Find out what you need to know about thoracic outlet syndrome associated with a car accident and the potential long-term consequences.
Introduction
Your life may be completely upended by a car accident more quickly than you can say “fender bender.” They may leave you with injuries that linger like an unwanted visitor, in addition to crumpled bumpers and insurance-related hassles. The cervical spine, the unsung hero that keeps your head up as you binge-watch your favorite program, is one such damage. A disease known as Thoracic Outlet Syndrome (TOS), which may cause your arms to feel like they’re trying out for a zombie movie with all that numbness and tingling, can result from ligament damage caused by an accident that jolts your neck. We’ll explore the clinical viewpoint of these injuries in this essay, emphasizing how El Paso physician Dr. Alexander Jimenez aids in victims’ recovery and the need to record these injuries for your health and any future legal claims.
What Happens to the Cervical Spine After a Car Accident?
Picture your neck as a tower of Jenga blocks carefully stacked to keep everything in place. Now, imagine a car rear-ending you, sending those blocks wobbling like a bad game night. Whiplash is a rapid back-and-forth motion of the neck that occurs in approximately 1 million car accidents annually in the U.S., costing society up to $29 billion and affecting individuals’ socio-economic lifestyles. Whiplash doesn’t just give you a sore neck; it can seriously mess with the ligaments that hold your cervical spine together.
The Anatomy of Your Neck
The seven vertebrae in the cervical spine are cushioned by discs and held together by ligaments, which are the anterior longitudinal ligament, posterior longitudinal ligament, capsular ligaments, interspinous ligaments, supraspinous ligaments, and ligamentum flavum. These ligaments are like the seatbelts of your spine, keeping everything secure. However, in a crash, the sudden force, ranging from 3.5 to 8 g’s in a rear-end collision, can stretch or tear these ligaments, thereby reducing their strength. A study found that whiplash decreases the force required for ligament failure by approximately 20% (149.4 N vs. 186.0 N) and energy absorption by roughly 22% (308.6 J vs. 397.0 J). (Tominaga et al., 2006). This damage can lead to cervical instability, where your neck becomes as wobbly as a bobblehead on a dashboard.
The Whiplash Effect
Whiplash is like your neck trying to do an impromptu dance move it wasn’t prepared for. The rapid motion overstretches ligaments beyond their normal range, sometimes causing micro tears or complete ruptures. This instability can lead to chronic pain, stiffness, and even more complex issues down the road, like Thoracic Outlet Syndrome. It’s as if your neck says, “I’m done holding it together!” and passes the problem to other parts of your body. It’s like a disaster with the neck and ligaments, which is no laughing matter, as it can significantly impact your daily life, from simply turning your head to lifting your arms.
Can Ligament Damage Cause Thoracic Outlet Syndrome?
Now, let’s discuss Thoracic Outlet Syndrome, or TOS, which may sound like something you’d find in a haunted mansion, but it is, in fact, a medical condition. TOS happens when the nerves or blood vessels in the thoracic outlet—the narrow space between your collarbone and first rib get compressed, causing pain, numbness, or tingling in your arms and hands, making you feel like your limbs are staging a protest. But how does a neck injury from a car crash lead to this?
The Connection Between Whiplash and TOS
When your cervical spine ligaments are damaged, they can’t hold the vertebrae as tightly, leading to instability or misalignment. This can affect nearby structures, like the scalene muscles in your neck, which are part of the thoracic outlet. Inflammation or scar tissue from the injury can further narrow this space, squeezing the brachial plexus nerves or subclavian vessels. A study found that 30 out of 35 whiplash patients had thoracic outlet syndrome (TOS), confirmed by slowed ulnar nerve conduction velocity, suggesting a direct link. (Sanders et al., 2007) It’s like your neck’s injury sends a ripple effect, turning the thoracic outlet into a crowded subway station where nerves and vessels get squished.
Types of TOS
TOS comes in three flavors:
Neurogenic TOS: The most common (95% of cases), where nerves like the brachial plexus are compressed, causing arm pain and numbness.
Venous Thoracic Outlet Syndrome (TOS): Affects veins, leading to swelling or thrombosis in approximately 5% of cases.
Arterial TOS: The rarest (1%) form involves compression of the artery, which can cause issues with blood flow.
Whiplash typically leads to neurogenic thoracic outlet syndrome (TOS) due to nerve compression from damaged muscles or ligaments. It’s like imagining the nerves are trapped in a dark, cramped corridor, crying out for freedom!
Why It Happens
In a car accident, trauma can damage or injure the scalene muscles, causing inflammation and narrowing of the thoracic outlet. Cervical instability may also alter your posture, causing your shoulders to shift forward and compress the outlet further. It’s like your body’s architecture gets a bad renovation, and the nerves pay the price.
What Is Thoracic Outlet Syndrome?- Video
Understanding TOS Symptoms After Whiplash Injuries
So, what does TOS feel like? If you’ve been in a car crash and now your arms feel like they’re buzzing with static or aching like you’ve been arm-wrestling Uncle Fester from the Addams Family, TOS might be to blame. Let’s break down the symptoms and why they happen.
Symptoms of TOS
Pain in the neck, shoulder, or arm.
Numbing/Tingling sensation in the arms or hands, especially the ring and pinky fingers.
Muscle Weakness in the upper extremities
Swelling or Discoloration: In venous TOS, your arm might swell or turn blue.
These symptoms arise because the brachial plexus nerves, which carry signals from your spine to your arms, are compressed. (Cavanna et al., 2022) This is akin to a traffic jam on the nerve highway, where signals become stuck, causing pain or sensory changes.
Acute vs. Chronic Symptoms
In the acute phase (within 3.5 months post-accident), neck pain might dominate, with TOS symptoms being mild. But in chronic cases (over 2 years), TOS symptoms like arm pain and numbness can become the main issue. This is why early treatment is crucial, and when individuals ignore the pain associated with TOS, it is like neglecting a creaky floorboard in the Addams Family mansion; it only worsens over time.
Pathophysiology of Nerve Pain
When the brachial plexus is compressed, it disrupts nerve signals, leading to pain, tingling, or weakness. The capsular ligaments, which contain sensory nerves, can also be injured, contributing to chronic pain. Studies show that nerve blocks or radiofrequency ablation can relieve this pain, confirming the link between nerve compression. (Li et al., 2021) It’s as if your nerves are sending SOS signals, but the message gets garbled.
How Dr. Alexander Jimenez Helps MVA Victims in El Paso
In El Paso, Dr. Alexander Jimenez is like the Lurch of injury recovery—big on expertise and always there to help. As a chiropractor and family nurse practitioner, he brings a unique blend of holistic and evidence-based care to MVA victims. His clinic specializes in treating whiplash, back pain, and conditions such as thoracic outlet syndrome (TOS), utilizing functional medicine and advanced therapies to restore mobility and alleviate pain.
Integrative Care Approach
Dr. Jimenez’s dual licensure allows him to combine chiropractic adjustments with medical interventions, addressing both the structural and physiological aspects of injuries. His team, including chiropractors, nurse practitioners, and nutritionists, creates personalized treatment plans. For example, they might use chiropractic adjustments to correct spinal misalignment, physical therapy to strengthen muscles, and nutritional guidance to reduce inflammation. This integrative approach is like a well-orchestrated dance, as everyone works together for a flawless performance.
Supporting Legal and Medical Needs
Dr. Jimenez excels at correlating soft tissue and spinal injuries for personal injury attorneys and healthcare teams. By thoroughly documenting injuries through clinical evaluations and imaging, he ensures that the link between the MVA and symptoms, such as TOS, is clear. This is vital for legal claims, as it proves the accident caused the injury. His clinic’s focus on spine health and pain management makes him a trusted provider in El Paso.
Treatment Options
Some treatments offered include:
Chiropractic Adjustments: To realign the spine through mechanical and manual manipulation and reduce nerve compression.
Physical Therapy: Various exercises can help strengthen neck and shoulder muscles, improving stability. (Service, 2025)
Functional Medicine: Addressing inflammation and overall health to support recovery.
Pain Management: Techniques like nerve blocks or manual therapy to alleviate symptoms.
Dr. Jimenez’s approach helps to tinker with the body with a creative, precise, and effective method to promote health and wellness to the individual.
Documenting Ligamentous Injuries for Personal Injury Claims
Documenting injuries after an MVA is like keeping a detailed diary in the household. You need to record every creak and groan to understand the full story, as accurate documentation is essential for treatment and legal purposes.
Why Documentation Matters
Medical Treatment: Identifying ligament tears or instability through MRI or dynamic X-rays guides treatment, ensuring you receive the appropriate care, such as physical therapy or surgery, as needed.
Legal Claims: Proving that the accident caused your injuries is crucial for insurance claims or lawsuits. Detailed records link symptoms like TOS to the MVA.
Preventing Misdiagnosis: TOS is often misdiagnosed due to its vague symptoms. Proper documentation helps differentiate it from conditions like cervical radiculopathy.
How to Document
Clinical Evaluation: A thorough examination conducted by a healthcare provider, such as Dr. Jimenez, can identify signs of ligament damage or thoracic outlet syndrome (TOS).
Nerve Studies: Tests such as ulnar nerve conduction velocity can confirm thoracic outlet syndrome (TOS). (Hanif et al., 2007)
Medical Records: Detailed notes on symptoms, timeline, and treatments strengthen your case.
Without this, it’s like trying to convince people there’s no ghost in the attic. (Archie & Rigberg, 2017)
Challenges in Documentation
TOS is tricky to diagnose because its symptoms overlap with other conditions, like cervical disc disease. Studies note that TOS lacks standardized tests, making clinical expertise crucial. (Wang et al., 2019) Providers like Dr. Jimenez bridge this gap by combining clinical insight with diagnostic tools.
A Serious Note on Recovery
Auto accidents can have a negative impact on your quality of life, in addition to causing damage to your vehicle. After an MVA, don’t dismiss any neck discomfort, arm numbness, or weakness as a bad day; get care right away. Serious disorders, such as cervical instability or TOS, which may develop if left untreated, may be indicated by these symptoms. Seek treatment from a reputable physician, such as Dr. Alexander Jimenez, who can compassionately and expertly assist you in your recuperation. Thoroughly documenting your injuries can aid in your treatment and ensure that you have the necessary evidence to support any future legal claims. You should be able to return to your life without suffering and with confidence.
Injury Medical Chiropractic & Personal Injury Clinic
We associate certified medical providers who understand the importance of assessing individuals experiencing TOS (thoracic outlet syndrome) associated with an auto accident. When asking important questions to our associated medical providers, we advise patients to incorporate customized treatment plans for reducing the overlapping risk profiles of TOS correlated with being involved in an auto accident to promote speedy recovery. Dr. Alex Jimenez, D.C., utilizes this information as a professional academic service. Disclaimer
Cavanna, A. C., Giovanis, A., Daley, A., Feminella, R., Chipman, R., & Onyeukwu, V. (2022). Thoracic outlet syndrome: a review for the primary care provider. Journal of Osteopathic Medicine, 122(11), 587-599. https://doi.org/10.1515/jom-2021-0276
Hanif, S., Tassadaq, N., Rathore, M. F., Rashid, P., Ahmed, N., & Niazi, F. (2007). Role of therapeutic exercises in neurogenic thoracic outlet syndrome. J Ayub Med Coll Abbottabad, 19(4), 85-88. https://www.ncbi.nlm.nih.gov/pubmed/18693607
Li, N., Dierks, G., Vervaeke, H. E., Jumonville, A., Kaye, A. D., Myrcik, D., Paladini, A., Varrassi, G., Viswanath, O., & Urits, I. (2021). Thoracic Outlet Syndrome: A Narrative Review. Journal of Clinical Medicine, 10(5), 962. https://doi.org/10.3390/jcm10050962
Sanders, R. J., Hammond, S. L., & Rao, N. M. (2007). Diagnosis of thoracic outlet syndrome. Journal of Vascular Surgery, 46(3), 601-604. https://doi.org/10.1016/j.jvs.2007.04.050
Tominaga, Y., Ndu, A. B., Coe, M. P., Valenson, A. J., Ivancic, P. C., Ito, S., Rubin, W., & Panjabi, M. M. (2006). Neck ligament strength is decreased following whiplash trauma. BMC Musculoskelet Disord, 7, 103. https://doi.org/10.1186/1471-2474-7-103
Wang, X. T., Yao, M., Zhong, M., Wang, Y. J., Shi, Q., & Cui, X. J. (2019). Thoracic outlet syndrome in a postoperative cervical spondylotic myelopathy patient: A case report. Medicine (Baltimore), 98(11), e14806. https://doi.org/10.1097/MD.0000000000014806
Comprehensive Guide to Ligamentous Injuries and Sciatica from Motor Vehicle Accidents
Introduction to Ligamentous Injuries from Motor Vehicle Accidents
Motor vehicle accidents (MVAs) are a significant cause of injuries worldwide, often resulting in damage to ligaments, the tough, fibrous tissues that connect bones and stabilize joints. These ligamentous injuries, commonly referred to as sprains, occur when ligaments are overstretched or torn due to the sudden, forceful movements experienced during a crash. Understanding these injuries is critical for victims seeking recovery and, often, legal compensation.
What Are Ligamentous Injuries?
Ligaments provide structural support to joints, ensuring stability during movement. In MVAs, the rapid acceleration and deceleration forces can strain or tear ligaments, leading to sprains. These injuries vary in severity:
Mild sprains: Slight stretching of the ligament, causing minor pain and swelling.
Moderate sprains: Partial tearing, resulting in more significant pain and reduced joint function.
Severe sprains: Complete ligament tears, leading to joint instability and prolonged recovery.
Common sites for ligamentous injuries in motor vehicle accidents (MVAs) include the cervical spine (neck), lumbar spine (lower back), knees, and shoulders. A well-known example is whiplash, where the ligaments in the neck are strained due to rapid back-and-forth motion (Pinder Plotkin LLC, 2019). Symptoms typically include pain, swelling, bruising, and limited range of motion, which can significantly impact daily activities.
Mechanisms of Injury in MVAs
MVAs generate immense forces that jolt the body, often causing it to collide with vehicle components, such as seatbelts, dashboards, or steering wheels. For instance:
Whiplash: Rear-end collisions thrust the head and neck backward and then forward, straining cervical ligaments. This can lead to chronic pain if untreated (Pinder Plotkin LLC, 2019).
Lower Back Injuries: The force of an impact can compress or twist the lumbar spine, damaging ligaments and potentially leading to conditions like herniated discs.
Knee and Shoulder Injuries: Impact with dashboards or sudden twisting can tear ligaments, such as the posterior cruciate ligament (PCL) in the knee or the rotator cuff ligaments in the shoulder (Applied Radiology, 2018).
According to HG.org (n.d.), soft tissue injuries, including ligament damage, are more common than severe injuries like fractures in MVAs due to the body’s susceptibility to being jolted or twisted. These injuries may not be immediately apparent, with symptoms sometimes appearing days or weeks later, which reinforces the importance of prompt medical evaluation.
Symptoms and Complications
Ligamentous injuries present with a range of symptoms, including:
Pain and Tenderness: Localized discomfort around the affected joint.
Swelling and Inflammation: Resulting from tissue damage and fluid accumulation.
Bruising: Visible discoloration from blood vessel damage.
Reduced Mobility: Difficulty moving the joint due to pain or instability.
Joint Instability: In severe cases, the joint may feel loose or unable to support weight.
If untreated, these injuries can lead to complications such as chronic pain, osteoarthritis, or long-term joint instability. For example, spinal ligament damage can contribute to disc degeneration or misalignment, thereby increasing the risk of nerve-related conditions, such as sciatica (Pinder Plotkin LLC, 2019).
References
Pinder Plotkin LLC. (2019, December 20). What is ligamentous instability and how does it relate to car accidents? What is Ligamentous Instability
Applied Radiology. (2018, January 18). Understanding types of injuries caused by motor vehicle components. Injuries from Vehicle Components
Connection Between Ligamentous Injuries and Sciatica
Sciatica is a debilitating condition characterized by pain, numbness, or tingling that radiates along the sciatic nerve, which extends from the lower back through the hips, buttocks, and down each leg. While ligamentous injuries from MVAs may not always directly cause sciatica, they can contribute to spinal conditions that compress or irritate the sciatic nerve, which leads to this painful condition.
Understanding Sciatica
The sciatic nerve is the longest and thickest nerve in the body, originating from the lumbar and sacral nerve roots (L4-S3) and controlling leg movement and sensation. Sciatica, also known as lumbar radiculopathy, occurs when this nerve or its roots are compressed or irritated, causing symptoms such as:
A sharp or burning pain radiates from the lower back to the leg.
The leg or foot may experience numbness or tingling.
Weakness in the affected leg impacts mobility.
Sitting, coughing, or sneezing exacerbates the pain.
Sciatica is typically unilateral, affecting one side of the body, and can range from mild discomfort to severe, debilitating pain (Michigan Auto Law, 2024).
How MVA Injuries Lead to Sciatica
MVAs can cause spinal trauma that precipitates sciatica. Ligamentous injuries in the lumbar spine may destabilize the vertebral column, leading to conditions that compress the sciatic nerve roots. Common mechanisms include:
Herniated Discs: The force of an MVA can cause the gel-like center of a spinal disc to bulge or rupture, pressing on nearby nerve roots. This is a leading cause of sciatica following an accident (Tracey Fox & Walters, n.d.).
Spinal Instability: Damaged ligaments may fail to maintain proper alignment of the vertebrae, causing abnormal motion that irritates nerves (Pinder Plotkin LLC, 2019).
Pelvic or Lumbar Fractures: Fractures from high-impact crashes can result in bone fragments or swelling that compress the sciatic nerve (Portland Urgent Care, 2024).
Soft Tissue Swelling: Inflammation from ligament injuries can encroach on nerve pathways, contributing to sciatica symptoms.
For example, a case study described by Portland Urgent Care (2024) highlighted a patient who developed sciatica after an MVA due to a herniated disc at the L5-S1 level, confirmed by MRI. Another case involved pelvic fractures causing nerve compression, illustrating the diverse ways MVAs can trigger sciatica.
Prevalence and Risk Factors
While exact statistics on sciatica following MVAs are limited, research suggests that back injuries, including those affecting ligaments and discs, are common in car accidents. Individuals with pre-existing conditions like spinal stenosis or prior back injuries are at higher risk of developing sciatica post-MVA (Tracey Fox & Walters, n.d.). Prompt diagnosis and treatment are essential to prevent chronic pain and long-term disability.
References
Michigan Auto Law. (2024, July 1). Sciatica nerve damage from car accident: Here’s what to know. Sciatica Nerve Damage
Portland Urgent Care. (2024, April 19). Can a car accident cause sciatica pain? Causes, symptoms & treatment for sciatic nerve pain after an accident. Sciatica Pain After Accident
Pinder Plotkin LLC. (2019, December 20). What is ligamentous instability and how does it relate to car accidents? What is Ligamentous Instability
Dr. Alexander Jimenez: Expert in Personal Injury Cases
In El Paso, TX, Dr. Alexander Jimenez stands out as a leading provider for victims of personal injuries, particularly those from MVAs. His unique qualifications as both a chiropractor and a board-certified family nurse practitioner (FNP-BC) enable him to provide comprehensive care that addresses both immediate pain and long-term recovery needs.
Background and Qualifications
Dr. Jimenez has over 25 years of experience, having graduated from the National University of Health Sciences in 1991. He holds additional certifications in functional medicine (IFMCP, CFMP) and is affiliated with The Hospitals of Providence-Memorial Campus. His dual licensure enables him to integrate chiropractic expertise with medical diagnostics and treatments, making him uniquely qualified to manage complex injuries related to motor vehicle accidents (Medical News Today, n.d.). Patient reviews consistently rate him 5.0 out of 5, praising his ability to explain conditions clearly and provide trustworthy care (Healthgrades, n.d.).
Services at El Paso Back Clinic
At his Injury Medical & Chiropractic Clinic, Dr. Jimenez specializes in treating conditions such as:
Sciatica
Neck and back pain
Whiplash
Joint injuries
Sports injuries
Degenerative arthritis
His clinic utilizes advanced therapies, including chiropractic adjustments, functional medicine assessments, acupuncture, and electroacupuncture, to restore mobility and promote overall health. The clinic’s integrative approach focuses on addressing the root causes of pain, rather than just its symptoms, to ensure optimal recovery (El Paso Back Clinic, n.d.).
Approach to MVA Injuries and Sciatica
Dr. Jimenez’s treatment protocols are tailored to each patient’s needs, combining non-invasive chiropractic techniques with medical interventions. For MVA victims, he focuses on:
Restoring Mobility: Through chiropractic adjustments and mobility training.
Reducing Inflammation: Using functional medicine and acupuncture to address soft tissue damage.
Preventing Chronic Pain: By addressing injuries early to avoid complications like sciatica.
His ability to order and interpret diagnostic tests, such as MRIs, enhances his capacity to develop evidence-based treatment plans, which are critical for both recovery and legal documentation (A4M, n.d.).
References
Medical News Today. (n.d.). Dr. Alexander Jimenez, DC: Chiropractor – El Paso, TX. Dr. Jimenez Profile
Healthgrades. (n.d.). Dr. Alexander Jimenez, DC – Chiropractor in El Paso, TX. Dr. Jimenez Healthgrades
El Paso Back Clinic. (n.d.). Dr. Alex Jimenez – Doctor of Chiropractic | El Paso, TX Back Clinic. About Dr. Jimenez
A4M. (n.d.). Injury Medical & Chiropractic Clinic – Alex, Jimenez DC, APRN, FNP-BC, CFMP, IFMCP. Integrative Care by Dr. Jimenez
Advanced Diagnostic and Treatment Methods
Dr. Jimenez’s approach to treating MVA-related injuries, including those that cause sciatica, relies on advanced diagnostic tools and a dual-scope intervention strategy that leverages his expertise in both chiropractic and medical care.
Enhanced Imaging and Diagnostic Assessments
Accurate diagnosis is critical for effective treatment and legal documentation in personal injury cases. Dr. Jimenez employs:
X-rays: To identify fractures or misalignments in the spine or joints.
Magnetic Resonance Imaging (MRI): To detect soft tissue injuries, such as herniated discs or ligament tears, that may contribute to sciatica (Michigan Auto Law, 2024).
Computed Tomography (CT) Scans: For detailed imaging of complex injuries.
Physical Examinations: Comprehensive assessments to evaluate range of motion, pain levels, and neurological function.
These tools enable Dr. Jimenez to accurately assess the extent of ligamentous damage and nerve involvement, ensuring the development of precise treatment plans. For example, an MRI can confirm a herniated disc causing sciatica, guiding targeted interventions (Portland Urgent Care, 2024).
Dual-Scope Interventions
Dr. Jimenez’s dual licensure enables a unique treatment approach:
Chiropractic Care: Adjustments to correct spinal misalignments, reduce nerve pressure, and restore mobility. The procedure is particularly effective for whiplash and sciatica caused by spinal issues.
Medical Interventions: As an FNP-BC, he can prescribe medications, administer corticosteroid injections, or recommend surgical consultations if necessary.
Functional Medicine Addresses underlying factors, such as inflammation or nutritional deficiencies, to support long-term healing.
Rehabilitation Programs: Include physical therapy, acupuncture, and mobility training to enhance recovery and prevent chronic pain.
This integrative approach ensures comprehensive care, addressing both immediate symptoms and underlying causes. For instance, a patient with sciatica resulting from a motor vehicle accident (MVA) might receive chiropractic adjustments to relieve nerve pressure, alongside injections to reduce inflammation (A4M, n.d.).
Importance in Personal Injury Cases
The detailed diagnostic reports generated from these assessments are invaluable for personal injury claims. They provide objective evidence of injury severity, which is crucial for securing fair compensation. Dr. Jimenez’s ability to interpret and document findings bridges the gap between medical care and legal proceedings (Personal Injury Doctor Group, 2017).
References
Michigan Auto Law. (2024, July 1). Sciatica nerve damage from car accident: Here’s what to know. Sciatica Nerve Damage
Portland Urgent Care. (2024, April 19). Can a car accident cause sciatica pain? Causes, symptoms & treatment for sciatic nerve pain after an accident. Sciatica Pain After Accident
A4M. (n.d.). Injury Medical & Chiropractic Clinic – Alex, Jimenez DC, APRN, FNP-BC, CFMP, IFMCP. Integrative Care by Dr. Jimenez
Personal Injury Doctor Group. (2017, May 22). Personal injury doctor | El Paso, TX | Dr. Alex Jimenez D.C. Personal Injury Doctor
Role in Personal Injury Cases
Dr. Jimenez’s expertise is particularly valuable in the context of personal injury cases, where accurate medical documentation and effective treatment are essential for both recovery and legal outcomes.
Medical Documentation for Legal Purposes
In personal injury cases, detailed medical reports are critical for proving the extent of injuries and securing compensation. Dr. Jimenez’s dual qualifications allow him to produce comprehensive documentation that includes:
Diagnostic Findings: Results from X-rays, MRIs, or CT scans that confirm injuries like ligament tears or herniated discs.
Treatment Plans: Detailed descriptions of interventions, from chiropractic adjustments to medical therapies, demonstrating the care required.
Prognosis and Impact: Assessments of long-term effects, such as chronic pain or disability, influence the amounts of compensation.
These reports are often used by attorneys and insurance companies to evaluate claims, making Dr. Jimenez an essential intermediary between medical care and legal proceedings (Personal Injury Doctor Group, 2017).
Supporting Recovery and Compensation
Dr. Jimenez’s treatment plans not only aid physical recovery but also strengthen legal cases by demonstrating the need for ongoing care. For example, a patient with sciatica resulting from a motor vehicle accident (MVA) may require months of rehabilitation, which Dr. Jimenez can document to support claims for medical expenses and lost wages. His clinic collaborates with legal professionals to ensure patients receive fair compensation (El Paso Back Clinic, n.d.).
Testimonials and Community Impact
Patients consistently praise Dr. Jimenez for his compassionate and effective care. On LinkedIn, he is described as a “true blessing to the El Paso community” for his dedication to patient recovery (LinkedIn, 2025). His clinic’s focus on integrative care has helped numerous MVA victims regain their health and navigate the complexities of personal injury claims.
References
Personal Injury Doctor Group. (2017, May 22). Personal injury doctor | El Paso, TX | Dr. Alex Jimenez D.C. Personal Injury Doctor
El Paso Back Clinic. (n.d.). Dr. Alex Jimenez – Doctor of Chiropractic | El Paso, TX Back Clinic. About Dr. Jimenez
LinkedIn. (2025, February 26). Dr. Alexander Jimenez DC, APRN, FNP-BC, IFMCP, CFMP, ATN. Dr. Jimenez LinkedIn
Conclusion
Ligamentous injuries from MVAs, such as whiplash or lumbar sprains, can have significant consequences, including the potential to cause sciatica through nerve compression or spinal instability. Dr. Alexander Jimenez, with his extensive experience and dual qualifications, offers a lifeline for El Paso residents affected by these injuries. His use of advanced imaging, comprehensive diagnostics, and integrative treatment approaches ensures effective recovery while providing critical documentation for personal injury claims. For anyone involved in a motor vehicle accident (MVA), seeking prompt care from a provider like Dr. Jimenez is essential to address injuries, prevent complications, and secure fair compensation. Contact his clinic at (915) 850-0900 or visit El Paso Back Clinic to start your recovery journey.
Key Citations
Pinder Plotkin LLC. (2019, December 20). What is ligamentous instability and how does it relate to car accidents? What is Ligamentous Instability
Portland Urgent Care. (2024, April 19). Can a car accident cause sciatica pain? Causes, symptoms & treatment for sciatic nerve pain after an accident. Sciatica Pain After Accident
Medical News Today. (n.d.). Dr. Alexander Jimenez, DC: Chiropractor – El Paso, TX. Dr. Jimenez Profile
Healthgrades. (n.d.). Dr. Alexander Jimenez, DC – Chiropractor in El Paso, TX. Dr. Jimenez Healthgrades
El Paso Back Clinic. (n.d.). Dr. Alex Jimenez – Doctor of Chiropractic | El Paso, TX Back Clinic. About Dr. Jimenez
A4M. (n.d.). Injury Medical & Chiropractic Clinic – Alex, Jimenez DC, APRN, FNP-BC, CFMP, IFMCP. Integrative Care by Dr. Jimenez
Personal Injury Doctor Group. (2017, May 22). Personal injury doctor | El Paso, TX | Dr. Alex Jimenez D.C. Personal Injury Doctor
LinkedIn. (2025, February 26). Dr. Alexander Jimenez DC, APRN, FNP-BC, IFMCP, CFMP, ATN. Dr. Jimenez LinkedIn
Get insights into back problems, fender bender symptoms, and effective ways to address your discomfort and promote healing.
Introduction
Even though a fender accident may not seem like much, the upper, middle, and lower parts of the back can be severely damaged by the unexpected shock. Injuries from even minor incidents may result in chronic pain and suffering. Do you experience back discomfort when twisting and turning due to stiffness? Do you find that moving your extremities helps to reduce tingling or numbness sensations? Or do you get recurring headaches that force you to lie down in bed? Following a fender-bender collision, these situations are often associated with a range of pain-like sensations. With a particular emphasis on the role that chiropractic care plays in many people’s recovery, today’s post will examine the five main back issues that may develop after a vehicle accident, along with their symptoms and effective non-surgical solutions.
Whiplash-Associated Disorders
Whiplash, in which the neck and upper back are violently wrenched back and forth quickly like a whip, is one of the most frequent injuries sustained in rear-end or front-end crashes. (Stroke, 2023) People experience pain and suffering as a consequence of the tension on their muscles, ligaments, and soft tissues.
Symptoms
Pain or stiffness in the upper back and neck
Decreased range of motion
A headache
Arm tingling or discomfort in the shoulders
Weariness or lightheadedness
Non-Surgical Treatments
Chiropractic Care: To alleviate stress and increase mobility, chiropractors use mild spinal adjustments to realign the cervical and thoracic spine. Chiropractors employ a range of techniques, including soft tissue treatment and spinal manipulation, to help alleviate pain and promote back recovery.
Physical therapy: To assist regain flexibility and avoid stiffness, people may do a variety of stretching and strengthening activities.
Ice and Heat Therapy: While heat helps loosen tense muscles, cold packs first minimize inflammation.
Pain management: Ibuprofen and other over-the-counter anti-inflammatory medications may be used to help control pain.
Because it corrects misalignments that may be causing discomfort and limited mobility, chiropractic therapy is particularly beneficial for whiplash, offering a drug-free approach to recovery.
Lumbar Sprains & Strains
The lower back (lumbar spine) is vulnerable to sprains (ligament injuries) and strains (muscle or tendon injuries) during a collision. The sudden impact can overstretch or tear these tissues, leading to acute pain.
Symptoms
Lower back pain that worsens with movement
Muscle spasms or cramping
Stiffness or difficulty standing upright
Pain radiating to the buttocks or thighs
Non-Surgical Treatments
Chiropractic Care: Chiropractors perform lumbar adjustments to correct spinal misalignments and relieve pressure on affected tissues. They may also employ techniques such as myofascial release to reduce muscle tension.
Rest and Activity Modification: Short-term rest followed by gradual reintroduction of movement prevents stiffness.
Therapeutic Exercises: Core-strengthening exercises, guided by a professional, stabilize the lower back. (Quentin et al., 2021)
Massage Therapy: This complements chiropractic care by relaxing tight muscles and improving circulation.
Chiropractic adjustments help restore proper spinal function, reducing pain and preventing chronic issues from developing in the lumbar region.
Herniated Discs
Herniated discs can happen when the soft inner portion of the spinal disc bulges through its outer portion within the spine. (Jin et al., 2023) Individuals involved in an auto collision may experience herniated discs due to the compressive forces, which can cause irritation to nearby nerves and lead to significant discomfort.
Symptoms
Sharp or burning pain in the back
Numbing or tingling sensations in the upper and lower extremities
Weakness in the affected area
Pain that worsens with sitting, bending, or coughing
Non-Surgical Treatments
Chiropractic Care: Chiropractors use non-invasive techniques, such as spinal decompression and gentle adjustments, to reduce pressure on the affected disc and nerves. These methods aim to reposition the disc and improve spinal alignment.
Epidural Steroid Injections: These can reduce inflammation around the nerve roots.
Physical Therapy: Exercises improve spinal stability and reduce strain on the disc.
Lifestyle Modifications: Avoiding activities that aggravate the injury, such as heavy lifting, supports healing.
Chiropractic care is a cornerstone of herniated disc treatment, as it focuses on restoring spinal mechanics without surgery, often providing significant relief from symptoms.
Facet Joint Injuries
Facet joints, which connect the vertebrae, can become irritated or injured during a fender bender, especially in side-impact crashes. (Du et al., 2022) This can lead to localized pain and restricted movement.
Symptoms
Localized back pain, often on one side
Pain that worsens with twisting or bending
Tenderness when pressing on the affected area
Stiffness in the spine
Non-Surgical Treatments
Chiropractic Care: Chiropractic adjustments target the facet joints to restore proper motion and reduce inflammation. Mobilization techniques can also alleviate stiffness.
Anti-inflammatory medications help manage pain and swelling.
Chiropractors excel at treating facet joint injuries by realigning the spine back to its neutral position and improving joint function, which can significantly reduce pain and restore mobility.
Thoracic Spine Injuries
The mid-back (thoracic spine) is less commonly injured due to its stability. However, a fender bender can still cause sprains, strains, or misalignments in this region, especially if the torso twists during impact.
Symptoms
Mid-back pain or aching
Stiffness when rotating the torso
Radiating chest pain in the ribs
Difficulty taking deep breaths
Non-Surgical Treatments
Chiropractic Care: Adjustments to the thoracic spine correct misalignments and improve joint mobility. Chiropractors can also incorporate soft tissue techniques, such as MET (muscle energy technique therapy), to address muscle tension.
Breathing Exercises: These help maintain rib cage mobility and reduce discomfort.
Postural Exercises: Strengthening the upper back prevents further strain. (Dareh-Deh et al., 2022)
TENS Therapy: Electrical stimulation therapy can reduce pain by interrupting nerve signals. (Teoli et al., 2025)
Chiropractic care is highly effective for thoracic injuries, as chiropractors can assess the root cause of pain and spinal misalignments while promoting natural healing and recovery.
Why Choose Chiropractic?- Video
The Power of Chiropractic Care
Chiropractic care stands out as a safe, non-invasive, and effective treatment for back problems after a fender bender. By focusing on spinal alignment, joint function, and soft tissue health, chiropractors address the underlying causes of pain rather than just masking symptoms. (Stephen Dies, 1992) Regular chiropractic visits can:
Reduce pain and inflammation
Restore range of motion
Prevent chronic pain by addressing injuries early
Support overall spinal health
Unlike surgical options, chiropractic care requires no downtime and avoids the overlapping risk profiles associated with invasive procedures. It’s also customizable, with chiropractors tailoring treatments to each patient’s specific injuries and needs.
When to Seek Care
If you experience back pain, stiffness, or other symptoms after a fender bender, don’t wait to seek treatment. Early intervention from auto collisions can help prevent minor injuries from developing into chronic conditions. Consult a chiropractor or healthcare provider for a thorough evaluation, which may include various imaging tests (such as X-rays or MRIs) to assess the extent of the injury that the body has sustained.
Conclusion
From whiplash to herniated discs, a fender accident may cause a variety of back issues. However, there is a way to heal with non-surgical therapies, especially chiropractic therapy. People can restore their mobility and enhance their quality of life by using spinal adjustments, therapeutic exercises, and complementary treatments to alleviate symptoms such as pain, stiffness, and numbness. If you have been in an automobile accident, it is crucial that you put your spinal health first and consider chiropractic adjustments as a vital component of your recovery.
Injury Medical Chiropractic & Personal Injury Clinic
We associate certified medical providers who understand the importance of assessing individuals with back pain associated with a fender bender collision. When asking important questions to our associated medical providers, we advise patients to incorporate customized treatment plans for their back pain correlated with being involved in an auto accident to promote speedy recovery. Dr. Alex Jimenez, D.C., utilizes this information as a professional academic service. Disclaimer
References
Dareh-Deh, H. R., Hadadnezhad, M., Letafatkar, A., & Peolsson, A. (2022). Therapeutic routine with respiratory exercises improves posture, muscle activity, and respiratory pattern of patients with neck pain: a randomized controlled trial. Sci Rep, 12(1), 4149. https://doi.org/10.1038/s41598-022-08128-w
Du, R., Xu, G., Bai, X., & Li, Z. (2022). Facet Joint Syndrome: Pathophysiology, Diagnosis, and Treatment. J Pain Res, 15, 3689-3710. https://doi.org/10.2147/JPR.S389602
Jin, Y. Z., Zhao, B., Zhao, X. F., Lu, X. D., Fan, Z. F., Wang, C. J., Qi, D. T., Wang, X. N., Zhou, R. T., & Zhao, Y. B. (2023). Lumbar Intradural Disc Herniation Caused by Injury: A Case Report and Literature Review. Orthop Surg, 15(6), 1694-1701. https://doi.org/10.1111/os.13723
Quentin, C., Bagheri, R., Ugbolue, U. C., Coudeyre, E., Pelissier, C., Descatha, A., Menini, T., Bouillon-Minois, J. B., & Dutheil, F. (2021). Effect of Home Exercise Training in Patients with Nonspecific Low-Back Pain: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health, 18(16). https://doi.org/10.3390/ijerph18168430
Stephen Dies, J. W. S. (1992). Chiropractic treatment of patients in motor vehicle accidents: a statistical analysis †. J Can Chiropr Assoc., 36(3), 139-145. https://pmc.ncbi.nlm.nih.gov/articles/PMC2484939/
Torres-Pareja, M., Sanchez-Lastra, M. A., Iglesias, L., Suarez-Iglesias, D., Mendoza, N., & Ayan, C. (2019). Exercise Interventions for Improving Flexibility in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Medicina (Kaunas, Lithuania), 55(11). https://doi.org/10.3390/medicina55110726
How can one effectively manage the early signs of bunions?
Bunions
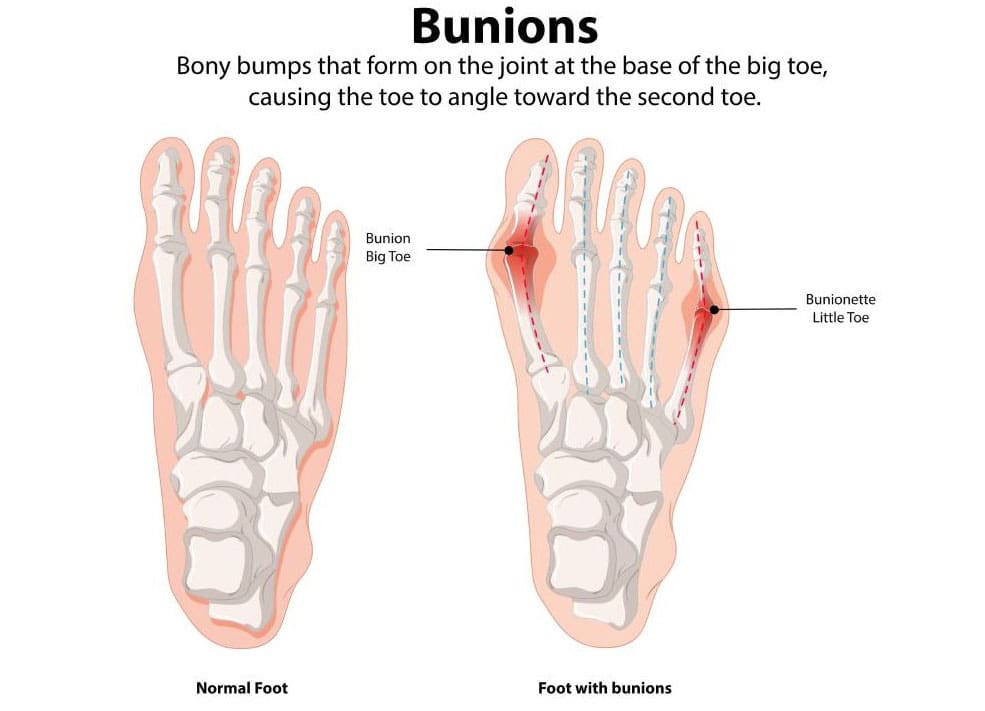
A bunion, also known as hallux valgus, is a bony, often painful protrusion on the side of the big toe. The most common cause of bunions is a misalignment of the big toe. Early symptoms of a bunion include redness, thicker skin, edema, and discomfort around the big toe joint. While you can’t stop a bunion from growing, you can manage the symptoms along the way. Early indicators of bunions include pain management measures and treatment choices. (MedlinePlus, 2024)
Early Visual Signs
Bunions are initially minor and don’t result in many noticeable issues. The following symptoms may be present in the early stages of a bunion around the metatarsophalangeal (MTP) joint, which joins the base of your big toe to the rest of your foot. (American Academy of Orthopaedic Surgeons, 2022)
Redness
Skin that is darker and swollen
Skin that has gotten thicker and harder
There is a bony bump
A bump where the big toe goes toward the second toe or even under it
Corns and calluses
Early Physical Signs
While bunions may not be visible immediately, they can cause discomfort even in the early stages. Here are some early physical indicators of a developing bunion. (MedlinePlus, 2024)
Pain in the foot and big toe
This pain is especially noticeable when walking or wearing tight, narrow-toed shoes.
Decreased movement of the big toe
Tenderness
Inflammation
Swelling
Stiffness
Heat
Stages
Bunions often worsen over time, a condition known as progressive. You could have problems if you don’t do anything to stop your bunions from getting bigger. Bunions in later stages might cause the following symptoms: (American Academy of Orthopaedic Surgeons, 2022)
Long-lasting, intense pain in and around the MTP joint and the sides and bottom of your foot
Bursitis causes a sac full of fluid to form at the bottom of your big toe.
The big toe bends toward and even crosses over the second toe.
Too much bone development on the side of your big toe
Not being able to wear your regular shoes
Hard to walk
Abnormalities known as “hammer toe” occur when your second, third, or fourth toes bend upward in the middle, resembling a hammer or claw.
Hallux rigidus is a form of arthritis affecting the big toe.
Manage the Progression
Bunions tend to remain in place once they start to develop. However, there are several steps you can take to prevent them from worsening or causing additional problems. These are some of them: (American Academy of Orthopaedic Surgeons, 2022)
Place spacers between your toes to prevent friction and chafing.
Use over-the-counter (OTC) pads made of felt, silicone, or foam to cover the bunion.
You should also stretch your calf muscles to improve joint alignment.
Managing Pain
Advil and Motrin (ibuprofen) are two examples of non-steroidal anti-inflammatory medicines (NSAIDs) that can aid with bunion pain. Studies also show that injecting Botox into the muscles in the forefoot can help with pain. (Hurn, S. E., et al., 2022)
Nonsurgical Early Stage Treatment
If your bunions continue to worsen despite using the self-care procedures listed above, you may need to consult a podiatrist (a foot expert) or another healthcare provider. A healthcare provider may recommend.
Orthotics, or foot orthoses
Foot orthoses, also known as orthotics, are customized inserts that help alleviate bunion pain and prevent chafing.
Splints
Bunion splints are orthotic devices that can help straighten out your toes. People typically use them at night. (Aebischer, A. S., & Duff, S. 2020)
Physical Therapy
A physical therapist can help you by giving you exercises that will help your feet and joints line up better. They might also do manual therapy to help with pain. (Hurn, S. E., et al., 2022)
Podiatrist
A podiatrist is a medical doctor (M.D.) who specializes in treating health problems that affect the feet, ankles, and lower legs. If you want help with your bunion issues, ask your doctor for a referral to a podiatrist. (American Podiatric Medical Association, 2025)
Chiropractic Treatment
Chiropractors and nurse practitioners (NPs) have distinct roles in managing bunions, which are bony bumps at the base of the big toe caused by joint misalignment, often resulting in pain, swelling, and restricted movement. Here’s how each can help:
Chiropractors:
Focus: Chiropractors primarily address musculoskeletal issues through manual adjustments and manipulations.
Bunion Support:
Foot Adjustments: They may perform adjustments to improve foot alignment and joint mobility, which can potentially reduce bunion-related discomfort.
Soft Tissue Therapy: Techniques such as massage or myofascial release can help alleviate tension in surrounding muscles and tissues.
Orthotics or Taping: Some chiropractors recommend custom orthotics or use taping to support proper foot mechanics.
Exercise Guidance: They may suggest stretches or exercises to strengthen foot muscles and improve alignment.
Limitations: Chiropractors don’t prescribe medications or perform surgeries, so severe cases requiring these interventions would need referral to a podiatrist or orthopedic specialist.
Evidence: While some patients report relief from chiropractic care for foot issues, evidence specifically for bunions is limited, and results vary.
Nurse Practitioners:
Focus: NPs are advanced practice registered nurses with broad medical training, able to diagnose, treat, and prescribe medications within their scope of practice.
Bunion Support:
Diagnosis and Assessment: NPs can evaluate bunion severity, often using physical examinations or ordering imaging, such as X-rays, to assess joint damage.
Pain Management: They may prescribe anti-inflammatory medications (e.g., ibuprofen) or corticosteroid injections for pain and swelling.
Conservative Treatments: NPs can recommend padding, splints, or orthotic devices to reduce pressure and improve alignment.
Lifestyle Advice: They provide guidance on footwear (such as wide-toed shoes) and weight management to reduce stress on the bunion.
Referrals: For severe cases, NPs can refer patients to podiatrists or orthopedic surgeons for surgical options, such as bunionectomies.
Scope: NPs offer a medical approach, bridging conservative care and coordination with specialists.
Key Differences:
Chiropractors focus on non-invasive, manual techniques and alignment, while NPs can incorporate medications and broader medical management.
NPs are more likely to coordinate with other healthcare providers for comprehensive care, whereas chiropractors tend to work more independently.
General Notes:
Both can assist in managing mild to moderate bunion symptoms, but neither can “cure” bunions, particularly if the structural deformity has progressed.
Consult a podiatrist or an orthopedic specialist for persistent or worsening symptoms, as severe cases may require surgical intervention.
Always verify the provider’s credentials and experience in treating bunions.
Injury Medical Chiropractic and Functional Medicine Clinic
Dr. Jimenez, a nurse practitioner, treats a wide range of conditions using a combination of medical knowledge and chiropractic care. The clinic offers personalized care plans that incorporate functional medicine, acupuncture, electroacupuncture, and sports medicine. The clinic treats chronic pain syndromes and injuries, focusing on strength, agility, and flexibility. Comprehensive care plans, when paired with in-person and virtual health coaching, offer personalized treatment and wellness outcomes for patients of all ages and abilities.
Enhance Your Performance with Functional Foot Orthotics
References
MedlinePlus (2024). Bunions. U.S. Department of Health and Human Services.
American Academy of Orthopaedic Surgeons. (2022). “Bunions.” OrthoInfo. from https://orthoinfo.aaos.org/en/diseases–conditions/bunions/.
Hurn, S. E., Matthews, B. G., Munteanu, S. E., & Menz, H. B. (2022). Effectiveness of Nonsurgical Interventions for Hallux Valgus: A Systematic Review and Meta-Analysis. Arthritis care & research, 74(10), 1676–1688. https://doi.org/10.1002/acr.24603
Aebischer, A. S., & Duff, S. (2020). Bunions: A review of management. Australian Journal of General Practice, 49(11), 720–723. https://doi.org/10.31128/AJGP-07-20-5541
American Podiatric Medical Association. (2025). “What is a podiatrist?” Advancing foot and ankle medicine and surgery. from https://www.apma.org/patients-and-the-public/what-is-a-podiatrist/.
Identify the signs of delayed symptoms that an auto accident may bring. Knowledge can aid in a better recovery process.
Introduction
Even little car accidents may have a significant effect on a person’s physical and mental health. Some injuries could show up right away, while others might take days, weeks, or months to manifest. Recovery and quality of life may be much enhanced by identifying these delayed symptoms, comprehending their effects, and learning how to react. The seven typical delayed symptoms are examined, along with the implications on the body and day-to-day activities, effective treatments, such as chiropractic therapy, and what to do during the symptom-free time.
Seven Common Delayed Symptoms
Delayed symptoms often arise due to the body’s initial adrenaline surge, which can mask pain, or because soft tissue injuries take time to manifest. Here are seven symptoms to watch for:
Neck Pain or Stiffness: Whiplash, a common injury resulting from rear-end collisions, can cause neck pain, stiffness, or a reduced range of motion. Symptoms can emerge days or weeks after the accident. This common injury causes sudden biphasic movements, thus leading to injuries to the bony, muscular, and ligamentous structures of the body. (Alektoroff & Papanagiotou, 2021)
Headaches: Post-traumatic headaches, often linked to whiplash or mild traumatic brain injury, may start days later and range from tension-type to migraines. These cause the individual to have increased pain sensitivity and cervical musculoskeletal impairments. (Di Antonio et al., 2023)
Back Pain: Strains, sprains, or herniated discs in the lower or upper back may not cause immediate discomfort but can develop as inflammation builds. Additionally, back pain is associated with impaired movement coordination, which can affect the body’s sensory function. (Delitto et al., 2012)
Numbness or Tingling: Nerve damage or compression, such as from a pinched nerve or herniated disc; these musculoskeletal issues can lead to tingling or numbness in the arms, legs, or hands.
Fatigue or Sleep Issues: Physical trauma or stress from the accident can disrupt sleep patterns, leading to chronic fatigue or insomnia over time.
Cognitive or Emotional Changes: Symptoms like difficulty concentrating, memory problems, anxiety, or irritability may indicate a concussion or post-traumatic stress.
Joint Pain or Swelling: Joint injuries, such as those to the shoulders or knees, may cause delayed swelling, stiffness, or pain due to inflammation or damage to the cartilage.
What to Do During the Delay Period
The period before symptoms appear is critical for protecting your health and legal rights. Here are key steps to take:
Seek Medical Evaluation: Even if a person feels fine, visiting a healthcare provider within 24–72 hours is crucial. They can perform a thorough exam, order imaging (e.g., X-rays or MRIs), and document latent injuries.
Monitor Your Health: Keep a daily journal of physical and mental changes, no matter how minor. Note pain, discomfort, or mood shifts to help identify patterns.
Avoid Strenuous Activity: Individuals should refrain from heavy lifting, intense exercise, or activities that could exacerbate underlying injuries, such as running or participating in contact sports.
Document the Accident: Individuals should take photos of everything, including the accident scene, vehicle damage, and any visible injuries that may have occurred during the accident. They should also collect witness statements and file reports with the police for insurance and legal purposes within the time frame of the accident.
Consult a Specialist: If symptoms emerge or your primary provider recommends it, schedule appointments with specialists, such as chiropractors, neurologists, or orthopedic doctors.
Follow Up Regularly: Schedule follow-up visits to track your condition, as some symptoms may take several weeks to appear.
Notify Your Insurance: Make sure to report the accident to the insurance company promptly, but avoid giving detailed statements about your health until you have been fully evaluated.
Car Accident Injury Rehabilitation- Video
Impact on Quality of Life & the Body
Delayed symptoms can significantly affect both physical health and daily life. Physically, untreated injuries may worsen, leading to chronic conditions. For example:
Musculoskeletal Damage: Whiplash or back injuries can lead to muscle spasms, reduced mobility, or chronic pain if left untreated.
Neurological Effects: Concussions or nerve compression may impair cognitive function, balance, or sensation, complicating daily tasks.
Inflammation and Scarring: Soft tissue injuries can lead to prolonged inflammation or the formation of scar tissue, which can limit flexibility and cause discomfort. Additionally, chronic inflammation, when left untreated, can lead to joint damage and tenderness if there are pre-existing conditions like rheumatoid arthritis. (Gessl et al., 2021)
Quality of life often suffers as a result. Chronic pain or fatigue can hinder work performance, leading to lost income or job stress. Sleep disturbances and emotional changes, like anxiety or depression, may strain relationships or reduce social engagement. Simple activities, such as driving, exercising, or sitting for extended periods, may become painful or difficult, which can lower overall well-being.
Treatment Options: Chiropractic Care & More
Treating delayed symptoms requires a comprehensive approach tailored to the injury. Below are effective treatments with a focus on chiropractic care:
Chiropractic Care: Chiropractors specialize in diagnosing, assessing, and treating musculoskeletal injuries, especially those involving the spine. They use spinal adjustments, manipulations, and soft tissue therapies to:
Restore joint mobility and alignment to reduce pain from whiplash or back injuries. (Stephen Dies, 1992)
Relieve nerve compression to address numbness or tingling.
Chiropractic care promotes natural healing by improving blood flow and reducing inflammation.
Regular chiropractic sessions can prevent chronic pain and improve recovery outcomes.
Physical Therapy: Targeted exercises and stretches strengthen muscles, improve flexibility, and restore range of motion. Therapists may use heat, ice, or ultrasound to relieve pain. To that point, physical therapy can improve the individual’s body function and reduce disability. (Hon et al., 2021)
Pain Management: Over-the-counter medications (e.g., ibuprofen) or prescription drugs can reduce inflammation and pain. In severe cases for pain management, corticosteroid injections may be recommended.
Massage Therapy: This complements chiropractic care by relaxing tight muscles, reducing spasms, and improving circulation, especially for neck or back pain.
Cognitive or Psychological Therapy: For concussion-related symptoms or emotional distress, cognitive behavioral therapy (CBT) or counseling can address anxiety, memory issues, or PTSD.
Lifestyle Adjustments: Incorporating rest, a balanced diet, and stress management techniques (e.g., meditation or yoga) supports recovery and reduces fatigue.
Medical Interventions: In rare cases, surgery may be needed for severe injuries like herniated discs or fractures. Consult an orthopedic specialist for evaluation.
Conclusion
After a car accident, delayed symptoms might be unexpected, but they can be lessened with prompt action and appropriate care. By identifying symptoms like headaches, neck discomfort, or cognitive problems, getting medical attention right once, and implementing therapies like chiropractic adjustments, you can always safeguard your health and well-being. To restore strength and wellbeing, be proactive by keeping an eye on your symptoms, heeding your doctor’s recommendations, and making your recovery a top priority. For individualized medical advice on your health and well-being, generally speaking, you should always speak with a healthcare expert.
Injury Medical Chiropractic & Functional Medicine Clinic
We associate certified medical providers who understand the importance of assessing individuals with pain-like delayed symptoms affecting their musculoskeletal system when involved in an auto accident. When asking important questions to our associated medical providers, we advise patients to incorporate customized treatment plans for their pain correlated with musculoskeletal issues after being involved in an auto accident to promote recovery. Dr. Alex Jimenez, D.C., utilizes this information as a professional academic service. Disclaimer
References
Alektoroff, K., & Papanagiotou, P. (2021). [Whiplash injury of the cervical spine]. Radiologe, 61(8), 710-713. https://doi.org/10.1007/s00117-021-00877-5 (Schleudertrauma der Halswirbelsaule.)
Delitto, A., George, S. Z., Van Dillen, L., Whitman, J. M., Sowa, G., Shekelle, P., Denninger, T. R., & Godges, J. J. (2012). Low Back Pain. Journal of Orthopaedic & Sports Physical Therapy, 42(4), A1-A57. https://doi.org/10.2519/jospt.2012.42.4.a1
Di Antonio, S., Arendt-Nielsen, L., & Castaldo, M. (2023). Cervical musculoskeletal impairments and pain sensitivity in migraine patients. Musculoskelet Sci Pract, 66, 102817. https://doi.org/10.1016/j.msksp.2023.102817
Gessl, I., Popescu, M., Schimpl, V., Supp, G., Deimel, T., Durechova, M., Hucke, M., Loiskandl, M., Studenic, P., Zauner, M., Smolen, J. S., Aletaha, D., & Mandl, P. (2021). Role of joint damage, malalignment and inflammation in articular tenderness in rheumatoid arthritis, psoriatic arthritis and osteoarthritis. Ann Rheum Dis, 80(7), 884-890. https://doi.org/10.1136/annrheumdis-2020-218744
Hon, S., Ritter, R., & Allen, D. D. (2021). Cost-Effectiveness and Outcomes of Direct Access to Physical Therapy for Musculoskeletal Disorders Compared to Physician-First Access in the United States: Systematic Review and Meta-Analysis. Phys Ther, 101(1). https://doi.org/10.1093/ptj/pzaa201
Stephen Dies, J. W. S. (1992). Chiropractic treatment of patients in motor vehicle accidents: a statistical analysis †. J Can Chiropr Assoc., 36(3), 139-145. https://pmc.ncbi.nlm.nih.gov/articles/PMC2484939/
El Paso, TX’s Leading Spine and Back Injury Specialist: Dr. Alex Jimenez, DC, APRN, FNP-C, IFMCP
Welcome to El Paso’s premier destination for advanced spine and back injury care, led by Dr. Alex Jimenez, a board-certified Family Practice Nurse Practitioner (FNP-C) and Chiropractor (DC). At www.dralexjimenez.com and www.chiromed.com, Dr. Jimenez and his team deliver cutting-edge, evidence-based treatments that integrate chiropractic care, functional medicine, and advanced rehabilitation protocols to address complex neuromusculoskeletal conditions. Our mission is to restore mobility, alleviate pain, and empower patients to live vibrant, pain-free lives through personalized, holistic care.
Specialized Spine and Back Injury Care
Dr. Jimenez’s practice is renowned for its expertise in treating intricate spine and back injuries, including herniated discs, severe sciatica, scoliosis, spinal stenosis, and chronic low back pain. By combining his chiropractic expertise with his advanced training as a Family Practice Nurse Practitioner and Institute for Functional Medicine Certified Practitioner (IFMCP), Dr. Jimenez offers a unique, integrative approach to spine care that addresses both symptoms and underlying causes.
Complex Spine Care Treatments
Dr. Jimenez utilizes cutting-edge techniques to address complex spine conditions in his chiropractic and rehabilitation clinic.
Chiropractic Spinal Adjustments use precise manual and instrument-assisted adjustments to restore spinal alignment, reduce nerve compression, and improve mobility. A 2020 study in Spine Journal found that spinal manipulative therapy significantly reduces pain and disability in patients with chronic low back pain (Rubinstein et al., 2020).
Decompression Therapy: Non-surgical spinal decompression to relieve pressure on herniated discs and pinched nerves, promoting disc healing and pain relief. Research in Journal of Physical Therapy Science (2017) supports its efficacy for lumbar disc herniation (Choi et al., 2017).
Regenerative Therapies: Platelet-rich plasma (PRP) and stem cell support therapies to enhance tissue repair and reduce inflammation in degenerative spine conditions. A 2019 meta-analysis in Pain Physician confirmed PRP’s effectiveness in managing lumbar pain (Sanapati et al., 2019).
Electro-Acupuncture: Targeted electrical stimulation of acupuncture points to reduce pain and promote healing in sciatica and chronic back pain. A 2018 study in Evidence-Based Complementary and Alternative Medicine demonstrated its benefits for neuropathic pain (Li et al., 2018).
Customized Rehabilitation Programs: Tailored exercises focusing on flexibility, core strength, and spinal stability to prevent re-injury and enhance long-term recovery.
As a Family Practice Nurse Practitioner, Dr. Jimenez offers comprehensive medical evaluations and functional medicine protocols to complement spine care:
Functional Medicine Assessments: In-depth evaluations using the Living Matrix Functional Medicine Assessment to identify root causes of chronic spine pain, including inflammation, nutritional deficiencies, and hormonal imbalances. A 2021 study in Frontiers in Medicine highlighted functional medicine’s role in improving outcomes for chronic pain patients (Beidelschies et al., 2021).
Nutritional Therapy: Personalized nutrition plans to reduce inflammation and support spinal health, incorporating anti-inflammatory diets rich in omega-3s and antioxidants. Research in Nutrients (2020) supports dietary interventions for reducing chronic pain (Kaushik et al., 2020).
Hormone Optimization: Addressing hormonal imbalances that exacerbate pain and delay healing, such as cortisol dysregulation in chronic stress. A 2019 study in Journal of Clinical Endocrinology & Metabolism linked cortisol imbalances to chronic pain syndromes (Hannibal et al., 2019).
Lifestyle Medicine: Guidance on stress management, sleep optimization, and ergonomic adjustments to support spine health and prevent injury recurrence.
Why Choose Dr. Jimenez for Spine and Back Injury Care?
Dr. Jimenez’s dual expertise as a chiropractor and nurse practitioner, combined with his IFMCP certification, sets him apart as El Paso’s top spine care specialist. Key differentiators include:
Holistic, Evidence-Based Approach: Integrating chiropractic care, functional medicine, and advanced diagnostics to address the whole person, not just symptoms.
Non-Invasive Protocols: Natural, non-surgical solutions should be prioritized to avoid the risks and recovery time associated with invasive procedures. A 2022 study in The Lancet emphasized the efficacy of non-invasive treatments for chronic low back pain (Foster et al., 2022).
Collaborative Care Network: Partnerships with leading orthopedic surgeons, neurologists, and rehabilitation specialists ensure seamless referrals when advanced interventions are needed.
Patient-Centered Plans: Using advanced diagnostics like MRI analysis, electromyography (EMG), and functional health assessments to create targeted treatment plans tailored to each patient’s unique needs.
Conditions Treated
Our clinic specializes in a wide range of spine- and back-related conditions, including:
Herniated Discs: Comprehensive care to reduce disc protrusion, alleviate nerve compression, and restore spinal function.
Severe Sciatica: Targeted therapies to relieve radiating leg pain and improve mobility.
Scoliosis: Customized bracing and exercise programs to manage spinal curvature and prevent progression.
Spinal Stenosis: Decompression and strengthening protocols to alleviate pain and improve quality of life.
Chronic Low Back Pain: Multifaceted treatment plans addressing biomechanical, inflammatory, and lifestyle factors.
Transform Your Spine Health Today
Whether you’re recovering from a traumatic spine injury, managing chronic back pain, or seeking preventive care, Dr. Alex Jimenez and his team are here to guide you. Contact us today at www.dralexjimenez.com or www.chiromed.com to schedule a consultation and discover how our integrative approach can transform your health. With evidence-based protocols and a compassionate, patient-centered philosophy, we help you live pain-free and thrive in El Paso’s vibrant community.
What are the advantages of having a team of nurse practitioners and chiropractors help maintain the health of your spine after a car accident?
Benefits of Chiropractic and Nurse Practitioners for Motor Vehicle Collisions
One of the main causes of spinal injuries, such as whiplash, herniated discs, and soft tissue injury, which can cause severe pain and impair movement, is motor vehicle collisions (MVCs). For both short-term symptoms and long-term rehabilitation, these injuries frequently necessitate a multimodal therapy strategy. While nurse practitioners, as advanced practice registered nurses, conduct medical evaluations, write prescriptions, and oversee overall health management, chiropractors focus on musculoskeletal care, including spine adjustments and manual therapies. These professionals’ collaboration aims to provide a comprehensive, patient-centered strategy for spine health following MVC. (Kent, R., et al., 2023)
For those recuperating from auto accident injuries, a chiropractic and nurse practitioner team can offer thorough spinal health care with an emphasis on pain management and increased mobility.
A chiropractic and nurse practitioner team can offer a comprehensive approach to spinal health after a car accident by addressing pain, improving mobility, and facilitating faster recovery.
Chiropractors focus on spinal alignment and joint mobility.
Nurse practitioners provide broader medical oversight and patient education.
The team approach can lead to more effective and personalized care for individuals recovering from car accident injuries. (Riva, J. J., et al., 2010)
Key advantages of this collaborative approach
A chiropractor and nurse practitioner (NP) therapy team can combine their skills to provide comprehensive care for spine health following a motor vehicle collision (MVC) and address acute and long-term requirements.
Care that is multidisciplinary and holistic
Collaboration between chiropractors and NPs to address structural and systemic issues enhances treatment outcomes, particularly for spine injuries related to motor vehicle collisions (MVC), as well as for chronic headaches and neck discomfort. (Riva, J. J., et al., 2010)
Plans for Treatment That Are Unique to You
Chiropractors and NPs create personalized patient treatment plans, focusing on their specific injuries and overall health, including pre-existing conditions and medication needs. This approach enhances outcomes by tailoring care to the patient’s unique circumstances.
Managing Pain Without Relying Too Much on Drugs
By using non-invasive methods to alleviate pain, chiropractic therapy may help reduce the use of opioids. NPs can prescribe short-term pain relief and monitor side effects, ensuring safe use and reducing dependency risks. Natural pain management combined with medical supervision lessens dependence and side effects. (Prater, C., Tepe, M., & Battaglia, P. 2020)
Quicker Recuperation and Rehabilitation
As demonstrated in the treatment of auto accidents, chiropractic adjustments can lessen muscle spasms and restore joint function. By referring patients to physical therapy and tracking their progress, NPs can hasten recovery and reduce the likelihood of developing persistent back pain. This integrated therapy not only reduces chronic back pain and other long-term problems, but it also accelerates healing.
Help with Insurance and the Law
Chiropractic and medical providers must carefully record injuries and treatments for insurance claims or legal cases after an MVC to ensure just reimbursement and coverage for care.
Why It Works After MVC
Following a motor vehicle collision (MVC), a chiropractor and nurse practitioner team offers a patient-centered approach to spine health. This team enhances recovery, lowers chronic risks, and improves patient outcomes by fusing NP’s medical management with chiropractic knowledge. This method ensures rapid alleviation and long-term health, especially helpful for complex spine injuries due to MVC.
Injury, Chiropractic, and Functional Medicine Clinic
Dr. Jimenez, a nurse practitioner, uses medical knowledge and chiropractic care to treat various conditions. The clinic provides tailored care programs incorporating functional medicine, acupuncture, electroacupuncture, and sports medicine. The clinic focuses on strength, agility, and flexibility for treating chronic pain syndromes and injuries. Patients of all ages and abilities benefit from comprehensive care plans and in-person and virtual health coaching, ensuring tailored treatment and wellness outcomes.
Personal Injury Rehabilitation
References
Kent, R., Cormier, J., McMurry, T. L., Johan Ivarsson, B., Funk, J., Hartka, T., & Sochor, M. (2023). Spinal injury rates and specific causation in motor vehicle collisions. Accident; analysis and prevention, 186, 107047. https://doi.org/10.1016/j.aap.2023.107047
Riva, J. J., Muller, G. D., Hornich, A. A., Mior, S. A., Gupta, A., & Burnie, S. J. (2010). Chiropractors and collaborative care: An overview illustrated with a case report. The Journal of the Canadian Chiropractic Association, 54(3), 147–154.
Prater, C., Tepe, M., & Battaglia, P. (2020). Integrating a Multidisciplinary Pain Team and Chiropractic Care in a Community Health Center: An Observational Study of Managing Chronic Spinal Pain. Journal of primary care & community health, 11, 2150132720953680. https://doi.org/10.1177/2150132720953680
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine