�54.�doi:10.1097/NRL.0b013e31826754e1[PMC free article]�[PubMed]
7.�Cassidy JD, Boyle E, Cote P et al.�Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study.�Spine�2008;33(4�Suppl):S176�83.�doi:10.1097/BRS.0b013e3181644600�[PubMed]
8.�Rothwell DM, Bondy SJ, Williams JI.�Chiropractic manipulation and stroke: a population-based case-control study.�Stroke�2001;32:1054�60.�doi:10.1161/01.STR.32.5.1054�[PubMed]
9.�Smith WS, Johnston SC, Skalabrin EJ et al.�Spinal manipulative therapy is an independent risk factor for vertebral artery dissection.�Neurology�2003;60:1424�8.�doi:10.1212/01.WNL.0000063305.61050.E6[PubMed]
10.�Volker W, Besselmann M, Dittrich R et al.�Generalized arteriopathy in patients with cervical artery dissection.�Neurology�2005;64:1508�13.�doi:10.1212/01.WNL.0000159739.24607.98�[PubMed]
11.�Evangelista A, Mukherjee D, Mehta RH et al.�Acute intramural hematoma of the aorta: a mystery in evolution.�Circulation�2005;111:1063�70.�doi:10.1161/01.CIR.0000156444.26393.80�[PubMed]
12.�Tweet MS, Hayes SN, Pitta SR et al.�Clinical features, management, and prognosis of spontaneous coronary artery dissection.�Circulation�2012;126:579�88.�doi:10.1161/CIRCULATIONAHA.112.105718[PubMed]
13.�Choi S, Boyle E, Cote P et al.�A population-based case-series of Ontario patients who develop a vertebrobasilar artery stroke after seeing a chiropractor.�J Manipulative Physiol Ther�2011;34:15�22.�doi:10.1016/j.jmpt.2010.11.001�[PubMed]
14.�Naggara O, Louillet F, Touze E et al.�Added value of high-resolution MR imaging in the diagnosis of vertebral artery dissection.�AJNR Am J Neuroradiol�2010;31:1707�12.�doi:10.3174/ajnr.A2165�[PubMed]
16.�Nebelsieck J, Sengelhoff C, Nassenstein I et al.�Sensitivity of neurovascular ultrasound for the detection of spontaneous cervical artery dissection.�J Clin Neurosci�2009;16:79�82.�doi:10.1016/j.jocn.2008.04.005�[PubMed]
17.�Bendick PJ, Jackson VP.�Evaluation of the vertebral arteries with duplex sonography.�J Vasc Surg1986;3:523�30.�doi:10.1016/0741-5214(86)90120-5�[PubMed]
18.�Murphy DR.�Current understanding of the relationship between cervical manipulation and stroke: what does it mean for the chiropractic profession?�Chiropr Osteopat�2010;18:22�doi:10.1186/1746-1340-18-22[PMC free article]�[PubMed]
19.�Engelter ST, Grond-Ginsbach C, Metso TM et al.�Cervical artery dissection: trauma and other potential mechanical trigger events.�Neurology�2013;80:1950�7.�doi:10.1212/WNL.0b013e318293e2eb�[PubMed]
20.�Peters M, Bohl J, Th�mke F et al.�Dissection of the internal carotid artery after chiropractic manipulation of the neck.�Neurology�1995;45:2284�6.�doi:10.1212/WNL.45.12.2284�[PubMed]
21.�Nadgir RN, Loevner LA, Ahmed T et al.�Simultaneous bilateral internal carotid and vertebral artery dissection following chiropractic manipulation: case report and review of the literature.�Neuroradiology2003;45:311�14.�doi:10.1007/s00234-003-0944-x�[PubMed]
22.�Dittrich R, Rohsbach D, Heidbreder A et al.�Mild mechanical traumas are possible risk factors for cervical artery dissection.�Cerebrovasc Dis�2007;23:275�81.�doi:10.1159/000098327�[PubMed]
23.�Chung CL, Cote P, Stern P et al.�The association between cervical spine manipulation and carotid artery dissection: a systematic review of the literature.�J Manipulative Physiol Ther�2014; doi:10.1016/j.jmpt.2013.09.005�doi:10.1016/j.jmpt.2013.09.005�[PubMed]
24.�Thomas LC, Rivett DA, Attia JR et al.�Risk factors and clinical features of craniocervical arterial dissection.�Man Ther�2011;16:351�6.�doi:10.1016/j.math.2010.12.008�[PubMed]
25.�Klineberg E, Mazanec D, Orr D et al.�Masquerade: medical causes of back pain.�Cleve Clin J Med2007;74:905�13.�doi:10.3949/ccjm.74.12.905�[PubMed]
Holistic: Migraine headaches are typically debilitating, and require a comprehensive approach for successful treatment. It is helpful to consider migraine headache as a symptom of an underlying imbalance, rather than simply a diagnosis. A holistic approach is a satisfying way to think about and treat migraine headache. Physicians trained in this approach will consider a broad array of features that may contribute to the experience of migraine headache, including disturbances within the following key areas:
Nutrition
Digestion
Detoxification
Energy production
Endocrine function
Immune system function/inflammation
Structural function
Mind-body health
Migraine headache is an excellent example of biologic uniqueness; the underlying factors participating in each individual�s outcome may differ quite a bit from person to person. The journey of identifying and addressing these factors often results in an impressive improvement in frequency and intensity of the expression of migraine. Committed individuals will find the added benefit of better general health along the way.
Contents
Nutritional Considerations: Holisitic
Food Allergy/Intolerance
Numerous well-designed studies have demonstrated that detection and removal of foods not tolerated will greatly reduce or eliminate migraine manifestations. True allergy may not be associated with migraine in most individuals, but food intolerance is more common. Migraine frequency and intensity have been demonstrated to respond well to elimination diets, in which commonly offending foods are removed for several weeks. Elimination diets are easy to perform (although they do require a high degree of commitment and education), and can help in identifying foods that are mismatched to an individual. The majority of patients who undergo an elimination diet learn that their diets were contributing to chronic symptoms, and they typically feel much better during the elimination phase. Common foods that act as migraine triggers include: chocolate, cow�s milk, wheat/gluten grains, eggs, nuts, and corn. In children specifically, common migraine triggers include cheese, chocolate, citrus fruits, hot dogs, monosodium glutamate, aspartame, fatty foods, ice cream, caffeine withdrawal, and alcoholic drinks, especially red wine and beer.
There are several methods which may be used to detect food allergies. Laboratory testing can be convenient, but is not always a reliable means of detecting food intolerance. (See Summary of Recommendations for information on how to implement the elimination diet).
Foods such as chocolate, cheese, beer, and red wine are believed to cause migraine through the effect of �vasoactive amines� such as tyramine and beta-phenylethylamine. These foods also contain histamine. Individuals who are sensitive to dietary histamine seem to have lower levels of diamine oxidase, the vitamin B6-dependent enzyme that metabolizes histamine in the small bowel. The use of vitamin B6 improves histamine tolerance in some individuals, presumably by enhancing the activity of this enzyme.
Other diet-related triggers associated with migraine headache include: glucose/insulin imbalances, excessive salt intake, and lactose intolerance. Aspartame, commonly used as a sweetener, may also trigger migraines. Each of these factors may be readily avoided by adopting more conscious eating habits, and by carefully reading labels.
Magnesium
An estimated 75% of people consuming the standard American diet (SAD) are not getting adequate magnesium, and it is felt to represent one of the most common micronutrient deficiencies, manifested by a diverse range of problems. Though many elements can contribute to magnesium depletion, stress is among them, and both acute and chronic stress are associated with increased episodes of migraine. Daily doses of magnesium should be first line considerations for migraine sufferers (caution if kidney function is impaired), and intravenous magnesium can be very helpful in an emergency room setting, but probably only works to terminate an acute migraine if the individual is truly magnesium deficient.
Essential Fatty Acids
It is important to remember that the brain is largely composed of fat. Although essential fatty acids have not received much research attention relative to migraine, there may be a significant role of fatty acids and their metabolites in the pathogenesis of migraine headache. Two small placebo-controlled studies demonstrated that omega-3 fatty acids significantly outperformed placebo in reducing headache frequency and intensity. High quality fish oil should always be used. A good frame of reference is that each capsule should contain at least 300 mg of EPA and 200 mg of DHA. A reasonable starting dose would be two to four capsules twice daily with meals.
Digestive Function: Holistic
Holistic practitioners are generally sensitive to the centrality of the gastrointestinal tract in producing overall health. Though we utilize a reductionistic approach to understanding human anatomy and physiology, we might consider that no system functions as an independent entity (GI, endocrine, cardiovascular, immune, etc.), and that a complex symphony of interrelated functions cuts across organ systems. For example, much of the immune system is found in the Peyer�s patches of the GI tract; in this light, we can see how food, chemicals, and unhealthy microbes might produce immune system activation from gastrointestinal exposure. We also recognize the importance of a balanced ecosystem of intestinal microbes; intestinal dysbiosis, or disordering of the gastrointestinal ecology, may readily produce symptoms, both within and distant from the GI tract. Some colonic bacteria act upon dietary tyrosine to produce tyramine, a recognized migraine trigger for some individuals. H. pylori infection is a probable independent environmental risk factor for migraine without aura, especially in patients not genetically or�hormonally susceptible. A high percentage of migraine patients experienced relief from migraines when H. Pylori infection was eradicated.
Detoxification: Holistic
Patients with migraine headache sometimes report that strong chemical odors such as tobacco smoke, gasoline, and perfumes may act as triggers. It is not uncommon for migraineurs to report that they are triggered by walking down the laundry soap aisle in the grocery store. Support for phase 1 and especially phase 2 detoxification may be beneficial for these individuals, as toxic overload or impaired enzymes of detoxification could theoretically be a significant mediator of headaches. Susceptibility to toxicity may be potentiated by a combination of excessive toxic exposures, genetic polymorphisms leading to inadequate detoxification enzyme production, or depletion of nutrient cofactors that drive phase two detoxification conjugation reactions Support for detoxification function is particularly important in modern life, given our exposure to unprecedented high levels of toxic chemicals. Some nutrients that supply support for detoxification function include: n-acetyl cysteine (NAC), alpha lipoic acid, silymarin (milk thistle), and many others.
Energy Production: Holistic
Riboflavin (Vitamin B2)
Energy production within the parts of the cell called mitochondria can be impaired in some migraine sufferers. Riboflavin is a key nutrient that is involved in energy production at this level. Riboflavin at 400 mg/day is an excellent therapeutic choice for migraine headache because it is well tolerated, inexpensive, and provides a protective effect from oxidative toxicity. Its use in children has been investigated, leading to similar conclusions,suggesting that, for pediatric and adolescent migraine prophylaxis, 200 mg per day was an adequate dose, but four months were necessary for optimal results.
Coenzyme Q10
CoenzymeQ10 (CoQ10) is also a critical component of energy function, and is an important antioxidant. Evidence supports the administration of CoQ10 in reducing the frequency of migraines by 61%. After three months of receiving 150 mg of CoQ10 at breakfast, the average number of headache days decreased from seven to three per month. Another study, using 100 mg of water soluble CoQ10 3x/day, revealed similar results. CoQ10 deficiency appears to be common in the pediatric and adolescent population, and can be an important therapeutic consideration in these age groups. Like riboflavin, CoQ10 is well tolerated (though expensive), with little risk of toxicity. It must be used with extreme caution in patients who also take warfarin, as CoQ10 may counteract the anticoagulation effects of warfarin. It is also noteworthy that many medications can interfere with CoQ10 activity, including statins, beta-blockers, and certain antidepressants and antipsychotics.
Endocrine (Hormone) Function
Female Hormones
It does not appear coincidental that migraine onset correlates with the onset of menstruation and that episodes are linked to menstruation in roughly 60% of female migraineurs. Although there is no universal agreement over the precise relationship between female hormones and migraine headache, it is apparent that the simultaneous fall of estrogen and progesterone levels before the period correlates with menstrual migraine. Estrogen gel used on the skin can reduce headaches when used premenstrually. Some researchers have found that continuous use of estrogen may be necessary to control menstrual migraines, which tend to be more severe, frequent, longer lasting, and debilitating than general migraines. Although published studies are lacking, many practitioners have used transdermal or other bioidentical forms of progesterone premenstrually with success. Of course, the risks of using hormones must be weighed against the benefits. Interestingly, administration of magnesium (360 mg/day) during second half of the menstrual cycle in 20 women with menstrually related migraines resulted in a significant decrease of headache days.
Melatonin
Melatonin, the next downstream metabolite of serotonin, is important in the pathogenesis of migraines. Decreased levels of plasma and urinary melatonin have been observed in migraine patients, and melatonin deficiency appears to increase risk for migraine. Melatonin has been used with some success, presumably via a restorative effect on circadian rhythms. A small study in children demonstrated significant improvement in their migraine or tension headache frequency with a 3 mg nightly dose of melatonin Melatonin appears to modulate inflammation, oxidation, and neurovascular regulation in the brain, and in one study, a dose of 3 mg/day was shown to be effective in reducing migraine headache frequency by at least 50% in 25 of 32 individuals. Ironically, some patients anecdotally report an increase of headaches (generally not migraine) when administered melatonin. The brains of migraineurs do not seem adaptable to extremes; a regular schedule of sleep and meals and avoidance of excessive stimulation are advisable to reduce excessive neural activation.
Immune Function/Inflammation: Holistic
Medications that produce an anti-inflammatory effect, such as aspirin and nonsteroidal agents, frequently produce an improvement in migraine symptoms during an acute attack. The herbs described below also play a role in reducing inflammation. Inflammation and oxidative stress can be identified in many conditions and disease states. It is important to acknowledge that the standard �modern� lifestyle is pro-inflammatory; our bodies are constantly reacting to one trigger after another (foods mismatched to our physiology, toxic burden, emotional stressors, excessive light and other stimulation) that activate our inflammatory cytokines (messengers of alarm). Providing broad-based support through lifestyle change and targeted nutrients may improve outcomes substantially, and this may be achieved foundationally by simplifying our�ingestions/exposures and supporting metabolic terrain. Herbal therapies are included in this section because of their relevant effects upon inflammation.
Feverfew (Tanacetum parthenium)
The precise mechanism of action of feverfew as a migraine preventive is unknown Though at least three studies found no benefit with feverfew, several controlled studies have revealed favorable results in improving headache frequency, severity, and vomiting when feverfew was compared to placebo. There are several caveats that should accompany the use of this herb:
Because of its anti-platelet effects, feverfew must be used with caution in patients on blood thinning products; avoid in patients on warfarin/Coumadin.
Feverfew does not have a role in managing acute migraine headache.
When withdrawing feverfew, do so with a slow taper, since rebound headache may occur.
Feverfew is not known to be safe during pregnancy and lactation.
Proceed with caution if an individual has an allergy to other members of the Asteraceae family (yarrow, chamomile, ragweed).
Most commonly reported adverse effects are oral ulceration (particularly for those chewing the leaves raw), and GI symptoms, reversible with discontinuation.
Feverfew is otherwise well tolerated. The typical dosage range is 25-100 mg 2x/day of encapsulated dried leaves with meals.
Butterbur (Petasites hybridus)
Butterbur is another effective herbal therapy for migraine headache. Butterbur is well tolerated, with no known interactions. Some individuals have reported diarrhea when using butterbur. In one study, its efficacy was demonstrated in children and adolescents between the ages of 6 and 17 years. Its safety is unknown during pregnancy and lactation. The plant�s pyrrolizidine alkaloids can toxic to the liver and carcinogenic, so only extracts that have specifically removed these compounds should be utilized. Many of the studies on Butterbur utilized the product Petadolex� because it is a standardized extract that has removed these alkaloids of concern. The usual dosage is 50 mg, standardized to 7.5 mg petasin and isopetasin, 2-3x/day with meals (although recent studies show that higher doses appear to be more effective1,2 ). Interestingly, butterbur�s diverse qualities make it useful for other conditions, including seasonal allergic rhinitis, and possibly painful menstrual cramps.
Ginger (Zingiber officinalis)
Ginger root is a commonly used botanical, known to suppress inflammation and platelet aggregation. Little clinical investigation has been performed relative to ginger use in migraine headache, but anecdotal reports and speculation based on its known properties make it a safe and appealing choice for migraine treatment. Some practitioners advise patients with acute migraine to sip a cup of warm ginger tea. Though evidence for this practice is lacking, it is a low-risk, pleasant, and relaxing intervention, and ginger is known to have anti-nausea effects. The most anti-inflammatory support is found in fresh preparations of ginger and in the oil.
Structural Considerations: Holistic
Practitioners of manual medicine seem to achieve success in reducing headache through various techniques such as spinal manipulation, massage, myofascial release, and craniosacral therapy Manual medicine practitioners frequently identify loss of mobility in the cervical and thoracic spine in migraineurs. While many forms of physical medicine seem helpful in shortening the duration and intensity of an episode of migraine, literature support is sparse with regard to manipulation as a modality to prevent recurrent migraine episodes. However, a randomized controlled trial of chiropractic spinal manipulation performed in 2000 revealed a significant improvement in migraine frequency, duration, disability, and medication use in 83 treatment group participants. Tension headache may also respond favorably to these techniques because of the structural component involved in muscular tension. The incidence of migraine in patients with TMJ dysfunction is similar to that in the general population, whereas the incidence of tension headache in patients with TMJ dysfunction is much higher than in the general population. Craniosacral therapy is a very gentle manipulative technique that may also be safely attempted with migraine.
Mind-Body Health: Holistic
There are few things more insulting than to be told by a medical professional to �Just reduce your stress.� Though the total load of stress experienced by an individual can be reduced through paring down unnecessary obligations, many everyday life stressors are unavoidable and cannot be simply eradicated. Thus, the answer to reducing stress for unavoidable contributors lies in two important areas: enhancing physical and mental resilience to stress, and modifying the emotional response to stress.
A multitude of programs to reduce the impact of stress on our physical and emotional well-being are rapidly becoming mainstream. For example, mindfulness meditation programs by Jon KabatZinn, PhD and many others are being offered to communities by hospitals around the country. This technique is simple to perform and has demonstrated positive outcomes in heart disease, chronic pain, psoriasis, hypertension, anxiety, and headaches. Breathwork and guided imagery techniques are likewise effective in producing a relaxation response and helping patients to feel more empowered about their health.
Biofeedback and relaxation training have been used with mixed success for migraine headache. Thermal biofeedback uses the temperature of the hands to help the individual learn that inducing the relaxation response will raise hand temperature and facilitate other positive physiologic changes in the body. Learning how to take more active control over the body may reduce headache frequency and severity. The effectiveness of biofeedback and relaxation training in reducing the frequency and severity of migraine headaches has been the subject of dozens of clinical studies, revealing that these techniques can be as effective as medication for headache prevention, without the adverse effects. Other relevant modalities to consider in this light include cognitive behavioral therapy, neurolinguistic programming, hypnosis, transcutaneous electrical nerve stimulation, and laser therapy.
Exercise should not be overlooked as a modality helpful in migraine headache. Thirty-six patients with migraine who exercised 3x/week for 30 minutes over six weeks experienced significant improvement in headache outcomes. Pre-exercise beta-endorphin levels in these individuals were inversely proportional to the degree of improvement in their post-exercise headache parameters. All patients should understand the critical importance of exercise on general health.
Acupuncture: Holistic
A discussion about a holistic integrative approach to migraine headache would be incomplete without acupuncture, which is an effective treatment modality for acute and recurrent migraine. A qualified/licensed practitioner of Traditional Chinese Medicine or a physician trained in medical acupuncture should be consulted.
Holistic: Summary Of Recommendations
Since initiators of migraine headache may be cumulative, identify and avoid them when possible. Consider the basic areas of dysfunction bulleted on the first page of this syllabus.
The incidence of food intolerance is high in patients with migraine headache; consider a comprehensive elimination diet for four to six weeks, during which time the following foods are eliminated: dairy products, gluten-containing grains, eggs, peanuts, coffee/black tea, soft drinks, alcohol, chocolate, corn, soy, citrus fruits, shellfish, and all processed foods. Careful reintroduction of one food at a time, no more often than every 48 hours, may help identify a food culprit. Meticulous recording of foods reintroduced is necessary. Most patients feel improved vitality during the elimination phase. Foods that clearly produce migraine (or other) symptoms should be avoided or used on a rotation schedule of not more than once every four days. If multiple foods introduced back into the diet seem to produce migraine headache, consider the possibility of altered intestinal permeability (leaky gut syndrome).
Consider the following supplements (Consult a qualified practitioner for advice):
Magnesium glycinate: 200-800 mg/day in divided doses (decrease to tolerance if diarrhea occurs)
Vitamin B6 (pyridoxine): 50-75 mg/day, balanced with B complex o 5-HTP: 100-300 mg 2x/day, with or without food, if clinically appropriate
Vitamin B2 (riboflavin): 400 mg/day, balanced with B complex
Coenzyme Q10: 150 mg/day
Consider hormonal therapies
Trial of melatonin: 0.3-3 mg at bedtime
Trial of progesterone or estradiol, carefully individualized, under medical supervision.
Botanical medicines
Feverfew: 25-100 mg 2x/day with meals
Butterbur: 50 mg 2-3x/day with meals
Ginger root
Fresh ginger, approximately 10 gm/day (6 mm slice)
Dried ginger, 500 mg 4x/day
Extract standardized to contain 20% gingerol and shogaol; 100-200 mg 3x/day for prevention, and 200 mg every 2 hours (up to 6 x/day) for acute migraine
Manual medicine may be helpful for some individuals.
Acupuncture
Mind-body support
Thermal biofeedback
Read The Relaxation Response by Herbert Benson, MD
Mindfulness meditation programs
Centering prayer
Breathwork
Guided imagery
Yoga, tai chi, qi gong, etc.
Many other modalities to consider!
Conclusion: Holistic Medicine
Patients will often request a more natural and self directed approach to health care. The recommendations above are typically very safe to implement, and are often welcomed by migraine sufferers. A practitioner with an integrative holistic focus will investigate an extensive array of predisposing factors to determine the underlying features most likely involved in a given individual�s condition. In this way, we treat the individual, rather than his or her diagnosis, and we will generate a favorable impact upon his/her overall health in the process.
Chiropractic Care & Headaches
�American Board of Integrative Holistic Medicine. All rights reserved.
The diagnosis of a variety of diseases has been effectively determined through clinical and experimental data. Research studies provide valuable information on the pathogenesis of many conditions and are often the primary source of information regarding new diseases or conditions. Case reports and case series are first level research studies, offering the most initial insights on a particular health issue through the personal experience of one or more people with a disease or condition. The following article describes the purpose of case reports and case series, and how they provide clinical and experimental data.
Contents
Learning Objectives
1. Case reports and case series describe the experience of one or more people with a disease.
2. Case reports and case series are often the first data alerting to a new disease or condition.
3. Case reports and case series have specific limitations:
a. Lack of a denominator to calculate rates of disease
b. Lack of a comparison group
c. Selecting study populations
d. Sampling variation
Case Reports and Case Series
Case reports and case series represent the most basic type of study design, in which researchers describe the experience of a single person (case report) or a group of people (case series). Typically, case reports and case series describe individuals who develop a particular new disease or condition. Case reports and case series can provide compelling reading because they present a detailed account of the clinical experience of individual study subjects. In contrast, studies that evaluate large numbers of individuals typically summarize the data using statistical measures, such as means and proportions.
Example 3.1. A case series describes 15 young women who develop breast cancer; 9 of these women report at least once weekly ingestion of foods packaged with the estrogenic chemical bisphenol A (BPA). Urine testing confirms the presence of BPA among all nine case women.
It is tempting to surmise from these data that BPA might be causally related to breast cancer. However, case reports/case series have important limitations that preclude inference of a causal relationship.
First, case reports/case series lack denominator data that are necessary to calculate the rate of disease. The denominator refers to the population from which the diseased subjects arose. For example, to calculate the incidence proportion or incidence rate of breast cancer among women exposed to BPA, the total number of women who were exposed to BPA or the total number of person-years at risk is needed.
Disease rates are needed for comparison with historically reported disease rates, or with rates from a selected comparison group. Unfortunately, obtaining the necessary denominator data may not be easy. In this example, additional data sources are needed to determine the total number of BPA-exposed women from whom the breast cancer cases arose. The case series data alone cannot be used to calculate the rate of breast cancer because they do not include the total number of women who were exposed to BPA.
A second problem with case report/case series report data is the lack of a comparison group. The 60% prevalence of BPA exposure among women with breast cancer seems unusually high, but what is prevalence of BPA exposure among women without breast cancer? This comparison is critical for addressing the hypothesis that BPA might be a cause of breast cancer.
A third limitation of case reports/case series is that these studies often describe highly select individuals who may not represent the general population. For example, it is possible that the 15 breast cancer cases originated from a single hospital in a community with high levels of air pollution or other potential carcinogens. Under these conditions, a fair estimate of breast cancer incidence among non-BPA exposed women from the same community would be required to make an inference that BPA causes breast cancer.
A fourth limitation of case reports/case series is sampling variation. This concept will be explored in detail later in this book. The basic idea is that there is tremendous natural variation in disease development in humans. The fact that 9 of 15 women with breast cancer reported BPA exposure is interesting; however, this number may be very different in the next case series of 15 women with breast cancer simply due to chance. A precise estimate of the rate of a disease, independent from chance, can be obtained only by increasing the number of diseased subjects.
Recall the list of factors that are used to judge whether a factor may be a cause of disease:
1. Randomized evidence
2. Strength of association
3. Temporal relationship between exposure and outcome
4. Dose-response association
5. Biological plausibility
In general, case reports/case series rely almost exclusively on biological plausibility to make their case for causation. For the BPA and breast cancer case series, there is no randomized evidence, no measure of the strength of association between BPA and breast cancer, no reported dose�response association, and no evidence that BPA exposure preceded the development of breast cancer. The inference for causation derives completely from previous biological knowledge regarding the estrogenic effects of BPA.
Despite limitations of case series data, they may be highly suggestive of an important new association, disease process, or unintended side effect of a medication or treatment.
Example 3.2. In 2007, a case series described three cases of male prepubertal gynecomastia. The report included detailed information on each subjects� age, body size, serum levels of endogenous steroids, and known exposures to exogenous hormones. It was discovered that all three otherwise healthy boys had been exposed to some product containing lavender oil (lotion, shampoo, soap), and that in each case, the gynecomastia resolved upon discontinuation of the product. Subsequent in vitro studies demonstrated endocrine-disrupting activity of lavender oil. This novel case series data may lead to further investigations to determine whether lavender oil, a common ingredient in commercially available products, may be a cause of gynecomastia.
Example 3.3. A vaccine designed to prevent rotavirus infection was found to cause weakening of the intestinal muscle layers in animals. Following release of the vaccine, a number of cases of intussusception (when one portion of the bowel slides into the next) were reported in children who received the vaccine, with some fatal cases. The strong biological plausibility underlying this initial association, and knowledge that intussusception is otherwise rare in infants, was highly suggestive of a causal relationship and the vaccine was removed from the market.
Information referenced from B. Kestenbaum, Epidemiology and Biostatistics: An Introduction to Clinical Research, DOI 10.1007/978-0-387-88433-2_3, � Springer Science+Business Media, LLC 2009. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Referenced by Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Effectiveness: We all know and understand the importance of maintaining a healthy weight. Some individuals do quite nicely at managing their pounds with seemingly little effort, while other struggle constantly.
A recent study by the Center for Disease Control and Prevention (CDC) reports that 78 million American adults suffer from obesity. A person who has sustained an injury or suffers from an illness that affects their back, hips, knees or ankles are especially susceptible to weight gain, because they must deal with limited mobility and the stress of daily pain.
Striving to stay in the ideal weight range for your body type and height provides a variety of health benefits such as adding less pressure on your back and joints, and increasing your range of motion. Patients who receive chiropractic care often enjoy the effectiveness of increased healing by pursuing weight loss.
Successfully fight the battle of the bulge with these four handy weight loss tips to:
Contents
Amplify The Effectiveness Of Chiropractic Care
First, Start Small
Replace a couple of negative behaviors with positive ones, and commit to making them stick. Great examples of these are substituting water for soft drinks, eating a high-protein breakfast, or changing out your nightly bowl of ice cream with yogurt.
Simply removing 100 calories a day adds up to a 10 pound weight loss over a year’s time. Small modifications offer the dual benefits of being easier to implement while still showing results.
Next, Keep A Journal
Write down every bite you eat along with the portion size. Listing your food intake provides accountability, which may keep you from noshing on that third slice of pizza or super-sizing those fries.
It also arms you with important intel that will be helpful throughout your weight loss journey. If you hit a plateau, read back through the journal to see what you may have changed over time that caused the scales to stall.
And speaking of scales….
Don’t Live And Cry By The Scales
Often, dieters weigh every day and are elated or depressed based on the number on the scales. That’s a roller coaster way to live, and those emotions can cause calorie laden binges!
Plus, daily weighing is not accurate, as fluctuations in water weight are common. Weigh once a week at the most, at roughly the same time each day. A weekly routine gives you a good idea of your success without the stressful up and down of daily weighing.
Decrease Your Sedentary Ways
Even if you are dealing with an injury or medical condition that limits the ability to exercise, you can still probably be less sedentary than you are now. Again, simplicity is the key.
Walk into the bank instead of using the drive through window, stand up to fold clothes instead of sitting down, and take periodic breaks at your desk to stand for a bit.
Ask your chiropractor about any limitations you need to follow, and request stretching exercises as your personal situation permits. Moving more on a daily basis will aid in shedding those extra pounds and keeping them off long-term.
It’s important for individuals to maintain a normal weight range in order to enjoy a healthy life. Chiropractic patients benefit even more from shedding those extra pounds.
By committing to a healthier lifestyle with fewer pounds to carry around, individuals with back and joint injuries will see greater positive impact from their chiropractic visits. Over time, the combination of a leaner body and chiropractic care will bring greater mobility, less pain, and a decreased chance for re-injury to the patient.
Shea Vaughn Talks “Targeting Obesity”
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Consider the following, sciatica is a medical term used to describe a collective group of symptoms resulting from the irritation or compression of the sciatic nerve, generally due to an injury or aggravated condition. Sciatica is commonly characterized by radiating pain along the sciatic nerve, which runs down one or both legs from the lower back. The following case vignette discusses Mr. Winston’s medical condition, a 50-year-old bus driver who reported experiencing chronic, lower back and leg pain associated with sciatica during a 4-week time period. Ramya Ramaswami, M.B., B.S., M.P.H., Zoher Ghogawala, M.D., and James N. Weinstein, D.O., provide a comprehensive analysis of the various treatment options available to treat sciatica, including undergoing lumbar disk surgery and receiving nonsurgical therapy.
On a personal note, as a practicing doctor of chiropractic, choosing the correct treatment care for any type of injury or condition can be a personal and difficult decision. If the circumstances are favorable, the patient may determine what is the best form of treatment for their type of medical issue. While nonsurgical therapies, such as chiropractic care, can often be utilized to improve symptoms of sciatica, more severe cases of sciatica may require surgical interventions to treat the source of the issue. In most cases, nonsurgical therapies should be considered first, before turning to surgical therapies for sciatica.
Contents
Case Vignette
A Man with Sciatica Who is Considering Lumbar Disk Surgery
Ramya Ramaswami, M.B., B.S., M.P.H.
Mr. Winston, a 50-year-old bus driver, presented to your office with a 4-week history of pain in his left leg and lower back. He described a combination of severe sharp and dull pain that originated in his left buttock and radiated to the dorsolateral aspect of his left thigh, as well as vague aching over the lower lumbar spine. On examination, passive raising of his left leg off the table to 45 degrees caused severe pain that simulated his main symptom, and the pain was so severe that you could not lift his leg further. There was no leg or foot weakness. His body-mass index (the weight in kilograms divided by the square of the height in meters) was 35, and he had mild chronic obstructive pulmonary disease as a result of smoking one pack of cigarettes every day for 22 years. Mr. Winston had taken a leave of absence from his work because of his symptoms. You prescribed 150 mg of pregabalin per day, which was gradually increased to 600 mg daily because the symptoms had not abated.
Now, 10 weeks after the initial onset of his symptoms, he returns for an evaluation. The medication has provided minimal alleviation of his sciatic pain. He has to return to work and is concerned about his ability to complete his duties at his job. He undergoes magnetic resonance imaging, which shows a herniated disk on the left side at the L4�L5 root. You discuss options for the next steps in managing his sciatica. He is uncertain about invasive procedures such as lumbar disk surgery but feels limited by his symptoms of pain.
Treatment Options
Which of the following would you recommend for Mr. Winston?
Undergo lumbar disk surgery.
Receive nonsurgical therapy.
To aid in your decision making, each of these approaches is defended in a short essay by an expert in the field. Given your knowledge of the patient and the points made by the experts, which option would you choose?
Option 1: Undergo Lumbar Disk Surgery Option 2: Receive Nonsurgical Therapy
1. Undergo Lumbar Disk Surgery
Zoher Ghogawala, M.D.
Mr. Winston�s case represents a common scenario in the management of symptomatic lumbar disk herniation. In this particular case, the patient�s symptoms and the physical examination are consistent with nerve-root compression and inflammation directly from an L4�L5 herniated disk on his left side. The patient does not have weakness but has ongoing pain and has been unable to work for the past 10 weeks despite receiving pregabalin. Two questions emerge: first, does lumbar disk surgery (microdiskectomy) provide outcomes that are superior to those with continued nonoperative therapy in patients with more than 6 weeks of symptoms; and second, does lumbar microdiskectomy improve the likelihood of return to work in patients with these symptoms?
The highest quality data on the topic come from the Spine Patient Outcomes Research Trial (SPORT). The results of the randomized, controlled trial are difficult to interpret because adherence to the assigned treatment strategy was suboptimal. Only half the patients who were randomly assigned to the surgery group actually underwent surgery within 3 months after enrollment, and 30% of the patients assigned to nonoperative treatment chose to cross over to the surgical group. In this study, the patients who underwent surgery had greater improvements in validated patient-reported outcomes. The treatment effect of microdiskectomy was superior to that of nonoperative treatment at 3 months, 1 year, and 2 years. Moreover, in an as-treated analysis, the outcomes among patients who underwent surgery were superior to those among patients who received nonoperative therapy. Overall, the results of SPORT support the use of microdiskectomy in this case.
Results of clinical trials are based on a comparison of treatment options in study populations and may or may not apply to individual patients. SPORT did not specify what type of nonoperative therapy was to be used. Physical therapy was used in 73% of the patients, epidural injections in 50%, and medical therapies (e.g., nonsteroidal antiinflammatory drugs) in more than 50%. In the case of Mr. Winston, pregabalin has been tried, but physical therapy and epidural glucocorticoid injections have not been attempted. Despite widespread use of physical therapy for the treatment of lumbar disk herniation, the evidence supporting its effectiveness is inconclusive, according to published guidelines of the North American Spine Society. On the other hand, there is evidence that transforaminal epidural glucocorticoid injection provides short-term relief (30 days) in patients with nerve-root symptoms directly related to a herniated disk. Overall, there is evidence, from SPORT and from a randomized trial from the Netherlands published in the Journal, that early surgery between 6 and 12 weeks after the onset of symptoms provides greater alleviation of leg pain and better overall pain relief than prolonged conservative therapy.
The ability to return to work has not been formally studied in comparisons of operative with nonoperative treatments for lumbar disk herniation. Registry data from the NeuroPoint-SD study showed that more than 80% of the patients who were working before disk herniation returned to work after surgery. The ability to return to work may be dependent on the type of vocation, since patients who are manual laborers may need more time to recover to reduce the risk of reherniation.
It is well recognized that many patients who have a symptomatic lumbar disk herniation will have improvement spontaneously over several months. Surgery can alleviate symptoms more quickly by immediately removing the offending disk herniation from the affected nerve root. The risk�benefit equation will vary among individual patients. In the case of Mr. Winston, obesity and mild pulmonary disease might increase the risk of complications from surgery, although in SPORT, 95% of surgical patients did not have any operative or postoperative complication. For Mr. Winston, a patient with pain that has persisted for more than 6 weeks, microdiskectomy is a rational option that is supported by high-quality evidence.
2. Receive Nonsurgical Therapy
James N. Weinstein, D.O.
This case involves a common presentation of low back pain radiating to the buttock and posterolateral thigh that might represent either referred mechanical pain or radiculopathy. Classic radiculopathy resulting from compression of a lower lumbar nerve root (L4, L5, or S1) results in pain that radiates distal to the knee and is often accompanied by weakness or numbness in the respective myotome or dermatome. In this case, the pain is proximal to the knee and is not associated with weakness or numbness. In SPORT, surgery resulted in faster recovery and a greater degree of improvement than nonoperative treatment in patients with pain that radiated distal to the knee and was accompanied by neurologic signs or symptoms. However, since Mr. Winston would not have met the inclusion criteria for SPORT, the results of diskectomy in this case would be somewhat unpredictable. He does not have radiculopathy that radiates below the knee, and he does not have weakness or numbness; nonoperative treatment should be exhausted before any consideration of a surgical procedure that in most cases has not been shown to be effective in patients with this type of presentation. In this issue of the Journal, Mathieson and colleagues report the results of a randomized, controlled trial that showed that pregabalin did not significantly alleviate pain related to sciatica. Mr. Winston has been treated only with pregabalin; therefore, other conservative options should be explored.
Saal and Saal reported that more than 80% of patients with radiculopathy associated with a lumbar disk herniation had improvement in a matter of months with exercise-based physical therapy. In the nonoperative SPORT cohort, patients had significant improvement from baseline, and approximately 60% of those with classic radiculopathy who initially received nonoperative treatment avoided surgery. Mr. Winston has had minimal treatment and has had symptoms for only 10 weeks. He should undergo a course of exercise-based physical therapy and a trial of a nonsteroidal antiinflammatory medication and may consider a lumbar epidural glucocorticoid injection. Although there is little evidence of the effectiveness of these nonoperative options alone, the combination of these treatments and the benign natural history of the patient�s condition could result in alleviation or resolution of symptoms. If these interventions � and time � do not resolve his symptoms, surgery could be considered as a final option, but it may not have long-term effectiveness and could in and of itself cause the possibility of more harm than good. Mr. Winston has risk factors, such as obesity and a history of smoking, that have been shown to contribute to poor surgical outcomes of certain spinal procedures.
Mr. Winston has symptoms of back pain that interfere with his quality of life. He would need to understand, through shared decision making, that a nonsurgical approach is likely to be more effective than surgery over time.
Information referenced from the National Center for Biotechnology Information (NCBI) and the New England Journal of Medicine (NEJM). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Cited by Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
1. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA2006;296:2441–2450
2. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA2006;296:2451–2459
3. Kreiner DS, Hwang SW, Easa JE, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J2014;14:180–191
4. Ghahreman A, Ferch R, Bogduk N. The efficacy of transforaminal injection of steroids for the treatment of lumbar radicular pain. Pain Med2010;11:1149–1168
6. Ghogawala Z, Shaffrey CI, Asher AL, et al. The efficacy of lumbar discectomy and single-level fusion for spondylolisthesis: results from the NeuroPoint-SD registry: clinical article. J Neurosurg Spine2013;19:555–563
8. Lurie JD, Tosteson TD, Tosteson AN, et al. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial. Spine (Phila Pa 1976)2014;39:3–16
11. Pinto RZ, Maher CG, Ferreira ML, et al. Drugs for relief of pain in patients with sciatica: systematic review and meta-analysis. BMJ2012;344:e497–e497
12. Pearson A, Lurie J, Tosteson T, et al. Who should have surgery for an intervertebral disc herniation? Comparative effectiveness evidence from the Spine Patient Outcomes Research Trial. Spine2012;37:140–149
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
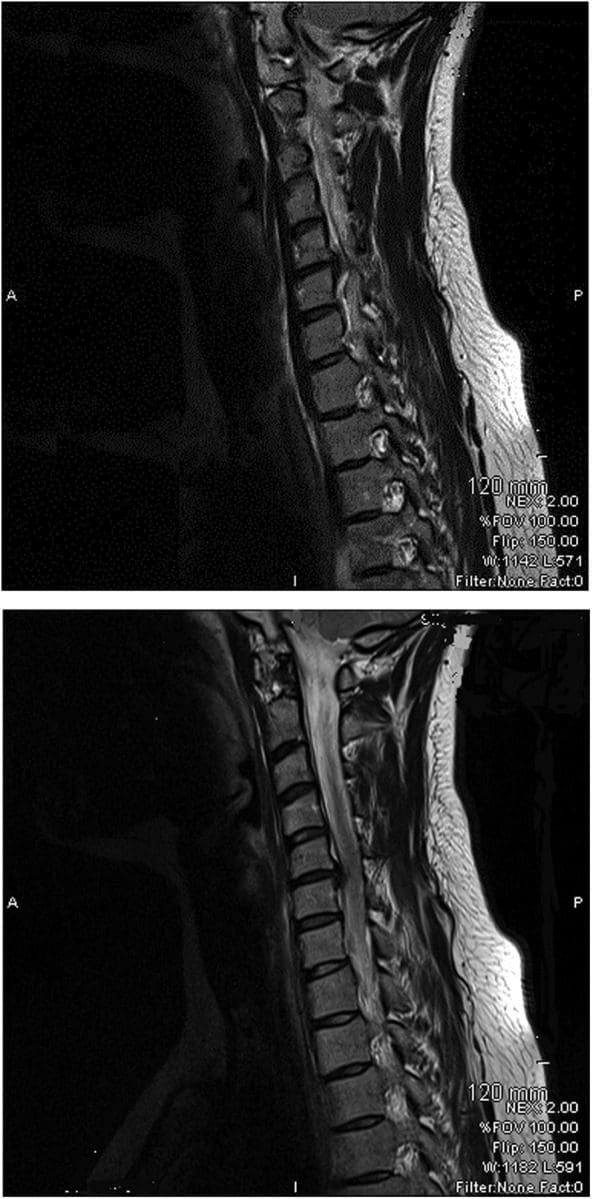



 #4: Avoid Overexertion
#4: Avoid Overexertion
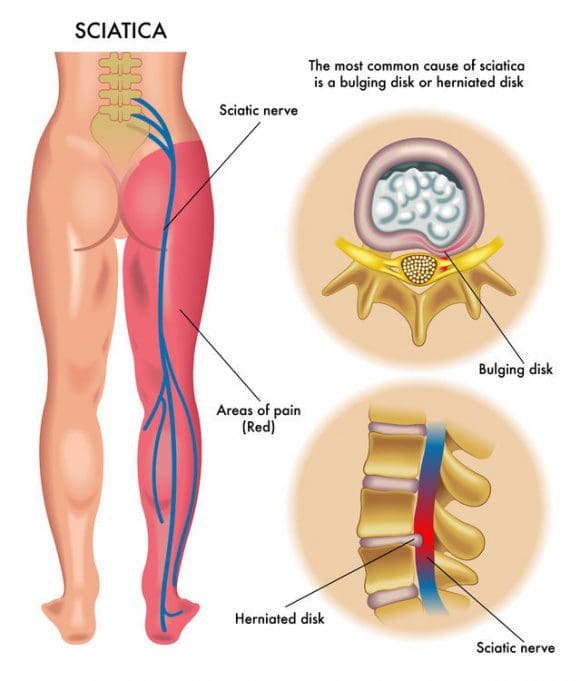 What Causes Sciatic Nerve Compression?
What Causes Sciatic Nerve Compression?
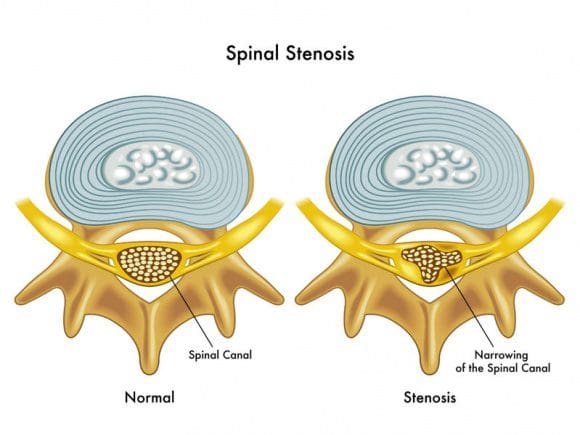 Spinal stenosis is a nerve compression disorder most often affecting older adults. Leg pain similar to sciatica may occur as a result of lumbar spinal stenosis. The pain is usually positional, often brought on by activities such as standing or walking and relieved by sitting down.
Spinal stenosis is a nerve compression disorder most often affecting older adults. Leg pain similar to sciatica may occur as a result of lumbar spinal stenosis. The pain is usually positional, often brought on by activities such as standing or walking and relieved by sitting down.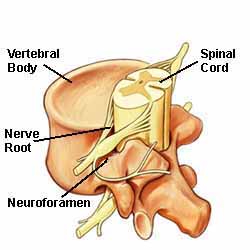 The neuroforamen are the passageways that are naturally created between the vertebrae through which spinal nerve roots exit the spinal canal.
The neuroforamen are the passageways that are naturally created between the vertebrae through which spinal nerve roots exit the spinal canal.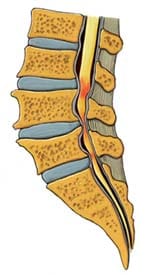 Anatomy Overview Can Help You Understand Spinal Stenosis
Anatomy Overview Can Help You Understand Spinal Stenosis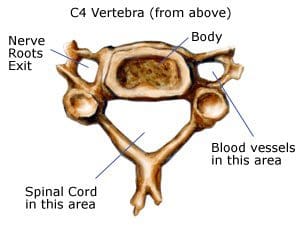 Normally, the spinal channel is wide enough for the spinal cord, and the foramen are wide enough for the nerve roots. But either or both can become narrowed, and cause spinal stenosis.
Normally, the spinal channel is wide enough for the spinal cord, and the foramen are wide enough for the nerve roots. But either or both can become narrowed, and cause spinal stenosis.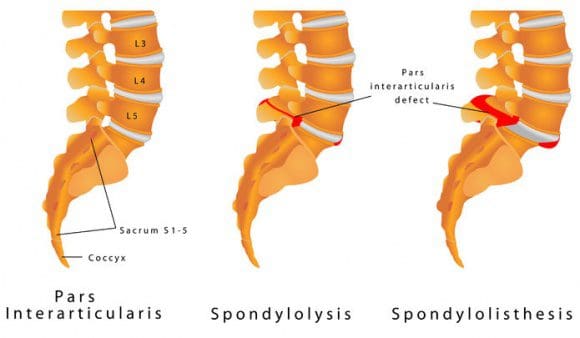
 Arrow Points To A Lumbar Spondylolisthesis
Arrow Points To A Lumbar Spondylolisthesis The muscles in and around the gluteal region help with three areas
The muscles in and around the gluteal region help with three areas
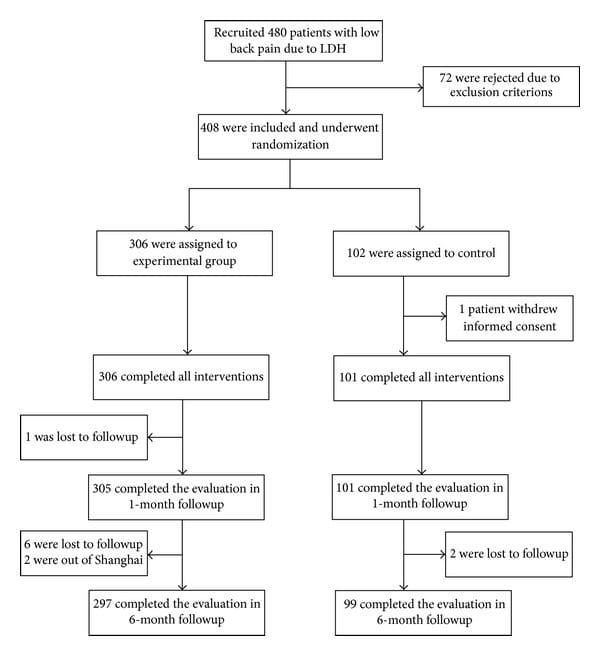
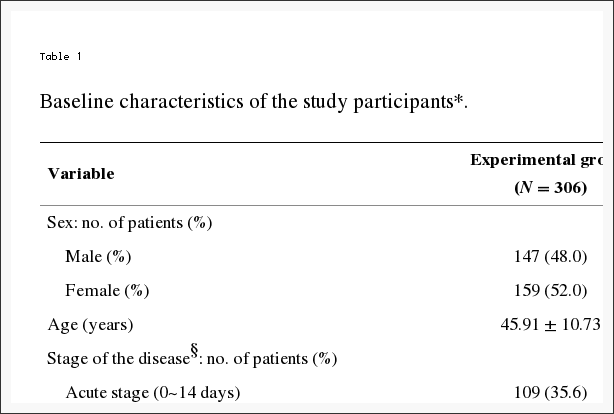
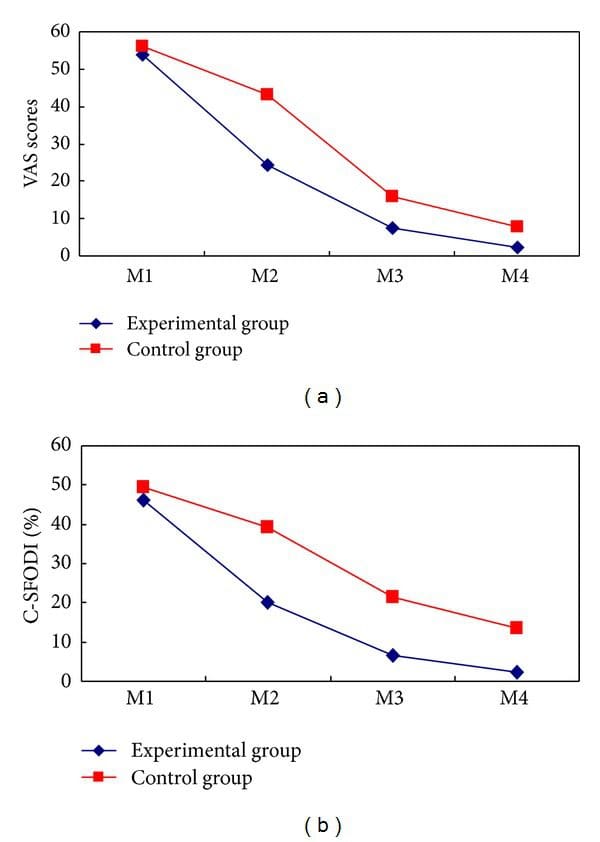
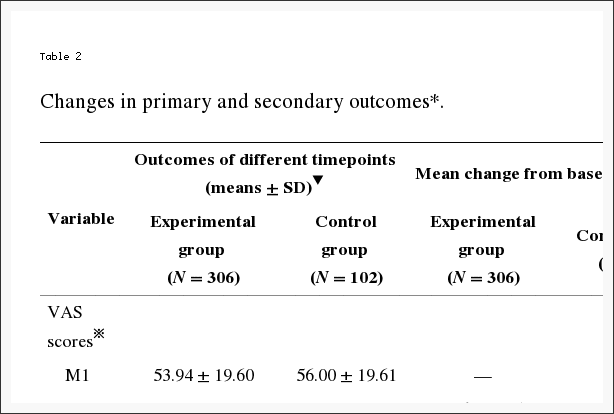

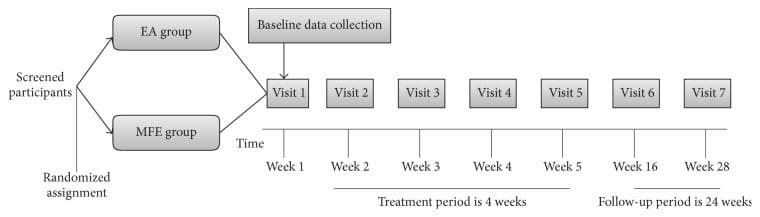
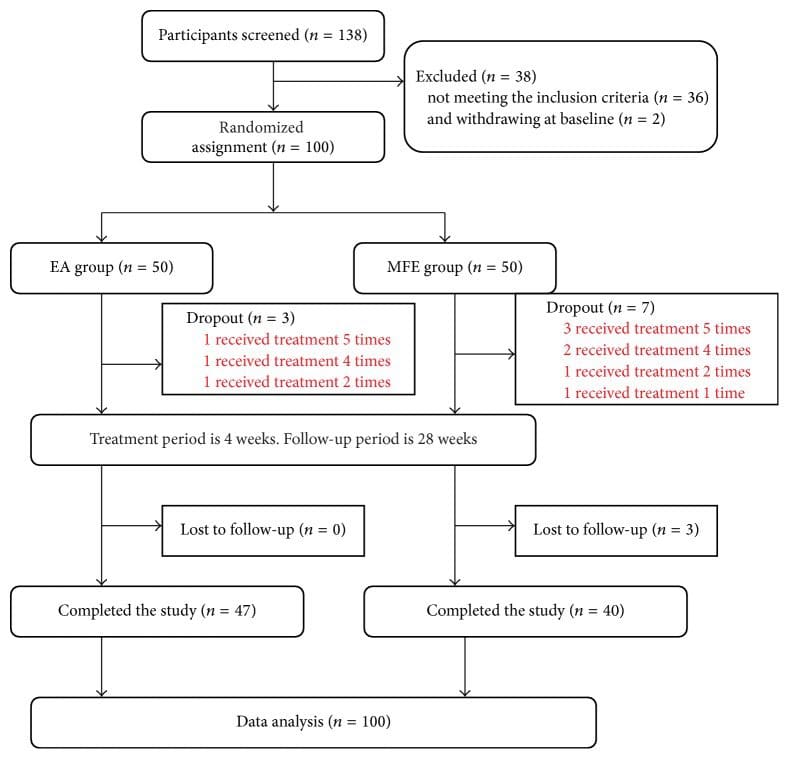
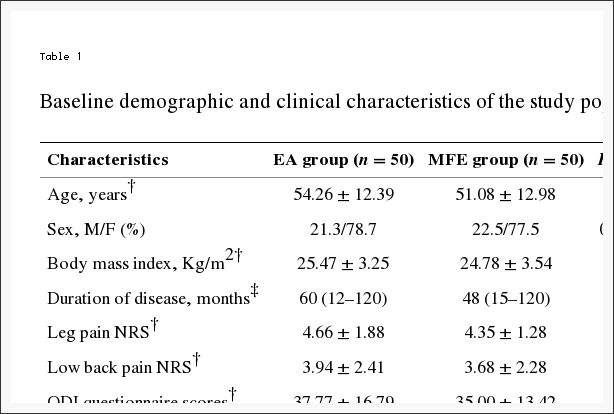
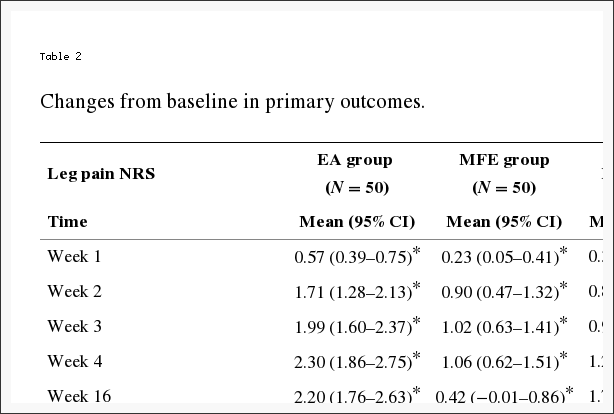
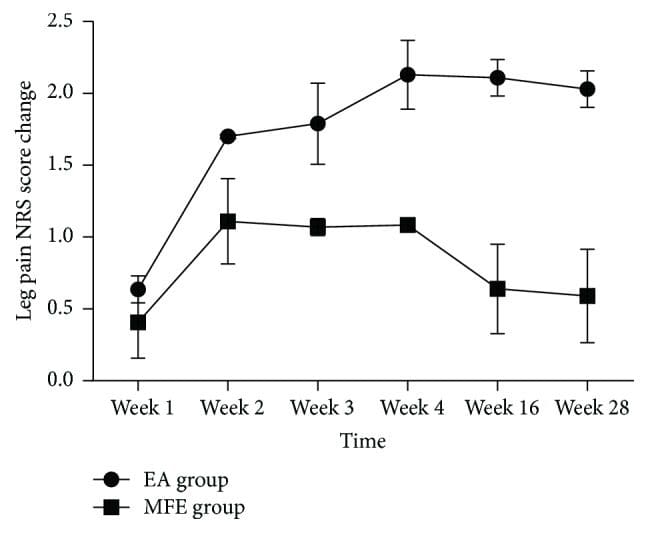
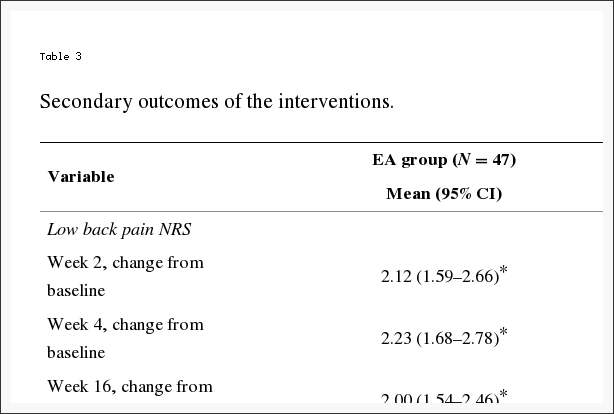

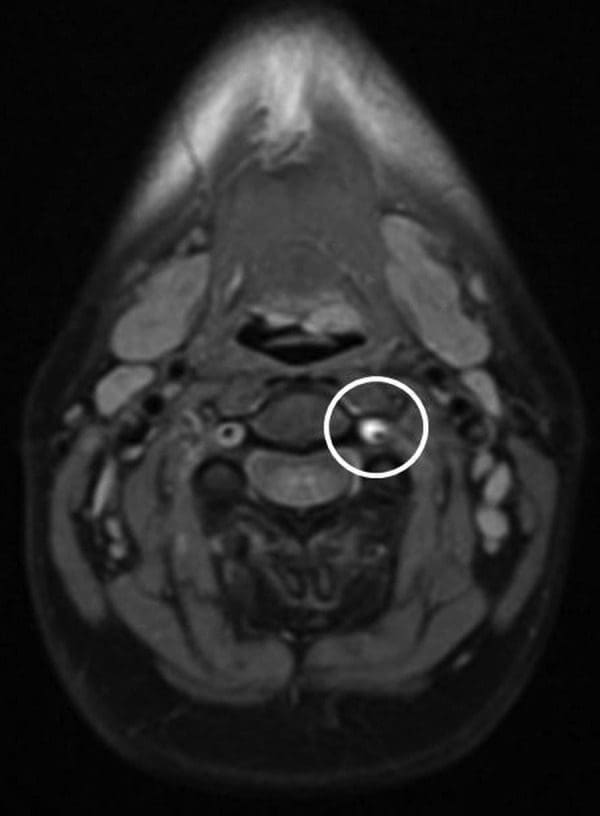
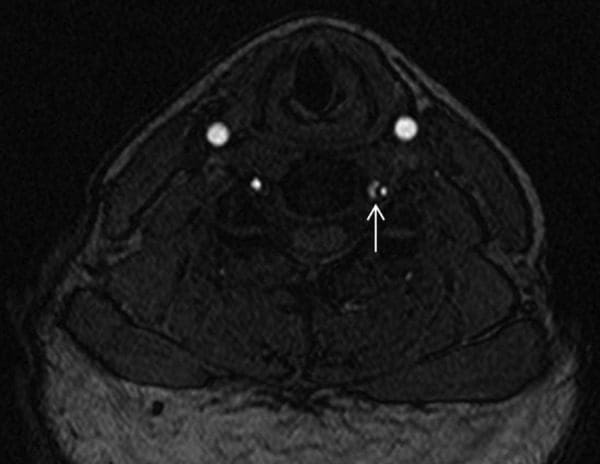
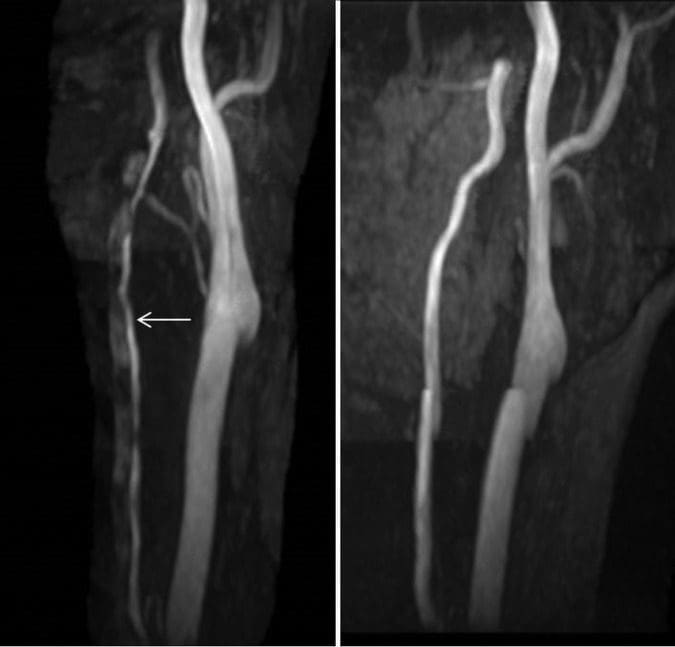



 Don’t Live And Cry By The Scales
Don’t Live And Cry By The Scales






