Part of understanding the body and treating symptoms such as fatigue, headaches, joint pain, and overall discomfort is realizing that the body is an intricate system that functions as one. In modern medicine, we have become used to seeing different specialists for different body systems ( i.e the endocrine system, the nervous system, etc.). However, in all reality, the body is made up of all these systems to work together to maintain homeostasis.
Wellness is best defined by the National Wellness Institute as, ” An active process through which people become aware of, and make a choice toward, a more successful existence (The Six Dimensions Of Wellness)”.
In general, wellness is applied in one’s life to incorporate all aspects of health. Similar to the systems in the body, wellness is not just isolated to one part. The National Wellness Institute has promoted and defined there to be six dimensions of wellness.
Emotional
Occupational
Physical
Social
Intellectual
Spiritual
These dimensions dive deep to incorporate mental health and physical health. Mental and physical health are closely intertwined and often times relate to each other. By applying the six dimensions of wellness into your life, you are treating the body as a whole and allowing yourself to embrace the mind-body connection for optimal wellness.
Emotional:
The ability to be alone and have your own feelings and thoughts not overwhelm you, expressing emotions in a healthy way, and to be able to be compassionate towards others’ emotional state.
Occupational:�
The work you put in every day and understanding that it has a purpose and point to fulfill not only the necessary job duties but also the soul.
Physical:
The practice of regular physical activity, healthy eating/nutrition, and a regular healthy sleep schedule. These are essential elements to fuel life and heal the body.
Social:
To be able to regularly socialize and react with others. This includes interacting with people in all aspects of life and engaging in a healthy living environment.
Intellectual:
Not only referring to education, but allowing the mind to open up and connect to the lively world around.� Intellectual wellness has a main focus of creativity while exploring problem-solving and critical thinking.
Spiritual:
Knowing that there is a purpose in life that the life you are living is meaningful.
Essentially, by applying these six dimensions of wellness into everyday life, a person becomes more aware of how each dimension is connected to another and how they contribute to healthy living. Emotional health has a lot to do with mental health. By aligning emotional health with mental health, the physical health the body receives is less inflammation, a healthier gut, and more mental clarity.
Similarly speaking, occupational health has a lot to do with physical health. If the occupation one has is constantly exhausting them and causing high levels of stress, the hormones in their body will start to become off balance. This will affect their health in the way that they will not be sleeping as well, causing fatigue and the body to react with inflammation because it is not getting an adequate amount of rest to properly heal.
Physical health is important because by incorporating regular physical activity into one’s life, endorphins will be released more often. Physical activity is used to treat many mental health disorders as well as prevent many physical disabilities.
Often times, anxiety or stomach issues can be brought on by social events. Social wellness works on healthy communications with others around you while also being able to be comfortable and confident.
Intellectual wellness happens as individuals explore and connect with others. If one is not complete or working on the intellectual wellness side of things, this can cause depression and poor health due to not being stimulated and interactive.
The last dimension of wellness is spiritual.� Spiritual wellness does not mean that you believe in a specific thing, but rather that your life has a meaning and you have a purpose.
By incorporating these six dimensions, it allows the human body to connect with itself. by opening up the communication between the systems, a new level of wellness can be achieved.
The six dimensions of wellness is a more holistic approach to healthy living. These dimensions will help individuals reach their full potential while learning and acknowledging their strengths and weaknesses when it comes to health. I highly recommend incorporating the six dimensions of wellness into everyone’s life as the healing benefits it can bring are remarkable. Treating the body as a whole and realizing that your gut health is related to your brain health is eye-opening and creates a lot of room for potential healing. – Kenna Vaughn, Senior Health Coach�
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Keyboards and mice come in all sorts of colors and styles, which is great but for those that work on a computer for a job, using the right type is essential to prevent injury keeping the hands, wrists, and arms healthy and moving.
Overuse can cause painful musculoskeletal disorders like:
There are a variety of ergonomic designs for these devices. Keyboard designs include four separate key areas:
The alphanumeric area with letters, numbers, and control keys
An area with cursor keys
Numeric keypad
Function keys or the ‘F’ keys
Contents
Keyboard Key Combinations or The Mouse
Basic typing and many other actions can be performed on the keyboard using the:
Function keys
Cursor keys
Control keys
Keyboard macros
Pretty much all of these actions can be done with the mouse. Many users operate the computer with the mouse instead of using the key combinations.
To obtain correct posture when working align the center of your body with the center of the keyboard area used the most or during a task.
Keyboard Layout
The layout follows the original ASDF design from the first typewriter.
From the beginning of this design, there was a realization that angling and splitting the keys would reduce the bending of the hands. The first split keyboard typewriter was manufactured in 1886.
The idea of splitting and angling the keys was implemented into ergonomic keyboard designs with the alphanumeric keys being separated at an angle into two sloped sections. For a� non-touch typist, this can be difficult to use, as some keyboards only angle the keys without splitting into halves.
The split design reduces the sideways bending of the hand but also important is the reduction of vertical bending.
However, this can be overcome by taking some simple steps like:
Flattening the keyboard feet on the desk can keep the hands flat
Putting the keyboard on a vertical tilted tray can also help improve the hands’ posture
Keyboards are available in left and right-handed styles
Choosing a Mouse
The shape along with the location of the mouse in relation to the keyboard is important for maintaining a healthy hand posture. Here are some considerations when choosing a mouse. The mouse buttons should:
Have easy clickability
Is easy to move around/feels natural
The screen cursor should move accurately with your movements
There are mice with programmable buttons allowing you to control additional functions. Important things to check:
Make sure the size and shape of the mouse feels natural in your hand
Hold the mouse in a neutral position meaning your hand should not be bent up, down or sideways
Position and operate the mouse with your upper arm relaxed and close to your body, and don’t reach too far forward or too far out to the side
There are keyboards with a separate numeric pad that allows the mouse to be located closer to the keyboard. Some keyboards include a cursor positioning device like a trackball, touchpoint or touchpad. These types eliminate having to reach for a mouse. However, it is a good practice to mix it up using the keyboard for certain operations and the mouse for others. This allows different muscles and ligaments to work while the others take a break.
The Ideal Setup
All keyboards and mice are designed differently. The key is to find well-made products that are built with ergonomic injury prevention as the focus. You can use trackballs, touchpads, and pen mice instead of a regular mouse.
Find what works for you, is ergonomic, comfortable and easy to use and will keep your hands in a neutral posture. If you do a lot of typing and mouse movement, your hands are going to get tired even with top designed keyboards and mice. Take frequent short rest and stretch breaks to let your muscles recover. The stretching exercises should include the:
Wrist
Forearm muscles
Shoulders
Neck
Upper back muscles
Working like this will protect you against over-use injuries.
Carpal Tunnel Chiropractic Treatment
NCBI Resources
Chiropractic care is one of the most common forms of treatment for carpal tunnel syndrome. Foremost, a doctor of chiropractic will evaluate the extent of the condition as well as diagnose the individual to determine any underlying cause behind the condition. Through a series of chiropractic adjustments and manual manipulations, the hand, wrist, and arm are adjusted to reduce the pressure around the median nerve, and ultimately reducing the symptoms.
Movement disorders are characterized as health issues that cause abnormal and involuntary body positions or movements. Many neurological conditions are caused by brain signal problems and they can ultimately affect quality, fluency, speed, and ease of movement. Dyskinesia is characterized as abnormal and involuntary fluency and/or speed of movement while hyperkinesia is characterized as excessive movement and hypokinesia is characterized as slow or absent, abnormal and involuntary movements. Movement disorders are also referred to as conversion disorders and/or psychogenic movement disorders. � Injuries or underlying conditions to the brain, spinal cord, and nervous system don’t always cause movement disorders. Movement disorders can include: �
Tics, characterized as abnormal and/or involuntary contractions of the muscles,
Tremor, also referred to as a resting tremor or essential tremor,
Ataxia, characterized by “jerky” movements and coordination problems,
Dystonia, characterized as abnormal and/or involuntary, generally prolonged contractions of the muscles,
Huntington’s disease, also referred to as chronic progressive chorea,
Parkinson’s disease, a well-known movement disorder, including tremors,
Multiple system atrophies, also referred to as Shy-Drager syndrome,
Restless legs syndrome (RLS) and reflex sympathetic dystrophy/periodic limb movement disorder (RSD/PLMD),
Myoclonus, characterized by rapid, brief, irregular movements,
Tourette’s syndrome, another well-known movement disorder, including repetitive or unwanted sounds and movements,
Wilson disease, known as an inherited health issue that causes a variety of symptoms and liver disease, and
Progressive supranuclear palsy, characterized as a rare health issue that affects movement.
As previously mentioned in the list above, tics are a well-known, movement disorder characterized by abnormal and/or involuntary contractions of the muscles that can ultimately affect an individual’s regular physical activities as well as their overall quality of life. Tics are generally triggered by a powerful urge or sensation that is temporarily relieved after the contraction of the muscles. Several examples of common tics can involve the following, including: �
Twitching of the face,
Clearing of the throat,
Grunting,
Sighing,
Blinking, and/or
Shrugging of the shoulders.
Dystonia can include spasmodic torticollis, characterized by abnormal and/or involuntary movements of the eyelids, face, head, neck, and blepharospasm. � Tourette’s syndrome is another well-known movement disorder characterized as a health issue that causes a variety of vocal and motor tics or repetitive contractions of the muscles. Common symptoms of Tourette’s syndrome generally manifest during childhood and/or early adolescence and they can commonly vary in severity and frequency. Patients diagnosed with Tourette’s syndrome can also ultimately develop a variety of other behavioral problems, including inattention, hyperactivity, impulsivity, compulsions, and obsessions. A diagnosis is necessary to determine the presence of Tourette’s syndrome. �
Contents
What are the Symptoms of Movement Disorders?
Movement disorders are characterized by abnormal and involuntary movements. But, patients may also experience a variety of other symptoms, including: �
Jerky movements or twitching,
Spasms and/or contractures, characterized as limbs “freezing” in an abnormal or involuntary body position,
Tremors, characterized by abnormal or involuntary movement of a limb, can range from moderate to severe and occasional or constant, and
Gait problems, characterized as walking problems that can ultimately cause difficulty while standing or unsteady walking.
The symptoms of the movement disorders previously mentioned above can be treated. Treatment can help improve the symptoms of movement disorders. �
What are the Treatments for Movement Disorders?
Movement disorders can cause stress and ultimately affect an individual’s overall quality of life. Qualified and experienced healthcare professionals that specialize in a variety of movement disorders can help diagnose as well as develop a treatment program for every patient’s unique needs and symptoms. The goal of a doctor is to help improve the quality of life of patients with movement disorders through the use of lifestyle modifications, therapy, and medicines. According to the diagnosis, the healthcare professional will ultimately suggest treatments and possible referrals to other specialists, including: �
Referral to neurobehavioral healthcare professionals,
Physical therapy,
Chiropractic care,
Medication
Movement disorders are ultimately characterized as a variety of neurological health issues that can also generally cause various abnormal and involuntary body positions or movements. Many other neurological health issues are commonly caused by problems in the transmitting signals of the brain and they can ultimately affect quality, fluency, speed, and ease of movement. Movement disorders are also frequently referred to as conversion disorders and/or psychogenic movement disorders. Treatment of the symptoms of movement disorders will ultimately depend on the diagnosis of the patient. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Movement disorders are characterized as health issues that cause abnormal and involuntary body positions or movements. Many neurological conditions are caused by brain signal problems and they can ultimately affect quality, fluency, speed, and ease of movement. Dyskinesia is characterized as abnormal and involuntary fluency and/or speed of movement while hyperkinesia is characterized as excessive movement and hypokinesia is characterized as slow or absent, abnormal and involuntary movements. Movement disorders are also referred to as conversion disorders and/or psychogenic movement disorders. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Stanford Health Care (SHC) – Stanford Medical Center. �Functional Movement Disorders.� Stanford Health Care (SHC) – Stanford Medical Center, stanfordhealthcare.org/medical-conditions/brain-and-nerves/functional-movement-disorders.html.
Stanford Health Care (SHC) – Stanford Medical Center. �Symptoms.� Stanford Health Care (SHC) – Stanford Medical Center, stanfordhealthcare.org/medical-conditions/brain-and-nerves/functional-movement-disorders/symptoms.html.
Stanford Health Care (SHC) – Stanford Medical Center. �Treatments.� Stanford Health Care (SHC) – Stanford Medical Center, stanfordhealthcare.org/medical-conditions/brain-and-nerves/functional-movement-disorders/treatments.html.
Swierzewski, Stanley J. �Movement Disorders Overview.� Movement Disorders Overview – Movement Disorders – HealthCommunities.com, 1 Jan. 2000, www.healthcommunities.com/movement-disorders/overview-of-movement-disorders.shtml.
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
If you are experiencing any of these situations, then it might be your stress hormone affecting your mind-body connection.
By discovering how hormones and stress can alter the brain�s function, it is impressive how science and psychology are behind the mind and body connection and how it is disconnected due to two concept idealism. Amazingly though, hormones in the body can affect a person’s perception of the world as well as showing how stress is producing in the body while making visible changes in the brain by enhancing the neurological functions. In the previous article, it talks about how the mind-body connection was formed.
By exploring how stress can rewire the brain’s neural architecture, researchers can see how this is being done, understanding allostasis and how the body responds to stress, as well as seeing how five molecules are being required to help rebuild the brain in the body.
How Stress Remodels the Brain
Known as cognitive deficits, any altercations to the brain can make a person more susceptible to neurological dysfunction in their bodies. Studies show that people can become acutely sensitive to stimuli in their bodies, like having fearful facial expressions due to amygdala hyper responsivity. This condition can happen to schizophrenia patients, and recent research shows that the amygdala response can become hyperactive and can decrease over time gradually. With the bidirectional relationship between the environment and the mind, it shows the spheres of the brain can correspond with each other. When there is chronic or severe stress in the body and affecting the brain, it can result in behavioral abnormalities that can be manifested into cognitive impairments.
In a study, the research shows how animals were being exposed to stressful situations, and researchers are examining their stress response. The results show how animals are being exposed to different situations that are causing them to be stress, and the stress hormones are producing dendritic remodeling in the hippocampal neurons.
When the human body is continually adapting to its environment, the brain is being rewired since the brain is the center for regulating the cytoskeleton, epigenetic, and nongenomic mechanism for the body. Surprisingly, the stress hormone can remodel the neural architecture of the brain by gene expression that is continually being mediated by epigenetic mechanisms. This mechanism makes the human body to adapt to its environment and helps the response and corresponding changes in the body; there is a factor that can help mediate these changes.
BDNF or brain-derived neurotrophic factor is a factor that is being directly involved in the neurological function of the brain while also playing an essential role in the hippocampal aging so the brain can function correctly. So when stress is affecting not only the brain but the body as well, it can cause cognitive dysfunction to a person depending on the stress and the situation a person is in.
How Allostasis and The Body Responds To Stress
When the body achieves homeostasis, a process known as allostasis helps the body be adaptive and is connected to the entire human body. Since the HPA axis, the nervous system, the metabolic system, and the immune system are involved with the stress response and can become a stressor. If there is an overabundance of stress, the body can start to fail and cannot regulate these mechanisms, causing the body to burn out. This is known as “allostatic overload.”
With homeostasis, it is there to make sure that the body is doing okay by adapting to stressor mediators. These mediators include the endocrine system that produces hormones, the metabolic system that helps regulate glucose levels, and the immune system. With these meditators, they are there to help maintain the body, while allostasis and “allostatic overload” are the biological concepts that can describe how the body can adapt to stressors. When a person is overly stressed or is suffering from a high allostatic load, they may develop some bad habits in the future. Whether it is smoking, consuming alcohol, eating poorly, or even sleeping less, this can cause their body to develop chronic illnesses over time.
There are three main types of stress that the body can undergo. They are:
Good stress: This type of stress is an essential part of life that everyone has. What good stress does to the body is that it briefly increases the heart rate and mild hormone rate. This type of stress is a good motivation boost to anyone that is getting their work done.
Tolerable stress: This type of stress is a bit more severe and temporary in the body. What tolerable stress does is that it is associated with non-normative that can be presented from a more significant threat. This type of stress can be from experiences of the death of a family member, natural disasters, or an act of terrorism.
Toxic stress: This type of stress can cause prolong activation of the stress response and can cause chronic impairments to the body. Research at Harvard showed how toxic stress could alter the developmental process on kids, thus producing damaging effects that can affect a child’s development throughout their life. Toxic stress can produce long-lasting abnormalities to a person and can hinder them from being socially active.
The 5 Molecules To Remodel The Brain
Even though the body gets involved when there is a stressful experience, the brain becomes the primary target. The stress hormone can alter the brain’s function and structure, causing the body to have neurological impairments. Surprisingly though, the brain can rebuild itself, and many healthcare professionals can offer patients that have neurological dysfunction a positive therapeutic advancement through the correct internal, external, and environmental conditions that the patient is in.
There are five main groups of molecules that the brain needs, so it can be remodeled and can offer positive treatments for the person. They are:
With the mind-body connection being in a bidirectional relationship, it is essential to know that these two are not separate entities and that they affect the body by sending out hormones to the crucial organs to make sure that it is functioning correctly. When it comes to stress, however, it can cause the brain to rewire itself, and if there is prolonged stress in the body, it causes many disruptive factors that will impact not only the mind-body connection but the body’s system as well. Some products can help the mind-body connection by providing support to the endocrine system, the gastrointestinal system, as well as relieving temporary stress the body may encounter.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Team, Biotics Education. �Managing Inflammation through Gut Microbiota.� Biotics Research Blog, 7 May 2019, blog.bioticsresearch.com/managing-inflammation-through-gut-microbiota.
McEwen, Bruce S. �The Neurobiology of Stress: from Serendipity to Clinical Relevance.� Harold and Margaret Milliken Hatch Laboratory of Neuroendocrinology, The Rockefeller University, 25 Sept. 2000.
Shi, Shou-Sen, et al. �Acute Stress and Chronic Stress Change Brain-Derived Neurotrophic Factor (BDNF) and Tyrosine Kinase-Coupled Receptor (TrkB) Expression in Both Young and Aged Rat Hippocampus.� Yonsei Medical Journal, Yonsei University College of Medicine, Sept. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2908888/.
Suslow, Thomas, et al. �Automatic Amygdala Response to Facial Expression in Schizophrenia: Initial Hyperresponsivity Followed by Hyporesponsivity.� BMC Neuroscience, BioMed Central, 13 Nov. 2013, www.ncbi.nlm.nih.gov/pubmed/24219776.
Team, Biotics Education. �Stress – The Mind-Body Connection Part 2.� Biotics Research Blog, 12 Dec. 2019, blog.bioticsresearch.com/stress-the-mind-body-connection-part-2.
Team, Harvard University. �Toxic Stress.� Center on the Developing Child at Harvard University, 2019, developingchild.harvard.edu/science/key-concepts/toxic-stress/.
If you are experiencing any of these situations, then your mind-body connection might be unbalanced.
Throughout history, there have been studies and theories that the mind and body are separate. This theory has been accepted by many; however, there is so much evidence showing the mind, and the body having a bidirectional relationship in the body like the gut system that sends signals to the brain and vise versa. Since each organ sends its signals to the brain, the endocrine system sends out signals to the brain in the form of hormones, which can alter the person’s perception of the world through their eyes.
With that in mind, neuroplasticity has shown people that when they are in their environment, it can be altered the physical make up of the environment. Many modern scientists have acquired very sophisticated tools that can monitor the body’s brainwaves, the microbes, and many other factors that can change the body’s mind. Since stress is a full-body response, it can be both a good thing and a bad thing for the body. Good stress in the body gives the “fight or flight” response while the bad stress can become chronic and can lead the body to be dysfunctional. So the idea of having the mind and the body being a separate function seems to be a bit outdated but also informational.
By exploring the science and psychology of the mind-body disconnect, researchers can see how a person�s hormones can affect their perception of the world. By diving into the body, researchers can also see how stress can produce any visible changes in the brain as well.
How Experiences Alters the Mind
Many experiences can alter the mind. Whether it be good experiences that can be used in the work atmosphere or it can be bad experiences like being traumatized from horrible events. Studies show that trauma can alter the mind and depend on the situation. Even though the damage that is caused by trauma can be healed if it is minor. In some cases, it can scar a person even though the physical damage is healed. The mental damage is affected as a person can relive the traumatic experience that they encountered.
With good experience, they can be useful to a person if the damage has minored. If a person accidentally hurt themselves from any activities, they know not to do that again. Although if a person practices on specific activities and get better at it with time, it becomes a skill they can use. Sometimes a person can have a set of specific skills that are beneficial when they are working in the job they are in. So depending on the experiences that a person is dealing with, it can be either good or bad, but their brains will remember it.
The Difference Between Dualism and Monism
There has always been a philosophical debate on the mind and body. There are different ways to look at the mind-body connection, as many researchers have debated whether the mind is part of the body or that the body is part of the mind. Thus the difference between Dualism and Monism has different views on the mind-body connection.
Dualism is defined as being born out of the body as a physical object, and the mind or the consciousness is being constructed. The origins of dualism started with the Cartesian ways of thinking, where people started to argue that there was a two-way relationship between the mental and physical substances in the body. Surprisingly, the belief of the physical and mental systems are compartmentalized and not inter-related like what some people think.
French philosopher Ren� Descartes stated that the mind interacts with the body through the pineal glands and that the mind controls the body. He also summed his thoughts with one of his famous statements: �I think therefore I am.� With this statement, it tells researchers that the mind is a nonphysical and non-spatial substance that is being identified with consciousness and self-awareness in the body.
With monism, it is defined as a material point of view and that all humans are just merely complex physiological organisms. There is another type of monism known as phenomenalism. It also goes by subject idealism, and the concept of this monism is that the mind and the body are two separate entities. With each type of monism, the concepts always seem to be the same, which shows that each type of monism seems to ignore either the mind or the body. It is always one or the other, never together at the same time.
How Stress Hormones Influences the Brain
When it comes to stress and hormones, there has been a lot of scientific advancements on how the stress hormone affects the brain in the body. Since hormones have been found to alter the hippocampal neurons with stress hormones, they can give the body the burst of energy that it needs. Although, if there is a long-term activation of the stress hormone can wear the brain down and kill the brain’s cells. If someone has any psychological disorders that cause prolonged stress, it can impair cognitive function, and the results can be enhanced emotionally.
Conclusion
With the mind-body connection, they can send signals to each other and make sure that the human body is functioning correctly. When there is prolonged stress in the body, it can disrupt the signals and cause the body to dysfunction. The next article will be discussing how stress can rewire the brain in the body. Some products can help the body by supporting the endocrine system as well as helping the body to relieve temporary stress.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Perry, Bruce D., et al. �Childhood Trauma, the Neurobiology of Adaptation, and �Use?Dependent� Development of the Brain: How �States� Become �Traits.�� Semantic Scholar, 1 Jan. 1995, www.semanticscholar.org/paper/Childhood-trauma%2C-the-neurobiology-of-adaptation%2C-Perry-Pollard/1d6ef0f4601a9f437910deaabc09fd2ce2e2d31e.
Team, Biotics Education. �Stress – The Mind-Body Connection Part 1.� Biotics Research Blog, 9 Dec. 2019, blog.bioticsresearch.com/stress-the-mind-body-connection-part-1.
Woolley, C S, and P A Schwartzkroin. �Hormonal Effects on the Brain.� Epilepsia, U.S. National Library of Medicine, 1998, www.ncbi.nlm.nih.gov/pubmed/9915614.
Most of us know what sciatica means and that is low back pain that radiates/spreads into the buttock down into the leg and sometimes into the foot. The pain can be mild to excruciating, but fortunately, if it is mild�sciatica can usually be alleviated in 3 months.�These are a few non-invasive conservative treatment therapies that can be done at the house.
Here are a few at the house sciatica remedies for people who started experiencing sciatic nerve pain or whose pain is not severe. But you should get a doctor�s approval before trying any of these at the house therapies.
If sciatica has been present for a few weeks or the low back and leg pain has become debilitating you should see a doctor.
Contents
House Tip 1. Exercise is OK & Beneficial
It might seem strange to exercise when you�re in pain, but research has shown that too much rest can aggravate back and leg symptoms.
Remember this is not a hardcore burning massive calories exercise, but a gentle exercise routine that you can work into your day.
These Exercises should not be painful or strenuous.
A walk around the house is a great form of physical activity that keeps your spine strong without worsening the injury.
Make your spine stronger with core exercises, but make sure they will not exacerbate your sciatica symptoms. And remember that exercise triggers the release of endorphins to reduce the pain.
House Tip 2. Start Stretching
Start doing gentle stretches regularly. Stretching will improve your spinal flexibility and motion range and also builds core strength. Most stretches can be done while watching your favorite show/movie.
House Tip 3. Ice Packs and Heating Pads Help
Alternating heat and ice therapy can bring relief from nerve pain. Ice helps reduce inflammation, and heat generates blood flow to the areas of pain that speeds up healing. Both help reduce muscle spasms that usually come with sciatica.
Apply the ice pack for 15 minutes once every hour, and then bring the heat for 15 minutes every 2 or 3 hours. Remember to protect your skin when using these pads, and never sleep with the heat or ice pads.
House Tip 4. Change Your Posture
If you are working at your desk or just relaxing, don’t stay in the same position too long, as it can make the pain spike.
Therefore move around and change your posture every 20 minutes. Using the correct posture for various activities will help take the pressure off your spine and reduce symptoms.
House Tip 5. If You Need To Use Medication Properly
Over-the-counter non-steroidal anti-inflammatory medications can help ease symptoms when they present. These medications can relieve inflammation and pain, whereas acetaminophen (Tylenol) only reduces pain.
However, there are health risks, so make sure to discuss their safety with your doctor.
Examples include:
Ibuprofen (Advil, Motrin)
Aspirin (Ecotrin)
Naproxen (Aleve)
The Remedies Are Not Working
Recognize when at the house remedies are not reducing your symptoms. When the treatments aren’t helping, it could be time to see a doctor, chiropractor or spine specialist.
People including myself want to avoid the doctor. It could be knowing how to use your health insurance or if you don�t have any. Whatever the reason do not opt for the ignorance is bliss and hope it will all go away.
If you need help figuring out how to use your insurance here at Injury Medical our staff are trained to help guide you through the process. And if you don’t have insurance we can still help and work out different types of plans.
Now there are sciatica symptoms that warrant immediate medical attention. In these rare cases, holding off medical care could cause permanent nerve damage.
If any of the following occur, please see your doctor as soon as you can:
There is severe throbbing/stinging pain in your low back and legs
Nerve associated symptoms like:
Weakness
Numbness
Tingling
Electric shock-like pain
The pain is not improving after 2 weeks
The pain gets worse, even with house therapies
Loss of bowel or bladder control
At the end of the day reducing sciatica symptoms doesn�t always mean having to use an extreme treatment approach. Relieving sciatica symptoms at the house with light exercise, ice/heat therapy, correct posture, and medication can help speed up recovery. The most important thing you can do is to take it seriously and call your doctor or chiropractor if relief is not happening.
Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again!
*Effective Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
A study cited by the health magazine�Prevention�found that sixty percent of sciatica sufferers who failed to get relief from other treatments found their symptoms improved after chiropractic care. In fact, they got the same level of relief as those who went through surgery � without any of the serious side effects that so often come with surgical procedures.
The blood-brain barrier is a protective shield that allows nutrients to enter the brain while keeping harmful components in the bloodstream from passing into the brain. However, many factors can cause a leaky blood-brain barrier. This can allow harmful components to penetrate the blood-brain brain, ultimately causing inflammation and brain health issues. A leaky blood-brain barrier is associated with many mental health issues and neurological diseases, including anxiety, depression, brain fog, fatigue, Alzheimer’s disease, Parkinson’s disease, attention deficit hyperactivity disorder (ADHD), and schizophrenia. In the article below, we will discuss natural ways which have been demonstrated to help fix a leaky blood-brain barrier and improve overall brain health.
Contents
Take Berberine
A variety of plants have an alkaloid known as berberine. This extracted substance has anti-inflammatory properties and it can ultimately promote brain health by protecting neurons. Scientists have also found that taking berberine can help lower “bad” cholesterol, improve gut health, and many others believe it may even have possible antidepressant properties. Other research studies have shown that it can reduce inflammation, improve blood-brain barrier permeability and decrease damage following a traumatic brain injury. However, further research studies are still required to demonstrate these effects.
Avoid Exposure to Mold
Mold and mycotoxins, or toxic metabolites released by mold, can cause severe brain health issues in people with certain sensitivities and intolerances. Exposure to these can also cause a leaky blood-brain barrier. In 2010, scientists demonstrated that exposure to mold and mycotoxins can increase BBB permeability by breaking down the blood-brain barrier. Moreover, low amounts of mold and mycotoxins can also be found in the foods we eat, including nuts, tea, coffee, and chocolate. Charcoal or bentonite clay supplements are powerful remedies that can capture toxins and release them out of the body.
Take B Vitamins
According to healthcare professionals, B vitamins have been found to help improve a leaky blood-brain barrier. B vitamin deficiencies can ultimately affect brain health. Taking vitamin B1 (thiamine) supplements can help fix BBB permeability. Research studies have also shown that vitamins B6, B9, and B12 can help improve brain health in older adults with increased homocysteine and moderate cognitive impairment. Homocysteine is an inflammatory component that can breakdown the blood-brain barrier. Fortunately, healthcare professionals have found that taking B vitamins can balance the blood-brain barrier.
Take Magnesium
Magnesium is a fundamental mineral that plays a vital role in a variety of structures and functions in the body, including enzyme, hormonal, and neurotransmitter activity. Magnesium is also one of the nutrients that people are most deficient in. This important mineral can increase growth hormones in the brain, support mitochondria, protect the brain from alcohol and help people overcome addiction and withdrawal. Research studies have also shown that taking magnesium can improve BBB permeability. Bananas, avocado, spinach, chard, almonds, pumpkin seeds, and dark chocolate have magnesium.
Take R-Lipoic Acid (RLA) and Acetyl-Carnitine (ALCAR)
R-Lipoic Acid (RLA) is a fat-soluble and stable, bioavailable form of lipoic acid or an antioxidant created by the body, that can pass through the blood-brain barrier and enter the brain. This essential antioxidant can also protect the brain from alcohol and support mitochondria. Research studies have found that RLA can decrease oxidative stress and inflammation as well as improve BBB permeability and. Acetyl-Carnitine (ALCAR) is an acetylated form of the amino acid carnitine that is synergistic with RLA. ALCAR is neuroprotective and it can help people improve brain fog as well as addiction and withdrawal.
Eat or Take Turmeric or Curcumin
Turmeric or curcumin, the spice that gives curry its yellowish color, is another fundamental ingredient for brain health that can help reduce stress and increase growth hormones in the brain. Turmeric or curcumin can also improve BBB permeability and promote overall brain health by maintaining and regulating the integrity of the blood-brain barrier. Research studies have also found that eating or taking turmeric or curcumin can help prevent damage to the blood-brain barrier due to glucose and oxygen deprivation by considerably decreasing oxidative stress and inflammation in the brain and body.
Take Vitamin D
Vitamin D is another fat-soluble vitamin that the skin produces when exposed to the sun. The brain, heart, muscles, and immune system, among other cells and tissues in the body, have vitamin D receptors. This fat-soluble vitamin is fundamental for a variety of structures and functions. Vitamin D deficiencies can also cause a variety of brain health issues and neurological diseases. Scientists have shown that vitamin D can decrease inflammation and improve BBB permeability. Vitamin D has also been demonstrated to help protect endothelial cells and improve BBB permeability in patients with multiple sclerosis.
Take Citicoline or Alpha GPC
Citicoline or CDP-Choline is another essential B vitamin and bioavailable form of choline. This substance can help improve brain fog. Research studies have also found that citicoline or CDP-Choline can prevent the breakdown of the blood-brain barrier following a stroke or traumatic brain injury and brain ischemia. Alpha GPC is another form of choline that has been shown to help support the blood-brain barrier. Scientists have also found that it can fix damage to the blood-brain barrier following a stroke or TBI, restoring cognitive function. You can also find some choline in egg yolks and beef liver.
Avoid Exposure to EMFs
According to a variety of research studies, radiofrequency electromagnetic fields or EMFs emitted from smartphones, laptops, and WiFi can affect the brain and mental health. Radiofrequency electromagnetic fields or EMFs can cause a leaky blood-brain barrier.��Several other research studies have found that radiofrequency electromagnetic fields or EMFs can increase BBB permeability. Increased blood-brain barrier permeability may ultimately result in the accumulation of brain cell and tissue damage as well as cognitive impairment. It’s important to be aware of the effects of being exposed to these devices.
Many factors can cause a leaky blood-brain barrier, ultimately causing increased BBB permeability, oxidative stress, inflammation and a variety of brain and mental health issues, including neurodegenerative diseases. The blood-brain barrier is a protective shield which allows nutrients to enter the brain while keeping harmful components in the bloodstream from passing into the brain. A leaky blood-brain barrier is associated with anxiety, depression, brain fog, fatigue, Alzheimer’s disease, Parkinson’s disease, attention deficit hyperactivity disorder (ADHD), and schizophrenia. Fortunately, several natural ways have been demonstrated to help improve overall brain health and wellness as well as help fix a leaky blood-brain barrier. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The blood-brain barrier is a protective shield that allows nutrients to enter the brain while keeping harmful components in the bloodstream from passing into the brain. However, many factors can cause a leaky blood-brain barrier. This can allow harmful components to penetrate the blood-brain brain, ultimately causing inflammation and brain health issues. A leaky blood-brain barrier is associated with many mental health issues and neurological diseases, including anxiety, depression, brain fog, fatigue, Alzheimer’s disease, Parkinson’s disease, attention deficit hyperactivity disorder (ADHD), and schizophrenia. In the article above, we discussed more natural ways which have been demonstrated to help fix a leaky blood-brain barrier and improve overall brain health.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
The Star Academy. �How to Repair a Leaky Blood-Brain Barrier.� The Star Academy, The Star Academy, 16 Oct. 2018, thestaracademy.co.za/repair-leaky-blood-brain-barrier/.
Neurotransmitter Assessment Form
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”52657″ /]
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download* All of the above XYMOGEN policies remain strictly in force.
The blood-brain barrier is a protective shield that allows nutrients to enter the brain while keeping harmful components in the bloodstream from passing into the brain. However, many factors can cause a leaky blood-brain barrier. This can allow harmful components to penetrate the blood-brain brain, ultimately causing inflammation and brain health issues. A leaky blood-brain barrier is associated with many mental health issues and neurological diseases, including anxiety, depression, brain fog, fatigue, Alzheimer’s disease, Parkinson’s disease, attention deficit hyperactivity disorder (ADHD), and schizophrenia. In the article below, we will discuss natural ways which have been demonstrated to help fix a leaky blood-brain barrier and improve overall brain health.
Contents
Improve Gut Health
Understanding the connection between the brain and the gut is important to treat a leaky blood-brain barrier. In 2014, scientists found that a group of mice that didn’t have bacteria in their gastrointestinal tract had very leaky blood-brain barriers. However, when the scientists of the research study introduced bacteria into the intestines of the unhealthy mice through a fecal transfer, their BBB permeability considerably improved. Increasing good bacteria in your gut can ultimately help improve a leaky blood-brain barrier. Eating probiotics, prebiotic fiber, and fermented foods can increase good bacteria in your GI tract.
Avoid Eating Gluten
According to many healthcare professionals, we should avoid eating gluten to promote brain health. In 2006, scientists found that gluten can cause a leaky blood-brain barrier because it increases zonulin, a protein that affects BBB permeability and results in neuroinflammation. Gluten sensitivity or intolerance can also cause visible changes in the white matter of the brain. Dr. David Perlmutter, MD, author of Grain Brain and Brain Maker states that gliadin, another protein found in gluten, can also affect BBB permeability. Moreover, other food sensitivities or intolerances can also cause a leaky blood-brain barrier.
Eat Food with Sulforaphane
Cruciferous vegetables, including Brussels sprouts, cabbage, and broccoli, among others, have sulforaphane, a phytochemical and well-known antioxidant with powerful anti-inflammatory properties, similar to turmeric or curcumin. Many research studies have shown that sulforaphane can help improve a leaky blood-brain barrier by decreasing BBB permeability, preventing the breakdown of the BBB, and improving cognitive functions after stroke and traumatic brain injuries. Sulforaphane in myrosinase-activated supplement form can also be taken. Myrosinase is an enzyme in broccoli that helps metabolize sulforaphane.
Eat Food with Resveratrol or Pterostilbene
Foods like raspberries, grapes, red wine, and dark chocolate have resveratrol, another powerful antioxidant with potent anti-inflammatory properties that can help prevent the development of neurodegenerative diseases caused by a leaky blood-brain barrier. Scientists have found that eating food with resveratrol can ultimately help promote growth hormones in the brain and support mitochondria function. According to research studies, resveratrol can also protect the blood-brain barrier. Numerous other research studies have also found that eating foods with resveratrol can have other health benefits, including:
Decreasing a leaky blood-brain barrier
Protecting the blood-brain barrier
Improving blood-brain barrier permeability
Research studies have also shown that resveratrol can help protect the blood-brain barrier against oxidized LDL-induced damage. Furthermore, scientists believe that eating food with resveratrol may be a safe and effective way to naturally reduce the severity of multiple sclerosis.�Foods like blueberries have pterostilbene, a substance similar to resveratrol, that can also help protect the blood-brain barrier by decreasing oxidative stress and inflammation. Many healthcare professionals also refer to pterostilbene as the “better resveratrol” because it is often believed to be best absorbed by the body than resveratrol.
Drink More Coffee
Caffeine can help promote overall brain health and support the blood-brain barrier. Research studies have shown that drinking coffee can help prevent the development of dementia, Alzheimer’s disease, and Parkinson’s disease, among other health issues, by protecting the BBB. Scientists have also found that caffeine blocks blood-brain barrier permeability. Other research studies have also shown that drinking coffee can help prevent neurodegeneration by balancing the BBB. Because drinking coffee and caffeine can commonly affect sleep, however, make sure to consume these early in the morning.
Take Omega-3 Fatty Acids
Omega-3 fatty acids are essential fats that are primarily found in fish. Although the body can’t produce these by itself, they are necessary for overall brain health. Omega-3 fatty acids can also help increase the growth hormones in the brain, help support mitochondria function, or help people overcome addiction and withdrawal, as well as help protect the blood-brain barrier. Scientists have found that taking omega-3 fatty acids can decrease damage to the BBB following a stroke or TBI and improve BBB permeability in people with multiple sclerosis. Omega-3 fatty acids can also be taken in supplement form.
Take Melatonin and Improve Sleep
Sleep is fundamental for brain health. Poor sleep has also been shown to increase blood-brain barrier permeability. Taking melatonin supplements can also help improve sleep.�Melatonin is a hormone that is released by a small gland in the brain, known as the pineal gland. Melatonin helps regulate the circadian rhythm, or sleep and wake cycles. Enough melatonin is necessary to fall asleep quickly and sleep deeply throughout the night. Research studies have also shown that taking melatonin can help balance the blood-brain barrier and prevent further damage following a stroke and/or traumatic brain injury.
Manage and Reduce Stress
According to research studies, stress can ultimately damage the blood-brain barrier. Chronic stress has also been found to increase inflammation and BBB permeability. Fortunately, managing and reducing stress can help fix the blood-brain barrier. Massage, acupuncture, eye movement desensitization and reprocessing (EMDR), emotional freedom techniques (EFT), heart-rate variability (HRV) training, and mindfulness meditation can also help manage and reduce stress. Taking supplements to help improve stress can also include, zinc, magnesium, ashwagandha, and phosphatidylserine, among others.
Avoid Drinking Alcohol
According to healthcare professionals, drinking too much alcohol can cause a leaky blood-brain barrier. Research studies have shown that acetaldehyde, a byproduct of alcohol metabolism, can increase oxidative stress and affect the blood-brain barrier, resulting in inflammation and a variety of neurological diseases and brain health issues. Although some types of alcohol are better than others, it’s best to considerably decrease or avoid drinking alcohol. If you suspect that you may have a leaky blood-brain barrier, make sure to talk to your doctor about how drinking too much alcohol may cause a leaky BBB.
Many factors can cause a leaky blood-brain barrier, ultimately causing increased BBB permeability, oxidative stress, inflammation and a variety of brain and mental health issues, including neurodegenerative diseases. The blood-brain barrier is a protective shield which allows nutrients to enter the brain while keeping harmful components in the bloodstream from passing into the brain. A leaky blood-brain barrier is associated with anxiety, depression, brain fog, fatigue, Alzheimer’s disease, Parkinson’s disease, attention deficit hyperactivity disorder (ADHD), and schizophrenia. Fortunately, several natural ways have been demonstrated to help improve overall brain health and wellness as well as help fix a leaky blood-brain barrier. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The blood-brain barrier is a protective shield that allows nutrients to enter the brain while keeping harmful components in the bloodstream from passing into the brain. However, many factors can cause a leaky blood-brain barrier. This can allow harmful components to penetrate the blood-brain brain, ultimately causing inflammation and brain health issues. A leaky blood-brain barrier is associated with many mental health issues and neurological diseases, including anxiety, depression, brain fog, fatigue, Alzheimer’s disease, Parkinson’s disease, attention deficit hyperactivity disorder (ADHD), and schizophrenia. In the next article, we will discuss more natural ways which have been demonstrated to help fix a leaky blood-brain barrier and improve overall brain health.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
The Star Academy. �How to Repair a Leaky Blood-Brain Barrier.� The Star Academy, The Star Academy, 16 Oct. 2018, thestaracademy.co.za/repair-leaky-blood-brain-barrier/.
Neurotransmitter Assessment Form
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”52657″ /]
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download* All of the above XYMOGEN policies remain strictly in force.
Head and neck injuries related to phone use are on the rise. Since the first iPhone was released, according to a study in JAMA Otolaryngology-Head & Neck Surgery.
Doctors are warning cell phone users to be especially careful when:
Walking around and texting
It is a distraction and one of the leading causes of head and neck injuries.
2,501 reported cases of phone-related head and neck injuries that lead to emergency room visits between January 1998 and December 2017 found in a nationwide database. Injuries in teens and young adults aged 13 to 29 years old were about 40%, in women (55%) and men (45%).
Contents
Common Phone Injuries
Common injuries include:
Cuts
Bruises
Abrasions
Internal injuries usually happen around the eyes and nose
Possible trauma to the brain
Over 41% of these injuries happened at home and were minor with little or no treatment needed. Around 50% of injuries were a result of distracted driving and 30% from distracted walking.
Any type of phone distraction in and out of the home puts you and others at risk for:
Falls
Slips
Trips
All of which can lead to injuries and other possible consequences (e.g. a busted phone).
More individuals are getting injured because of phone use while moving around and not paying attention to what’s around them.
Children
Children under the age of 13 were at higher risk to suffer a mechanical injury like parents accidentally dropping the phone on their child or children hitting themselves in the face. For example, ninety cases of injuries occurred while playing Pokemon Go.
Spending as little as two to four hours a day hunched over a smartphone is enough to make a serious impact on the body over time. And though two to four hours may not seem like a long time, it isn�t hard to arrive at two hours by adding several 15-minute or half-hour segments together.
For teenagers, specifically, two to four hours on a smartphone has changed as of now teenagers spend around seven to eight hours on their phones. Spending twice as much time on afternoons or the space between classes or lunch. Think about the impact of 1500 plus hours of bad posture throughout the year. There is no surprise that teenagers are at risk.
The lasting impact of text neck and distracted phone use on today�s young people will be costly. Therefore, the public needs to be educated about the risks of distracted phone use and reducing this distracted behavior.
*Neck* Pain Chiropractic Care El Paso, Texas
NCBI Resources
If you begin noticing pain, spasms, or irritation around the neck, shoulders, or back make an appointment with a professional chiropractor. Explain when the pain occurred, the severity, and the activity that started it. A simple adjustment may be all that is needed to get re-aligned and gain relief from pain caused by overuse. A chiropractor can also help decrease the chances of the injury worsening over time.
If you are experiencing any of these situations, why not try to fix your resolution for the New Year.
New Year�s Resolution
With the new year coming up, many people make resolutions to better themselves for the upcoming year. Whether it be getting healthier, being more organized, stressing less, or living life to the fullest, resolutions are little reminders for anyone to get back on track on themselves. With the end of the month and during the holiday season, more people are more likely to put aside their health habits aside and indulge in the seasonal sweet and savory foods. The holiday season is filled with frequent gatherings with family and friends, which involves more consumption of food. In many parts of the U.S., sedentary behaviors have become a form of hibernation. Even though these holiday habits tend to make many people feel guilty, they always fuel resolutions so they can create healthier habits for when the new year begins.
Surprisingly, the most natural part is making resolutions; however, keeping them is the hardest part. Sometimes a person can make too many resolutions and can not follow through with them due to so many that they want to achieve. Other times there are people that are more likely to stick to their resolutions in the long run when their goals are more realistic than unattainable. There are a few changes that can make a tremendous impact on the person’s overall wellbeing and can make their lives a bit easier if they have a hectic lifestyle. One of the significant changes is getting healthier, and the majority of any chronic health issues can be rooted through a few practices that can sabotage a person’s physical, mental, and emotional health. So focusing on making good choices and making them habits or lifelong practices can provide a significant influence to not only the body but to the individual as well.
Getting Rid of Sugar
One of the first things that a person should do if they want to keep track of their health resolution is to ditch the overabundance sugar consumption. Many healthcare practitioners have continued to try and stop their patients from unbridled sugar consumption. It has been on the top list of chronic health problems that are plaguing the industrialized world since everyone in the world has consumed refined sugar into their bodies. Studies show that consuming refined sugar is the leading cause of dental cavities and being linked to obesity, type 2 diabetes, and endocrine dysfunction.
Studies even show that sugar consumption can also lead to hypertension and obesity-related cancers, as well as common mental disorders like depression. Research from the American Heart Association recommends that if both males and females want to limit their sugar consumption, then females must consume no more than six teaspoons of sugar a day. At the same time, males consume no more than nine teaspoons of sugar a day. The interesting fact is that people can reach that intake by just consuming a peanut butter and jelly sandwich. Sadly though, according to a 2012 research study, the average American individuals in the U.S. have consumed 19 teaspoons of sugar a day.
The body�s metabolism requires sugar to make sure that the person�s energy is leveled. Research shows that the metabolic mechanisms in which sugar helps contribute to diseases that can be both indirect and direct to the body. When there either a low sugar count or even a high sugar count in a person, it can lead to a dysregulation of the lipids and carbohydrate metabolism. When this happens, the body can have chronic conditions like dyslipidemia, reduce beta-oxidation as well as insulin resistance. Other mechanisms can affect the body when sugar is traveling through the bloodstream, like a positive energy balance. In some cases, when the sugar metabolism is too high, it can lead to hyperuricemia, oxidative stress, and chronic inflammation in the body, and it can cause developing problems for the individual. So by making the right choices and eliminating added sugars that are in packaged foods out of the diet can result in a drastic shift towards better health for the person.
Staying Hydrated
It is highly essential that everyone at least drinks about eight glasses of 8 ounces of water every day. Sadly though, not many people drink the recommended amount of water, thus getting dehydrated. Studies show that dehydration is a common, under-recognized condition that many individuals have. Sometimes chronic dehydration starts in childhood and continues throughout their lifespan. Research shows that an estimated 54% of the population lives with chronic dehydration since the human body is nearly 85% of water and why dehydration can be problematic.
Sometimes dehydration can go beyond merely feeling thirsty. Studies show that when a person is mildly dehydrated, it can impair cognitive functions, and when it is prolonged, it can cause urinary and bladder dysfunction in the body. A good rule for anyone who wants to maintain adequate hydration is to drink at least half of their body weight in ounces of water since hydration is directly linked to body mass and making sure that the weight is leveled. By drinking plenty of water, it is a simple yet easy health resolution that people can get for free and can provide a powerful impact.
Eating a Healthy Protein Breakfast
Another health resolution that can have a significant positive impact on a person’s health is by consuming a protein-rich breakfast. Sadly though in North America, people have developed two breakfast habits that can be bad for their health. They are skipping breakfast altogether and consuming a high refined carbohydrate breakfast. Both of these bad habits have been associated with obesity and other related comorbidities.
In contrast, though when a person starts eating a protein-rich breakfast, the results are remarkable. Research shows that eating a protein-rich breakfast can help reduce a person�s appetite, increased their satiety, and provide a healthier energy intake that can get a person over the mid-afternoon slumps. The positive effects show that consuming a protein-rich diet can lower the effects of obesity and being overweight as well as reducing the risk of obesity-related health conditions that can affect the body. By eating a sumptuous protein breakfast, the results show that it can help the body by changing the blood lipids and blood pressure as well as reducing the risk of metabolic syndrome and chronically elevated insulin for individuals that have diabetes and cardiovascular diseases.
Conclusion
With the new year coming around the corner, making resolutions to not only better oneself, but it can provide a positive change to the person. Many healthcare professionals can encourage their patients to make these simple yet highly effective changes to promote wellness. New Year’s resolutions do not have to be complicated or unattainable; they can be simple and easily attainable with these fundamental changes. By eliminating added sugars, drinking more water, and consuming a protein-rich breakfast can make anyone keep track of their resolution. Some products can help make sure that anyone can keep track of their resolutions by providing support to the body’s metabolism as well as regulating sugar metabolism as well.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Association, American Heart. �Added Sugars.� Www.heart.org, 17 Apr. 2018, www.heart.org/en/healthy-living/healthy-eating/eat-smart/sugar/added-sugars.
Chang, Tammy, et al. “Inadequate Hydration, BMI, and Obesity Among U.S. Adults: NHANES 2009-2012.” Annals of Family Medicine, American Academy of Family Physicians, July 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4940461/?report=reader.
Chow, Kai Foo. �A Review of Excessive Sugar Metabolism on Oral and General Health.� The Chinese Journal of Dental Research: the Official Journal of the Scientific Section of the Chinese Stomatological Association (CSA), U.S. National Library of Medicine, 2017, www.ncbi.nlm.nih.gov/pubmed/29181456.
Kn�ppel, Anika, et al. �Sugar Intake from Sweet Food and Beverages, Common Mental Disorder and Depression: Prospective Findings from the Whitehall II Study.� Scientific Reports, Nature Publishing Group U.K., 27 July 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5532289/.
Leidy, Heather J, et al. �Beneficial Effects of a Higher-Protein Breakfast on the Appetitive, Hormonal, and Neural Signals Controlling Energy Intake Regulation in Overweight/Obese, �Breakfast-Skipping,” Late-Adolescent Girls.� The American Journal of Clinical Nutrition, American Society for Nutrition, Apr. 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3718776/.
Maki, Kevin C, et al. �The Effects of Breakfast Consumption and Composition on Metabolic Wellness with a Focus on Carbohydrate Metabolism.� Advances in Nutrition (Bethesda, Md.), American Society for Nutrition, 16 May 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4863265/?report=reader.
Stanhope, Kimber L. �Sugar Consumption, Metabolic Disease and Obesity: The State of the Controversy.� Critical Reviews in Clinical Laboratory Sciences, U.S. National Library of Medicine, 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4822166/.
Team, DFH. �New Year’s Health Resolutions � Easy Does It.� Designs for Health, 23 Dec. 2019, blog.designsforhealth.com/node/917.
Urkin, Jacob, and Yair Bar-David. �Voluntary, Nonintentional Dehydration and Health.� American Journal of Public Health, American Public Health Association, Nov. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4605154/.
Vos, Miriam B, et al. �Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement From the American Heart Association.� Circulation, U.S. National Library of Medicine, 9 May 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5365373/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine













 When the human body is continually adapting to its environment, the brain is being rewired since the brain is the center for regulating the cytoskeleton, epigenetic, and nongenomic mechanism for the body. Surprisingly, the stress hormone can remodel the neural architecture of the brain by gene expression that is continually being mediated by epigenetic mechanisms. This mechanism makes the human body to adapt to its environment and helps the response and corresponding changes in the body; there is a factor that can help mediate these changes.
When the human body is continually adapting to its environment, the brain is being rewired since the brain is the center for regulating the cytoskeleton, epigenetic, and nongenomic mechanism for the body. Surprisingly, the stress hormone can remodel the neural architecture of the brain by gene expression that is continually being mediated by epigenetic mechanisms. This mechanism makes the human body to adapt to its environment and helps the response and corresponding changes in the body; there is a factor that can help mediate these changes.











 2,501 reported cases of phone-related head and neck injuries that lead to emergency room visits between January 1998 and December 2017 found in a nationwide database. Injuries in teens and young adults aged 13 to 29 years old were about 40%, in women (55%) and men (45%).
2,501 reported cases of phone-related head and neck injuries that lead to emergency room visits between January 1998 and December 2017 found in a nationwide database. Injuries in teens and young adults aged 13 to 29 years old were about 40%, in women (55%) and men (45%).
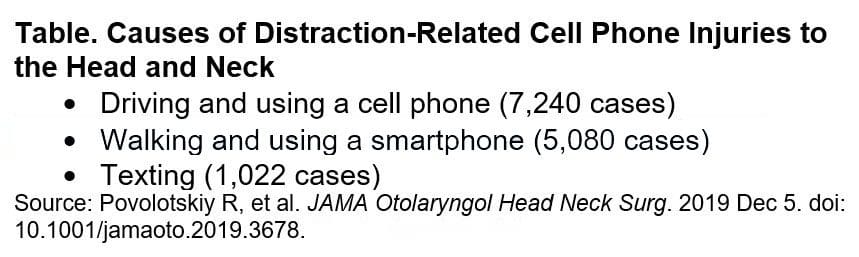 Any type of phone distraction in and out of the home puts you and others at risk for:
Any type of phone distraction in and out of the home puts you and others at risk for:
 Children under the age of 13 were at higher risk to suffer a mechanical injury like parents accidentally dropping the phone on their child or children hitting themselves in the face. For example, ninety cases of injuries occurred while playing Pokemon Go.
Spending as little as two to four hours a day hunched over a smartphone is enough to make a serious impact on the body over time. And though two to four hours may not seem like a long time, it isn�t hard to arrive at two hours by adding several 15-minute or half-hour segments together.
For teenagers, specifically, two to four hours on a smartphone has changed as of now teenagers spend around seven to eight hours on their phones. Spending twice as much time on afternoons or the space between classes or lunch. Think about the impact of 1500 plus hours of bad posture throughout the year. There is no surprise that teenagers are at risk.
The lasting impact of
Children under the age of 13 were at higher risk to suffer a mechanical injury like parents accidentally dropping the phone on their child or children hitting themselves in the face. For example, ninety cases of injuries occurred while playing Pokemon Go.
Spending as little as two to four hours a day hunched over a smartphone is enough to make a serious impact on the body over time. And though two to four hours may not seem like a long time, it isn�t hard to arrive at two hours by adding several 15-minute or half-hour segments together.
For teenagers, specifically, two to four hours on a smartphone has changed as of now teenagers spend around seven to eight hours on their phones. Spending twice as much time on afternoons or the space between classes or lunch. Think about the impact of 1500 plus hours of bad posture throughout the year. There is no surprise that teenagers are at risk.
The lasting impact of 







