Can using a cane help individuals after an injury, living with chronic pain or balance issues, or post-surgery?
Walking With A Cane
A cane is an assistive device that can help individuals walk after injury or surgery and aids with balance and stability. It can be used for:
Balance or Stability Issues
Canes can help with minor balance or stability issues, such as weakness in the leg or trunk, or after an injury.
Pain
Canes can help reduce stress on painful joints or limbs.
Independence
Canes can help people continue living independently, especially the elderly.
There are different types of canes, including single-point and quad canes. Single-point canes are generally the least expensive. Quad canes have four points and can provide more stability. It is important to use it correctly to prevent falls and injuries.
Post-surgery or Injury
A cane can help reduce pressure on the leg or back after surgery or injury. Healthcare providers may recommend a cane as a step-down device after using a walker or crutches. Before walking with the cane, ensure it is at the right height. Hold the cane in the hand on the opposite side of the injury. Hold the cane’s handle at the level of the bend in the wrist when standing with the elbow slightly bent. (American Academy of Orthopaedic Surgeons, 2020) If there are issues in both legs or a cane is used after back surgery, keep the cane in the hand with the most support.
Step forward with the cane and injured leg at the same time.
Step the non-injured leg up with the cane firmly on the ground to meet the injured leg.
The feet should be side by side.
Walking Normally
Once comfortable taking practice steps, try walking normally with the cane. Step forward with the cane and injured leg simultaneously. The cane should be off the ground when the wounded leg is in the air. Firmly plant the cane when stepping onto the injured leg. Step forward with the cane and the injured leg first, then step past the injured leg with the good leg.
Step down with the injured leg while lowering the cane to the step below.
Make sure the cane is firmly on the stairs.
Bring the good leg down to the same step.
If a handrail is available, use it. Although doing so may require moving the cane to the other hand, even if it’s on the same side as the injured leg, it will improve stability and reduce the risk of falling. Once proficient on the stairs, individuals may alternate placing one foot on each step.
Walking With Chronic Pain
Walking with a cane with a chronic pain condition is similar to using it with an injury. The location of the pain will determine which hand the cane is held in. If the pain is on the right side of the body, keep the cane on the left side or vice versa. If chronic pain is not in the legs but, for example, back pain makes it difficult to walk, hold the cane on either side, whichever feels more supportive and comfortable. If there is weakness on one side of the body or decreased sensation/numbness in one of the legs or feet, hold the cane on the opposite side of the pain, weakness, or numbness. Walking with a cane can also benefit individuals with other medical conditions. For example, assistive devices may be recommended for those with balance issues. (National Library of Medicine, 2023)
Cane Types
There are two primary types of canes, characterized by their points, and choosing the right one depends on the reason it’s needed. (Arthritis Foundation, N.D.)
Single-point
Single-point canes have one tip at the end.
These are recommended for those who need to relieve some pressure off an injured leg or need support due to occasional difficulties with balance.
Quad
Quad canes have four tips or feet to provide more stability.
They provide more support and are recommended for those with significant weakness in one leg or difficulty maintaining their balance while walking.
The traditional cane has a rounded C handle. Other types have contoured handles for a more secure grip. Talk to a doctor, physical therapist, or other health care professional for suggestions on which cane is right for you.
Losing Balance
A potential risk of using a cane is losing balance. If unable to maintain balance with a cane, individuals may want to consider a different walking device, such as a walker or crutches. To reduce the risk of falls, consider the following tips (American Academy of Orthopaedic Surgeons, 2020)
Wear shoes with nonskid soles.
Add lighting so you can see where you are walking.
Remove throw rugs or objects that can cause tripping.
Arrange furniture to allow for wide walking paths throughout the home.
Carry objects in a backpack or fanny pack rather than holding them.
Injury Medical Chiropractic and Functional Medicine Clinic
Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other associated medical professionals to develop a personalized treatment plan to help relieve muscle pain, improve the body’s flexibility and mobility, resolve musculoskeletal issues, and prevent future pain symptoms from reoccurring.
Osteoporosis
References
American Academy of Orthopaedic Surgeons. (2020). How to use crutches, canes, and walkers. https://orthoinfo.aaos.org/en/recovery/how-to-use-crutches-canes-and-walkers/
Hirayama, K., Otaka, Y., Kurayama, T., Takahashi, T., Tomita, Y., Inoue, S., Honaga, K., Kondo, K., & Osu, R. (2022). Efficiency and Stability of Step-To Gait in Slow Walking. Frontiers in human neuroscience, 15, 779920. https://doi.org/10.3389/fnhum.2021.779920
National Library of Medicine. (2023). Using a cane. Retrieved from https://medlineplus.gov/ency/patientinstructions/000343.htm
Arthritis Foundation. (N.D.). How to choose the right cane. https://www.arthritis.org/health-wellness/healthy-living/managing-pain/joint-protection/how-to-choose-the-right-cane
Individuals who have experienced spinal or back trauma, suffered fractures, are going through spinal degeneration, or are dealing with a spinal condition have an increased risk of anterolisthesis, where a vertebra slips forward relative to the vertebra below it. Can healthcare providers help prevent and treat the condition?
Anterolisthesis
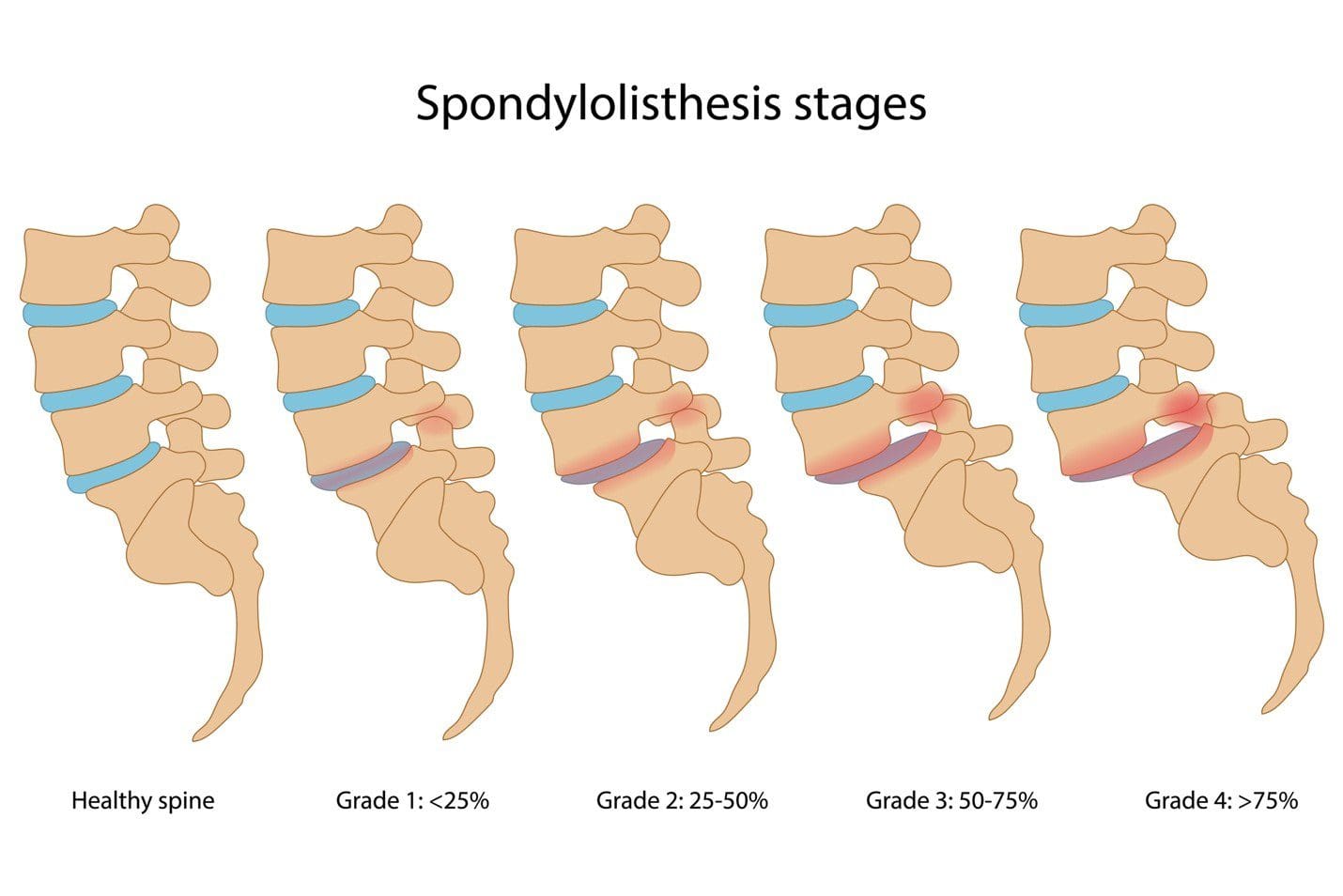
The spine consists of 33 individual bones or vertebrae stacked on one another. Anterolisthesis occurs when one vertebral segment slips forward over another. The condition can be mild, asymptomatic, or cause significant pain and neurological symptoms. Many different things, including osteoarthritis, osteoporosis, trauma, or a fracture, can cause this vertebral shifting. (Cedars Sinai, 2022) Spondylolisthesis is a general term for shifting a spinal vertebra over the one below it. It includes anterolisthesis, forward moving, and the less common retrolisthesis, or backward shifting.
Grades
Anterolisthesis is typically graded using the Meyerding scale, which assigns one of five grades according to how much slippage has occurred. These grades include:
Anterolisthesis can lead to various symptoms, depending on the severity and if the surrounding spinal nerves have been affected. The most common complaints include:
Diagnosis begins with a subjective evaluation and a physical examination. During these, the healthcare provider will assess sensation, strength, and reflexes and will order one of several diagnostic tests, including:
X-rays
Visualizes the vertebrae in the spine and their position relative to those above and below.
Also provides a clear picture of spinal arthritis or disc degeneration.
Magnetic Resonance Imaging – MRI
Allows the spinal cord, nerves, muscles, and discs to be assessed for compression or damage.
Several factors determine how the condition is treated, including:
The grade of the slippage.
The cause.
The symptoms.
The presence of instability on a diagnostic test such as an X-ray.
Stable and mildly symptomatic cases are usually treated with a combination that can involve:
Physical therapy
Activity modification
Bracing
Nonsteroidal anti-inflammatory medications/NSAIDs like ibuprofen.
Spinal injections
In more severe cases in which spinal instability or significant neurological symptoms are present, surgery may be recommended. This commonly involves a spinal decompression or fusion procedure. The technique varies based on the surgeon’s preferences and anatomy. (Koslosky E., and Gendelberg D. 2020)
Prognosis
Most individuals with this condition don’t know they have it until it is found accidentally on an X-ray or an MRI for something else. Mild cases can cause minimal symptoms and can be well-managed with conservative treatments. Cases of unstable anterolisthesis or those with neurological compression often require surgical intervention. These surgeries restore stability to the spine and alleviate any pressure on the nerves. More than 85% of individuals who need surgery have a successful outcome. (American Academy of Orthopaedic Surgeons, 2021)
Self-Care and Management
For individuals experiencing pain, numbness, or tingling from anterolisthesis, getting symptoms evaluated by a healthcare provider is an important first step. The healthcare provider may suggest one of several management strategies, which include:
Core Strengthening
To alleviate symptoms, exercises targeting the core muscles in the hips, pelvis, abdomen, and lower back are recommended.
Formal physical therapy may also be recommended.
Over-the-counter Meds
A healthcare provider may suggest pain-relieving medications like ibuprofen or naproxen to reduce soreness.
Activity Modification
Sticking to gentle, pain-free activities and avoiding excessive or repetitive extension of the spine can help prevent symptom aggravation. (American Academy of Orthopaedic Surgeons, 2021)
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for you to relieve pain and restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Koslosky, E., & Gendelberg, D. (2020). Classification in Brief: The Meyerding Classification System of Spondylolisthesis. Clinical orthopaedics and related research, 478(5), 1125–1130. https://doi.org/10.1097/CORR.0000000000001153
American Academy of Orthopaedic Surgeons. (2021). Adult spondylolisthesis in the low back. https://orthoinfo.aaos.org/en/diseases–conditions/adult-spondylolisthesis-in-the-low-back
Hospital for Special Surgery. (2023). Spondylolisthesis. https://www.hss.edu/condition-list_spondylolisthesis.asp
Can individuals incorporate proper posture in their workouts to provide effective results and reduce muscle pain in their bodies?
Introduction
Many people have started participating in various physical activities to improve their health and wellness. Additionally, engaging in different physical activities can provide numerous beneficial properties for the body as it can help strengthen the various muscles, bones, and ligaments that have succumbed to multiple injuries, strains, or conditions that cause many individuals to be in pain. When many people with musculoskeletal conditions start incorporating exercises as part of their treatment, maintaining proper posture while doing each set of stretches or exercises for each muscle can help reduce any unwanted strain or pulls that can cause more harm than good. Today’s post focuses on how maintaining proper posture can help make any workouts more efficient, how adequate posture can provide stability and strength to weak muscles, and how incorporating proper posture in a customized treatment plan can prevent numerous injuries from reoccurring. We discuss with certified associated medical providers who consolidate our patients’ information to assess many individuals to understand the importance of proper posture. We also inform and guide patients while asking their associated medical provider intricate questions to integrate non-surgical treatments to reduce the overlapping symptoms correlating with poor posture and help create a customized treatment plan that utilizes proper posture during exercises. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
Maintaining Posture Is Important For Effective Workouts
How often do you feel muscle strain on your shoulders, neck, and lower back after a strenuous long day? Do you notice that you feel more hunched over that you feel muscle aches and discomfort? Or do you feel discomfort when stretching your muscles that it causes temporary relief? More often than not, when the world has been on its entire feet or sitting down all day from working, school, or commuting to different locations, many individuals will often slip into an unhealthy habit of slouching when relaxing after a hard day. This, in turn, can cause many individuals to develop neck and back issues that often correlate with an increased stress load in the neck and lower back area. (Hansraj, 2014) Hence, postural correction and its beneficial effects on the back and neck are limited. However, when manual and physical therapists incorporate a PSB (postural-structural-biomechanical) model, it can help ascertain the various causes of musculoskeletal conditions and play an important role in clinical assessment and managing multiple muscle pains. (Lederman, 2011)
So why is it important to exercise to maintain proper posture? Well, when many individuals are in a hunched position from looking at their phones or leaning a lot more while being on the computer or driving, itcan cause the muscles in the neck, shoulders, and upper back to be in a static position, causing the muscles to be overused. (Abd El-Azeim et al., 2022) Additionally, say a person is working out to relieve stress, they would have to maintain a proper posture to prevent injuries and use the equipment to achieve muscular activity. When doing an effective workout, many individuals can improve their posture through muscle stretching exercises that can help improve postural alignment, which plays a role in preventing and treating musculoskeletal pain disorders. (Matsutani et al., 2023) At the same time, maintaining proper posture while working out can provide effective, good-quality movement and neutral spinal alignment.(Katzman et al., 2021)
Discovering The Benefits Of Chiropractic Care- Video
Proper Posture Stabilizes Weak Muscles
At the same time, having proper posture can help stabilize weak muscles in the upper and lower body quadrants. This is because environmental factors like obesity, repetitive movements, andexcessive sitting or standing can cause the muscles to be overused and weak over time when a person is not taking a break. This causes strength imbalances between the muscle groups, causing the accessory muscles to take over the main muscle’s job function and causing the spine to compensate and exaggerate the body’s natural curve. Hence why, exercises, especially core exercises, can help distribute the weight of the overbearing load and can help many individuals reduce the forward lean motion while decreasing muscle strain and fatigue on the upper and lower quadrants. Core exercises can help induce muscular contractions while influencing neuromuscular potentiation. (Lyons et al., 2021) This can help strengthen the weak muscles and stabilize the other muscles so the body can be realigned to invoke proper posture. Also, poor posture can correlate with lumbar spine and pelvis instability as the muscles can become weak. (Kim & Yim, 2020) Incorporating stability exercises into the weak muscles can help many individuals improve their posture when performing exercises.
Incorporating Proper Posture In A Customed Treatment Plan
When it comes to musculoskeletal pain conditions, many individuals can seek out pain specialists like chiropractors, acupuncturists, massage therapists to ease the pain in the muscles from an initial visit. Visiting a chiropractic care office or going to a gym and being assigned to a personal trainer can help practice healthy habits in maintaining and incorporating proper posture in a customized treatment plan. A chiropractic team can help mitigate the pain through spinal adjustments that can help the body realign itself and can work with other associated medical professionals to come up with a customer treatment plan that can help relieve muscle pain, improve the body’s flexibility and mobility, resolve musculoskeletal issues and prevent future pain symptoms from reoccurring. Additionally, a physical therapist can work together with a chiropractor to incorporate targeted exercises to help improve posture while stretching and strengthening the targeted muscles. This, in turn, helps with improving neuromuscular improvement to maintain correct posture. When many individuals develop improper posture over time, it can lead to dire consequences, as muscle pain can cause overlapping risk profiles in the body. Making small adjustments to how people sit or stand can help maintain proper posture. That way, the body can realign itself over time, and many can have a pain-free, healthy lifestyle.
References
Abd El-Azeim, A. S., Mahmoud, A. G., Mohamed, M. T., & El-Khateeb, Y. S. (2022). Impact of adding scapular stabilization to postural correctional exercises on symptomatic forward head posture: a randomized controlled trial. Eur J Phys Rehabil Med, 58(5), 757-766. https://doi.org/10.23736/S1973-9087.22.07361-0
Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int, 25, 277-279. https://www.ncbi.nlm.nih.gov/pubmed/25393825
Katzman, W. B., Parimi, N., Gladin, A., Wong, S., & Lane, N. E. (2021). Long-Term Efficacy of Treatment Effects After a Kyphosis Exercise and Posture Training Intervention in Older Community-Dwelling Adults: A Cohort Study. J Geriatr Phys Ther, 44(3), 127-138. https://doi.org/10.1519/JPT.0000000000000262
Kim, B., & Yim, J. (2020). Core Stability and Hip Exercises Improve Physical Function and Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial. Tohoku J Exp Med, 251(3), 193-206. https://doi.org/10.1620/tjem.251.193
Lederman, E. (2011). The fall of the postural-structural-biomechanical model in manual and physical therapies: exemplified by lower back pain. J Bodyw Mov Ther, 15(2), 131-138. https://doi.org/10.1016/j.jbmt.2011.01.011
Lyons, K. D., Parks, A. G., Dadematthews, O., Zandieh, N., McHenry, P., Games, K. E., Goodlett, M. D., Murrah, W., Roper, J., & Sefton, J. M. (2021). Core and Whole Body Vibration Exercise Influences Muscle Sensitivity and Posture during a Military Foot March. Int J Environ Res Public Health, 18(9). https://doi.org/10.3390/ijerph18094966
Matsutani, L. A., Sousa do Espirito Santo, A., Ciscato, M., Yuan, S. L. K., & Marques, A. P. (2023). Global posture reeducation compared with segmental muscle stretching exercises in the treatment of fibromyalgia: a randomized controlled trial. Trials, 24(1), 384. https://doi.org/10.1186/s13063-023-07422-w
Can determining whether arm numbness occurs suddenly or gradually and whether there are other symptoms help healthcare providers diagnose and treat the condition?
Arm Numbness
Arm numbness or tingling are common symptoms that various medical conditions can cause. Numbness can be caused by a sudden health emergency, nerve disorder, or nutritional deficiency. (National Institute of Neurological Disorders and Stroke, 2024) Sometimes, this symptom results from an arm falling asleep and could resolve after just a few minutes. The sensation may be temporary, caused by something like sleeping in the wrong position. However, arm numbness and tingling may also be caused by neuropathy and chronic and progressive nerve damage and can also suddenly occur due to serious conditions, such as a heart attack or a stroke.
Circulation Issues
Deficient blood circulation in the arm could cause numbness and tingling as the nerves cannot receive enough oxygen. Conditions can interfere with normal blood flow and include: (Bryan L. and Singh A. 2024)
Atherosclerosis – plaque buildup in the arteries that may require medication or surgery.
Severe frostbite can damage the blood vessels but can be resolved with proper warming and wound care.
Vasculitis – is inflammation of the blood vessels that can be treated with medication.
Sleeping Position
A common example of sudden numbness and tingling is the feeling that the arm has fallen asleep. This usually occurs after sleeping awkwardly or leaning on the arm for a long time. Known as paresthesia, this sensation is related to the compression or irritation of nerves. (Bryan L. and Singh A. 2024) Sleeping in certain positions has been associated with nerve compression, especially when the hands or wrists are tucked or curled under the body, as well as maintaining proper spine alignment when sleeping, is the best way to prevent arm numbness.
Nerve Injuries and Conditions
Numbness that persists may be related to an injury or underlying health problem that affects the brachial plexus, a group of nerves that runs from the lower neck to the upper shoulders and controls movement and sensation in the arms. (Mount Sinai, 2022) Possible injuries that affect these nerves include: (Smith, S. M. et al., 2021)
A herniated disc caused by aging or trauma causes the disc to leak out and press on the nerve root.
Many medications, like gabapentin, can be used to alleviate the sensations of arm numbness.
Some medications can cause numbness as a side effect.
Some medications can cause complications, and arm numbness could be a symptom of those complications.
Inform healthcare providers about medications being taken to determine the relationship between them and any sensory changes.
Vitamin Deficiency
Peripheral neuropathy can also be caused by nutritional deficiencies and vitamin imbalances, which can damage nerves and cause sensation loss in the left or right arm. The most common sources are vitamin B12 deficiency and excess vitamin B6. (National Institute of Neurological Disorders and Stroke, 2024) Excessive alcohol consumption and other disorders that affect nutritional intake can also lead to nerve damage.
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for you to relieve pain and restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Chiropractic Care: The Natural Way to Recover From Injuries
References
National Institute of Neurological Disorders and Stroke. (2024). Paresthesia. Retrieved from https://www.ninds.nih.gov/health-information/disorders/glossary-neurological-terms#paresthesia
Bryan, L., Singh, A. Sleep Foundation. (2024). Numbness in Hands While Sleeping: Causes and Remedies. https://www.sleepfoundation.org/physical-health/numbness-in-hands-while-sleeping
Mount Sinai. (2022). Brachial plexopathy. https://www.mountsinai.org/health-library/diseases-conditions/brachial-plexopathy
Smith, S. M., McMullen, C. W., & Herring, S. A. (2021). Differential Diagnosis for the Painful Tingling Arm. Current sports medicine reports, 20(9), 462–469. https://doi.org/10.1249/JSR.0000000000000877
National Heart, Lung, and Blood Institute. (2023). Vasculitis. Retrieved from https://www.nhlbi.nih.gov/health/vasculitis/symptoms#:~:text=Nerve%20problems%2C%20including%20numbness%2C%20tingling,can%20also%20occur%20with%20vasculitis.
Centers for Disease Control and Prevention. (2024). Stroke signs and symptoms. Retrieved from https://www.cdc.gov/stroke/signs-symptoms/?CDC_AAref_Val=https://www.cdc.gov/stroke/signs_symptoms.htm
National Heart, Lung, and Blood Institute. (2022). What Is a Heart Attack? Retrieved from https://www.nhlbi.nih.gov/health/heart-attack
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Spinal Stenosis Basics. Retrieved from https://www.niams.nih.gov/health-topics/spinal-stenosis/basics/symptoms-causes
Senderovich, H., & Jeyapragasan, G. (2018). Is there a role for combined use of gabapentin and pregabalin in pain control? Too good to be true?. Current medical research and opinion, 34(4), 677–682. https://doi.org/10.1080/03007995.2017.1391756
National Institute of Neurological Disorders and Stroke. (2024). Peripheral Neuropathy. Retrieved from https://www.ninds.nih.gov/health-information/disorders/peripheral-neuropathy
Marshmallows and calories can add up when eating more than a single serving. Can marshmallows be consumed in moderation and still be healthy?
Marshmallows
Many enjoy marshmallows with hot chocolate, sweet potatoes, and s’mores. However, their nutritional value is not the healthiest, as the ingredients typically include water, sugar, corn syrup, gelatin, and sometimes other ingredients for flavor and color. The key ingredient is whipped air, giving marshmallows their signature texture.
Nutrition
A serving weighs about 28 grams, around four large marshmallows or a half-cup of mini marshmallows. If consumed in their original form, they contain about 80 calories. (United States Department of Agriculture, 2018)
Carbohydrates
Marshmallows are made of different types of sugar (sucrose and corn syrup), and most of their calories come from carbohydrates. One marshmallow contains a little under 6 grams of carbohydrates, and a single serving provides about 23 grams of carbohydrates, primarily sugar. The glycemic index is estimated to be 62, making it a high-glycemic food. The estimated glycemic load of one marshmallow is 15, which is low. However, the glycemic load takes serving size into account. Because the serving size is small, the glycemic load is lower than expected.
Fats
Very little fat, less than 1 gram, is in a single serving.
Protein
Marshmallows are not a recommended source of protein.
There is less than 1 gram of protein in a single serving.
Micronutrients
There is no significant vitamin or mineral intake by consuming marshmallows.
A single serving does contain a small amount of phosphorus, around 2.2 milligrams, and potassium, around 1.4 milligrams.
It also increases sodium intake by 22.4 mg, providing little selenium 0.5 micrograms.
Health Benefits
Marshmallows are processed and provide little to no health benefits, but there are ways to include them in a balanced, healthy diet. They are a low-calorie, nearly fat-free food, so for those watching their weight, eating a marshmallow is a quick and easy way to satisfy a sweet tooth. Also, adding marshmallows to certain foods might help increase the intake of healthy vegetables, such as adding marshmallows to sweet potatoes, which are almost always gluten-free. For gluten-intolerant individuals, marshmallows are probably safe to consume. Some brands have also developed vegan marshmallows that use tapioca starch or agar instead of gelatin.
Storage
Marshmallows have a long shelf life. A bag can last up to six or eight months if not opened. They can last four months or less if the bag is open. Some can be purchased in an airtight tin and stored that way. However, they are most often in a plastic bag. Therefore, they should be placed in an airtight plastic container or sealed tightly after opening. Marshmallows do not need refrigeration, but many cooks freeze them to make them last longer. An unopened bag can be frozen, forming cubes that may stick together. To prevent sticking, dust with powdered sugar and place in an airtight container. When they are thawed, they regain their fluffy texture.
Allergies
Allergies are rare. However, those allergic to gelatin may want to avoid marshmallows since gelatin is a primary ingredient in almost all prepared and homemade versions.(Caglayan-Sozmen S. et al., 2019)
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic providers use an integrated approach to create customized plans for each patient and restore health and function to the body through nutrition and wellness, chiropractic adjustments, functional medicine, acupuncture, Electroacupuncture, and sports medicine protocols. If other treatment is needed, patients will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Balancing Body and Metabolism
References
United States Department of Agriculture. FoodData Central. (2018). Candies, marshmallows. Retrieved from https://fdc.nal.usda.gov/fdc-app.html#/food-details/167995/nutrients
Caglayan-Sozmen, S., Santoro, A., Cipriani, F., Mastrorilli, C., Ricci, G., & Caffarelli, C. (2019). Hazardous Medications in Children with Egg, Red Meat, Gelatin, Fish, and Cow’s Milk Allergy. Medicina (Kaunas, Lithuania), 55(8), 501. https://doi.org/10.3390/medicina55080501
Can knowing the characteristics of each stage of healing help expedite recovery for individuals who are healing after neck and back injuries?
Back or Neck Injury Healing Stages
At each stage, different things happen at the injury site. This means recommended exercises and activity levels will vary depending on how long it’s been since the injury. The stages to know about when healing from a neck or back injury. (Brumitt J., and Cuddeford T. 2015)
Inflammation or Acute Stage
Also known as the inflammatory stage, the acute stage occurs during the injury and can continue for 72 hours. The body releases repair chemicals in response to tissue damage, causing inflammation and pain. Symptoms of inflammation, including redness, swelling, pain at rest, and diminished function, are expected. Inflammation and pain during the inflammation stage are caused by the body’s repair chemicals released in response to tissue damage. (Wu, Y. S. and Chen S. N. 2014) The biological reaction decreases mobility so the injured area can rest and heal, but the substances that promote healing also cause pain and swelling. (Shah A. and Amini-Nik S. 2017) Scar tissue also begins to form during the inflammatory stage. (Wilgus T. A. 2020) Initial treatment focuses on reducing pain, swelling, and muscle spasms. Individuals are encouraged to use ice packs, compression, and over-the-counter anti-inflammatory medications like ibuprofen or naproxen. (Duchesne E., Dufresne S. S., and Dumont N. A. 2017)
Subacute Stage
Inflammation decreases, and new connective tissue and capillaries grow to help repair damaged structures. The subacute phase generates new connective tissue and capillary growth and reduced inflammation. (Brumitt J., and Cuddeford T. 2015) Scar tissue continues to grow during this time, as well. The tissues are still fragile at this stage, stressing the injured area should be limited to when the therapist or doctor is examining or working with the patient. Most physical therapists recommend beginning with gentle movement during the subacute phase and gradually building up the intensity of exercise. Mild isometric and low-intensity exercises are often used. Because activity is restricted, the muscles may seem weak. Depending on the severity of the injury and the type of tissue that was injured (i.e., tendons have less blood circulation and tend to heal more slowly, it can take a few days to several weeks. (Brumitt J., and Cuddeford T. 2015)
The Chronic Stage or Maturation
The inflammation disappears entirely during the chronic or maturation stage of neck or back injury healing. The new collagen fibers build strength, and the wound shrinks. (Brumitt J., and Cuddeford T. 2015) During this stage, pain associated with the injury tends to be limited to the end joint’s range of motion. The first ten weeks of the chronic stage are essential for engaging in exercises that enhance healing and help remodel the fibers so they will function as close as possible to the way they did before the injury. (Azevedo P. S. et al., 2016) Exercises during the ten weeks are important because otherwise, individuals can permanently lose some of their ability to move and function.
After around ten weeks, the scar tissue can permanently change, so re-acquiring strength and flexibility may necessitate surgery or manual release treatment from a physical therapist or chiropractor. During this time, the scar tissue can be remodeled with exercise, meaning that the activities and motions performed on the injured area will affect the formation of new tissue fibers. The chronic stage of healing begins after 21 days and doesn’t end after the 10-week prime time (Brumitt J., and Cuddeford T. 2015). It can continue for quite some time.
Treatment
Treatment focuses on engaging the injured muscles in light isometric contractions to help align new collagen fibers. Physical therapy helps rebuild mobility, strength, balance, and flexibility and can also help learn about injury and how to recover. A treatment that may also help during these phases is massage therapy. Extended bed rest or immobility can prolong symptoms and delay recovery. Tips to manage pain and recovery:
When sitting for long periods, get up and move around frequently.
Wear comfortable shoes.
When driving long distances, stop frequently to stand up and walk around.
Sleep on the side with a small pillow between the knees.
Limit how much weight is carried.
Add exercises gradually.
Most symptoms of back strain or sprain improve in about two weeks. Individuals may need additional treatment if symptoms continue for longer than two weeks. Maintaining exercises will continue to make the body stronger, more flexible, more functional, and pain-free.
Chiropractic Care for Healing After Trauma
References
Brumitt, J., & Cuddeford, T. (2015). CURRENT CONCEPTS OF MUSCLE AND TENDON ADAPTATION TO STRENGTH AND CONDITIONING. International journal of sports physical therapy, 10(6), 748–759.
Wu, Y. S., & Chen, S. N. (2014). Apoptotic cell: linkage of inflammation and wound healing. Frontiers in pharmacology, 5, 1. https://doi.org/10.3389/fphar.2014.00001
Shah, A., & Amini-Nik, S. (2017). The Role of Phytochemicals in the Inflammatory Phase of Wound Healing. International journal of molecular sciences, 18(5), 1068. https://doi.org/10.3390/ijms18051068
Wilgus T. A. (2020). Inflammation as an orchestrator of cutaneous scar formation: a review of the literature. Plastic and aesthetic research, 7, 54. https://doi.org/10.20517/2347-9264.2020.150
Duchesne, E., Dufresne, S. S., & Dumont, N. A. (2017). Impact of Inflammation and Anti-inflammatory Modalities on Skeletal Muscle Healing: From Fundamental Research to the Clinic. Physical therapy, 97(8), 807–817. https://doi.org/10.1093/ptj/pzx056
Azevedo, P. S., Polegato, B. F., Minicucci, M. F., Paiva, S. A., & Zornoff, L. A. (2016). Cardiac Remodeling: Concepts, Clinical Impact, Pathophysiological Mechanisms and Pharmacologic Treatment. Arquivos brasileiros de cardiologia, 106(1), 62–69. https://doi.org/10.5935/abc.20160005
Individuals getting into fitness may wonder whether they should join a gym or exercise at home. Is there an advantage to one versus the other?
Gym or Home
Exercising, whether at the gym or at home, depends on individual preference and budget. The first step is committing to a fitness health plan. Where to work out depends on the individual and their characteristics. For those who are self-motivated and will exercise no matter what, a home workout may be the best option. (Essery R. et al., 2017) Going to a gym may be a better choice for those who find too many distractions at home and other things to do besides the workout, like laundry, checking the phone, cleaning, etc. Working out at home is convenient; it takes driving out of the equation, changing into gym clothes, and going at the right time. However, the gym provides fewer distractions, community access, equipment like weights and cardiovascular machines, and group fitness classes. Each has pros and cons.
Pros and Cons – The Gym
Pros
Gym features and resources
Motivation
Focus
Classes
Community
Cons
Membership fees
Inconvenience
Too many people
Pros of a Gym
Features and Resources
Exercise can be so much easier when there are plenty of options.
There are various machines, such as treadmills, ellipticals, stair climbers, stationary bikes, and rowing machines.
Weights and machines, free weights, cable machines, bands, and more.
Motivation
Paying for a membership can be a motivating factor to regularly working out.
There is a friendly, competitive vibe with the other members who can help motivate each other.
Focus
Exercising at the gym can help maintain focus on fitness goals.
No chores, kids, or distractions to break off from the workouts.
Classes
Working out in a class can increase motivation and make working out fun.
There are online classes for working out at home, but it’s not the same as going to the gym and being around people.
Other features like a swimming pool, hot tub, tennis courts, etc may be available.
Community
Working out with others can give a sense of community.
People draw energy from others, pushing us to work harder.
Cons of a Gym
Gym membership drawbacks.
Cost
Membership fees can cause stress.
Some high-end gyms charge more than $100 monthly, while smaller gyms may charge only $10.
Inconvenience
Going to the gym includes packing a bag, driving there, parking, and waiting for the machines, weights, etc.
Total time will be longer because of the drive time.
Too Many People
At times, the gym can be packed with people.
Sometimes, individuals talk too loudly on their phones, leave sweat on the machines, and do not put weights away.
These could be the days or nights to work out at the house.
At Home Workouts
Pros
Cost
Convenience
Mix workouts
Cons
Space
Excuses
Boredom
Pros at Home
For some, home workouts could be the better option, and the benefits include:
Cost
There’s no membership fee.
Individuals can do bodyweight workouts that require no equipment.
Develop a house gym with inexpensive resistance bands, a few weights, and an exercise ball.
Convenience
Individuals do not have to get their gym bag, drive, and arrange for child care.
Individuals can work out in pajamas or underwear.
Individuals can also work out whenever they like if they need to split their workouts or work out at a specific time.
Mix Workouts
Although gyms also mix things up, individuals can do it at home at their convenience.
Combining weights and cardio and finishing up with yoga.
Individuals can go outside, watch exercise videos, stream live classes, use fitness mirrors, play exercise games, or download workout apps.
There is also versatile home gym equipment.
Cons at Home
These can cause individuals to lose home workout motivation.
Space
Although not much space is needed to work out, wanting to use a treadmill or other large equipment might not be practical, which could lead to boredom.
Excuses
There can be endless excuses to skip a workout.
Individuals who are not self-motivated might avoid workouts with chores or other important home tasks.
Boredom
At a gym, there is energy potential that motivates individuals to move.
If there is not enough exercise variety at home, boredom can set in.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic treats patients’ injuries and chronic pain syndromes. We focus on improving ability through flexibility, mobility, and agility programs tailored to the individual. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes. Our providers use an integrated approach to create customized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body. Suppose he feels the individual needs other treatment. In that case, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide our community with the best clinical treatments.
The Right Way To Implement an Exercise Prescription
References
Essery, R., Geraghty, A. W., Kirby, S., & Yardley, L. (2017). Predictors of adherence to home-based physical therapies: a systematic review. Disability and rehabilitation, 39(6), 519–534. https://doi.org/10.3109/09638288.2016.1153160
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine