For individuals with cervical arthritis, can physical therapies help manage symptoms and bring pain relief?
Cervical Arthritis
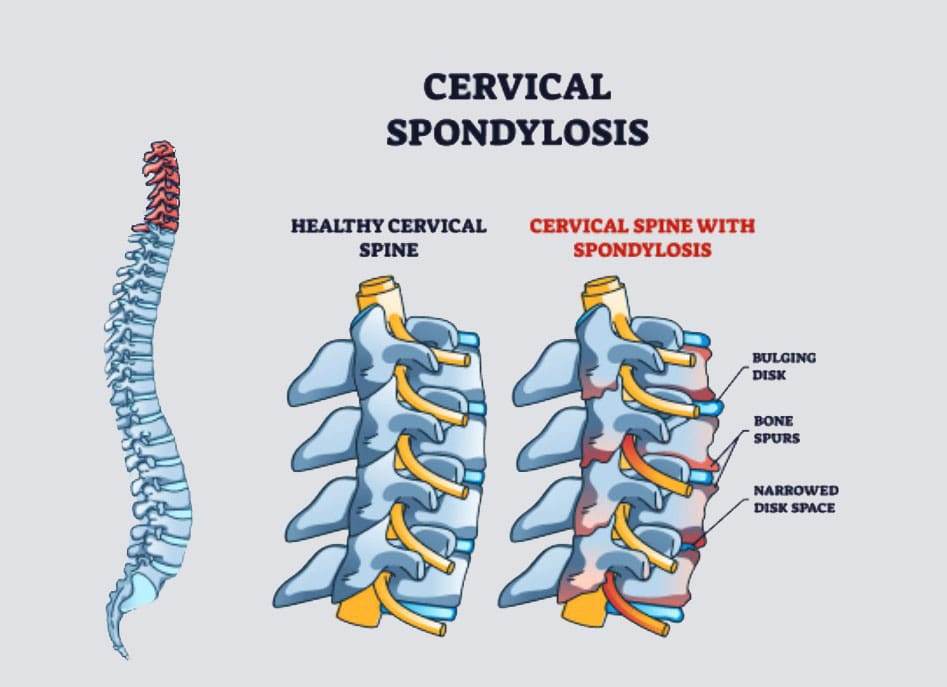
Cervical spondylosis, more commonly known as cervical arthritis or arthritis of the neck, refers to the wearing down of neck bones, discs, tendons, ligaments, and joints. The primary symptoms are neck pain and stiffness. However, it is also possible to have cervical spondylosis and not have any symptoms. The condition affects over 85% of individuals over age 65. (American Academy of Orthopaedic Surgeons, 2021) Treatment can consist of conservative therapies and includes physical therapies, alternative medicine therapies, at-home self care, and over-the-counter and prescription medications. Severe cases of cervical spondylosis are treated with surgery to repair damaged parts of the spine.
Symptoms
Neck pain and headaches at the back of the head are usually the first symptoms. (Kazeminasab S. et al., 2022) The neck can also feel stiff, with worse morning symptoms that improve throughout the day. (Johns Hopkins Medicine, 2024) Symptoms can range from mild discomfort to severe pain. As cervical spondylosis progresses, individuals can experience:
Inability to turn the head or bend the neck.
A clicking or grinding noise when turning the neck.
Tenderness with pressure on the neck.
Pain that radiates to the shoulders or shoulder blades.
Pain and symptoms that disrupt sleep, sometimes causing waking up throughout the night.
Symptoms that decrease with rest.
More severe symptoms include:
Cervical Bone Spurs – Osteophytes
Some with cervical spondylosis have bony growths that can place pressure on the spinal nerves (a pinched nerve) (Bon Secours, 2024). Compression of spinal nerve roots produces cervical radiculopathy, which leads to pain, tingling, and weakness that radiates into the shoulders, arms, and hands.
Cervical Myelopathy
This refers to spinal impingement that leads to spinal cord dysfunction. (Spinal cord dysfunction is a nervous system disorder with interruptions in the spinal cord’s motor, sensory, and autonomic functions.) Symptoms include pain, tingling, numbness, muscle spasms, and weakness in areas below the neck. Spinal cord dysfunction can affect mobility, hand use, and bladder or bowel function control.
Causes
Where degenerative changes are commonly associated with cervical spondylosis, other conditions, and factors can lead to it and include:
Autoimmune Diseases
Rheumatoid arthritis and psoriatic arthritis can cause chronic inflammation in the cervical spine.
Trauma
Neck trauma, including injury and repetitive stress on the neck.
Cervical spondylosis is commonly seen in occupations that involve neck-stressing activities, such as sports.
Age
Wearing down of the spinal discs cartilage between the vertebrae.
Genetic components have been identified in connection with cervical spondylosis, meaning that some types of arthritis that lead to spinal damage are hereditary. (Kazeminasab S. et al., 2022)
Treatment
Treatment begins conservatively, using protocols to preserve function and avoid surgery. Nonsurgical treatments include medications, physical therapy, at-home exercises, and alternative medicine. The treatment method a healthcare provider chooses will depend on how severe the spondylosis is and other factors like age, how much pain is being experienced, the cause, and overall health. The main objectives are to relieve pain, prevent long-term damage to the spinal cord and nerves, and help maintain performing daily activities. (Bon Secours, 2024)
Medications
Medicines used to treat cervical spondylosis include:
Nonsteroidal Anti-inflammatory Drugs NSAIDs
NSAIDs, including ibuprofen and naproxen sodium, are available without a prescription to relieve pain and inflammation.
A healthcare provider can prescribe a more powerful NSAID to help manage severe symptoms.
Corticosteroids
A corticosteroid injection or a short course of an oral corticosteroid, like prednisone, can ease pain and reduce inflammation.
Muscle Relaxants
If cervical spondylosis causes muscle spasms, a healthcare provider can prescribe cyclobenzaprine, a muscle relaxant, to manage symptoms.
Antidepressants
Some types of antidepressants can ease neck pain from cervical spondylosis.
Anti-seizure Meds
Some anti-seizure drugs can cause nerve pain resulting from damaged nerves.
Physical Therapies
Physical therapy will help manage pain and stiffness and keep muscles loose and relaxed.
A physical therapist will teach the patient exercises to stretch and strengthen neck and shoulder muscles.
At-Home Self Care
At-home exercises can help relieve pain, stiffness, and swelling. Some can include:
Reducing inflammation and stress on the neck through posture training.
At-home targeted stretches and exercises will help bring pain relief.
Ice treatment reduces swelling.
Heat will increase circulation.
A neck brace may be recommended briefly to avoid muscle weakness and stiffness.
Alternative Medicine
Chiropractic adjustments and massage therapy are alternative treatments that will help manage cervical spondylosis.
Acupuncture can also be beneficial in reducing neck pain and increasing energy circulation. (Gu C. L. et al., 2019)
Various therapeutic massage therapies will help relieve neck pain and stiffness. Talk to a healthcare provider before starting treatment so they can advise on whether neck massages are safe.
Surgery
A healthcare provider may recommend surgical treatment when all other treatments have failed, if neurological symptoms are severe, or if neck arthritis causes extreme pain or disability. Surgery to treat cervical spondylosis can involve removing bone spurs, part of the cervical vertebra, or a herniated disc. The removed portions of the cervical spine are fused with hardware and bone grafts.
Injury Medical Chiropractic and Functional Medicine Clinic
Chiropractic therapy is among the more conservative treatment options and may be tried first before proceeding with surgery. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution.
Arthritis Explained
References
American Academy of Orthopaedic Surgeons. (2021). Cervical spondylosis (arthritis of the neck). https://orthoinfo.aaos.org/en/diseases–conditions/cervical-spondylosis-arthritis-of-the-neck/
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC musculoskeletal disorders, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Johns Hopkins Medicine. (2024). Spinal arthritis (arthritis in the back or neck). https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-arthritis
Bon Secours. (2024). Cervical osteoarthritis (arthritis in the neck). https://www.bonsecours.com/health-care-services/spine-care/conditions/cervical-osteoarthritis
American Chiropractic Association. (2024). Neck pain. https://www.acatoday.org/patients/neck-pain-and-chiropractic/
Jenkins, H. J., Downie, A. S., Moore, C. S., & French, S. D. (2018). Current evidence for spinal X-ray use in the chiropractic profession: a narrative review. Chiropractic & manual therapies, 26, 48. https://doi.org/10.1186/s12998-018-0217-8
Gu, C. L., Yan, Y., Zhang, D., & Li, P. (2019). An evaluation of the effectiveness of acupuncture with seven acupoint-penetrating needles on cervical spondylosis. Journal of pain research, 12, 1441–1445. https://doi.org/10.2147/JPR.S199798
Can individuals support their parasympathetic nervous system to maintain a relaxed state and avoid excessive agitation, stress, anxiety, and dysregulation?
Parasympathetic Nervous System
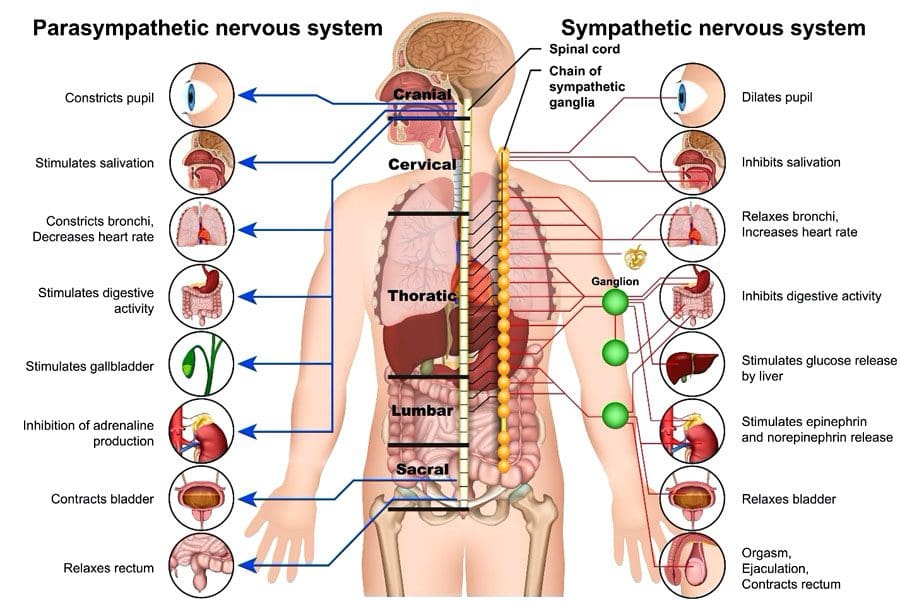
The parasympathetic nervous system (PSNS) involves organs and cells that release neurotransmitters that help the body maintain essential functions like heart rate, breathing, digestion, relaxation, thinking, and sleep. It is part of the autonomic nervous system, which includes the nerves and neurotransmitters that control the body’s internal organs to maintain reliable function. The autonomic nervous system regulates a continual balance between the parasympathetic nervous system’s rest-and-digest functions and the sympathetic nervous system’s fight-or-flight responses.
Functions and Responses
The parasympathetic nervous system includes nerves and neurotransmitters (chemical messengers) distributed throughout the body and is often described as promoting the body’s rest-and-digest state. The body’s needs regulate the control and effects of the system. Certain medications and health issues can modify or alter the function of the autonomic nervous system, including sympathetic and parasympathetic areas. The parasympathetic and sympathetic nervous systems collaborate to control cells, tissues, and organs. The body requires constant functioning and adjustment of both systems. (McQuade J. D. et al., 2017) Functions include: (Valenti V. E. et al., 2024)
Saliva secretion to break down food.
Maintaining blood pressure, resting heart, and breathing rate.
Producing enzymes in the stomach and intestines to break down food further and absorb nutrients.
Kidney balancing of fluid and mineral levels by producing urine.
Constricting pupils (making the dark circle in the eye smaller) to see details up close.
Maintaining focus and concentration to think, remember, and make decisions.
Releasing hormones to fall asleep and stay asleep.
Providing consistent muscle stimulation to maintain endurance for muscle activity.
All functions are adjusted based on the body’s needs.
Activation
The parasympathetic response constantly works to keep the body active, engaged, and healthy and can be stimulated simply by relaxing and resting. Individuals can sometimes focus on promoting their body’s parasympathetic activity through stretching, slow movements, relaxing sounds or music, meditation, and similar activities. Individuals who frequently feel anxious or stressed and have difficulty relaxing could benefit from guidance from a therapist or coach on learning to engage the parasympathetic nervous system. (Goren O. et al., 2024) This can involve activities such as guided meditation or talk therapy, which can help individuals work through fears and anxieties.
Dysregulation
Some medical conditions are associated with dysregulation. Heart disease, respiratory disease, sleep disorders, mental health conditions, and behavioral conditions can be associated with overactive or underactive parasympathetic or sympathetic nervous system regulation. (Veerakumar A. et al., 2022) Various mental health and physical health disorders can involve symptom fluctuations that affect the autonomic nervous system. For example, anxiety disorders can cause periods of overeating as well as loss of appetite and episodic indigestion, nausea, and vomiting. Symptoms of dysregulation can include: (McQuade J. D. et al., 2017)
Excessive sleepiness
Insomnia
Difficulty concentrating
Confusion
Anxiety – nervousness or agitation
A feeling of a rapid heart rate
Shortness of breath
Dry mouth
Throat tightness
Indigestion
Stomachaches
Nausea
Vomiting
Cold hands and feet
Sweating or clammy hands
Sadness
Depression
Dizziness or feeling physically off-balance
Any of these symptoms can develop and resolve quickly. Most individuals experience symptoms or parasympathetic nervous system dysfunction when an unexpected stressful event occurs, and the response is considered normal in traumatic, shocking, sad, or high-stress circumstances. (Veerakumar A. et al., 2022)
Medications may induce parasympathetic overactivity or underactivity until the medicine is broken down and removed from the body. (Valenti V. E. et al., 2024)
Nerves
The system comprises nerves that release hormones and neurotransmitters and nerves that respond to the hormones and neurotransmitters. Parasympathetic activation and response include: (Valenti V. E. et al., 2024)
The nerves that activate the parasympathetic nervous system run throughout the body, primarily in the brain, heart, lungs, stomach, and intestines.
The brain, heart, lungs, stomach, intestines, muscles, liver, kidneys, reproductive organs, eyes, and mouth are among the areas of the body that respond to stimulation.
The vagus nerve, one of the cranial nerves, is closely associated with parasympathetic nervous system activity. It runs from the brainstem down into the throat, heart, lungs, and digestive system. (Valenti V. E. et al., 2024) Surgical, medical, and alternative interventions are used to regulate the activity of the parasympathetic nervous system and are targeted toward regulating and controlling the activity of the vagus nerve. (Hernández-Domínguez R. A. et al., 2024)
PSNS Support
Living with any parasympathetic nervous system dysfunction can be challenging. For individuals with heart or lung disease, healthcare providers will evaluate the medical condition and recommend surgery or medication to control symptoms and avoid complications. (Hernández-Domínguez R. A. et al., 2024) Individuals who are living with a mental health disorder or behavioral disorder that is associated with any dysregulation of the parasympathetic nervous system activity may benefit from a combination of behavioral interventions and medication to help control symptoms long term. (Goren O. et al., 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
The spinal cord has multiple functions in restoring, rejuvenating, and strengthening the nervous system. Chiropractic care has a highly responsive therapeutic effect on the nervous system because of its focus on the spine. Spinal decompression, traction, soft tissue manipulation, and other treatments help regulate and restore the function of the nervous system. Chiropractic benefits:
Reduce and/or eliminate pain.
Improves the quality of sleep.
Increases energy.
Improves cognition and clarity.
Reduces or eliminates headaches and migraines.
Improves digestive function.
Improves balance and coordination.
Increases flexibility and mobility.
Regulates respiration.
Regulates lower heart rate.
At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for every patient to restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, or ailment.
Chiropractic Secrets Exposed
References
McQuade, J. D., Penzel, T. E., Silk, J. S., & Lee, K. H. (2017). Parasympathetic Nervous System Reactivity Moderates Associations Between Children’s Executive Functioning and Social and Academic Competence. Journal of abnormal child psychology, 45(7), 1355–1367. https://doi.org/10.1007/s10802-016-0246-5
Valenti, V. E., Vanderlei, L. C. M., & Godoy, M. F. (2024). Editorial: Understanding the role of the autonomic nervous system in health and disease. Frontiers in neuroscience, 18, 1446832. https://doi.org/10.3389/fnins.2024.1446832
Goren, O., Paz, A., Bar-Kalifa, E., Gilboa-Schectman, E., Wolff, M., & Atzil-Slonim, D. (2024). Clients’ and therapists’ parasympathetic interpersonal and intrapersonal regulation dynamics during psychotherapy for depression. Psychotherapy research : journal of the Society for Psychotherapy Research, 1–15. Advance online publication. https://doi.org/10.1080/10503307.2024.2378038
Veerakumar, A., Yung, A. R., Liu, Y., & Krasnow, M. A. (2022). Molecularly defined circuits for cardiovascular and cardiopulmonary control. Nature, 606(7915), 739–746. https://doi.org/10.1038/s41586-022-04760-8
Hernández-Domínguez, R. A., Herrera-Orozco, J. F., Salazar-Calderón, G. E., Chávez-Canales, M., Márquez, M. F., González-Álvarez, F., Totomoch-Serra, A., Reyes-Cruz, T., Lip, F., & Aceves-Buendía, J. J. (2024). Optogenetic modulation of cardiac autonomic nervous system. Autonomic neuroscience : basic & clinical, 255, 103199. https://doi.org/10.1016/j.autneu.2024.103199
Can incorporating an ab roller help individuals achieve their fitness goal of building stronger core muscles?
Ab Roller
An ab roller is exercise equipment that helps build core strength and stability by engaging the core, including the abs, obliques, and lower back. It’s a small, robust wheel with handles on each side that glides along surfaces. An ab roller makes an excellent addition to any workout routine and benefits those who do not have an established workout routine. Strengthening the core muscles will help in other areas, whether achieving further exercise goals or reducing injuries. It works by holding on to the handles and rolling the entire body forward over the wheel, improving abdominal strength and endurance while activating the shoulders, arms, and upper back muscles. These movements target different areas, including the obliques, rectus abdominis, and serrated anterior muscles.
Benefits
Enhanced Core Muscle Strength
The primary benefit of using an ab roller is improved core strength, which can help build a solid foundation for various other exercises and physical activities that might be done daily. The body uses its core when moving other muscle groups. Strengthening core muscles increases sports performance, speed, and consistency.
Decrease Injury Risks
Building a strong abdominal core will help stabilize other body areas, such as hip flexors and hamstrings, ultimately reducing the likelihood of injuries. (Huxel Bliven, K. C. and Anderson B. E. 2013) This improved strength and stability is especially beneficial as a strong core can help reduce the chance of an exercise, sports, or work-related injury.
Posture Improvement
Most of us know posture is important but may not realize it (Wilkes C. et al., 2017). A healthy posture can help reduce back pain and even boost energy levels. Performing regular abdominal workouts using an ab roller helps to reinforce proper posture. Healthy posture is more than just standing up straight—it involves incorporating core abdominal activity to help strengthen the muscle endurance of the hips and trunk regions, enabling individuals to stand up straight without much effort.
Tips and Advice
It is important to introduce an ab roller gradually into a workout regimen. Here are a few tips for incorporating one.
Duration
As a beginner, start by trying to do one to two sets with six to 10 repetitions. Individuals may notice that their muscles are sore after doing this for the first time. If the soreness is too much, cut back for the next workout and ease into it more gradually. After a few weeks, the body will start getting used to the movement and may be ready to level up to two to four sets. Speed and performing the exercise as fast as possible is not the goal. Individuals should focus on slow but steady motions, core stability, and proper form. Rushing through a workout could increase the chance of an injury.
Frequency
When starting an ab roller workout, the recommendation is to do it once or twice a week, ideally combined with other workouts like walking, running, swimming, or cycling. This will allow the body to get used to the motion. Because this exercise is difficult and requires balance, some may need to adjust to the training, which is perfectly normal.
Intensity
How intense individuals go with the ab roller depends on current activity and fitness level. It takes time to adapt to this particular exercise. For a beginner, start at a mild intensity by kneeling on the ground. As the core gets used to the motion, individuals can progress to putting their legs straight and omit kneeling. This advanced motion will incorporate posture, strength, endurance, and proprioception.
Injury Medical Chiropractic and Functional Medicine Clinic
Ask a qualified fitness coach or personal trainer if you are unsure where to begin. As with any exercise or fitness program, always talk with your healthcare provider. At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other associated medical professionals to integrate into a treatment plan to improve the body’s flexibility and mobility and resolve musculoskeletal issues.
Core Exercises and Back Pain
References
Huxel Bliven, K. C., & Anderson, B. E. (2013). Core stability training for injury prevention. Sports health, 5(6), 514–522. https://doi.org/10.1177/1941738113481200
Wilkes, C., Kydd, R., Sagar, M., & Broadbent, E. (2017). Upright posture improves affect and fatigue in people with depressive symptoms. Journal of behavior therapy and experimental psychiatry, 54, 143–149. https://doi.org/10.1016/j.jbtep.2016.07.015
Can incorporating selenium-rich foods into one’s diet improve overall health?
Selenium
Selenium is a chemical element and a micronutrient with antioxidant properties that protect cells from damage and increase immune function (University of Florida Health, 2023). It has also been linked to heart health and longevity. Most individuals in the U.S. can acquire a healthy amount of selenium through a balanced diet. Research has shown that selenium supports healthy aging and reduces the risk of heart disease. (Alehagen U. et al., 2021) (Zhang Y. et al., 2024) A recent study found a region in China where residents have sustained longevity with soil that is rich with selenium. (Li B. et al., 2024) The body does not produce the chemical, so it must be obtained through food or supplements. (National Institutes of Health Office of Dietary Supplements, 2024) However, excessive amounts can build up in the body and be toxic, causing gastrointestinal problems, hair loss, kidney failure, neurological issues, and death. (National Institutes of Health Office of Dietary Supplements, 2024)
Only A Small Amount Is Needed
The body only needs small amounts of selenium to support bodily functions, including thyroid hormone metabolism and antioxidant defense. Most adults need 55 micrograms daily, and pregnant and lactating adults require an additional 5–15 micrograms daily (National Institutes of Health Office of Dietary Supplements, 2024). Individuals can get selenium from many food sources, including Brazilian nuts, meat, seafood, vegetables, and grains. A large hard-boiled egg comprises 15 micrograms, a cup of cooked spaghetti provides 33 micrograms, and 3 ounces of cooked shrimp offer 42 micrograms of selenium. (National Institutes of Health Office of Dietary Supplements, 2024)
Individuals who eat healthy and eat various foods will meet their selenium needs. However, in some parts of the world, poor selenium soil may not provide enough of this mineral for individuals through their diet. (National Institutes of Health Office of Dietary Supplements, 2024) Low selenium intake is linked to a heart condition called Keshan disease, which may weaken the heart’s ability to pump blood. (National Library of Medicine, 2023) However, individuals are recommended not to take more than 400 micrograms daily.
Longevity
Various researchers are trying to understand the link between selenium and aging. A study associated dietary intake with increased telomere length (protein structures at the ends of chromosomes that protect DNA and help control cell division), a biological marker that may indicate aging and other health conditions. (Liang C. et al., 2024) Shorter telomeres generally indicate aging and disease progression. Another study suggests moderate amounts of dietary selenium may protect against cardiovascular disease and death. However, the observational study included data from over 25,000 adults but did not prove a cause-and-effect relationship between selenium and improved longevity. (Zhang Y. et al., 2024) Further research is needed before experts recommend selenium as an anti-aging dietary component.
Injury Medical Chiropractic and Functional Medicine Clinic
Selenium helps with cell growth and thyroid function and is known to increase immune system function. However, avoiding excessive intake is important, as high levels can be harmful. Injury Medical Chiropractic and Functional Medicine Clinic providers use an integrated approach to create customized care plans for each patient and restore health and function to the body through nutrition and wellness, chiropractic adjustments, functional medicine, acupuncture, Electroacupuncture, and various medicine protocols. If the individual needs other treatment, they will be referred to a clinic or physician, as Dr. Jimenez has teamed with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Smart Choices Better Health
References
University of Florida Health. (2023). Selenium in diet. https://ufhealth.org/conditions-and-treatments/selenium-in-diet
Alehagen, U., Opstad, T. B., Alexander, J., Larsson, A., & Aaseth, J. (2021). Impact of Selenium on Biomarkers and Clinical Aspects Related to Ageing. A Review. Biomolecules, 11(10), 1478. https://doi.org/10.3390/biom11101478
Zhang, Y., Meng, S., Yu, Y., Bi, L., Tian, J., & Zhang, L. (2024). Associations of dietary selenium intake with the risk of chronic diseases and mortality in US adults. Frontiers in nutrition, 11, 1363299. https://doi.org/10.3389/fnut.2024.1363299
Li, B., Liu, X., Yu, T., Lin, K., Ma, X., Li, C., Yang, Z., Tang, Q., Zheng, G., Qin, J., & Wang, Y. (2024). Environmental selenium and human longevity: An ecogeochemical perspective. Chemosphere, 347, 140691. https://doi.org/10.1016/j.chemosphere.2023.140691
National Institutes of Health Office of Dietary Supplements. (2024). Selenium: fact sheet for health professionals. Retrieved from https://ods.od.nih.gov/factsheets/Selenium-HealthProfessional/
National Library of Medicine: MedlinePlus. (2023). Selenium in diet. Retrieved from https://medlineplus.gov/ency/article/002414.htm
Liang, C., Zhao, R., Du, J., Zhao, G., & Zhang, Y. (2024). The association between dietary selenium intake and telomere length in hypertension. Journal of clinical hypertension (Greenwich, Conn.), 26(8), 990–996. https://doi.org/10.1111/jch.14861
For athletes and individuals who want to engage in physical and sports activities, can focusing on health-related fitness components improve overall fitness and conditioning so that they can participate in various sports and other forms of exercise?
Fitness Components For Improved Physical and Sports Performance
Improving cardiovascular fitness, muscular strength and endurance, and flexibility will enhance athletes’ abilities and the daily lives of individuals who exercise and play sports. When enhancing performance in a specific activity, skill-related fitness training that focuses on that activity will be most beneficial. For instance, cardiovascular endurance and flexibility are necessary to play sports that require a lot of running, jumping, and changing positions quickly and to be able to play for the entire time, along with various skills that need to be practiced for agility, power, speed, and hand-eye coordination. Activity-related skills can differentiate two areas of fitness.
Getting In Shape and Improving Performance
Health-related fitness components are important for everyone in all walks of life, regardless of competition in or performing physical activities at an optimum level. These are:
Cardiovascular endurance
Flexibility
Muscle endurance
Muscle strength
Body composition
When improving cardiovascular endurance, the risk of heart disease is reduced. When improving flexibility, a healthy range of motion is maintained, enhancing the ability to perform activities of daily living, like household chores and tasks. These fitness components are crucial for physical health and contribute to positive lifestyle outcomes. (Garber C. E. et al., and American College of Sports Medicine 2011) The American College of Sports Medicine recommends:
Moderate-intensity Cardio
30 minutes a day, five days a week for a total of 150 minutes/week or
Vigorous-intensity Cardio
For 20 minutes a day, three days a week, or
A Combination
Moderate- and vigorous-intensity exercise, plus
Resistance Training
Two to three days a week, along with
Flexibility Training
Two days a week
Skill Related Components
Skill-related fitness components are:
Agility
Balance
Coordination – hand-eye and/or foot-eye
Power
Reaction time
Speed
The skill-related fitness components can help those who want more training for a specific fitness-related goal.(Zemková E. and Hamar D. 2018) For example, while everyone can benefit from daily walks, weightlifters can focus most of their effort on power, balance, and strength.
Power
Power combines speed and strength, which is how fast maximal force can be generated. Athletes exert maximum strength in short, all-out efforts. Jumping requires leg power, while jumping and striking involve a combination of upper- and lower-body power. Power can be improved by combining resistance and speed with fast-paced strength-training exercises that include:
Kettlebell swings
Clean lifts
Jerk lifts
Plyometric box jumps
Pushing a weighted sled
Sprinting
Speed
Athletes train differently but with a similar goal: to become faster in their sport. Speed training will differ based on the sport being trained for. High-intensity interval training, or HIIT, is one of the best ways to improve speed. Training involves working at an all-out or near all-out effort for set periods, followed by set rest periods. (Alansare A. et al., 2018) It repeatedly challenges the aerobic and anaerobic systems, teaching the muscles, heart, and lungs to grow accustomed to working at higher intensity levels. Depending on the sport, the length and intensity of the intervals will be longer or shorter, less challenging, or more difficult. Runners can try these example HIIT speed drills:
Marathon Training
Mile repeats – a style of interval training where the runner goes all-out for a full mile before resting and doing it again.
Sprint Training
Focuses on shorter, more intense intervals.
Ranging from 40 to 400 meters, running all out and resting before repeating.
These same concepts apply to other sports as well.
Agility
Agility is the ability to move and change direction quickly and easily. For example, soccer, basketball, football, and tennis players are incredibly agile and have to move in every direction, jumping, sliding, twisting, and backpedaling in quick response to the ball’s movement and other players. Their bodies must be trained to respond and change course. Agility drills commonly involve exercises that develop foot speed and direction change, that include:
Ladder Drills
Using an agility ladder can help develop quick and specific foot placement.
Cone Drills
Set up cones in a T shape, then sprint, slide, backpedal, or change direction depending on the cone.
Coordination
Sports and physical activities require well-honed hand-eye and foot coordination. They require seeing an external object and responding precisely with the hands and/or feet. Think of hitting a ball, running and catching a ball, throwing a frisbee, or blocking a shot. To improve coordination, try skill-related fitness exercises like:
Playing catch
Jumping rope
Dribbling a ball
Throwing or hitting balls or specific sports objects at targets
Balance
Balance refers to the ability to adjust the body position to remain upright. It involves proprioception, or knowing where the body is in space and being able to adjust position as the center of gravity changes during movement. (Aman J. E. et al., 2015) Sports and daily physical activities require balance for performance and safety. Jumping on a trampoline or rebounder, for example, can help individuals better sense where their bodies are as they move. To improve balance, try these exercises:
Practice standing on one foot.
Practice standing yoga poses.
BOSU balance ball workouts.
Use balance discs to perform squats, lunges, and push-ups.
Reaction Time
Reaction time refers to how quickly one responds to an external stimulus and focuses on the mind-body connection. The eyes see a stimulus, the mind interprets the stimulus, and the body reacts to that interpretation. This mind-body reaction relates to knowledge of the sport or activity and enables individuals to respond more quickly and accurately to the stimulus. Reaction-time training tends to be sport-specific, but skill-related fitness activities can help and include:
Using tools like reaction balls
Fielding a ball
Protecting a goal as other players try to score
Playing table tennis
Playing hacky sack
Injury Medical Chiropractic and Functional Medicine Clinic
Ask a qualified fitness coach or personal trainer if you are unsure where to begin. Other athletes, local teams, gyms, athletic clubs, and healthcare organizations can direct individuals in the right direction. At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you to relieve pain, restore function, and prevent injury. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Improving Athletic Performance Through Chiropractic
References
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., Lee, I. M., Nieman, D. C., Swain, D. P., & American College of Sports Medicine (2011). American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Medicine and science in sports and exercise, 43(7), 1334–1359. https://doi.org/10.1249/MSS.0b013e318213fefb
Zemková, E., & Hamar, D. (2018). Sport-Specific Assessment of the Effectiveness of Neuromuscular Training in Young Athletes. Frontiers in physiology, 9, 264. https://doi.org/10.3389/fphys.2018.00264
Alansare, A., Alford, K., Lee, S., Church, T., & Jung, H. C. (2018). The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. International journal of environmental research and public health, 15(7), 1508. https://doi.org/10.3390/ijerph15071508
Aman, J. E., Elangovan, N., Yeh, I. L., & Konczak, J. (2015). The effectiveness of proprioceptive training for improving motor function: a systematic review. Frontiers in human neuroscience, 8, 1075. https://doi.org/10.3389/fnhum.2014.01075
Can incorporating these 7 exercises help individuals dealing with back pain help promote a healthy spine and functionality?
Introduction
Many individuals have dealt with back pain in their body’s upper, middle, and lower portions, which can correlate with other issues in the upper and lower body extremities. This is due to how many environmental factors affect a person’s daily routine. From stressful days that impact a person’s day to physical inactivity or even spinal issues that have developed over time can cause back pain. When individuals decide to make changes in their health and wellness journey to not only reduce back pain but also improve how they present themselves. Many individuals can start with exercises to reduce back pain and help their spinal health by making sure that they are doing it correctly to prevent injuries. Today’s article looks at how spinal issues correlate with back pain and how these seven simple exercises and stretches can help reduce lower back pain and help you have a healthy spine. We talk with certified associated medical providers who provide our patients’ information to assess back pain correlated with their spine. We also inform patients while asking their associated medical provider intricate questions to formulate customized treatment plans to reduce back pain by integrating exercises to help reduce the pain and promote wellness. Dr. Alex Jimenez, D.C., includes this information as an academic service. Disclaimer.
Spinal Issues Correlating To Back Pain
Do you feel stiffness or muscle aches in your back’s upper, middle, or lower areas? Have you noticed that your posture is hunched more than normal when looking at the phone or being on the computer for an extended period? Or does your back ache from lifting a heavy object or sleeping incorrectly? More often than not, these pain-related scenarios are associated with back pain combined with spinal issues. As one of the leading causes of disability, loss of productivity, and more visits to a health clinic, back pain can impact the body and cause individuals to be miserable. (Bang et al., 2021) Back pain can be specific or non-specific and can cause a person’s spine to degenerate through the spinal disc. The spinal disc provides stability, flexibility, and mobility to the spine, which then helps keep the host upright. However, as the body ages, so does the spine, as lower back pain is multifactorial. When the spinal disc degenerates, the spine has a reduced capacity for intrinsic self-repair within the tissues. (Mohd Isa et al., 2022)
At the same time, when many individuals are dealing with low back pain, depending on the severity of the issue, theywill often change their gait mechanics by adapting different strategies to mitigate the loading on the primary muscles associated with the locomotion that protects the pain-producing tissues. (Smith et al., 2022) When that happens, the pain from the lower back muscles can aggravate the spine further and lead to more chronic issues; however, there are ways to reduce the effects of lower back pain and to help keep the spine healthy.
Can Core Exercises Help with Back Pain?-Video
The 7 Exercises To Incorporate For Back Pain
When it comes to making sure that lower back pain can be reduced and to help with keeping a healthy spine, many people often seek out physical therapy to reduce the pain. Since low back pain is costly in a clinical approach, physical therapy is cost-effective, non-invasive, and can help individuals get a kick start in their health journey. Physical therapy involves whole-body movement that emphasizes breathing coordination, reducing pain from the lower back, and helping stabilize the lumbar spine to improve physical function. (Li et al., 2023) By going through a treatment plan that incorporates physical therapy, many individuals will begin to notice their pain is improving and their quality of life is getting better. (Fischer et al., 2021) Additionally, stretching and core stability exercises can activate the deep and superficial spinal muscles by strengthening them and help stretch out sore muscles affected by low back pain to help many individuals recover. (Calatayud et al., 2019) Below are seven exercises that can help reduce back pain and, when done correctly and consecutively, can help many individuals have a healthier spine while being more mindful of their bodies.
Knee-To-Chest Exercise
This knee-to-chest exercise can help stretch the lower back muscles and can be done in the morning or evening.
Lying on your back with knees bent and feet flat for stability.
Pull one knee up with both hands and press it towards your chest.
Keep the stomach muscles tight while pressing your spine to the floor, holding for at least 30 seconds before returning to position.
Repeat with the other knee and do each stretch 2-3 times.
Lower Back Rotational Stretch (On the Floor)
This lower back rotational stretch can help stretch tight muscles in the lower back.
Laying on the mat, ensure you are on your back with knees bent and feet flat.
Make sure the shoulders are firmly on the floor, and slowly roll the knees to one side until 45 degrees.
Hold that position for 30 seconds before slowly rotating the knees back to the starting position.
Repeat on the other side and do each stretch 2-3 times.
Lower Back Flexibility Exercise
This lower back flexibility will help stretch and strengthen the lower back and core muscles.
Lay flat on the mat. For stability, make sure that the knees are bent with feet are flat on the floor.
Tighten the stomach muscles so the lower back can be pulled away from the floor.
Hold the position for 5 seconds and relax, slowly lowering to the floor.
Flatten the back as your belly button starts to go towards the floor, and hold the position for 5 seconds before relaxing.
Do five repetitions a day to slowly work up to 30 reps.
Bridge Exercise
The bridge exercise can help with core stability and help strengthen core muscles.
Laying flat on your back on the floor, with knees bent and feet flat. Make sure that your shoulders and head are relaxed.
Tighten the core and glute muscles while slowly raising from the hips to form a straight line from the knees to the shoulders.
Stay in that position for 30 seconds while taking deep breaths.
Slowly go down to the floor and relax.
Do five repetitions a day to slowly work up to 30 reps.
Cat-To-Cow Stretch
The cat-to-cow stretch helps with shoulders, upper back, and lower back muscles.
On your hands and knees, hip-width apart on the mat, be in a neutral spine position.
Slowly arch your back by pulling your belly towards the ceiling and your head down for 30 seconds.
Then, slowly let the back and belly sag towards the floor as the head rises for 30 seconds.
Return to the neutral spine position and repeat about 3-5 times twice daily.
Lower Back Rotational Stretch (Seated)
This lower back rotational stretch is seated if the floor is uncomfortable for individuals with severe back pain.
Sitting in an armless chair or stool in a seated upright position, cross one leg over the other.
Then, place the left elbow against the outside of the right knee and twist and stretch the side.
Hold the postion for 10 seconds before slowly returning to a seated position.
Repeat the stretch on the opposite side.
Do this stretch 3-5 times on each side to stretch tight back muscles about twice daily.
Shoulder Blade Squeeze
This shoulder blade squeeze helps individuals properly posture while stretching and strengthening tight upper back and shoulder muscles.
Start in a seated upright position on an armless chair or stool.
Slowly pull the shoulder blades together in the upright position and hold for 5-30 seconds.
Relax, return to the upright position, and repeat 3-5 times twice daily.
References
Bang, A. A., Bhojraj, S. Y., & Bang, A. T. (2021). Back pain and musculoskeletal pain as public health problems: Rural communities await solution. J Glob Health, 11, 01007. https://doi.org/10.7189/jogh.11.01007
Calatayud, J., Escriche-Escuder, A., Cruz-Montecinos, C., Andersen, L. L., Perez-Alenda, S., Aiguade, R., & Casana, J. (2019). Tolerability and Muscle Activity of Core Muscle Exercises in Chronic Low-back Pain. Int J Environ Res Public Health, 16(19). https://doi.org/10.3390/ijerph16193509
Fischer, S. C., Calley, D. Q., & Hollman, J. H. (2021). Effect of an Exercise Program That Includes Deadlifts on Low Back Pain. J Sport Rehabil, 30(4), 672-675. https://doi.org/10.1123/jsr.2020-0324
Li, Y., Yan, L., Hou, L., Zhang, X., Zhao, H., Yan, C., Li, X., Li, Y., Chen, X., & Ding, X. (2023). Exercise intervention for patients with chronic low back pain: a systematic review and network meta-analysis. Front Public Health, 11, 1155225. https://doi.org/10.3389/fpubh.2023.1155225
Mohd Isa, I. L., Teoh, S. L., Mohd Nor, N. H., & Mokhtar, S. A. (2022). Discogenic Low Back Pain: Anatomy, Pathophysiology and Treatments of Intervertebral Disc Degeneration. Int J Mol Sci, 24(1). https://doi.org/10.3390/ijms24010208
Smith, J. A., Stabbert, H., Bagwell, J. J., Teng, H. L., Wade, V., & Lee, S. P. (2022). Do people with low back pain walk differently? A systematic review and meta-analysis. J Sport Health Sci, 11(4), 450-465. https://doi.org/10.1016/j.jshs.2022.02.001
Can using ghee improve diet and overall health for individuals looking to cook healthier?
Ghee
Ghee is a type of clarified butter that is commonly used in Indian and Middle Eastern cooking. It’s made by heating butter to remove water and milk solids, a clarification process that results in a golden, pure fat with a high smoke point. The butter is cooked longer than in clarified butter, allowing milk solids to brown before being strained, giving ghee a richer, nuttier flavor than traditional clarified butter. The clarification process is believed to remove impurities, creating a healthier product. The clarification removes milk solids, decreasing ghee’s lactose and casein content. This could benefit people with a milk allergy or sensitivity.
Ghee is almost completely pure fat, so it contains no carbohydrates.
Fats
Ghee is nearly 100% fat; one tablespoon has 15 grams, 9 of which are saturated fat. The remaining fat content is divided between 5 grams of healthier monounsaturated fat and less than one gram of polyunsaturated fat. Ghee is more concentrated than butter, containing more calories and fat.
Protein
Ghee may contain trace amounts of leftover protein if the milk solids or whey have not been completely removed in the clarification process.
Vitamins and Minerals
The micronutrient content can vary by brand and the supplied milk. A one-tablespoon serving contains about 8% of the recommended daily intake of vitamin A, 2% of vitamin E, and 1% of vitamin K. It’s recommended to use a small amount when cooking vegetables and other foods with fat-soluble nutrients so the body can better absorb them.
Benefits
Ghee has been used to improve memory, increase flexibility, and promote healthy digestion. However, further research is needed and ongoing to obtain scientific evidence to support health claims. For example, one animal study found no difference in memory or cognition from a diet that included ghee instead of regular butter, and there is no research on how ghee can help with memory. (Karandikar Y. S. et al., 2016)
Skin Health
Some individuals apply ghee topically as a salve for wounds, burns, or rashes. Research has confirmed that ghee has healing properties for the skin due to its antimicrobial and antioxidant activity, more than likely because of its vitamin A and E content. However, some studies examined ghee combined with honey, which provides other benefits. (Udwadia T. E. 2011) (Kotian S. et al., 2018)
Produces Less Acrylamide
Acrylamide is a potentially toxic and carcinogenic compound. It is produced when cooking fats are exposed to high heat. (American Cancer Society, 2019) A study found that ghee produces much less acrylamide when heated than vegetable oils and other saturated fats. (Daniali G. et al., 2016)
Allergies
Ghee is a dairy-based product. Individuals with a milk protein allergy could provoke an immune response, such as a rash, hives, vomiting, or diarrhea. Likewise, for individuals with lactose intolerance, consuming ghee could lead to symptoms of bloating, gas, or upset stomach. However, it may be less likely to cause allergic symptoms than butter since the clarification removes most lactose and casein components that typically cause adverse reactions. Talk to a doctor, dietitian, or allergist about whether ghee could be beneficial.
Adverse Effects
Since saturated fat is associated with the development of heart disease, the American Heart Association recommends reducing saturated fat to 5% to 6% of total daily calories for individuals who need to lower their cholesterol. A tablespoon of ghee contains about 40 milligrams of cholesterol, or 13% of the recommended daily intake, slightly higher than butter, 30 milligrams, or 10% RDI of the recommended daily intake. Recommendations are to use small quantities to enhance other foods, such as butter or oils.
Storage and Safety
Ghee usually comes in a glass jar. Depending on how quickly it will be used, it can be kept in a cool, dark place at room temperature, where it will be good for about three months. To extend its shelf life, it can be stored in the refrigerator for up to one year. While it will solidify when cooled, it will return to a liquid state once removed from the fridge. Ghee is available year-round at Indian and mainstream stores and sold online. However, it will probably be more expensive than regular butter because it takes more time and requires 16 ounces of butter to create 12oz. of ghee.
Preparation
Ghee has a nuttier flavor, higher density, and oilier texture, so individuals may not want to use it in the same ways that regular butter is, like spreading it on toast or baking it into pastries. For example, substituting ghee for shortening for pie dough may result in a richer flavor but a greasier texture. However, using ghee in baked goods can yield a crispier crust in certain recipes. A small serving can be used to enhance vegetable dishes. Its high smoke point makes it ideal for sautéing and stir-frying.
Smoke Point
The smoke point is the temperature at which fat starts to burn and smoke.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic providers use an integrated approach to create customized care plans for each patient and restore health and function to the body through nutrition and wellness, chiropractic adjustments, functional medicine, acupuncture, Electroacupuncture, and sports medicine protocols. If the individual needs other treatment, they will be referred to a clinic or physician, as Dr. Jimenez has teamed with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Learning About Food Substitutions
References
U.S Department of Agriculture. FoodData Central. (2019). Ghee. Retrieved from https://fdc.nal.usda.gov/fdc-app.html#/food-details/718294/nutrients
Karandikar, Y. S., Bansude, A. S., & Angadi, E. A. (2016). Comparison between the Effect of Cow Ghee and Butter on Memory and Lipid Profile of Wistar Rats. Journal of clinical and diagnostic research: JCDR, 10(9), FF11–FF15. https://doi.org/10.7860/JCDR/2016/19457.8512
Udwadia T. E. (2011). Ghee and honey dressing for infected wounds. The Indian journal of surgery, 73(4), 278–283. https://doi.org/10.1007/s12262-011-0240-7
Kotian, S., Bhat, K., Pai, S., Nayak, J., Souza, A., Gourisheti, K., & Padma, D. (2018). The Role of Natural Medicines on Wound Healing: A Biomechanical, Histological, Biochemical and Molecular Study. Ethiopian journal of health sciences, 28(6), 759–770. https://doi.org/10.4314/ejhs.v28i6.11
American Cancer Society. (2019). Acrylamide and cancer risk. https://www.cancer.org/cancer/risk-prevention/chemicals/acrylamide.html
Daniali, G., Jinap, S., Hajeb, P., Sanny, M., & Tan, C. P. (2016). Acrylamide formation in vegetable oils and animal fats during heat treatment. Food Chemistry, 212, 244–249. https://doi.org/10.1016/j.foodchem.2016.05.174
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine