If you are currently thinking about the ketogenic diet, then you might be asking yourself, is the keto diet right for you? While you may have already heard about the benefits of the ketogenic diet, you might still be wondering about whether if it is worth it to completely change your diet to take advantage of these benefits.
The keto diet has many benefits, from weight loss and improved physical health to mental clarity and enhanced physical performance. In the following article, we will dive into the details of some of the ketogenic diet health benefits. These benefits can help with the particular health goal you may be attempting to attain.
Contents
Ketogenic Diet and Weight Loss
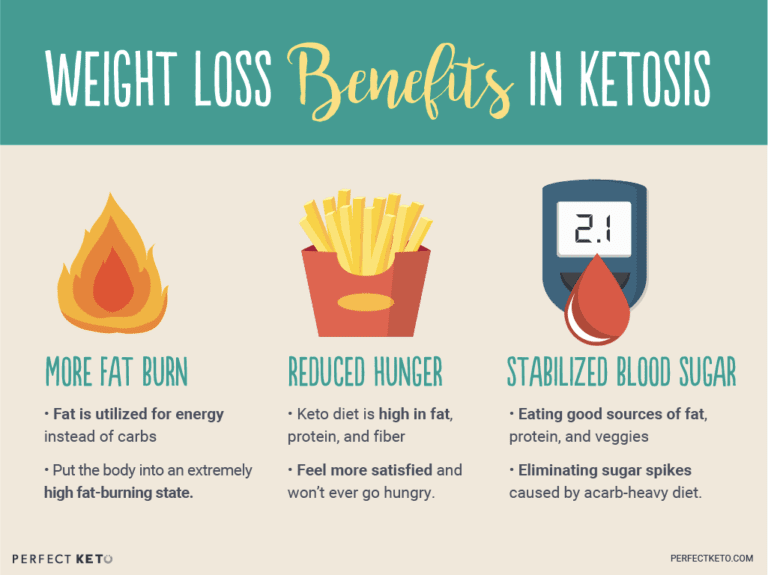
In comparison to low-fat dieting, a low-carb diet can deliver superior results within a shorter time period in terms of weight loss, and the management of cholesterol, and blood pressure. If you want to shed weight, the ketogenic diet plan provides the following benefits and will get you closer to attaining your objective. There can be many reasons for this, including:
Low-carb and ketogenic diets are more satisfying with their low carb content and higher quantities of fats and protein.
Going onto a low-carb diet usually makes you lose extra water weight.
Most individuals can undergo weight loss fairly quickly, especially within the first week�of beginning a ketogenic diet.
Increased HDL Cholesterol
Together with the high consumption of saturated fats and other healthy fats, the ketogenic diet may help raise HDL cholesterol and enhance triglycerides levels. Both of these are�considerably significant towards promoting heart health.
Ketogenic Diet and Physical Health
Acne
Following the ketogenic diet has been demonstrated to also be able to help reduce inflammation and lesions of the skin like those found in acne. This is believed to occur due to the effects of ketosis, or the state in which the cells use ketones instead of glucose for energy.
IBS Support
Moreover, several research studies have also associated a link between the reduced consumption of glucose, or sugar, and an improvement in symptoms of irritable bowel syndrome, or IBS. As a matter of fact, one research study demonstrated that following a ketogenic diet may improve bowel movement habits and help reduce abdominal pain, improving quality of life in people with IBS.
Ketogenic Diet and Physical Performance
Balanced Energy Levels
Do not be surprised if you’re ready to stop drinking coffee every day after adapting to the keto diet. Achieving and maintaining ketosis involves benefits like no day slumps, no mood swings, and reducing changes in energy levels that you might experience otherwise.
In addition, you’ll likely find it much easier to remain longer periods of time without feeling hungry. This is what ultimately helps with weight loss, steady blood sugar levels, and extended periods of fasting, which is one of the best ways to get into ketosis.
Enhanced Workouts
Adjusting to the ketogenic diet may take time, however, once your body gets used to burning fat for fuel rather than sugar, or glucose, from carbohydrates, you will likely notice a difference in your physical performance and endurance, such as more energy and focus for workouts. This makes sense because being in ketosis “instructs” the entire human body to burn fat for fuel more efficiently.
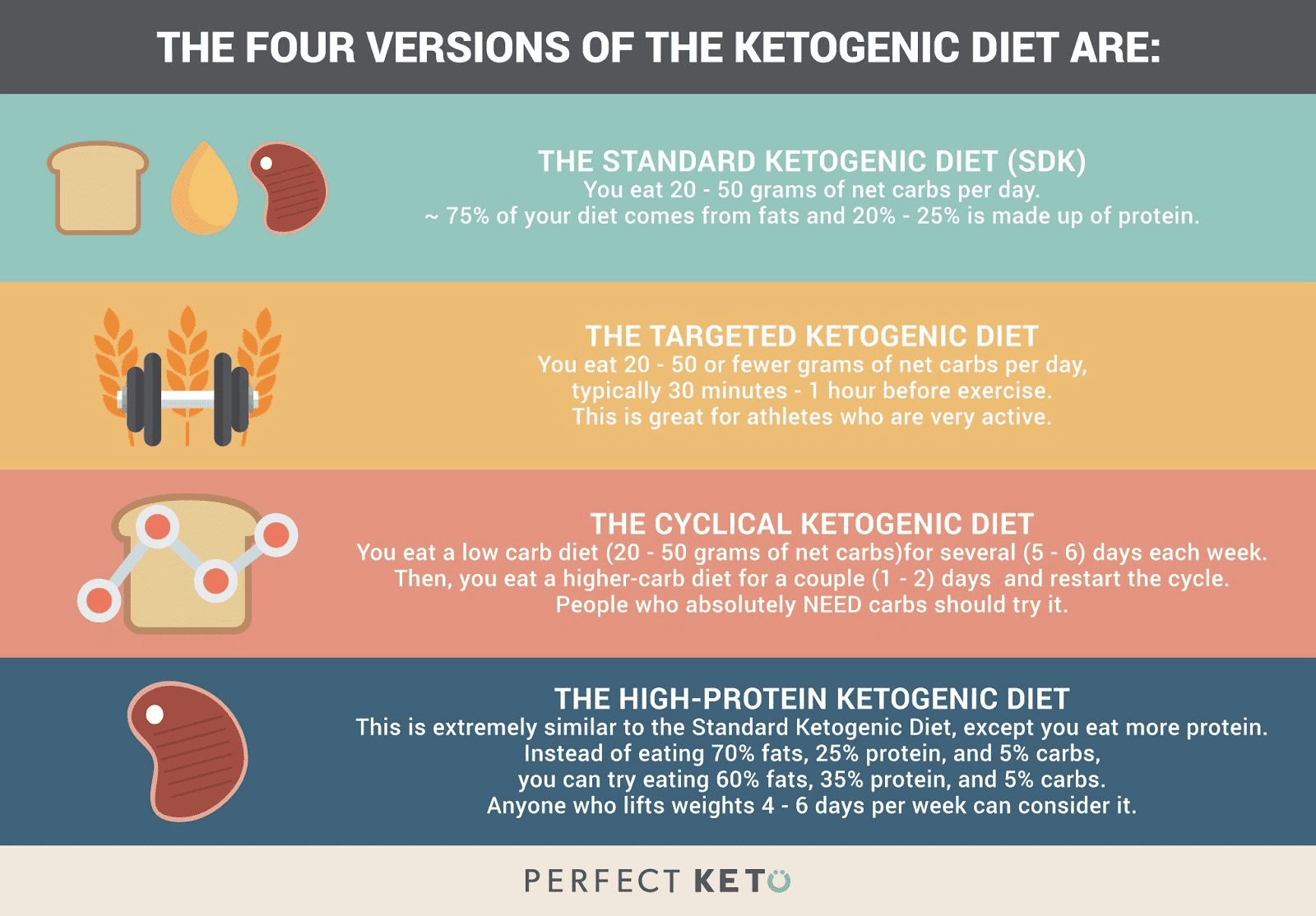
The most important first step in case you start the ketogenic diet and notice limitations in your physical performance is to give your body some time to adapt from utilizing carbohydrates as its primary fuel to utilizing ketones as a source of energy. For individuals who participate in a lot of physical activities and exercise as well as athletes may benefit from a cyclical or targeted ketogenic diet.
Fat Loss / Muscle Gain
The amount of protein intake on a ketogenic diet makes it excellent for building muscle mass. Results might seem to come more gradually than for someone fueling their workouts but that is usually because you’re building lean mass together with fat reduction. By way of instance, when documenting a keto fast for four days, the individual gained 2.4 lbs of muscle with 1.1 lbs of fat reduction.
Ketogenic Diet and Mental Clarity
Several research�studies have demonstrated that a ketogenic diet may have the ability to support mental clariy as well as help boost productivity, support better memory, and also, have positive effects in regard to moderate cognitive impairment.
Neurological Support
Early usage of the ketogenic diet has been used as a treatment for reducing seizures in people with epilepsy, especially children. Additionally, it has been shown to benefit people with Parkinson’s disease, Alzheimer’s disease, and other neurodegenerative disorders. This is likely because ketone bodies created through the keto diet can have neuroprotective effects.
Weight loss is one of the most well-known advantages of the ketogenic diet, however, this nutritional plan can have many other health benefits. By reducing the consumption of carbohydrates, the cells will go into a state of ketosis and instead utilize ketones created from fats, providing a steadier supply of energy than that of glucose, or sugar. Furthermore, research studies have also demonstrated the ketogenic diet’s possible role in disease prevention, such as for people with epilepsy. Dr. Alex Jimenez D.C., C.C.S.T. Insight
The benefits of the ketogenic diet are essential, not just for weight loss, but for overall health and wellness. When you are eating more fats and proteins with fewer carbohydrates, you are more likely to end up eating fewer calories. With this, you also don’t experience a change of energy levels but instead maintain a level of energy that lets you remain focused on your everyday tasks.
Regardless of the health goal you have in mind, the ketogenic, or keto, offers many benefits to improve your quality of life. Being aware of the proper foods you should eat on the keto diet is also important. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Exercise is an essential part of good health. It can help with weight loss and plays a crucial role in preventing many chronic health conditions like hypertension, diabetes, and heart disease. Regular exercise has also been shown to help with depression and anxiety. There is just something about getting your body moving and your blood pumping. It is what nature intended; as humans, we are supposed to be active. The more active you are, the better you will look and feel � and the healthier you will be.
There are many different types of exercise out there, though. It seems that everyone has �system� or some slick, branded fitness routine that is guaranteed to work. The thing is, the old-fashioned way is best. Cardio, the type of exercise that raises your heart rate and gets your blood pumping is categorized by aerobic and anaerobic. Understanding the similarities and differences will help you round out your workout for better results.
Contents
What is Aerobic Exercise?
Aerobic exercise involves low to high-intensity physical exercise. The movements are oxygen infused, relying on the oxygen to meet the demands of the activity. Typically, exercises that are light to moderate intensity fall under aerobic:
Walking
Cycling
Swimming
Rowing
Jogging
Running
These activities can be performed for longer. Many experts advise that an aerobic exercise workout is better when done for an extended period; at least 18 to 20 minutes. For instance, a person can walk on a treadmill for 20 to 30 minutes, then cycle for the same amount of time. This is sufficient for raising the heart rate and increasing metabolism.
Aerobic exercise was first introduced in the 1960s by doctor and Air Force Colonel, Kenneth Cooper. He created the Cooper Institute in 1970, which focused on preventive medicine, centered around education and research. The workout became very popular in the �70s and �80s as a class workout but over time has expanded to become a significant part of gym workouts all over the world.
What is Anaerobic Exercise?
Anaerobic exercise is high-intensity physical exercise. Where aerobic build endurance, anaerobic is more like a sprint, building power, speed, and strength. It increases muscle mass and improves performance. It lasts from several seconds to around 2 minutes. Engaging in physical activity for longer than 2 minutes becomes more aerobic. Types of anaerobic exercise include:
Jump rope
Cycling sprints
Running Sprints
Swimming sprints
Heavyweight training
Anaerobic activities are often interspersed with aerobic activities in interval training for maximum effect.
Levels of Intensity
Aerobic and anaerobic exercise can be combined to create a highly effective workout. It can involve increasing the intensity of an aerobic exercise, or it can mean changing from an aerobic activity to an anaerobic activity.
For instance, you may jog for five minutes, then sprint for two, and jog for five more minutes. Another option is to switch up the activities. Walk on a treadmill for seven minutes, do a cycle sprint for two minutes, row for seven minutes, and jump rope for two minutes. The combinations are endless, and you can customize it for your favorite exercises or accommodate physical limitations.
Health Benefits
Aerobic and anaerobic exercise has been shown to help prevent certain types of cancer, like breast cancer and colon cancer with just 30 to 60 minutes of moderate intensity exercise a day. Exercise has also been shown to prevent osteoporosis, diabetes, depression, cardiovascular disease, obesity, and it even improves cognitive function.
Find ways to incorporate some aerobic and anaerobic exercise into your fitness routine at least several times a week. It is how you get healthy, stay healthy, and feel better.
Being involved in strenuous physical activities and exercises as an athlete can often result in a variety of sports injuries. For several of Dr. Alex Jimenez’s patients, their painful symptoms tremendously affected their overall athletic performance. Chiropractic care is a safe and effective, alternative treatment option which focuses on the diagnosis, treatment, and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Several patients describe how Dr. Alex Jimenez’s sports injuries rehabilitation has helped them find pain relief from their symptoms and allowed them to return-to-play faster than with other treatments. Dr. Alex Jimenez is highly recommended as the non-surgical choice for sports injuries, among other common health issues.
Chiro Rehab
�
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us. Recommend: Dr. Alex Jimenez � Chiropractor
Have you started following the ketogenic diet? Are you confused with what type of fats you should eat to achieve and maintain ketosis? In the following article, we will list the different types of essential fats which are vital in the ketogenic diet.
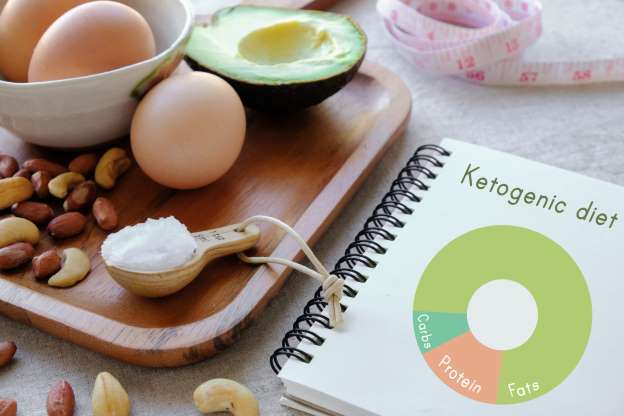
Fats are crucial in the ketogenic diet. To promote the breaking down of fat rather than protein or carbohydrates, you need to consume fat, a process known as ketosis. However, the value of the healthy fats you eat is fundamental.�Fat is satiating and it tastes good. Simply, be sure to eat the ideal kind of fat. There are four categories of fat permitted on the ketogenic, or keto, diet:
Polyunsaturated fats
Monounsaturated fats (MUFAs)
Polyunsaturated fats (PUFAs), which comprises omega 3
Only naturally-occurring trans fats
Remember that a balance of omega-3s and omega-6s can help maintain overall health and wellness, improving brain and nerve function and decreasing the risk of cardiovascular disease, Alzheimer’s disease,�and type-2 diabetes. While omega-6 is vital, however, too much of it can cause inflammation in the human body, therefore, avoid eating high amounts of omega-6 from sources like peanuts and vegetable oils, such as corn oil or sunflower oil.
Instead, focus largely on the intake of omega-3s from fish sources like trout, salmon, tuna, and mackerel or take a high-quality fish oil supplement. Additionally, be cautious of seeds and nuts since they do include some carbohydrates, particularly pistachios and almonds. Make certain that the fat you eat�is currently coming out of nutrient-dense foods, such as fatty cuts of meat. Below is a food listing of the major types of fat in the ketogenic diet.
Fats are the basis of the ketogenic diet. The high fat intake and the low fat intake helps achieve and maintain ketosis, or the creation of ketones. Utilizing ketones for fuel, the human body can burn fat instead of sugar or glucose from carbohydrates. Getting and keeping your body in the state of ketosis can provide many health benefits, including weight loss and overall health and wellness. The quality of fats you consume while on the keto diet is essential towards reaching ketosis. The following article discusses the different types of fats you can eat while on the ketogenic diet and which ones you should avoid. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Contents
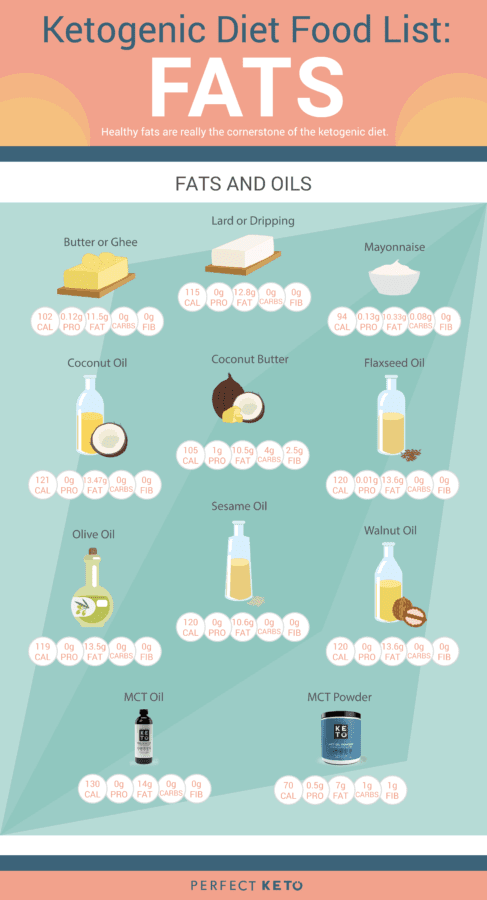
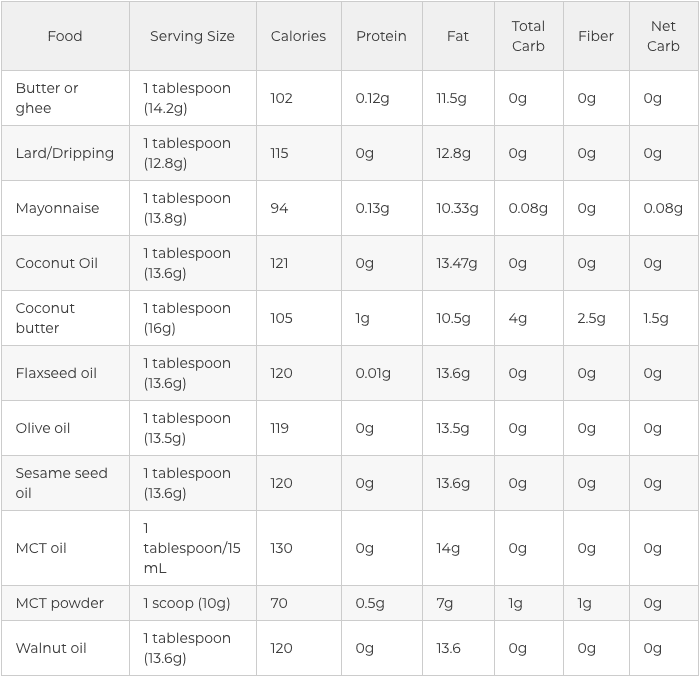
Fats and Oils in the Ketogenic Diet
The value of your dietary fat on keto creates a massive difference in the results that you’ll see. If you are taking an unhealthy approach for your new low-carb diet program, then you will quickly discover reverse health consequences. That is why it’s vital to understand which sources of fat are actually considered safe and healthy to consume on while on the ketogenic diet.
The very first sort of healthy fat to begin including on your keto diet plan is saturated fat. Saturated fat was analyzed and proven to enhance HDL and LDL cholesterol levels, both good and bad cholesterol markers, and it may also strengthen bone density and improve the function of your immune system as well as promote the production of important hormones in the human body.
Saturated fats include:
Grass-fed and organic red meats
High fat dairy like ghee, grass-fed butter, and heavy cream
Lard, tallow, and eggs
These are animal-based saturated fats but there are also plant-based selections like olive oil and MCT oil that could provide you with the wholesome dose of saturated fats that you need to maintain your�well-being. Branching out of healthy unsaturated fats, both monounsaturated fatty acids and polyunsaturated fatty acids can help you accomplish your ketosis objectives. Take a look at the graph below to get a visual of these wholesome oils and fats to focus on if following a ketogenic diet.
Monounsaturated fats include:
Virgin olive oil, avocado oil, and macadamia nut oil (eating avocados and olives also helps you reap these healthy fats)
Certain nuts and seeds
Polyunsaturated fats include:
Nuts and seeds such as walnuts, flaxseeds, chia seeds, sunflower, and pumpkin seeds
Flaxseed oil, sesame oil, fish oil, avocado oil, and krill oil
Fatty fish like trout, mackerel, salmon, and tuna
Fats and Oils to Avoid in the Keto Diet
You will also have to learn that some dietary fats should be avoided altogether. Simply because you are after a high-fat ketogenic diet does not mean that you ought to indulge in each fat you encounter. All fats aren’t created equal. Stay away from unhealthy fats like:
Hydrogenated and partially hydrogenated oils. These fats can be present in packaged foods. They may also increase your risk of developing higher cholesterol, cancer, obesity, and heart disease along with inflammation. If you are relying on packaged foods to get you through the ketogenic diet, check the tag and ditch any foods with them.
Highly processed vegetable oils. Peanut oil, corn oil, canola oil, soybean oil, sunflower oil, and grapeseed oil are fats which seem healthier than they are. These fats are generally created with genetically modified seeds which are possible allergens. Extreme heat can also make these oils go rancid. Additionally, they may leave fatty deposits on your body that may result in heart attacks and premature death. Finally, these oils contain higher levels of omega 6 fatty acids which can lead to chronic inflammation.
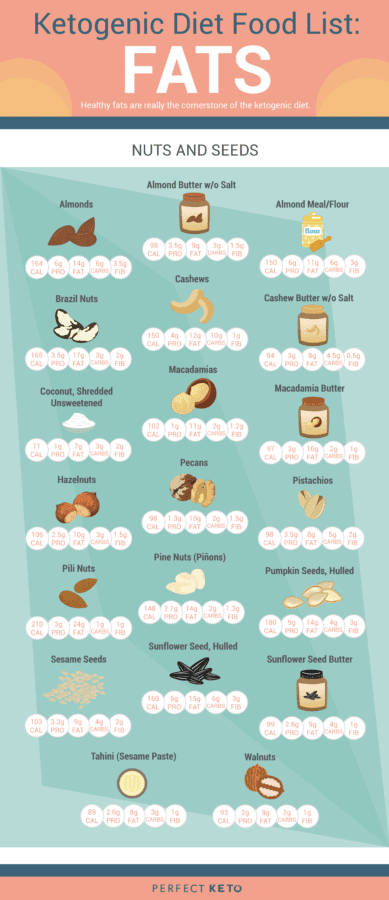
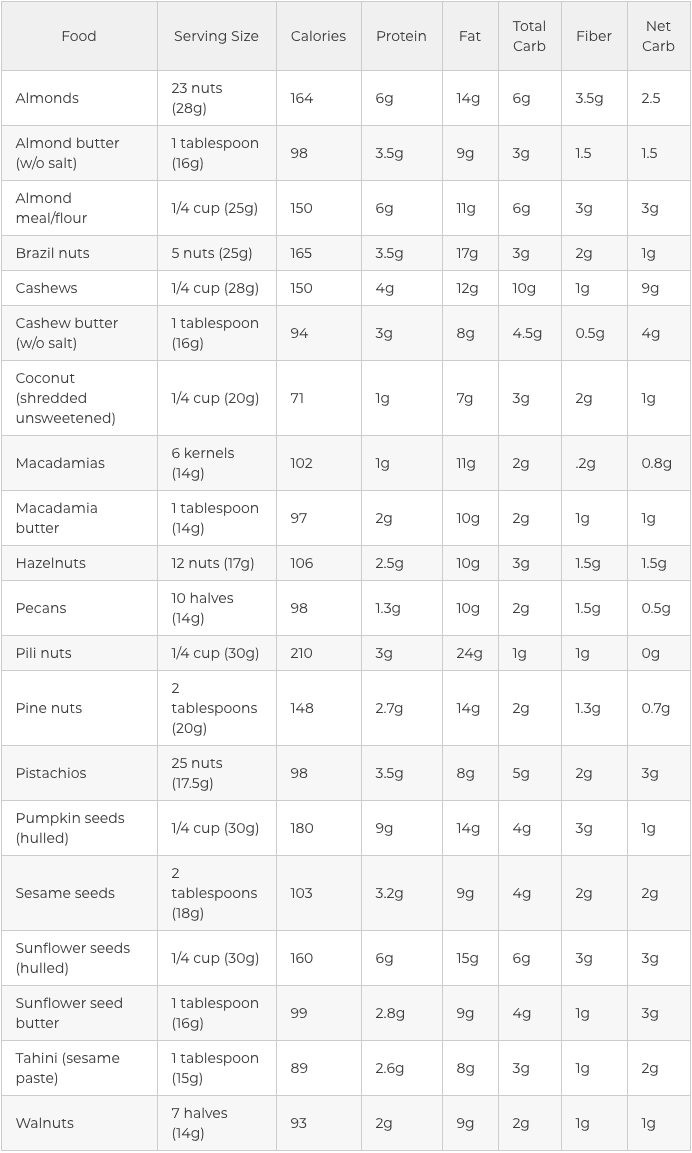
Nuts and Seeds in the Ketogenic Diet
Another simple and gratifying way to sneak healthy fats into the ketogenic diet would be to reach for uncooked seeds and nuts. These nutrient powerhouses are packed with essential nutrients, such as magnesium, selenium, and manganese. Seeds and nuts may enhance brain health, fortify your immune system, and assist with digestion and blood sugar control.
They are also high in healthy fats, have a moderate quantity of protein, and are usually low carb, based on the kind you select. Nuts and seeds are also simple to�carry, which makes them among the best snacks when on a keto diet. Some nuts and seeds, however, are better than others. In keto, this implies that they have more fat and less carbohydrates.
The five best nuts in the ketogenic diet include:
Macadamia nuts
Pecans
Brazil nuts
Walnuts
Hazelnuts
Pine nuts, almonds, cashews, and pistachios are also great nuts to include into the ketogenic diet. However, because they have more carbohydrates compared to the top five, they need to be consumed in moderation so that you don’t accidentally tip on your carbohydrate count daily. Consuming one or more one of these nuts as nut butter is a handy way to receive a spoonful of nourishment during snack time. However, you are going to want to practice portion control too since the serving size is really small.
The following best seeds in the ketogenic diet include:�
Pumpkin seeds
Sesame seeds
Sunflower seeds and sunflower seed butter
Tahini (sesame seed paste)
Chia seeds
Flaxseeds
Nuts and Seeds to Avoid in the Keto Diet
Are you wondering why peanuts and peanut butter is not part of the list of ketogenic diet foods? The majority of us have grown up eating and snacking on peanut butter. But a lot of us don’t recognize that peanut butter isn’t really made out of nuts; peanuts are a legume, which is part of the exact same family as peas, soybeans, and lentils. While the macro dysfunction and low-fat level of a serving of peanuts might be like other nuts, that is where their healthy comparison stops.
Peanuts and peanut butter are:
Packed with unnecessary added sugars
Loaded with hydrogenated oils (essentially harmful trans fats)
Low in fat and filled with junk as a replacement
Hard to digest
Covered in pesticides
High in oxalates (which prevent proper nutrient absorption and can lead to kidney stones)
High in inflammatory omega-6 fatty acids
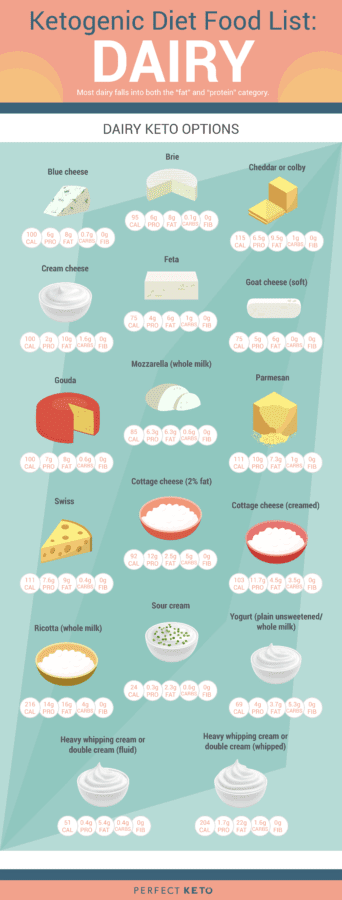
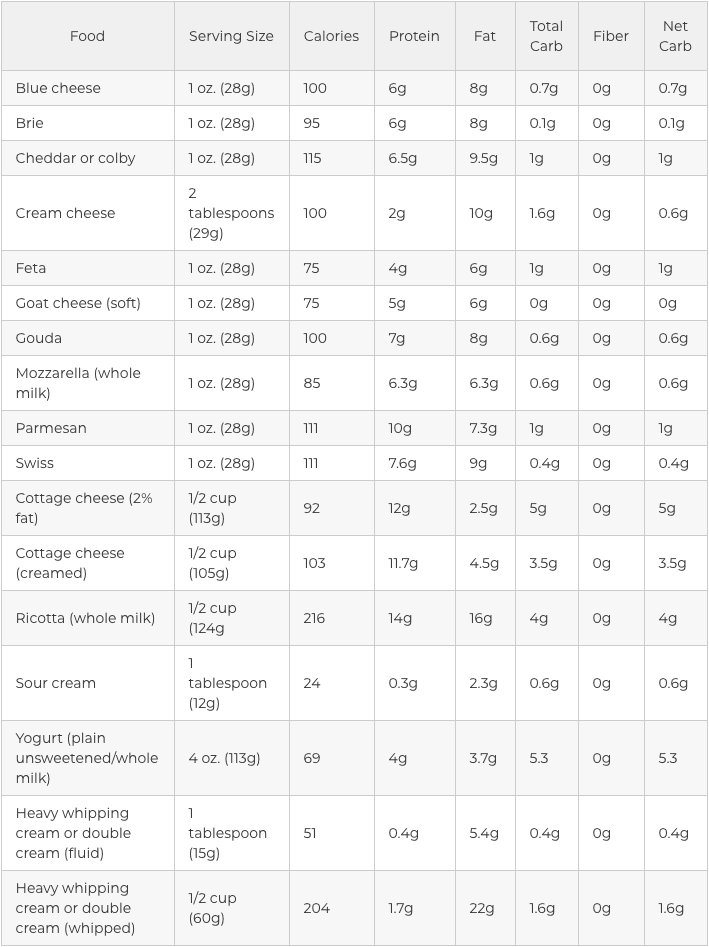
Dairy in the Ketogenic Diet
Most dairy products fit into the “fat” and “protein” category but they are accepted as part of the ketogenic diet as long as you’re not lactose intolerant. Simply make sure you eat the full-fat version and preferably choose organic and raw options, if possible. Dairy is not an extremely important element of a keto�diet. If you are lactose intolerant, you may safely omit it.
For people with dairy sensitivities:
Find hard and long-aged dairy
Use ghee, a butter alternative without the irritating milk solids
Get checked for a casein sensitivity to rule out the other common irritant found in dairy
Other dairy choices can include:
Unflavored greek yogurt, fermented yogurt, and kefir
Hard cheeses like blue cheese, gouda, and parmesan
Semi-hard cheese such as Colby, provolone, and swiss cheese
Softer cheeses like mozzarella, brie, muenster, and Monterey Jack
Cream cheese, mascarpone, creme fraiche, and cottage cheese, which are also okay on a high-fat diet
Dairy to Avoid in the Keto Diet
Very similar to healthy versus unhealthy fats, these dairy things are packed using the wrong ingredients and aren’t good if you are trying to achieve and maintain ketosis. To reach ketosis, avoid these 3 dairy products on the ketogenic diet.
Low fat, reduced fat, and fat-free milk. When fat is removed from dairy, sugar is added to fill in the gaps and make these taste much better. The sugar in these products will prevent you from going into ketosis. Whole milk is not much better, however, with 12.8 grams of carbohydrates per glass, you’re much better off enjoying low carb cheese over a glass of milk.
Half and half. Do not go with this particular half milk/half cream mix either. You are still getting a dose of sugar and less fat, two of which is not ideal for a keto diet. Reach for heavy whipping cream and you won’t hav carbohydrates or sugar to contend with.
Evaporated and condensed milk. Before incorporating these canned milk choices for your next recipe, you need to know these are essentially a cooked down variation of milk syrup and sugar in disguise. Luckily, it is simple to substitute this cooking staple with unsweetened, full-fat, canned coconut milk. Plus, as it is made from coconuts, you also receive healthy saturated fats.
Fats are ultimately essential in the ketogenic diet. Recognizing the different types of fats you can eat while on the keto diet is important in order to help you achieve and maintain ketosis. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
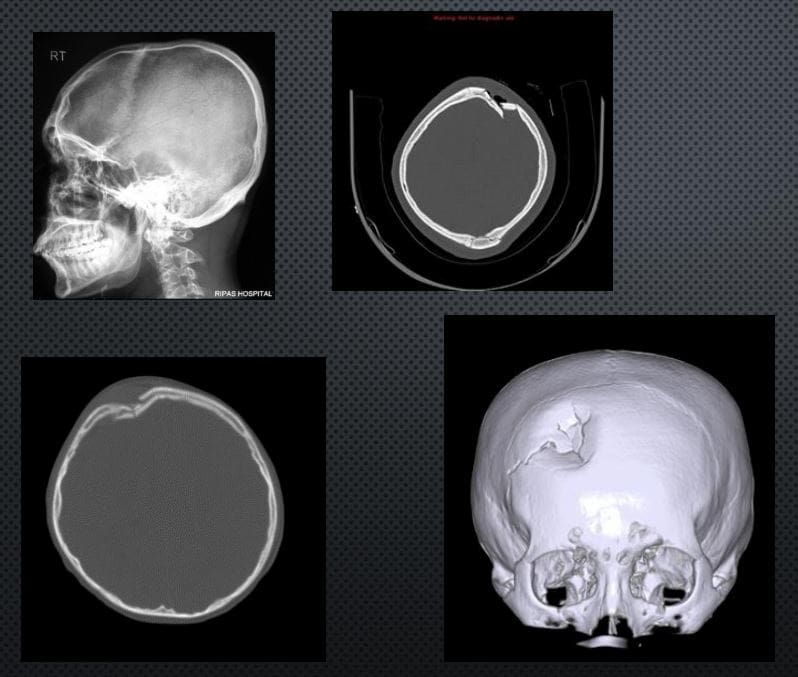
SKULL FX: COMMON IN THE SETTINGS OF HEAD INJURIES. SKULL FX OFTEN POINT TO OTHER COMPLICATING FACTORS: INTRA-CRANIALHEMORRHAGING, CLOSED TRAUMATIC BRAIN INJURY AND OTHER SERIOUS COMPLICATIONS
SKULL X-RAYS ARE VIRTUALLY OBSOLETE IN EVALUATING HEAD INJURY. CT SCANNING W/O CONTRAST IS THE MOST IMPORTANT INITIAL STEP IN EVALUATION OF ACUTE HEAD TRAUMA. MRI HASA POOR ABILITY TO REVEAL SKULL FRACTURES, AND NOT TYPICALLY USED FOR AN INITIAL DX OF ACUTE HEAD TRAUMA.
SKULL FX ARE IDENTIFIED AS FXS OF SKULL VAULT, SKULL BASE AND FACIAL SKELETON EACH ASSOCIATED WITH SPECIFIC FEATURES AND HELP TO PREDICT COMPLICATIONS.
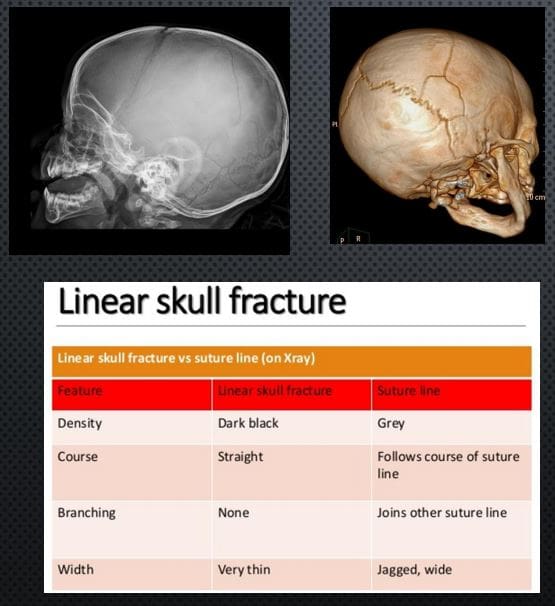
LINEAR SKULL FX: SKULL VAULT. M/C FX. CT SCANNING IS THE KEY TO EVALUATE ARTERIALEXTRADURAL HEMORRHAGING
X-RAY DDX: SUTURES VS. LINEAR SKULL FX. FX IS THINNER, �BLACKER� I.E. MORE LUCENT, CROSSESSUTURES,�AND VASCULAR GROOVES, LACKSSERRATIONS
RX: IF NO INTRACRANIAL BLEEDS THAT NO TREATMENT. NEUROSURGICAL CARE IF BLEEDSDETECTED BY CT SCANNING
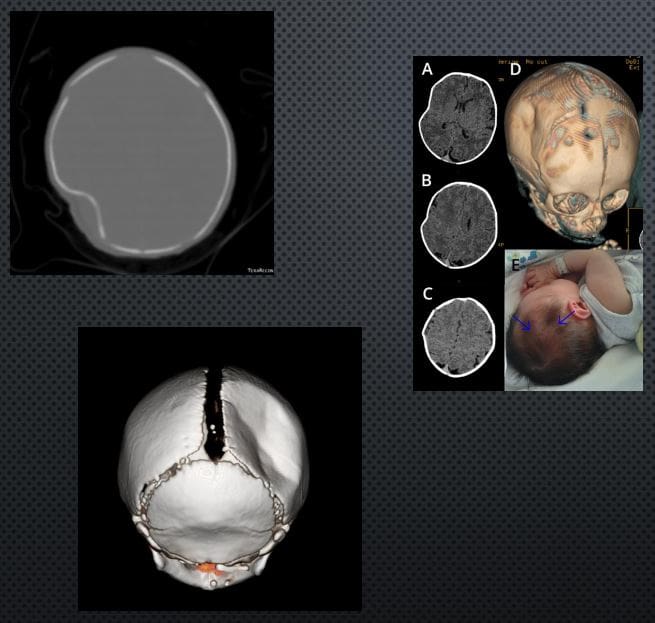
DEPRESSED SKULL FX: 75% IN THE VAULT. CAN BE DEADLY. CONSIDERED AN OPEN FX. MOST CASES NEED NEUROSURGICALEXPLORATION ESPECIALLY IFFRAGMENTS DEPRESSED >1-CM.COMPLICATIONS: VASCULAR INJURY/HEMATOMAS, PNEUMOCEPHALUS, MENINGITIS, TBI, CSF LEAK, BRAIN HERNIATION ETC.
IMAGING: CT SCANNING W/O CONTRAST
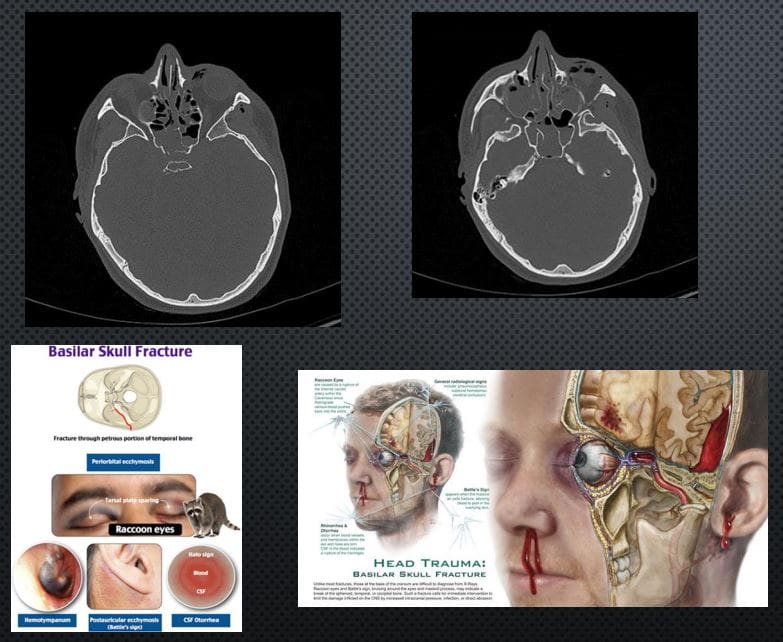
BASILAR SKULL FX: CAN BE DEADLY. OFTEN ALONG OTHER MAJOR HEAD TRAUMA OF THE VAULT AND FACIALSKELETON, OFTEN WITH TBI AND MAJORINTRACRANIAL HEMORRHAGING. OFTEN OCCUR AS �HEADBAND� EFFECT OF IMPACT AND MECHANICAL TENSION THROUGH THE OCCIPUT AND TEMPORAL BONES THROUGH SPHENOID AND OTHER BASE OF SKULL BONES. CLINICALLY: RACCOON EYES, BATTEL SIGN, CSFRHINO/OTORRHEA.
Contents
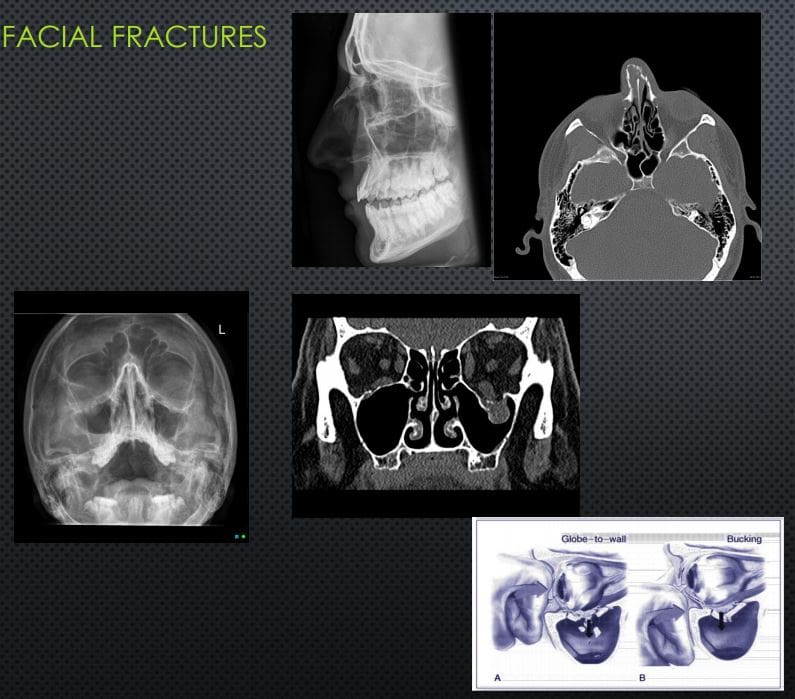
Facial Fractures
NASAL BONES FX: 45% OF ALLFACEFXM/C IMPACT IS LATERAL(FIST BLOW ETC.) IF UNDISPLACEDNO TREATMENT, IF DISPLACED MAY COMPLICATE AIR FLOW AND RESPIRATORY PASSAGE, MAY BE ASSOCIATED WITH OTHER FACIAL/SKULL INJURY. X-RAYS 80%SENSITIVE, FOLLOWED BY CT INCOMPLEX INJURIES.
ORBITAL BLOW OUT FX: COMMONORBITAL INJURY D/T IMPACT ON THE GLOBE AND/OR ORBITAL BONE. FX OF ORBITAL FLOOR INTOMAXILLARY SINUS VS. MEDIAL WALL INTO ETHMOID SINUS. COMPLICATIONS: ENTRAPPEDINFERIOR RECTUS M, PROLAPSEORBITAL FAT,�AND SOFT TISSUES, HEMORRHAGING AND OPTIC NERVE DAMAGE. RX: CONCERNS OF GLOBE INJURY ARE IMPORTANT, GENERALLY TREATEDCONSERVATIVELY IF NO COMPLICATIONS PRESENT
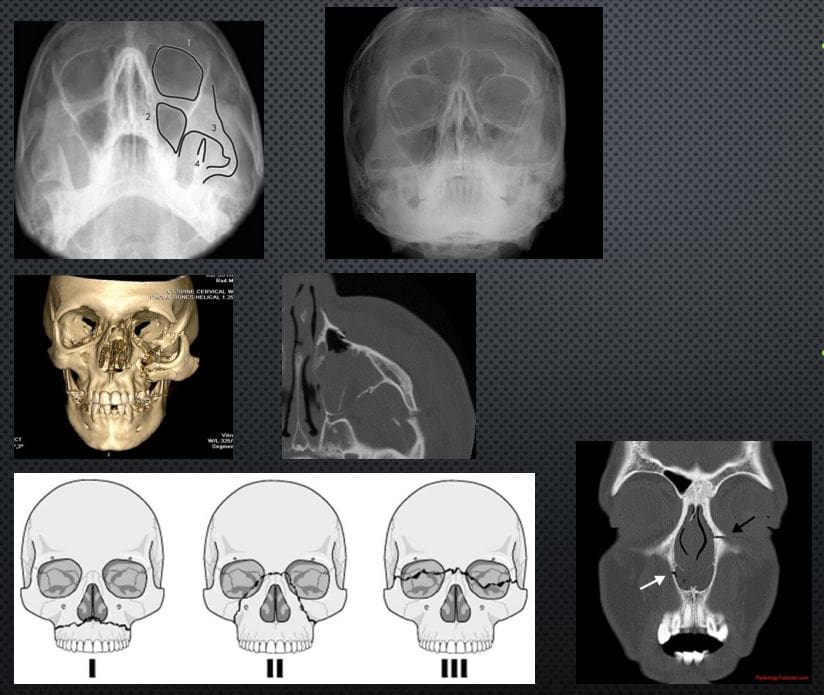
TRIPOD FX: 2ND M/C FACIAL FX#AFTER NASAL (40% OF MIDFACEFX) 3-POINT FX-ZYGOMATICARCH, ORBITAL PROCESS OF ZYGOMATIC BONE & SIDE OF MAXILLARY SINUS WALL, MAXILLARY PROCESS OF ZYGOMATIC BONE.COMPLICATED BY NERVE INJURY, TEMPORALIS M DAMAGE ETC. CT SCANNING IS MORE INFORMATIVE THAT X-RAYS (WATER�S VIEW).
LEFORT FX: SERIOUS FX ALWAYS INVOLVES PTERYGOID PLATES, POTENTIALLY SEPARATINGMIDFACE AND ALVEOLAR PROCESS WITH TEETH FROM THE SKULL. CONCERNS: AIRWAYS, HEMOSTASIS, NERVE INJURIES. CT SCANNING IS REQUIRED. POTENTIAL RISK OF BASILAR SKULL FX
PING-PONG FX:�EXCLUSIVELY IN INFANTS. AN INCOMPLETE FX D/T FOCALDEPRESSION: FORCEPS DELIVERY, DIFFICULT LABOUR ETC. FOCALTRABECULAR MICROFRACTURIINGLEAVING DEPRESSION RESEMBLING APING-PONG. DX IS MAINLY CLINICALSEEN AS FOCAL DEFECT �DEPRESSION� IN THE SKULL. TYPICALLYNEUROLOGICALLY INTACT. CT MAY HELP IF BRAIN INJURY IS SUSPECTED. RX: OBSERVATIONAL VS. SURGICAL IN COMPLICATED INJURIES. SPONTANEOUSREMODELING HAS BEEN REPORTED
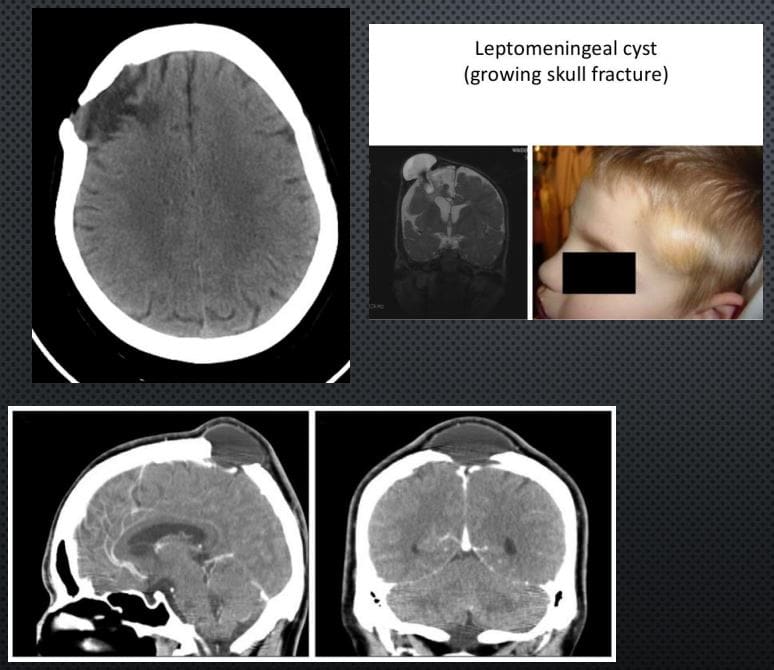
LEPTOMENINGEAL CYST (GROWING SKULL FX)- ARE AN ENLARGING SKULL FRACTURE THAT DEVELOPS ADJACENT TO POSTTRAUMATIC ENCEPHALOMALACIA
IT IS NOT A CYST, BUT AN EXTENSION OF THEENCEPHALOMALACIA THAT SEEN A FEW MONTHS POST-TRAUMA WITH PREVIOUS SKULL FX FOLLOWEDBY HERNIATION OF THE MENINGES AND ADJACENTBRAIN WITH PULSATIONS OF THE CSF. CT IS BEST ATDX THIS PATHOLOGY. INDICATES: GROWING FX AND ADJACENT ENCEPHALOMALACIA AS FOCALHYPOATTENUATING LESION.
DDX: INFILTRATING CELLS/METS/OTHER NEOPLASMSINTO SUTURES, EG, INFECTION ETC.
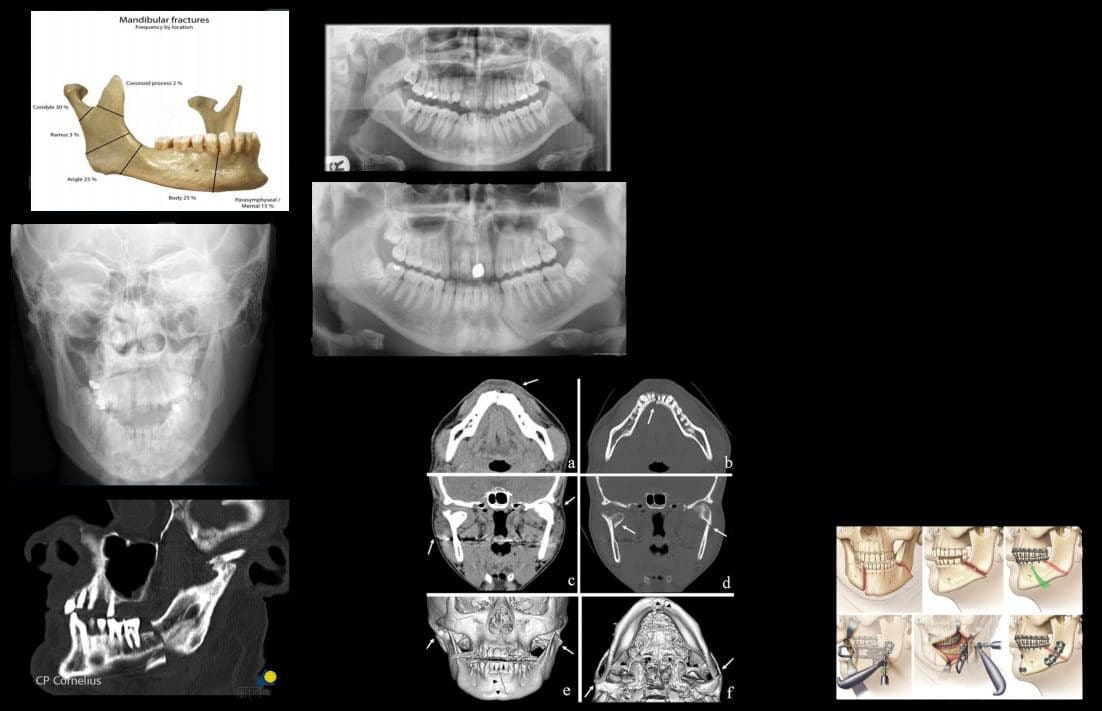
MANDIBULAR FXS: COMMON. POTENTIALLYCONSIDERED AN OPEN FX D/T INTRA-ORALEXTENSION. 40% FOCAL BREAK DESPITEMANDIBLE BEING A RING. DIRECT IMPACT(ASSAULT) M/C MECHANISM
PATHOLOGICAL FX D/T BONE NEOPLASMS, INFECTION ETC. IATROGENIC DURING ORAL SURGERY (TOOTH EXTRACTION)
IMAGING: MANDIBLE X-RAYS, PANOREX, CT SCANNING ESP. IN CASES OF ASSOCIATEDFACE/HEAD TRAUMA
COMPLICATIONS: AIRWAY OBSTRUCTION, HEMOSTASIS IS A MAJOR CONSIDERATION, DAMAGE TO MANDIBULAR N, OSTEOMYELITIS/CELLULITIS AND POTENTIAL SPREAD THROUGH FLOOR OF THE MOUTH (LUDWIGANGINA) AND NECK FASCIAL SOFT TISSUES INTOMEDIASTINUM. CANNOT BE NEGLECTED D/T HIGH MORTALITY RATES.
RX: CONSERVATIVE VS. OPERATIVE
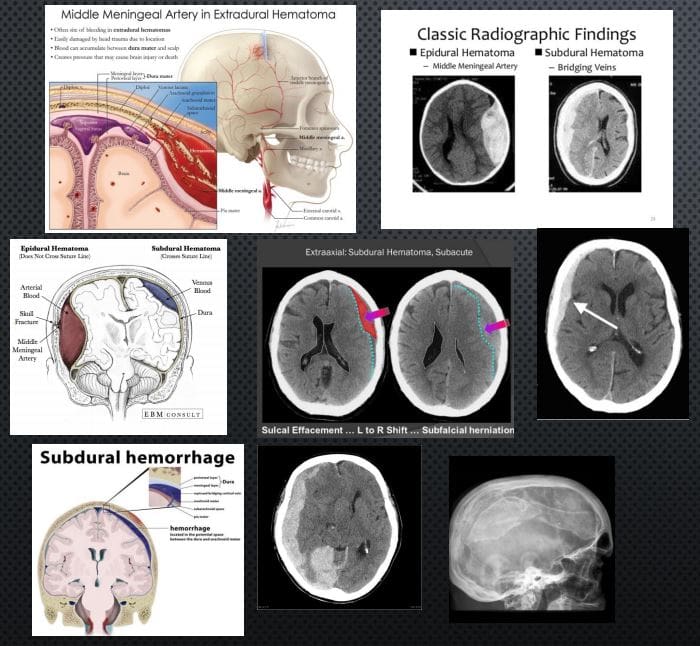
Acute Intracranial Hemorrhage
EPI AKA EXTRADURAL: (EDH) TRAUMATIC RAPTURE OF MENINGEAL ARTERIES (MMA CLASSIC) WITH RAPIDLY FORMING HEMATOMA BETWEEN THE INNER SKULL AND OUTER DURA. CT SCANNING IS THE KEY TO DX: PRESENTS AS �LENTIFORM� I.E. BICONVEX COLLECTION OF ACUTE (HYPERDENSE) BLOOD THAT DOES NOT CROSSSUTURES AND HELPS WITH DDX OF A SUBDURAL HEMATOMA. CLINICALLY: HA, LUCID EPISODE INITIALLY AND DETERIORATING IN A FEW HOURS.COMPLICATIONS: BRAIN HERNIATION, CN PALSY. O/A GOOD PROGNOSIS IF QUICKLY EVACUATED.
SUBDURAL HEMATOMA (SDH): RAPTURE OF BRIDGINGVEINS BETWEEN INNER DURA AND THE ARACHNOID.SLOW BUT PROGRESSIVE BLEED. MAY PARTICULARLYAFFECT THE VERY YOUNG AND ELDERLY AND IN ALL AGES (MVA, FALLS ETC.) MAY DEVELOP IN �SHAKEN BABY SYNDROME�. DX MAY BE DELAYED AND WORSEN THE PROGNOSIS WITH HIGH FATALITIES. IN ELDERLY HEAD TRAUMA MAY BE MINOR OR NOT RECALLED. EARLYIMAGING WITH CT IS CRUCIAL. PRESENTS AS CRESCENTSHAPEDCOLLECTION THAT CAN CROSS SUTURES BUT STOPPED AT DURAL REFLECTIONS. DIFFERENTATTENUATION ON CT D/T DIFFERENT STAGES OF BLOODDECOMPOSITION: ACUTE, SUBACUTE,�AND CHRONIC.MAY FORM A CHRONIC COLLECTION-CYSTICHYGROMA. CLINICALLY: VARIABLE PRESENTATION, 45-60% PRESENT WITH SEVERELY DEPRESSED CNS STATUS, PUPILLARY INEQUALITY. OFTEN WITH INITIAL BRAIN CONTUSION, THEN A LUCID EPISODE BEFORE SEVERELYDETERIORATING. IN 30% CASES OF FATAL BRAIN INJURY PATIENTS HAD SDH. RX: URGENT NEUROSURGICAL.
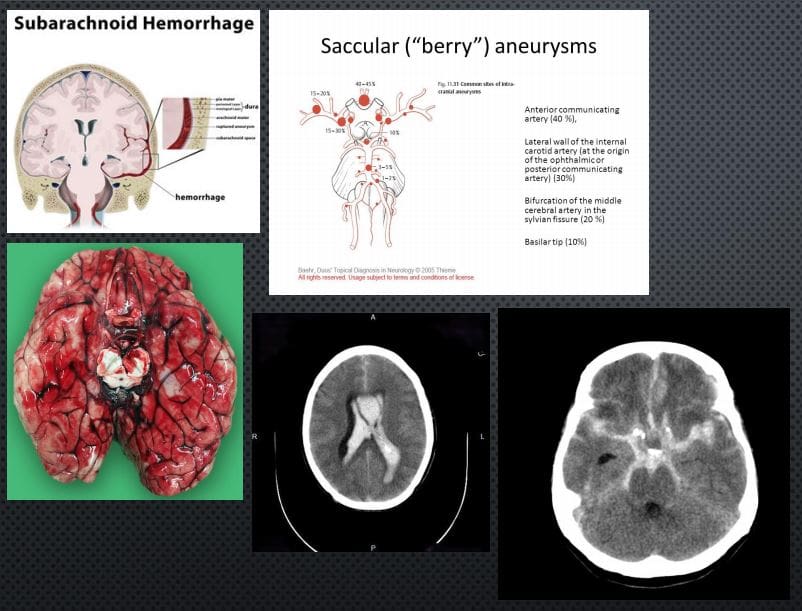
SUBARACHNOID HEMORRHAGE (SAH): BLOOD IN THE SUB-ARACHNOID SPACE AS THE RESULT OF TRAUMATIC OR NON-TRAUMATIC ETIOLOGY: BERRY ANEURYSMS AROUND CIRCLE OF WILLIS.SAH 3% OF STROKES, 5% OF FETAL STROKES.CLINICALLY: PRESENTS AS A �THUNDERCLAP HEADACHE� DESCRIBED AS A �WORST HA INLIFE�. PT COLLAPSES MAY OR MAY NOT REGAIN CONSCIOUSNESS. PATHOGY: DIFFUSE BLOOD INSA SPACE 1)SUPRASELLAR CISTERN WITH DIFFUSE PERIPHERAL EXTENSION, 2)�PERIMESENCEPHALIC, 3) BASAL CISTERNS. BLOOD LEAKED INTO SA SPACE UNDERARTERIAL PRESSURE INDUCES GLOBAL INCREASE IN INTRACRANIAL PRESSURE, ACUTE GLOBAL ISCHEMIA WORSENED BY VASOSPASM AND OTHER CHANGES.
DX: IMAGING: URGENT CT SCANNING W/O CONTRAST, CT ANGIOGRAPHY MAY HELP TO RULE OUT 99% OF SAH. LUMBAR PUNCTUREMAY HELP IN DELAYED PRESENTATION. AFTER INITIAL DX: MR ANGIOGRAPHY HELPS TO FIND THE CAUSE AND OTHER IMPORTANT FEATURES
IMAGING FEATURES: ACUTE BLOOD IS HYPERDENSE ON CT. FOUND IN DIFFERENTCYSTERNS: PERIMESENCEPHALIC, SUPRASELLA, BASAL, VENTRICLES,
RX: INTRAVENOUS ANTIHYPERTENSIVE MEDS, OSMOTIC AGENTS (MANNITOL) TO DECREASEICP. NEUROSURGICAL CLIPPING AND OTHER APPROACHES.
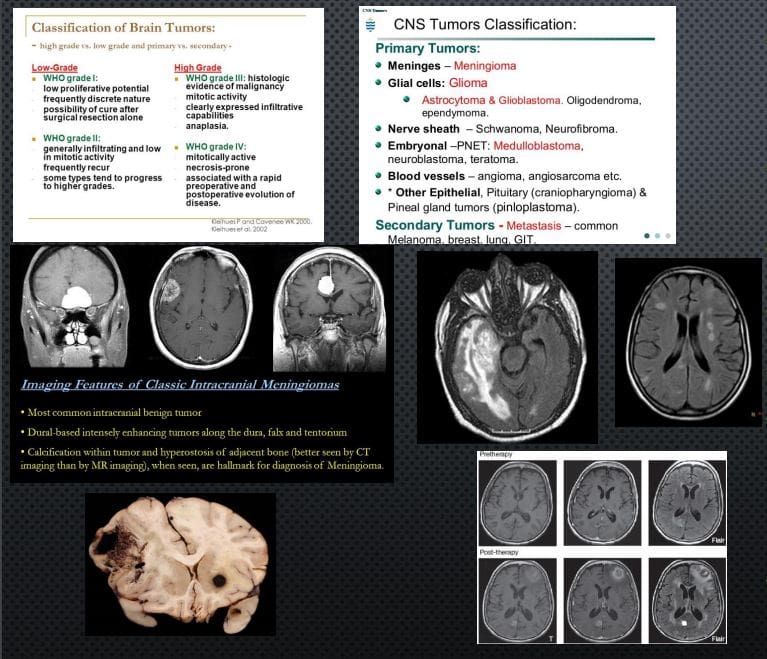
CNS Neoplasms: Benign vs. Malignant
BRAIN TUMORS REPRESENT 2% OF ALL CANCERS. ONE THIRD ARE MALIGNANT, OF WHICH METASTATIC BRAIN LESIONS ARE THE MOST COMMON
CLINICALLY PRESENT WITH LOCAL CNS ABNORMALITIES, INCREASED ICP, INTRACEREBRAL BLEEDING ETC. FAMILIALSYNDROMES: VON-HIPPEL-LANDAU, TUBEROUS SCLEROSIS, TURCOT SYNDROME, NF1 & NF2 INCREASE THE RISK. IN CHILDREN: M/C ASTROCYTOMAS, EPENDYMOMAS, PNETNEOPLASMS (E.G. MEDULLOBLASTOMA) ETC. DX: BASED ON WHO CLASSIFICATION.
IMAGING IS CRUCIAL: INITIAL SYMPTOMS MAY PRESENT AS SEIZURE, ICP SIGNS HA. EVALUATED BY CT AND MRI WITH IV GADOLINIUM.
IMAGING DETERMINES: INTRA-AXIAL VS. EXTRA-AXIALNEOPLASMS. METS FROM PRIMARY BRAIN NEOPLASMS MAYO CCUR VIA CSF AND LOCAL VESSELS INVASION
NOTE AXIAL CT SLICE OF MENINGIOMA WITH AVIDCONTRAST ENHANCEMENT.
AXIAL MRI ON FLAIR PULSE SEQUENCE REVEALED EXTENSIVE NEOPLASM AND MARKED CYTOTOXIC EDEMA OF THE BRAIN PARENCHYMA CHARACTERISTIC OF GRADE IV GLIOMA (GBM) WITH VERY POOR PROGNOSIS. ABOVE FAR RIGHT IMAGE: AXIAL MRI FLAIR: BRAIN METASTASIS FROM BREAST CANCER. MELANOMA IS COMMONLY METASTASIZESTO THE BRAIN (SEE PATH SPECIMEN) MRI CAN BE DIAGNOSTIC D/T HIGH SIGNAL ON T1 AND CONTRAST ENHANCEMENT.
RX: NEUROSURGICAL, RADIATION, CHEMOTHERAPY,�IMMUNOTHERAPY TECHNIQUES ARE EMERGING
Fats are an essential�part of the ketogenic diet since they constitute approximately 70 percent of your dietary calories. However, the type of fat you eat on the ketogenic diet is also important and there may be some confusion regarding good fats and bad fats. The following article discusses exactly what fats you need to include and what fats you must avoid while on the keto diet.
Contents
Good Fats on the Ketogenic Diet
The type of “good” fats included while on the ketogenic diet are divided into four groups: saturated fats, monounsaturated fats (MUFAs), polyunsaturated fats (PUFAs), and naturally-occurring trans fats. All fats can be classified into more than one group, however, we classify them according to the most dominant of these mixtures. It’s essential to be able to recognize what type of fat you are eating on the ketogenic diet. Below, we will describe each group of good fat so you can properly implement them into your own food choices.
Saturated Fats
For many years, saturated fats were considered to be detrimental for heart health and we were advised to�limit their�consumption as much as possible. However, recent research studies have demonstrated no substantial connection between saturated fats and the increased risk of cardiovascular disease. As a matter of fact, including healthy saturated fats into your diet can have many benefits.
One type of saturated fat contains medium-chain triglycerides (MCTs), which can be largely found in coconut oil, or in small quantities in butter and palm oil, and it may be digested quite easily by the human body. Medium-chain triglycerides pass through the liver for immediate use as energy when consumed. MCTs are beneficial towards promoting weight loss and improving athletic performance.
Health benefits of saturated fats on the keto diet can include:
Improved HDL and LDL cholesterol levels
Maintenance of bone density
Boosting of immune system health
Support in creation of important hormones like cortisol and testosterone
Raising of HDL (good) cholesterol in the blood to prevent buildup of LDL in the arteries
Improved HDL to LDL ratio
Recommended types of saturated fats while on the ketogenic diet include:
Butter
Red meat
Cream
Lard
Coconut oil
Eggs
Palm oil
Cocoa butter
Monounsaturated Fats
Unlike saturated fats, monounsaturated fats, also referred to as monounsaturated fatty acids or MUFAs,�have been approved as a healthy source of fat for several years. A variety of research studies have connected them to numerous health benefits associated with improved levels of “good” cholesterol and better insulin resistance, among other health benefits, as described below.
Health benefits of MUFAs on the keto diet can include:
Increased HDL cholesterol
Lowered blood pressure
Lowered risk for heart disease
Reduced belly fat
Reduced insulin resistance
Recommended types of MUFAs while on the ketogenic diet include:
Extra virgin olive oil
Avocados and avocado oil
Macadamia nut oil
Goose fat
Lard and bacon fat
Healthy Polyunsaturated Fats
The most important point to keep in mind about eating polyunsaturated fats, also referred to as polyunsaturated fatty acids or PUFAs, on the ketogenic diet is that the specific type you consume actually matters. When heated, some polyunsaturated fats may produce substances that can cause inflammation in the human body, increasing the risk of cardiovascular disease and even cancer.
Many PUFAs must be consumed cold and they should never be utilized for cooking. PUFAs can be found both in very processed oils and in very healthy sources. The right types can additionally provide many health benefits on the ketogenic diet, particularly because several of these include omega 3s and omega 6s, both of which are essential nutrients in a healthy and balanced diet.
Health benefits of PUFAs on the keto diet can include:
Reduced risk of heart disease
Reduced risk of stroke
Lowered risk of autoimmune disorders and other inflammatory diseases
Improved symptoms of depression
Improved symptoms of ADHD
Recommended types of PUFAs while on the ketogenic diet include:
Extra virgin olive oil
Flaxseeds and flaxseed oil
Walnuts
Fatty fish and fish oil
Sesame oil
Chia seeds
Nut oils
Avocado oil
Naturally-Occurring Trans Fats
Many people might be confused to see trans fats classified as “good” fats. While most trans fats are considered to be extremely unhealthy and even harmful, one type of trans fat, known as vaccenic acid, can be found naturally in various kinds of food, such as in grass-fed animal products and dairy fats. These naturally-occurring trans fats also provide several health benefits on the keto diet.
Health benefits of naturally-occurring trans fats on the keto diet include:
Reduced risk of heart disease
Reduced risk of diabetes and obesity
Possible protection against cancer risk
Recommended types of naturally-occurring trans fats while on the ketogenic diet include:
Grass-fed animal products
Dairy fats like butter and yogurt
When following a ketogenic diet, or any other low carb diet, eating the right type of fat is essential, especially since these make up about 70 percent of your daily caloric intake. The type of fat you eat is classified into various groups depending on the dominant amount found in the mixture. Extra Virgin Olive Oil, for example, is approximately 73 percent monounsaturated fat, therefore, it is considered a monounsaturated fat. Butter is about 65 percent saturated fat and thus, is a saturated fat.�It’s essential to be able to recognize what type of fat you are eating on the ketogenic diet in order to enjoy its health benefits. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Bad Fats on the Ketogenic Diet
One of the greatest advantages of the ketogenic diet is the capacity to eat lots of satisfying dietary fats such as those mentioned previously. However, we have to also cover the kinds of fats that you should reduce or eliminate from your diet in order to prevent damaging your�well-being. On the keto diet, the quality of food you eat is especially important to achieve ketosis.
Unhealthy Polyunsaturated Fats and Processed Trans Fats
Processed trans fats are the group of fat which most people as the “bad” fats and the truth is, they can actually be quite damaging to your overall health and wellness.� Artificial trans fats are made during food production via the processing of polyunsaturated fats. That is the reason why it’s very important to choose PUFAs which are unprocessed and not overheated or modified. The consumption of unhealthy PUFAs can create harmful free radicals where processed trans fats often contain genetically modified seeds.
Health risks of unhealthy polyunsaturated fats and processed trans fats include:
Increased risk of heart disease
Increased risk of cancer
Reduced HDL cholesterol and increased LDL cholesterol
Pro-inflammatory
Bad for the health of your gut
Examples of unhealthy polyunsaturated fats and processed trans fats to avoid include:
Hydrogenated and partially hydrogenated oils found in processed products like cookies, crackers, margarine, and fast food
Processed vegetable oils like cottonseed, sunflower, safflower, soybean, and canola oils
In conclusion, it’s essential to recognize what type of fat you are eating while on the ketogenic diet. In the end, the function of the ketogenic diet will always be to enhance your health, which includes eating the appropriate amount of fat, protein, and carbohydrate ratio as well as picking food resources which promote health and wellness. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
A baker�s cyst can cause pain, swelling, and limit the mobility in the affected knee. In some cases, complications can develop, causing severe problems with the leg. The problem with this type of cyst is that even if it is drained�if the underlying cause isn�t addressed, the cyst can return. Chiropractic can be used to treat baker�s cyst and help relieve the pain that it causes.
Contents
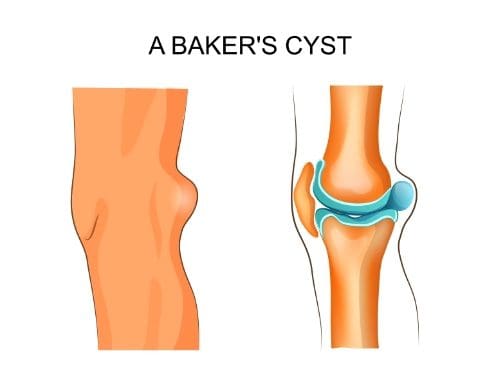
What is a Baker�s Cyst?
A Baker�s cyst, also known as a popliteal cyst, is a fluid-filled lump behind the knee. Synovial fluid builds up to form the benign cyst. It starts inside the knee but eventually extruded through the back part of the knee and forms a lump. Many times there is no discomfort or pain from the cyst, although there may be some pressure on the back side of the knee. The pain that is often associated with a Baker�s cyst is usually caused by the underlying problem that causes it. In some cases, a Baker�s cyst can become large enough to inhibit movement which can impact mobility.
What Causes a Baker�s Cyst?
A Baker�s cyst is caused by overproduction of synovial fluid in the knee that leads to the fluid building up and forming a lump. There are several reasons that this can happen, including knee joint inflammation and injury to the knee. A meniscal cartilage tear or another cartilage injury of the knee can cause a cyst to develop. Certain types of arthritis in the knee, such as osteoarthritis and rheumatoid arthritis can cause the excess fluid to accumulate. Knee arthritis, a common condition among older adults, can also cause the development of a Baker�s cyst.
What are the Potential Complications of Baker�s Cyst?
Sometimes the location or size of a Baker�s cyst can cause swelling in the back of the knee. The cyst itself can be as large as a golf ball. This can put pressure on the joint, making it difficult to bend the knee. This pressure can extend through the calf muscle. The patient may experience tenderness and pain after exercising.
In rare cases, a Baker�s cyst can burst, causing the synovial fluid to leak into the calf. This can cause swelling and knee pain that is sharp and can be intense. The patient may notice redness in the calf or experience the sensation of water running down the back of the calf area. Because symptoms of a burst Baker�s cyst can closely resemble a blood clot in the leg, the patient should seek immediate medical attention to rule out a more severe condition.
How is a Baker�s Cyst Treated?
Some no treatment for popliteal cysts and they go away on their own. If a form of arthritis is causing the cyst, treating that problem may resolve the cyst. The same goes for a cyst caused by an injury to the knee. Once the damage is fixed, the cyst typically resolves as well.
If the cyst does not go away or if it is problematic, causing intense pain or limits mobility, the patient may talk to their doctor about getting it drained. The doctor will use a needle, insert it directly into the cyst and drain the fluid. Steroid medications may also be prescribed to reduce inflammation and swelling. In sporadic cases, surgery may be required to remove the cyst.
Chiropractic for Baker�s Cyst
Many patients choose to seek chiropractic care to treat a Baker�s cyst because it is noninvasive and does not use medications that can have unpleasant or harmful side effects. The chiropractor will assess the cyst and conduct diagnostic tests to determine the cause. This will help them decide the best course of treatment. Sometimes an old injury can continue to put stress on the joint, causing a lingering tension pattern. A chiropractor can address this, bringing the body back into alignment, thus alleviating the problem. This will help reduce the pain, inflammation, and swelling. Chiropractic is also an effective treatment for arthritis so if that is the cause of the cyst; regular chiropractic care can help considerably. Often, once the underlying condition is corrected, the cyst goes away on its own.
Once back pain begins to affect an individual’s well-being, Dr. Alex Jimenez helps treat the source of the health problem to relieve the individual’s symptoms. In a work environment, painful symptoms can severely restrict the quality of work of an individual. Chiropractic care can help treat a variety of health issues associated with symptoms of back pain by using spinal adjustments and manipulations. By carefully adjusting the alignment of the spine, Dr. Alex Jimenez can help alleviate a patient’s back pain and other spinal problems. The patients highly recommend Dr. Alex Jimenez and his team as the non-surgical choice for back pain, among other health issues.
Chiropractic
�
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Ketones serve as a source of energy for the mitochondria found inside the cells of the human body. These are an alternative fuel to sugar. Ketones are basic substances with a simple molecular structure. Ketones are natural,�or carbon-based, chemicals made up of a central carbon atom double-bonded into an oxygen atom and two carbon-containing substituents, denoted by”R”.
Genetic Ketone Structure
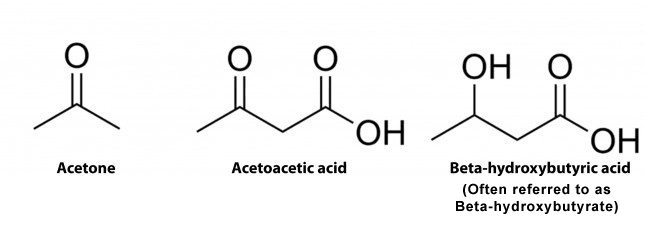
In humans, there are 3 distinct ketones created by the mitochondria. These are referred to as ketone bodies. The 3 ketones are:
Acetone
Acetoacetate, also known as Acetoacetic Acid
Beta-Hydroxybutyric Acid, also known as Beta Hydroxybutyrate or BHB. Additional compound names include 3-hydroxybutyric acid or 3-hydroxybutyrate.
BHB isn’t particularly considered a ketone because it comprises a reactive OH-group rather than a double-bonded oxygen which would generally function as demonstrated in the diagram below. However, BHB continues to function much like a ketone because it transforms into energy, such as acetone and acetoacetate. The following is demonstrated in the diagram below.
Structures of Ketone Bodies
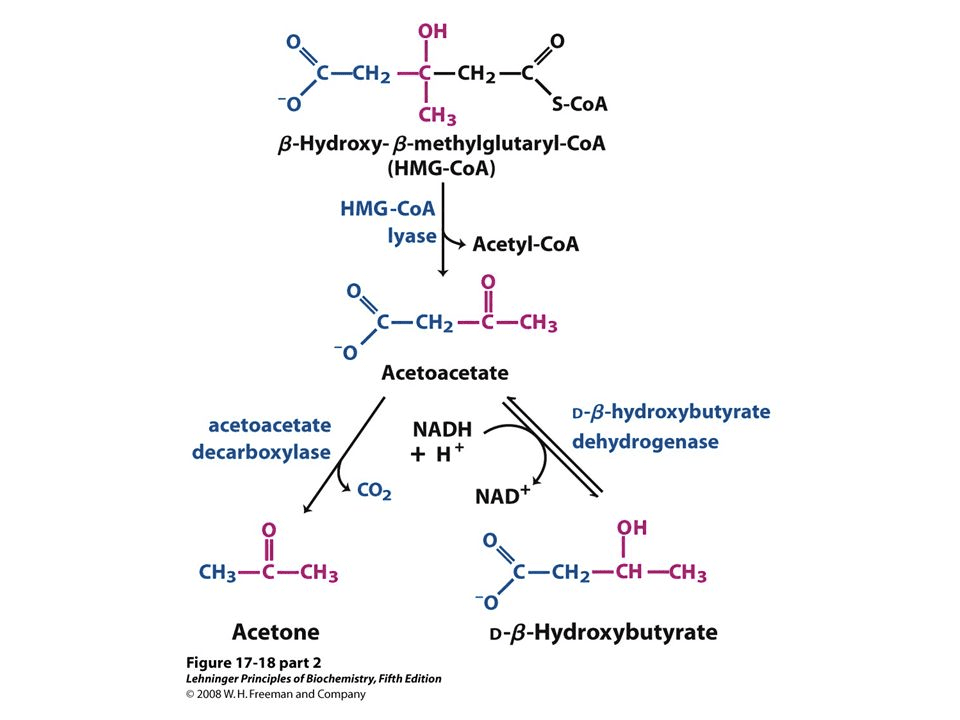
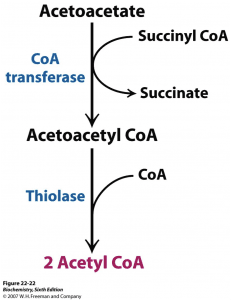
Ketogenesis is the metabolism of fatty acids through ?-oxidation. This procedure provides acetyl CoA which converts to ?-hydroxy-?-methyglutaryl-CoA, or HMG-CoA, as shown below. HMG-CoA turns into Acetoacetone which may change back-and-forth to BHB. The conversion of Acetoacetate into Acetone is irreversible (as seen on the bottom left). Acetoacetate and BHB, through acetoacetate, are utilized to make energy when converted into acetyl-CoA in the cell’s mitochondria whilst Acetone is excreted in the breath and urine.
Formation of Ketone Bodies from Acetyl-CoA2
Contents
Understanding Exogenous Ketone Bodies
Exogenous ketone bodies are simply ketone bodies which are consumed via a nutritional supplement. Ketone bodies created in the liver are more correctly referred to as endogenous ketone bodies. The following is described below.
Most nutritional supplements depend�on BHB as the origin of the exogenous ketone bodies. BHB transforms into acetoacetic acid where a small amount is turned into acetone via an acetoacetate decarboxylase waste pathway. A percentage of that acetoacetic acid may enter the energy pathway utilizing beta-ketothialase, which transforms acetoacetic acid into 2 Acetyl-CoA molecules.
Ketosis Pathway Before Entering the Krebs (Energy) Pathway
The Acetyl-CoA will then enter the Krebs cycle and creates ATP. Exogenous ketone body nutritional supplements provide an instantaneous supply of ketones to consumers. Even when you’re not in the state of ketosis before eating, such as when ingesting a higher-carb diet. These also increase blood ketones even in the presence of insulin, which inhibits ketogenesis.
Researchers do not completely comprehend what the long-term ramifications of combining a non-ketogenic diet with exogenous ketone bodies nutritional supplements really are. Research studies are at their first phases and much more information is required. A standard issue involves why BHB is the ketone body to receive exogenous ketone nutritional supplements. The explanation is a mixture in the simplicity of its formula and its conversion to energy. it is simpler to devise BHB into a nutritional supplement.
Are “Raspberry Ketones” Similar to “Ketone Bodies”?
Raspberry ketones are a�common ingredient used in weight-loss nutritional supplements. However, despite their title, they don’t have any connection. This has generated some confusion for individuals considering ketone nutritional supplements that are exogenous.
Raspberry ketones are in reality phenolic compounds that provide raspberries their pleasant odor. They are similar to the stimulant synephrine. Regardless of the research studies, raspberry ketones don’t seem to have much impact on weight loss.
Ketone Salts vs. Ketone Esters
Exogenous ketones of all beta-hydroxybutyrate can be found in two kinds:
Ketone Salts are naturally-derived chemicals which blend sodium as well as potassium and/or calcium with BHB to boost absorption. Commercially available nutritional supplements are all created from ketone salts now (contains KetoForce, KetoCaNa and Keto OS). These are also occasionally called “Ketone Mineral Salts” or “BHB Mineral Salts”.
Ketone Esters are Synthetically-made chemicals that connect an alcohol to a ketone body, where this can be metabolized in the liver as a ketone. Ketone esters are used primarily in search for testing their effectiveness on improving ketone body levels. Below is a standard arrangement of a BHB ester. The very first Ketone Ester beverage is currently accessible by HVMN. Research esters are very unpleasant tasting, something which HVMN expects to modify soon.
Structure of a Beta-Hydroxybutyrate Ester
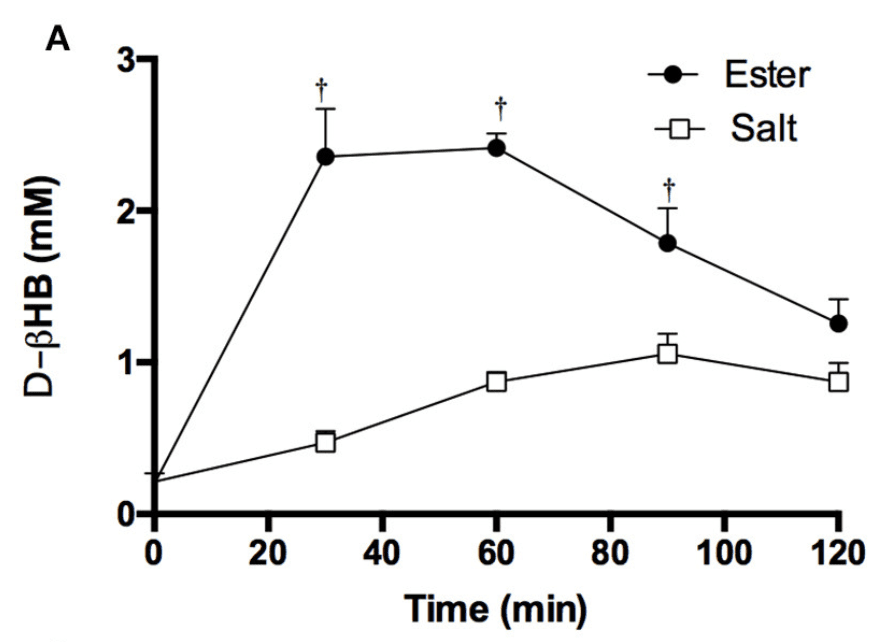
Ketone Esters increase blood levels of beta-hydroxybutyrate to greater levels compared to Ketone Salts. There’s strong evidence supporting that esters are more powerful than Ketone Salts, so much as their advantages proceed. It’s not apparent why this occurs, but it might be from the gastrointestinal, or GI, tract due to a gap in the absorption rate.
However, esters are normally somewhat tougher to endure because of gut distress after intake and they do not have the most agreeable taste, as stated previously in the article. Figure 1 below demonstrates the difference between eating equivalent quantities of BHB in the kind of a Ketone ester and Ketone salts on bloo BHB. The supplements contained are:
BMS (Beta-hydroxybutyrate Mineral Salt) — sodium/ potassium established (KetoForce)
KE (Ketone Ester) — (R- 3-hydroxybutyl-R-1,3-hydroxybutyrate) (HVMN)
Figure 1: Blood BHB level after consuming a ketone ester vs a ketone salt drink.
What are the Benefits of Exogenous Ketones?
Exogenous ketone nutritional supplements can offer a great number of benefits. These include more effective weight reduction, athletic performance improvement, cancer prevention, cognitive advancement,�and anti-inflammatory properties.
Weight Loss Goals
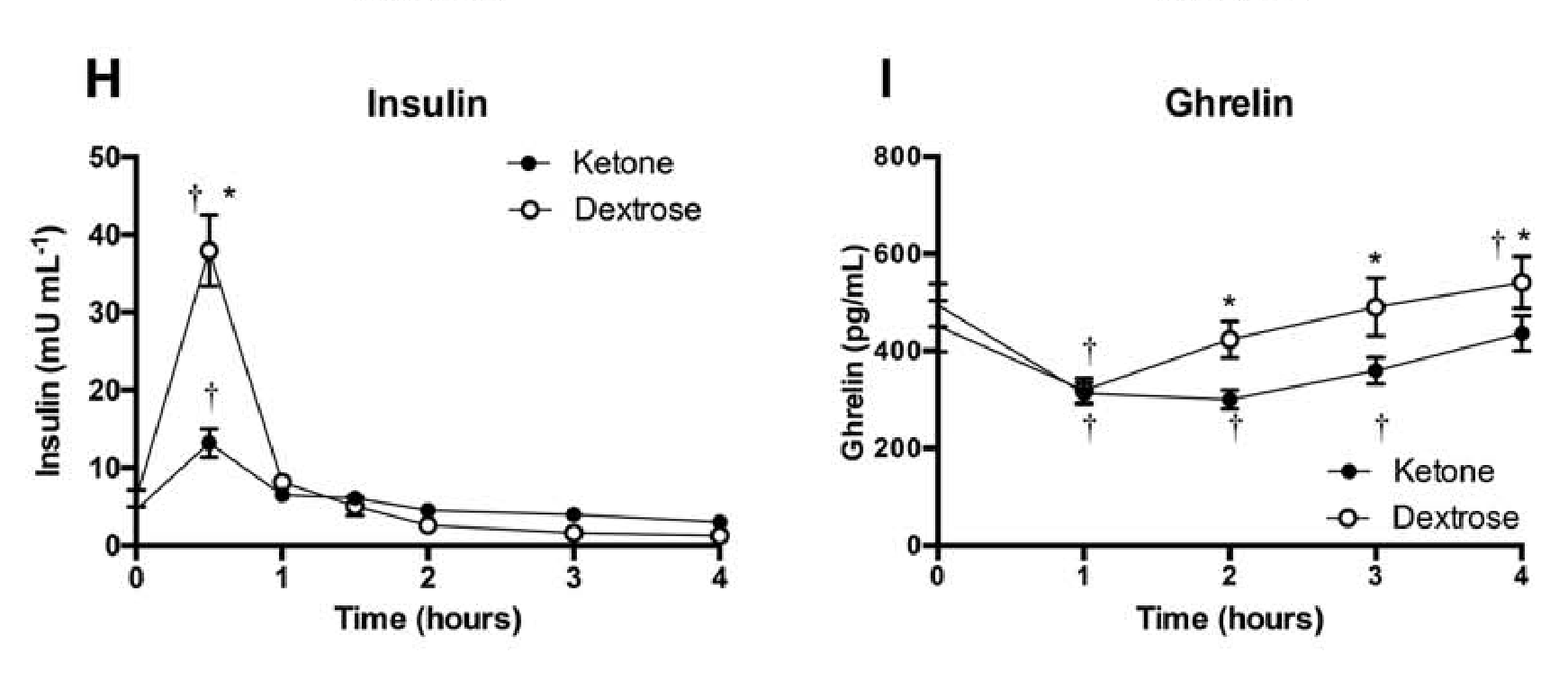
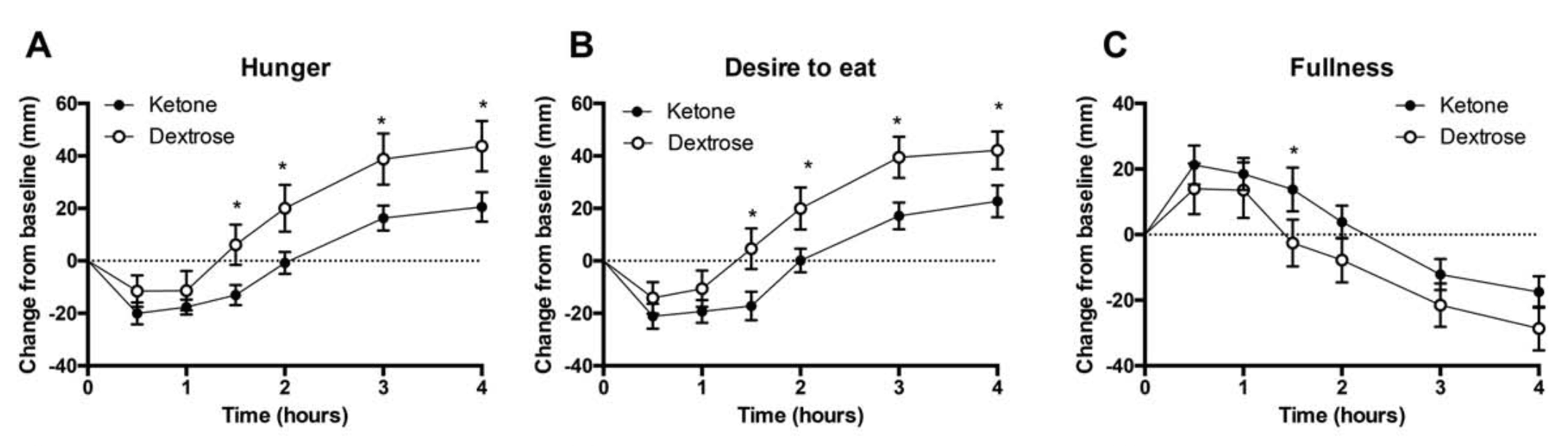
Appetite suppression: Appetite was quantified in 10 males and 5 females after taking a ketone ester, abbreviated as KE, or a dextrose, abbreviated as DEXT, beverage. The wish to consume and perception of appetite dropped after both supplements, however, the KE was 50 percent more successful for 1.5 to 4 hours. Insulin levels rose with both supplements but were 3 times lower with the KE beverage after 30 minutes, according to Figure 2. The desire hormone, ghrelin, was considerably lower between 2 to 4 hours after ingesting the KE, as seen on Figure 2. Ketone esters lower the urge and delays appetite.
Figure 2: Perceived hunger, fullness, and satiety after consuming a dextrose or ketone ester drink over time. Effects of ketone ester or dextrose drink on plasma insulin and ghrelin levels over time.
Extra ketones: In case someone has an inordinate number of ketones in the bloodstream, the human body, especially the kidneys, will function as swiftly as possible to filter out ketones via urine instead of converting them into adipose tissue. This isn’t to say you can not gain fat with�exogenous ketones, however, they are not as inclined to be converted into fat than other nourishment.
More tolerable compared to MCT oil: MCT oil was known to cause gastrointestinal distress in consumers, particularly when taken in high quantities. Exogenous ketones as ketone salts are well-tolerated. They prevent adverse GI events while supplying similar kinds of benefits. Figure 2 demonstrates how Ketone esters may be capable of reducing hunger. A combo of exogenous ketones and MCT oil can help with weight loss and permit a loading of nutritional supplements, with no GI distress.
Athletic Performance Goals
Athletic enhancem: The development of energy and�fuel pairing mechanisms. Exogenous ketone supplementation may boost these components of athletic performance. There’s a promising prognosis in this area for many different motives:
Exogenous ketones induce severe ketosis, lasting for many hours. This is without having to possess depleted muscle glycogen stores. Low muscle nourishment is well-known to inhibit sustained physical functionality.
The “carb-sparing” impact from BHB inhibits the breakdown of muscle glycogen. This contributes to reduced lactate levels. When raising exercise intensity, fat oxidation, or burning, reaches a limit. Carbohydrates are then burned�for energy.�But when swallowing Ketone esters, the body doesn’t make this change. This implies ketones are used instead.
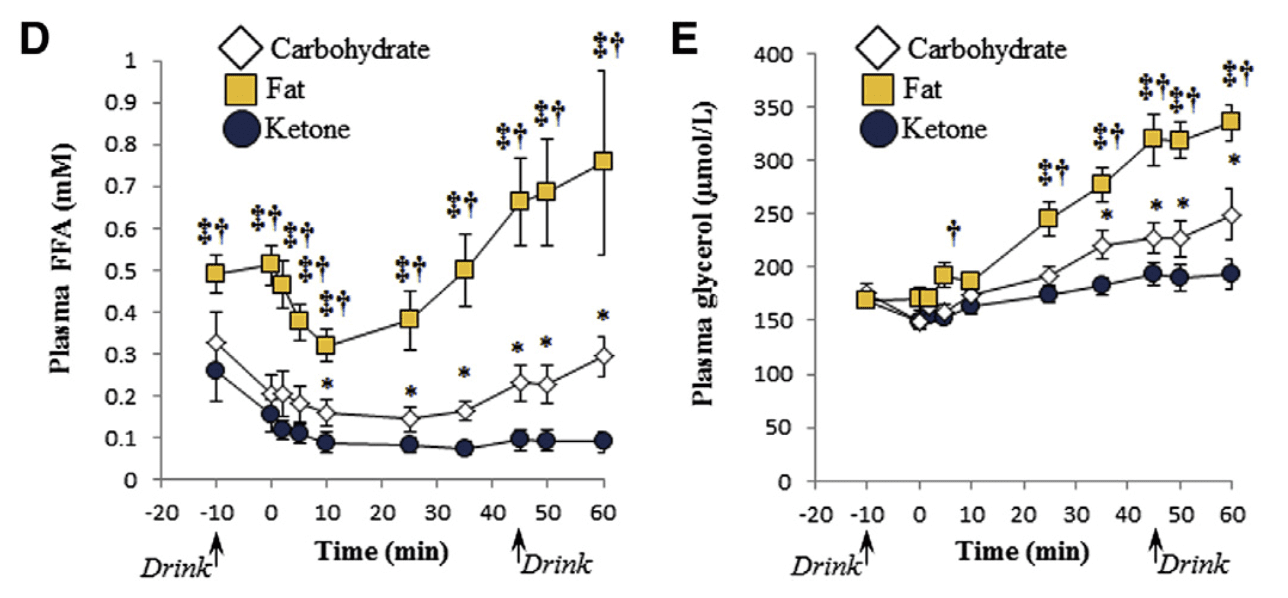
Exogenous ketones induce your system to rely on fat as fuel, as seen in Figure 3. Fat takes longer to metabolize compared to muscle glycogen for vitality. That is because fatty acids aren’t the fuel that is favored by the human body under exercise. This might be useful for athletes performing resistance training or cardiovascular exercises. This is especially helpful for�athletes that would like to experience cardiovascular or resistance training.
Ketone esters boost free carnitine whilst exercising which appears to enhance physical performance.
Exogenous ketones decrease the usage of Branched-chain amino acids, or BCAAs, as�energy, a process known as deamination. The growth was decreased by consumption of a ester beverage by 50 percent during exercise in muscle BCAAs.
Figure 3: Plasma free fatty acid (FFA) and glycerol concentrations after consuming high fat, carbohydrate, or ketone ester drink.
Increased cognition: Elevated plasma ketone concentrations divert the brain to use ketone bodies for the synthesis of phospholipids, which drives growth and myelination. Sugar is often the preferred�fuel for this process, which is not as efficient. BHB appears to work as a signal for pathways. These improve cognition, plasticity and stress immunity. In rat research studies, ingestion of a ketone ester for 5 days enhanced memory and their learning.
Health & Longevity
Anti-carcinogenic properties: Statistics appears to imply that exogenous ketones are a powerful anti-carcinogen. The motive for this is that cancer cells cannot utilize ketone bodies efficiently. In fact ketone supplementation was demonstrated to improve survival rates of mice with cancer.
Neuroprotection: As people age, the brain becomes more prone to neurodegeneration and following conditions like Alzheimer’s and Parkinson’s disease. Ketone supplementation seems to ameliorate the decline. The mechanism is that ketone bodies decrease hyperexcitability and the redness that’s ordinarily shown as sugar metabolism declines from the brain.
Anti-Inflammatory attributes: There’s proof that ketone bodies play an essential part in reducing inflammation by inhibiting a particular class of proteins known as inflammasones.
Gene regulation profile alterations: There’s proof that gene sets could be regulated with an alteration in mitochondrial 3-hydroxy-3-methylglutaryl-CoA synthase, or mHS, as see in rats on a ketogenic diet.
Ketones are a source of energy which is produced when there is not enough sugar or glucose for the human body to burn as fuel. They serve as an alternative fuel source to glucose. Ketogenesis, the metabolism of fatty acids through ketosis, can have a variety of health benefits. Many people achieve these benefits by following the ketogenic diet, however, these advantages can be achieved without the keto diet as well. Exogenous ketone bodies are simply ketones which are consumed through a nutritional supplement. Although the over-consumption of any supplement can have risks, exogenous ketone bodies can provide similar benefits to ketosis. Dr. Alex Jimenez D.C., C.C.S.T. Insight
How Exogenous Ketones Function
Exogenous ketones possess many different physiological effects soon after ingestion:
For starters, ingesting ketones, particularly ketone esters, is an effective approach to Boost BHB from the bloodstream above 2 mMol for almost 8 hours. Ketone salts do not seem to elevate BHB from the bloodstream as efficiently or significantly where ketone esters do, however.
Exogenous ketone supplementation induces blood sugar to reduce significantly, likely as a result of an intense increase in insulin sensitivity. Exogenous ketones may pose a possible treatment.
Exogenous ketones additionally improve oxygen use, particularly in the central nervous system, or CNS. This effect reduces the odds of oxygen reaching potentially hazardous levels in the CNS, which then has a variety of additional favorable health effects like the ones discussed in the prior section.
Potential Downsides to Ketone Supplementation
Like any other nutritional supplement, side effects and drawbacks are possible after consuming exogenous ketones. As ketone supplementation becomes more notable, they are generally quite benign and will improve. The most frequent side effects to know about when using exogenous ketones consist of:
Electrolyte Imbalance: The physiological rationale supporting electrolytes during a state of ketosis is a result of the absence of water retention and frequent urination. The frequency of urination will�increase when supplementing exogenous ketones, but it will not deplete glycogen stores. It could be handy after taking ketones if you’re urinating a lot to drink an electrolyte solution, but it is dependent upon the way you are feeling.
Halitosis or bad breath: If you are on a ketogenic diet, you’re most likely aware that since the body begins to metabolize fat, ketones may cause bad breath. There is little one can do about this. This may arise when utilizing exogenous ketones, but it is not quite as durable as when on the ketogenic diet. If it turns into a problem, chewing gum or mints is the best choice. This issue may occur due to the over-consumption of this nutritional supplement, tailoring extra BHB.
Potential GI distress (flatulence) at exceptionally substantial doses: Exogenous ketones taken in massive doses sometimes lead to GI distress, particularly flatulence. On the other hand, this cause can be hypothesized to be a result of how ketones were blended in a fluid which was palatable. If you are taking a balanced dose of ketones GI distress can be avoided. If some GI distress is widespread, it must improve as you become accustomed to carrying ketones.
Hypoglycemia: Accepting exogenous ketones can induce blood sugar levels to become very low, but you’re unlikely to feel the normal signs of hypoglycemia. That is because if levels are large enough, they control energy in the brain; despite having low blood sugar, therefore, you may feel just fine. A research by George Cahill, discovered that if they had been administered insulin to induce hypoglycemia, ketone levels can protect fasted participants.
Future Research Studies
Research studies on exogenous ketones concentrates on the advantages of their use. Research studies will also concentrate more on their therapeutic use. The information on all those applications is currently limited. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Low back pain affects millions of people each year and is the number one cause of disability worldwide. In the US, it is estimated that 31 million people experience pain in their lower back. It is prevalent and can be debilitating. As patients search for relief, they soon find that not all lumbar pain is created equal. There are many causes and treatments vary widely depending on the issue. Radiculopathy is a condition that can contribute to lower back pain, but chiropractic care can help patients better manage it.
Contents
What is Lumbar Radiculopathy?
Radiculopathy is associated with some of the most significant causes of chronic or acute low back pain. However, it is important to note that the condition itself does not cause the pain. Instead, elements of radiculopathy, such as disc herniation, nerve root impingement, and facet arthropathy are actually what causes the pain.
Radiculopathy is a condition of the spine that occurs when a nerve is compressed, causing pain, weakness, tingling, or numbness along the nerve�s course. In the lower back, that course is in the leg. While it is most common in the lower back, radiculopathy can occur in the cervical or thoracic regions of the spine as well.
Symptoms of Lumbar Radiculopathy
The symptoms of lumbar radiculopathy include pain, tingling, and numbness in the legs. Some patients experience extreme, painful sensitivity to light touch.
The nerves in the lumbar region of the spine supply sensations to the buttocks and legs as well as control muscles. So, when a nerve is compressed in the lumbar spine, those are the areas that are affected. The condition is often called a �pinched nerve� or sciatica because of the way that the pain radiates through the buttock and into the leg.
Causes of Radiculopathy
Irritation or compression of certain nerves are what causes radiculopathy, but it is worth looking at the causes of this irritation or compression to see the deeper cause of radiculopathy. These may include mechanical nerve compression due to:
Degeneration or trauma can cause inflammation in the spinal nerves which can lead to pain.
Who is at Risk for Radiculopathy?
Certain people are more prone to radiculopathy based on the activities they engage in and their genetics. Patients who regularly participate in contact sports, heavy labor�or any activity that puts a repetitive or excessive load on the back are more likely to have the condition. Patients who have a family history of spine disorders, including radiculopathy, are also more at risk of developing it.
Chiropractic for Lumbar Radiculopathy
A review published in the Journal of Chiropractic Medicine examined 162 patients with radiculopathy who were treated with chiropractic care. Of those patients, more than 85% not only experienced pain relief, but their conditions were resolved. This was done over 9 treatment sessions. Most of the patients saw an�improvement of their symptoms within 4 days of their first treatment.
There are a number of treatments for lumbar radiculopathy, including pain medication, epidural steroid injection, and surgery. However, chiropractic care is non-invasive and does not have the unpleasant, sometimes harmful of many pain medications. It is safe and effective, treating the entire body instead of just the part that hurts.
When treating lumbar radiculopathy, the chiropractor may use several techniques such as spinal adjustments as well as stabilization exercise and neuromobilization. They will also work with the patient to determine if there are engaging in any activities that increase their risk factor for the condition. In some cases, the chiropractor may recommend certain lifestyle and dietary changes to increase whole body wellness and a stronger, healthier spine.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine