Sandra Rubio talks about personal injury rehabilitation, including stretches and exercises, which are provided by Dr. Alex Jimenez and his staff, aside from chiropractic care. Dr. Jimenez offers the services of personal trainers and physical therapists to help improve the patient’s strength, mobility and flexibility to prevent further injury as well as to help speed up the patient’s recovery process.
Personal Injury Rehabilitation
Physical therapy (PT), also known as physiotherapy, is one of the allied health professions which, by utilizing mechanical force and motions (bio-mechanics or kinesiology), manual therapy, exercise therapy, and electrotherapy, helps treat injuries and conditions by promoting proper function. Physical therapy is used to improve a patient’s quality of life through examination, diagnosis, prediction and physical intervention. It’s generally performed by physical therapists (called physiotherapists in several nations).
A personal injury doctor or chiropractor is an effective, alternative treatment option for a variety of injuries surrounding the spine. When an individual has suffered an injury as a result of an auto accident, work accident or home accident a personal injury doctor can positively influence the proper progress of their rehabilitation, helping the individual obtain the fair compensation they need and deserve for their injuries. An experienced and well-trained personal injury doctor can provide quality treatment as well as support patients throughout their injury claim procedures.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of each and every one of my patients.
I assure you, I will only accept the best for you�
God Bless You & Your Health�?
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Cerebral palsy is a lifelong set of movement disorders with no cure. There are, however, many options for either retraining patients with cerebral palsy or supplying some kind of relief for individuals with cerebral palsy. Among the more untraditional yet commonly sought after types of treatment for cerebral palsy is visiting a chiropractor which specializes in patients with cerebral palsy.
There is no clear reason behind the development of cerebral palsy. In most cases, though, it is believed to be caused by some injury shortly before, during, and after pregnancy. This injury is to the unborn embryo or the baby after it is delivered. Many cases of cerebral palsy are being found to have happened during the delivery process. Lack of oxygen and/or failure to detect fetal distress are all believed to be the most common reasons for the development of cerebral palsy. As previously mentioned, individuals with cerebral palsy can benefit from a variety of treatment options, including chiropractic care, rehabilitation and neuromuscular reeducation.
Chiropractic Care and Cerebral Palsy
Chiropractic techniques are a sort of healthcare which uses spinal adjustments and manual manipulations, together with other treatment procedures, in order to aid a person’s body in adapting to a more normal position. In patients with cerebral palsy, different body parts can and are generally affected, such as one or both arms and legs, and chiropractic care may be helpful in assisting those limbs regain some semblance of strength, mobility and flexibility.
Additionally, because cerebral palsy is generally believed to be caused by a brain injury, chiropractic treatment methods can be used in healing other, less noticeable, aspects of the motor disease. Behind the doctrine of chiropractic healing lays the idea that the brain and central nervous system control all facets of the body’s functioning. The concept of chiropractic care is that by correcting health issues and symptoms around the central area of the spine, the extremities as well as other areas of the body can regain some stability.
With the rise of “unconventional” medical clinics, chiropractic care has also turned into one of the most popular types of Complementary and Alternative Medicine techniques. In 2004, a report revealed that chiropractic was in the top five kinds of complementary and alternative therapies used for the treatment of a variety of injuries and/or conditions in the United States, including cerebral palsy.
When utilized as an alternative treatment option for cerebral palsy, chiropractic techniques could assist in helping to improve some of the problematic symptoms associated with the movement disorder, including reducing muscle spasms, seizures, and arm and leg issues. As research on the effectiveness of chiropractic care for the safe and effective treatment of many health issues comes to light, there are more encouraging signals for the growth of a successful course of action for individuals with cerebral palsy.
Dr. Alex Jimenez’s Insight
As a qualified and experienced chiropractor in the treatment of a variety of injuries and/or conditions, including genetic neuromuscular disorders, many of our patients with cerebral palsy have experienced tremendous improvements in their quality of life through chiropractic care. Chiropractic care can provide assistance in the improvement of several range of motion aspects associated with cerebral palsy as well as offer significant relief of other symptoms related to this movement disorder. Patients with cerebral palsy currently receiving chiropractic care have experienced improved mobility and an improved gait or ability to walk, including restored sleeping habits. Our treatment methods for patients with cerebral palsy include, upper thoracic pain release, full-body mobility exercises, where multiple joint complexes are moved to increase range of motion, and two-men protocols, to safely and effectively assist the individual throughout their treatment process.
Rehabilitation and Cerebral Palsy
You will find an assortment of rehabilitation alternatives for individuals and children with cerebral palsy. Some are dependent on which kind of cerebral palsy the patient has. Each one of the rehabilitations, however, usually center on creating a few important regions of improvement including physical motion and coordination, language, vision, and intellectual development. Cerebral palsy rehabilitation will invariably involve some type of long-term physical therapy, or physiotherapy. These slight exercises will often involve stretching the individual’s range of motion and to concentrate primarily on developing fundamental motor abilities.
Ongoing treatments and options are becoming more available that could make life with cerebral palsy better. Most rehabilitation centers and treatments use some mix of physical therapy, biofeedback, occupational and speech therapy, occasional use of drugs and/or medications, and on rare cases even surgery.�There are several techniques touted in the field of cerebral palsy rehabilitation, such as the Bobath technique. The Bobath technique centers on positive reinforcement of voluntary movements on the individual’s part and on gradual physical conditioning. The physical therapy may also include external aids such as wheelchairs, walkers, braces, and how to use them for maximum mobility.
Neuromuscular Reeducation and Cerebral Palsy
Chiropractors handle a number of soft-tissue injuries. Unstable or injured muscles can become a source of chronic pain. The only way to remedy the challenge is by dividing those scar tissues and supporting the body to heal in healthy ways. Neuromuscular reeducation accomplishes this in several ways, for example, exercises, deep-tissue massage and vibration therapy.
Exercises for neuromuscular reeducation are often a part of chiropractic care or other rehabilitation program which focuses on helping to improve various adverse conditions that occur from faulty nerve and muscle activities. Neuromuscular reeducation is particularly beneficial for unnatural movement patterns. The purpose of neuromuscular reeducation is to improve balance, coordination, posture and proprioception involving a natural mind-body connection.�Neuromuscular reeducation exercises aim to restore natural movement patterns, optimize joint biomechanics and reduce pain that may result from neuromuscular deficiencies.
Neuromuscular reeducation exercises include a variety of functional strengthening, stretching, balancing and coordination activities. Practitioners that administer these exercises encourage patients to focus on joint positioning and movement.�A variety of stretching and bending movements on an exercise ball also have neuromuscular applications.
Whole body vibration (WBV) treatment is also helpful in the treatment of many physical conditions. WBV lowers inflammation, builds muscle, increases flexibility and breaks apart scar tissues and fused bone fragments. The technology is used to treat an endless number of injuries, along with ailments like scoliosis and cerebral palsy.
As vibrations affect your body, your muscles engage and relax in rapid success in an effort to enhance your movements. This burst of activity helps to break apart these deep scar tissues. The process also can help promote healthy recovery by placing your muscle bands under short spurts of increased stress. For the identical reason, Whole body vibration, or WBV, is very effective in increasing bone density and muscle mass.
In addition, when guided by a trained therapist, you may use vibration treatment to reeducate your muscles on how to respond to stimulation without getting hurt. Partly, While a lot of the process is occurring beneath the surface, WBV may require the individual to perform specific work in the clinic or on their own. This takes a combination of unconscious muscle training and altering habits to protect vulnerable areas while building strength and enhancing mobility and flexibility. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
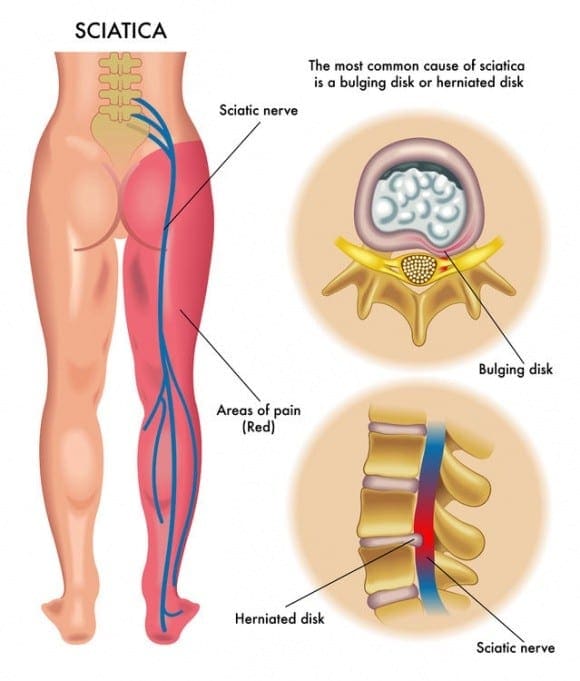
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Health Wellness: Chiropractic has been increasing in popularity over the last few years as the medical community is recognizing its value for treating many conditions as well as improving overall health wellness. There was a time when chiropractic was used to treat back pain, but studies are showing that it can be used to effectively treat a wide variety of health issues. This is due, at least in part, to chiropractic�s whole body approach to health care. It is much, much more than just spinal adjustments.
Health Wellness
Better Neck & Back Health
This is the most obvious and prevalent benefit of chiropractic care � what most people think of when they think about chiropractic care – but its merit goes deeper than may first meet the eye. The traditional spinal alignment is very beneficial for treating pain and improving mobility.
When the spine is aligned the neck and back is healthier which leads to a decrease in tension, better posture, reduced pain, and the central nervous system functions far more efficiently. When the central nervous system is working the way it should, overall health is improved and the body as a whole functions better.
Stronger Immune System
Regular chiropractic treatments have been linked to a stronger immune system. When the spine is in proper alignment, the central nervous system is able to function much more efficiently and effectively. This means that the body is better able to receive messages from the brain.
When the spine is out of alignment, the messages that that are sent and received by the central nervous system can�t complete their path like they should, leaving the organs and other parts of the body not operating as it should. This translates to a better functioning immune system, which means that you may find that you are sick as lot less often.
More Effective Pain Management
Another benefit of a properly functioning central nervous system is better pain management. Chiropractic is an effective treatment for migraines, injuries, fibromyalgia, and pain caused by other conditions.
When the spine is out of alignment it can affect various nerves and conditions like sciatica may occur. Bringing the spine into alignment can relieve the compression of nerves, alleviating pain.
Chiropractic is regularly used to treat sports related injuries for pro athletes to weekend warriors � and everyone in between. Even more, there are many studies that show chiropractic is an effective form of pain management.
Improved Activity Level
A lesser known or recognized benefit of chiropractic that improves your overall health is its ability to improve your activity level. Pain management definitely plays a part in this, but regular treatments also help improve mobility and flexibility. This, in turn, helps to reduce your risk of injury, allowing you to be more active.
When you are more mobile you are better able to stay active which means it is easier to get the exercise that you need to maintain a healthy lifestyle. This is particularly important for older people. As we age, we tend to lose our mobility and flexibility. By starting chiropractic care early, it helps stave off some of those effects of aging. However, even elderly patients have noticed a marked improvement in just a few treatments.
Chiropractic care is a very good way to give your health wellness a great boost. When you make it a part of your regular routine, you are much more likely to enjoy fewer sick days, less pain, the ability to be more active, and a healthier neck and spine. The whole body approach means you will be exposed to not only spinal adjustments, but also recommendations on diet, supplements, exercise, and lifestyle changes that can definitely change your life.
Several lumbar spine (lower back) disorders can cause sciatica. Sciatic nerve pain is frequently described as mild to extreme pain at the right or left leg. Sciatica is caused by compression of one or more of the five sets of nerve roots in the lower spine. Sometimes doctors call sciatica a radiculopathy.
Radiculopathy is a medical term used to describe pain, numbness, tingling sensations, and weakness in the arms or legs caused by a nerve root issue. If the nerve problem is in the neck, it is referred to as a cervical radiculopathy. But since sciatica affects the low back, or the lumbar spine, it is known as a lumbar radiculopathy.
Pathways to Reduce Sciatic Nerve Pain
Five sets of nerve roots at the lumbar spine unite to create the sciatic nerve. Starting in the rear of the pelvis (sacrum), the sciatic nerve runs in the back, under the buttock, and downward through the hip area into every leg and foot. Nerve roots aren’t “solitary” structures but are part of the body’s whole nervous system capable of transmitting pain and feeling to other areas of the body.
Radiculopathy occurs when compression of a nerve root from a disc rupture (herniated disc) or bone spur (osteophyte) happens in the lumbar spine before it joins the sciatic nerve.
Causes of Sciatic Nerve Pain
Several spinal disorders can lead to spinal nerve pain and compression or lumbar radiculopathy. The 6 leading causes of sciatic nerve pain are:
a bulging or herniated disc
lumbar spinal stenosis
spondylolisthesis
trauma from an injury
piriformis syndrome
spinal tumors
Lumbar Bulging Disc or Herniated Disc
A bulging disc is also known as a contained disc disorder. This means that the gel-like center (nucleus pulposus) of an intervertebral disc stays “contained” within the tire-like outer wall (annulus fibrosus) of the intervertebral disc.
A herniated disc occurs when the nucleus pulposus breaks through the annulus fibrosus. It’s known as a “non-contained” disc disorder. If the disc bulges or herniates, disc material can push against an adjacent nerve root and compress delicate nerve tissue and lead to sciatica.
The results of a herniated disc may often be worse. When the herniated disc causes direct compression of the nerve root from the inside of the bony spinal canal, the disc material itself also includes an acidic, chemical irritant (lipoic acid) which causes nerve irritation. In both situations, nerve compression and irritation cause pain and inflammation, often leading to extremity numbness, tingling sensations, and muscle fatigue.
Lumbar Spinal Stenosis
Spinal stenosis is a nerve compression disease most frequently affecting older adults. Leg pain similar to sciatica may happen as a result of lumbar spinal stenosis. The pain is generally positional, frequently brought on by actions like standing or walking and relieved by sitting down.
Spinal nerve roots branch outward in the spinal cord through passageways called neural foramina comprised of bone and ligaments. Between each set of vertebrae, situated on the left and right sides, is a foramen. Nerve roots pass through those openings and extend outward beyond the spinal column to innervate different areas of the human body. Whenever these passageways become narrow or obstructed causing nerve compression, the term foraminal stenosis is utilized.
Spondylolisthesis
Spondylolisthesis is a disease that most often affects the lumbar spinal column. It’s characterized by a single vertebra slipping forward over an adjacent vertebra. When a vertebra slips and is displaced, spinal nerve root compression occurs and often triggers sciatic nerve pain. Spondylolisthesis is categorized as developmental (discovered at birth, develops through childhood) or acquired from spinal illness, injury or physical strain (eg, lifting weights).
Trauma from an Injury
Sciatica can result from sciatic nerve compression brought on by external forces into the lumbar or sacral spinal nerve roots. Examples include automobile accidents, falling down as well as football and other sports injuries. The impact may injure the nerves or, sometimes, fragments of broken bone may compress the nerves.
Piriformis Syndrome
Piriformis syndrome is named for the piriformis muscle and the pain generated if the muscle irritates the sciatic nerve. The piriformis muscle is located at the lower part of the spine, joins to the thighbone and also aids in hip rotation. The sciatic nerve runs beneath the piriformis muscle. Piriformis syndrome develops when muscle spasms develop in the piriformis muscle thereby compressing the sciatic nerve. It may be difficult to diagnose and treat due to the lack of x-ray or magnetic resonance imaging (MRI) findings.
Spinal Tumors
Spinal tumors are abnormal growths which are either benign or cancerous (malignant). Luckily, spinal tumors are infrequent. But if a spinal tumor develops in the pelvic region, there’s a danger for sciatica to grow as a result of nerve compression.
If you feel you’ve got sciatica, call a healthcare professional. The first step toward relieving pain would be a proper diagnosis.
Sciatic pain normally improves within about 4 to 6 weeks. Weakness and numbness may take more time to resolve. Symptomatic treatment such as cold packs, anti-inflammatory medications, and physical therapy/stretches/exercise may help ease discomfort and promote return to regular activities. Surgery to take pressure from the nerve is generally reserved for cases of severe pain. Alternative treatment options, such as chiropractic care, can help improve symptoms of sciatic nerve pain.
Dr. Alex Jimenez’s Insight
Sciatica is correctly defined as a collection of symptoms, rather than a single injury or condition, caused by the compression or irritation of the sciatic nerve. Also known as sciatic nerve pain, sciatica is generally an indication of a serious underlying health issue along the length of the lumbar spine, or low back. Sciatica can develop as a result of a variety of injuries and/or aggravated conditions, including but not limited to, a bulging or herniated disc, trauma or due to piriformis syndrome caused by sports injuries. Because sciatic nerve pain can manifest due to many health issues, diagnosing it can often be challenging. Fortunately, a doctor of chiropractic, or chiropractor, can properly diagnose sciatica in order to follow-up with the best treatment.
Chiropractic for Sciatic Nerve Pain
Diagnosis of sciatica Is crucial. A chiropractor assesses the patient and reviews medical history to ascertain what is causing the patient’s sciatic nerve pain. Chiropractic care is based on the principle which limited spinal motion results in pain and decreased function. Chiropractic care helps the body heal itself with non-invasive (non-surgical), drug-free treatment.
Chiropractic treatment methods for sciatic nerve pain include:
Ice/Cold therapy reduces inflammation and assists control sciatic nerve pain.
Ultrasound is mild warmth made by sound waves which penetrates deep into the soft tissues. It boosts circulation and reduces muscle spasms, cramping, swelling, stiffness, and pain.
Spinal Adjustments (Manual Manipulations). Spinal adjustments and manual manipulations are in the heart of chiropractic care. Manipulation supports restricted motion of the spine and helps restore misaligned vertebral bodies with their appropriate status in the spine. Adjustment techniques vary in the swift high velocity push to people who unite minimal force and mild pressure. Mastery of every technique is an art which requires great skill and precision. Spinal adjustments and manual manipulations are the treatment methods that differentiates chiropractic care from other medical disciplines.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Chiropractic care for individuals with cerebral palsy is considered (in most cases) a natural form of treatment that helps with several musculoskeletal and nervous system conditions that normally affect individuals with the disorder. Past results have been so successful that chiropractic care is an extremely sought plan of treatment to assist with numerous health issues.
What is Chiropractic Care?
Chiropractic care, sometimes known as chiropractic intervention, is an alternative treatment option where licensed chiropractors perform various techniques to help decrease pain and discomfort, and also to restore proper musculoskeletal and nervous system functions. According to the American Chiropractic Association, or the ACA, chiropractic care concentrates on musculoskeletal system disorders and nervous system disorders.
The Palmer College of Chiropractic reports that “no portion of your body leaks the dominance of your nervous system.” This usually means that misalignments of the spine, or subluxations, as well as other improper functions of the spinal cord along with different regions of the human body can lead to poor health and improper musculoskeletal and nervous system functioning.
Treatment includes focusing on various areas of the human body, such as the back, neck, shoulders, upper and lower extremities, and joints in the arms and legs. Chiropractic care may also center on rehabilitation and therapeutic exercises as well as individualized diet programs in order to help increase strength, mobility and flexibility. Treatment is normally performed without any drugs, although some chiropractors have the capacity of prescribing specific medications, if needed.
Chiropractic Care and Cerebral Palsy
A range of documented case studies show that kids with cerebral palsy who received chiropractic care were able to sit up (when they formerly couldn’t), walk up stairs without help, and use their arms and hands better.
For example, Dr. Dan Van Roon, of Van Roon Chiropractic in Massachusetts, wrote that an 8-year-old girl with cerebral palsy, who suffered from frequent seizures and tremors, was treated with chiropractic care after previous clinical efforts, such as physical therapy and acupuncture, proved to be ineffective. Within fourteen days of getting chiropractic care, that comprised of 22 chiropractic adjustments, her mother reported that the child was able to walk upright and walk up stairs by herself (two things she had been incapable of performing).
The young girl’s parents also reported that not only were her muscles not as limp, but she gained confidence, walked and also had a large improvement in her emotional and psychological state of being.
In another case, Dr. Van Roon wrote that a 7-year-old boy who didn’t start walking until he was 5, also revealed significant improvement after receiving chiropractic care. Before treatment, he had seizures, pain and numbness in his limbs, tremors, throat pain, nosebleeds, anemia and excruciating foot pain. After his first chiropractic care session, he started showing improvement.
As treatment progressed, so did the boy’s progress. He gained strength, began walking longer distances, and had progress in both sleeping quality and education.
Additional areas of improvement reported after kids with cerebral palsy had chiropractic care included a decrease in:
Pain and muscle stiffness
Breathing problems
Drooling
Muscle contractions
Neck pain
Musculoskeletal conditions
Gait issues
Spine issues
Anxiety and stress
Headaches and chest pain
Leg/arm problems
Speech problems due to respiratory issues
Spasticity
Urinary incontinence
Common Chiropractic Care Treatment Methods
Throughout the initial chiropractic care session, a full medical history should be supplied so that the chiropractor is first familiar with the individual’s medical history. Then, the chiropractor may ask you and/or your child specific questions about pain and any activities which make the symptoms worse, followed by an exam which could include diagnostic tests, such as X-rays or a MRI test, that may include analyzing the individual’s:
Neurological integrity
Range of movement (in the affected region)
Muscle tone and strength
Abnormalities
Misalignment
Flexion Distraction therapy, and much more
Treatment depends upon medical history and physical exam results. However, common chiropractic care treatment methods include:
Spine adjustments, which can include spinal adjustments and manual manipulations, the “Activator” technique, and/or the “Gonstead” method
Adjustment to joint dysfunctions
Massaging
Electrical stimulation
Traction
Heat/cold applications
Myofacial release
Treatment will consist of a variety of sessions over time. Each session may last anywhere from 30 minutes to an hour, based upon the chiropractor’s techniques and the medical issues and problems. For instance, treatment for lower back pain may require 1 to 3 visits weekly for up to 2 to 3 weeks. Chiropractic care is used in many different settings, like hospitals, clinics, or a private healthcare professional’s office. Most chiropractors run their business from a private office.
Furthermore, a chiropractor may utilize or recommend a series of rehabilitation stretches and exercises to improve some of the conditions associated with cerebral palsy. Daily range-of-motion (ROM) exercises are important to prevent or delay contractures which are secondary to spasticity and to keep the mobility of joints and soft tissues. Stretching exercises are performed to increase range of motion. Progressive resistance exercises must be used so as to increase strength. Also, the utilization of age-appropriate play and of adaptive toys and games based on the desired exercises are important to elicit the child’s complete alliance in the case of cerebral palsy. Strengthening knee extensor muscle exercises aids improve crouching and stride length. Postural and motor control training is essential and should follow the developmental sequence of normal kids (that is, neck and head control ought to be achieved, if at all possible, before advancing to back control).
Dr. Alex Jimenez’s Insight
Chiropractic care is an alternative treatment option which utilizes spinal adjustments and manual manipulations to carefully influence the human body’s musculoskeletal and nervous system. Chiropractic interventions focus on improving overall health and wellness by alleviating pain and discomfort associated with neck and back pain as well as for specific health conditions, such as cerebral palsy and fibromyalgia. Several research studies have demonstrated that chiropractic care is a safe and effective, treatment method towards increasing strength and range of motion in individuals with cerebral palsy, improving quality of life and affecting longevity. Because spinal adjustments and rehabilitation improve the way the brain and the rest of the body function together, evidence has shown how chiropractic care can help improve some conditions of cerebral palsy.
Things to Know Before Visiting a Chiropractor
Sometimes, young children, and parents may get fearful of a few things that happen in a chiropractor’s office, but rest assured these things are normal and there’s no need to stress. For example, when a chiropractor is in the process of performing a chiropractic adjustment, you’ll probably hear a popping noise. This does not mean that any bones are broken. It simply means that the chiropractor released gas from fluids surrounding the joints.
The individual may also experience mild discomfort, but typically, visiting a chiropractor should not be painful. If your child cries due to pain or complains that the treatments are excessively painful, don’t be afraid to talk about it with the healthcare professional, and when needed, seek out another one.
When choosing a chiropractor, especially for children with cerebral palsy, it’s suggested to locate somebody with experience not just with treating children, but also treating individuals with cerebral palsy. Other factors to consider when picking a chiropractor comprise of:
Education
Training
Accreditation or Licensing
Expertise working with other healthcare providers and readily coordinating care
If you have any questions or need tips on which chiropractor to select, start with your or your child’s primary healthcare provider. You’ll also need to contact your insurance provider, to be sure they pay for chiropractic care. While some insurances will cover it, other insurances may not cover what’s considered “complementary” care. Some insurances may cover the costs of a chiropractor only after your child’s primary care doctor grants a medical referral to a chiropractor. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Chiropractic Therapy: Sandra Rubio discusses how Dr. Alex Jimenez and his staff can help relieve your sciatica symptoms. Chiropractic care can improve pain and discomfort as well as reduce irritation and inflammation caused by sciatica. In addition, a chiropractor like Dr. Jimenez can also provide nutritional and fitness advice for sciatic nerve pain. Other treatment methods, like deep-tissue massage, can help relieve sciatica symptoms. Dr. Alex Jimenez is the homeopathic, non surgical choice for sciatic nerve pain and its associated symptoms.
Chiropractic Therapy For Sciatica Pain
Sciatica is generally caused by the compression of lumbar or sacral nerves or by compression of the sciatic nerve. When sciatica is caused by compression of a dorsal nerve root, it’s known as lumbar radiculopathy. This can occur because of a spinal disk bulge or spinal disk herniation (a herniated intervertebral disc), or by roughening, enlarging, or misalignment (spondylolisthesis) of the fascia, or as a consequence of degenerated discs which can reduce the diameter of the lateral foramen by which nerve roots exit the spine.
Our objective is to alleviate your pain and restore freedom, in�treating��our�sciatica�sufferers. Employing state of the art x-ray/fluoroscopic and ultrasound helps our experts pinpoint what�s going on. For treating sciatica we believe in the ability of medicine. By stimulating the body�s natural healing response, these procedures let us naturally provide long-term and deep pain relief.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of each and every one of my patients.
I assure you, I will only accept the best for you�
God Bless You & Your Health�?
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Sciatica Sufferers:Sciatica is a common back ailment that affects approximately 1 in 10 adults in the United States. It is most prevalent in people between the ages of 25 and 45. Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock and back of leg. The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their home, or just enjoying their life. Traditionally, doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
What Is Sciatica?
Sciatica is a condition that affects the lower back, specifically pain that travels along the sciatic nerve path. This path originates in the lower back and extends down each side of the hip, buttocks, and down the leg to the feet. Usually, only one side is affected during a case of sciatica.
Sciatica commonly occurs when there is a spinal condition, such as a bone spur on the spine, a herniated disk, or when a condition like spinal stenosis (narrowing of the spine) compresses the nerve. The result is inflammation, numbness, pain, and stiffness in the leg that is affected.
While sciatica pain can be severe, the majority of the time the condition is resolved in a matter of weeks without surgical intervention. Some doctors may suggest surgery if the patient experiences extreme weakness in the leg or has problems with their bowel or bladder. Most of the time doctors will prescribe medication to treat the pain and relax the muscles that surround the sciatic path in an effort to provide the patient with some relief.
How Chiropractic Treatments Help Sciatica Sufferers
Chiropractic has been shown to be very effective in treating sciatica by helping the body heal itself. It is non-invasive and does not use medications, making it an optimal choice for many patients. There are various treatments that a chiropractor may use or recommend. They may be used alone or in conjunction with other therapies.
Adjustments. Spinal manipulation, or adjustments, is the core of chiropractic treatment. It helps to realign the spine, freeing restricted movement and helps bring the body back into its proper alignment so that it functions better and more effectively. It also helps to reduce the pain that is associated with nerve inflammation, particularly that associated with sciatica.
Ultrasound. A very mild heat that is created by sound waves at a frequency that is beyond human hearing providing deep tissue penetration. This therapy stimulates circulation and aids in reducing muscle spasms, stiffness, swelling, pain, and cramping.
Ice or Cold Therapy. This therapy helps to reduce and control the pain of sciatica, as well as reduce inflammation.
TENS. Transcutaneous electrical nerve stimulation is a therapy that employs a TENS unit, a small battery powered, portable box that stimulates the muscles. It uses electrical currents at variable intensities to help control pain and reduce the occurrence of muscle spasms. Some chiropractors and physical therapists use larger versions of this device in their offices, but many use the portable units because they are more convenient.
A chiropractor may incorporate exercises and nutritional recommendations into their treatment for sciatica sufferers. This often depends on the patient�s individual needs, the severity of the condition, and their lifestyle and habits. A variety of chiropractic techniques may also be used to treat sciatica. Since each patient is different, the chiropractor will talk with the patient to better understand what they do on a day-to-day basis and what may be causing the sciatic pain to occur. From there they will treat the problem from the patient�s perspective, seeking the best, most effective approach.
If you or a loved one is suffering from this condition, please give us a call. Our Doctor of Chiropractic is here to help!
Is sciatica a spinal disorder or a symptom of a spinal disorder?�The term sciatica is commonly used to describe pain traveling in the distribution of the sciatic nerve, therefore it is more accurate to state that it is a symptom of a spinal disorder not a spinal disease itself.
Frequent symptoms of sciatica are listed below.
Sciatica usually affects one side of the human body, although it may affect both.
Pain from sciatic nerve pain may feel dull, sharp, burning, or accompanied by irregular shocks of shooting pain starting in the buttock and traveling downward into the thigh and/or leg.
Sciatica may also extend below the knee and might be felt at the feet.
Occasionally, symptoms of sciatic nerve pain include tingling sensations and numbness.
Sitting and attempting to stand up could be painful and challenging.
Coughing and sneezing can intensify the pain.
Where is the Sciatic Nerve?
Sciatic nerve fibers start at the 4th and 5th lumbar vertebra (L4, L5) and the first few segments of the sacrum. The nerve passes through the sciatic foramen, a nerve passageway just beneath the piriformis muscle which rotates the thigh laterally, towards the rear of the extension of the hip and into the lower part of the gluteus maximus, or the muscle in the buttocks,� that helps with thigh extension. The sciatic nerve then runs vertically down to the rear of the thigh, behind the knee and branches out into the hamstring muscles, or the calf, and farther downward into the feet.
Sciatica Caused by Nerve Compression
Compression of the sciatic nerve may cause any of the above-cited symptoms. Rarely is neurological damage permanent and paralysis is rarely a threat due to sciatica since the spinal cord ends before the first vertebra of the lumbar spine.
When to seek immediate medical attention for sciatica: Increasing back or leg weakness and/or bladder or bowel incontinence is a sign of cauda equina syndrome, a severe illness requiring emergency treatment. If you are experiencing these symptoms at the moment, please seek immediate medical attention from a qualified and experienced back pain specialist.
Certain lumbar spinal diseases can cause or lead to sciatica symptoms, including:
Herniated discs are the usual cause of sciatica in the lumbar spine.
Degenerative disc disease, a natural biological process related to aging, is known to cause disc weakness that may be a precursor to disc herniation.
Lumbar spinal stenosis is a narrowing of one or more neural passageways due to disc degeneration and/or facet arthritis. The sciatic nerve may become impinged as a consequence of these changes.
Isthmic spondylolisthesis results from a stress fracture frequently at the 5th lumbar vertebra (L5). The fracture together with disc space collapse may enable the vertebra to slide forward on the first sacral segment (S1). The slippage might cause the L5 nerve root to become pinched as it leaves the spine, developing into symptoms of sciatica.
Spinal tumors and illnesses are other ailments that may compress the sciatic nerve, but this is rare.
How Your Doctor Diagnoses Sciatica
A healthcare professional’s diagnosis of your pain and other symptoms may include discussing your medical history, recent accidents or injuries (eg, falls) as well as also a review of your current medicines (both over-the-counter and prescription drugs). Your doctor may additionally perform a physical evaluation using one or more movement evaluations to help determine the origin or causes of your pain. During the neurological portion of the evaluation, your reflexes and muscle strength are tested. If needed, they may order imaging studies, like an x-ray, CT scan, or even an MRI. The imaging tests can help confirm their diagnosis.
Furthermore, a healthcare professional may ask you a few questions, such as:
“How did the pain develop?”
“On a scale from 1 to 10, with 10 being the worst pain possible, rate your pain.”
“Is the pain caused by walking uphill or downhill?”
“How does the pain affect activities of daily living?”
“What kind of treatment was attempted and what was effective?”
Not all buttock and leg pain is sciatica as there are a number of different structures in the spine that can cause these kinds of pain. For example, the sacroiliac joint, or the joint between the pelvis and sacrum, the smallest segment of the spine, may cause or refer pain to the buttock as well as a sprain of the facet joints, which would be the connecting joints at the rear part of the spine. A bulging or herniated disc�can also refer pain down into the leg. If buttock and leg pain symptoms are correlated with any neurologic signs of numbness or weakness, it is “true sciatica” and has to be evaluated by a spine care expert, such as a chiropractor. If severe neurologic symptoms occur along with bowel and/or bladder control problems, it needs to be evaluated as soon as possible.
Chiropractic Diagnosis
In the assessment of lower back pain and sciatica, differential diagnosis using a “triage” concept of classifying back injuries and/or conditions to one of three categories helps guide the chiropractor when determining the source of the patient’s symptoms. These categories of chiropractic diagnosis include:
Potentially severe: tumor, infection, fracture, major neurological issues, such as cauda equina, local open wound or burn, prolonged bleeding (hemophilia), artificial joint enlargement, pacemaker problems and joint infection
Nerve issues: whenever the nerve roots from the lower back are pinched or compressed, they may cause� radiculopathy or sciatica. Typical causes of nerve root pinching and irritation include aherniated disc, spondylolisthesis and spinal stenosis
Non-specific: mechanical back pain in the lumbar spinal column. This type of lower back pain is the most frequent presentation, also contains pain for that there is not any identifiable cause.
Once the chiropractor has categorized the patient’s source of their sciatica, they may begin with the proper treatment. With chiropractic diagnosis of potentially serious injuries and/or conditions, the chiropractor will generally refer the patient to a relevant medical specialist, and as appropriate, the chiropractor might co-manage the patient’s care along with other back pain healthcare professionals. With this classification, chiropractic care may be used accordingly to avoid further spinal health issues.
In addition, with chiropractic diagnosis of a nerve root problem causing sciatica and/or non-specific causes of low back pain, chiropractors normally describe the symptoms experienced on the following scale:
Acute (symptoms lasting less than 6 months)
Subacute (symptoms lasting between 6 and 12 months)
Persistent (symptoms lasting for 12 months or more)
Recurrent/flare up (symptoms are similar to original symptoms and return sporadically or due to exacerbating circumstances).
Dr. Alex Jimenez’s Insight
Through the use of several physical evaluations and neurological assessments, a doctor of chiropractic is able to properly diagnose the source of a patient’s sciatica symptoms. Once a diagnosis has been established, a chiropractor will follow-up with the best, most recommended treatment for the individual’s specific needs and requirements. A spinal misalignment, or subluxation, is the most prevalent cause of sciatica. Spinal adjustments and manual manipulations are the most common treatment methods used to help carefully restore the natural alignment of the spine. A variety of other treatment methods can also be used by a doctor of chiropractic, to help speed up the patient’s recovery process. If the diagnosis of a patient’s sciatica symptoms determines that the source of their sciatic nerve pain is severe, a chiropractor may also refer the patient to the most appropriate healthcare professional to continue treatment.
These back pain or sciatica symptoms might be further broken down as mild, moderate or severe in pain. Once a chiropractor has properly diagnosed your sciatica symptoms, they may utilize a series of treatment modalities, including spinal adjustments and manual manipulations, among other well-known alternative treatment options, to help improve sciatic nerve pain.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Crossfit Rehabilitation:Daniel Alvarado, owner of Push-as-RX Fitness, discusses how he carries out his CrossFit personal injury rehabilitation and athletic training program as a part of Dr. Alex Jimenez’s chiropractic rehabilitation plan. Daniel Alvarado ensures that his rehabilitation procedures complements well with Dr. Alex Jimenez’s chiropractic treatment in order to help patients return to their original state of well-being. Both Daniel Alvarado and Dr. Alex Jimenez work hard to maintain a strong dynamic between their collaborative services.
Crossfit Rehabilitation & Chiropractic Care
Crossfit Rehabilitation is a big part of Physical therapy (PT), also referred to as physiotherapy, as one of the allied health professions. By utilizing mechanical force and motions (bio-mechanics or kinesiology), manual therapy, exercise therapy, and electrotherapy, remediates impairments and promotes mobility and purpose. Physical therapy is used to enhance a patient’s quality of life through examination, diagnosis, prognosis and physical intervention. It’s performed by physical therapists (called physiotherapists in many countries).
CrossFit originated as a plan for military forces, police and fire departments, as well as other such organizations to keep their members in the very best shape in their lives. CrossFit has taken the country by storm encouraging anyone from grandparents to specialized elite military personnel to join this growing fitness movement, today.
CrossFit is a core strength and conditioning program made to generate wide-ranging responses out of anyone who engages consistently in this training. That is not a specialized program but one designed to optimize physical performance in every one of the ten fitness realms.
The CrossFit program is intended to increase physical performance of athletes in all physical performance jobs. Qualified CrossFit athletes perform at the maximal amount in multiple, physical challenges that are varied, and randomized.
This is actually the kind of strength and fitness called upon in the line of work such as police, fire fighters, as well as the military. CrossFit has been demonstrated time and time again to be successful in these venues.
Nevertheless, you don�t need to be a top athlete to engage and gain from CrossFit. In fact, everyone from highly conditioned athletes to senior citizens have began CrossFit and benefited from the plans profoundly. The load as well as intensity of the workouts predicated on amount of physical fitness although the difference isn�t in the program.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Sciatica is described as a series of intense and painful symptoms in one or both legs along the course of the sciatic nerve. The pain is generally felt at the back of the leg and runs from the buttocks down the back of the thigh into the calf and foot. The pain may begin suddenly or start gradually, and is typically distinguished by a sharp, shooting, or electric shock-like in quality. Movement of the lower extremities often worsens the symptoms. Pain may be uniformly spread along the leg, but there are certain areas where pain may be more intense. Also,� pain is frequently associated with numbness and/or tingling sensations along the sciatic nerve.
Sciatica can result from any health issue that causes pressure or irritation of the nerve roots that compromise the sciatic nerve. This pressure may result from a variety of injuries and/or aggravated conditions, such as a ruptured intervertebral disc, narrowing of the bony spinal canal, medically referred to as spinal stenosis, or infrequently from infection or tumor. The sciatic nerve is the longest and largest nerve in the body; it measures three-quarters of an inch in diameter and it originates from the sacral plexus; a network of nerves found in the low back, or the lumbosacral spine. The lumbosacral spine refers to the lumbar spine and the sacrum combined. The sciatic nerve and its associated nerves allow movement and enable feeling, known as motor and sensory functions, in the thigh, knee, calf, ankle, foot, and toes.
About the Sciatic Nerve
The sciatic nerve begins in your low back, which is known as the lumbar spine. The nerve roots are in the L4 and L5 vertebrae (the ‘L’ means lumbar, as well as the numbers indicate the degree of the vertebra found along the spine). The sciatic nerve also travels throughout your pelvic area, or the sacrum. In most individuals, the sciatic nerve runs beneath the piriformis muscle, which functions by moving your thigh from side to side. From there, the sciatic nerve descends through the buttocks and the back of your thighs. Behind your knee, smaller nerves branch out from the sciatic nerve and journey down to your toes.
Your sciatic nerve is a part of an intricate arrangement of the human body’s nervous system. The nervous system is responsible for transmitting pain and feelings, as well as other sensations, to other parts of the body. Therefore, when an injury and/or a condition presses on a nerve, you are going to feel it, and many of the times it won’t feel great. With sciatica, a health issue on your low back, such as a herniated disc, for instance, permeates the sciatic nerve, which then transmits pain down your legs.
The sciatic nerve exits the sacrum in the pelvic area of the body through a nerve passageway called the sciatic foramen. At the top part of the sciatic nerve, two branches form; the articular and muscular branches. The articular branch goes to the hip joint. The muscular branch serves the leg flexor muscles, which are the muscles that enable movement. Other complicated nerve structures are also involved, both the peroneal nerves and the tibial nerves. The peroneal nerves originate from the nerve roots in the fourth and fifth vertebrae of the lumbar spine (L4-L5) and first and second levels of the sacrum (S1-2). When the peroneal nerves leave the pelvis, they move down the front and side of the leg and along the outer side of the knee to the foot.
The tibial nerves originate from the nerve roots in L4-5 and S1-3. The tibial nerves move in the front of the knee and then back into the foot, through the heel, sole and toes. In case your sciatic nerve is compressed or irritated, it can cause pain along these pathways; this is how sciatic pain can “spread” or radiate to some of the other parts of the body.
Common Questions and Answers of Sciatica
What is causing my pain? Your sciatic nerve pain, or sciatica, may be commonly caused by but not limited to a bulging disc or a herniated disc, degenerative disc disease, piriformis syndrome, pregnancy, spinal stenosis, a spinal tumor or other spinal illness, spondylolisthesis, or due to trauma from a injury. Any one of those conditions, among others, can put pressure on the sciatic nerve or related nerve roots in your low back. That stress is what causes your pain and other symptoms.
Will I need surgery? Most patients with lumbar radiculopathy respond positively to non-surgical treatments, such as chiropractic care, therefore, spine surgery for sciatica symptoms is seldom needed to treat it. However, there are situations when you might want to check with your healthcare professional about considering spinal surgery, particularly if:
You have bowel or bladder dysfunction. This is rare, but it might happen with spinal cord compression.
You have spinal stenosis, and your doctor believes that surgery is your best way to take care of it.
You are having other neurologic dysfunctions, such as intense or severe leg weakness.
Your symptoms become severe and/or non-invasive treatments are no longer effective.
What types of surgery are used for lumbar radiculopathy? Two frequent spinal surgeries for sciatica are:
Discectomy or microdiscectomy: In both these procedures, the surgeon removes part or all of a herniated disc that is pushing in your sciatic nerve and causing the symptoms. The distinction between the processes is that a microdiscectomy is a minimally invasive operation. The surgeon uses microscopic magnification to operate through a really small incision with very tiny instruments. Because the surgery is minimally invasive, you should recover more quickly from a microdiscectomy.
Laminectomy or laminotomy: These processes both involve a part of the spine known as the lamina, a bony plate that protects the spinal canal and spinal cord. A laminectomy involves the removal of the whole lamina; a laminotomy removes only a section of the lamina. These processes can produce more space for the nerves, therefore reducing the likelihood of the nerves being compressed or pinched.
Can I utilize over-the-counter drugs and/or medications to deal with my pain? Over-the-counter non-steroidal anti-inflammatory drugs, or NSAIDs, can help reduce swelling and inflammation while relieving your pain. You and your doctor have plenty to choose from. You may use acetaminophen (eg, Tylenol), ibuprofen (eg, Advil), or naproxen (eg, Aleve). However, the use of drugs and/or medications only temporarily relieves the symptoms of sciatica without treating the source of the pain. Make sure to talk to a healthcare professional regarding the utilization of these and continue to seek the most appropriate treatment for your sciatic nerve pain, such as chiropractic care.
How Chiropractic Can Help Treat Sciatica
Sciatica is a frequent issue for a lot of people that is identified by pain that begins in the lower back or buttocks, then radiates into one or both legs. It may vary in terms of frequency and severity, but it may often be constant.
The pain from sciatica can often be severe, and in addition, it can be very sharp. It may be associated with tingling sensations, burning, or numbness and weakness. What people may not realize is that it’s a collection of symptoms, an indication that something isn’t right, rather than a single type of injury and/or condition itself. The problem which leads to pain is generally a misalignment, or subluxation, of the lumbar spine. The sciatic nerve begins in the lower back and extends to the lower leg. That is why the pain may often be felt everywhere along the sciatic nerve.
A chiropractor commonly treats patients with symptoms of sciatica. Spinal adjustments and manual manipulations will aim to realign the spine, taking the pressure from the sciatic nerve and often bringing immediate relief. When the stress is off, the body can begin to heal itself. While spinal adjustments and manual manipulations are probably most frequently used, other treatments may be provided, particularly if common chiropractic care may not be advisable. Other treatment modalities might include using ultrasound, a TENS, or transcutaneous electrical nerve stimulation, device, or ice therapy. Ultrasound warms the region and increases circulation, which can lessen the swelling and muscular tension. A TENS device brings relief using a minor electric current to relax muscle spasms and also to increase endorphins. Furthermore, physical therapy, massage and or a series of stretches and/or exercises, may also help improve sciatica.
Dr. Alex Jimenez’s Insight
Chiropractic care is a popular, alternative treatment option commonly utilized to help treat symptoms of sciatica. Sciatica is characterized as a collection of symptoms, rather than a single injury or condition. A chiropractor can help diagnose the source of a patient’s sciatic nerve pain, or sciatica, in order to properly determine the best treatment for their specific health issue. Spinal adjustments and manual manipulations can be utilized to help carefully correct the alignment of the spine, restoring the natural integrity of the spine and allowing the body to heal itself, without the need for drugs and medications or surgery.
In certain individuals, sciatica may fix itself, possibly happening just once or a few times throughout their lifetime. But, it’s important to remember that if an injury and/or aggravated condition is not treated effectively, symptoms may worsen. A chiropractor can help provide relief from your sciatic nerve pain. Physical activity will most likely be recommended to strengthen the muscles in the back to help prevent sciatica as well as to speed up the recovery process. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
 A personal injury doctor or chiropractor is an effective, alternative treatment option for a variety of injuries surrounding the spine. When an individual has suffered an injury as a result of an auto accident, work accident or home accident a personal injury doctor can positively influence the proper progress of their rehabilitation, helping the individual obtain the fair compensation they need and deserve for their injuries. An experienced and well-trained personal injury doctor can provide quality treatment as well as support patients throughout their injury claim procedures.
A personal injury doctor or chiropractor is an effective, alternative treatment option for a variety of injuries surrounding the spine. When an individual has suffered an injury as a result of an auto accident, work accident or home accident a personal injury doctor can positively influence the proper progress of their rehabilitation, helping the individual obtain the fair compensation they need and deserve for their injuries. An experienced and well-trained personal injury doctor can provide quality treatment as well as support patients throughout their injury claim procedures.







 Our objective is to alleviate your pain and restore freedom, in�treating��our�sciatica�sufferers. Employing state of the art x-ray/fluoroscopic and ultrasound helps our experts pinpoint what�s going on. For treating sciatica we believe in the ability of medicine. By stimulating the body�s natural healing response, these procedures let us naturally provide long-term and deep pain relief.
Our objective is to alleviate your pain and restore freedom, in�treating��our�sciatica�sufferers. Employing state of the art x-ray/fluoroscopic and ultrasound helps our experts pinpoint what�s going on. For treating sciatica we believe in the ability of medicine. By stimulating the body�s natural healing response, these procedures let us naturally provide long-term and deep pain relief.



 CrossFit originated as a plan for military forces, police and fire departments, as well as other such organizations to keep their members in the very best shape in their lives. CrossFit has taken the country by storm encouraging anyone from grandparents to specialized elite military personnel to join this
CrossFit originated as a plan for military forces, police and fire departments, as well as other such organizations to keep their members in the very best shape in their lives. CrossFit has taken the country by storm encouraging anyone from grandparents to specialized elite military personnel to join this 






