Every day construction workers lift, stoop, bend, reach, push, pull, twist, and climb. It�s no wonder that 25% of construction worker injuries are to the back. An estimated 1 in every 100 construction workers misses work because of a back injury with an average of seven missed work days. Many just power through the pain which isn�t healthy and can lead to further injury and pain. Repeated back injury and failure to take care of the back by taking proactive steps to prevent injury, can lead to permanent damage, even disability. That can end a construction worker�s career.
Chiropractic care can help keep the spine healthy so construction workers can stay on the job and be pain-free. Regular treatment can offset the stress that is put on the body each day in this rigorous, physically demanding profession. There are several benefits that a construction worker can gain from seeing a chiropractor on a regular basis.
Contents
It helps to maintain mobility
When muscles are stiff and sore, it is natural to try to avoid moving too much. When a person has pulled muscles, or they have a muscle strain, their first instinct is to protect that area. This can lead to stiffness and lack of mobility, especially if the pain is in the back. A painful lower back can make it difficult to move your legs, bend, or even move about normally. Chiropractic helps to relieve the pain and reduce the stiffness so that mobility is restored.
The range of motion is improved
Stiffness can lead to a limited range of motion. If the spine is out of alignment, it can decrease flexibility and significantly limit the joint�s range of motion, whether it�s the back, shoulders, legs, or neck. Chiropractic brings the spine into the correct alignment which improves range of motion.
In one study, 73% of the participants reported an improvement in their back pain. This means fewer missed days of work and much more productive on the job. This is one of the most common reasons that people seek chiropractic care, but it isn�t the only reason. It can help with so much more.
Corrects muscle imbalance
Workers who perform repetitive motions can experience muscular imbalance. This means that some muscles are tight (the ones being used) and others are not being worked as hard. It can cause pain in the area of the muscle as well as in other parts of the body.
A chiropractor can perform a technique called myofascial release to loosen the tight muscles. At the same time, they will recommend exercises for the muscles that don�t get worked as often so that the body can come back into balance. Muscular imbalance can also cause spinal misalignment so the chiropractor will also do an adjustment to bring the whole body back into balance.
Helps the body heal from injuries
Construction injuries are fairly common on a worksite. Most are fairly minor and tend to be ignored by the person until they are in so much pain they can�t function properly. Back strain is a common ailment among construction workers, and it can put someone out of commission for a week or more.
Chiropractic care helps the body heal faster and more efficiently by focusing on the whole body instead of just the part that hurts. The patient receives the treatments at the chiropractor�s office then goes home with advice on lifestyle changes, supplements, and exercises to facilitate and speed healing.
For anyone in the construction industry, especially if their position is physically demanding, regular chiropractic care just makes sense. It keeps the spine healthy and the body moving as it should. It is a simple, natural, effective way to help the body function correctly � because pain is not normal.
Truide Torres desarroll� dolor de espalda durante su embarazo. Y, como resultado de su empeoramiento del dolor y la incomodidad, no pudo continuar participando y participando en sus actividades f�sicas regulares. Truide Torres analiza c�mo encontr� alivio para el dolor de espalda con el Dr. Alex Jimenez, a pesar de sus dudas iniciales sobre la atenci�n quiropr�ctica durante su embarazo. El Dr. Alex Jimenez y su personal ayudaron a Truide Torres a sentirse c�moda y segura al educarla sobre los beneficios de la atenci�n quiropr�ctica durante el embarazo. Truide Torres recomienda al Dr. Alex Jimenez como la opci�n no quir�rgica para el dolor de espalda y el tratamiento durante el embarazo, entre otros problemas de salud. La atenci�n quiropr�ctica es una opci�n de tratamiento alternativa segura y eficaz que corrige los desajustes o subluxaciones de la columna, mediante ajustes de la columna y manipulaciones manuales. Los quiropr�cticos est�n capacitados para trabajar con mujeres embarazadas y no se conocen contraindicaciones para recibir atenci�n quiropr�ctica durante el embarazo.
Quiropr�ctica para el embarazo
�
Tenemos la suerte de presentarle a la Cl�nica Premier de Atenci�n de Lesiones y Bienestar de El Paso.
Como Cl�nica de Rehabilitaci�n Quiropr�ctica y Centro de Medicina Integrada de El Paso, nos enfocamos apasionadamente en el tratamiento de pacientes despu�s de lesiones frustrantes y s�ndromes de dolor cr�nico. Nos enfocamos en mejorar su capacidad a trav�s de programas de flexibilidad, movilidad y agilidad dise�ados para todas las edades y discapacidades.
Queremos que viva una vida llena de m�s energ�a, actitud positiva, mejor sue�o, menos dolor, peso corporal adecuado y educaci�n sobre c�mo mantener esta forma de vida.
Te aseguro que solo aceptar� lo mejor para ti …
Si ha disfrutado de este video y le hemos ayudado de alguna manera, no dude en suscribirse y recomendarnos.
When it comes to body composition analysis and body composition testing, most tend to think about muscle mass and body fat percentages. However, today’s medical BIA (bioelectrical impedance analysis) equipment does a lot more than that.
Body fat percentages are only a small part of a body composition analysis. For body composition equipment utilizing Direct Segmental Multi Frequency-BIA technology (DSM-BIA), means that you are able to measure and monitor other valuable indicators of your health such as visceral fat, body water, segmental readings, and phase angle values.
Contents
What�s Phase Angle?
Phase Angle or PhA allows us to see how the body is responding to changes in health – good or bad.
For example, people with cancer or who are malnourished have low PhA’s.
PhA decreases with age. This is due to the body’s slowed down capacity to repair cells quickly.
When ill, the Phase Angle goes down
When healthy the Phase Angle goes up.
When you boost your Phase Angle, aging slows down.
Solving The Riddle of Phase Angle
PhA is a�direct measurement of cell integrity and the distribution of water inside and outside the cell membrane.
How Do You Measure Phase Angle?
In healthy humans, the cell membrane is made of a layer of non-conductive (insulator) lipid material that’s between two layers of conductive fluids (the body’s water).
Two conducting materials that surround an insulator are often referred to as a capacitor.
The cell membrane is a fortress with capacitor capabilities that prevent currents from entering the cells and other unwanted materials, e.g., toxins and waste.
This means healthy cells/tough capacitors better prevent unwanted substances from entering.
Lean Body Mass (LBM) is the total weight of the body’s organs, skin, bones, body H2O, and muscles.
Describes the entire body weight minus body fat.
Also referred to Fat-free mass.
Resistance/Reactance/Impedance
Resistance is when a conductor transfers the energy of an electric current.
Greater the conductor, lower the resistance.
Low resistance/associated with large LBM.
High resistance/associated with low LBM.
A person that has large lean body mass, has a lot of body water, which means greater conductivity of the current and less overall resistance.
Reactance�measures the cells� ability to store energy.
The body has high reactance if the cells can store energy easily and has low reactance if it stores energy poorly.
Healthy cells with healthy cellular membranes hold the electrical energy charge longer.
Impedance�is the sum of resistance and reactance.
Measuring PhA and cell health can be done with a Bioelectrical impedance device, which assesses cell membrane health.
To measure impedance a small alternating current is run into the body, which then measures the effects on the current caused by the body.
50 KHz is considered ideal to maximize reactance and determine the point where the strongest cells resist the current.
As current travels through your body, the body’s water will naturally resist the flow of the current and this is referred to as resistance.
When current encounters a cell, the cell wall causes a delay, as the voltage builds up, in order to pass through the cell wall while the current continues instantly.
This brief time delay, which is caused by the cells is compared to the amount of water, which provides us with a PhA.
Impedance is a combination of these two values.
Phase Angle and Overall Health
Tracking your PhA, allows you to gain a more precise picture of your health, as it examines cell health/integrity and the amount of water inside.
Higher PhA values mean greater cellular integrity and reflect better cell health.
Low PhA, is predictive of decreased muscle strength, compromised quality of life, and increased mortality in older adults with cancer.
Low phase angles are consistent in individuals with malnutrition, HIV/AIDS, cancer, and chronic alcoholism.
How To Know If My PhA Is Normal?
Certain factors can influence PhA such as (Age, Gender, BMI) but there are differences in PhA’s across different populations. Which means that PhA values tend to differ based on the BIA equipment being used.
Example of a Phase Angle Reading Utilizing The InBody 770:
What everyone needs to know is that phase angle depends on the individual makeup of everyone.
The Connection Between My Body’s Composition & Phase Angle
Inflammation reduction along with body fat reduction
Phase�Angle�Decrease�May�Result�From:
Muscle tissue loss
Increased inflammation
Phase Angle In A Clinical Practice
A study, monitoring PhA values in a hospital setting found that it helped identify nutritionally at-risk patients quickly, thus saving the staff time, as the patients did not have to answer the in-depth nutritional questions. Instead, they took a quick BIA.
Phase Angle Takeaway
PhA values can be highly informative of what is going on in one’s body.
PhA can help in identifying health risks/issues
Track lifestyle change progress
Medical Clinics can use PhA to help create custom treatment and health care plans
Back pain and neck pain are common symptoms brought on by auto accident injuries, sports accident injuries, personal/work accident injuries. The daily actions affecting their wellbeing of an individual can be ultimately affected by symptoms. A group of patients discuss�their neck pain and spine pain symptoms and how they improved when they saw Dr. Alex Jimenez. Chiropractic focuses on the identification, therapy, and prevention of a number of accidents/injuries and/or aggravated conditions related to the musculoskeletal and nervous system.
Top Quality Non-Surgical Care
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.�
Teachers do a lot in a day. They stand for long periods of time, they stoop and bend, pick up children, carry stacks of papers, and sit for long periods while they grade papers. It�s no wonder that so many teachers end up with aching backs! While low back pain is the number one cause of disability worldwide, it�s easy to see how teachers may be more susceptible to experiencing it.
Chiropractic care can help keep teachers standing upright and moving about � as well as other great benefits. A teacher with back pain can�t be as effective as they would be if they weren�t in pain. It makes it harder for them to do their job. Regular chiropractic care can help offset what their body goes through in a day and relieves the pain so they can do what they love � shape young minds.
Contents
What Teachers Do
Teaching is a tough profession. The typical teacher arrives at school before it starts (usually between 6:30 am, and 7:30 am) and they don�t leave until well after the last bell has rung (often between 3:30 pm and 5:30 pm). They grade exams during their vacations and spend hours preparing lessons, quizzes, activities, and tests. In middle and high school, they teach five or six classes a day which means a lot of talking and a lot of standing. Combine the stress with the physical demands of the job, and it�s no wonder aching feet and backs are the bane of a teacher�s existence.
The Impact of Teaching on the Body
There have been several studies that explore the effects of the physical demands that are put upon a teacher. One study analyzed the incidence of musculoskeletal disorders in special education teachers and teachers� aides. It found that the three areas most affected were the wrist, shoulder, and back. It found that 86% of the teachers who participated had physical pain and musculoskeletal condition. Another study examined teachers in a municipal school network in Brazil. It found that:
41.1% complained of foot, leg, and knee pain (lower limbs)
23.7% complained of shoulder, neck, and wrist pain (upper limbs)
41.1% complained of back pain
A third study that assessed teachers in Malaysia reported that 62.5% of the teachers surveyed complained of low back pain.
How Chiropractic Care Helps Teachers with Low Back Pain
Several studies show that chiropractic care is a very effective treatment for back pain. The chiropractor will perform a spinal manipulation to bring the spine (and body) into proper alignment. He may also offer advice on exercises, stretching, and ways to improve posture as well as recommending lifestyle changes and what to look for in supportive shoes. Chiropractic�s whole-body approach not only helps relieve back pain, it helps prevent it as well.
Additional Benefits Teachers can Gain from Chiropractic
While less back pain is great news for teachers, there are other benefits they can reap form chiropractic as well. That�s because it doesn�t focus solely on the back or pain, it looks at the whole body. Every day teachers put a lot of stress on their bodies, bending over to help a child with their work, standing to give a lecture, sitting for hours grading papers, and reaching to write on the blackboard. All of this can take a toll on the body, not just physically, but in other ways as well. It can result in headaches, insomnia, and even frequent illness. A chiropractor can address all those things and make recommendations regarding lifestyle and diet as well as spinal manipulation.
This allows the patient to gain whole body benefits from chiropractic.
When you spend a lot of time behind the wheel, whether you are going on a long trip or your job requires you to drive around town all day, it can be a real pain � in the back. Many car seats may be comfortable for short rides, but they are not built to support the back on the long hauls. However, there are some things that you can do to offset a non-back friendly seat design and alleviate, or even prevent, back pain while driving.
Contents
Create a Comfortable Space
Before you settle in behind the wheel, you want to make sure that you are comfortable. Keeping things like your wallet and cellphone in your pocket may be convenient when you are moving about, but can be an irritant when you are sitting on them mile after mile. Wear comfortable clothing and shoes. Any discomfort can put stress on your body so even if it is not necessarily pain related, it can exacerbate pain as your body�s sensitivity heightens in response to the pressure.
Adjust your seat so that you are comfortable, but sitting reasonably upright. If you recline, it could put stress on your neck and upper back, causing pain. Your seat should also be high enough so that you can place your feet flat on the floor � at least for a while (you can do this while driving if you have cruise control). There should be a slight bend in your elbows as you reach for the steering wheel and you should not have to stretch to reach the pedals. Make sure that your mirrors are adjusted so that you don�t have to bend or crane your neck to get good visibility.
Put Together a Healthy Back Kit
Bring along some things to help keep your back comfortable and pain-free � even if you�ve never experienced back pain while driving. There is always a first time. Some of the items you might want to bring along include:
A towel that you can roll up and place behind the small of your back
A lumbar support pillow
A cold or hot pack
Something for pain relief
A cushion for your car seat to absorb the vibration
Water (so you can stay hydrated)
Essential Oil like lavender or peppermint (put a few drops in a carrier oil and apply to the sore areas)
Take Breaks and Move a Little
Driving straight through without any breaks is never a good idea. It can make you more tired, stiff and sore � and less alert on the road. Instead, take breaks to get out of the car, walk around, and stretch. When you move, you stimulate your circulation which brings oxygen and vital nutrients to your muscles. You�ll feel better, be more alert, and will be less likely to experience back pain.
Stopping every hour or so will help considerably with alleviating back pain. It doesn�t have to be a big production, walk around for a few minutes, stretch your neck, shoulders, and back, then get back on the road. In between stops you can move your ankles up and down or rotate them to increase circulation to the lower leg. You should also adjust your position or your seat about every 20 minutes. Even these slight movements can help keep the blood flowing which will prevent your muscles from getting stiff and sore.
Regular chiropractic care, as well as a consistent exercise routine, can help prevent back pain in many situations, including while driving. Your chiropractor can also recommend some back strengthening exercises and stretches that will help make your spine even healthier.
Each chemical reaction which occurs in the human body requires enzymes and each one of these processes needs a coenzyme. But what are coenzymes? They are vitamins and minerals. Approximately 37 billion, billion chemical reactions occur in the human body every second.
That is why proper nutrition and a balanced diet rich in whole foods with vitamins and minerals is fundamental towards overall health and wellness. The majority of people in the United States are vitamin and/or mineral deficient. But, how do you know if you�re a part of the 90 percent of individuals with enough deficiencies to develop disease? We will discuss the tests you can utilize to find out if you�re vitamin and/or mineral deficient and what you can do about it.
Contents
What�is�Nutrition?
Hello, welcome to part three of �Taking Control of your Healthcare�. Today, we will discuss one of the fun topics of functional medicine: nutrition. Unfortunately, nutrition is one of the most essential conversations that many doctors aren�t willing to have with their patients. The average medical doctor learns about disease and malnutrition rather than learning how to use nutrition as treatment or even how to use nutritional therapies to achieve optimal health and wellness.
I personally believe that food can be utilized as a form of medicine. That it should be the foundation of medical practice, not an afterthought in medicine. There is no better treatment than proper nutrition. Approximately 90 percent of individuals in the United States aren�t getting the essential nutrients they require for healthy bodily functions. And more than that probably aren�t getting enough nutrients to prevent diseases associated with nutritional deficiencies. However, what is ultimately needed to achieve optimal well-being? More than 98 percent of Americans are deficient in omega-3, 80 percent in vitamin D, 50 percent in magnesium, and 10 percent in vitamin C. Nutrient deficiencies can also continue to cause health issues for years.
Acute diseases, such as rickets, scurvy, beriberi, or iron deficiency anemia, are often the most talked about health issues associated with nutrient deficiency, however, there�s also something known as long latency deficiency diseases. So, how much vitamin D do we need to not get rickets? Not a lot, only 30 units really. And how much do we need to not get osteoporosis? Perhaps about 3,000 to 4,000 units per day. Now, how much folate do we need to not get anemia? Also not very much. But, how much do we need to prevent heart disease, cancer, and dementia? You definitely need a lot more units per day.
Each chemical reaction which occurs in the human body requires enzymes and each one of these processes needs a coenzyme. But what are coenzymes? They are vitamins and minerals. Approximately 37 billion, billion chemical reactions occur in the human body every second.
That is why proper nutrition and a balanced diet rich in whole foods with vitamins and minerals is fundamental towards overall health and wellness. The majority of people in the United States are vitamin and/or mineral deficient. But, how do you know if you�re a part of the 90 percent of individuals with enough deficiencies to develop disease? There are only several nutrients which we are generally tested for. And for a majority of these, doctors aren�t aware of what the optimal values should be which can make correcting the nutrient deficiency so much difficult to do.
Taking Control of Your Nutrition
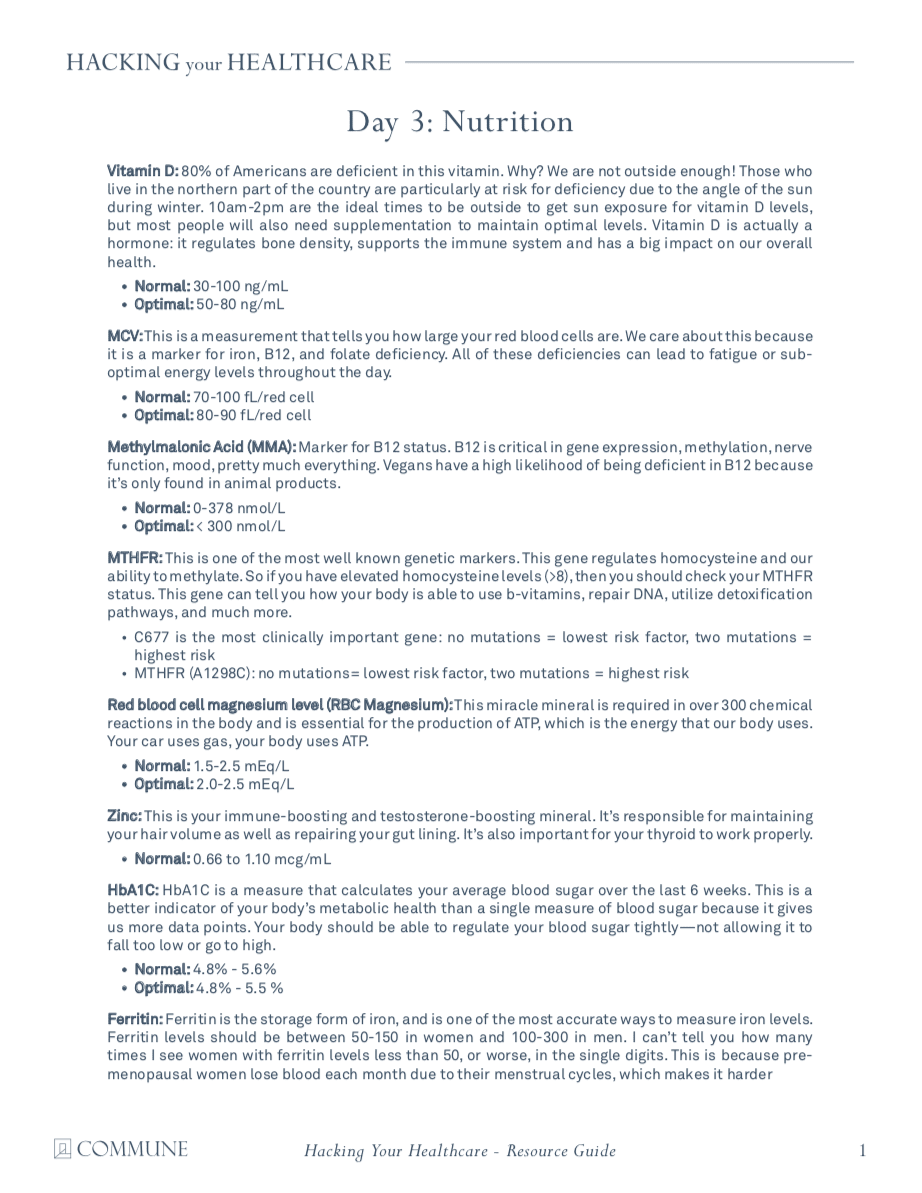
One of the most fundamental nutrients you need to measure is vitamin D. Although it�s referred to as a vitamin, it�s actually more like a hormone and it�s produced from cholesterol. This is yet another reason why cholesterol is essential. Approximately 80 percent of the population is deficient in vitamin D. Unless you�re in the sun 20 minutes every day between 10:00am and 2:00pm, you might need to take vitamin D supplements. In order to supplement properly, however, we need to know from what level you are starting at first. By way of instance, optimal vitamin D levels should be anywhere between 50 and 80 nanograms per milliliter of blood. The recommended amount of vitamin D we can supplement is about 2,000 to 4,000 units.
If you have lower vitamin D levels or if you have genetic problems, you may actually need to supplement with up to 10,000 units of vitamin D. That�s why it�s fundamental to work with a doctor or functional medicine practitioner who can measure and test your nutrient levels as well as help you optimize them. Most supplements contain about 400 units which is 10 times less than the amount most of us need. The optimal levels are generally just over 20. This is way too low. In one research study, women with vitamin D levels between 45 and 60 experienced reduced preterm labors by up to 60 percent. Vitamin D is also essential to help build strong bones and muscles, to improve immune system function, to prevent cancer, and ultimately, to help you live longer. It�s incredible.
Another measurement or test that�s performed by most doctors but is not always interpreted correctly is referred to as the MCV or mean corpuscular volume. The MCV measurement evaluates the size of your red blood cells in a test called CBC, or complete blood count, which is one of the most common blood panels ordered by healthcare professionals. So, if you are deficient in nutrients, your cells can either become smaller or larger. By way of instance, if your cells are too big, it could be a signs of a folate or vitamin B12 deficiency.
B vitamins are essential in numerous chemical reactions within the human body. They help us produce energy as well as help us regulate gene expression in order to create proteins that will ensure our overall health and wellness. If our B vitamins are too low, we could eventually develop an iron deficiency, anemia, or it could even cause a genetic disorder.
Optimal levels of B vitamins should be between 80 to 90. B complex vitamin supplements can help easily optimize levels of B vitamins. But, why would anyone be deficient in B vitamins? Is their diet not providing them with enough nutrients? Are they vegan? Are they taking any drugs and/or medications that prevent vitamin B12 absorption? Moreover, B vitamins are depleted during times of high stress which, as a practicing chiropractor, I can say it happens frequently to a majority of the population in the United States alone.
MCV is not the only measurement or test which evaluates a patient�s levels of B vitamins. Homocysteine is an alternative marker we will discuss in future articles which demonstrates B6, folate, and B12 levels. However, both the MCV and the homocysteine measurement or test only demonstrates that one or more of these nutrients may be deficient. It doesn�t necessarily tell us which one. Therefore, some additional, follow up evaluations may be required.
The MMA, or methylmalonic acid, measurement or test also shows vitamin B12 levels. Ultimately, vitamin B12 is essential for many processes in the human body, including energy production, gene expression, methylation, nerve function, and mood, among many other processes. Vegans have a higher chance of developing a B12 deficiency because it�s only found in animal products. Folate is another fundamental B vitamin. It can be determined directly in the blood, but, homocysteine is a more precise marker for folate levels.
In this section, we�re also going to discuss genetics because there is a measurement or test which can demonstrate a lot more regarding the status of your B vitamins and your ability to utilize them. Our genes are capable of making proteins. We have approximately 20,000 genes which are designed to create proteins. And one third of all the proteins they make are for our enzymes. Enzymes convert molecules into other molecules. These enzymes are also largely dependent on specific nutrients. One of the most fundamental genes which can be affected is known as MTHFR, or methylenetetrahydrofolate reductase. But you can just call it MTHFR.
MTHFR is essential because it helps regulate methylation, homocysteine, and folate, which are vital towards our overall health and wellness. When you have elevated levels of homocysteine, you should check your methylation status by looking for the MTHFR gene through a simple blood test.
Methylation is a key biochemical process which is fundamental towards the proper function of most of the human body�s systems. It triggers billions of times each second. And it ultimately helps control homocysteine, a substance which can damage blood vessels and has been associated with dementia, heart disease, and cancer, among other health issues. Methylation also helps repair your DNA on a regular basis as it helps recycle molecules necessary for detoxification, or getting rid of toxins. It also helps control your mood and it helps manage inflammation. Methylation is critical.
But, to make sure that methylation is active, the human body needs optimal levels of B vitamins. Without enough B vitamins, the methylation process can break down and the effects can be destructive. This is where we start seeing an increase in birth defects, such as spina bifida, down syndrome, and more miscarriages.
MTHFR is frequently abnormal in approximately 35 percent of the population. Methylation breakdown can also increase the risk of developing health issues like osteoporosis and diabetes, cervical dysplasia or cancer, including colon cancer and lung cancer, and even depression, pediatric cognitive dysfunction as well as mood and behavioral disorders, dementia, and stroke. Methylation is truly a key biochemical process.
When we discuss genetics, we have to understand that our environment can alter our genes. So, what if you have an MTHFR variation in your genes? First of all, not all mutations cause health issues. One mutation, by way of instance, known as C677T, is one version of the gene which is more significant than another version of the gene, known as A1298C. Now there�s no need to worry about these gene variations. They serve as examples to demonstrate you the quality of these mutations and how they function. People with these variations of the gene, by way of instance, might only need more folate or they might need a particular type of folate known as methylfolate. This is where a functional medicine practitioner can help their patients.
A genetic test can let you known if you have one of these gene variations. But, don�t get stressed. There�s a lot you can do to optimize your overall health and wellness. Many patients have visited my office after they find out they have these variations in their genes. And they quickly learn that they do have the option to take control of their well-being. However, what you do control is not your genes, you control your gene expression.
If you alter your healthy eating habits, you alter your nutrients. If you alter your environment, you alter which genes become active and which genes become inactive. And with these mutations, you can do just about the same thing by simply following the proper nutrition. When you find a doctor or functional medicine practitioner that�s willing to work with you, they�re going to tell you what lifestyle modifications you should follow to prevent health issues.
So, we�ve only just discussed the B vitamins. Next, we will discuss another fundamental nutrient in the human body: magnesium. Magnesium is a super essential mineral. Approximately 48 percent of people in the United States consume less than the required amount of magnesium from food. Magnesium is necessary in over 300 chemical reactions in the human body. It is also fundamental in the production of ATP, or the energy the human body utilizes as fuel.
A magnesium level blood measurement or test can help determine if you have a deficiency. Magnesium can also help reduce anxiety, calm the nervous system, and improve sleep. It is also an essential nutrient in the management of blood sugar levels. If you�ve been told by a healthcare professional that you have an average blood sugar level of over five and a half in something known as A1c, then magnesium can help.
Also, it�s very easy to know if you have a magnesium deficiency by looking at your current diet and symptoms. Do you eat enough magnesium rich foods like dark, leafy greens, beans, nuts and seeds? Or do you eat a lot of processed foods? Perhaps you also have symptoms such as anxiety, insomnia, constipation, muscle twitching, muscle cramps, PMS, and/or palpitations. If you have one or more of the symptoms I just mentioned, you may have a magnesium deficiency.
Next, we will talk about zinc, the immune-boosting and testosterone-boosting mineral in the human body. This important nutrient is in charge of maintaining your hair volume as well as repairing your gut lining. It�s also responsible for making sure your thyroid is functioning properly. Zinc can be easily measured or tested in the blood and unfortunately, it�s another nutrient we are highly deficient in, in the United States. Additionally, you can also look at your alkaline phosphatase levels, which can be calculated through a liver function evaluation on a regular blood panel. High levels of alkaline phosphatase may indicate the presence of cancer or bone problems, among other health issues, however, low levels of alkaline phosphatase may indicate a zinc deficiency, because it�s a zinc-dependent enzyme.
Finally, the last fundamental nutrient we are going to discuss is iron. Iron is frequently deficient in vegans and vegetarians, or in women in general due to menstruation. Iron is necessary for transporting oxygen throughout the human body and it�s ultimately essential for brain health and wellness. Iron is also important for hair and nails, sleep, and so many other things.
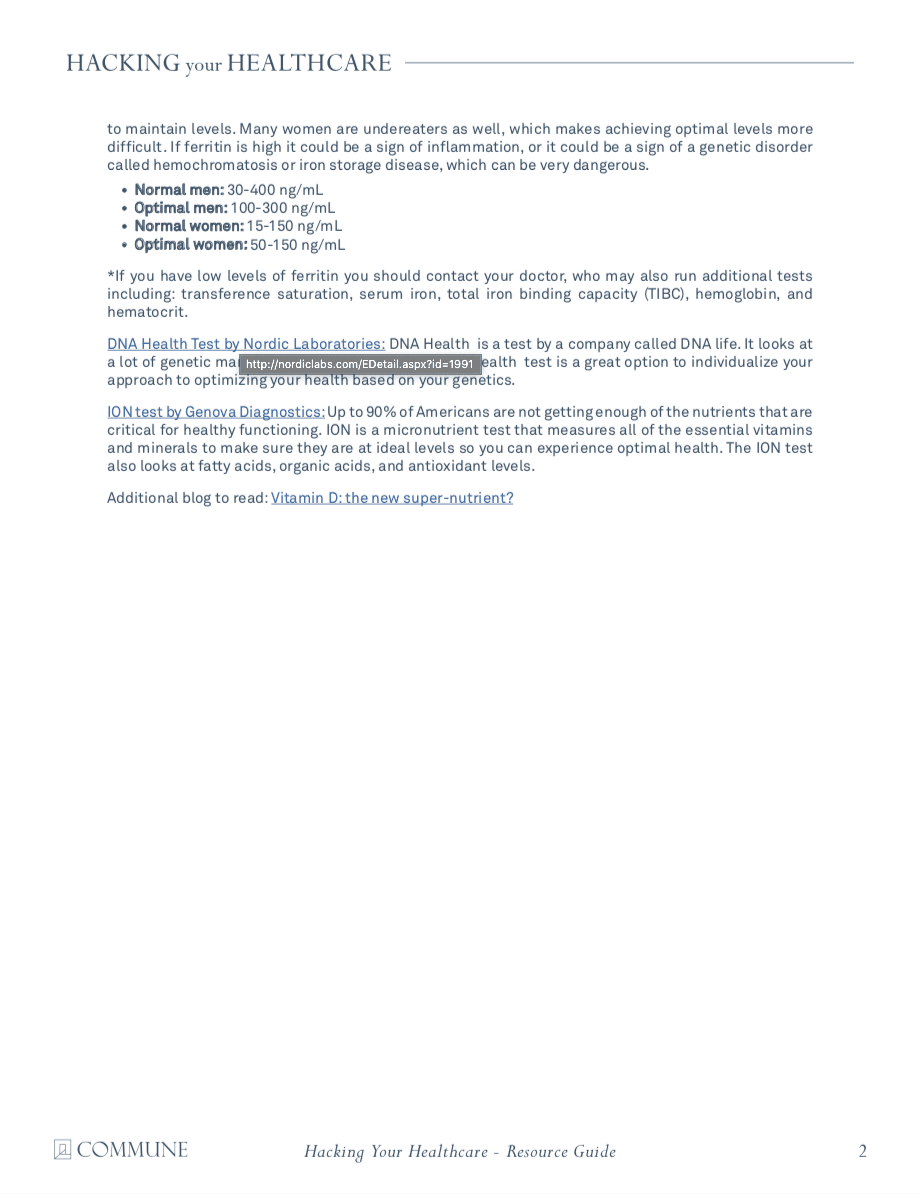
Ferritin is a stored type of iron and it�s this nutrient which helps you see your iron levels. Optimal ferritin levels should be between 50 to 150 in women and 100 to 300 in men. And many times I�ve seen women visit my office who have ferritin levels of less than 50, or worse, in the single digits. This is because pre-menopausal women lose blood every month due to their menstrual cycles and it becomes so much harder for them to maintain proper ferritin levels. Many women also eat way less than what they�re supposed to be eating every day. High levels of ferritin, on the other hand, could be a sign of inflammation, generally caused by insulin resistance to sugar, or it could be a sign of hemochromatosis or iron storage disease, a very dangerous genetic disorder.
Having decreased levels of ferritin can also make you feel tired, and it can cause hair loss, it can cause insomnia. So, even if your blood count is normal, if your ferritin levels are low or your iron levels are low, it can also cause these symptoms. That�s why if you experience symptoms of fatigue, it�s essential to measure or test your ferritin levels. And it can be easily supplemented.
Aside from ferritin, a low MCV can also determine if you have an iron deficiency. Iron deficiencies can cause red blood cells to become very small and that can be demonstrated in low MCV levels, which evaluate the size of your red blood cells. Additionally, transference saturation, serum iron, TIBC, or total iron binding capacity, and hemoglobin, can provide us with a more in depth look at your iron status to distinguish different causes of anemia. These are included on a regular iron blood panel in a lab test.
We�ve discussed several nutrients which can be ordered by a majority of healthcare professinals with access to conventional lab testing. Furthermore, there�s another test which can tell us more about which type of nutrients we need based on our genes. It�s called the DNA health test and it�s provided by a company called DNAlife. This test evaluates a variety of genetic markers associated with detoxification, lipid metabolism, and inflammation, including the MTHFR gene and other B vitamin markers. Now, DNA Health demonstrates the different genes we evaluate. And most of these are common genes, they�re those we can do something about. We analyze the genes we can change based on your nutrition and other lifestyle factors.
It shows us the MTHFR gene, other B vitamin markers, genes that control B6, folate, and B12 as well as demonstrating how they function and whether you have nutrient deficiencies. Then it tells us which nutrients you will need to supplement and how much we will need to give to you. It�s tremendously helpful.
There was an individual who had two variables of the MTHFR gene. This woman had miscarriage after miscarriage after miscarriage. She visited her doctor for an evaluation and it turns out that she had a folate-regulating mutation. So her doctor then started giving her the proper amount of folate she needed and she started having healthy babies. Sometimes, nutrition can be that powerful towards improving a patient�s overall health and wellness.
The DNA health test can help personalize your approach when optimizing your well-being based on your genetics. What we measure utilizing the DNA health test provide well-established insights about your genes as well as what you can do about them.
A micronutrient test known as the individualized optimized nutrition profile or the ION panel, are alternative test options which can also provide information about your current nutritional status. This test is by Genova. This is a robust test which measures all the essential vitamins and minerals, fatty acids, organic acids, and antioxidants you currently have. Ultimately, this test looks for imbalances, insufficiencies, or deficiencies, rather than looking for a specific disease. It looks for things that a majority of doctors never look at.
Functional medicine practitioners or doctors look at patient�s amino acid levels, mineral levels, and even toxin levels from heavy metals like mercury, lead, arsenic, and many more. We also look at your antioxidant levels, vitamin A and vitamin E levels, as well as your CoQ10 antioxidant and beta carotene status. We can determine if a person eats vegetables or not if, by way of instance, they have low levels of beta carotene. We also look at vitamin D levels, essential fatty acids, including your omega-3 fats and your omega-6 fats. We can tell if a person eats junk food. We can tell if a person is eating fish. And We can tell if a person is eating too much olive oil or saturated fats. It�s all demonstrated in these measurements and tests.
An OAT test, or organic acids test, also looks at what is known as organic acids. This test demonstrates a wide array of parameters associated with your mitochondria, which we will discuss in the next article, your B vitamins, your neurotransmitters, your gut flora, and your detoxification. It�s ultimately a comprehensive test which shows me if a patient is well or sick. It shows me where the imbalances are and where I need to recommend lifestyle modifications. It also helps provide clues about other health issues.
By way of instance, if your mitochondria aren�t functioning correctly because you have decreased levels of essential amino acids or you have increased oxidative stress or if you simply have low levels of selenium and zinc, there�s a possibility that you might have some form of toxic overload due to heavy metals. And that�s precisely what I would go looking for. Signs like these provide a lot of information about what we can do to treat a patient. And an experienced functional medicine practitioner or doctor can determine what�s really going on with a patient or they can help patients discover how to optimize their overall health and wellness.
Nutrition is the study of nutrients in food and how the human body utilizes nutrients as well as the relationship between diet, disease and overall health and wellness. Nutrients are a source of nourishment, including carbohydrates, proteins, fats, vitamins, minerals, fiber and water. Functional medicine focuses on the use of food as a form of medicine. A balanced nutrition can help prevent as well as treat a variety of health issues. Similarly, nutrition in functional medicine involves how certain diseases and conditions may be associated with dietary factors, such as poor diet or malnutrition, food allergies and food intolerances. Dr. Alex Jimenez D.C., C.C.S.T.
Understanding Your Nutrition
As good functional medicine doctors we�re often left asking ourselves, why is it that so many people in the United States are overfed but undernourished? Or, why is it that Americans eat too many calories and too few nutrients? The leading causes for the widespread nutritional deficiencies are the following: First, humans evolved from eating wild foods which contained tremendously higher levels of nutrients. Second, the soil we currently utilize to grow our crops in has become greatly depleted of nutrients. Hybridization techniques from industrial farming are yielding animals and vegetables to have decreased levels of nutrients. Third, processed foods have absolutely no nutrients, which is why they frequently have to be fortified. And last but not least, exposure to environmental toxins, lack of sunlight, chronic stress, and poor diet, including increased alcohol, caffeine, and sugar consumption, can increase our nutritional needs, much of which we�re already not getting enough from our current nutrition.
Well you might not need any vitamins, however, if you can meet certain conditions. Perhaps if you only hunted and gathered wild food and if you weren�t exposed to environmental toxins. Or maybe if you went to sleep with the sun and woke up with the sun, sleeping nine hours a night. And if you experienced absolutely no amount of chronic stress. Ultimately if you only drank pure, clean water and breathed pure, clean air. Then, you probably wouldn�t need any vitamins. But the rest of us that don�t follow these conditions, we do need them.
And with that thought, we wrap up this article. In the next article, we will talk about hormones. Hormones can affect almost every aspect of our well-being, and many healthcare professionals don�t understand what our optimal hormone levels should be or even when to test them and what to do about it once they do. Measuring and testing hormone levels should be standard practice, and many patients have never had a blood panel to look at their hormones. It�s fundamental to know as well as understand what�s going on inside your own body. And that�s why this next article is so important. You won�t want to miss our next update. See you soon.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Low back pain which gradually influenced his quality of life was developed. David Garcia was unable to walk as his symptoms worsened and his back pain became excruciating. He first visited Dr. Alex Jimenez, chiropractor in El Paso, TX, following a recommendation from his sister. Dr. Jimenez managed to supply David Garcia with all the aid he deserved for his low back pain, restoring his well-being. David Garcia clarifies the wonderful service Dr. Alex Jimenez and his team have given him to offer him relief from his painful symptoms and he highly recommends chiropractic care as the non-surgical pick for low back pain, among other health problems.
Chiropractic Non-Surgical Relief
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Chiropractic care is enjoying an upsurge in popularity as more people are veering away from invasive procedures and pharmaceuticals in favor of more natural treatment options for their pain. A recent Gallup poll for Palmer Chiropractic College confirms this. Of the people surveyed:
More than 35.5 million people said they sought chiropractic care within the 12 months (the Gallup survey was conducted from February 8, 2016, through March 11, 2016).
95% said chiropractic was effective in treating their condition.
89% said they would recommend chiropractic to friends and family.
97% said that they would likely see a chiropractor for neck or back pain.
88% said that chiropractic care is a good value for the money.
Contents
Non-Drug Treatments for Back Pain should be Sought First
In April 2017, the American College of Physicians published their updated guidelines for managing and treating low back pain. In it, they recommended seeking non-drug treatments which include the application of heat, exercise, stress reduction, and spinal manipulation before turning to medications. The purpose is to steer patients away from unnecessary medicating and toward healthier, more natural options as the first line of defense in managing low back pain.
Another study published in2017 in the Journal of the American Medical Association supported spinal manipulation as a preferred first treatment option over pharmaceuticals for patients with acute low back pain. While these recommendations are primarily in response to the opioid epidemic, it is also in response to the numerous studies that show chiropractic care is safe and effective for back pain management.
Chiropractic is a Healthier, Safer Option
The Centers for Disease Control (CDC) reports that opioid abuse and overdose has reach epidemic proportions. An estimated 91 Americans die every day from an opioid overdose. This includes opioids obtained by a prescription from a doctor.
Popular pain medications like oxycodone and hydrocodone have seen steadily increasing abuse, overdose, and death rates over the past two decades. In fact, deaths caused by an overdose of these drugs as well as methadone and others, have quadrupled since 1999.
These medications are highly addictive and have many unpleasant and even dangerous side effects. While most states are taking aggressive steps to curb the over-prescribing of these medications, patients are still finding ways around the prescribing guidelines and restrictions. This is a compelling reason for patients to seek natural, non-medicinal pain relief options first � and for their doctors to recommend them.
More People are Turning to Natural Remedies
Many patients are simply getting fed up with invasive treatments and numerous pills, causing them to turn to remedies that are more natural. One benefit of chiropractic and other natural remedies is that they rarely treats only the symptom.
Instead, it addresses the root of the problem to treat the cause. This approach has many benefits beyond being medication free and non-invasive. When the cause of the condition or problem is corrected, it can eliminate other troubling symptoms as well.
Chiropractic is a Healthier, Whole Body Option
A patient who sees their chiropractor for low back pain may find that after a few treatments their headaches, constipation, and digestive issues are also resolved. This is because chiropractic treats the body as a whole, unlike traditional medicine that tends to treat it in parts.
In the body, everything is connected, so a problem in one area could easily cause problems in other areas. By correcting the root of the problem, the patient receives more rounded healthcare.
Where traditional medicine will often opt to prescribe a pain pill for lower back pain, chiropractic care looks for the cause of the back pain and treats the pain symptom from the cause. The chiropractor may advise lifestyle changes, changes in diet, and even recommend supplements. With chronic health conditions like diabetes, heart disease, and obesity increasing at an alarming rate, chiropractic care offers a solution that treats the body as a whole in a more natural, safer way.
Sciatica is a set of symptoms characterized by discomfort and pain along the length of the sciatic nerve, which runs down the buttocks, hips, and thighs, into the feet and the legs. Also known as sciatic nerve pain, sciatica is brought on by the compression or impingement of the nerve through harms and/or ailments such as a herniated disc. The patients in the following video describe the way their quality of life has influenced. After getting chiropractic care with Dr. Alex Jimenez, chiropractor, patients talk how treatment has helped them achieve pain relief from their sciatica. Sciatic nerve pain is one of the most frequent health issues. The people highly recommend Dr. Alex Jimenez as the non-invasive pick for sciatica.
Nerve Pain Therapy
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine