Running is one of the most popular forms of exercise, and offers many benefits. It can be done anywhere, it tones the lower body, and it burns a ton of calories. Pounding the pavement over time, however, can result in injuries to the knees, ankles, and hips.
Whether you run a few miles a week to keep the extra pounds off, or hoof it in several marathons a year, there is unfortunately a good chance you will get hurt at some point.
The first step to recovery if you injure yourself running is to give your body time to heal. A visit to the doctor, ice packs, and over the counter pain medication are all ways to treat an injury. However, one of the best ways runners can treat their injuries is by visiting a chiropractor.
If you are dealing with a running injury and think a chiropractor may be able to help you get back on your feet with less pain, you are most likely correct. Here are four important things to know about chiropractors and how runners can benefit from chiropractic care:
Runners: Chiropractors Work On More Than Necks And Backs
It’s a common misconception that a chiropractor’s sole purpose is to adjust their patients’ necks and backs. The entire body can benefit from a chiropractic manipulation. For example, the American Chiropractic Association (ACA) states that knee pain is the most common running injury.
Chiropractors are often able to work with an injured knee and bring about a positive outcome. Strains, sprains, and other trauma to your body’s joints can be treated by a chiropractor. Soft tissue around the joints benefit from chiropractic treatment, which can greatly ease an injury to the ankle, knee, or hip.
Chiropractic Promotes Quicker Healing Of The Injured Area
From increasing blood flow to the hurt area to breaking up restrictions with manual manipulation, chiropractic treatment helps the body heal itself. Chiropractors view the body in its entirety, and may use manipulations and adjustments on other parts of the body to stimulate healing of the afflicted area.
Chiropractors Assist In Pain Management
Running injuries can often cause great pain that lasts for weeks. Visiting a chiropractor can help reduce the severity of the pain and shorten the amount of time you experience pain. This is an especially attractive benefit for those who avoid taking medicine. Chiropractic care helps manage the discomfort and soreness associated with the injury, allowing the patient to rely less on drugs.
Chiropractic Reduces The Risk Of Getting Re-Injured
A common reason runners end up hurt is their bodies had something “out of whack” in the first place. Since chiropractors take the wellness of the body as a whole into consideration, they often work with runners to minimize the chance of re-injuring themselves or suffering a different injury. By making certain an individual’s body is in alignment and functioning properly, a chiropractor can help the runner feel comfortable moving back into the routine of running.
Running is a great form of exercise and stress relief, and many people run for years without incident. However, it�s vital to take steps up front to minimize the chances of getting hurt, including choosing proper shoes, stretching beforehand, and avoiding overexertion.
Stephanie Rothstein-Bruce: Professional Marathoner
If, however, you feel a twist, pop, or crack as you are out for your morning run or finishing your half marathon, know there are chiropractic treatment options available to you that will decrease pain, healing time, and the risk of re-injury. Just pick up the phone and give us a call. We�re here to help!
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
There’s something about gastrointestinal issues that makes them difficult to talk about in polite company, which unfortunately leaves many of us suffering one problem or another in silence. “What’s more, gastrointestinal, or GI, diseases are putting an increasing weight on Americans, causing an unprecedented number of clinical visits and hospitalizations than ever before”, stated Stephen Bickston, an American Gastroenterological Association professor of internal medicine at Virginia Commonwealth University.
What are the most prevalent gastrointestinal diseases?
Nevertheless, treatments for gastrointestinal diseases can be as simple as making informed lifestyle modifications or even taking over-the-counter drugs and medications. Peppermint oil and soluble fiber, for instance, has been used to help people with irritable bowel syndrome, or IBS, where a 2008 British Medical Journal study suggested that both of these natural remedies ought to be first-line treatment therapies for IBS. Here’s a rundown of the latest medical knowledge on five of the most common gastrointen.
Acid Reflux
Symptoms of acid reflux, such as heartburn, are among several of the most common digestive discomforts reported by the general population. In a Swedish study, approximately 6 percent of people reported suffering from acid reflux symptoms daily and 14 percent had them at least weekly. Such frequent symptoms may indicate the presence of gastroesophageal reflux disorder, or GERD. Aside from being painful, GERD, or gastroesophageal reflux disorder can damage the esophagus throughout the years or even lead to esophageal cancer.
“Heartburn typically involves a hot or burning sensation which rises up from the center of the abdomen area and to the chest under the breastbone or sternum”, states Michael Gold, a gastroenterologist at MedStar Washington Hospital Center in Washington, D.C. “It might also be accompanied by a sour taste in the mouth, or hypersalivation, in addition to discovering fluid or food out of your mouth, particularly at night time.” Pregnancy, several drugs and medications, as well as consuming alcohol or certain foods can cause heartburn. Children under the age of 12 and a few adults may have GERD without heartburn, instead experiencing asthma-like symptoms, difficulty swallowing, or a dry cough.
Treatment options for acid reflux include drugs and medications that reduce acid levels, like the proton pump inhibitors Aciphex, Nexium, Prevacid, Prilosec, and Protonix, along with the H2 blockers Axid, Pepcid, Tagamet, and Zantac. But taking these drugs and/or medications is not without risk. In 2008, a study found that a proton pump inhibitor can weaken the heart-protective impact of the blood thinner Plavix in patients taking the two drugs/medications together. In severe cases of gastroesophageal reflux disorder, surgeons can tighten a loose muscle found between the esophagus and the stomach, to inhibit the upwards flow of gastric acid. Laparoscopic surgery, which involves small incisions, has been proven to reduce scarring and shorten recovery time in comparison with open procedures.
Diverticulitis
By one estimate, about 3 in 5 Americans older than 70 years of age have the abnormal lumps called diverticula someplace in the wall of their intestinal tract. However, only 20 percent may experience a complication like diverticulitis, inflammation of a pouch, a tear, or an abscess.
Individuals with Crohn’s disease or ulcerative colitis, the two most prevalent inflammatory bowel diseases, complain of abdominal pain and diarrhea and may sometimes experience anemia, rectal bleeding, weight loss and other symptoms. “No definitive tests and evaluations exist for either disease and patients generally endure two primary misdiagnoses”, says R. Balfour Sartor, chief medical adviser to the Crohn’s & Colitis Foundation of America. “With Crohn’s”, he states, “appendicitis, irritable bowel syndrome, an ulcer, or an infection can be incorrectly diagnosed.”
In case diverticulitis does develop, symptoms are most likely to manifest through abdominal pain and potentially fever, however, antibiotics can treat the problem. In severe instances, a tear can result in an abscess, which might result in nausea, vomiting, fever, and intense abdominal tenderness which demands surgical repair. Some healthcare specialists consider that a diet too low in fiber could trigger the gastrointestinal disease, which develops growingly common with age and is most widespread in western societies.
Inflammatory Bowel Disease
Both disorders may emerge from a wayward immune system that leads the body to attack the gastrointestinal tract, or GI tract. Crohn’s disease involves ulcers that could seep deep into the tissue lining at any given section of the GI tract, leading to infection and thickening of the intestinal wall and blockages which may need surgery. Ulcerative colitis, by comparison, interrupts only the colon and rectum, where it also causes ulcers; colitis is characterized by bleeding and pus.
Treating either disease requires beating back, then constantly holding in check, the inappropriate inflammatory response. Both steps are accomplished by means of a combination of prescription anti-inflammatories, steroids and immunosuppressants. Crohn’s patients might also be given antibiotics or other specialized drugs and medications. The current debate stands as to whether Crohn’s disease sufferers benefit if given highly potent treatment therapies early in the course of the gastrointestinal disease instead of escalating potency with time from milder initial treatments, as is traditionally done, clarified Themos Dassopoulos, manager of inflammatory bowel diseases at Washington University at St. Louis. Surgery “cures” ulcerative disorders by simply taking away the colon but signifies that patients will need to wear a pouch, internally or externally, for waste. “Inflammatory bowel disease, or IBD, patients must take particular caution when using NSAIDs, such as aspirin, since these painkillers may cause additional gut inflammation in 10 to 20 percent of individuals, ” states Dassopoulos.
Constipation
The fact that Americans spend $725 million annually on laxatives indicates that trying to unclog the nation’s plumbing, so to speak, is a national pastime. But overuse of stimulant laxatives, which cause the intestines to contract rhythmically, can make the gut more reliant on these, requiring more of them and finally rendering the aid ineffective. First, a little bit of clarification on the frequency of your flushing: “There is no need to worry about having a daily bowel motion; anywhere between three times a day and three times per week is normal”, says Sandler.
“However, if you are having discomfort and can not make your bowels move, try out an over-the-counter remedy such as milk of magnesia’,’ he states. And should you have attempted laxatives or not, going a week without a bowel movement is a very good reason to see the doctor, ” says Sandler. Constipation, hard stools, and straining could result in hemorrhoids or an anal fissure. Constipation is best avoided through regular exercise and a diet high in fiber from whole grains, fruits, and vegetables. To elderly folks, that are inclined to become constipated more frequently: Be sure you’re hydrating properly and conscious of any drugs and medications which may be causing your bowel movements to be backed up.
Gallstones
Just a quarter of people with gallstones typically require treatment. That’s fortunate, because every year nearly 1 million Americans are diagnosed with these small pebbles, which are largely made of cholesterol and bile salts. Eliminating these typically requires removal of the gallbladder, one of the most frequent surgeries in the United States.
“Gallstones can get blamed for symptoms caused by other, more elusive culprits, such as irritable bowel syndrome”, states Robert Sandler, chief of the division of gastroenterology and hepatology together with the University of North Carolina School of Medicine. An ultrasound evaluation may pick them up while missing the real issue. “If you’re told you’ve got to have gallstones out however they aren’t bothering you, get a second opinion”, he advises. Removal may be mandatory when the stones instigate infection or inflammation of the gallbladder, pancreas, or liver. This can happen if a stone going out of the intestine becomes trapped, blocking the flow of bile, at the ducts between the liver and the small intestine.
The pain of a gallstone lodged at a duct normally comes on quickly at the right upper abdomen, between the shoulder blades, or beneath the right shoulder,� and also means a visit to the ER is necessary, as may fever, vomiting, nausea, or pain lasting more than five hours. Gallbladder removal may be accomplished laparoscopically and more recently has been completed with no external incision by going through your mouth or vagina. Obesity can also be a risk factor for gallstones, and it is theorized that they increase due to a lack of fiber and an excessive amount of fat from the western diet. Losing weight then regaining it also seems to set the stage for the common gastrointestinal disease. In a 2006 study of men, the more frequent the weight cycling and the bigger the amount of pounds fall and are regained, the larger the chances of developing gallstones. Women, in particular those people who are pregnant or using birth control pills, face an increased risk of developing gallstones as well.
We will continue to discuss the common issues affecting the gastrointestinal tract, or GI tract, including the colon as well as rectum and anal problems, in the following series of articles. The 5 common gastrointestinal diseases mentioned above can manifest pain and discomfort as well as a variety of other symptoms if left untreated. Be sure to seek proper medical attention. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Asthma is a chronic lung disease that has afflicted more people in the last 20 years than ever. Some doctors attribute the increase to the pollutants in the air, the changes in the modern diet, and lack of adequate ventilation in homes.
According to the Mayo Clinic, asthma symptoms vary by individuals and may be mild, severe, or somewhere in between. Shortness of breath and tightness in the chest, along with a wheezing sound when exhaling are common asthma symptoms. Common treatments include inhalers and other medications.
With the millions of asthma sufferers seeking relief, non-traditional treatments have emerged in addition to the everyday remedies. One of the alternatives that has shown positive results is chiropractic care.
A person who suffers from asthma can enjoy multiple benefits from chiropractic. Four of the top benefits chiropractic care can bring to asthma patients are the following:
Reducing The Frequency Of Attacks
Over time, spinal adjustments can help some asthma sufferers decrease the number of attacks. When a spine is in alignment, energy flows through the nerves to the person’s organs. A nonaligned spine can cause the energy to fail to flow through the nerve endings as effectively, and a host of issues can arise.
The lungs can suffer when the spine is not aligned. Chiropractors are able to treat the spine so that, over time, it aligns. In some cases, this helps lung function and decreases the number of asthma attacks.
Stimulating Air Flow
The lungs are obviously vital for breathing, but the airway and diaphragm also play a part. Both of these can be hindered by a spine that is not aligned.
When a chiropractor works with a patient to align the spine, the airways and diaphragm can move more freely, allowing better airflow. While this is not a cure for asthma, in many cases stimulating a body’s airflow can help decrease the suffering the chronic condition causes.
Boosting The Immune System
A significant number of asthma attacks are brought on and exacerbated by an individual’s low immune system. Chiropractic care helps increase the effectiveness of the immune system.
Think of it this way: The autonomic nervous system is connected to the body’s immune system by way of the endocrine system. When the spine is out of line, it can affect the immune system.
If a person suffers from chronic asthma attacks, this could be the time when he or she has an episode. A chiropractor who can align the spine can create a positive domino effect. The nervous system improves, the immune system improves, and the asthma attacks decrease.
Working In Conjunction With Traditional Asthma Medication
People with asthma commonly use inhalers and steroids to manage their symptoms. Chiropractic care is non-invasive and works with these treatments to lessen the instances and severity of attacks.
A study by Michigan Chiropractic Council showed that asthma sufferers who went through 30 days of chiropractic treatments reported a 70% reduction in medication.
Patients who commit to chiropractic can sometimes manage the symptoms more naturally, and lessen their dependence on medications. (It’s important to note that patients should never go off medications on their own. Always speak to a doctor before changing medications).
Patients fortunately have a variety of treatment options. For those who don’t respond to traditional medication, or who wish to decrease their dosage, non-traditional choices like chiropractic may be the answer.
Tips For Preventing Dehydration
It’s advisable to speak to both your medical doctor and Doctor of Chiropractic about your asthma symptoms. By having both disciplines co-manage your case, you�ll work toward a healthier outcome, possibly even without the use of drugs. Give us a call to learn more.
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Food is one of the most essential basic needs. It is made up of nutrients, micronutrients, such as vitamins and minerals, and macronutrients, such as carbohydrates, proteins and fats. A balanced diet, consisting of a variety of these nutrients is the foundation of good health. While consuming the necessary daily intake of carbohydrates, high-quality proteins, heart-healthy fats, vitamins, minerals and water is essential towards maintaining the body’s overall well-being and function, staying healthy and productive could not be achieved without one important structure: the digestive system.
What is the digestive system?
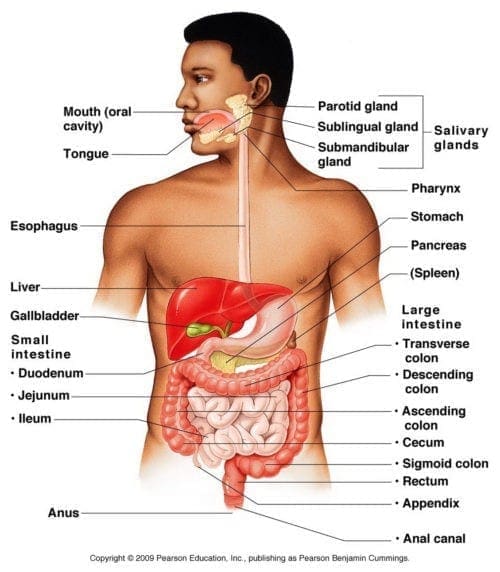
The digestive system is a collective group of organs which function together to convert food into energy and provide basic, fundamental nutrients in order to nourish the entire body. Food is delivered through a long tube inside the body known as the alimentary canal, best referred to as the gastrointestinal tract, or the GI tract. The gastrointestinal tract consists of the oral cavity, or mouth, pharynx, esophagus, stomach, small intestines, and large intestines. Along with the gastrointestinal tract, there are various important accessory organs which additionally help the human body to digest foods, however, these do not have food pass through them. Accessory organs of the digestive system include the teeth, the tongue, salivary glands, liver, gallbladder, and the pancreas.
Digestive System Anatomy
Mouth
Food begins its course through the digestive system at the mouth, also known as the oral cavity. As a matter of fact, digestion is considered to begin here as soon as you take the first bite of a meal. Within the mouth are numerous accessory organs which aid in the digestion of food: the teeth, the tongue, and the salivary glands. Teeth chop food into smaller pieces, to allow for an easier digestion, which are then moistened by saliva to begin the process of breaking the food down, before the tongue and other muscles of the mouth push the food into the pharynx.
Teeth. The teeth are 32 small, hard organs located along the anterior and lateral edges of the mouth. Each tooth is created from a bone-like material called dentin and coated in a layer of enamel, the hardest substance in the human body. Teeth are living organs that also contain blood vessels and nerves under the dentin in a soft region, best referred to as the pulp. The structure of the teeth is made for cutting and grinding food into smaller pieces.
Tongue. The tongue is located on the inferior section of the mouth only posterior and medial to teeth. It’s a small organ composed of several pairs of muscles coated in a thin but strong, bumpy, skin-like layer. The outside of the tongue contains many papillae designed for grasping food as it’s moved by the tongue’s muscles. The taste buds on the surface of the tongue distinguish flavor molecules in food and link to nerves in the tongue to deliver taste information to the brain. The tongue can also help push food toward the posterior area of the mouth for swallowing.
Salivary Glands. Surrounding the mouth are three varieties of salivary glands. The salivary glands are sets of accessory organs that produce a watery secretion known as saliva. Saliva helps to moisten food and starts the digestion of food. The body also uses saliva to continue lubricating food as it moves through the mouth, pharynx, and esophagus.
Pharynx
The pharynx, or throat, is a funnel-shaped tube connected to the back end of their mouth. The pharynx is responsible for the delivery of a mass of chewed food from the mouth to the esophagus. The pharynx also has a significant role in the respiratory system, as air from the nasal cavity passes through the pharynx on its way to the larynx and finally the lungs. Since the pharynx serves two different functions, it includes a flap of tissue called the epiglottis which behaves as a switch to effectively route food into the esophagus and air into the larynx.
Esophagus
The esophagus is a muscular tube which connects the pharynx to the stomach, that is part of the upper gastrointestinal tract, or upper GI tract. By means of a series of contractions, referred to as peristalsis, it transports the eaten masses of chewed food along its span. At the inferior end of the esophagus is a muscular ring known as the lower esophageal sphincter or cardiac sphincter. The role of the sphincter is to shut off the end of the esophagus and keep food from passing backwards into the esophagus, and instead maintain it in the stomach.
Stomach
The stomach is a muscular sac that’s located on the left side of the abdominal cavity, just inferior to the diaphragm. In an average individual, the stomach is about the size of their two fists placed alongside each other. This major organ plays the role of serving as a sort of storage tank for foods so the body has enough time to digest large meals properly. The stomach also contains hydrochloric acid and digestive enzymes which continue the digestion of food that began from the mouth. When it leaves the stomach, food is the consistency of a liquid or paste.
Small Intestine
Made up of three segments, the duodenum, the jejunum and the ileum, the small intestine is a long, thin tube about 1 inch in diameter and approximately 10 feet long which is part of the lower gastrointestinal tract, or lower GI tract. It is located only inferior to the stomach and takes up nearly all the space in the abdominal cavity. The entire small intestine is coiled like a hose and the interior surface is filled with lots of ridges and folds. These folds are utilized to make the most of the digestion of food and absorption of nutrients. The small intestine continues the process of breaking down food with the help of accessory organs. Contractions known as peristalsis are also at work within this organ. By the time food leaves the small intestine, approximately 90 percent of nutrients are extracted from the food which entered it.
Liver and Gallblader
The liver is a roughly triangular accessory organ of the digestive system found to the right of the stomach, just inferior to the diaphragm and superior to the small intestine. The liver weighs about 3 pounds and is the second largest organ in the human body. The liver has many different functions, but its primary purpose is the production of bile and its secretion into the small intestine for digestion. Another of its important functions include the cleansing and purification of the blood flowing from the small intestine, which contains the absorbed nutrients. The gallblader is a small, pear-shaped organ found just posterior to the liver. The gallbladder is used to store and recycle surplus bile from the small intestine, through a channel known as the cystic duct, so that it might be re-utilized for the digestion of subsequent meals.
Pancreas
The pancreas is a large gland situated just inferior and posterior to the stomach. It is approximately 6 inches long and shaped like short, lumpy snake with its “head” attached into the duodenum and its “tail” pointing towards the left wall of the abdominal cavity. The pancreas secretes digestive enzymes into the small intestine to complete the digestion of foods. These enzymes break down carbohydrates, proteins and fats from the food we eat.
Large Intestine
The large intestine, best referred to as the colon, is a long, thick tube about 2.5 inches in diameter and approximately 5 feet long.�It is made up of the cecum, the ascending colon, the transverse colon, the descending colon, and the sigmoid colon, which connects to the rectum. It is located only inferior to the stomach and wraps across the lateral and superior border of the small intestine. The large intestine absorbs water and also contains many symbiotic bacteria which aid in the breaking down of wastes to extract small quantities of nutrients. Stool, or waste left over from the digestive process, is passed through the colon by means of peristalsis, or contractions, first in a liquid state and ultimately in solid form as the water is removed from the stool. Stool, or feces, in the large intestine exits the body through the anal canal, to begin the process of elimination.
In conclusion, the digestive system is ultimately essential to effectively break down the food we consume to provide our body with energy and basic nutrients. Unfortunately, however, as with other systems of the body, gastrointestinal diseases can alter the healthy function of the digestive system. The gastrointestinal tract may appear normal but may not be working properly. Symptoms can vary widely on the individual depending on the problem.� We will discuss the common issues affecting the gastrointestinal tract, or GI tract, including the colon as well as rectum and anal problems, in the following series of articles.�The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Fibromyalgia is one of today’s most common chronic pain conditions. According to the American College of Rheumatology, around 1 in 50 Americans currently suffer from fibromyalgia. Unfortunately, the condition is difficult to diagnose, and, being chronic in nature, can linger for several months or even years. Fibromyalgia typically causes pain throughout the body and creates areas so tender that the slightest pressure hurts.
Patients diagnosed with the condition have both traditional and alternative treatment options available to them. Traditional approaches to managing the pain and treating fibromyalgia are anti-inflammatory prescriptions, sleep medications, and muscle relaxers. Patients frequently choose natural remedies instead of or in addition to traditional medication, such as vitamin therapy, acupuncture, and meditation. One of the most common treatments is chiropractic care.
The main ways chiropractic care benefits those who suffer from fibromyalgia are:
Reduces Fibromyalgia Pain Levels
The most difficult issue to deal with for fibromyalgia sufferers is the constant pain, which often affects the entire body for weeks or months at a stretch. Although these patients initially seek care for the pain they�re experiencing, they soon realize that chiropractic also helps restore overall health and aids the body in self-healing.
By adjusting the spine to improve alignment, as well as incorporating some form of soft tissue work, chiropractors can assist fibromyalgia patients in minimizing their painful pressure points. Many who suffer with this condition look for relief with chiropractic treatment options, and experience a decrease in the tender spots.
Increases Range Of Motion
Chiropractors are also able to adjust the body’s joints and help loosen them. For fibromyalgia patients, this can sometimes increase their range of motion and allow them to move more easily.
Sometimes it takes several treatments to see significant results, so it’s important to note that chiropractic treatment of fibromyalgia takes a commitment from the patient. The effects, however, are well worth the time invested.
Boosts Sleep Quality
A common by-product of the pain associated from fibromyalgia is lack of sleep. As anyone knows, being unable to snag several hours sleep can leave you feeling tired, foggy, and irritable.
By working with a chiropractor to loosen their joints and manage their tender points, patients suffering from this condition can enjoy a deeper sleep, and stay asleep longer.
Complements Other Treatments
Sometimes medicines counteract with each other, or mix together and cause side effects. A big advantage of chiropractic care is it can be utilized in tandem with medications or other remedies, whether traditional or natural.
An individual who is diagnosed with this condition should speak to his or her chiropractor about the various ways to treat it, and remember that there is not a one-stop solution. A treatment regimen should be built on a case-by-case basis tailored to the specific needs of that patient.
Empowers The Patient
Individuals who must cope with painful, chronic illnesses can become exasperated with treatment options, and feel as if they have no control over their situations. Unfortunately, these feelings can bring on stress and depression, which only works against getting better. By working with a chiropractor, patients can feel more in charge of their pain management and more optimistic in their recovery.
People who are diagnosed with fibromyalgia need to understand that there are options available to them for pain management, and they may decide to try more than one at a time. Chiropractic care is a valuable tool to treat the symptoms of fibromyalgia, and patients who will commit will see the benefits of less pain, greater mobility, and better sleep. And, perhaps the best benefit of all, they can take control of their circumstances and be a vital part of managing their personal well-being.
Retired Brig. General Rebecca Halstead Shares How Chiropractic Care “Saved Her Life”
If you or a loved one are suffering from fibromyalgia, don�t do it alone. Our chiropractor has a passion for helping sick people get well. So contact us today to schedule an appointment.
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Sitting: It’s no big secret that exercise is good for you. Many articles and books have been written and studies completed on the subject of physical fitness. However, lately it’s been discussed as to whether that five mile run or spin class is really enough. Is our work environment undoing any positive effort we put into staying healthy?
The short answer is YES. Human bodies were not built to sit for long periods of time. Our twenty-first century workplace � working behind a desk, typing on the computer, endless video conferences � unfortunately stacks against us to keep us on our� well, not our feet.
There are four harmful results on a person’s body that stem from sitting at work.
Sitting For Many Hours Each Day Takes A Toll On Our Backs.
Working at a desk for many hours a day causes employees to stay in one position for an extended length of time. This puts a great deal of pressure on their backs. Over time, painful back problems can develop and, if left untreated, continue to worsen.
Sitting Also Takes A Toll On Our Waistline.
Obesity is at an all time high in the United States, and at least a good chunk of the reason is our sedentary lifestyle. Sitting for a long period (8 or more hours a day) decreases our metabolism, causing us to burn fewer calories. The time at our desks can end up packing on the pounds.
Sitting Can Increase The Chance Of Developing A Life-Threatening Disease.
Studies show individuals with sedentary jobs have more health problems than their active counterparts. Cardiovascular disease and Type 2 diabetes are both examples of health issues that arise more often in people who regularly sit down most of the day.
Sitting Can Cause Premature Death.
This may sound melodramatic, but it’s true. As we talked about above, sitting for prolonged periods of time puts you at greater risk of diseases that may end up killing you. A study published in the Archives of Internal Medicine, “found people who sat for over 11 hours a day had a 40% greater risk of dying within three years from any cause than people who sat less than 4 hours a day.”
So, what should a sedentary office person do to improve their health and decrease the risk many hours of daily sitting causes?
Get on your feet! Schedule times during the day to stand up and walk around. If you can’t remember to do it, add an alarm on your cell phone. Even a couple minutes on your feet every hour will help balance prolonged sitting.
Learn to sit correctly. If you must sit, make certain your chair isn’t causing more damage. Select a chair that is height and angle adjustable. The seat should support your lower body, and the back should fit the curves of your spine. Special bonus points go to chairs with lumbar support and that rock.
Visit your chiropractor.Back problems brought on by a job behind a desk are not going to magically go away, and can get worse over time. Make a chiropractor appointment, get examined, and work to correct the issue.
Invest in a standing desk. A growing trend is to turn a sitting job into a standing job. Desks that are taller have the ability to keep you on your feet longer, which will provide many health benefits in the long run.
Good health is one of our greatest assets, and it pays to protect it. By understanding the risks of a sedentary working environment, we can be proactive in increasing activity and promoting our individual fitness.
Avoid Back Surgery
If you or a loved one needs more insight on how chiropractic can guide you toward a healthier lifestyle, give us a call. We�re here to help!
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Calcium is one of the most omnipresent mineral in the human body. An average-sized adult’s body, for instance, can contain approximately 1000 to 1200 grams of calcium, which is generally, invisibly integrated into bones and teeth by the widely available type of mineral, identified as calcium-hydroxyapatite (Ca10(PO4)6(OH)2) crystals. The rest circulates throughout the blood and soft tissues, as it plays fundamental roles in cell conduction, muscle function, hormone regulation and vitamin K-dependent pathways, as well as for proper cardiac and blood vessel function.
What role does calcium play in heart health?
Several research studies indicate that just about 30 percent of the United States population consumes the Recommended Dietary Allowance of calcium, which calls for approximately 1000 to 1200 milligrams on a regular daily basis. Furthermore, humans can absorb only about 30 percent of calcium from foods, based on the particular source. The body will in turn, demineralize its own skeletal system to maintain the proper serum calcium levels in scenarios where dietary calcium is inadequate and/or absorption is decreased, and/or excretion is increased.
Epidemic of Osteopenia/Osteoporosis
Starting at around the age of 50 years old, postmenopausal women lose about 0.7 to 2 percent of their bone mass each year, while men over age 50 years lose 0.5 to 0.7 % annually. Between ages 45 and 75 years of age, women lose 30 percent bone mass, whereas men lose 15 percent.
According to the US Surgeon General’s Report, one in two Americans over the age of 50 are expected to have an increased risk of developing osteoporosis. Osteoporosis causes 8.9 million fractures annually, with an estimated cumulative cost of incident fractures predicted at US $474 billion over the next 20 years. Among mature women over the age of 45, osteoporosis accounts for more days spent in the hospital than many other conditions and diseaes, such as diabetes, myocardial infarction (MI), chronic obstructive airway disease and even breast cancer. Fragility fractures are the primary cause of hospitalization and/or death for US adults age 65 years and older; and 44 percent of nursing home admissions are caused by fractures.
A Mayo Clinic study noted that compared to 30 years ago, forearm fractures have increased more than 32 percent in men and 56 percent in women. The authors of the research study concluded that dietary changes, such as inadequate calcium and extra phosphate, were considerably associated with increased fractures. Public health approaches are critical to prevent symptomatic bone disease, however, widespread psychiatric prophylaxis is prohibitively costly and carries potentially serious adverse effects.
Cardiovascular Disease and Bone Disease
Strong epidemiological associations exist between decreased bone mineral density (BMD) and increased risk of the cardiovascular disease (CVD) and CVD death. For instance, individuals with osteoporosis have been reported to have a higher risk of developing coronary heart disease (CHD), as well as cardiovascular disease. This issue will be magnified if the remedies for osteoporosis (eg, calcium supplements) separately increase the risk of MI.
Issues with Dairy as Primary Source of Calcium
Dairy foods and drinks account for about 70 percent of dietary calcium intake among Americans. Dozens of epidemiological and randomized controlled trials in adults and children have utilized dairy products as the main source of calcium, and have credited dairy intake with preventive benefits on study end points such as bone mass, fractures and osteoporosis. A current meta-analysis of over 270,000 people revealed a strong trend for dairy intake protecting against hip fracture; the relative risk (RR) of hip fracture each day glass of milk was 0.91, 95 percent CI 0.81 to 1.01.
In most industrialized countries, milk is frequently the most cost-effective strategy for achieving recommended levels of calcium consumption in a population level. However, legitimate concerns exist regarding potential deleterious effects of chronic dairy intake on health. Dairy foods, on a time scale, are relative new-comers to the hominin diet. Domestication of cattle, sheep and goats first happened approximately 11,000 to 10,000 years ago. Furthermore, it seems that an estimated 65 percent of the global population expresses the pheno-type of lactase non-persistence.
Consumption of cow’s milk has been inconsistently associated with cataracts, ovarian and prostate cancers, and Parkinson’s disease, as it’s also been implicated in certain autoimmune diseases, such as type 1 diabetes and multiple sclerosis. Overall, the evidence for dairy-induced human diseases seems to be consistent for prostate cancer and for type 1 diabetes. A recent study of over 106,000 adults followed for 20 years showed that drinking three or more glasses of milk per day was associated with increased risks for bone fracture and higher mortality rates in comparison to ingesting more than 1 glass of milk every day. By comparison, for the women in that study, daily serving of cheese and/or other fermented milk products such as yogurt was associated with a 10 to 15 percent decrease in the rates of mortality and hip fractures (p<0.001). However, this was an observational study with inherent constraints such as residual confounding and reverse causation. In conclusion, solid results cannot be drawn in the data.
The sugar in milk, lactose, is broken down in the gastrointestinal tract into d-galactose and d-glucose. D-Galactose has been proven to increase inflammation and oxidation in adult humans, and in mature animals this sugar triggers accelerated ageing, neurodegeneration, and a shortened life span. Therefore, cow’s milk, even though rich in many nutrients,including sodium, has issues that leave it less than ideal as a dietary staple for most adults. On the contrary, fermented milk foods, such as cheese and yogurt, appear to be safer than milk, perhaps because the mostor all of d-galactose has been metabolized by bacteria, to make these staple food products.
Calcium, as with many other vitamins and minerals, is a fundamental compound needed to support the proper function of the human body, particularly when it comes to cardiovascular disease and heart health. Although these results have been displayed in several research studies, it’s essential to consult a healthcare professional to discuss your nutritional options. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Boosting The Immune System
Boosting The Immune System