Dr. John Coppola and Dr. Valerie Monteiro know the symptoms associated with peripheral neuropathy. Since many health professionals clarify peripheral neuropathy as an irreversible and permanent health problem which can only be handled via the usage of drugs/medications, Dr. Coppola and Dr. Monteiro help cure cervical disease symptoms by treating the origin of the health dilemma.
Low-level laser therapy (LLLT) is a non-invasive treatment approach that could help naturally raise oxygen, blood circulation and flow within the human body. LLLT can speed up recovery to be stimulated by the mitochondria referred to as the cell’s powerhouses. Dr. Coppola and Dr. Monteiro clarify how low-level laser treatment can help treat cervical disease symptoms and help overall well-being. Dr. Alex Jimenez, a chiropractor in El Paso, TX, helps treat peripheral neuropathy symptoms and other wellness problems.
Contents
LLT Laser Therapy for Peripheral Neuropathy El Paso, TX (2019)
Neuropathy is a medical term used to describe a collection of general diseases or malfunctions which affect the nerves.
The causes of neuropathy, or nerve damage, can vary among individuals and these may be caused by different:
Diseases
Injuries
Infections
Vitamin deficiencies
Neuropathy can also be classified according to the location of the nerves being affected and according to the disease-causing it.
Neuropathy caused by diabetes is called diabetic neuropathy.
Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest.
Peripheral neuropathy is simply referred to as neuropathy, which is a state that happens when the nerves become damaged or injured, oftentimes simply disturbed.
It�s estimated that neuropathy affects roughly 2.4 percent of the general populace and approximately 8 percent of people older than age 55.
Type
Neuropathy can affect any of the three types of peripheral nerves:
Sensory nerves�transmit messages from sensory organs:
Eyes
Nose
Brain
Motor nerves track the movement of the muscles
Autonomic nerves regulate the involuntary body functions
Sometimes, neuropathy will only impact one nerve. This is medically referred to as mononeuropathy and instances of it include:
Ulnar neuropathy affects elbow
Radial neuropathy affects arms
Peroneal neuropathy affects knees
Femoral neuropathy affects thighs
Cervical neuropathy affects neck
Sometimes, two or more isolated nerves in separate regions of the body can become damaged, injured or disrupted, resulting in mono neuritis multiplex neuropathy.
Most of the time, multiple peripheral nerves malfunction at the same time, a condition called polyneuropathy.
Cause
Neuropathies are often inherited from birth or they develop later in life.
The most frequent inherited neuropathy is the Charcot-Marie-Tooth disease, which affects 1 in 2,500 people in the USA.
Although healthcare professionals are sometimes not able to pinpoint the exact reason for an acquired neuropathy, medically referred to as idiopathic neuropathy.
There are many known causes for them, including:
Systemic diseases – a systemic disease is one that affects the whole body.
Physical trauma
Infectious diseases
Autoimmune disorders
The most frequent systemic cause behind peripheral neuropathy is diabetes, which can lead to chronically high blood glucose levels that harm nerves.
Other systemic issues can cause neuropathy, including:
Kidney disorders permit high levels of nerve-damaging toxic chemicals to flow in the blood
Toxins from exposure to heavy metals include:
Arsenic
Lead
Mercury
Thallium
Drugs/medications, including anti-cancer medications, anticonvulsants, antivirals, and antibiotics
Chemical imbalances because of liver illnesses.
Hormonal diseases, like hyperthyroidism, which disturbs metabolic processes, and potentially induces cells and body parts to exert pressure on the nerves.
Deficiencies in vitamins, such as E, B1 (thiamine), B6 (pyridoxine), B12, and niacin can be vital for healthy nerves.
Alcohol abuse induces vitamin deficiencies and could harm nerves.
Cancers and tumors can exert damaging pressure on nerve fibers and paths.
Chronic inflammation can damage protective tissues around nerves, which makes them more vulnerable to compression, getting inflamed and swollen.
Blood diseases and blood vessel damage, which may damage or injure nerve tissue by decreasing the available oxygen supply
Symptoms
Depending on the reason and unique to each patient, signs, and symptoms of neuropathy can include:
Symptoms are dependent on autonomic, sensory, or motor nerves or a combination are affected.
Autonomic nerve damage can start a chain reaction of physiological functions like blood pressure or create gastrointestinal problems and issues.
Damage or dysfunction in the sensory nerves may impact sensations and sense of equilibrium or balance, while injury to motor nerves affects movement and reflexes.
When both sensory and motor nerves are involved, the condition is known as sensorimotor polyneuropathy.
Complications
Peripheral�neuropathy�may result in several complications, as a result of disease or its symptoms.
Numbness from the ailment can allow you to be less vulnerable to temperatures and pain, making you more likely to suffer from burns and serious wounds.
The lack of sensations in the feet, for instance, can make you more prone to developing infections from minor traumatic accidents, particularly for diabetics, who heal more slowly than other people, including foot ulcers and gangrene.
Furthermore, muscle atrophy may cause you to develop particular physical disfigurements, such as pes cavus, a condition marked by an abnormally high foot arch, and claw-like deformities in the feet and palms.
Treatment
The first step in neuropathy treatment should be finding the root cause that’s causing the neuropathy.
Treatment of diseases such as:
Diabetes
Guillain-Barre syndrome
Rheumatoid arthritis
Sarcoidosis
Other underlying diseases
Prevents continued nerve damage and in cases heals the damaged nerves.
If you are unaware of any underlying disease that is causing the peripheral neuropathy, make sure to let your doctor know of abnormal symptoms.
Medication
Peripheral neuropathy can be treated with various medications.
The first type used to treat mild symptoms are:
Over-the-counter pain medications
In more severe cases:
Opiates
Narcotic medications
Anti-seizure medications
A doctor may prescribe a lidocaine patch or anti-depressants to relieve symptoms.
Patients should thoroughly discuss�neuropathymedication with a doctor before proceeding.
Chiropractic/Massage/Physical Therapy
Various manual therapies can benefit symptoms in neuropathy treatment.
A therapist or chiropractor will perform various manipulation techniques, and teach exercises and stretches to help improve symptoms combined with increased muscle strength/control.
A therapist may also recommend braces or splints to improve mobility.
Patients should attend all physical therapy sessions to gain maximum benefits.
Low-level-laser-therapy LLT
The primary and most debilitating symptom of diabetic peripheral neuropathy is a sensation of tingling, prickling, buzzing, pinching, burning, and/or sharp jabbing stabbing pain in the feet.
Low-Level Laser Therapy (LLT) takes information from the receptors on the membrane of the cell and mitochondrion or the engine of the cell.
This information reaches the cell’s DNA, that directly controls cell function.
When cells receive better information, they work better, along with the tissues they make up like:
Bones
Cartilage
Tendons
Ligaments
LLT promotes the healing and regeneration of damaged tissues,� and its�systemic effects on tissue function are also carried throughout the body by blood and meridians or energy channels.
The key basic physiological effects of llt low-level laser light include:
Increased cell membranepolarization/permeability
Adenosine-5-triphosphate (ATP) production and respiratory activity
Enzyme activity
Collagen and epithelial production
Capillary formation
Macrophage (immune system) activity
Analgesic effects due to elevated endorphin production
Electrolytic nerve blockage
Improved blood and lymph flow
An anti-inflammatory effect from improved circulation and accelerated tissue regeneration
Increased production of antioxidants
An additional benefit is that the light energy from llt low-level lasers will only be absorbed by cells and tissues that are not functioning normally and do not go after healthy cells.
Low-level laser therapy llt has the potential of providing an effective means of reducing low back pain that is:
While every type of neuropathy, such as diabetic neuropathy or autoimmune disease-associated neuropathy, develops its own unique group of symptoms, many patients will often report common complaints. Individuals with neuropathy generally describe their pain as stabbing, burning or tingling.�Low-level laser llt therapy can help relieve these symptoms.
If you experience unusual or abnormal tingling or burning sensations, weakness and/or pain in your hands and feet, it�s essential to seek immediate medical attention in order to receive a proper diagnosis of the cause of your specific signs and symptoms. Early diagnosis can help prevent further nerve injury.� And early laser treatment can help before symptoms really become severe. Visit http://www.neuropathycure.org.
Are you constantly feeling exhausted? Have you been noticing any mood changes? Do you struggle to focus on regular tasks? Brain fog, which often includes depression and fatigue, is a health issue that can have consequences on all facets of your life. �
Contents
Why Depression Causes Fatigue
Depression is just one of the most frequent mental health issues in the United States. Some symptoms, which may stem from depression, are excessive feelings of guilt, hopelessness, insomnia, and fatigue as well as brain fog, among others. �
Depression, brain fog, and fatigue, or chronic tiredness, can frequently go hand in hand. It is a vicious cycle: brain fog makes you spend energy for you to make it through the day, which in turn, makes you feel even more tired when you also have depression. Then when you’re feeling unproductive, it worsens your depression even more and it can affect your sleep. �
The direction of causality has not been ascertained but researchers have found definite links between inflammation, brain fog, and depression. These links can go beyond just the cognitive and psychological aspects of depression and brain fog. �
Other health issues that can involve autoimmune and/or inflammatory processes also correlate with brain fog, including chronic fatigue syndrome, fibromyalgia, or rheumatoid arthritis. Therefore, several healthcare professionals and researchers now believe that inflammation may be a significant origin of depressive symptoms, although not the sole one. �
Understanding Brain Fog
We hear the term brain fog a lot nowadays but what exactly is brain fog? Brain fog isn’t a health issue on its own but rather a symptom of several different health issues. It’s a collection of symptoms, such as lack of motivation, irritability, inability to focus, and memory problems. It may generally feel like you’re losing control of your brain or your overall health and wellness. �
If you’ve ever experienced brain fog, you will know that its intensity may differ from day to day, even from one moment to the other. It may also ultimately feel almost as if the exterior world is moving too quickly for you to keep up with it. �
It can also become extremely frustrating if you can’t recall an ideal word during a conversation or in the event that you forget if you’ve locked the door in the morning. You must understand that it’s brain fog and know that it’s not who you really are. However, with long-standing depression, it may also begin to feel as if you’ve just become lethargic and slow. �
Health issues, such as brain fog, can be caused by several different physical and mental health issues. It can be difficult to explain to others that you’re feeling fatigued since it’s often simply mistaken for being tired after a long day of work. �
But fatigue is much more than just being tired. People experiencing fatigue feel tired even after mild exertion. Getting through an average day appears to be a marathon. And waking up feeling unrefreshed is a major indicator that your feelings of fatigue can possibly be a much more intricate health issue associated with inflammation, brain fog and depression. �
Why Depression Causes Brain Fog
Because brain fog can be an indication of many different health issues and not just depression, the relationship between both is not entirely clear. Depression disturbs the balance of the “feel good” chemicals in the brain, known as dopamine, which can also result in a chronic sense of sadness and lack of health and wellness. But that is not the whole story. �
Your upbringing can also set you up with a lack of self-compassion, which the helplessness of brain fog amplifies. Research studies show that these states can relate to elevated inflammatory chemicals that make you feel much more brain fog. �
Another cause of brain fog includes depression medicines, like antidepressants. The purpose of these drugs and/or medications is to relieve depression symptoms and re-establish the balance of chemicals in the brain. �
However, these medicines appear to contribute to brain fog as a side-effect due to the biochemical changes which they cause in the mind. If you feel that your antidepressants may be the actual culprit, it may be well worth monitoring when you experience a brain fog episode. Tracking your symptoms, in general, can help you figure out ways to counter brain fog. �
Research shows that depression negatively affects the brain’s reward system by changing the amount of dopamine, a neurotransmitter involved in feelings of pleasure, reward, and motivation. A reward system that is disrupted can ultimately make it difficult to find the point in spending some energy to perform or participate in regular everyday activities. �
Insomnia, which is distinguished by difficulty falling or staying asleep, is closely related to depression. This usually means that the probability of depression raises since it deprives us of the physical repairs of sleep and power. And having depression, in turn, makes it difficult to get a good night’s sleep because of the cycle of unwanted thoughts. The end-product is, as you may have guessed, unbeatable tiredness or fatigue. After all, brain fog, depression, and fatigue all seem to be connected. �
Brain fog is closely associated with both depression and fatigue. Being open and honest about your symptoms can be a fundamental step in your recovery process. Although inflammation is the human body’s immune response to injury, infection, or illness, too much inflammation can actually cause a variety of health issues. Evidence from research studies has demonstrated that inflammation can ultimately be associated with brain fog, depression, and even fatigue symptoms.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Are you constantly feeling exhausted? Have you been noticing any mood changes? Do you struggle to focus on regular tasks? Brain fog, which includes depression and fatigue, is a problem that can affect your overall health and wellness. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
How often do you become fatigued when driving compared to in the past? Or how often do you become fatigued when reading compared to in the past? And, how often do you feel you are not getting enough sleep or rest? If you experience any of these problems often, you may be experiencing brain inflammation and fatigue due to a variety of health issues. �
Chronic fatigue syndrome (CFS) and other similar health issues, such as Gulf War illness (GWI), share many common symptoms, several of which can include muscle pain and discomfort, fatigue, cognitive impairment, disrupted sleep, sore throat, headaches, and general malaise, typically after participating in any type of physical activity or exercise. �
CFS has frequently been referred to as a mental health issue. In 2015, a National Academy of Medicine-led comprehensive overview of scientific literature and patients’ accounts cautioned that many healthcare professionals are doubtful about the seriousness of CFS, commonly mistaking it for a mental health issue or believe it a figment of the patient’s imagination.” �
Moreover, the research study also supports that healthcare professionals should admit CFS as a health issue which needs diagnosis and treatment. The review also discussed what at the time was ultimately considered unknown causes of CFS. �
Although important progress was developed in the manner that chronic fatigue syndrome (CFS) is diagnosed and perceived in the medical community, there’s currently no known treatment for the health issue and its causes still remain unknown. �
New research studies, however, offer new hope for fast and precise diagnosis of the health issue, as changes in brain chemistry associated with inflammation and neurological diseases have been found. Between 836,000 and 2.5 million people in the United States suffer from CFS. The findings may also help people with CFS receive successful treatment. �
Furthermore, one research study, which was directed by researchers at Georgetown University Medical Center in Washington, D.C., identified changes in brain chemistry that also exist in other similar health issues, such as GWI, a health issue which is ultimately believed to have affected approximately 175,000 war veterans returning from the Gulf War. �
Contents
Analyzing the Brain in Chronic Fatigue Syndrome
Dr. James N. Baraniuk, a professor of medicine at Georgetown University School of Medicine, led the new research study, along with the findings which have been published in the journal Scientific Reports. Dr. Baraniuk and his group of researchers analyzed the cerebrospinal fluid of people with CFS and other health issues, such as GWI, in addition to healthy controls. �
The group pulled the fluid with a lumbar puncture, before and after the individuals participated in a session of physical activity or exercise. The group additionally analyzed the brains of the individuals utilizing functional MRI (fMRI). � The physical activity or exercise sessions lasted for 25 minutes and consisted of riding a stationary bicycle. The bike immunity increased as predicted by their own era, so the participants reached 85 percent of their maximum heart rate. �
Before participating in any physical activities or exercises, amounts of microRNA (miRNA), which are responsible for regulating protein generation, were exactly the exact same in all the individuals participating in the research study. However, 24 hours following the physical activities or exercises, this changed for the three distinct groups of participants. �
Every class had a different pattern of modification. The researchers stated, “CFS had 12 diminished miRNAs following physical activity or exercise.” Despite symptom overlap of CFS, GWI and other health issues in their differential diagnosis, miRNA patterns in cerebrospinal fluid signaled different mechanisms for post-exertional malaise in CFS and GWI. �
Additionally, the analysis also discovered miRNA changes in just two subtypes of GWI. Tachycardia that lasted for two to three days after the workout was developed by 1 subgroup. FMRI investigations revealed that these individuals had smaller brainstems in brain regions responsible for controlling the heartbeat. FMRI scans showed decreased brain activity. �
Another GWI group, however, introduced neither modifications to heart rate nor brainstem atrophy, but its own associates appeared to need extra brain regions so as to do a memory task. Surprisingly, Dr. Baraniuk discussed that the miRNA changes found in such states were different from those observed in depression, fibromyalgia, and Alzheimer’s disease, among others. �
“We certainly see three distinct patterns in the brain’s production of those molecules at the CFS group and both GWI phenotypes. This information will probably be well-received by individuals that suffer from such ailments that are misdiagnosed and rather may be medicated for depression or other psychological disorders,” stated Dr. James N. Baraniuk �
New research studies have demonstrated that changes in brain chemistry associated with inflammation may cause fatigue. Health issues like chronic fatigue syndrome and Gulf War illness are believed to be caused by neuroinflammation and other molecule changes in the brain. In the following article, inflammation and fatigue, can be caused due to a variety of causes, although the causes still remain mostly unknown. Although fatigue may be a frustrating symptom, relief is possible with proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. � Has it become harder for you to learn new things? Or is your temperament generally getting worse? How often do you get fatigued after meals? If you’ve experienced any of these situations, you may have brain inflammation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Lower abdominal pain relieved by passing stool or gas
Alternating constipation and diarrhea
A hard, dry, or small stool
Use laxatives frequently
If you are experiencing any of these situations, then you must be experiencing gastrointestinal impairments in your body.
Gastrointestinal Impairments
The digestive system is consisting of the gastrointestinal tract, which is home to the intestines, the liver, the colon, the gallbladder, the pancreas, and the stomach. When there is a disruption in the gastrointestinal tract, it can cause inflammation and chronic illnesses that can harm the body. Functional disorders in the digestive tract (GI tract) can look normal in the body, but it doesn’t work correctly.
Many factors can upset the GI tract and its motility, including:
Eating a diet low in fiber
Not getting enough exercise
Traveling or changes in a routine
Eating large amounts of dairy blankets
Stress
Resisting the urge to have a bowel movement
Overusing laxatives
Taking certain medicines
Some of the most common problems that can affect the GI tract are constipation, IBS, and colon cancer.
Irritable Bowel Syndrome
IBS (irritable bowel syndrome) is a long term gastrointestinal disorder. It can cause abdominal pain, bloating, mucus in the stool, irregular bowel habits, and can alternate diarrhea and constipation. IBS can cause persistent discomfort to individuals, but they can improve the symptoms over time as they learn to manage the condition.
Some of the symptoms caused by IBS are:
Changes in bowel habits
Abdominal pain and cramping that lessens after using the bathroom
A feeling that the bowels not fully emptied after using the bathroom
Excess gas
The passing of mucus from the rectum
The sudden urgent need to use the bathroom
Swelling or bloating from the abdomen.
Signs and symptoms of IBS can vary between individuals and can often resemble other diseases and conditions. IBS symptoms can often get worst after earing, and a flare-up may last about 2 to 4 days, then the symptoms may either improve or go away entirely, but IBS symptoms can affect different body parts.
These can include:
Frequent urination
Bad breath
Headaches
Joint or muscle pain
Persistent fatigue
Anxiety
Depression
Constipation
Constipation is one of the most common digestive problems that affects around 2.5 million individuals. It is a syndrome that is defined by bowel symptoms (painful or infrequent passage of stool, the hardness of stool, or a feeling of incomplete evacuation) that may occur either in isolation or secondary to another underlying disease like for example, Parkinson’s disease.
The cause of constipation is through the colon. The colon’s main job is to absorb water from leftover food as it passes through the digestive system and creates waste. When the waste is ready to be excreted out, the colon’s muscles propel the waste out through the rectum to eliminate from the body. If the debris remains in the colon for too long, though, it can be tough and challenging to excrete it out of the body.
Some factors can cause constipation; this can include:
Stress
Low-fiber diet
Lack of exercise
Certain medications
Particular diseases like a stroke, Parkinson’s disease, and diabetes
Problems with the colon or rectum
Hormonal issues
Everyone’s definition of a regular bowel movement may be different. Some people can go about three times a day, while others can go to relieve themselves about three times a week. Some of the symptoms of constipation included are:
Fewer than three bowel movements a week
Passing hard, dry stools
Straining or pain during bowel movements
Still feeling full after a bowel movement
Experiencing a rectal blockage
Colon Cancer
Colon cancer is the third most common type of cancer. When tumorous growths develop in the large intestine or the colon, it develops colon cancer in the GI tract. The colon, the one organ where the body draws out water and salt from solid wastes. The waste then moves through the rectum and excretes out of the body through the anus.
Even though colon cancer doesn’t cause any symptoms in the earliest stages, but it can become more noticeable as the disease progresses. Some of the sign and symptoms of colon cancer include:
Diarrhea or constipation
Changes in stool consistency
Loose, narrow stools
Blood in the stool
Abdominal pain
Weakness and fatigue
Iron deficiency
If colon cancer spreads to a new location the gastrointestinal system, it can cause additional problems in the new area.
Conclusion
Having gastrointestinal impairments can cause the body to develop chronic illnesses. There are ways to make sure that the digestive tract is functioning correctly. An individual can change their diets and lifestyle and can make sure that their gut is working properly. When there is a disruption in the GI tract like IBS, constipation, and colon cancer, it can lead to many health problems if the individual is not careful. If an individual prolongs the symptoms, then they will develop life-long issues for their body. Some products help support the intestinal tract and help strengthens the natural defenses and support the intestinal immune function.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bharucha, Adil E, et al. �American Gastroenterological Association Technical Review on Constipation.� Gastroenterology, U.S. National Library of Medicine, Jan. 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3531555/.
Brazier, Yvette. �Irritable Bowel Syndrome (IBS): Symptoms, Diet, Causes, and Treatment.� Medical News Today, MediLexicon International, 18 Dec. 2017, www.medicalnewstoday.com/articles/37063.php.
Crosta, Peter. �Colon Cancer: Symptoms, Treatment, and Causes.� Medical News Today, MediLexicon International, 28 Aug. 2019, www.medicalnewstoday.com/articles/150496.php.
Sethi, Saurabh. �What You Should Know About Constipation.� Healthline, 23 Aug. 2019, www.healthline.com/health/constipation.
Unknown, Unknown. �Digestive Disorders & Gastrointestinal Diseases.� Cleveland Clinic, 2017, my.clevelandclinic.org/health/articles/7040-gastrointestinal-disorders.
Whitfield, K Lynette, and Robert J Shulman. �Treatment Options for Functional Gastrointestinal Disorders: from Empiric to Complementary Approaches.� Pediatric Annals, U.S. National Library of Medicine, May 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2830707/.
The percentage of individuals that are affected by fatigue, headaches, and overall pain is continuously growing. For the most part, these symptoms can all be linked back to a hormone imbalance. Hormone imbalances are more common than individuals realize and can affect people of all ages. Originally, hormone testing was completed through a blood draw (serum testing). However, as science is improving, there are now better, more functional ways of testing.��
As more and more studies are done, it is becoming more clear that salivary testing is superior to serum (blood) testing for hormones. There are two forms in which hormones exist in the human body, free (5%) and protein-bound (95%). Due to the protein-bound hormones being bound, they become too large to pass through into the salivary glands. This meaning that they are not bio-available and can not be delivered to the receptors in the tissues of the body.� The unbound hormones, or free hormones, are the relevant hormones that are found in the saliva. Considering the fact that free hormones are not as abundant, the hormone levels found in saliva are significantly less than those found in serum. However, many patients who are treated with serum hormone results are often overdosed because of the lack of correlation between bio-availability.
Contents
Labrix by Doctor’s Data
Similar to the D.U.T.C.H�hormone testing previously discussed, this company Labrix offers a variety of hormone testing as well.
Neurotransmitters:
NeuroBasic: ideal for monitoring therapeutic interventions of neurotransmitter imbalances previously tested or when symptoms are indicating an imbalance. This test measures Serotonin, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, and Phenethylamine
Comprehensive Neurotransmitter: best when a comprehensive look at neurotransmitter secretion and metabolism of markers is needed. This test measures Serotonin, GABA, Dopamine, Norepinephrine, Epinephrine, Glutamate, Glycine, Histamine, and Phenethylamineand DOPAC, 3-MT, Normetanephrine, Metanephrine, 5-HIAA, Tryptamine, Tyrosine, Tyramine, and Taurine.
NeuroHormones:�
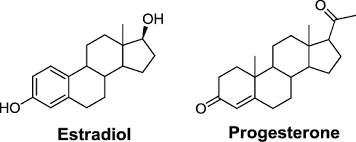
NeuroHormone Complete Plus:� provides insight on how the HPA axis function may be contributing to patients’ symptoms, such as mood swings, fatigue, and pain. In addition, this test is ideal for those who are at risk for breast cancer, PCOS, or a strong family history of autoimmune disease.�This test is recommended for women only.� This test measures�Estrone, Estradiol, Estriol, Progesterone, Testosterone, DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine
NeuroHormone Complete: useful for patients (men or women) who are experiencing any type of mood disorder, addiction, fatigue, chronic illness, confusion, weight issues, low libido, PMS, or chronic pain. This test measures Estradiol, Progesterone, Testosterone, DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine.�
NeuroAdrenal: Included in this test is a full diurnal cortisol pattern, DHEA, and 6 primary neurotransmitters to help those with symptoms such as depression, anxiety, addiction, chronic illness, and low libido. This test measures DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine
Salivary Hormone:�
Comprehensive Plus: provides an assessment of breast cancer risk. This test is a considerationfor women only who have an increased risk for developing breast cancer, other hormonally sensitive cancers, PCOS or a family history of autoimmune disease. This test measures estrone, estriol, and Estrogen Quotient.
Women’s Helth and breast Profile: includes two risk assessment ratios, the Estrogen Quotient and the Pg/E2 ratio
Comprehensive Hormone: �assessment of hormonal status and endocrine function and includes estradiol, progesterone, testosterone, DHEA and four cortisols. This profile is useful with male and female patients because it looks at the full diurnal cortisol pattern; it is especially important in patients who are experiencing the full diurnal pattern ( weight gain, high blood sugar, elevated lipids, chronic fatigue)
Short Comprehensive: useful in men and women whose primary symptoms are related to sex hormone imbalances (elevated or depressed E2, P or T)
Basic Hormone: a basic evaluation of the sex hormones and a brief glimpse at the adrenal function with the AM cortisol level. Best for men who are experiencing decreased libido, erectile dysfunction, loss os stamina, decreased mental sharpness and metabolic syndrome. Best for women who are experiencing hot flashes, anxiety, night sweats, breast tenderness, irritability, forgetfulness, and acne.�
Comprehensive Adrenal Function: provides insight into the body�s stress response. This test measures sIgA
Adrenal Function: comprehensive view of adrenal function, DHEA, and cortisol levels. This is best for people who are fatigued, nervous, weak, crave sugar, have headaches, irritability, and depression
Diurnal Cortisol: Similar to the test above but for patients who do not need DHEA testing
Melatonin: Provides a snapshot of the sleep/wake cycle during a one day period
Salivary Hormone + CAR :
CAR: has the capability to test all the same markers as above but adds Cortisol Awakening Response “CAR” to all of them.�
For more information regarding testing and hormones tested, please visitlabrix.com��
LABRIX BASIC BOX CONTENTS:
Upon opening every box (no matter the labrix test) the patient will see a requisition form, a billable stamp, and a FedEx envelope. Under these two items, a styrofoam box (insulated cooler) with the imprint “doctorsdata.com” will be present. Once the patient lifts the lid off of the styrofoam box, they will see two more pieces of paper.� The first being a list of symptoms (patient survey) on a white sheet of paper that the patient is to fill out and place back in the styrofoam box and the second a small instruction manual.
Neurotransmitter Tests Breakdown
For the Neurotransmitter Tests, the patient is provided with the basic kit described above. The only sample type required for the neurotransmitter tests is urine.
The contents of the styrofoam box include a small plastic cup, a clear plastic bag consisting of a white tube, a dropper, an absorbent pad, and a Lab-Brix ice pack. The first step is to freeze the ice-pack and keep it frozen until ready to ship.�
In order for this test to have proper results, the patient should collect their sample with their first or second-morning urine upon waking. Then, select on the requisition form which urine ( first or second ) the sample was collected from. It is also important to note on the requisition form what time the patient woke and what time the sample was collected. The urine sample should be collected midstream. Patients will collect their sample in the plastic cup provided, not directly in the tube. Next, the patients will use the dropper provided to transfer 10 ml of the sample from the cup into the tube. Ensure the lid is screwed on tightly and gently rock the tube back and forth for 3-5 seconds to mix the urine with the preservative. The patients will then wrap the absorbent pad around the tube (not inside the tube), and place the sample tube back in the plastic bag. The bag is then to be placed in the freezer for 4-6 hours, and is to be kept frozen until ready to ship!�
Neurotransmitter + Hormone Tests Breakdown
The Neurotransmitter + Hormone analysis tests consist of urine and saliva samples. This basic test kit includes everything above. However, upon opening this styrofoam box the patient will find two plastic bags. The first being a plain plastic clear bag with a dropper, white test tube, and absorbent pad. The second plastic bag is a biohazard bag that has multiple colors on the outside and consists of 4 clear small straws, an absorbent pad, and 4 small saliva collection tubes of various colors.�
The urine sample is instructed to be taken the same way as the neurotransmitter test.
The patient should collect their sample with their first or second-morning urine upon waking. Then, select on the requisition form which urine ( first or second ) the sample was collected from. (Remember, the individual is� to note on the requisition form time they woke and what time the sample was collected). Patients will collect their sample mid-stream in the plastic cup provided, not directly in the tube. Next, use the dropper provided to transfer 10 ml of the sample from the cup into the tube. Be sure to check that the lid is screwed on tightly and gently rock the tube back and forth for 3-5 seconds to mix the urine with the preservative. The patients will then wrap the absorbent pad around the tube (not inside the tube), and place the sample tube back in the plastic bag. The bag is then to be placed in the freezer for 4-6 hours, and is to be kept frozen until ready to ship!��
The salivary collection has a few more steps considering it is 4 samples rather than one. The timing for the salivary testing is critical, so timers are encouraged. As the patient wakes up, a timer should be set for 30 minutes later. This is when the first salivary sample (the pink tube) is to be collected. Before this test, the patient should not eat, drink, brush or floss. The second collection (green tube) is to be taken right before lunch, around noon. The third (orange tube), is to be collected in the evening before dinner, and the final collection (blue tube) before bed at night.�
For all salivary collections, each tube needs to be 3/4 of the way full. The straws provided are the patient’s choice to be used. As soon as the tube is 3/4 of the way full, snap the saliva lid tightly, put into the bag in which it came, and freeze for 4-6 hours, until ready to ship. Patients are to record the date and times of the saliva collections on the bag and requisition form.�
Salivary Hormone
Considering the salivary hormone testing is done using 4 saliva samples, the instructions are the same as the saliva collection in the test mentioned above. However, to review them again,�the timing for the salivary testing is critical, so timers are highly encouraged.
As the patient wakes up, a timer should be set for 30 minutes later. This is when the first salivary sample (the pink tube) is to be collected. Before this test, the patient is not to eat, drink, brush or floss. For the second collection (green tube), it should be collected right before lunch, around noon. The third (orange tube), is to be obtained in the evening before dinner, and the final sample (blue tube) before bed at night.�
For all salivary collections, each tube needs to be 3/4 of the way full. The straws provided are to be used at the patient’s discretion. As soon as the tube is 3/4 of the way full, snap the saliva lid tightly, put into the bag in which it came, and freeze for 4-6 hours, until ready to ship. Patients are to record the date and times of the saliva collections on the bag and requisition form.�
Salivary Hormone + CAR Breakdown
Aside from the basic components, the styrofoam box includes 6 colored salvia collection tubes, 6 straws, and an absorbent pad. The tests that fall under this category require 6 samples throughout the day. It is important to remember to write down the time the samples were collected as well as the time when the patient first woke up. The first sample (yellow tube) is to be taken as soon as the patient is awake but has not gotten out of bed. In order to accomplish this properly, it is best the patient sets the tube next to their bed the night before. This makes it easy to collect first thing in the morning. It is very important that the patient sets an alarm for 30 minutes after they wake up ( second test, pink tube)and for 1 hour after they wake up (third test, lavender tube). These tests are all to be done prior to eating breakfast, brushing and flossing teeth. The fourth collection (green tube) is to be taken before lunch and the fifth (orange tube) before dinner. The sixth and final sample (blue tube) is to be collected at least one hour after dinner. Just as the other saliva samples mentioned above, these tubes are to be filled 3/4 of the way, tightly closed, placed back in the bag they came in and frozen for 4-6 hours, or until they are ready to ship.
SHIPPING INSTRUCTIONS FOR ALL TESTS:
Shipping should be done Monday-Friday as this will ensure the sample will be delivered to the lab on time. Make sure all paperwork is filled out properly and place contents back in the styrofoam box in the following order:�
sealed plastic bag with frozen specimen tubes
frozen ice pack�
requisition form, symptom sheet, and payment (if applicable)�
Next, place the lid back on the box and place the entire styrofoam box in the cardboard collection kit. Close the cardboard box and place it inside the FedEx shipping envelope provided. The patient will then write their name and address on the Billable Stamp and tear off the customer receipt for their records. Then, place on the FedEx envelope. The final step is to schedule a pick-up. In order to do this, the patient will call the FedEx toll-Free number at 1-800-463-3339 and select “schedule a pickup”. This MUST be a scheduled pick up from an address and NOT a dropbox.�
* It is important to note that patients should avoid eating avocados, eggplant, tomatoes, bananas, melons, pineapples, plums, nuts, nut butter, wine, cheese and chocolate 48 hours before and during the testing period as these could impact the results.
* Patients should keep in mind that strenuous exercise, alcohol, coffee, tea, tobacco or any other product containing nicotine is to be avoided 24 hours before and during the collection period.
Labrix is a great company that allows patients a noninvasive way to have their hormone levels checked. Almost every patient who walks in the door can benefit from this test. I highly recommend this test because hormone levels can change based on age, PMS symptoms, fatigue, blood sugar issues, or stress! These results are accurate and have a decently quick turn around time. Gaining insight and taking control of your body is now easier than ever. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
*All information and photos/video content for this article are directly sourced from labrix. Please see labrix for more information and credit.
The goal is to have an economical stance and gait that does not require excessive energy.
The curves need to be well-balanced.
The gravity line should fall through:
The head and cervical spine
Behind the sacrum
Through the center of the hips
Like this minimum energy is exerted for standing and walking.
When these curves are not balanced, like what happens with excessive kyphosis in the thoracic spine or loss of normal lordosis in the lumbar spine, the patient may begin to experience symptoms.
Loss of lumbar lordosis or actual kyphosis in the lumbar spine that presents symptoms is named flatback syndrome.
Symptoms
The main symptoms of flatback are:
Difficulty standing up straight
Low back pain
Thigh pain
Groin pain
Symptoms will worsen as the day progresses with fatigue and increasing difficulty to stand up straight with correct posture.
Individuals will flex or bend their hips and knees to get into an upright position.
This is what causes the exhaustion as the day goes on.
Some patients also have symptoms of:
Sciatica
Spinal stenosis
Leg pain
Weakness made worse from walking
Some individuals have neck and upper back pain as they strain to get themselves upright.
Trying to live like this can lead to a disabling condition that requires pain medications, and limits the individual’s ability to perform daily activities.
This was the earliest type of spine implantation to correct scoliosis.
This instrumentation had a tendency to flatten the normal curve or lordosis in the lumbar spine.
This system was used from the 1960s to the 1980s.
With today’s implant systems and techniques, this problem doesn’t really occur anymore.
But not to knock the system, those treated with�Harrington�rods did very well for decades.
The spine compensates for the flattening of the lordosis with the normal discs underneath the fused area.
However, when the discs below the fusion would wear out (degenerate), the patients would lose the ability to stand upright and pain would develop.
Other causes include:
Ankylosing Spondylitis
A chronic inflammatory arthritic disease that causes stiffness and loss of lordosis.
Degenerative Disc Disease
The normal aging process of the wear and tear/degeneration of the discs, that are the shock absorbers of the spine.
In the lumbar area, these discs contribute to normal curvature.
As the discs degenerate, the spine stiffens and the curvature disappears.
The patient has progressive difficulty in achieving an upright posture.
Post-Laminectomy Syndrome
After a laminectomy procedure used to decompress the spine nerves, loss of lordosis and instability can develop.
This type of procedure is associated with failed back surgery syndrome.
Compression Fractures
Single or multiple vertebrae collapsing can result in loss of lordosis and flatback.
The vertebrae are the building blocks of the spine.
Diagnosis
The diagnosis begins with a patient’s history.
A doctor will look for the common symptoms like the presentation of difficulty standing upright along with back pain.
If there is a history of prior surgery or a disease making them susceptible to the syndrome.
Full standing x-rays will be ordered.
The lateral side view is specifically the side that will be helpful (see x-ray).
The patient stands, knees straight, the posture can be seen to be stooped forward.
This is depicted by the gravity line/plumb line falling in front of the sacrum.
Finally, MRI’s, CT scans, can be utilized to provide information about the health of the:
Discs
Vertebrae
Degree of openness of the spinal canal to see if there is compression of the spinal nerves or not
Non-surgical Treatment
Patients should try non-surgical treatment first like:
Chiropractic
Physical therapy
Non-steroidal anti-inflammatory medication
Conditioning and endurance exercise programs can provide relief. But, if the structural problem is too great for conservative therapy then surgery is an option.
Proven Reduced Back Pain with *FOOT ORTHOTICS* | El Paso, Tx
In a recent research study published by the American Congress of Rehabilitation Medicine (ACRM), researchers demonstrated that Foot Levelers custom foot orthotics help considerably reduce back pain and several of its associated health issues.
The research study also demonstrated that Foot Levelers custom foot orthotics and chiropractic care help tremendously reduce low back pain and sciatica.
Foot Levelers custom foot orthotics and chiropractic care helped improve the patient’s overall health and wellness.
Dr. Jimenez is a chiropractor in El Paso, TX who can help provide these benefits through the utilization of chiropractic care and Foot Levelers custom foot orthotics, among other treatments.
NCBI Resources
Sometimes low back pain comes out of nowhere, but that sudden twinge in the lower back does have a cause. With some cases, there�s a�trigger, like picking up a heavy object/furniture from an awkward position.� But sometimes it can be a mystery and a challenge to diagnose.
It is important to know the cause of lower back pain to figure out the proper treatment plan. Otherwise, one could receive treatment for the wrong diagnosis and possibly exacerbate the existing injury.
Is your memory noticeably declining? Are you having a hard time remembering names and phone numbers? Or is your ability to focus noticeably declining? If you’ve experienced any of these situations, you may ultimately be experiencing brain fog. �
Contents
What is Brain Fog?
Brain fog is not a health issue but rather a symptom of other injuries or conditions. It is a cognitive dysfunction involving: �
memory problems
lack of mental clarity
poor concentration
inability to focus
Several people can also experience brain fog as mental fatigue. Based on the seriousness of brain fog, it may ultimately interfere with work, school, or any other regular tasks. However, it doesn’t have to be a permanent problem in your lifetime. �
What Causes Brain Fog?
There are many reasons why brain fog happens. By identifying the underlying reason, you may fix the health issue. �
Stress
Chronic stress can raise blood pressure, weaken the immune system, and trigger anxiety, depression, and other mood changes. It can also result in fatigue. It becomes more difficult to think, reason, and focus when your mind is tired. �
Lack of Sleep
Poor sleep quality may also interfere with how well your brain works. Try to get between 8 to 9 hours of sleep each night. Lack of sleep, or sleeping too little. may ultimately lead to poor concentration and cloudy thoughts, among other symptoms. �
Hormonal Changes
Hormonal changes can also activate brain fog, including increased levels of estrogen and the growth of the hormones progesterone. Memory can also be affected by hormonal changes and may cause short-term cognitive impairment. �
Similarly, a drop in estrogen levels during menopause can cause forgetfulness, poor concentration, and cloudy thinking. �
Diet
Diet may also play a part in brain fog. Vitamin B-12 supports healthy brain function and a vitamin B-12 deficiency can result in brain fog. Similar to food allergies or sensitivities, brain fog can also develop after eating particular foods, including: �
MSG
aspartame
peanuts
dairy
Eliminating trigger foods out of your diet and consuming more anti-inflammatory foods can ultimately improve symptoms. �
Medications
If you begin to experience brain fog whilst taking any types of drugs and/or medications, talk to your doctor. Brain fog may be a side effect. Reducing your dosage or switching to different medications may also help improve your symptoms. � Moreover, brain fog can also happen after certain cancer treatments. This is most commonly known as the chemo brain. �
Other Health Issues
Other health issues associated with inflammation, fatigue, or changes in blood sugar levels, can also cause brain fog as well as mental fatigue. By way of instance, brain fog is a symptom of chronic fatigue syndrome, which involves mental fatigue. � People who have fibromyalgia can also experience brain fog. Other health issues that may cause brain fog includes: �
anemia
depression
diabetes
Sjo?gren syndrome
migraines
Alzheimer�s disease
hypothyroidism
autoimmune diseases, such as lupus, arthritis, and multiple sclerosis
dehydration
Brain Fog Diagnosis and Treatment
Talk to your doctor if you have a persistent absence of clarity that worsens or doesn’t improve. A test can’t diagnose brain fog. Brain fog may indicate an underlying problem. Your doctor will conduct a physical examination and discuss your: �
mental health
diet
level of physical activity
current medications or supplements
You should tell your doctor about any other symptoms you may have. By way of instance, people with hypothyroidism may also have weight gain, dry skin, and hair loss. Blood work can also help identify brain fog. A blood test can also determine: �
abnormal glucose levels
poor liver, kidney, and thyroid function
nutritional deficiencies
infections
inflammatory diseases
Based on the results, your doctor will decide whether to investigate the diagnosis further. Diagnostic tools may include imaging tests to look within the body, such as X-rays, MRI, or CT scans. The doctor can also conduct allergy testing or a sleep study to check for a sleeping disorder. Keeping a food diary can help you determine if your diet contributes to brain fog. �
Brain fog treatment is dependent upon the cause. By way of instance, if you are anemic, iron supplements may boost your production of red blood cells and reduce your brain fog. If you’re diagnosed with an autoimmune disorder, your doctor may suggest a corticosteroid or alternative medication to help decrease inflammation or to suppress the immune system. �
Furthermore, relieving brain fog may ultimately be an easy matter of simply correcting a nutritional deficiency, altering medications, or even improving the quality of your sleep. Home remedies to help improve brain fog can include: �
sleeping 8 to 9 hours per night
managing stress by knowing your limitations and avoiding excessive alcohol and caffeine
exercising
strengthening your brainpower (try volunteering or solving brain puzzles)
finding enjoyable activities
increasing your intake of protein, fruits, vegetables, and healthy fats
Brain inflammation has been associated with a variety of symptoms, including brain fog. Inflammation is an essential function of the immune system, however, excess brain inflammation, can cause brain fog and a variety of other symptoms. In the following article, inflammation and brain fog, can be caused due to a variety of causes. Although brain fog may be a frustrating symptom, relief is possible with proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Has it become harder for you to learn new things? How often do you have a hard time remembering your appointments? Or is your temperament generally getting worse? If you’ve experienced these situations, you may have brain fog. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Do you feel that you must have sweets after meals? Do you get light-headed if you miss a meal? Or feel that craving for sweets during the day? Does your body feels shaky jittery or have tremors? If you are experiencing any of these situations, you may be experiencing LADA.
Contents
LADA
Autoimmune diabetes is a heterogeneous disease that can arise at any age. Anyone with adult-onset autoimmune diabetes who does not necessitate insulin therapy for at least six months after being diagnosed may have LADA (latent autoimmune diabetes of adulthood). LADA is a slowly progressing form of autoimmune diabetes, and it has been estimated that 20% of people are diagnosed with having non-obesity-related type 2 diabetes.
LADA occurs when the pancreas stops producing adequate insulin and slowly damages the insulin-producing cells in the pancreas, harming the body�s function. It is clear, however, that the frequency of autoimmune diabetes among adults can be underestimated, and clinical features such as age and severity of symptoms are of no help in identifying patients that have LADA since there is still more research being done to treat LADA. The body mass index and C peptide levels in the general population can increase with age, and these parameters are of limited use in identifying LADA patients.
Different Types of Diabetes
In a person, diabetes is a condition that impairs the body’s ability to process blood glucose, and roughly the estimated number of people over 18 years of age that are diagnosed and undiagnosed with diabetes is about 30.2 million. Without ongoing, careful management, diabetes can lead to a build-up of sugars in the blood, which can increase the risk of dangerous complications, including stroke and heart disease.
There are different kinds of diabetes, including LADA, that can occur, and managing the condition depends on the type of diabetes an individual has.
Type 1 Diabetes
Type 1 diabetes is also known as juvenile diabetes, and the body does not produce enough insulin, and the blood glucose level remains high in the body. People with type 1 diabetes are insulin-dependent and must take artificial insulin daily to stay alive. The immune system attacks a cluster of cells known as islets in the pancreas that would typically produce insulin and stopping or slowing down the insulin production in the body.
When a person receives a diagnosis of type 1 diabetes from healthcare professionals, the islet cells are responsible for insulin secretion from the pancreas may continue to produce the insulin hormone for a while before ceasing. It can also lead to the production of LADA if it is not being monitored.
The physical effects of type 1 diabetes include:
Increased hunger and thirst
Frequent urination
Blurry vision
Tiredness and fatigue
Weight loss without an apparent trigger or causes.
Type 2 Diabetes
Type 2 diabetes is one of the most common forms of diabetes and can appear at any age, affecting over 30 million Americans. It happens when the blood sugar levels rise due to problems with the use or production of insulin.
Studies show that most people do not experience the symptoms in the early stages of type 2 diabetes, and they might have symptoms for many years. For those that do have type 2, diabetes may have acanthosis nigricans. Acanthosis nigricans is a skin condition that causes the skin to become thicker and darker. It often appears mostly on the neck, elbows, knees, knuckles, the folds around the neck and the groin.
Other early symptoms of type 2 diabetes that an individual may have included:
Frequent bladder, kidneys, or skin infections
Cuts that take longer to heal
Fatigue
Extreme hunger
Increased thirst
Urinary frequency
Blurred vision
Mixed Diabetes (Type 1.5)
Mixed diabetes or LADA is an autoimmune condition that shares the characteristics of both type 1 and type 2 diabetes in adults. It is diagnosed during adulthood and sets in the bloodstream gradually; however, unlike type 2, LADA is an autoimmune disease and is not reversible if the person changes their diet and lifestyle. �It can be triggered by the damage done to the pancreas from the antibodies against the insulin-producing cells.
If a person has LADA, their beta cells stop functioning much more quickly than type 2 diabetes. Researchers have found out that an estimated 10 percent of people who have diabetes will have LADA. It stated that the treatment for LADA patients is far less elucidated than the cases for type 1 and type 2 diabetes. Finding a treatment strategy for LADA can reduce the decline of beta-cell function, ensures adequate metabolic treatment so far.
Some of the symptoms that LADA patients may have include:
Frequent thirst
Increased urination, including at night
Unexplained weight loss
Blurred vision
Tingling nerves
If LADA is left untreated, it can lead to diabetic ketoacidosis, which is a condition where the body can not utilize sugar as fuel due to the absence of insulin and starts burning fat. It produces ketones, which are toxic to the body.
Type 3 Diabetes
Type 3 diabetes is known as brain diabetes and has an established linked to Alzheimer’s disease. This type of diabetes is triggered by a type of insulin resistance and an insulin-like growth factor dysfunction that occurs specifically in the brain, causing dementia.
Alzheimer�s disease has characteristics histopathological, molecular, and biochemical abnormalities in the brain’s cell structure. Since it has been linked with type 3 diabetes, characteristic features of type 3 diabetes include impairments in insulin actions and signaling that result in chronic hyperglycemia, irrespective of subtype, etiology, pathogenesis, or insulin availability.
Conclusion
Autoimmune diabetes can affect anyone at any age. It can damage the pancreas walls to stop producing insulin to the body, causing problems for an individual. LADA (latent autoimmune diabetes in adults) is an autoimmune disease that has the characteristics of type 1 and type 2 diabetes that are in adults. There is still more research being done to treat LADA, and there are products that can help support sugar metabolism and maintain blood sugar levels to a healthy range.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Barhum, Lana. �Type 2 Diabetes: Symptoms, Early Signs, and Complications.� Medical News Today, MediLexicon International, 16 Apr. 2019, www.medicalnewstoday.com/articles/317462.php.
Castro, M. Regina. �Latent Autoimmune Diabetes in Adults (LADA): What Is It?� Mayo Clinic, Mayo Foundation for Medical Education and Research, 10 May 2019, www.mayoclinic.org/diseases-conditions/type-1-diabetes/expert-answers/lada-diabetes/faq-20057880.
de la Monte, Suzanne M, and Jack R Wands. �Alzheimer’s Disease Is Type 3 Diabetes-Evidence Reviewed.� Journal of Diabetes Science and Technology, Diabetes Technology Society, Nov. 2008, www.ncbi.nlm.nih.gov/pmc/articles/PMC2769828/.
Felman, Adam. �Type 1 Diabetes: Overview, Symptoms, and Treatment.� Medical News Today, MediLexicon International, 19 Nov. 2018, www.medicalnewstoday.com/articles/323729.php.
Hals, Ingrid K. �Treatment of Latent Autoimmune Diabetes in Adults: What Is Best?� Current Diabetes Reviews, U.S. National Library of Medicine, 2019, www.ncbi.nlm.nih.gov/pubmed/30009709.
Leonard, Jayne. �Acanthosis Nigricans: Causes, Symptoms, Treatment, and Pictures.� Medical News Today, MediLexicon International, 21 Dec. 2018, www.medicalnewstoday.com/articles/324062.php.
MSN, Rachel Nall RN. �Diabetes: Symptoms, Treatment, and Early Diagnosis.� Medical News Today, MediLexicon International, 8 Nov. 2018, www.medicalnewstoday.com/articles/323627.php.
Pozzilli, Paolo, and Silvia Pieralice. �Latent Autoimmune Diabetes in Adults: Current Status and New Horizons.� Endocrinology and Metabolism (Seoul, Korea), Korean Endocrine Society, June 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC6021307/.
Prelipcean, Maria S. �What You Need to Know About Type 1.5 Diabetes.� Healthline, 2 Nov. 2018, www.healthline.com/health/type-1-5-diabetes.
Watson, Kathryn. �Type 3 Diabetes and Alzheimer’s Disease: What You Need to Know.� Healthline, 16 Oct. 2019, www.healthline.com/health/type-3-diabetes.
Wint, Carmella, and Marijane Leonard. �What You Should Know About Diabetic Ketoacid.� Healthline, 4 Dec. 2018, www.healthline.com/health/type-2-diabetes/ketoacidosis.
A doctor will rule out these causes to make a proper diagnosis.
Diagnosing
A doctor utilizes medical history and physical exam to diagnose coccydynia.
Imaging scans are usually not necessary, but a doctor may order:
Computed tomography (CT) scan
Magnetic resonance imaging (MRI) scan
If they believe a separate:
Bone
Nerve
Tissue
Problem to be the cause of tailbone pain.
Medical history is important, a doctor wants to know if a
Fall
Accident
Recent trauma
Might have caused the pain.
A physical exam is next in line along with symptoms.
The pain is usually localized in the tailbone, making it straightforward to diagnose.
A doctor will want to know if the pain strikes when sitting or leaning back and which is worse.
A doctor might ask the patient to point to where they’re feeling the pain.
Pointing could be enough for the doctor to tell if the pain is coccydynia when compared to other low back pain conditions.
The doctor will want to palpate the tailbone area for signs of inflammation.
Non-surgical Treatment
Conservative treatment is extremely effective for coccydynia.
Ninety percent of people experience pain reduction using non-surgical means or any medical intervention.
It is first treated with noninvasive methods:
Ice or heating pad can help provide immediate, short-term relief.
Donut/Wedge cushion provides extra padding taking the pressure off the coccyx when sitting. These cushions are available at pharmacies.
Avoid sitting for long times, like a long flight will help prevent additional pain and injury.
Rest is very important to help avoid further injury during recovery.
If there is still pain after these therapies, a doctor may recommend over-the-counter or prescription-strength non-steroidal anti-inflammatory drugs (NSAIDs) or other pain medications.
If the medication doesn’t work then a doctor may try cortisone injection or local spine blocker to send strong medicine directly to the tailbone area.
Surgical Procedure
If none of the conservative treatments work then surgery could be the next step.
The procedure is called a coccygectomy, which means the removal of the tailbone.
A surgeon will discuss the procedure in great detail before it is performed.
These risks include:
Infection
Hematoma (abnormal collection of blood outside an artery or vein)
Perineal hernia (weakened pelvic muscles)
Chronic Coccydynia
A small portion of people can develop chronic coccydynia, which means the pain lasts for more than 2 months.
Chronic coccydynia can take a major toll on the quality of life. Talk to a doctor if symptoms are not resolving.
They may refer you to a doctor that specializes in coccydynia management.
Protecting the Tailbone
There is no exact way or method to prevent coccydynia,
However, reducing the risk of tailbone pain can be achieved by using caution when participating in sports like:
Skating – Ice, Inline, and Roller
Biking
Horseback riding
And take extra care when walking on icy/slippery/hazardous conditions so nobody falls.
El Paso, TX Severe Back Pain Chiropractic Treatment
Gale Grijalva suffered from acute back pain because of an automobile incident injury. Where it was once very tough to do her routine daily tasks, Gale Grijalva is now able to take part in physical activities she was not able to engage in earlier thanks to Dr. Alex Jimenez, a chiropractor in El Paso, TX. Gale Grijalva clarifies how patient Dr. Jimenez is and she discusses how completely he’s been able to help her, such as answering any concerns she might have.
Severe chronic back pain is a serious, recurring condition that affects an individual’s everyday life. Back pain lasting over three weeks is deemed chronic. The backbone is an essential component of the body. Severe chronic back pain might be the backbone’s way of telling the body that there’s a problem. The spine consists of bony vertebrae, soft spinal discs, facet joints, tendons, ligaments, and tendons. Within the bony vertebral artery lies that the spinal cord, the delicate but effective nerve pathway of the central nervous system.
NCBI Resources
Before you run screaming in horror to the medicine cabinet, one of the best reasons to participate in chiropractic treatment is that it helps reduce the chance of a recurrence. By working on the total body and getting it in the best shape possible, the patient is stronger and more balanced to handle their workload and other strenuous activities. Chiropractors also impart advice on how to minimize the chances of re-aggravating the lower back.
Millions of people suffer from back pain each year, and some never visit a chiropractor. Those who do choose�chiropractic treatment�are privy to treatment that reduces their pain, increases healing, shortens their downtime and lessens their chances of a recurrence. If over the counter medication and ice packs haven�t worked within a few days, it�s time to make an appointment for a consultation with a licensed chiropractor. You will be happy you did.
Microbes have multicellular hosts and can have many effects on the host�s health and well-being. Researchers have stated that microbes influence metabolism, immunity, and behavior on the human body. One of the most important but understudied mechanisms that microbes have is that they can involve hormones. In the presence of gut microbiota, specific changes in hormone levels can correlate in the gut. The gut microbiota can produce and secrete hormones, respond to the host hormones, and regulate their expression levels. There is also a link between the endocrine system and the gut microbiota as more information is still being researched.
Contents
The Gut to Hormone Connection
Since the human microbiome contains a vast array of microbes and genes that shows a higher complexity. Unlike other organs in the body, the gut microbiota’s function is not fully understood yet but can be disrupted easily by antibiotics, diet, or surgery. The best-characterized function is how the gut microbiota interacts with the endocrine system in the body.
Emerging research has indicated that the gut microbiome plays a central role in regulating estrogen levels within the body. When the estrogen hormone levels are too high or too low, it can lead to the risk of developing estrogen-related diseases like endometriosis, polycystic ovary syndrome, breast cancer, and prostate cancer to males and females.
The gut to hormone connection is essential since the gut is one of the producers to create hormones that travel through the entire body system. With the endocrine system is being involved, it is the first network to produce and transport hormones to the organs that need the hormones to function. When there is an imbalance of hormones in the human body, it can disrupt all the other hormones.
The gut microbiota influences nearly every hormone that the endocrine system creates, including:
The thyroid hormones
Estrogen hormones
Stress hormones
Thyroid Hormones
If the gut has inflammation, then the hormones in the body will create an excessive or low quantity in the body. If the endocrine glands like thyroid, are producing a low quantity of hormones and the gut can be imbalanced and lead to hypothyroidism. When there is low microbial diversity in the gut, studies have shown that the low microbial diversity is linked to high TSH (thyroid-stimulating hormone) levels. The excessive quantity of thyroid hormones can lead to hyperthyroidism. Both hyperthyroidism and hypothyroidism can cause symptoms like irritability, anxiety, poor memory, and many symptoms that can affect the body.
“If you are experiencing excessive belching, burping, bloating, difficult bowel movements difficulty digesting proteins and meats; undigested food found in stools, digestive problems subside with rest and relaxation or any symptoms. Then this article will give you a better understand what is happening with the gut and how hormones can affect the gut system.”
Estrogen Hormones
The gut and an individual’s hormones are meant to be in communication with each other. They not only support each other, but they also work together to make sure the body is running smoothly. Studies have found out that the gut’s intestinal cells have special receptors for hormones that allow them to detect any hormonal shifts that affect the body.
Since estrogen is typically associated with women, it is common that men need the right amount of estrogen levels to function. The gut microbiota is the key regulator of leveling and circulating estrogen in the body. The microbes produce an enzyme called beta-glucuronidase, which then converts the estrogen hormone to its active form.
The gut microbiome can regulate estrogen levels by functioning a specific bacteria in the microbiome called estrobolome. Estrobolome is the aggregates of enteric bacterial genes that are capable of metabolizing estrogen. It might affect women’s risk of developing postmenopausal estrogen receptor-positive breast cancer. The estrobolome is highly essential to keep estrogen levels in the body at a stable state.
In the gut microbiota, both the estrogen and progesterone hormones can impact the guts’ motility and peristalsis ( The rhythmic movement of the intestines that move food through the stomach and out of the body) by playing opposing roles in the guts� motility. Progesterone helps slow down the gut�s motility by relaxing the smooth and slowing transit the time the food is moving out of the body. Estrogen helps increase the contraction of the smooth muscles in the intestines. When the estrogen hormones are leveled right, it can help keep the gut moving smoothly and help increase the diversity of the body�s microbiomes, which is a good thing for the immune system.
Stress Hormones
Stress hormones or cortisol plays a massive part in the gut microbiota. Since cortisol hormones connect to the brain, it sends the signals to the gut and vice versa. If it is a short stressor like getting ready for a presentation or a job interview, the person will feel “butterflies” in their gut. The longer stressors, for example, like having a highly stressful job or feeling anxious consistently, can lead to chronic illnesses in the gut like inflammation or leaky gut. Since the hormone and gut connection is in sync with the gut and brain connection, it is crucial to lowering the cortisol levels to a stable state for a healthy functional body.
Conclusion
The gut and hormone connections are profoundly meaningful since they are linked closely together. When there is a disruption on the gut, it can cause hormones to be imbalanced, causing many disruptions like inflammation and leaky gut. When there is a disruption in the hormones, it can disrupt the gut as well by negatively shifting the gut’s microbiome. So to ensure that the gut is functioning correctly, it is crucial to eat food that contains probiotics and is fermented to keep the gut flora healthy. Some products can help counter the metabolic effects of temporary stress and supporting estrogen metabolism by incorporating other essential nutrients and cofactors to support the endocrine system.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Author, Guest. �How Your Gut Microbiome Influences Your Hormones.� Bulletproof, 21 Aug. 2019, www.bulletproof.com/gut-health/gut-microbiome-hormones/.
Evans, James M, et al. �The Gut Microbiome: the Role of a Virtual Organ in the Endocrinology of the Host.� The Journal of Endocrinology, U.S. National Library of Medicine, 28 Aug. 2013, www.ncbi.nlm.nih.gov/pubmed/23833275.
Kresser, Chris. �The Gut�Hormone Connection: How Gut Microbes Influence Estrogen Levels.� Kresser Institute, Kresserinstitute.com, 10 Oct. 2019, kresserinstitute.com/gut-hormone-connection-gut-microbes-influence-estrogen-levels/.
Kwa, Maryann, et al. �The Intestinal Microbiome and Estrogen Receptor-Positive Female Breast Cancer.� Journal of the National Cancer Institute, Oxford University Press, 22 Apr. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC5017946/.
Neuman, Hadar, et al. �Microbial Endocrinology: the Interplay between the Microbiota and the Endocrine System.� OUP Academic, Oxford University Press, 20 Feb. 2015, academic.oup.com/femsre/article/39/4/509/2467625.
Szkudlinski, Mariusz W, et al. �Thyroid-Stimulating Hormone and Thyroid-Stimulating Hormone Receptor Structure-Function Relationships.� Physiological Reviews, U.S. National Library of Medicine, Apr. 2002, www.ncbi.nlm.nih.gov/pubmed/11917095.
Wieselman, Brie. �Why Your Gut Health and Microbiome Make-or-Break Your Hormone Balance.� Brie Wieselman, 28 Sept. 2018, briewieselman.com/why-your-gut-health-and-microbiome-make-or-break-your-hormone-balance/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
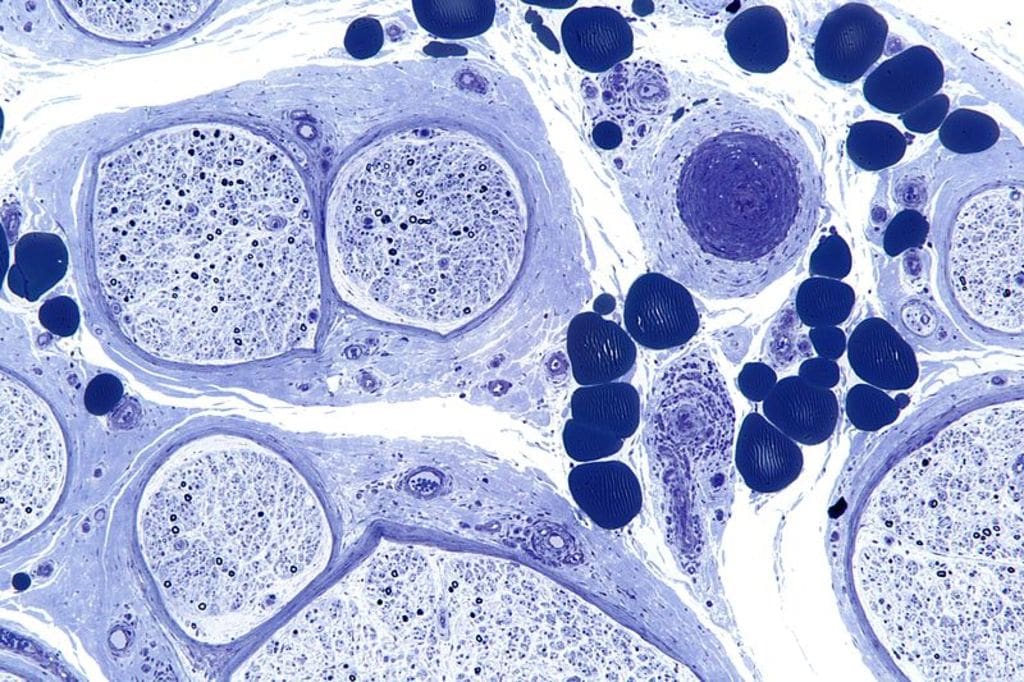





 The digestive system is consisting of the gastrointestinal tract, which is home to the intestines, the liver, the colon, the gallbladder, the pancreas, and the stomach. When there is a disruption in the gastrointestinal tract, it can cause inflammation and chronic illnesses that can harm the body.
The digestive system is consisting of the gastrointestinal tract, which is home to the intestines, the liver, the colon, the gallbladder, the pancreas, and the stomach. When there is a disruption in the gastrointestinal tract, it can cause inflammation and chronic illnesses that can harm the body. 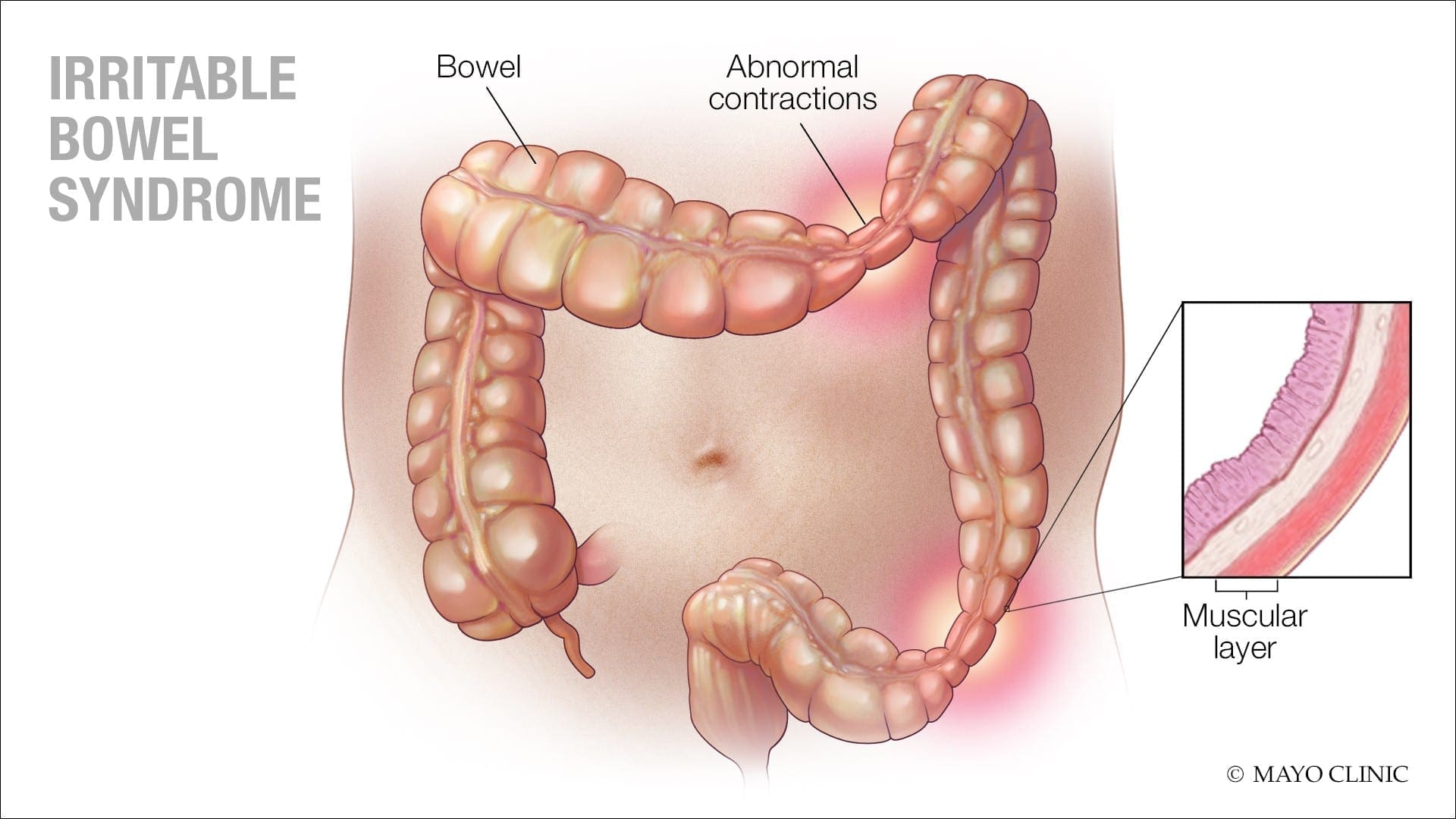 Some of the symptoms caused by IBS are:
Some of the symptoms caused by IBS are:
 The cause of constipation is through the colon. The colon’s main job is to absorb water from leftover food as it passes through the digestive system and creates waste. When the waste is ready to be excreted out, the colon’s muscles propel the waste out through the rectum to eliminate from the body. If the debris remains in the colon for too long, though, it can be tough and challenging to excrete it out of the body.
Some factors can cause constipation; this can include:
The cause of constipation is through the colon. The colon’s main job is to absorb water from leftover food as it passes through the digestive system and creates waste. When the waste is ready to be excreted out, the colon’s muscles propel the waste out through the rectum to eliminate from the body. If the debris remains in the colon for too long, though, it can be tough and challenging to excrete it out of the body.
Some factors can cause constipation; this can include:
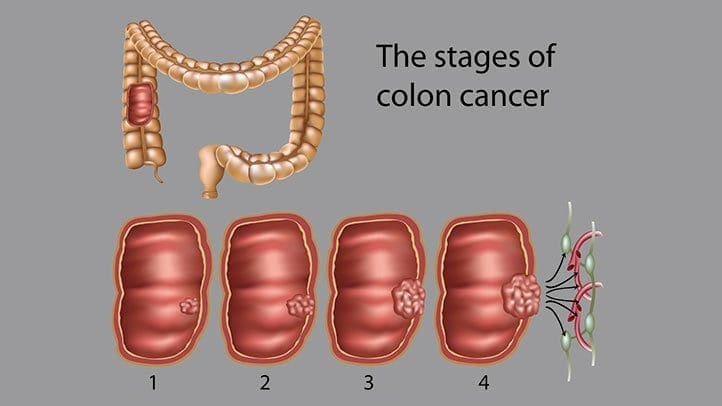 Even though colon cancer doesn’t cause any symptoms in the earliest stages, but it can become more noticeable as the disease progresses. Some of the sign and symptoms of colon cancer include:
Even though colon cancer doesn’t cause any symptoms in the earliest stages, but it can become more noticeable as the disease progresses. Some of the sign and symptoms of colon cancer include:




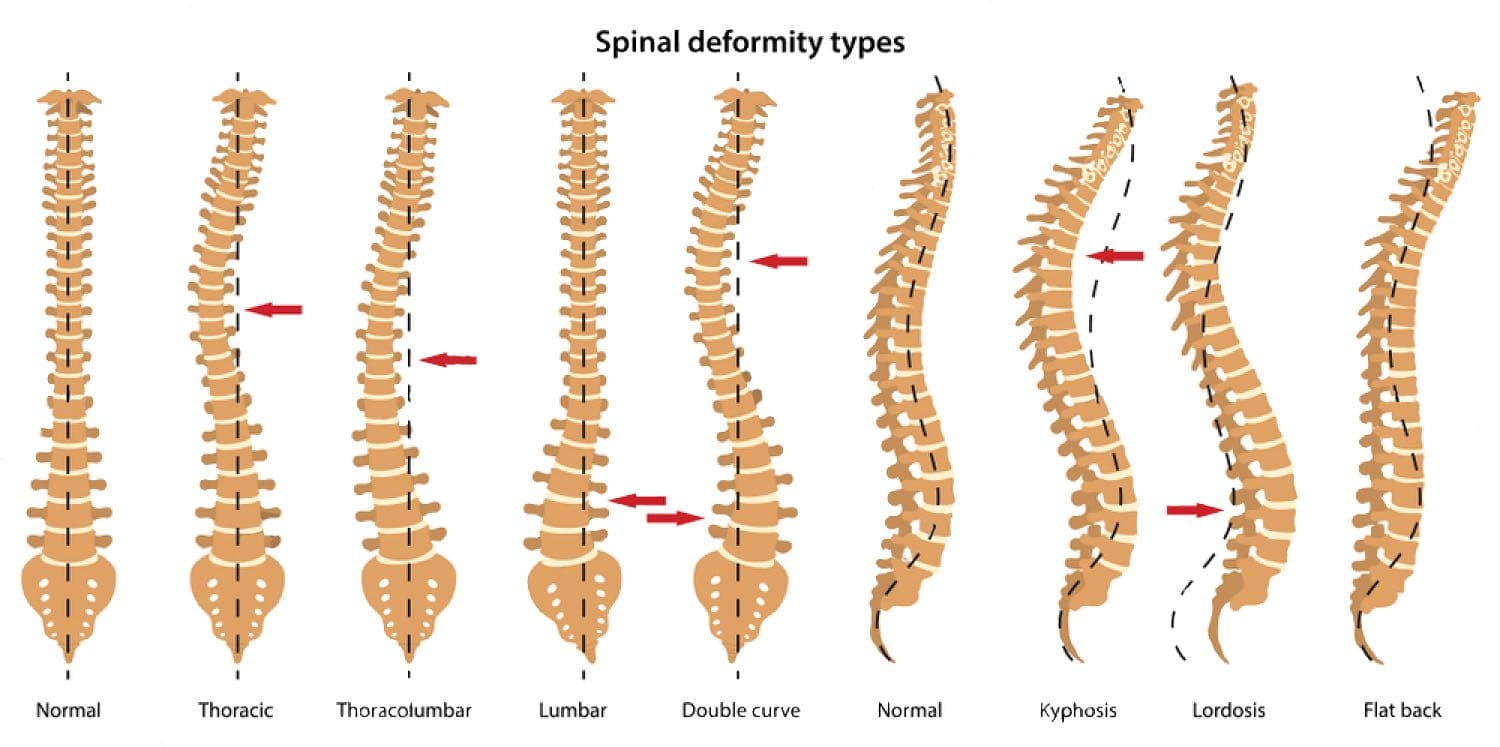

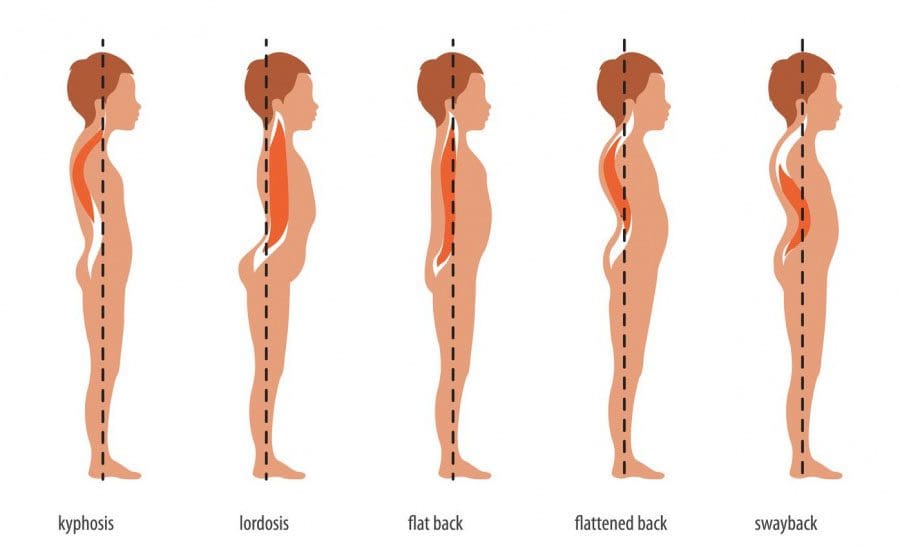

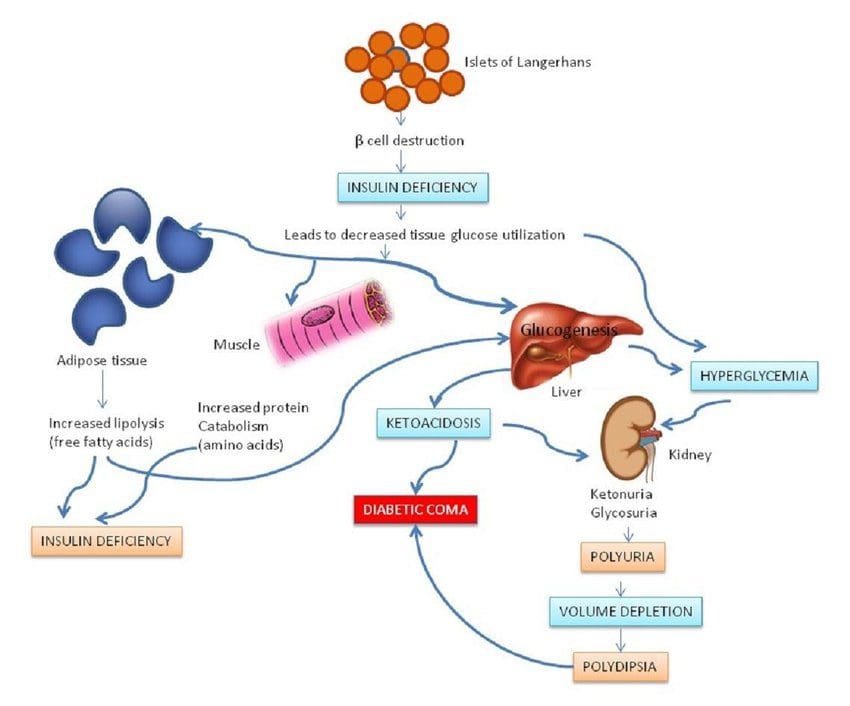 When a person receives a diagnosis of type 1 diabetes from healthcare professionals, the islet cells are responsible for insulin secretion from the pancreas may continue to produce the insulin hormone for a while before ceasing. It can also lead to the production of LADA if it is not being monitored.
The physical effects of type 1 diabetes include:
When a person receives a diagnosis of type 1 diabetes from healthcare professionals, the islet cells are responsible for insulin secretion from the pancreas may continue to produce the insulin hormone for a while before ceasing. It can also lead to the production of LADA if it is not being monitored.
The physical effects of type 1 diabetes include:

 If a person has LADA, their beta cells stop functioning much more quickly than type 2 diabetes.
If a person has LADA, their beta cells stop functioning much more quickly than type 2 diabetes.