The adrenal glands are small glands located on top of the kidneys, and they are essential for our everyday wellness because they create a variety of hormones, such as cortisol and sex hormones. In addition, the adrenal glands create hormones that control sugar and blood pressure, react to stress, and burn protein and fat. If these small glands don’t create enough of the essential hormones for our everyday wellness, it can ultimately cause various health issues. Adrenal fatigue is a health issue recognized by many healthcare professionals. However, there is no evidence to prove that the condition exists. Adrenal fatigue is characterized as a collection of non-specific symptoms. James Wilson, Ph.D., naturopath, and alternative healthcare professional, coined the term in 1998 when he first identified the condition as a collection of associated symptoms when the adrenal glands aren’t functioning accordingly. He also described that the condition is typically associated with severe stress and fatigue that doesn’t get better with sleep, followed by other health issues, such as bronchitis, flu, or pneumonia. In the following article, we will discuss how to improve adrenal fatigue with diet ultimately.
What is Adrenal Fatigue?
According to healthcare professionals, adrenal fatigue can commonly develop in people that have experienced mental, physical, or emotional stress for an extended period of time. However, as previously mentioned, there is currently no evidence to prove that the condition exists. Many doctors are also concerned that if a patient is told that they have this condition, it may ultimately cause them to miss another underlying source of their symptoms that probably also won’t be diagnosed and treated accordingly. However, there are a variety of other health issues that may affect the adrenal glands. Adrenal fatigue develops when the adrenal glands are overworked due to chronic stress. Many healthcare professionals believe that excessive, long-term stress causes these small glands to become fatigued and unable to keep up with the demands to produce enough hormones. All of the symptoms below are relatively generic; however, they could signal an underlying health issue. Many of the symptoms could also be due to a busy life and a lack of sleep and caffeine addiction, poor nutrition, or increased amounts of stress. The common symptoms associated with adrenal fatigue can include:
tiredness
craving sugar and salt
abnormal weight loss
trouble getting to sleep and waking up
dependence on stimulants like caffeine
nonspecific digestive problems
What is Adrenal Insufficiency?
Adrenal insufficiency, commonly referred to as Addison’s disease, develops when the adrenal glands aren’t producing enough hormones we need for overall health. Adrenal fatigue is believed to be a mild type of adrenal insufficiency caused by severe stress over a long period of time. Adrenal insufficiency develops when the adrenal glands are damaged, causing them not to produce enough hormones, including cortisol and aldosterone. Cortisol regulates our stress response, while aldosterone regulates sodium and potassium. Symptoms associated with adrenal insufficiency can include:
fatigue
muscle weakness
lightheadedness
headaches or head pain
loss of appetite
unexplained weight loss
salt cravings
excessive sweating
loss of body hair
irregular menstruation in women
irritability and/or depression
hypoglycemia
low blood pressure
abdominal pain, nausea, and diarrhea
In more severe cases, when the adrenal glands aren’t producing enough of the necessary hormones due to adrenal insufficiency, you may experience:
nausea
vomiting
diarrhea
low blood pressure
hyperpigmentation
depression
Understanding the Adrenal Fatigue Diet
As previously mentioned, adrenal fatigue is a health issue that occurs when the adrenal glands aren’t creating enough of the essential hormones we need for our everyday wellness. Fortunately, many healthcare professionals recommend following the adrenal fatigue diet to help improve symptoms ultimately. The adrenal fatigue diet is a nutritional treatment approach that helps improve adrenal fatigue. The adrenal fatigue diet can increase energy levels and control various bodily functions because it promotes healthier eating habits and lifestyle modifications. Following the adrenal fatigue diet can help promote:
proper adrenal gland function
increased nutrients in the body
balanced blood pressure
reduced stress levels
Moreover, the adrenal fatigue diet is similar to the most balanced diets recommended by healthcare professionals, including eating plenty of vegetables, high-protein foods, and whole grains. This nutritional treatment approach aims to naturally increase your energy levels for the body, not burn too many essential nutrients. The adrenal fatigue diet is still being tested. Healthcare professionals are still performing research studies on adrenal fatigue. However, it has been demonstrated that eating a proper diet, and lifestyle modifications can ultimately make you feel overall wellness.
Foods to Eat with Adrenal Fatigue
Following a balanced diet is the best way to regulate the essential functions of the human body and maintain overall wellness. Healthcare professionals recommend eating complex carbohydrates, proteins, and healthy fats. Also, eat plenty of vegetables to get the necessary amount of vitamins and minerals and eat foods that are high in vitamin C, B vitamins, and magnesium to support the adrenal glands. It’s also essential to stay hydrated. Dehydration can affect your stress levels and make the adrenal glands produce cortisol. Foods to eat on the adrenal fatigue diet can include:
low-sugar fruits
leafy greens and colorful vegetables
nuts
legumes
whole grains
dairy
fish
lean meats
eggs
healthy fats such as olive oil and coconut oil
sea salt (in moderation)
Foods to Avoid with Adrenal Fatigue
Although the adrenal fatigue diet also doesn’t require any major dietary restrictions that could harm your health, you should still talk with your healthcare professional before changing your eating habits. If you begin to experience any adverse symptoms or if the adrenal fatigue diet makes your condition worse, visit your healthcare professional immediately. Furthermore, if you decide to try following the adrenal fatigue diet, many healthcare professionals recommend limiting foods and drinks high in refined and processed sugars and fats. Several foods to avoid eating with adrenal fatigue can include:
refined white sugar
refined white flour
fried food
processed food
fast food
artificial sweeteners
soda
caffeine
alcohol
The adrenal glands are small glands found on top of each kidney. The outer region of the adrenal gland, known as the adrenal cortex, creates a variety of hormones, including cortisol and aldosterone. The inner region of the adrenal gland, known as the adrenal medulla, creates other hormones, such as adrenaline or epinephrine and norepinephrine. These essential hormones are necessary for a variety of functions in the human body, including: regulating sugar, salt, water, metabolism, and blood pressure, as well as regulating stress and inflammation, among other essential bodily functions. Adrenal fatigue can commonly develop in people that have experienced severe mental, physical, or emotional stress for an extended period of time. However, as previously mentioned above, there is currently not enough evidence to ultimately prove that the condition exists.– Dr. Alex Jimenez D.C., C.C.S.T. Insight
The adrenal glands are small glands located on top of the kidneys, and they are essential for our everyday wellness because they create a variety of hormones, such as cortisol and sex hormones. In addition, the adrenal glands create hormones that control sugar and blood pressure, react to stress, and burn protein and fat. If these small glands don’t create enough of the essential hormones for our everyday wellness, it can ultimately cause various health issues. Adrenal fatigue is a health issue recognized by many healthcare professionals; however, there is no evidence to prove that the condition exists. Instead, adrenal fatigue is characterized as a collection of non-specific symptoms. James Wilson, Ph.D., naturopath, and alternative healthcare professional, coined the term in 1998 when he first identified the condition as a collection of associated symptoms when the adrenal glands aren’t functioning accordingly. He also described that the condition is typically associated with severe stress and fatigue that doesn’t get better with sleep, followed by other health issues, such as bronchitis, flu, or pneumonia. In the article above, we will discuss how to improve adrenal fatigue with diet ultimately.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Curated by Dr. Alex Jimenez References:
Newman, Tim. Adrenal Fatigue: Myths, Symptoms, Disorders, and Treatment. Medical News Today, MediLexicon International, 27 June 2018, www.medicalnewstoday.com/articles/245810.php#treatment.
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”52657″ /] The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized to diagnose any type of disease, condition, or other type of health issue.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals. However, chronic pain is different than the average type of pain. The human body will continue sending pain signals to the brain with chronic pain, regardless of the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility, reducing flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual’s reactivity to 48 neurological antigens with connections to various neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with various food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers particular antibody-to-antigen recognition. This panel measures an individual’s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Finally, utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient’s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). In addition, the Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine. It has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). Therefore, it is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders at the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
The adrenal glands are small glands found on top of each kidney and they are necessary for our everyday health because they produce a variety of hormones, including cortisol and sex hormones. The adrenal glands produce the hormones that regulate sugar and blood pressure, respond to stress, as well as burn protein and fat. If these small glands don’t produce enough of the necessary hormones, it can ultimately cause a variety of health issues. Adrenal fatigue is a health issue recognized by many healthcare professionals, however, there is no evidence to prove that the condition exists.
Adrenal fatigue is characterized as a collection of non-specific symptoms. James Wilson, Ph.D., naturopath and alternative healthcare professional, coined the term in 1998 when he first described the condition as a group of associated symptoms that developed when the adrenal glands aren’t functioning accordingly. He also stated that the condition is generally associated with severe stress and fatigue that doesn’t get better with sleep which follows with other health issues, such as bronchitis, flu, or pneumonia. In the following article, we will discuss adrenal fatigue as well as its diagnosis and treatment.
Understanding Adrenal Fatigue
According to healthcare professionals, adrenal fatigue can commonly develop in people that have experienced mental, physical, or emotional stress for an extended period of time. However, as previously mentioned, there is currently no evidence to prove that the condition exists. Many doctors are also concerned that if a patient is told that they have this condition, it may ultimately cause them to miss another underlying source of their symptoms that probably also won’t be diagnosed and treated accordingly. However, there are a variety of other health issues that may affect the adrenal glands.
Adrenal Fatigue Symptoms
Adrenal fatigue develops when the adrenal glands are overworked due to chronic stress. Many healthcare professionals believe that excessive, long-term stress causes these small glands to become fatigued and unable to keep up with the demands to produce enough hormones. All of the symptoms below are relatively generic, however, they could signal an underlying health issue. Many of the symptoms could also be due to a busy life and a lack of sleep, as well as due to caffeine addiction, poor nutrition, or increased amounts of stress. The common symptoms associated with adrenal fatigue can include:
tiredness
craving sugar and salt
abnormal weight loss
trouble getting to sleep and waking up
dependence on stimulants like caffeine
nonspecific digestive problems
Adrenal Fatigue Diagnosis
Many healthcare professionals may take blood samples or utilize salivary cortisol tests to determine if a patient has adrenal fatigue as well as any other underlying health issue. However, because there is no evidence to prove that adrenal fatigue exists, there are currently no definitive ways to properly diagnose the condition. People who do believe in adrenal fatigue argue that modern diagnosis methods and/or techniques are not sensitive enough to determine the decreased function of the adrenal glands, however, they do describe that their bodies still feel the symptoms of adrenal fatigue.
Adrenal Fatigue Treatment
Many healthcare professionals start adrenal fatigue treatment by recommending patients to quit caffeine, alcohol, drugs, and cigarettes. They will also recommend patients to start eating healthy, exercise more, and sleep better. Following these diet and lifestyle modifications can make anyone feel better. Despite the lack of evidence, there is a wide variety of products, often in the form of vitamins and supplements, available to relieve symptoms associated with adrenal fatigue. Because the Food and Drug Administration (FDA) does not regulate these treatments, they may have not been tested for safety.
If you are experiencing any symptoms associated with adrenal fatigue, it’s essential to visit a healthcare professional immediately in order to receive a proper diagnosis and follow-up with treatment. Moreover, if you take vitamins or supplements for adrenal fatigue without an underlying health issue, the adrenal glands can start to rely on or be suppressed by the treatment, ultimately causing another health issue known as adrenal insufficiency. A healthcare professional physician will be willing to help a patient determine the source of their symptoms and start the proper treatment for their health issues.
Adrenal Insufficiency or Adrenal Fatigue?
Adrenal insufficiency, commonly referred to as Addison�s disease, is a health issue that develops when the adrenal glands aren�t producing enough of the hormones we need for overall health. Adrenal fatigue is believed to be a mild type of adrenal insufficiency caused by severe stress over a long period of time. Adrenal insufficiency develops when the adrenal glands are damaged, causing them to not produce enough hormones, including cortisol and aldosterone. Cortisol regulates our stress response while aldosterone regulates sodium and potassium. Symptoms associated with adrenal insufficiency can include:
fatigue
muscle weakness
lightheadedness
headaches or head pain
loss of appetite
unexplained weight loss
salt cravings
excessive sweating
loss of body hair
irregular menstruation in women
irritability and/or depression
hypoglycemia
low blood pressure
abdominal pain, nausea, and diarrhea
There are two adrenal glands, one on top of each kidney in the human body. The outer region of the adrenal gland, known as the adrenal cortex, produces hormones, such as cortisol and aldosterone. The inner region, known as the adrenal medulla, produces adrenaline or epinephrine and norepinephrine. These necessary hormones are important for a variety of functions including: regulating sugar, salt, water, metabolism, and blood pressure, as well as regulating stress and inflammation, among other functions. Adrenal fatigue can commonly develop in people that have experienced severe mental, physical, or emotional stress for an extended period of time. However, as previously mentioned above, there is currently no evidence to prove that the condition exists.Dr. Alex Jimenez D.C., C.C.S.T. Insight
The adrenal glands are small glands found on top of each kidney and they are necessary for our everyday health because they produce a variety of hormones, including cortisol and sex hormones. The adrenal glands produce the hormones that regulate sugar and blood pressure, respond to stress, as well as burn protein and fat. If these small glands don’t produce enough of the necessary hormones, it can ultimately cause a variety of health issues. Adrenal fatigue is a health issue recognized by many healthcare professions, however, there is no evidence to prove that the condition exists.
Adrenal fatigue is characterized as a collection of non-specific symptoms. James Wilson, Ph.D., naturopath and alternative healthcare professional, coined the term in 1998 when he first described the condition as a group of associated symptoms that developed when the adrenal glands aren’t functioning accordingly. He also stated that the condition is generally associated with severe stress and fatigue that doesn’t get better with sleep which follows with other health issues, such as bronchitis, flu, or pneumonia. In the article above, we discussed adrenal fatigue as well as its diagnosis and treatment.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
Newman, Tim. �Adrenal Fatigue: Myths, Symptoms, Disorders, and Treatment.� Medical News Today, MediLexicon International, 27 June 2018, www.medicalnewstoday.com/articles/245810.php#treatment.
Felson, Sabrina. �Adrenal Fatigue: Is It Real? Symptoms, Causes, Treatments.� WebMD, WebMD, 8 Feb. 2019, www.webmd.com/a-to-z-guides/adrenal-fatigue-is-it-real#1.
Neurotransmitter Assessment Form
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”52657″ /]
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
As 2020 is off to a bustling start, New Year resolutions are in full swing! Most individuals want to make healthier choices throughout their year in 2020, whether that be exercising more, eating better, or just feeling energized. After the holidays hit, most people are left feeling fatigued,� suffering headaches, and overall discomfort.
A great way to stay on track with your goals is to keep track of them! The human body requires micronutrients and macronutrients to function. Micronutrients consist of essential vitamins and minerals. Macronutrients refer to protein, fat, and carbohydrates. Macronutrients all provide the body with energy. This energy is essential to properly repair cells as well as maintain metabolism, immunity, and growth.
Carbohydrates are the main energy system in the human body. These carbohydrates provide over 50% of the daily diet. However, not all carbohydrates are created equal. There are simple and complex carbohydrates. Simple carbohydrates are those found in glucose and fructose (examples: fruit, sugar, and milk). Complex carbohydrates are those that require the body to work a little harder to break down and contain glycogen. Glycogen is important to eat as it is a valuable source of fiber.
The main function of protein is to maintain and grow the body tissue. Proteins are made up of amino acids.� Amino acids are the stepping stones used for neurotransmitters, cell membranes, nucleic acids, and hormones. Protein is widely stored in the human body due to the large amount of muscle tissue the body is comprised of. Overall, there are amino acids that must be obtained through the diet to maintain optimal health. Some of these amino acids include lysine, threonine, and tryptophan.
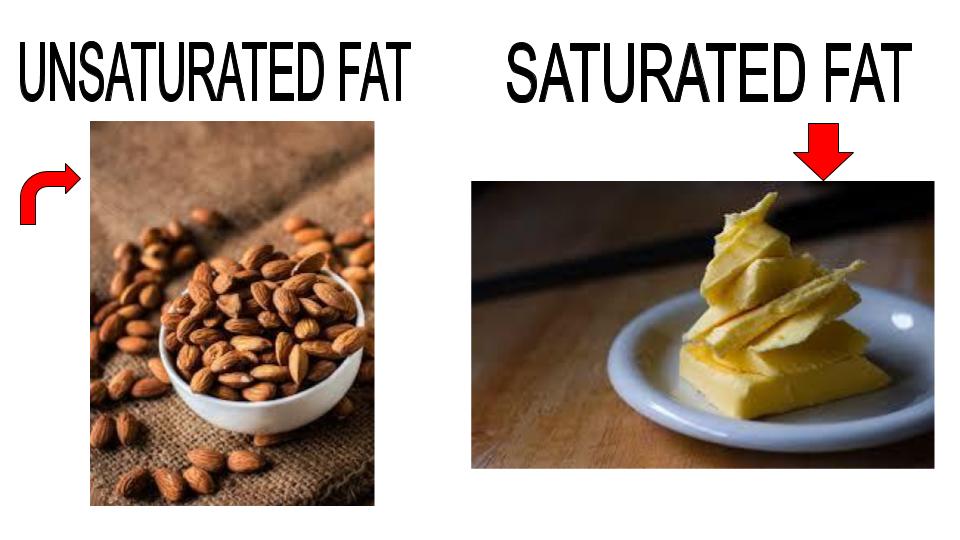
Out of all the macronutrients, dietary fats require the least amount of grams per day. Similar to carbohydrates, there are two types of fat. Saturated and unsaturated. Saturated fats can be found in butter, where unsaturated fats mainly consist of nuts and avocados. A great supplement to take for healthy fats is Omega-3 and Omega-6, also known as fish oils. Fish oils also help improve cardiovascular health and help the Body generate specialized lipid mediators.
Although each individual requires protein, fat, and carbohydrates, the optimal amount of each depends on each person as well as their body composition. Tracking macronutrients has been shown to improve weight loss and reduce inflammation.
�Tracking macros or macronutrients coupled with exercise is a great way to see results. The macronutrients each person needs depends on their body type, their goals, and their lifestyle. Health coaches such as myself can help determine what an individual’s macronutrient intake should be for weight loss results. Personally, I use the Dr. J Today app, wrist band, and scale. This app allows patients to track their food, steps, water intake, and exercise as well as provides an informative digital library. The scale directly syncs to the app, allowing me to get instant access to the weight and body composition of the patient. This scale not only measures individuals but it also measures their lean body mass, water mass, BMI, and body fat. These resources allow us to gain optimal insight and make corrections that will actually make a difference. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Inversion tables and inversion treatment/therapy could help with low back/leg pain and sciatica. It�s non-surgical and an option your doctor, or chiropractor could recommend to you before looking into more invasive options. Individuals with low back pain, sciatica or both found inversion therapy with an inversion table provided relief from symptoms, and continued use has kept them and their spines healthy.
With an inversion table, you don�t have to use gravity boots or completely hanging upside down. There are inversion boots and hanging racks that also offer inversion therapy, this type is not for beginners. With experience, you can move on to this type but for now, leave it to individuals in top health and athletic condition. This type of inversion table therapy is an alternative that doesn’t require being completely upside down.
An Ancient Therapy Brought Back
Inversion therapy is nothing new. Hippocrates, the father of medicine, saw what inversion therapy could do and the benefits around 400 BC. The goal is to use gravity to release compression in the spine. The downward force pulls everything toward the earth’s center.
How It Works
Inversion therapy works in a way like spinal traction.
For example, when we stand and sit gravity pulls the spine downward and this is what compresses the discs, vertebral bodies, nerves, and other spinal structures. The physical dynamics along with gravity helps relieve spinal compression. As the spine is stretched out the pressure on your back is reduced.
The theory behind inversion therapy sounds like a fantastic non-surgical option to back pain. However, the research going into inversion therapy is a bit more mixed. One study found that almost 77% of patients that were candidates for surgery no longer needed the surgery after using inversion therapy. For patients that didn�t use inversion therapy, only 23% avoided surgery.
But like all back pain/sciatica treatment plans, it’s what works for you. Ask your doctor/chiropractor about the pros and cons of this type of treatment as it relates to your condition to make an informed decision.
Other Benefits
Many patients report that inversion therapy is a great way to:
Stretch the muscles and ligaments
Reduce muscle spasms
Improve circulation
Stretching stimulates the lymph glands which increases the flow of lymphatic fluids, that are part of the body’s waste disposal. Cellular health depends on healthy blood circulation to be delivered, to nourish and remove waste.
The therapy also helped to relieve motion sickness and stress. This is because the body is more aware of its spatial orientation along with balance as the inner ear gets stimulated while inverted. As stated earlier it is not necessary to be positioned completely upside down to benefit from this therapy. Inversion tables are adjustable and offer the flexibility to find the best angle.
Discuss Inversion Therapy with A Doctor
Before you start using an inversion table�talk to your doctor. Certain medications and health conditions could make using an inversion table unsafe.
It could be recommended against inversion table therapy if you have:
There could be other medical conditions that are not listed but could interfere with inversion therapy, so make sure your doctor knows all your medical history/conditions and current health state before beginning.
Starting Inversion Therapy
How to start an inversion therapy program? Take it very slow, easy, taking your time and have someone there to help and assist until you are comfortable doing it on your own.�The tables can be set at different angles and it is recommended you start at the first and work your way to the last. At the 15-degree angle, your body will feel a stretch along with the benefits of increased blood circulation.
Most people don’t have to go beyond 60-degrees, as the spine decompresses at this angle. But you might want to completely invert yourself as you work through the different degrees and go for the full inversion. But don’t overdo it and listen to what your body tells you.
The tables come in a variety of styles, so be sure to research the different brands. Some tables can include a sliding backrest and foot lock that lets you work in gentle stretching exercises during inversion. This could include head movements from side-to-side, stretching the arms overhead, and doing abdominal sit-ups or crunches.
But first, find out from your doctor how often you should invert and the kinds of movements that will help with your condition and enhance your inversion program. Inversion therapy is another option for a back, sciatic pain treatment plan. For the different forms of spine pain, a doctor will try several non-surgical treatment options before discussing surgery. Inversion therapy could be part of a conservative treatment plan and could help prevent the need for spine surgery.
*Effective Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
The spine is the primary support for the body. When it breaks down, the body suffers. Regular chiropractic treatment ensures that the spinal column remains in proper alignment which, in turn, keeps the body in proper alignment. It helps with joint health as well as the health of the related muscles and ligaments.
Your chiropractor can also recommend stretching and strength-building exercises to help keep your spine healthy and supple. Chiropractic helps to keep the back flexible which aids in preventing injury. A healthy spine is also less likely to become misaligned or experience pain. It can significantly improve your quality of life as you are more flexible and mobile.
Dopamine and serotonin are known as the “happy chemicals” because they play a fundamental role in regulating our mood. These two neurotransmitters or chemical messengers control a variety of functions in the brain and body, including digestion and sleep. Although dopamine and serotonin are in charge of many of the same things, these happy chemicals do so in slightly different ways. Dopamine and serotonin deficiencies can also cause a variety of health issues, including mood changes and depression. In the following article, we will ultimately discuss the differences between dopamine and serotonin. �
What is a Neurotransmitter?
As previously mentioned, a neurotransmitter is a chemical messenger in the brain that sends signals to other areas of the body. Dopamine and serotonin are two of the many different types of neurotransmitters in the brain and body. Below is a list of some of the most well-known neurotransmitters, including: �
Dopamine
Serotonin
Norepinephrine
Acetylcholine
Glycine
Glutamate
GABA
Understanding Neurotransmitters
Our brain is one of the most complex organs in the human body. The nervous system contains more than 100 billion nerves which are continuously sending signals from the brain to the rest of the body, ultimately regulating our mental and physical health. However, various factors can cause many problems. Dopamine and serotonin deficiencies, by way of instance, can cause a variety of mental and physical health issues, such as depression. While these two neurotransmitters are both commonly referred to as “happy chemicals”, it’s important to understand that dopamine and serotonin also play different roles. �
What is Dopamine?
Dopamine is a well-known neurotransmitter released in the brain to send signals between nerve cells. Our brain and body use dopamine to produce other compounds known as norepinephrine and epinephrine. Dopamine plays a fundamental role in the “pleasure and reward center” in the brain, or a collection of functions in the brain that control mood, motivation, and movement. Healthy dopamine levels can also affect a variety of other functions, including: �
alertness
learning
mood
motivation
movement
blood circulation
urine output
sleep
What is Serotonin?
Serotonin is another neurotransmitter used to send signals between nerve cells. However, about 90 percent of the human body’s serotonin can be found in the gut, where it helps control a variety of functions in the digestive system. Healthy serotonin levels can also affect a variety of other functions, including: �
focus and concentration
mood, emotions, and feelings
appetite and digestion
hormonal activity
circadian rhythm or sleep-wake cycle
blood clotting
body temperature
Dopamine, Serotonin, and Depression
Depression is one of the most common and well-known mental health issues which is ultimately caused by a variety of factors, such as dopamine and serotonin deficiencies. Both of these neurotransmitters or chemical messengers can also play a fundamental role in depression, however, many healthcare professionals are still trying to understand the true cause of depression. Research studies have demonstrated that dopamine and serotonin deficiencies caused by other underlying health issues may be associated with depression. Several common symptoms of depression can ultimately include: �
decreased or reduced motivation
feelings of helplessness
loss of interest in things that used to interest you
Dopamine, Serotonin, and Other Health Issues
Because dopamine and serotonin play a fundamental role in a variety of functions in the brain and body, it is no surprise that these “happy chemicals” are also essential in our mental and physical health. When both of these neurotransmitters are functioning accordingly, they can ultimately help us feel happy and more emotionally balanced. As previously mentioned, however, dopamine and serotonin deficiencies can also cause various other health issues. � Doing anything that we find enjoyable, from eating a good meal to having sex, can trigger the release of dopamine in the brain and body. That release is what makes several things addicting like drugs and gambling. Scientists have determined that it doesn’t take long for the brain to associate several of these things with a release of dopamine. Research studies have also found that dopamine deficiencies may be associated with other health issues, such as: �
Parkinson’s disease
attention deficit hyperactivity disorder (ADHD)
schizophrenia
bipolar disorder
Furthermore, according to several research studies in 2014, serotonin deficiencies were also associated with a variety of other health issues, including: �
anxiety disorders
obsessive-compulsive disorder (OCD)
autism
bipolar disorder
What are the Differences Between Dopamine and Serotonin?
Dopamine and serotonin are both neurotransmitters or chemical messengers that send signals between the brain and body. However, the primary functions of these well-known “happy chemicals” are very different. Dopamine is associated with the pleasure and reward center in the brain while serotonin is associated with our mood and it is more of a stabilizer than a booster. Also, dopamine controls movement while serotonin controls digestion and sleep. �
Dopamine and serotonin are two well-known neurotransmitters, or chemical messengers, that play a fundamental role in our mood and a variety of other functions in the brain and body. Dopamine helps control mood, motivation, and movement while serotonin helps control positive feelings and social behavior, learning and memory, appetite as well as our circadian rhythm or sleep-wake cycle. Dopamine and serotonin deficiencies can cause a variety of mental and physical health issues, including anxiety, depression, Parkinson’s disease, schizophrenia, obsessive-compulsive disorder (OCD), and bipolar disorder. In this article, we will discuss the differences between the release of dopamine and serotonin in the brain and body.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Dopamine and serotonin are known as the “happy chemicals” because they play a fundamental role in regulating our mood. These two neurotransmitters or chemical messengers control a variety of functions in the brain and body, including digestion and sleep. Although dopamine and serotonin are in charge of many of the same things, these happy chemicals do so in slightly different ways. Dopamine and serotonin deficiencies can also cause a variety of health issues, including mood changes and depression. In the article above, we ultimately discussed the differences between dopamine and serotonin. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Eske, Jamie. �Dopamine vs. Serotonin: Similarities, Differences, and Relationship.� Medical News Today, MediLexicon International, 19 Aug. 2019, www.medicalnewstoday.com/articles/326090.php.
Vandergriendt, Carly. �What’s the Difference Between Dopamine and Serotonin?� Healthline, Healthline Media, 5 Dec. 2018, www.healthline.com/health/dopamine-vs-serotonin.
Puskar, Michael. �What Is The Difference Between Serotonin And Dopamine?� Betterhelp, BetterHelp, 6 May 2018, www.betterhelp.com/advice/medication/what-is-the-difference-between-serotonin-and-dopamine/.
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
� XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
� �
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine. �
In today’s workforce, many jobs place workers at a higher risk for a back injury. The list is pretty extensive and may surprise you! Individuals that have suffered a� neck or back injury at work know the cost goes beyond lost wages. The impact of these injuries on employees, employers, and the economy is staggering.
In a report published by the Bureau of Labor Statistics, there were 2.8 million cases of non-fatal occupational injuries and in 2018.� Of these cases, more than 50% lost time from work, transferred to a different job, or restricted work activity. Not all of these cases were spine-related injuries. However, 880,000 cases were back pain-related injuries.
The World Health Organization’s International Labour Office says that the problem is global.
Musculoskeletal diseases are a very common part of 270 million non-fatal work/job accidents where employees missed at least 3 workdays.
Risky Jobs
Occupational safety experts gather all kinds of information that they factor. This includes job requirements, work environment, and work station set up. In compiling the list of risky occupations, here are some of the criteria:
Heavy physical work
Forceful lifting movements
Bending
Twisting
Awkward work postures
Whole-body vibration
Static work postures like standing/sitting but never changing position compounds the risks to workers.
Two occupations that lead the list of jobs placing workers at the highest risk are construction and nurses/nursing home workers. Workers in both of these jobs tend to share the under-reporting of work-related injuries. This happens as the employees fear they will lose their job and cannot afford to take any time off.
Construction Workers
Employees at a construction site are repeatedly lifting, bending, carrying, pulling, and tugging. These repetitive movements lead to overuse injuries and back strain/sprains are a common part of this. More than 30% of workers have to miss job time. Those that must climb ladders or work on scaffolds have a greater risk of falling. This is where some serious spinal injuries can occur, causing disability and sometimes being fatal.
Nurses/Nursing Workers
Nursing homes and employment opportunities are growing from elderly population growth. These workers are at high risk for back pain and spine injury. This comes from transferring patients’ from their beds, bathtub, and bathroom facilities. All these actions require lifting, carrying, holding, pulling, pushing, and turning. The Bureau of Labor Statistics reports nearly all back and shoulder injuries are the result of moving patients.
Warehouse Workers
This is another job that requires lifting, along with using forceful movements, bending, twisting, carrying, and placing the body in awkward positions. Sometimes these workers have to drive a truck or an industrial vehicle that creates whole-body vibration. Continual exposure to vibration can cause backache and soreness that can lead to lost work time.
Dentists and Surgeons
Both of these professions involve prolonged standing, stooping, bending, and awkward body positioning. Not to mention the mental strain that diverts the doctor’s attention to proper posture and body mechanics that results in injury and pain.
Landscapers
The American Chiropractic Association puts landscapers in the top 10 list of jobs that cause back pain. This job puts these workers at a greater risk for cumulative trauma disorders. All the tasks that a landscaper has to do that include hedge trimming, tree pruning, and planting. These actions/movements involve lifting, reaching, bending, and stooping. This is a perfect set up for an overuse back injury.
Hand tools that get used over and over can cause painful conditions like carpal tunnel syndrome and thoracic outlet syndrome. Thoracic outlet syndrome is when the nerves and blood vessels become compressed between the neck and shoulder.
Store Cashier
Grocery and retail store cashiers require workers to stand in one place for a long time. This along with the repetitive motions of scanning, typing, opening, closing combined with bagging and lifting bags over and over can cause neck, shoulder, back, leg and foot pain. Over half of checkout workers complain of back pain.
We may not be able to instantly change our occupation, but there are steps to help prevent neck and back injuries. The key is workplace ergonomics and safety. Be proactive to help reduce workplace risk for neck and back injury and share what you learn with co-workers.
*BEST* Heel Spurs Treatment | El Paso, Tx (2020)
NCBI Resources
Injuries that are caused by repetitive movements often develop gradually.�This is the time when the symptoms are mild and come and go, so the individual just works through it and doesn�t think about it. It�s�not until the symptoms get very painful and debilitating that the individual realizes that something is wrong, and then they seek medical attention. Don�t wait, as soon as you feel a tingle, slight pinch, or a little soreness�and you feel that it stems from your work�s repetitive movements, get in touch with a doctor or chiropractor before it becomes excruciating.
Serotonin is a neurotransmitter that plays a fundamental role in a variety of brain and bodily functions. This chemical messenger helps regulate mood and social behavior as well as support our circadian rhythm or sleep-wake cycle. Research studies demonstrated that “healthy” serotonin levels are associated with positive feelings and longevity. We can naturally increase our serotonin levels by eating tryptophan-rich foods or taking tryptophan supplements. This essential amino acid is used to synthesize serotonin. In the following article, we will discuss foods that can help naturally increase serotonin. �
Pineapple
According to several research studies, eating pineapple may boost bromelain, a well-known protein that can help suppress coughs as well as reduce the side-effects of chemotherapy in the brain and body. Combine pineapple with other tryptophan-rich foods to also naturally increase your serotonin levels. �
Nuts and Seeds
All nuts and seeds are excellent sources of tryptophan. Research studies demonstrate that eating a handful of nuts and/or seeds every day can ultimately help lower your risk for respiratory health issues, heart disease, and cancer. Nuts and seeds are also excellent sources of vitamins, antioxidants, and fiber. �
Salmon
Salmon is a well-known tryptophan-rich food that also has a variety of other nutritional benefits, including being another tremendous source of omega-3 fatty acids as well as helping to lower blood pressure and regulate cholesterol. Combine salmon with other tryptophan-rich foods to boost serotonin. �
Turkey
There’s a good reason why many people take a relaxing nap on the couch after their Thanksgiving day meal. Turkey is basically filled with a lot of tryptophan. �
Eggs
According to research studies, the amount of protein that is found in eggs can considerably help naturally increase tryptophan levels in your blood plasma, leading to the production of serotonin. And always make sure to never leave out the egg yolks. Egg yolks contain omega-3 fatty acids, biotin, choline, tyrosine, tryptophan, and a variety of other nutrients, many of which can provide you with many health benefits. Eggs also have antioxidant properties. �
Cheese
Cheese is yet another tryptophan-rich food that you can eat to help naturally increase serotonin. Although you can eat many different types of cheese in a variety of ways, a popular meal you could make is mac and cheese which combines cheddar cheese with eggs and milk, other tryptophan-rich foods. �
Tofu
Eating plenty of soy products like tofu can also help naturally increase serotonin because these are also full of tryptophan. Substitute tofu for any protein source as an excellent source of tryptophan for vegetarians and vegans. Tofu or soy products are also calcium-set and can provide us with calcium. �
Nutrition and Serotonin
Because serotonin isn’t found in food, eating foods that have tryptophan, the amino acid used to synthesize serotonin, is fundamental to help naturally increase this neurotransmitter or chemical messenger in the brain and body. Eating foods that are also excellent sources of protein, iron, riboflavin, and vitamin B-6 generally have great amounts of this essential amino acid. However, eating tryptophan-rich foods alone won’t boost serotonin levels. Eating carbohydrates triggers the release of insulin which can promote the absorption of other amino acids while leaving more tryptophan in the bloodstream. �
Combining tryptophan-rich foods with carbs can help naturally increase serotonin in the brain and body. Tryptophan has to compete with many other amino acids in order to penetrate the BBB and enter the brain from the bloodstream which is why the tryptophan in the foods we eat may ultimately have a minor effect on serotonin levels. However, this effect is different from tryptophan supplements that have pure tryptophan which can considerably boost serotonin. Always make sure to talk to your healthcare professional before taking any supplements. Eating tryptophan-rich foods can safely help increase serotonin. �
Other Ways to Naturally Increase Serotonin
Eating tryptophan-rich foods and taking tryptophan supplements aren�t the only ways to naturally increase serotonin in the brain and body. �
Take probiotics. Eating fiber can support gut bacteria that play a fundamental role in serotonin levels through the gut-brain connection.
Do Exercise. Research studies have shown that doing regular exercise and physical activity can help balance your mood.
Get Sunlight. Getting plenty of sunlight is a common remedy for seasonal depression. Research studies have shown a connection between being exposed to sunlight and serotonin levels in the brain and body. To boost your mood, try getting enough (but not too much) sunlight.
Be Positive. Research studies have also shown that simply being more positive can naturally help increase serotonin levels.
Serotonin is a well-known neurotransmitter, or chemical messenger, that is associated with mood and a variety of other important functions in the human brain and body. Serotonin helps promote positive feelings and social behavior, control appetite, support learning and memory as well as regulate our circadian rhythm or sleep-wake cycle. Serotonin deficiencies can cause a variety of brain and mental health issues, including anxiety, depression, sleep problems, fatigue, abnormal appetite and cravings as well as nausea and digestive problems. Fortunately, eating tryptophan-rich foods can help naturally increase serotonin levels in the human brain and body. In the following article, we will discuss how eating certain well-known tryptophan-rich foods can help naturally increase serotonin as well as promote overall health and wellness.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Serotonin is a neurotransmitter that plays a fundamental role in a variety of brain and bodily functions. This chemical messenger helps regulate mood and social behavior as well as support our circadian rhythm or sleep-wake cycle. Research studies demonstrated that “healthy” serotonin levels are associated with positive feelings and longevity. We can naturally increase our serotonin levels by eating tryptophan-rich foods or taking tryptophan supplements. This essential amino acid is ultimately used to synthesize serotonin. In the article, we discussed foods that can ultimately help naturally increase serotonin. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Healthline Editorial Team. �7 Foods That Could Boost Your Serotonin: The Serotonin Diet.� Healthline, Healthline Media, 29 Aug. 2018, www.healthline.com/health/healthy-sleep/foods-that-could-boost-your-serotonin.
Raypole, Crystal. �6 Ways to Boost Serotonin Without Medication.� Healthline, Healthline Media, 22 Apr. 2019, www.healthline.com/health/how-to-increase-serotonin.
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
� �
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual’s reactivity to 48 neurological antigens with connections to various neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual’s reactivity to 48 neurological antigens with connections to various neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.  Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with various food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers particular antibody-to-antigen recognition. This panel measures an individual’s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Finally, utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient’s specific needs.
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with various food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers particular antibody-to-antigen recognition. This panel measures an individual’s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Finally, utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient’s specific needs.  Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). In addition, the Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine. It has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). Therefore, it is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). In addition, the Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine. It has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). Therefore, it is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.