For individuals experiencing frequent bloating or constipation, could performing a colon cleanse help alleviate your symptoms?
Colon Cleanse
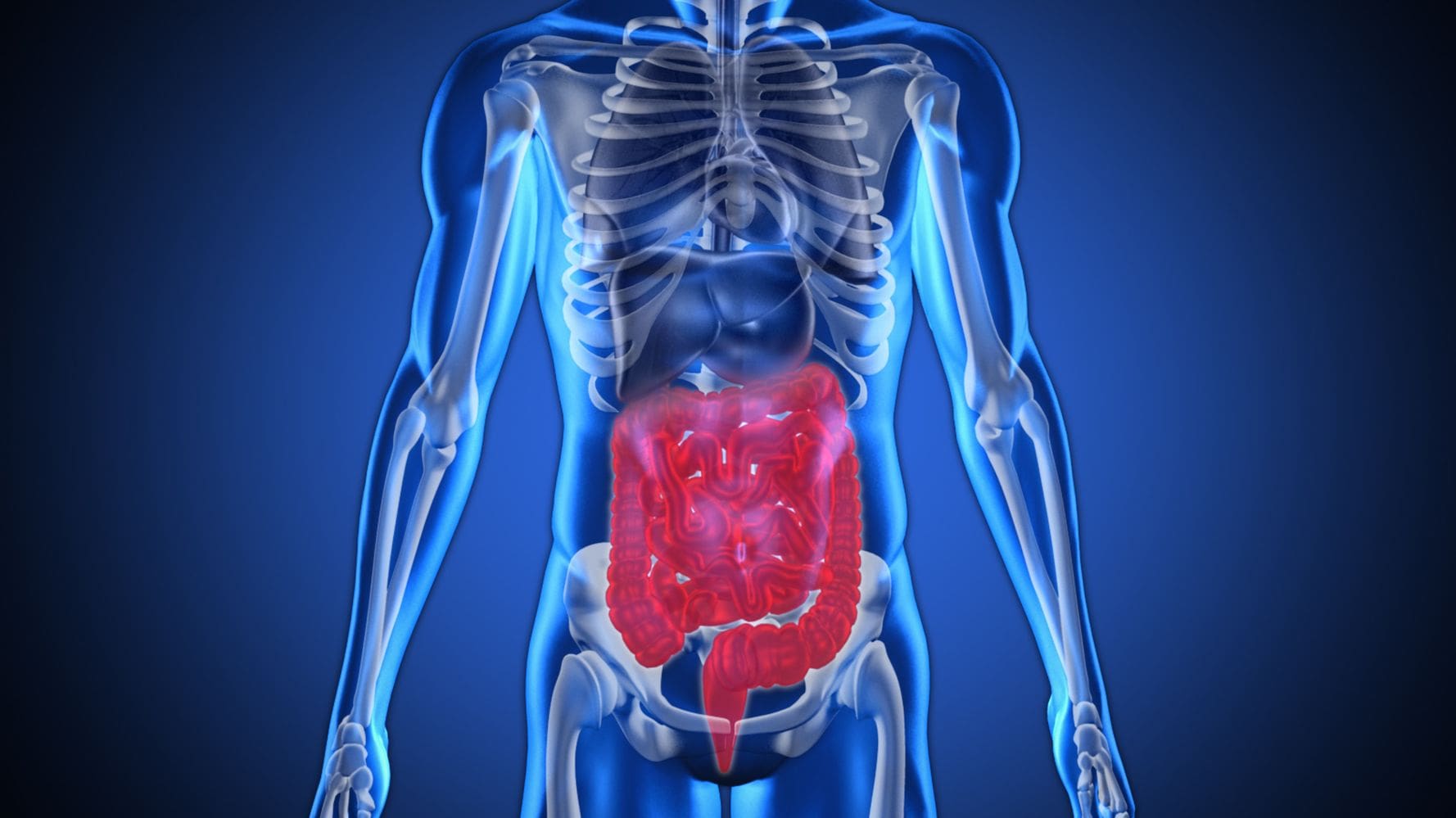
Individuals can clean out their bowels, colon, or large intestine by drinking more water and adding certain foods to their diet, like whole grains, fruits, and vegetables. Some may find that the practice helps decrease bloating or other digestive issues. While a colon cleanse is safe for most, the practice can cause side effects, like nausea or dehydration.
Benefits
Natural colon cleanses can provide various benefits that include:
Reducing bloating.
Improving the immune system.
Removing toxins from the body.
Helping with weight loss.
Decreasing the risk of colon cancer.
While individuals may feel better after a natural colon cleanse, there is currently no research to support the medical benefits. (Cedars Sinai. 2019)
Another type is known as hydrotherapy of the colon or irrigation.
A healthcare provider performs this type of cleansing and sends water into the colon with instrumentation.
This type of cleanse is not used to prepare individuals for a colonoscopy.
Cleansing
Cleansing the body safely can be done with ingredients from the local grocery store.
Thorough Hydration
Water will improve body function, including digestion and elimination.
Use the color of urine as a guide.
If it’s pale yellow, the body is getting enough water.
If it’s darker, the body needs more.
Increasing Fiber Consumption
Fiber is a type of carbohydrate that the body cannot digest but influences:
Fiber can be found in fruits, vegetables, oats, lentils, peas, and almonds.
Increasing fiber intake will help regulate the bowels and maintain overall colon health. (Cornell University. 2012)
Probiotics
Probiotics are live bacteria and yeasts that have health and digestion benefits.
Researchers believe they help to replace healthy bacteria and balance the healthy and unhealthy bacteria in the body, which maintains smooth digestion. (Mount Sinai. 2024)
Fermented foods like yogurt, kimchi, sauerkraut, and pickles are healthy sources of probiotics.
They also come as supplements.
Apple Cider Vinegar and Honey
Both ingredients contain probiotics, and mixing them can help improve gut health.
Individuals also believe that this concoction can help remove toxins from the body, but there’s no scientific evidence to support this.
Individuals can try 1 tablespoon of raw honey and 2 tablespoons of apple cider vinegar in a warm glass of water.
Juice and Smoothies
Adding more fruits, including juice and smoothies, is a healthy way to stay hydrated.
It also adds fiber and other nutrients to improve gut health.
Bananas and apples are a healthy source of probiotics.
Individuals can also add yogurt to the smoothies for extra probiotics.
These elements can help improve the gut microbiome and regulate bowel movements.
Precautions
Doing a colon cleanse should be safe for most, as long as the individual is not fasting at the same time or performing them too frequently. However, it’s recommended to consult a healthcare provider before changing eating patterns or trying new treatments or supplements, including a colon cleanse, especially for individuals who have an underlying condition.
Side Effects
Colon cleansing can come with risks that can include: (Cedars Sinai. 2019)
Dehydration
Cramping
Nausea
Electrolyte imbalance
Doing occasional colon cleanses may not result in side effects, but the chances of side effects increase the longer or more often cleanses are performed. It’s recommended to consult a healthcare provider if experiencing any symptoms.
Improving Colon Health
The best way to improve colon health is by drinking enough water and eating foods that promote a healthy digestive system. Healthy approaches include:
Increasing fruit and vegetable intake.
Increasing whole grain intake provides fiber and more nutrients.
Eating ground flaxseed improves digestion and elimination.
Integrative Medicine
References
Rosenblum, C. S. K. (2019). Ask a doc: Are colon cleanses healthy? (Cedars-Sinai Blog, Issue. https://www.cedars-sinai.org/blog/colon-cleansing.html
University., C. (2012). Fiber, digestion, and health. (Health Services, Issue. https://health.cornell.edu/sites/health/files/pdf-library/fiber-digestion-health.pdf
Sinai., M. (2024). Lactobacillus acidophilus. (Health Library, Issue. https://www.mountsinai.org/health-library/supplement/lactobacillus-acidophilus
For individuals dealing with fibromyalgia, can incorporating acupuncture as part of integrative treatment help with pain relief?
Introduction
The musculoskeletal system helps the various muscles, tendons, and ligaments be mobile while stabilizing the vertical pressure. The upper and lower extremities work together, enabling the host to be mobile without feeling pain and discomfort. However, many individuals have dealt with pain, whether it is acute or chronic, at one point in their lives. When the body is dealing with pain, the response signal from the brain will show where the pain is located, which causes muscle soreness. To that point, the immune system will start to heal the affected area naturally. However, when a person has an autoimmune disease, the body will be impacted for no reason, which then causes the immune system to release inflammatory cytokines to healthy cells and muscular structures. When this happens, it can affect their quality of life and cause painful sensations to the musculoskeletal system, forcing individuals to seek treatment. Today’s article focuses on the correlation between the musculoskeletal system and fibromyalgia and how treatments like acupuncture can help reduce the pain-like symptoms that are caused by fibromyalgia. We talk with certified medical providers who utilize our patients’ information to provide acupuncture treatments to lessen the overlapping risk profiles associated with fibromyalgia. We also inform and guide patients on how various treatments can help reduce the pain-like symptoms related to fibromyalgia. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from fibromyalgia. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
The Musculoskeletal System & Fibromyalgia
Have you been experiencing tingling sensations in your arms, legs, feet, and hands? Do you feel your muscles and joints lock up and feel stiff constantly in the morning? Or have you been dealing with unquestionable pain in your body that is affecting your daily routine? Many of these pain-like symptoms are associated with an autoimmune disease known as fibromyalgia. Fibromyalgia is often characterized by widespread chronic musculoskeletal pain that is associated with neurosensory disorders. People with fibromyalgia will have musculoskeletal pain symptoms from muscle and joint stiffness to fatigue and myofascial pain. (Siracusa et al., 2021) This is because the vagus nerve in the parasympathetic autonomic nervous system is in constant “fight or flight” mode, which causes many individuals to become hypersensitive and experience amplified painful sensations. This forces the muscle fibers in the musculoskeletal system to develop tiny nodules known as trigger points in the soft tissues. This causes muscle pathophysiology as a primary mechanism that mediates the onset of symptoms that pertain to fibromyalgia. (Geel, 1994) Unfortunately, fibromyalgia is a challenge to diagnose when comorbidities factors start to overlap and can play a role in this autoimmune disease.
Fibromyalgia is an autoimmune condition that increases a person’s sensitivity to pain while including multiple tender points at specific areas of the body, causing widespread chronic musculoskeletal pain. Many individuals dealing with chronic musculoskeletal pain are unaware of the proper pathway to care as it generates a negative impact on pain, disability, and quality of life. (Lepri et al., 2023) Since fibromyalgia is associated with musculoskeletal pain, it can be combined with myofascial pain syndrome since both are characterized by muscle tenderness. (Gerwin, 1998) However, there are numerous treatments available to reduce the painful effects of fibromyalgia and help restore a person’s quality of life.
From Inflammation to Healing- Video
Do you feel muscle pain and tenderness in various areas of your body? Do you feel muscle and joint stiffness in your upper and lower extremities? Or do you feel numbing or tingling sensations in your arms, hands, legs, and feet? Many people dealing with these pain-like issues are experiencing an autoimmune disorder known as fibromyalgia. Fibromyalgia is a challenging autoimmune disorder to diagnose. However, the symptoms are often correlated with muscular pain. This can cause many individuals to reduce their quality of life. Fibromyalgia can cause the body to be hypersensitive to pain and can cause chronic inflammation of the joints. However, some treatments are non-surgical, cost-effective, and can help provide the pain relief many people deserve. The video above explains how various non-surgical treatments can help reduce inflammatory and pain effects on the body through various treatments that can be combined to minimize the pain-like symptoms of fibromyalgia.
Acupuncture Reducing Fibromyalgia Pain
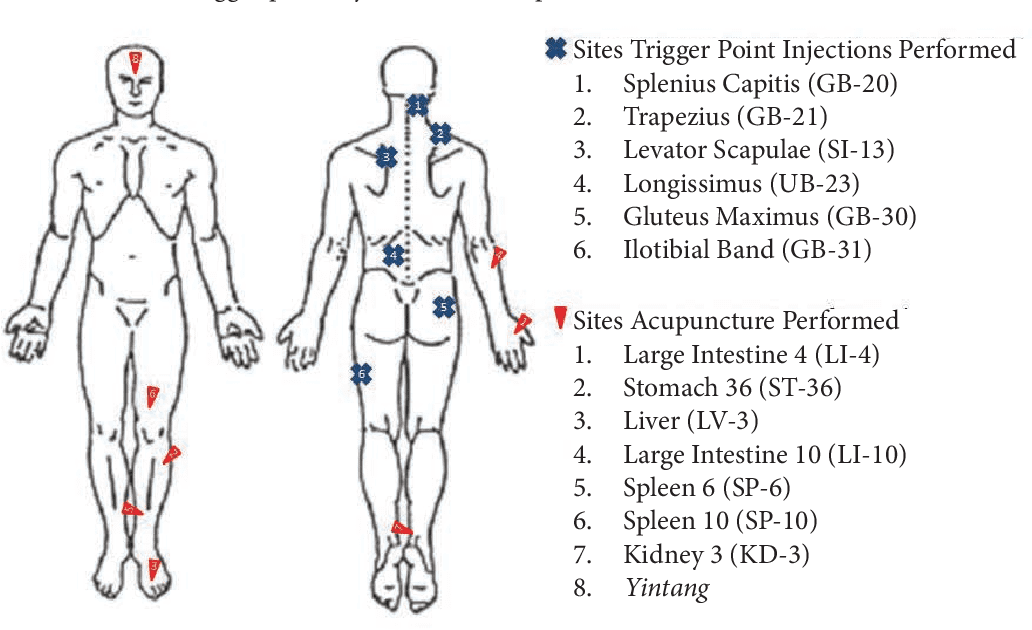
When it comes to treating fibromyalgia and reducing pain-like symptoms, many people will seek out non-surgical treatments to manage and improve the symptoms correlating with fibromyalgia. Acupuncture can help ease the pain-like symptoms that are affecting the body and reduce the myofascial trigger points correlating with fibromyalgia. Since acupuncture originated in China, it is one of the most popular sensory stimulation therapies that are non-surgical; acupuncturists who are highly trained use various techniques to insert and manipulate fine needles to stimulate specific anatomic trigger points in the body to restore balance to the body. (Zhang & Wang, 2020) For individuals dealing with fibromyalgia pain, acupuncture can be combined with other therapies as part of the individual’s personalized treatment plan. Acupuncture helps improve muscle pain caused by fibromyalgia.
Additionally, acupuncture can assist in regulating the somatosensory function of the body and reduce symptoms of muscle stiffness while enhancing a person’s quality of life. (Zheng & Zhou, 2022) Fibromyalgia is a chronic autoimmune disorder that can affect the musculoskeletal system and can cause unbearable pain to many people by disrupting a person’s quality of life. When combined with other therapies, acupuncture can provide a significant positive effect on managing fibromyalgia and enhancing a person’s quality of life. (Almutairi et al., 2022)
References
Almutairi, N. M., Hilal, F. M., Bashawyah, A., Dammas, F. A., Yamak Altinpulluk, E., Hou, J. D., Lin, J. A., Varrassi, G., Chang, K. V., & Allam, A. E. (2022). Efficacy of Acupuncture, Intravenous Lidocaine, and Diet in the Management of Patients with Fibromyalgia: A Systematic Review and Network Meta-Analysis. Healthcare (Basel), 10(7). https://doi.org/10.3390/healthcare10071176
Gerwin, R. D. (1998). Myofascial pain and fibromyalgia: Diagnosis and treatment. J Back Musculoskelet Rehabil, 11(3), 175-181. https://doi.org/10.3233/BMR-1998-11304
Lepri, B., Romani, D., Storari, L., & Barbari, V. (2023). Effectiveness of Pain Neuroscience Education in Patients with Chronic Musculoskeletal Pain and Central Sensitization: A Systematic Review. Int J Environ Res Public Health, 20(5). https://doi.org/10.3390/ijerph20054098
Siracusa, R., Paola, R. D., Cuzzocrea, S., & Impellizzeri, D. (2021). Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int J Mol Sci, 22(8). https://doi.org/10.3390/ijms22083891
Zheng, C., & Zhou, T. (2022). Effect of Acupuncture on Pain, Fatigue, Sleep, Physical Function, Stiffness, Well-Being, and Safety in Fibromyalgia: A Systematic Review and Meta-Analysis. J Pain Res, 15, 315-329. https://doi.org/10.2147/JPR.S351320
For individuals dealing with plantar fasciitis, every step can be painful. Can taking an integrative approach and utilizing acupuncture help treat this condition and accelerate symptom relief?
Acupuncture Plantar Fasciitis
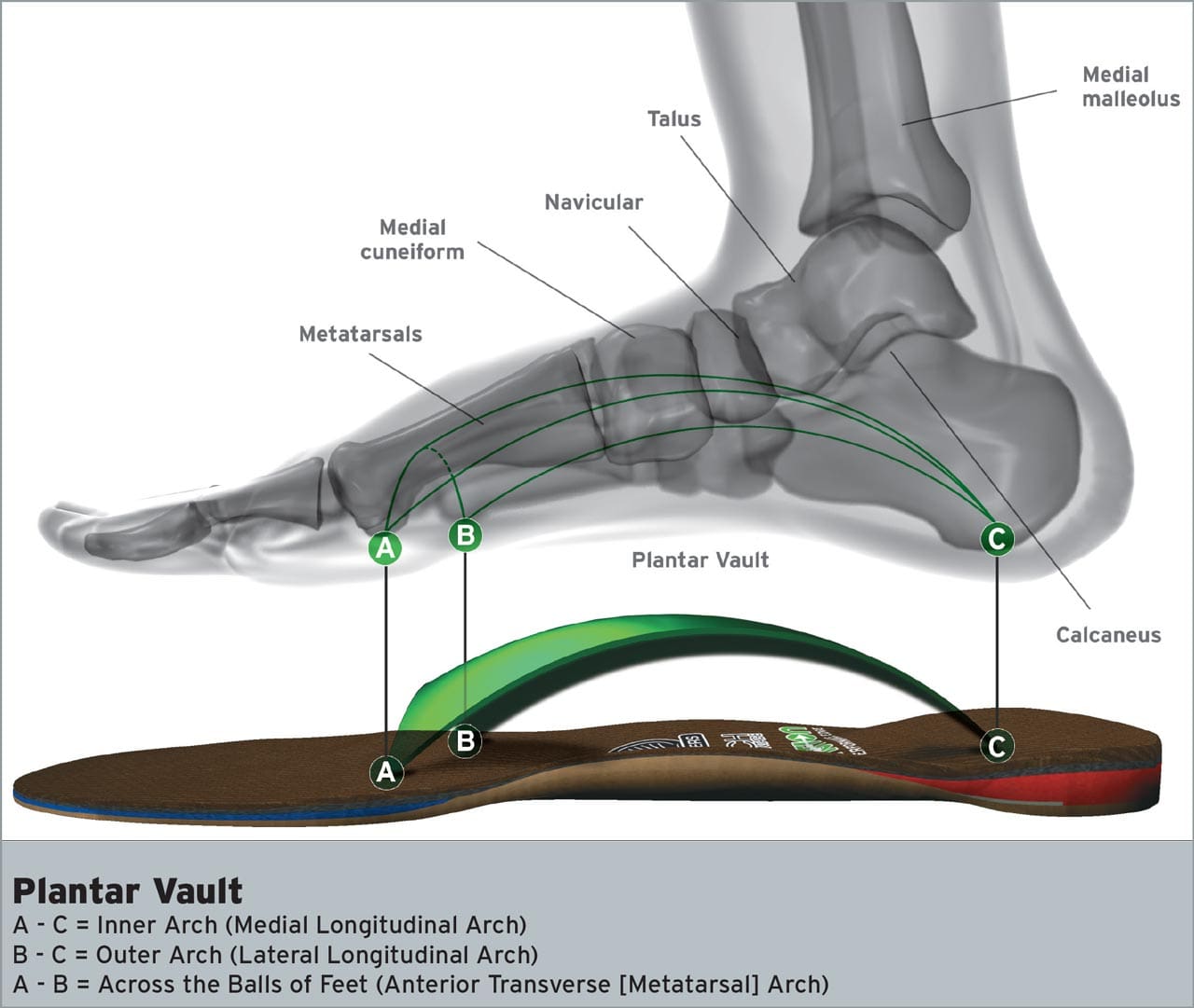
Plantar fasciitis is when the supportive tissue running under the foot, from the heel to the base of the toes, becomes irritated and painful. The disorder can be difficult to manage, but there are alternative treatment options. Acupuncture plantar fasciitis therapy is one potential method of relief, alleviating pain, and returning the individual to regular activities. Acupuncture involves inserting extremely thin needles into points in the body to restore and balance the normal flow of energy and improve overall health. (Johns Hopkins University. 2024) In traditional Chinese medicine or TCM, the body comprises a series of meridians/channels that supply energy flow or qi/chi.
Facts
Plantar fasciitis is a common disorder affecting the foot. The condition occurs when the plantar fascia, designed to absorb the forces that travel through the arch of the foot, becomes overloaded. When the bottom of the foot is constantly subjected to high amounts of strain, it leads to ligament degeneration, pain, and inflammation. The most common symptom is heel pain, the first thing an individual experiences in the morning or after a long day of work and activities. Anyone can get plantar fasciitis, but those who are more prone to the condition include individuals with:
Acupuncture and its effectiveness are still being studied, but there is evidence suggesting that it is beneficial in plantar fasciitis treatment.
One review found significant pain improvements in individuals who had acupuncture for the condition compared to individuals who received standard treatments like stretching, orthotics, and strengthening. (Anandan Gerard Thiagarajah 2017) The same review also found benefits when comparing acupuncture to a placebo version of the treatment, further reinforcing the findings.
Another medical review found that acupuncture helped alleviate heel pain and improve daily function when combined with nonsteroidal anti-inflammatory medications/NSAIDs such as ibuprofen or naproxen. (Richard James Clark, Maria Tighe 2012)
Side Effects
While acupuncture plantar fasciitis therapy is beneficial, it is important to remember there can be potential side effects that can include:
Pain in the area where the needles were placed.
Bleeding in the area where the needles were placed.
Bruising or skin discoloration.
Allergic reaction or contact dermatitis/itchy rash.
The chances of a serious adverse side effect are relatively low when undergoing acupuncture on the foot.
Acupuncture Points and Sensations
The ways acupuncture works are not yet fully understood, but like other neuromusculoskeletal therapies, the process activates the body’s healing properties.
Inserting a needle into the body’s points stimulates the central nervous system.
This leads to the release of chemicals in the brain, spinal cord, and muscles that promote healing.
These same chemicals and reactions also reduce the body’s sensation of pain. (Teng Chen et al., 2020)
Number of Sessions
The amount of sessions that acupuncture takes to provide pain relief varies from person to person and case to case.
One review found that treating plantar fasciitis weekly with acupuncture produced significant pain relief after four to eight weeks. (Anandan Gerard Thiagarajah 2017)
This corresponds to another medical review that included a study showing significantly improved pain levels in individuals undergoing weekly acupuncture sessions for four weeks. (Richard James Clark, Maria Tighe 2012)
Individuals are recommended to consult a healthcare provider about personalized treatment plans and if they have a bleeding disorder, are on blood thinner medications, or are pregnant.
American Academy of Orthopaedic Surgeons. (2022). Plantar fasciitis and bone spurs. (Diseases and Conditions, Issue. https://orthoinfo.aaos.org/en/diseases–conditions/plantar-fasciitis-and-bone-spurs
Thiagarajah A. G. (2017). How effective is acupuncture for reducing pain due to plantar fasciitis?. Singapore medical journal, 58(2), 92–97. https://doi.org/10.11622/smedj.2016143
Clark, R. J., & Tighe, M. (2012). The effectiveness of acupuncture for plantar heel pain: a systematic review. Acupuncture in medicine : journal of the British Medical Acupuncture Society, 30(4), 298–306. https://doi.org/10.1136/acupmed-2012-010183
Chan, M. W. C., Wu, X. Y., Wu, J. C. Y., Wong, S. Y. S., & Chung, V. C. H. (2017). Safety of Acupuncture: Overview of Systematic Reviews. Scientific reports, 7(1), 3369. https://doi.org/10.1038/s41598-017-03272-0
Chen, T., Zhang, W. W., Chu, Y. X., & Wang, Y. Q. (2020). Acupuncture for Pain Management: Molecular Mechanisms of Action. The American journal of Chinese medicine, 48(4), 793–811. https://doi.org/10.1142/S0192415X20500408
Can individuals dealing with neck pain incorporate acupuncture as part of their health and wellness treatment to relieve headaches?
Introduction
As part of the musculoskeletal system, the neck allows the head to go into full rotation without feeling discomfort or pain. The neck is part of the cervical spine region and is surrounded by numerous ligaments, muscles, and tissues that help protect the spinal cord and the spinal column. However, the neck is also the most susceptible to injury neck to back pain as it is one the top three complaints many individuals suffer from at some point in their lives. When people experience neck pain, numerous causes can contribute to developing neck pain, while pain-like symptoms like headaches contribute to the body. This causes many individuals to seek treatment and find the relief they are looking for to reduce neck pain while continuing their daily routine. Today’s article looks at how neck pain is associated with headaches and how treatments like acupuncture can help with neck pain and reduce the painful effects of headaches. We talk with certified medical providers who utilize our patients’ information to provide acupuncture treatments to lessen the impact of headaches caused by neck pain. We also inform patients how multiple non-surgical treatments can help reduce headaches and pain-like symptoms associated with neck pain. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from neck pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
Neck Pain & Headaches
Have you been experiencing unexplained stiffness along the sides of your neck? Do you feel a dull ache at the base of your neck or skull after looking down at your phone for an extended period? Or do you experience frequent headaches that are constant throughout the day? Many people dealing with these pain-like issues are associated with neck pain that is affecting their quality of life. Neck pain is amongst the top three complaints many people have experienced at some point. Neck pain has common presenting symptoms that are diagnosed, and the prevalence is much higher in older adults due to degenerative spinal changes in the facet joints and spinal discs. (Childress & Stuek, 2020) Many individuals experience common musculoskeletal pain conditions like muscle strains and stiffness when this happens. At the same time, neck pain can also be associated with neurological conditions that cause overlapping risk profiles, forcing many individuals to miss out on important events. Neck pain is a multifactorial musculoskeletal condition affecting many individuals as it induces them to miss work. This is because various modifiable and non-modifiable risk factors contribute to developing neck pain. (Kazeminasab et al., 2022) These risk factors can range from physical inactivity to poor posture, causing overlapping risk profiles that can trigger neck pain to advance over time.
So, how are headaches associated with neck pain? When a person is experiencing a headache, many would often think that the headaches are caused by not eating enough food or drinking enough water. Those are some of the factors that contribute to headaches, but they can also be due to the stress and comorbidities that are associated with neck pain. This is due to the risk factors many individuals don’t realize contribute to neck pain. Factors like the forward head position from smartphone usage cause tension on the cervical structures, generating potential degeneration and tearing of the neck structures. (Maayah et al., 2023) As repetitive motions affect the neck structure more over time, the nerve roots that surround the spine and spread through the upper extremities can become aggravated, and cause referred pain to different areas of the body, leading to headaches. When dealing with headaches associated with neck pain, they will feel stress, affecting their productivity. The headaches can range from acute to chronic, depending on the severity. Fortunately, many individuals dealing with headaches associated with neck pain will seek treatment to reduce the pain-like symptoms and feel the relief to return to their daily routine.
Healing After Trauma- Video
Many individuals who are dealing with neck pain often deal with headaches as a sign that risk factors are in play, like poor posture, slouching, or traumatic injuries that can affect their ability to work or participate in activities. This can cause many people to feel miserable and decrease their quality of life, thus causing them to seek out treatment for their pain, hence why many individuals opt for non-surgical treatments due to them being affordable and personalized. Non-surgical treatments range from chiropractic care to acupuncture, depending on the severity and location of where the pain is in the body. The video above shows how non-surgical treatments can help many individuals positively influence healing after a traumatic injury and restore a person’s well-being.
Acupuncture For Neck Pain
Non-surgical treatments are excellent for individuals trying to find the relief they seek in their neck pain. As stated earlier, non-surgical treatments are cost-effective and tailored to the person’s pain. Acupuncture is a form of non-surgical treatment that can help reduce the comorbidities associated with neck pain. Acupuncture is a medical practice in which highly trained, licensed, and certified professionals use solid, super-thin needles to be placed at specific points to treat the body. What this does is that when the needles are penetrating the points, it will begin to open any blockage or excess energy to flow correctly, restore balance to the body, and relieve the individual’s symptoms. (Berger et al., 2021) Some of the beneficial results that acupuncture can provide individuals with neck pain is a reduction of pain and disability to the neck while treating referred pain that is causing overlapping risk profiles to induce headaches. (Peron et al., 2022)
Acupuncture Relieving Headaches
Since headaches are associated with neck pain, acupuncture can help relieve the headaches from progressing further and enable many individuals to get back to their routine. Some overlapping risk profiles contributing to headaches include trigger points on the neck muscles that can cause non-dermatomal referral pain and discomfort. (Pourahmadi et al., 2019) When an acupuncturist is treating individuals for their headaches, many individuals will begin to feel the relief after a few consecutive sessions, and, combined with physical therapy to strengthen neck and shoulder muscles, will notice that the pain has been reduced significantly. Acupuncture is a safe, helpful, and available alternative treatment that is beneficial for many individuals dealing with headaches associated with neck pain. (Urits et al., 2020) By incorporating acupuncture as part of a person’s treatment plan, they can begin to feel the relief they deserve while also being more mindful of how they are treating their bodies to prevent pain-like symptoms from returning.
References
Berger, A. A., Liu, Y., Mosel, L., Champagne, K. A., Ruoff, M. T., Cornett, E. M., Kaye, A. D., Imani, F., Shakeri, A., Varrassi, G., Viswanath, O., & Urits, I. (2021). Efficacy of Dry Needling and Acupuncture in the Treatment of Neck Pain. Anesth Pain Med, 11(2), e113627. https://doi.org/10.5812/aapm.113627
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Maayah, M. F., Nawasreh, Z. H., Gaowgzeh, R. A. M., Neamatallah, Z., Alfawaz, S. S., & Alabasi, U. M. (2023). Neck pain associated with smartphone usage among university students. PLOS ONE, 18(6), e0285451. https://doi.org/10.1371/journal.pone.0285451
Peron, R., Rampazo, E. P., & Liebano, R. E. (2022). Traditional acupuncture and laser acupuncture in chronic nonspecific neck pain: study protocol for a randomized controlled trial. Trials, 23(1), 408. https://doi.org/10.1186/s13063-022-06349-y
Pourahmadi, M., Mohseni-Bandpei, M. A., Keshtkar, A., Koes, B. W., Fernandez-de-Las-Penas, C., Dommerholt, J., & Bahramian, M. (2019). Effectiveness of dry needling for improving pain and disability in adults with tension-type, cervicogenic, or migraine headaches: protocol for a systematic review. Chiropr Man Therap, 27, 43. https://doi.org/10.1186/s12998-019-0266-7
Urits, I., Patel, M., Putz, M. E., Monteferrante, N. R., Nguyen, D., An, D., Cornett, E. M., Hasoon, J., Kaye, A. D., & Viswanath, O. (2020). Acupuncture and Its Role in the Treatment of Migraine Headaches. Neurol Ther, 9(2), 375-394. https://doi.org/10.1007/s40120-020-00216-1
For individuals dealing with neck or arm pain and migraine headache symptoms it could be a splenius capitis muscle injury. Can knowing the causes and symptoms help healthcare providers develop an effective treatment plan?
Splenius Capitis Muscles
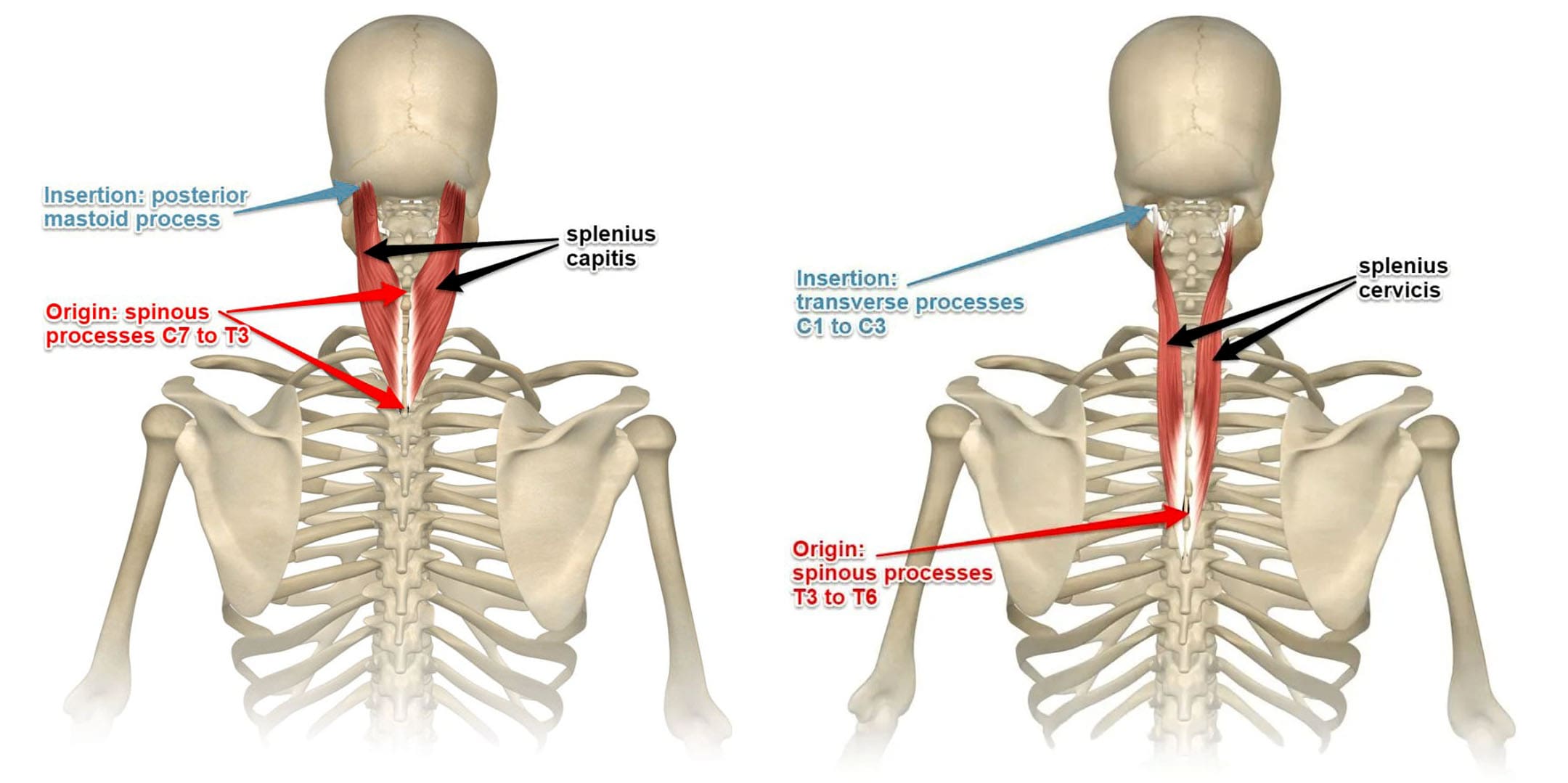
The splenius capitis is a deep muscle located on the upper back. Along with the splenius cervicis, it comprises the superficial layer – one of the three – of intrinsic back muscles. The splenius capitis works with the splenius cervicis, a smaller muscle located below it, to help rotate the neck and lower the chin to the chest, known as flexing. Maintaining a healthy posture is important because it helps keep the head in a neutral position.
Starting at the midline of the spine at C3 to T3, the splenius capitis spans the levels between the 7th cervical vertebra to the 3rd or 4th thoracic vertebrae, which varies for different individuals.
The muscle inserts at the nuchal ligament, which is a strong ligament of the neck.
The splenius capitis muscle angles up and out, attaching to the skull.
The splenius capitis and cervicis cover the vertical paraspinals, which are deeper and comprise the intermediate layer of the intrinsic back muscles.
The splenius muscles look like a bandage for the paraspinals and the vertical muscles that comprise the deepest layer.
The splenius muscles hold these deeper layers in the correct position.
These muscles start at the center of the spine and together form a V shape.
The sides of the V are thick, and the central indentation is shallow.
Pain
It’s common for individuals to experience pain associated with injury to the splenius capitis. This type of pain is known as splenius capitis syndrome. (Ernest E, Ernest M. 2011)
Symptoms
A headache stemming from injury often mimics a migraine headache. Symptoms of splenius capitis syndrome include: (Ernest E, Ernest M. 2011)
It’s recommended to contact a healthcare provider if experiencing symptoms that interfere with daily activities or quality of life. A healthcare provider will:
Can individuals with osteoarthritis incorporate spinal decompression therapy to restore spinal mobility and quality of life?
Introduction
As the body ages, so does the spine, as the spinal disc between the joints and the bones starts dehydrating from constant compression through repetitive motions. The many environmental factors contributing to this degenerative disorder can vary within the person and lead to arthritic conditions within the upper and lower extremities. One of the most common types of arthritis is osteoarthritis, and it can affect many people worldwide. Dealing with osteoarthritis in their joints can cause numerous pain-like symptoms that correlate with other body conditions, causing referred pain. However, many treatments can help slow the process of osteoarthritis and relieve the body from the pain-like symptoms of the joints. Today’s article looks at how osteoarthritis affects spinal mobility and how treatments can restore spinal mobility from the effects of osteoarthritis. We talk with certified medical providers who utilize our patients’ information to provide various treatments to reduce the impact of osteoarthritis on the joints. We also inform patients how multiple treatments can help slow down the degenerative process of osteoarthritis. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from osteoarthritis. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
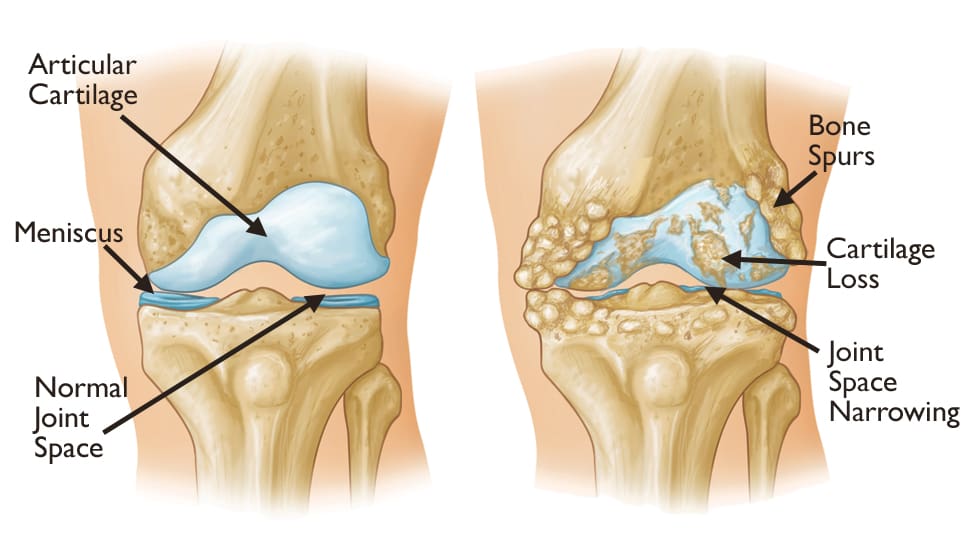
How Does Osteoarthritis Affect Spinal Mobility?
Have you noticed morning stiffness after a good night’s rest? Do you feel tenderness in your joints after some light pressure? Or do you feel limited mobility in your joints, causing a restricted range of motion? Many of these pain-like scenarios are correlated with osteoarthritis, a degenerative joint disorder that has affected many individuals, including older adults. As stated earlier, when the body ages, so do the joints, bones, and spine. Regarding osteoarthritis, the joints will degenerate through natural wear and tear around the cartilage. Osteoarthritis affects multiple joints like the hips and knees, which are the most common, and the spine, and causes numerous sensory-motor dysfunctions. (Yao et al., 2023) When the cartilage around the affected joints starts to deteriorate, the pathogenesis of osteoarthritis causes a disturbed cytokine balance of the proinflammatory cytokines to initiate a vicious cycle that causes cartilage and other intra-articular structure damage around the joint. (Molnar et al., 2021) What this does is that when osteoarthritis starts to affect the joints, it can lead to numerous referred pain-like symptoms.
However, although osteoarthritis can affect the joints, naturally, numerous environmental factors do play a part in the development of osteoarthritis. Physical inactivity, obesity, bone deformities, and joint injuries are some of the causes that can progress the degenerative process. The symptoms that are associated with these environmental factors include:
Pain
Joint stiffness
Tenderness
Inflammation
Swelling
Grating sensation
Bone spurs
Many individuals dealing with pain-like symptoms caused by osteoarthritis will explain to their primary doctors that the pain varies in duration, depth, type of occurrence, impact, and rhythm. This is because the pain from osteoarthritis is complex and multifactorial. (Wood et al., 2022) However, many individuals can look for the help they need to reduce the pain-like issues caused by osteoarthritis through treatments that can slow down the degenerative progress.
An In-depth Look At Spinal Decompression-Video
When it comes to seeking treatment to reduce the effects of osteoarthritis, many individuals seek out treatments that are cost-effective and safe for older individuals. Non-surgical treatments could be the solution many individuals seek to reduce the progress of osteoarthritis. When people experiencing osteoarthritis go to non-surgical treatments, they find out that the pain is decreased, their range of motion is increased, and their physical function has improved. (Alkhawajah & Alshami, 2019) At the same time, non-surgical treatments can be combined with other therapies to the individual’s personalized treatment plan. No-surgical treatments can range from chiropractic care to spinal decompression as they work on gently realigning the spine through traction and help reduce joint and muscle pain. The video above gives an in-depth look at spinal decompression and how it can benefit individuals who are in pain.
Spinal Decompression Restoring Spinal Mobility From Osteoarthritis
Since spinal decompression is a form of non-surgical treatment, it can help slow down the process of osteoarthritis. Spinal decompression incorporates traction to gently pull on the spine, allowing the discs and joints to be lubricated and permitting the natural healing process to occur. This is because the surrounding muscles that protect the joints are being stretched gently and the vertebral disc space is being increased to allow the disc to be rehydrated and the protrusion to recede back to its original position. (Cyriax, 1950) Spinal decompression can help slow down the degenerative process of osteoarthritis, and when combined with physical therapy, the surrounding muscles, tissues, and ligaments are strengthened.
In contrast, joint and spinal mobility and flexibility are increased. Spinal decompression can also help many individuals reduce their chances of surgery, as consecutive sessions can help provide pain relief and functional improvement to the spine. (Choi et al., 2022) When people regain their spinal mobility back to their bodies from spinal decompression, they can make small changes in their daily routine to slow down the degenerative process of osteoarthritis.
References
Alkhawajah, H. A., & Alshami, A. M. (2019). The effect of mobilization with movement on pain and function in patients with knee osteoarthritis: a randomized double-blind controlled trial. BMC Musculoskelet Disord, 20(1), 452. https://doi.org/10.1186/s12891-019-2841-4
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Molnar, V., Matisic, V., Kodvanj, I., Bjelica, R., Jelec, Z., Hudetz, D., Rod, E., Cukelj, F., Vrdoljak, T., Vidovic, D., Staresinic, M., Sabalic, S., Dobricic, B., Petrovic, T., Anticevic, D., Boric, I., Kosir, R., Zmrzljak, U. P., & Primorac, D. (2021). Cytokines and Chemokines Involved in Osteoarthritis Pathogenesis. Int J Mol Sci, 22(17). https://doi.org/10.3390/ijms22179208
Wood, M. J., Miller, R. E., & Malfait, A. M. (2022). The Genesis of Pain in Osteoarthritis: Inflammation as a Mediator of Osteoarthritis Pain. Clin Geriatr Med, 38(2), 221-238. https://doi.org/10.1016/j.cger.2021.11.013
Yao, Q., Wu, X., Tao, C., Gong, W., Chen, M., Qu, M., Zhong, Y., He, T., Chen, S., & Xiao, G. (2023). Osteoarthritis: pathogenic signaling pathways and therapeutic targets. Signal Transduct Target Ther, 8(1), 56. https://doi.org/10.1038/s41392-023-01330-w
For individuals that are feeling unmotivated to work out and exercise can developing a fitness mindset help improve and maintain motivation?
Fitness Mindset Motivation
Learning to exercise as part of a regular workout routine can have a significant impact on health and well-being. In the beginning, individuals are all in, but as time goes on, mental blocks can interfere with workout motivation. Being flexible with oneself and fitness/health goals is part of the process, and overcoming mental blocks is key to maintaining motivation. It’s all about creating a fitness mindset to maintain confidence and motivation and enjoy the benefits of regular exercise.
Feeling Tired
When feeling tired, individuals should ask themselves if it’s physical or mental fatigue. If the exhaustion is not from lack of sleep, illness, or a physically demanding job, it is more than likely mental tiredness. Mental exhaustion can often feel physical, and a recommended cure is physical activity. Often, once an individual starts working out and gets over the mental fatigue, they feel better. (Juriena D. de Vries et al., 2016) Regular physical activity can increase energy levels and leave the body feeling less fatigued. (Bryan D. Loy et al., 2013) However, individuals need to make sure there is ample recovery time to repair and restore the body after working out.
Self-Talk
Sometimes there is a small voice that says to take a day off or perform an easier workout. It’s okay to be flexible, but most times, individuals need to be ready to stand up to the skip-the-workout voices and stay motivated.
Remove Obstacles
Remove obstacles that can distract from exercising.
Have the workout gear ready and exercise time pre-scheduled so there are no second thoughts.
If limited space is an issue, find compact equipment like a cordless jump rope that doesn’t require a lot of room.
Don’t Allow Relaxation Takeover
Individuals who plan to exercise after school or work shouldn’t go home, sit down, and relax watching TV before working out.
Individuals who may need a transition to work out should try something gentle but active, like stretching or doing a light chore.
Individuals who exercise in the morning should wear their workout clothes immediately, so they can’t second guess and can continue their workout.
Remind yourself of the reasons for committing to exercise.
Research shows that using second-person self-talk can help maintain motivation. Encouraging oneself with phrases like you can do this, you got this, or you are going to achieve your fitness goals improves the chances of obtaining the desired outcome. (Sanda Dolcos, Dolores Albarracin. 2014)
Fight Through The Doubt
Start with small steps. Ask if doubt is stopping you from starting. If doubt begins to arise:
Ask For Help
A colleague, friend, or partner can help reinspire motivation.
Tell them about the challenges of sticking with exercise.
Ask them to work out together.
Do What Is Possible
If working out for 30 minutes is too difficult, don’t worry about it.
Go for as long as possible and try for more the next time.
Working out can feel like a job, but it does not have to.
For example, individuals sitting or standing all day can approach the workout as 30 minutes to get out and move around.
Or, after getting the kids settled in, it is time to do something for yourself and exercise the stress away.
Healthy Reminders
Write inspirational fitness mindset notes and put them where they will be seen regularly.
These can be exercise goals; for example, I will exercise for 30 minutes because I want more energy, better sleep, strength, etc.
Train The Brain For Exercise
When the issue is motivation, the mind needs to be convinced to exercise. How to use mind-over-matter skills:
Rewards
When finishing a workout, rewards can help.
Exercise has its own rewards – more energy, improved mood, stress relief, and reduced disease risk.
Maybe a new pair of shoes, earbuds or headphones, workout equipment, or a massage will increase motivation.
Make A Deal
Continue to exercise for whatever amount of time, and if the desire to stop is still present, then stop.
Nine times out of 10, individuals will keep going.
Pretend
Make-believe can encourage the fitness mindset.
Pretending to be in a race, or in a movie, anything that makes the body want to move.
Set Achievable Goals
Making difficult goals can generate the fear of being unable to achieve them.
Aim for small achievable goals that go along with a bigger overall goal.
That way, there are more victories, and the motivation to keep moving is maintained.
Competition
Healthy competition can be a great motivator.
Competing with oneself for faster times, heavier weights, or more frequency can keep the inspiration going.
Social media and apps to compete with family and friends can also help.
Visualization
Athletes use visualization techniques of going through the game, match, and tournament to get themselves prepared and ready to execute what they’ve been practicing.
Individuals can do the same thing by picturing themselves going through their workout from beginning to end.
Exercise provides meditation time to think about problems and challenges.
Use the workout time to work through the problems and refocus strategies to solve them.
Process Goals
Choosing specific goals that are part of the workout process, like working out 3-4 times per week, is recommended compared to using outcome goals, like losing ten pounds.
Outcome goals can be out of the individual’s control; instead, focus on the steps to achieve the goals, which lessens stress and is a more controllable method of working out. (Kylie Wilson Darren Brookfield. 2011)
Changing lifestyle to include exercise is not easy. The most important step is having the right attitude. (Margie E. Lachman et al., 2018) Thinking about exercise as an obligation will discourage motivation. Instead, create a fitness mindset to treat exercise like a break from all the stress and a reward for the mind and body to a healthier life.
Home Exercises for Pain Relief
References
de Vries, J. D., van Hooff, M. L., Geurts, S. A., & Kompier, M. A. (2016). Exercise as an Intervention to Reduce Study-Related Fatigue among University Students: A Two-Arm Parallel Randomized Controlled Trial. PloS one, 11(3), e0152137. https://doi.org/10.1371/journal.pone.0152137
Bryan D. Loy, Patrick J. O’Connor & Rodney K. Dishman (2013) The effect of a single bout of exercise on energy and fatigue states: a systematic review and meta-analysis, Fatigue: Biomedicine, Health & Behavior, 1:4, 223-242, DOI: 10.1080/21641846.2013.843266
Dolcos S, Albarracin D. (2014). The inner speech of behavioral regulation: Intentions and task performance strengthen when you talk to yourself as a You. Eur J Social Psychol. 44(6):636-642. doi:10.1002/ejsp.2048.
Lachman, M. E., Lipsitz, L., Lubben, J., Castaneda-Sceppa, C., & Jette, A. M. (2018). When Adults Don’t Exercise: Behavioral Strategies to Increase Physical Activity in Sedentary Middle-Aged and Older Adults. Innovation in aging, 2(1), igy007. https://doi.org/10.1093/geroni/igy007
Renner, F., Murphy, F. C., Ji, J. L., Manly, T., & Holmes, E. A. (2019). Mental imagery as a “motivational amplifier” to promote activities. Behaviour research and therapy, 114, 51–59. https://doi.org/10.1016/j.brat.2019.02.002
Kylie Wilson & Darren Brookfield (2009). Effect of Goal Setting on Motivation and Adherence in a Six‐Week Exercise Program, International Journal of Sport and Exercise Psychology, 7:1, 89-100, DOI: 10.1080/1612197X.2009.9671894
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine