Enzymes’ function is to help trigger bodily processes ranging from digestion to blood clotting to growth. What is the best way to support enzyme production?
Enzymes
Enzymes are proteins that act as biological catalysts. They cause and speed up crucial chemical reactions and help the body complete necessary chemical reactions. They are vital for many biological processes, including digestion, metabolism, and molecule building and breaking down. This includes breaking down food, facilitating growth, and forming blood clots. Too little of a certain type can lead to serious health implications like a fatal buildup of toxins. Individuals missing a certain kind of enzyme or having too little of it can develop serious health conditions.
Function
They help speed up chemical reactions in the body (National Human Genome Research Institute, 2025). They facilitate chemical reactions in everything from digesting food to muscle growth. Enzymes facilitate this by binding to a cell, creating the reactions needed. With enzyme binding, chemical reactions can occur without destroying the cell. (Nemours KidsHealth, 2023) Each cell in the body has thousands of enzymes to help facilitate all the complex reactions to maintain health. (National Human Genome Research Institute, 2025)
Factors Affecting Production
In healthy individuals, the body produces the enzymes it needs. However, metabolic disorders can occur if the body does not produce enough of a certain type. (Kennedy Krieger Institute, 2025) These disorders can be serious and are usually caused by a genetic malfunction that impacts production.
Types
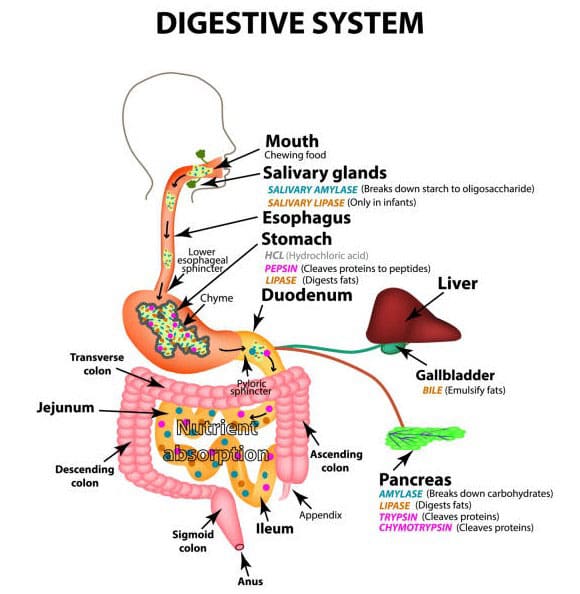
There are thousands of different types. Digestive enzymes, for example, aid in the breakdown of food and convert it into energy. Common enzymes that are critical for health include (Nemours KidsHealth, 2023)
Amylase
Digestive helps break down starches.
Aspartate aminotransaminase (AST) and Alanine Aminotransaminase (ALT)
Help the liver convert sugar into energy.
Creatine Kinase (CK)
Helps muscles create energy.
DNA Polymerase
Facilitates growth by allowing DNA to duplicate.
Glucose-6-Phosphate Dehydrogenase
Keeps red blood cells healthy by preventing damage to the cell.
Lipase
A digestive enzyme that helps break down fats and oils.
Protease
Digestive helps break down proteins.
Thrombin
Causes blood to clot.
Deficiencies
If the body doesn’t make enough of a certain enzyme, it cannot undergo the bodily processes that the enzyme helps facilitate. This can lead to a variety of symptoms. Some are minor, like not being able to eat lactose. Others are serious, like developmental delays caused by the build-up of toxins. (Kennedy Krieger Institute, 2025) Usually, these deficiencies are caused by genetics.
Types
There are various deficiencies. Some are very rare, while others can lead to conditions such as: (Nemours KidsHealth, 2023)
Lactose Intolerance
This is caused by not having enough of the enzyme that breaks down lactose, a sugar found in milk, leading to gas and bloating.
Tay-Sachs Disease
An often fatal disease caused by a missing hexosaminidase, which is responsible for breaking down fats
Gilbert’s Syndrome
This is caused by a missing enzyme that removes waste product (bilirubin) from the blood, leading to bilirubin buildup and
Jaundice or yellowing of the skin and whites of the eyes
Galactosemia
This leads to slow growth and trouble gaining weight, which is caused by the missing galactose-1-phosphate uridylyltransferase (GALT), which helps break down a sugar called galactose.
Phenylketonuria (PKU)
This is caused by having too little phenylalanine hydroxylase, which breaks down a protein called phenylalanine, causing brain damage.
Morquio Syndrome
This is caused by having too few enzymes that break down glycosaminoglycans, a type of sugar molecule.
This leads to bone and growth abnormalities.
Wilson’s Disease
A liver disease is caused by a missing protein that helps break down copper in the body.
Enzyme Production Support
Eat a healthy, well-balanced diet of fruits and vegetables to support enzyme production. Avoid processed foods, especially those that are very fatty (Johns Hopkins Medicine, 2025). The body produces all the necessary enzymes unless the individual has a genetic condition. Supplements aren’t usually required, but they can help with lactose intolerance or digestion in cystic fibrosis patients. (Nemours KidsHealth, 2023)
One supplement type, pancreatic enzyme replacement therapy (PERT), is available. PERT is an FDA-regulated prescription medication prescribed to patients with serious illnesses such as cystic fibrosis. (U.S. Food and Drug Administration, 2019)
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Care and Metabolism: The Hidden Link
References
National Human Genome Research Institute. (2025). Enzyme. Retrieved from https://www.genome.gov/genetics-glossary/Enzyme
U.S. Food and Drug Administration. (2019). FDA approves new breakthrough therapy for cystic fibrosis. Retrieved from https://www.fda.gov/news-events/press-announcements/fda-approves-new-breakthrough-therapy-cystic-fibrosis
For individuals experiencing musculoskeletal pain symptoms like lower back pain and shoulder pain, can incorporating cupping therapy help bring relief and manage pain?
Cupping Therapy
This ancient treatment is gaining public acceptance, and awareness has heightened, with various individuals and athletes being seen with round marks on their shoulders and backs. It is a pain treatment that, like acupuncture, comes from traditional Chinese medicine, or TCM. The therapy involves placing glass, silicone, or bamboo cups on the skin to create suction. The treatment is an alternative medicine technique used to relieve musculoskeletal pain. The suction is believed to promote healing (Cleveland Clinic, 2023)
Increasing Blood Circulation
The suction draws blood to the area, which can help reduce inflammation and promote healing.
Releasing Muscle Tension
The suction can stretch and pull on muscles, which can help relieve pain and tightness.
Breaking Up Adhesions
The suction can help break up scar tissue and adhesions that can cause pain and restricted movement.
Detoxifying the Body
Some practitioners believe that cupping can help remove toxins from the body.
It is typically performed by a trained practitioner who places the cups on the skin and leaves them in place for several minutes. The cups can be placed on various body areas, including the back, neck, shoulders, and legs. (Cleveland Clinic, 2023)
Benefits
Pain relief, especially for muscle and joint pain
Reduced inflammation
Improved circulation
Increased range of motion
Detoxification
Procedure
The medical practice involves creating skin suction using glass, ceramic, or plastic cups. How it’s done:
Preparation
The practitioner cleans the area where the cups will be placed.
They may apply oil or massage cream to the skin for easier movement of the cups.
Techniques
Dry
The practitioner heats the inside of the cup with a flame or pump, creating a vacuum.
The cup is then placed on the skin, which adheres due to the negative pressure.
The cup remains on the skin for several minutes, allowing the suction to draw blood and tissue into the cup.
Wet
Like the dry technique, the practitioner makes small incisions in the skin before applying the cup.
This allows blood to flow into the cup, creating a more intense suction.
Aftercare
The cups are removed, and the practitioner may apply pressure to the area to stop bleeding.
The patient is advised to avoid strenuous activity and hot showers for a few hours after the treatment.
The benefits of therapy include opening pores, stimulating blood flow, filtration, and balancing energy flow through the body. It’s often combined with massage and acupuncture. (Cleveland Clinic, 2023)
It also aims to alleviate symptoms of systematic diseases like diabetes and hypertension. However, more research is needed to see and fully analyze the effects of the treatment. (Aboushanab T. S., & AlSanad S. 2018)
Risks
The therapy is generally safe when done correctly and by a licensed professional. However, there is some risk of side effects like skin discoloration and scarring. Reports of rare side effects include bleeding inside the skull from cupping on the scalp and anemia from repeated wet techniques. (National Center for Complementary and Integrative Health, 2018) Other side effects can include:
Bruising
It can cause temporary bruising at the site of the cups.
Skin Irritation
Some people may experience skin irritation or burns from the suction.
Infection
There is a small risk of infection if the cups are not properly sterilized.
Injury Medical Chiropractic & Functional Medicine Clinic
It is important to consult with a healthcare professional before trying any new treatment, especially if you have any underlying health conditions. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Aboushanab, T. S., & AlSanad, S. (2018). Cupping Therapy: An Overview from a Modern Medicine Perspective. Journal of acupuncture and meridian studies, 11(3), 83–87. https://doi.org/10.1016/j.jams.2018.02.001
National Center for Complementary and Integrative Health. (2018). Cupping. Retrieved from https://www.nccih.nih.gov/health/cupping
Can stretching quadriceps help relieve stiffness and pain and improve flexibility for individuals with consistently tight quadriceps?
Quadriceps Stretches
Walking, running, biking, and other daily activities can tighten the quadriceps muscles. The quadriceps are four muscles in the front of the thigh that extend the leg and strengthen the knee. Stretching the quadriceps may be a part of a home or gym exercise program or physical therapy treatment to maintain quadricep flexibility. Resting the quadriceps with an exercise program can greatly maximize mobility and prevent injury.
Tight quadriceps may sometimes result from injuries such as patellofemoral stress syndrome or iliotibial band friction syndrome. The quads may also become tight for individuals with spinal stenosis or other related problems with the lower back. (International Sports Sciences Association, 2023) Ely’s test, also known as the Duncan-Ely test, is one way to determine whether your quadriceps are tight. It is a physical examination used to assess the flexibility and potential spasticity of the rectus femoris muscle (a quadriceps muscle) by passively flexing the patient’s knee. Lie on your stomach and try to touch your foot to your buttocks. If you can’t, the rectus femoris, one of the main muscles, may be tight and benefit from quadricep stretches. (Olivencia, O. et al., 2020)
Safety and Precautions
Before trying this or any other exercise program, consult a healthcare provider to ensure exercise is safe for you and your conditions. A professional can help diagnose any overuse injury that might be causing tight quadriceps. Quadriceps stretches will be a little more comfortable after warming up. A few minutes of walking or biking will warm the quadriceps muscles to stretch more easily.
Stretches
To stretch the quadriceps, try the standing, side-lying, and prone quadriceps stretch once fully warmed up and after a workout. Individuals who frequently experience quadriceps tightness should stretch them daily. Incorporate all or some of these stretches into a cool-down or off-day flexibility routine.
Standing Stretch
The standing quadriceps stretch can be done anywhere in the office, gym, or outside. All you need is a place to stand. Here is how:
While standing, hold onto a countertop or back of a chair to help with balance.
Bend your knee by grasping your ankle.
Move your foot toward your buttocks.
Gently pull on your ankle to bend your knee as far as possible.
Maintain position for 30 seconds.
Return to the standing position.
Repeat the exercise 3 to 5 times with each leg.
Stop stretching if there are any sharp pains.
Side-Lying Stretch
The side-lying quad stretch lengthens the quadriceps. On the floor in a supported position can help focus on the stretch. Here’s how:
Lie on your side.
Bend the knee of your top leg as far as you can, gently pulling with your hand.
Maintain position for 30 seconds.
Return to the starting position.
Repeat the exercise 3 to 5 more times with each leg.
Prone Stretch
Stretch the quadriceps while lying on your stomach. In this position, the floor helps to stabilize the pelvis, minimizing rocking and maximizing the stretch. To do the stretch:
Lie on your stomach.
Bend your knee back as far as you are able.
Grab your ankle to pull your foot toward your buttocks.
Maintain position for 30 seconds.
Return to the starting position.
Repeat the exercise 3 to 5 more times with each leg.
If you have difficulty reaching your ankle, pull the leg up, wrap a towel or strap around the ankle, and use it to pull. This can help stretch the quadriceps effectively even if you cannot reach the ankle easily.
Injury Medical Chiropractic & Functional Medicine Clinic
Consult a healthcare provider or physical therapist to learn the recommended quadriceps stretches or other strengthening exercises. Keeping the quadriceps healthy will help keep the knees moving and maximize functional mobility. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Care For Leg Instability
References
International Sports Sciences Association. (2023). How to Release Tight Quads in 2 Simple Steps. ISSA. https://www.issaonline.com/blog/post/how-to-release-tight-quads-in-2-simple-steps
Olivencia, O., Godinez, G. M., Dages, J., Duda, C., Kaplan, K., Kolber, M. J., Kaplan, & Kolber (2020). THE RELIABILITY AND MINIMAL DETECTABLE CHANGE OF THE ELY AND ACTIVE KNEE EXTENSION TESTS. International journal of sports physical therapy, 15(5), 776–782. https://doi.org/10.26603/ijspt20200776
Could making their own cervical neck roll help relieve pain and improve sleep for individuals who have neck pain after sleeping or during sleep?
Sleep Cervical Neck Roll
Neck pain can lead to sleep loss, leading to various health problems. Neck pain and everything that comes with it can limit the ability to work, drive, or sleep normally. A cervical roll may be one way to keep your neck in the optimal position while sleeping. Many with neck pain require extra support from their pillow. A cervical pillow can provide that support.
For individuals who develop neck pain, a visit to a chiropractic physical therapist can help manage symptoms. Treatments and modalities like traction may be necessary to relieve pressure on cervical nerves. (Gudavalli M. R. et al., 2015) Steps to self-manage neck pain may include performing specific neck exercises and maintaining proper posture (Hesby B. B. et al., 2019). Using the right pillow with the right support can help keep the neck in correct alignment, decrease or eliminate neck pain, and get you back to normal activities.
Neck Support During Sleep
The neck comprises seven vertebrae bones, normally forming a slight curve called lordosis. Maintaining a forward curve in the neck is important when treating neck pain, as it can help relieve pressure on spinal discs and nerves. A cervical roll, also known as a neck roll or cervical pillow, is a small pillow placed in the pillowcase that supports the neck while sleeping. The cervical roll provides the right amount of support for the neck and maintains alignment while lying down. (Gross A. R. et al., 2013)
Individuals can purchase a cervical roll online or at a store or pharmacy.
Individuals can also contact a physical therapist to help them obtain a cervical roll.
Making Your Own
Making a cervical roll is simple to do. Here’s how:
Using a hand towel.
Fold it in half.
Slide the towel into the pillowcase along the lower edge.
Be sure the towel is tucked in so it doesn’t slip out.
Individuals can place tape around it so it stays in the rolled shape.
The towel roll will also help support the neck when lying on one side or the other, filling in the space between the head and shoulder. Sleeping on the stomach is usually not recommended for neck pain. Exercise and postural correction training are essential components of treatment for neck pain, and finding the right sleeping posture can help quickly eliminate pain. (Harvard Publishing, 2022)
If neck pain persists, worsens, or is accompanied by arm weakness or numbness and tingling, a visit to a healthcare provider may be necessary to assess the cause. A visit to a local chiropractic physical therapist can also help. They can immediately show you how to treat neck pain.
Injury Medical Chiropractic & Functional Medicine Clinic
A cervical roll can give your neck the right support while sleeping. This can help you quickly and safely manage neck pain and return to your previous level of function. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
The Road To Recovery: Chiropractic Care
References
Gudavalli, M. R., Salsbury, S. A., Vining, R. D., Long, C. R., Corber, L., Patwardhan, A. G., & Goertz, C. M. (2015). Development of an attention-touch control for manual cervical distraction: a pilot randomized clinical trial for patients with neck pain. Trials, 16, 259. https://doi.org/10.1186/s13063-015-0770-6
Hesby, B. B., Hartvigsen, J., Rasmussen, H., & Kjaer, P. (2019). Electronic measures of movement impairment, repositioning, and posture in people with and without neck pain-a systematic review. Systematic reviews, 8(1), 220. https://doi.org/10.1186/s13643-019-1125-2
Gross, A. R., Kaplan, F., Huang, S., Khan, M., Santaguida, P. L., Carlesso, L. C., Macdermid, J. C., Walton, D. M., Kenardy, J., Söderlund, A., Verhagen, A., & Hartvigsen, J. (2013). Psychological Care, Patient Education, Orthotics, Ergonomics, and Prevention Strategies for Neck Pain: A Systematic Overview Update as Part of the ICON Project. The open orthopaedics journal, 7, 530–561. https://doi.org/10.2174/1874325001307010530
Harvard Health Publishing. (2022). Say “good night” to neck pain. https://www.health.harvard.edu/pain/say-good-night-to-neck-pain
Discover the versatility of pineapple in recipes and health benefits. This fruit is a must-have for your kitchen and diet.
Introduction
Many individuals will start eating more fruits and vegetables as part of a healthy diet in order to provide their bodies the necessary vitamins and minerals for optimum health. Many people may notice that overlapping pain-like symptoms, such as inflammation, are being lessened and controlled by eating a balanced diet. Pineapple is one fruit in particular that might lessen the inflammatory effects on the musculoskeletal system. The nutritional profile of pineapples, their ability to lower inflammation, and how to include them in one’s diet will all be covered in today’s article.
The Power Of The Pineapple
Pineapple (Ananas comosus L.) is more than just a tropical treat to snack on both frozen or on its own—it’s a nutritional powerhouse packed with essential vitamins, antioxidants, and enzymes that promote overall health. Innated in South America and anywhere tropical, the pineapple has been used to treat various ailments. (Kumar et al., 2023) This vibrant fruit is highly relished due to its unique aroma and sweet taste while containing vitamins and minerals that can be a delicious and natural way to incorporate into a healthy diet for optimal wellness. (Mohd Ali et al., 2020)
Nutritional Facts
While pineapple is being riched in nutrients, a single cup of fresh pineapple, which is about 165 grams, provides:
Calories: 82
Carbohydrates: 22g
Fiber: 2.3g
Sugars: 16g
Protein: 1g
At the same time, nutrients and vitamins from eating a pineapple provide immune function, energy production, and cellular repair. Some of the nutrients pineapple include:
Vitamin C: 131%
Manganese: 76%
Vitamin B6: 9%
Copper: 9%
Thiamine (B1): 9%
Fighting Inflammation Naturally- Video
Pineapple’s Role in Reducing Inflammation
When the body deals with pain-like issues, it can lead to inflammation. Inflammation is the body’s natural defense system that helps heal and attack pathogens in the affected area. This is due to the immune system sending out inflammatory cells and cytokines to start healing the affected area. One of the standout benefits of pineapple is its powerful anti-inflammatory properties. Pineapple has an enzyme known as bromelain.
One of the standout benefits of pineapple is its powerful anti-inflammatory properties, largely attributed to an enzyme called bromelain. This enzyme stems from the pineapple plant and has a double effect by modulating the immunological response that is significant for proper immune system functioning while preserving homeostasis. (Hikisz & Bernasinska-Slomczewska, 2021) Additionally, some of the benefits bromelain offers include:
Reduce Joint Pain and Swelling
Enhance Recovery After Exercise
Support Digestive Health
Additionally, bromelain can suppress the NF-KappaB signaling pathway by reducing inflammatory gene expression and attenuating the inflammatory cascade by breaking down the proteins involved in edema formation and swelling associated with inflammation. (Kansakar et al., 2024)
Additional Health Benefits of Pineapple
There are additional benefits when it comes to incorporating pineapple to not only reduce inflammation but also to help manage the body by:
Boosts Immunity
Supports Heart Health
Aids in Weight Management
This is because pineapple’s antioxidants help protect the body from free radicals that trigger illnesses caused by oxidative stress and inflammation. (Arulselvan et al., 2016) The fibers, antioxidants, and hydration levels can help the body even further when incorporated into a healthy diet.
Incorporating Pineapple Into Your Diet
Pineapple is incredibly versatile fruit and can be enjoyed in various ways. It provides an abundance of dietary fibers and phytochemicals and has a high nutritional value and medicinal properties. (Seenak et al., 2021) Some of the ways many people can incorporate pineapple into their diet include:
Fresh: Add chunks to smoothies, salads, or yogurt for an extra source of antioxidants. Additionally, put fresh pineapple chunks in the freezer for 2-3 hours on parchment paper for a delicious snack.
Grilled: Grilling pineapple can enhance its sweetness and be served with protein dishes.
Blended: Make refreshing pineapple juice or incorporate frozen chunks into tropical smoothies.
Cooked: Cooking pineapple on a stovetop can be a great option for incorporating it into stir-fries and salsas or as a topping for lean meats like chicken or fish.
Final Thoughts
In addition to being a summertime tropical fruit, pineapple is a superfood that is full of vitamins and nutrients with anti-inflammatory qualities that help the body fight against inflammation. A nutritious diet that includes pineapple can help many individuals feel more energized and control their pain-related symptoms. Eating fresh pineapple, whether it’s grilled, juiced, or combined into a smoothie, may improve their general health and well-being.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of incorporating anti-inflammatory foods to reduce the inflammatory effects from affecting the body. When asking important questions to our associated medical providers, we advise patients to implement small changes to their daily routine, like incorporating pineapple into a healthy diet, which can reduce the inflammatory effects in the body. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
References
Arulselvan, P., Fard, M. T., Tan, W. S., Gothai, S., Fakurazi, S., Norhaizan, M. E., & Kumar, S. S. (2016). Role of Antioxidants and Natural Products in Inflammation. Oxid Med Cell Longev, 2016, 5276130. https://doi.org/10.1155/2016/5276130
Hikisz, P., & Bernasinska-Slomczewska, J. (2021). Beneficial Properties of Bromelain. Nutrients, 13(12). https://doi.org/10.3390/nu13124313
Kansakar, U., Trimarco, V., Manzi, M. V., Cervi, E., Mone, P., & Santulli, G. (2024). Exploring the Therapeutic Potential of Bromelain: Applications, Benefits, and Mechanisms. Nutrients, 16(13). https://doi.org/10.3390/nu16132060
Mohd Ali, M., Hashim, N., Abd Aziz, S., & Lasekan, O. (2020). Pineapple (Ananas comosus): A comprehensive review of nutritional values, volatile compounds, health benefits, and potential food products. Food Res Int, 137, 109675. https://doi.org/10.1016/j.foodres.2020.109675
Seenak, P., Kumphune, S., Malakul, W., Chotima, R., & Nernpermpisooth, N. (2021). Pineapple consumption reduced cardiac oxidative stress and inflammation in high cholesterol diet-fed rats. Nutr Metab (Lond), 18(1), 36. https://doi.org/10.1186/s12986-021-00566-z
What type of exercise is recommended for individuals who want to exercise before bed?
Exercising Before Bed
Exercising sounds like a good way to tire the mind and body before bed. However, research shows that moderate to vigorous exercise later in the day can negatively impact sleep quality. (Alkhaldi E. H. et al., 2023)
To improve sleep, it is recommended that you exercise in the morning or earlier in the day, at least four hours before bed.
Individuals who exercise later should aim for lighter activities, such as non-strenuous walking or gentle, restorative yoga.
Light physical activity, like a slow walk after dinner, is OK.
Advantages
Daily exercise improves sleep quality. (Johns Hopkins Medicine, 2025) Mild exercise before bed and engaging in light activities like walking or stretching can positively affect health (Hijikata Y, Yamada S. 2011). These include:
Decrease muscle tension
Improve digestion
Improve blood sugar regulation
Relax the mind and body
Disadvantages
The nervous system naturally switches between active and calm. It is ready to work and engage in physical activities when it is active. When it is resting, sleep occurs. Activating the nervous system before bed can affect sleep, and exercising can affect body temperature, producing sleep challenges. Typically, body temperature decreases as the body prepares for sleep. Exercising before bed can increase core temperature and disrupt the process. (Szymusiak R. 2018) Moderate or vigorous physical activity close to going to sleep can: (Alkhaldi E. H. et al., 2023)
Make it more difficult to fall asleep
This leads to more waking up during the night.
Decrease sleep quality
Recommended Types of Exercise
Pre-bedtime activities should not be vigorous or engaging enough to make the body and mind more alert. Some exercises to calm the body and mind before bed include: (Sleep Foundation, 2023)
Restorative Yoga
Yoga Nidra and other low-intensity yoga can help promote sleep.
More intense forms of yoga, such as vinyasa/flow, should be done earlier.
Tai Chi
A Chinese practice that incorporates slow, gentle movements and focuses on breathing to promote peace and relaxation.
Slow Walking
Walking at a leisurely pace can help the body unwind and relax.
A slow heart rate and breathing indicate that the activity is calming and not stimulating.
Exercises to Avoid
Moderate to high-intensity workouts before bed that increase breathing and heart rate can disrupt sleep. Individuals who struggle to fall asleep or get restful sleep should try reducing the intensity of certain exercises or avoiding them one to two hours before bed. Examples of moderate to vigorous exercises include: (American Heart Association, 2024)
Gardening or heavy yard work
Running
Brisk walking
Cycling
Dancing
Sports activities
Working Out In The Evening
Sometimes, exercising later in the day or close to bedtime is the only time to get physical activity. If this is the case, late exercise is better than no exercise at all, but there are ways to lessen its impact on sleep, including:
Light physical activity, like walking, can be done up to an hour before bed.
Do more intense exercises at the beginning of the workout.
End the workout with a cooldown, like walking or stretching, to relax the mind and body.
Know how your workout schedule impacts your sleep, and adjust as necessary.
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Optimizing Your Wellness
References
Alkhaldi, E. H., Battar, S., Alsuwailem, S. I., Almutairi, K. S., Alshamari, W. K., & Alkhaldi, A. H. (2023). Effect of Nighttime Exercise on Sleep Quality Among the General Population in Riyadh, Saudi Arabia: A Cross-Sectional Study. Cureus, 15(7), e41638. https://doi.org/10.7759/cureus.41638
Johns Hopkins Medicine. (2025). Exercising for better sleep. https://www.hopkinsmedicine.org/health/wellness-and-prevention/exercising-for-better-sleep
Hijikata, Y., & Yamada, S. (2011). Walking just after a meal seems to be more effective for weight loss than waiting for one hour to walk after a meal. International journal of general medicine, 4, 447–450. https://doi.org/10.2147/IJGM.S18837
Szymusiak R. (2018). Body temperature and sleep. Handbook of clinical neurology, 156, 341–351. https://doi.org/10.1016/B978-0-444-63912-7.00020-5
Sleep Foundation. (2023). Bedtime routines for adults. https://www.sleepfoundation.org/sleep-hygiene/bedtime-routine-for-adults
American Heart Association. (2024). American Heart Association recommendations for physical activity in adults and kids. https://www.heart.org/en/healthy-living/fitness/fitness-basics/aha-recs-for-physical-activity-in-adults
Harvard Health Publishing. (2024). Does exercising at night affect sleep? https://www.health.harvard.edu/staying-healthy/does-exercising-at-night-affect-sleep
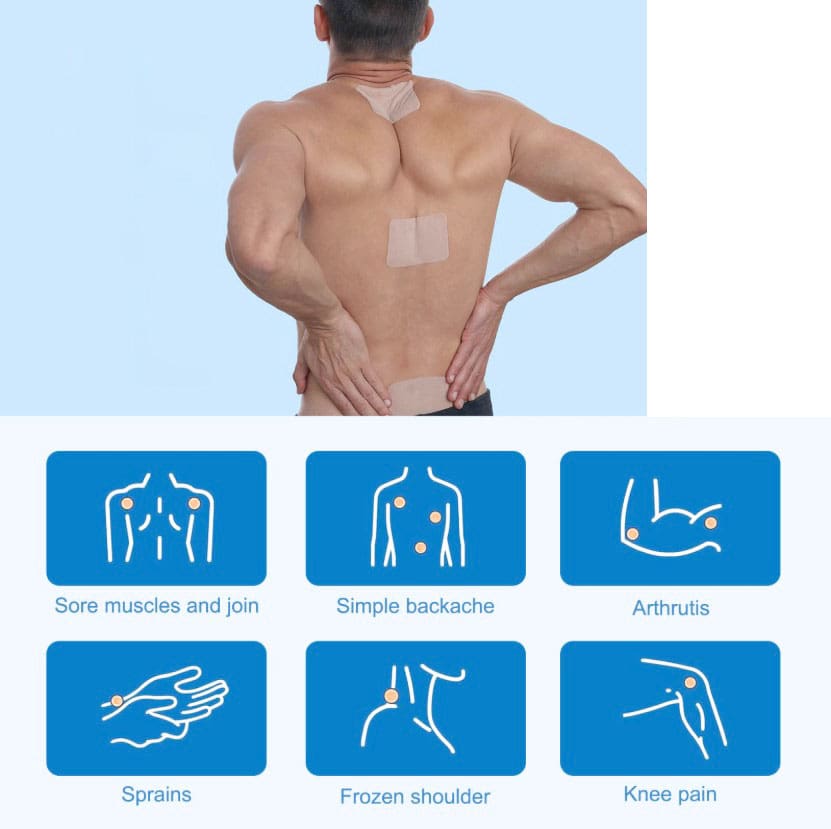
For individuals experiencing lower back pain and sciatica symptoms, can using a lidocaine patch help?
Lidocaine Patch
Lidocaine patches are in a drug class called local anesthetics (MedlinePlus, 2025) (Food and Drug Administration, 2022). They relieve pain in small body areas by blocking the nerves from sending pain signals. The Food and Drug Administration approved lidocaine 5% or 1.8% patches for relieving postherpetic neuralgia (PHN) pain. These lidocaine patches are prescription-only (Food and Drug Administration, 2022). They are available either by prescription or over the counter and are commonly used for back pain and other areas. Over-the-counter lidocaine, 4% patches, can be used to relieve minor aches and pains, including back pain. However, further research is needed to recommend the use of lidocaine patches as an effective method of pain relief. (Department of Veterans Affairs/Department of Defense, 2022) (North American Spine Society, 2020)
The Patch
They are available in prescription and over-the-counter forms. Over-the-counter forms come as a 4% patch in various brands, such as (MedlinePlus, 2025)
Aspercreme
Lidocare
Salonpas
Prescription-only patches come in 5% or 1.8% patches and are approved to relieve long-term nerve pain from shingles in adults. Zlido is a brand name for a 1.8% lidocaine patch. Five percent lidocaine patches are available generically. (DailyMed, 2018) (Food and Drug Administration, 2021) The safety and effectiveness in children are unknown. (Food and Drug Administration, 2022)
Other Lidocaine Forms
As a local anesthetic, it is available in several other forms, including:
Spray
Topical cream
Lotion
Liquid
Ear drops
Eye gel
Injection
It is also available as a short-term intravenous infusion for abnormal heart rhythm. (DailyMed, 2025)
Effectiveness
Clinical trials have shown that the patches effectively relieve chronic low back pain. However, these studies were nonrandomized and did not include a control group to compare against the treatment group. (Santana J. A., Klass S., & Felix E. R. 2020) The results may be subject to potential biases. For this reason, further evidence is needed to support lidocaine patches’ effectiveness in reducing low back pain. (North American Spine Society, 2020) High-quality randomized and controlled clinical trials are necessary to study the effectiveness. (North American Spine Society, 2020) (Santana J. A., Klass S., & Felix E. R. 2020)
Clean and dry the affected area before placing the patch.
Apply to the affected body area as directed.
Wash your hands after touching the patch.
Remove the patch after what is usually recommended after eight hours.
How Quickly Does It Work?
The amount of medication absorbed into the blood depends on how long the patch is placed on the body and how much is covered with the patch. In a study, healthy participants wore three lidocaine patches on their backs for 12 hours on and 12 hours off during 24 hours. Lidocaine levels were highest at 11 hours. At the end of the 24 hours, there was still some lidocaine left in the bloodstream. (Food and Drug Administration, 2022)
Individuals with PHN may notice a difference in pain intensity after four hours of using the patch. (Rowbotham, M. C. et al., 1996) (Food and Drug Administration, 2022) Experts may suggest using patches for four weeks for those who experience pain after their shingles rash disappears. However, if there is still pain after these four weeks, it is recommended to see a pain specialist. (Gross, G. E. et al., 2020)
Side Effects
Common side effects are typically mild skin reactions where the patch is. These reactions are usually temporary and will disappear within a few minutes or hours. Examples include: (Food and Drug Administration, 2022)
Severe allergic reactions are rare, but it is possible.
Symptoms include breathing problems, itchiness, and rash.
Methemoglobinemia
Methemoglobinemia is a condition that makes it hard for red blood cells to carry oxygen.
Individuals may experience symptoms of blue-looking skin, headache, lightheadedness, shortness of breath, abnormal heart rhythm, or seizures.
Using too many lidocaine patches to cover large parts of the body or using the patches longer than 12 hours within 24 hours may cause side effects that may include heart-related effects, such as a slow heart rate and low blood pressure. Individuals may also experience the following side effects (Food and Drug Administration, 2022)
Hot or cold sensation
Numbness
Dizziness
Ringing ears
Lightheadedness
Mood changes
Drowsiness to unconsciousness
Vision changes
Seizures
Tremors
Vomiting
Injury Medical Chiropractic & Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Sciatica Causes and Treatments
References
National Library of Medicine. MedlinePlus. (2025). Lidocaine transdermal patch. Retrieved from https://medlineplus.gov/druginfo/meds/a603026.html
Food and Drug Administration. (2022). Lidoderm label. Retrieved from https://www.accessdata.fda.gov/spl/data/eedfe43b-1019-19a0-e053-2995a90a7696/eedfe43b-1019-19a0-e053-2995a90a7696.xml
Department of Veterans Affairs/Department of Defense. (2022). VA/DoD clinical practice guideline for the diagnosis and treatment of low back pain. Retrieved from https://www.healthquality.va.gov/guidelines/Pain/lbp/VADoDLBPCPGFinal508.pdf
North American Spine Society. (2020). Evidence-based clinical guidelines for multidisciplinary spine care: diagnosis and treatment of low back pain. https://www.spine.org/Portals/0/assets/downloads/ResearchClinicalCare/Guidelines/LowBackPain.pdf
National Library of Medicine. DailyMed. (2018). Label: lidocaine patch. Retrieved from https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=5c66f3b9-6e04-47ab-8d94-21e89ceec154
Food and Drug Administration. (2021). Ztlido label. Retrieved from https://www.ztlido.com/wp-content/uploads/2022/12/ZTlido-LABEL.pdf
National Library of Medicine. DailyMed. (2025). Lidocaine-lidocaine hydrochloride injection, solution. Retrieved from https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=f1b26274-a55e-4321-b96c-ce0df830f205
Santana, J. A., Klass, S., & Felix, E. R. (2020). The Efficacy, Effectiveness and Safety of 5% Transdermal Lidocaine Patch for Chronic Low Back Pain: A Narrative Review. PM & R: the journal of injury, function, and rehabilitation, 12(12), 1260–1267. https://doi.org/10.1002/pmrj.12366
Rowbotham, M. C., Davies, P. S., Verkempinck, C., & Galer, B. S. (1996). Lidocaine patch: double-blind controlled study of a new treatment method for post-herpetic neuralgia. Pain, 65(1), 39–44. https://doi.org/10.1016/0304-3959(95)00146-8
Gross, G. E., Eisert, L., Doerr, H. W., Fickenscher, H., Knuf, M., Maier, P., Maschke, M., Müller, R., Pleyer, U., Schäfer, M., Sunderkötter, C., Werner, R. N., Wutzler, P., & Nast, A. (2020). S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology: JDDG, 18(1), 55–78. https://doi.org/10.1111/ddg.14013
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine