When it comes to the body, the various muscles, tissues, joints, and organs provide functionality and movement when it is in motion. Everyone worldwide cares for their bodies by resting them when needed, eating numerous foods to provide energy, and staying active to live longer. However, over time, many factors can contribute to the body by causing many individuals to develop musculoskeletal issues that can affect a person’s posture and the sensory-motor functions that the body provides to maintain motion and stability. In today’s article, we examine muscle imbalances, how it affects the body’s gait pattern, and how the MET technique can help with muscle imbalances. We provide information about our patients to certified medical providers that offer available therapy techniques like MET (muscle energy techniques) for individuals dealing with chronic conditions associated with muscle imbalances that could affect a person’s gait pattern and lead to pain in the muscles and joints. We encourage each patient appropriately by referring them to our associated medical providers based on their diagnosis results. We accept that education is a spectacular way when asking our providers the most crucial questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., assesses this information as an educational service. Disclaimer
What Are Muscle Imbalances?
Have you been dealing with tight back, shoulders, and hip muscles? Do you feel one side of your body is weaker than the other? Or do you feel unstable when walking? Many people who are experiencing these issues are associated with muscle imbalances that are affecting their bodies. So what are muscle imbalances, and how does it affect the body? Well, according to “Clinical Applications of Neuromuscular Techniques,” written by Leon Chaitow, N.D, D.O, and Judith Walker DeLany, L.M.T., stated that the soft tissues in our bodies are often changed from their normal elastic, pliable, and toned functional status to short, fibrous and weak function in the different muscle groups. Since the body compensates (without any chronic symptoms) to everyday activities, when the body’s muscles and tissues are exhausted, it can cause the symptoms to develop over time, causing pain, muscle restriction, and limited range of motion to the body. Thus, these symptoms often correlate to musculoskeletal disorders, leading to muscle imbalances.
Other issues that can cause muscle imbalances in the body could result from muscle injuries from traumatic forces. Research studies have revealed that repetitive motions from traumatic injuries could result in microtrauma tears to the muscles and tendons, which can develop into muscle-referred pain and increase the risk of chronic joint inflammation. To that point, it can lead to referred pain in different body areas and affect a person’s stability. When the body is dealing with traumatic injuries that affect the muscles over time, many people shift how they walk or change their postures to compensate for the pain, which can change their gait patterns.
How Does It Affect The Body’s Gait Pattern?
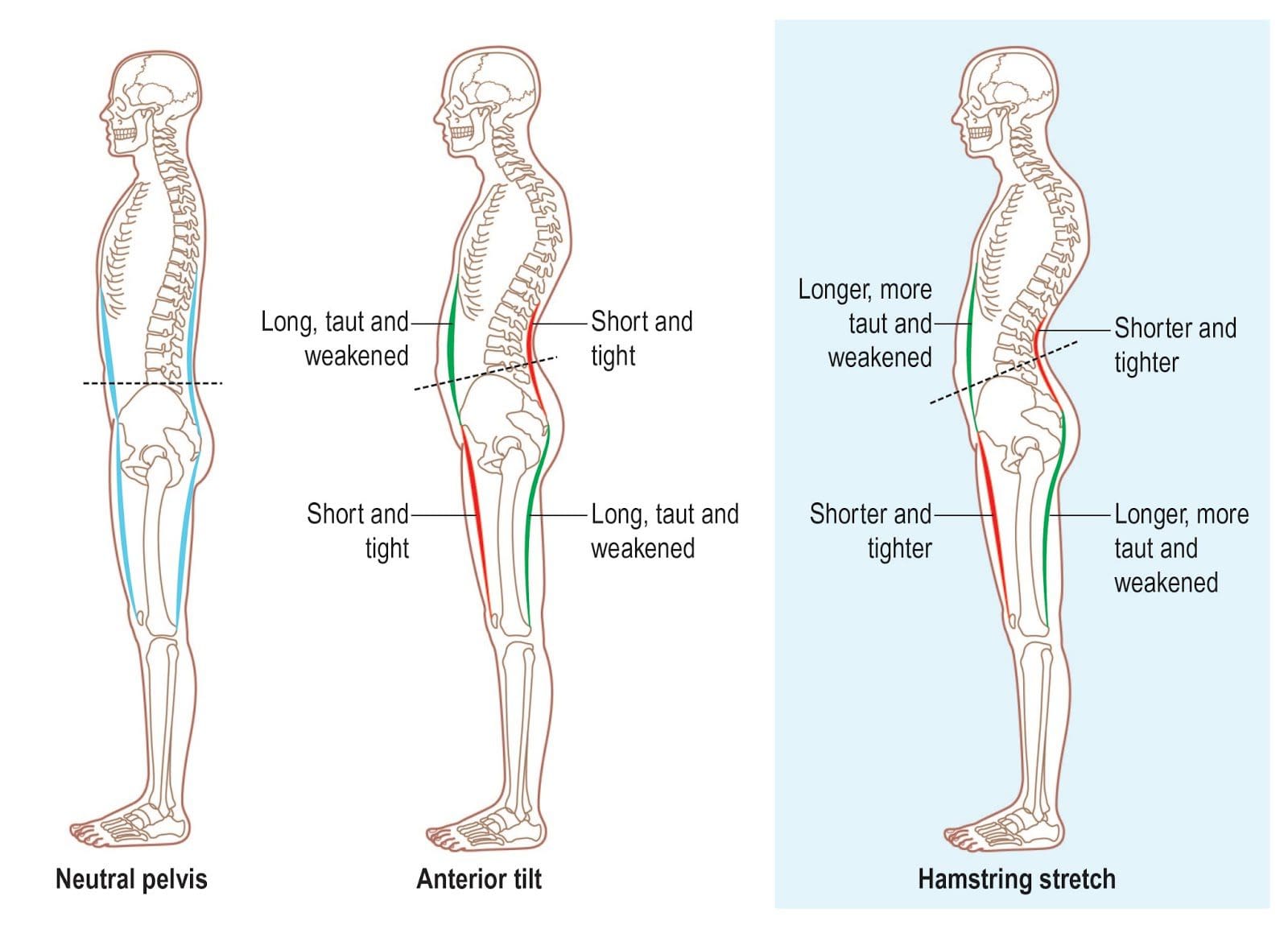
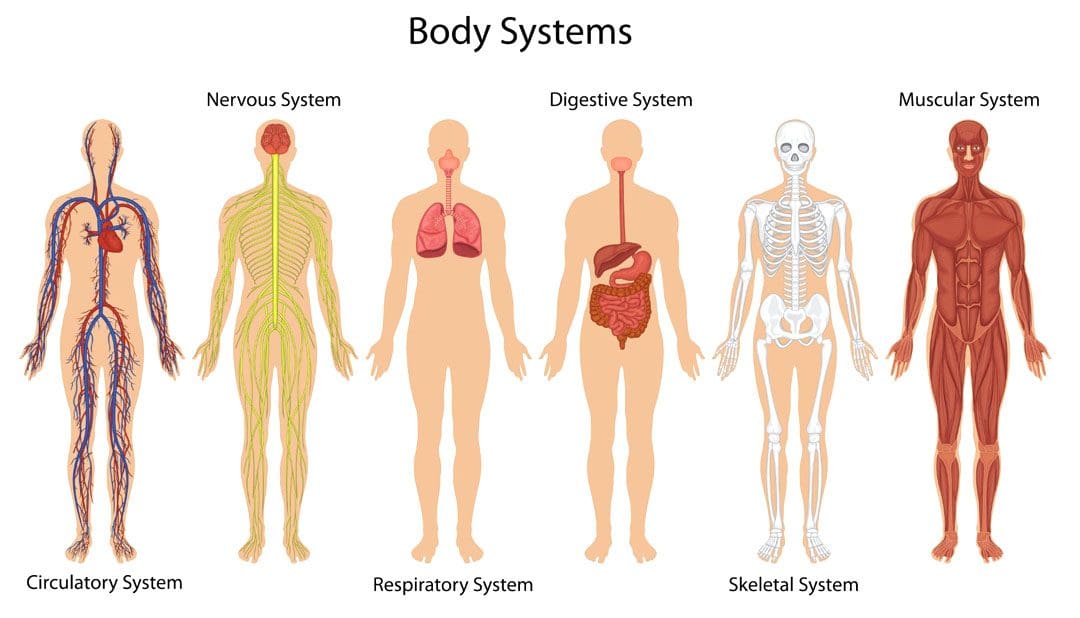
When a person is walking, their entire body is in motion, and over time their posture will change depending on the upper body’s weight bearing down to the hips and lower extremities. Studies reveal that loss of muscle strength can be characterized by musculoskeletal disorders like osteoarthritis that can cause pain symptoms, reduce physical function, decrease range of motion, and muscle/joint instability. So how would muscle imbalances affect the body’s gait pattern? First, we must look at the influences that the neurological and metabolic functions of the central nervous system provide on the musculoskeletal system. The central nervous system sends neuron signals to each muscle group from the upper and lower extremities to allow the individual to walk, run, and do other motor functions. When muscle imbalances are associated with traumatic injuries, it can cause the body to be hunched over over time, causing the short muscles to be tight and the long muscles to be weak. To that point, it can lead to a chain of dysfunctional phases of the gait cycle and its associated symptoms. Some of the signs that can affect a person’s gait pattern include:
Associated joint restriction on the hips
Muscle tension on the pelvis and lower extremities
Muscle tightness in the cervical-thoracic region of the back
Trigger points on the lower extremities causing referred pain
How Muscle Imbalances Associate With Low Back Pain- Video
Have you been dealing with pain in your joints or muscles? Do you find it difficult to walk or carry heavy objects? Or have you been experiencing tight hips and shoulders? Many of these issues are due to muscle imbalances associated with traumatic injuries. The video above explains how muscle imbalances could be related to low back pain. When environmental factors or traumatic forces begin to affect the muscles and joints in the body, it can change a person’s gait pattern (how they walk) and develop into chronic issues affecting the body. When the muscles are imbalanced and cause gait problems, it can lead to muscle and joint pain associated with poor posture and other chronic conditions. When this happens, it can lead to dysfunctional phases of the gait pattern. Luckily there are many treatments and techniques to reduce pain and restore gait function to the body.
How The MET Technique Help With Muscle Imbalances
Going to therapy treatments to restore muscle functionality, enable the body to recover naturally, and reduce the chances of future injuries to come back. When the body is dealing with muscle imbalances, there are many treatments and techniques that many pain specialists, like chiropractic care that are utilized to restore the body and prevent injuries from re-occurring. One of the techniques is called the MET technique (muscle energy technique). The MET technique is a form of manual therapy that uses isometric stretches to reduce pain in the soft tissues and lengthen weak muscles. Studies reveal that when pain specialists use the MET technique combined with other treatments like physical therapy and spinal manipulation, it can help reduce the pain affecting the muscle fibers while restoring the body to normalcy and lengthening tight muscles. When the MET technique is combined with other forms of therapy, it can help stretch and strengthen the weak muscles and allows the individual to be aware of how their posture is being corrected.
Conclusion
It is important to everyone that different factors and injuries could result from muscle imbalances that can affect your posture. Muscle imbalances in the body can lead to unwanted symptoms of muscle weakness, pain, and dysfunctional gait patterns that correlate with musculoskeletal disorders. Going to therapy treatments and incorporating techniques like MET, physical activities, and chiropractic care can help the body be restored and prevent future injuries from returning and affecting a person’s health and wellness.
References
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Joshi, Reema, and Nishita Poojary. “The Effect of Muscle Energy Technique and Posture Correction Exercises on Pain and Function in Patients with Non-Specific Chronic Neck Pain Having Forward Head Posture-a Randomized Controlled Trail.” International Journal of Therapeutic Massage & Bodywork, U.S. National Library of Medicine, 1 June 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9134480/.
Neme, Jamil R. “Balancing Act: Muscle Imbalance Effects on Musculoskeletal Injuries.” Missouri Medicine, U.S. National Library of Medicine, 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9324710/.
Vodička, Tomáš, et al. “Could the Evaluation of Muscle Strength Imbalances Be Used as a Predictor of Total Hip Arthroplasty?” International Journal of Environmental Research and Public Health, U.S. National Library of Medicine, 11 May 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8150769/.
Nutrition and Chiropractic Care: Chiropractic care treats the body as a whole. It can relieve and alleviate ailments from injuries, conditions, or diseases to help maintain optimal health. A treatment plan includes nutrition recommendations to support the body’s systems, reduce inflammation responses, build muscle and bone strength, and maintain chiropractic adjustments.
Nutrition and Chiropractic Care
Individuals can influence musculoskeletal system health by balancing what they consume. If food choices are unhealthy, the benefits of chiropractic may be lessened from the negative effects of unhealthy foods on the body.
Muscle Repair
Muscle injuries are common from normal wear and tear, work, sports, and personal injuries. Calorie-heavy foods can lead to increased weight. Increased weight puts extra stress on the body as it is healing, making the healing process last longer and less effective. A recommended nutritional plan to build muscle strength around the injured areas will supplement chiropractic care.
Foods include sweet potatoes, salmon, eggs, spinach, bananas, nuts, and seeds.
Bone Health
Misalignment, imbalances, and injuries can be caused in part by weakness in various bones.
Calcium is integral in improving bone strength.
Foods high in calcium can benefit chiropractic adjustments by strengthening the skeletal system.
A balanced intake of calcium and magnesium helps build bone strength and decreases the chances of developing osteoporosis.
Magnesium can be found in almonds, spinach, avocado, cashews, and bananas.
Digestion
Chiropractic treatments also help promote healthy digestion by relieving tension in the stomach and helping to restore proper function in the organs and muscles. Regular chiropractic has been shown to reduce symptoms associated with constipation, bloating, diarrhea, nausea, irritable bowel syndrome – IBS, Crohn’s disease, colitis, GERD – Gastroesophageal Reflux Disease, and vomiting.
Foods that help maintain a healthy gut include brown rice, beans, oats, and fruits and vegetables.
Respiratory Health
Breathing problems come in various forms depending on the individual and their case. The ribs, upper chest, and neck muscles all support breathing. Stress can cause rapid and shallow breathing that overworks these muscles. Breathing problems often correlate with other health issues, including back and neck pain, poor digestion, fatigue, and tension headaches. Chiropractic pinpoints subluxations or undue interruption of the nerve signals and corrects any misalignments so that nerve signals flow properly.
Foods that help with lung health include tomatoes, apples, berries, and broccoli.
Nervous System Health
Chiropractic focuses on restoring the body to optimal function so that it can heal through normal nervous system function. Treatment resets the vertebrae into proper alignment, reducing swelling, blockages, and nerve stress, allowing the nervous system to function at full capacity.
Foods that can help are dark chocolate, spinach, avocados, garlic, and asparagus.
Circulatory System
Chiropractic adjustments increase blood circulation. Adjustments and massage loosen the muscles attached to the specific areas, which also promotes the flow and movement of waste in the lymphatic system in and out of specific areas.
Foods that help with circulation include onions, beets, citrus fruits, tomatoes, walnuts, and fatty fish.
Nutrition and chiropractic care go hand in hand. When the body gets the nutrition it needs, it works more efficiently.
An unhealthy diet can cause sluggishness, low energy, and increase inflammatory responses that can lead to chronic conditions. A nutritionist can create a personalized nutrition plan to maximize the benefits as they work together to improve overall health and wellness.
Intermittent Fasting
References
Elma, Ömer, et al. “Chronic Musculoskeletal Pain and Nutrition: Where Are We and Where Are We Heading?.” PM & R: the journal of injury, function, and rehabilitation vol. 12,12 (2020): 1268-1278. doi:10.1002/pmrj.12346
Elma, Ömer, et al. “Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review.” Journal of clinical medicine vol. 9,3 702. 5 Mar. 2020, doi:10.3390/jcm9030702
Holtzman, Denise, and Jeanmarie Burke. “Nutritional counseling in the chiropractic practice: a survey of New York practitioners.” Journal of chiropractic medicine vol. 6,1 (2007): 27-31. doi:10.1016/j.jcme.2007.02.008
Koehler, Karsten, and Clemens Drenowatz. “Integrated Role of Nutrition and Physical Activity for Lifelong Health.” Nutrients vol. 11,7 1437. 26 Jun. 2019, doi:10.3390/nu11071437
Lee, Mi Kyung, et al. “The use of nutritional guidance within chiropractic patient management: a survey of 333 chiropractors from the ACORN practice-based research network.” Chiropractic & manual therapies vol. 26 7. 20 Feb. 2018, doi:10.1186/s12998-018-0175-1
Mangano, Kelsey M et al. “Dietary protein is associated with musculoskeletal health independently of dietary pattern: the Framingham Third Generation Study.” The American journal of clinical nutrition vol. 105,3 (2017): 714-722. doi:10.3945/ajcn.116.136762
Mendonça, Carolina Rodrigues et al. “Effects of Nutritional Interventions in the Control of Musculoskeletal Pain: An Integrative Review.” Nutrients vol. 12,10 3075. 9 Oct. 2020, doi:10.3390/nu12103075
Tajary, Zahra, et al. “Musculoskeletal Pain Is Associated with Dietary Diversity Score among Community-Dwelling Older Adult: A Cross-Sectional Study.” International journal of food science vol. 2022 4228925. 7 Feb. 2022, doi:10.1155/2022/4228925
Many people don’t often realize that stability and balance are two of the most reliable abilities to keep the body from falling, and it is often taken for granted from the earlier stages, where infants and toddlers are learning to stand upright, to adulthood where we are walking, running or performing any physical activities. Our bodies are complex machines comprised of upper and lower portions that provide balance and stability. The lower half of our bodies helps stabilize and balance the upper half weight and allows us to move around. This is known as gait. However, when the body begins to age naturally or chronic issues begin to affect the muscles and cause an imbalance in the lower half, it can lead to many disorders associated with these imbalances. Today’s articles examine what gait is, how gait disturbances are associated with the body, and how the MET technique improves gait. We provide information about our patients to certified medical providers that offer available therapy techniques like MET (muscle energy techniques) for individuals dealing with chronic conditions associated with gait disturbances that could affect a person’s ability to walk. We encourage each patient appropriately by referring them to our associated medical providers based on their diagnosis results. We accept that education is a spectacular way when asking our providers the most crucial questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., assesses this information as an educational service. Disclaimer
What Is Gait?
Have you been dealing with issues when walking for a short or long distance? Do your feet or ankles seem to feel tired or ache when stepping? Or have you been dealing with mobility issues in your hips? Many of these issues are associated with gait and can cause balance disturbances in the body. So what is gait? In the book by Leon Chaitow, N.D, D.O., and Judith Walker DeLany, L.M.T, titled “Clinical Applications of Neuromuscular Techniques,” gait is defined as how you walk and how each lower body section contributes to how you walk. This includes:
Feet
Ankles
Knees
Hips
Spine
The book also mentions how a person progresses from one location to another using muscular action and gravity to make them walk. Two functional units are in a casual relationship contributing to gait: the passenger and locomotor units. The passenger unit consists of the upper extremities, like the head, neck, arms, trunk, and pelvis, to be the center of gravity when moving forward. At the same time, the locomotor unit comprises the pelvis and lower extremities, like the legs, knees, feet, and ankles, to support the weight of the upper extremities and perform structural stability and mobility to make the body move forward.
Gait Disturbances Associated With The Body
So what happens when traumatic factors or natural aging begins to affect the body and causes gait disturbances. Research studies reveal that since gait depends on the interplay of the nervous, musculoskeletal, and cardiorespiratory system which can be influenced by age and other factors that can lead to issues in the lower extremities causing falls and injuries. Many factors can lead to gait disturbances that can affect how a person walks and how it can affect the joints and muscles, which can lead to pain-like symptoms. Additional studies mentioned that gait disorder affects elderly adults, increasing their fall risk and leading to mobility issues in their hips. Muscle shortening and joint health are other issues that can cause gait disturbances in the lower extremities. When the muscles in the lower extremities are tight and weak, it can cause them to be short and be accompanied by joint dysfunction. The health of the joints in the lower extremities depends on the balancing strength of the opposing flexor muscles. When the flexor muscles lose part or all of their function, it can cause the joint to be hyperextended. To that point, it causes abnormal joint stress, corresponding to lower back pain associated with gait disorders affecting a person’s ability to walk and keep their body balanced.
An Overview Of Gait Analysis-Video
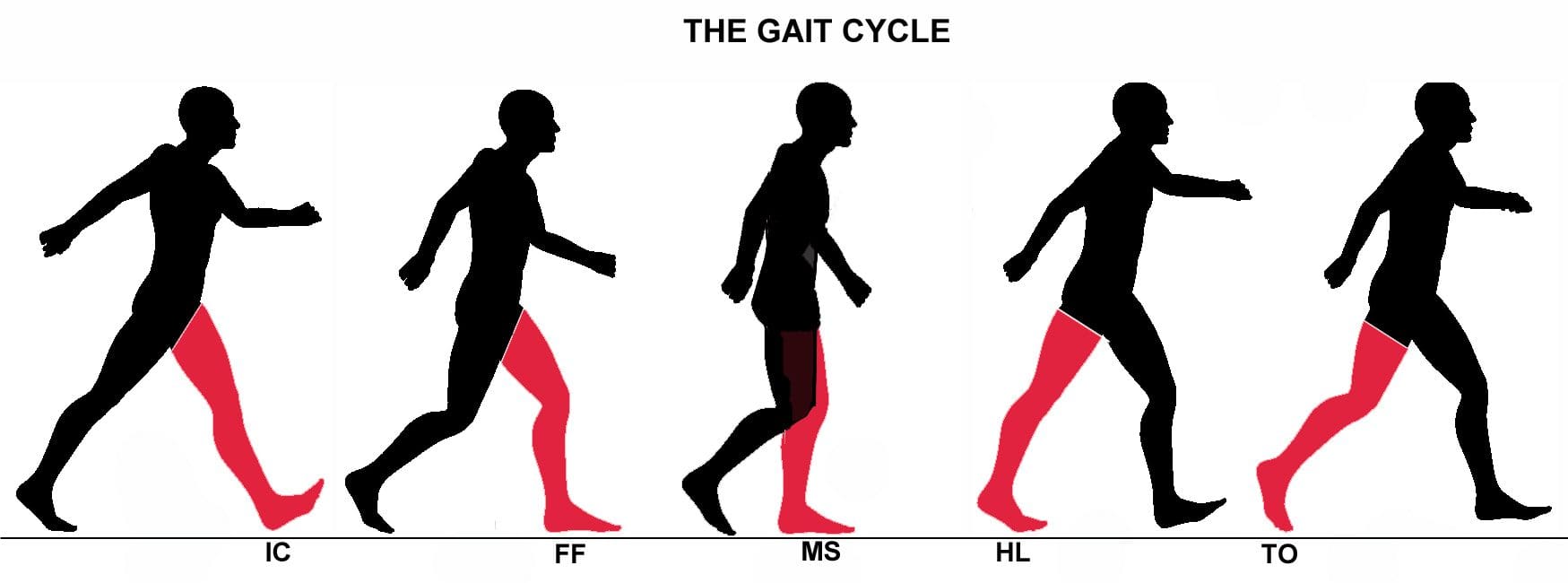
Have you been dealing with mobility issues in your joints? Do you find yourself becoming unstable every time you walk? Or do your leg muscles feel tight? If you have been dealing with these issues, it could be due to a gait problem. Many people have different ways of walking; if there are issues, they can be pointed out in an examination. When there is an issue with gait, it can indicate pain and other revealing problems that can affect the entire body. The video above explains the gait cycle and gait analysis of a person’s walk. Gait analysis is often used in a normal examination to evaluate how a person walks, their body mechanics, and muscle activity to provide insight into the issue. A person’s gait can offer many important clues that doctors and pain specialists can see and identify the problem by developing a treatment plan to improve a person’s gait and reduce pain-like symptoms.
How The MET Technique Improves Gait
So many treatment plans can effectively improve balance and gait disorders in the body. Many pain specialists like chiropractors use manual spinal manipulation to re-align the spine to loosen stiff joints that may have contributed to imbalances in the lower extremities. MET (muscle energy technique) and physical therapy can help stretch the tight muscles and strengthen the muscle groups affected. MET and other approaches to improve gait allow many individuals to regain their stamina and adopt new strategies for their posture and movement. These therapy treatments will enable a person to feel more confident and more aware of how they walk while providing muscle strength to the affected muscles to prevent fatigue and decrease the chances of injuries in the future, as studies reveal.
Conclusion
Walking is determined by a person’s gait and how they move in different scenarios. Our bodies are comprised of upper and lower portions that correspond with gait and allow us stability and balance when we are in motion. When various issues like traumatic factors or just normal aging affect the body, the joints and muscles can cause problems with a person’s gait, leading to balance issues and fall injuries. Incorporating treatment plans to improve gait can help prevent future chances of injuries and help stretch and strengthen the affected muscles while loosening up stiff joints. This allows a person to regain their balance and improve stability in their bodies.
References
Baker, Jessica M. “Gait Disorders.” The American Journal of Medicine, U.S. National Library of Medicine, 27 Dec. 2017, https://pubmed.ncbi.nlm.nih.gov/29288631/.
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Pirker, Walter, and Regina Katzenschlager. “Gait Disorders in Adults and the Elderly : A Clinical Guide.” Wiener Klinische Wochenschrift, U.S. National Library of Medicine, Feb. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5318488/.
Van Abbema, Renske, et al. “What Type, or Combination of Exercise Can Improve Preferred Gait Speed in Older Adults? A Meta-Analysis.” BMC Geriatrics, U.S. National Library of Medicine, 1 July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4488060/.
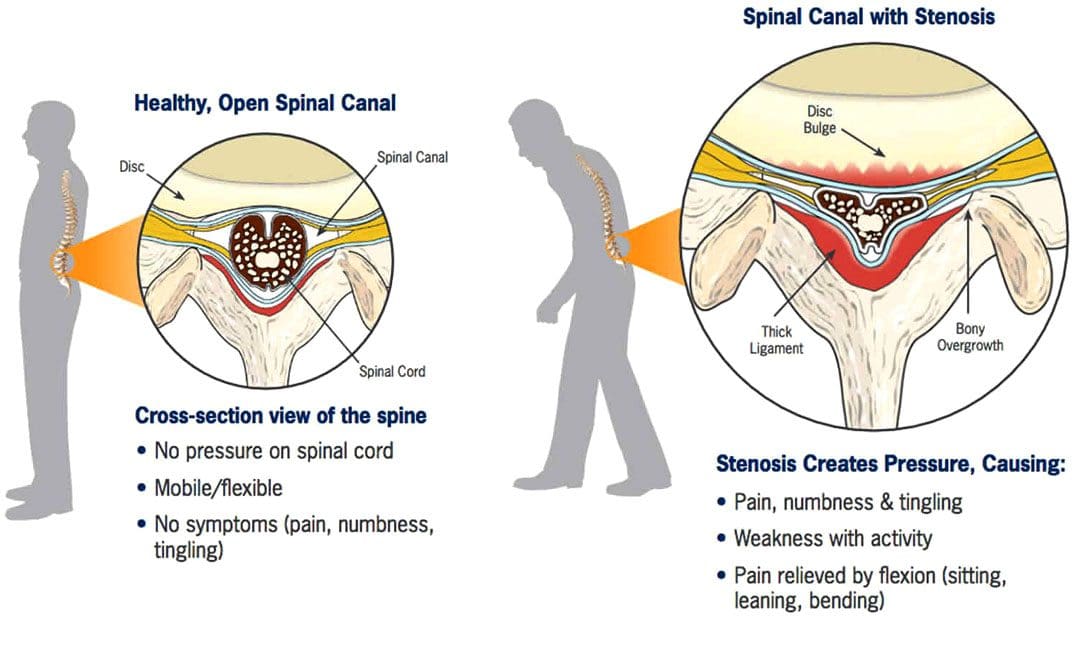
Spinal Stenosis Walking Issues:Stenosis means a narrowing. Spinal stenosis can happen in any spine region, but the neck and lower back are the most common locations. The spinal canal becomes narrower and can cause the nerves to become compressed, pinched, and irritated and can extend from the lumbar spine through the hips, buttocks, legs, and feet. Individuals with lumbar spinal stenosis may have difficulty walking caused by sensations of discomfort like numbness, electrical shocks, and pain, requiring the need to lean forward to relieve pressure and symptoms. Additionally, symptoms are likely to worsen the longer the walk. Chiropractic treatment can treat spinal stenosis because it corrects and re-aligns the spine, thus reducing pressure on the spinal cord, joints, and nerve roots.
Spinal Stenosis Walking Issues
The spine is made up of interlocking vertebrae. The regions are cervical, thoracic, lumbar, and sacral bones with a foramen opening. These openings form the protective tunnel/spinal canal surrounding the spinal cord. The spinal cord is a group of nerves that run through the tunnel. The narrowing suffocates the nerves supplying the lower extremities that can influence walking activity.
Symptoms
There may be no symptoms with early lumbar spinal stenosis. Most individuals develop symptoms gradually and may begin to notice them while walking or standing. These can include:
Lower back pressure sensations when standing upright or walking.
Leg numbness, tingling, weakness, burning, and/or cramping.
Muscle weakness.
Persistent pain in the back, hips, buttocks, or legs while walking.
Difficulty lifting the top part of the foot – known as drop foot.
Loss of sensation in the feet.
A weak foot that drops/slaps down when walking.
Loss of sexual ability.
In more serious cases, severe numbness, bladder problems, and inability to stand.
Individuals begin to lean forward when symptoms start, bringing relief by reducing the pressure on the nerves. However, constantly leaning forward leads to other posture and health problems.
Diagnosis
A doctor or chiropractor will ask questions about symptoms and medical history and perform a complete physical examination to diagnose lumbar spinal stenosis. During the physical examination, a healthcare provider will look for signs, such as loss of sensation, weakness, and abnormal reflexes.
Tests:
X-rays of the lumbar spine may show bone growths called spurs that push on spinal nerves and/or narrowing of the spinal canal.
Imaging tests – A CT or MRI scan can provide a detailed look at the spinal canal and nerve structures.
Other studies include – bone scans, myelogram, which is a CT scan that uses a color dye, and EMG, which is an electrical test of muscle activity.
Chiropractic Treatment
Chiropractic care combined with physical therapy is a tried-and-true treatment for spinal stenosis. A chiropractic treatment plan can include targeted and passive exercise programs. Targeted exercises involve strengthening the core and back muscles. Passive treatments include hot and cold therapy, massage, decompression, and electrical stimulation. The objective of chiropractic therapy is to:
Strengthen muscles in the core and legs
Correct posture and body mechanics.
Improve mobility.
Maintain ability to perform day-to-day activities.
Recommend stretches.
Educate on how to keep the spine and back muscles safe.
Train on using devices like a back brace, cane, or walker properly.
Advise about shoe inserts and splints.
Suggest work and home environment modifications, such as ergonomics and cushions.
Chiropractic Relief
References
Conway, Justin, et al. “Walking assessment in people with lumbar spinal stenosis: capacity, performance, and self-report measures.” The spine journal: official North American Spine Society journal vol. 11,9 (2011): 816-23. doi:10.1016/j.spinee.2010.10.019
Lurie, Jon, and Christy Tomkins-Lane. “Management of lumbar spinal stenosis.” BMJ (Clinical research ed.) vol. 352 h6234. 4 Jan. 2016, doi:10.1136/bmj.h6234
Macedo, Luciana Gazzi, et al. “Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review.” Physical therapy vol. 93,12 (2013): 1646-60. doi:10.2522/ptj.20120379
Tomkins-Lane, Christy C et al. “Predictors of walking performance and walking capacity in people with lumbar spinal stenosis, low back pain, and asymptomatic controls.” Archives of physical medicine and rehabilitation vol. 93,4 (2012): 647-53. doi:10.1016/j.apmr.2011.09.023
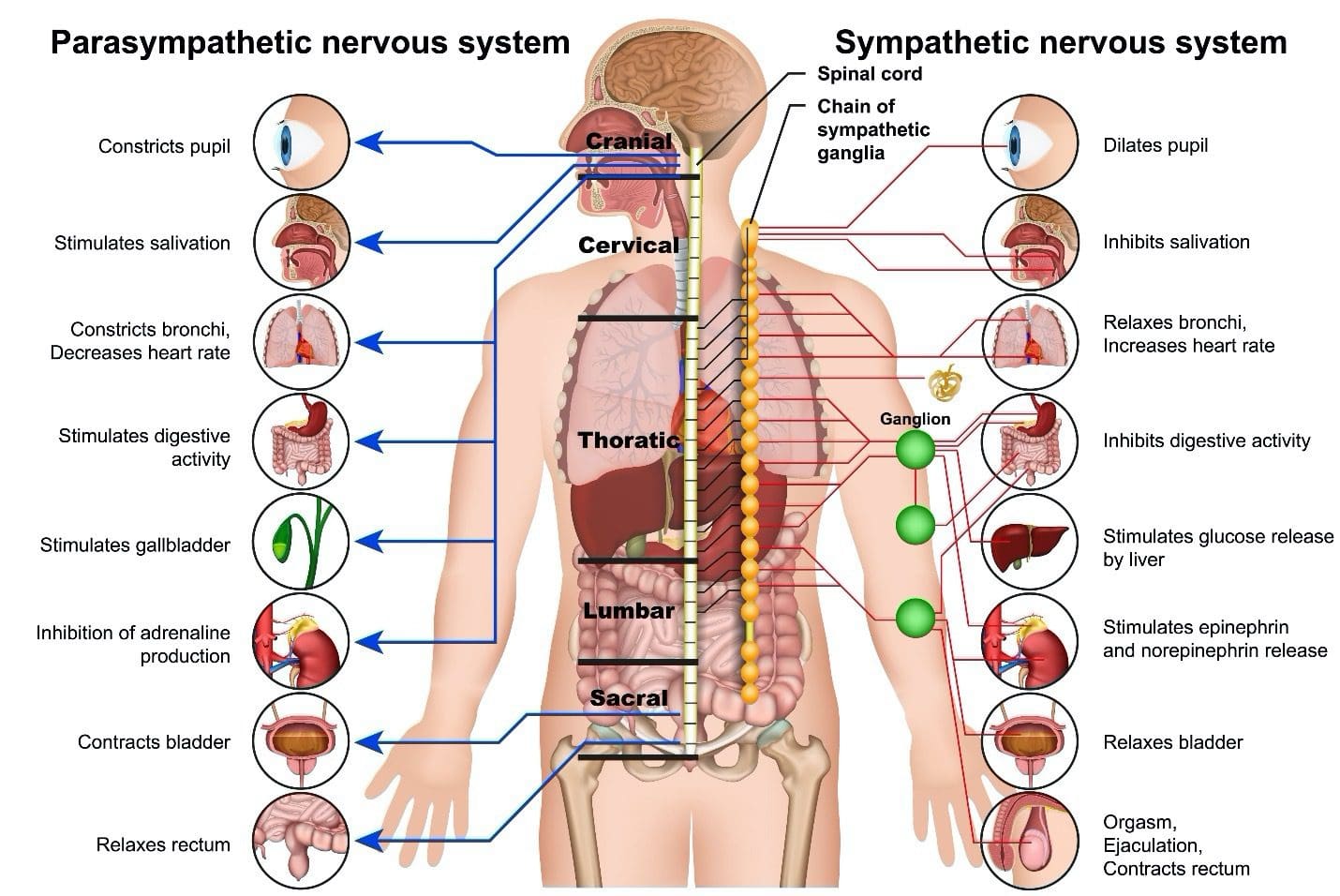
The nervous system is a network of roads that feed into highways that connect to an interstate system. The roads are the nerves that innervate the muscles and the extremities; the interstate is the spinal cord. When the system works optimally, the nerves consistently transmit signals/messages to and from the brain without any problems. The signals travel back and forth, and the traffic flows smoothly. When the activities of these nerves and cells get disrupted, the central nervous system fails to perform basic functions that can cause musculoskeletal issues, conditions, and CNS diseases. Keeping the nervous system strong can be done by adopting ways to maintain health and function.
The Nervous System
The system regulates and coordinates body activities and is made up of two major divisions, these include the following:
Central nervous system – consists of the brain and spinal cord.
Peripheral nervous system – consists of all other neural elements, including the peripheral and autonomic nerves.
The principal organs of the nervous system include:
Brain
Spinal cord
Eyes
Ears
Sensory taste organs
Sensory smell organs
Sensory receptors are located in the muscles, joints, skin, and other areas throughout the body.
A complex network of nerves, the nervous system reacts to internal and external stimuli through several physical actions to maintain vital bodily functions. These include:
The symptoms of a nervous system disorder may present like other medical conditions or problems. Always see a professional healthcare provider for proper diagnosis.
Keeping the Nervous System Strong
Nutrition To Transmit Signals
Nerves need minerals, proteins, and vitamins to send electrical impulses. Foods that contain these nutrients include:
Calcium — regulates the generated and transmitted electrical impulses. Milk, leafy greens and eggs are rich sources of calcium.
Potassium – bananas, oranges, pomegranates, and prunes, are good sources of potassium.
Dark chocolate contains tryptophan, an amino acid that produces and maintains neurotransmitters.
Vitamin B — Vitamins B1, B2, and B6 assist the nerves in sending impulses from the brain to the body.
B Vitamins Provide Nerve Protection
A myelin sheath covers the nerves for protection and provides insulation for transmitting. Worn-out or damaged myelin sheaths have been associated with illnesses like Alzheimer’s. Vitamin B12 helps repair damaged nerves and regenerate fibers. It is found in beef, poultry, eggs, and seafood.
Folate or vitamin B9 promotes Schwann cell proliferation, migration, and production of nerve growth factor. This vitamin is found in spinach, pomegranates, and beets.
Stretching and Breathing
Stress produces the hormone cortisol. Constant production of cortisol affects the nervous system, which can affect reflexes, concentration, and memory. Stretching the body and learning breathing exercises and relaxation techniques activates the part of the nervous system responsible for breathing and heart rate, decreasing cortisol levels.
Chiropractic Care and Functional Medicine
The spinal cord has multiple functions in restoring, rejuvenating, and keeping the nervous system strong. Chiropractic care has a highly responsive therapeutic effect on the nervous system because of its focus on the spine. Spinal decompression, traction, soft tissue manipulation, and other treatments help regulate and restore the function of the nervous system. Chiropractic benefits:
Reduces or eliminates pain.
Regulates respiration.
Lowers heart rate.
Improves the quality of sleep.
Increases energy.
Improves digestive function.
Improves cognition and clarity.
Improves balance and coordination.
Increases flexibility and mobility.
Reduces or eliminates headaches and migraines.
Hyperhomocysteinemia
References
Archibald, Lennox K., and Ronald G. Quisling. “Central Nervous System Infections.” Textbook of Neurointensive Care 427–517. 7 May. 2013, doi:10.1007/978-1-4471-5226-2_22
Bhagavati, Satyakam. “Autoimmune Disorders of the Nervous System: Pathophysiology, Clinical Features, and Therapy.” Frontiers in neurology vol. 12 664664. 14 Apr. 2021, doi:10.3389/fneur.2021.664664
Gyer, Giles, et al. “Spinal manipulation therapy: Is it all about the brain? A current review of the neurophysiological effects of manipulation.” Journal of integrative medicine vol. 17,5 (2019): 328-337. doi:10.1016/j.joim.2019.05.004
Jessen, Kristján R et al. “Schwann Cells: Development and Role in Nerve Repair.” Cold Spring Harbor perspectives in biology vol. 7,7 a020487. 8 May. 2015, doi:10.1101/cshperspect.a020487
Powers, Scott K et al. “Disease-Induced Skeletal Muscle Atrophy and Fatigue.” Medicine and science in sports and exercise vol. 48,11 (2016): 2307-2319. doi:10.1249/MSS.0000000000000975
The human body has numerous musculoskeletal muscles that allow the host to do various movements without pain or discomfort. Each muscle group has tendons, muscles, ligaments, and connective tissues surrounding the skeletal joint and protecting the skeletal structure. Each muscle group in the body allows different functions, from turning the neck from side to side to enabling the legs to provide motion when walking. Now naturally, the body ages over time, which can lead to muscle weakness in the muscle groups and affect the connective tissues, or various disruptors can develop in a healthy body that can also affect the muscles and connective tissues. Fortunately, the multiple muscle groups and connective tissues are affected by overlapping risk profiles. In that case, there are many treatments and techniques that many pain specialists utilize to restore the body and relieve pain-like symptoms associated with musculoskeletal disorders. Today’s article examines connective tissues, how conditions can affect the connective tissues, and how the MET technique stretches or strengthens the body’s connective tissue. We provide information about our patients to certified medical providers that offer available therapy techniques like MET (muscle energy techniques) for individuals dealing with chronic conditions associated with disorders affecting the body’s connective tissues that can correlate and develop with overlapping pain profiles. We encourage each patient appropriately by referring them to our associated medical providers based on their diagnosis results. We accept that education is a spectacular way when asking our providers the most crucial questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., assesses this information as an educational service. Disclaimer
What Are Connective Tissues?
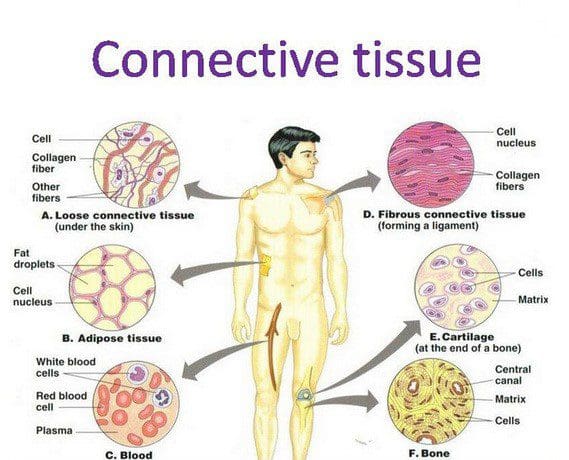
The human body is a multiplex machine that is composed of many tissues that surround the skeletal joints and vital organs with the basic functions that the body produces. Research studies reveal that, as the name has implied, connective tissues in the body refer to the several different body tissues that connect and support the other tissues by binding them to the body. Now there are three different categories that connective tissue can be broken down into:
Loose connective tissue
Dense connective tissue
Specialized connective tissues
These three different connective tissue categories have functions that allow the body to perform properly and provide support to the rest of the musculoskeletal system. The dense connective tissues make up the body’s tendons and ligaments that move the hands and feet while having a higher collagen fiber density. The loose connective tissues help keep the vital organs in place. And finally, the specialized connective tissues are composed of adipose tissues, cartilage, lymphoid tissues, etc. When the body begins to age naturally or is dealing with issues affecting the connective tissues, it can develop musculoskeletal disorders associated with the connective tissue.
Disorders Affecting The Connective Tissues
Have you been experiencing muscle pain or weakness in your body? Do your hands or feet feel tired? Or do you feel stiffness and pain in your joints? Many pain-like symptoms are associated with musculoskeletal disorders affecting the body’s connective tissues. As stated earlier, when the body begins to age naturally, the various muscles in the body can develop into musculoskeletal disorders associated with the connective tissues. Aging can affect connective tissue function as the cartilage from the specialized connective tissues has less elasticity and changes the proteoglycan both quantitatively and qualitatively, according to the book, “Clinical Applications of Neuromuscular Techniques,” written by Leon Chaitow, N.D., D.O., and Judith Walker DeLany, L.M.T. Additional research studies have revealed that environmental factors associated with the body’s immune system can affect the connective tissues. This is known as connective tissue disorder, and it can be comprised of numerous conditions that can affect the immune system and cause overlapping symptoms in the musculoskeletal system. This includes some of the following:
Inflammation in the joints causes them to lock up
Muscle weakness where myofascial entrapment affects the muscle fibers
Fatigue
Vitamin deficiency
An Introduction To MET- Video
Have you been feeling stiffness in your muscles or joints? Does it hurt when you are bending over and lifting heavy objects? Or are you feeling tired constantly? When the body deals with these issues, it can affect more than the muscles and connective tissues. This can lead to symptoms of stiffness and aches in the joints while restricting the range of motion to the muscles. When this happens to the body, many pain specialists utilize MET (muscle energy technique) and relieve those symptoms. Studies reveal that MET is a manual treatment for soft tissue, helping mobilize the joints and stretch tight muscles and fascia to improve circulation to the connective tissues and drain the lymphatic system. The video above introduces how MET is used on the body.
The MET Technique On Connective Tissues
Research studies reveal that since the muscles and joints are being held together by connective tissues, using the MET technique allows pain specialists to stretch the muscles and joints to release tension and other symptoms associated with pain. When pain specialists use the MET technique on the body, it can help strengthen the weaker muscles while paying attention to how short the muscles are affecting the body. While the MET technique can help support the muscles with combined physical therapy, it can help stretch the tight muscles and overworked connective tissues. This allows the body to be restored and get back to normal. Many pain specialists like chiropractic care allow the MET technique to stretch the trapped connective tissues and free the body’s structures to correct postural imbalances.
Conclusion
The body’s connective tissues support each muscle, organ, and skeletal structure. When issues affect the body, the various muscle groups, and connective tissues start to develop overlapping symptoms associated with pain. When pain-like symptoms affect the body, many people will go to a pain specialist and be treated using the MET technique to restore the muscles and body and return to normal.
References
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Kamrani, Payvand, et al. “Anatomy, Connective Tissue.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 24 Jan. 2022, https://www.ncbi.nlm.nih.gov/books/NBK538534/.
Page, Phil. “Current Concepts in Muscle Stretching for Exercise and Rehabilitation.” International Journal of Sports Physical Therapy, U.S. National Library of Medicine, Feb. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3273886/.
Rao, Vijay, and Simon Bowman. “Latest Advances in Connective Tissue Disorders.” Therapeutic Advances in Musculoskeletal Disease, U.S. National Library of Medicine, Aug. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3728978/.
Thomas, Ewan, et al. “The Efficacy of Muscle Energy Techniques in Symptomatic and Asymptomatic Subjects: A Systematic Review.” Chiropractic & Manual Therapies, U.S. National Library of Medicine, 27 Aug. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6710873/.
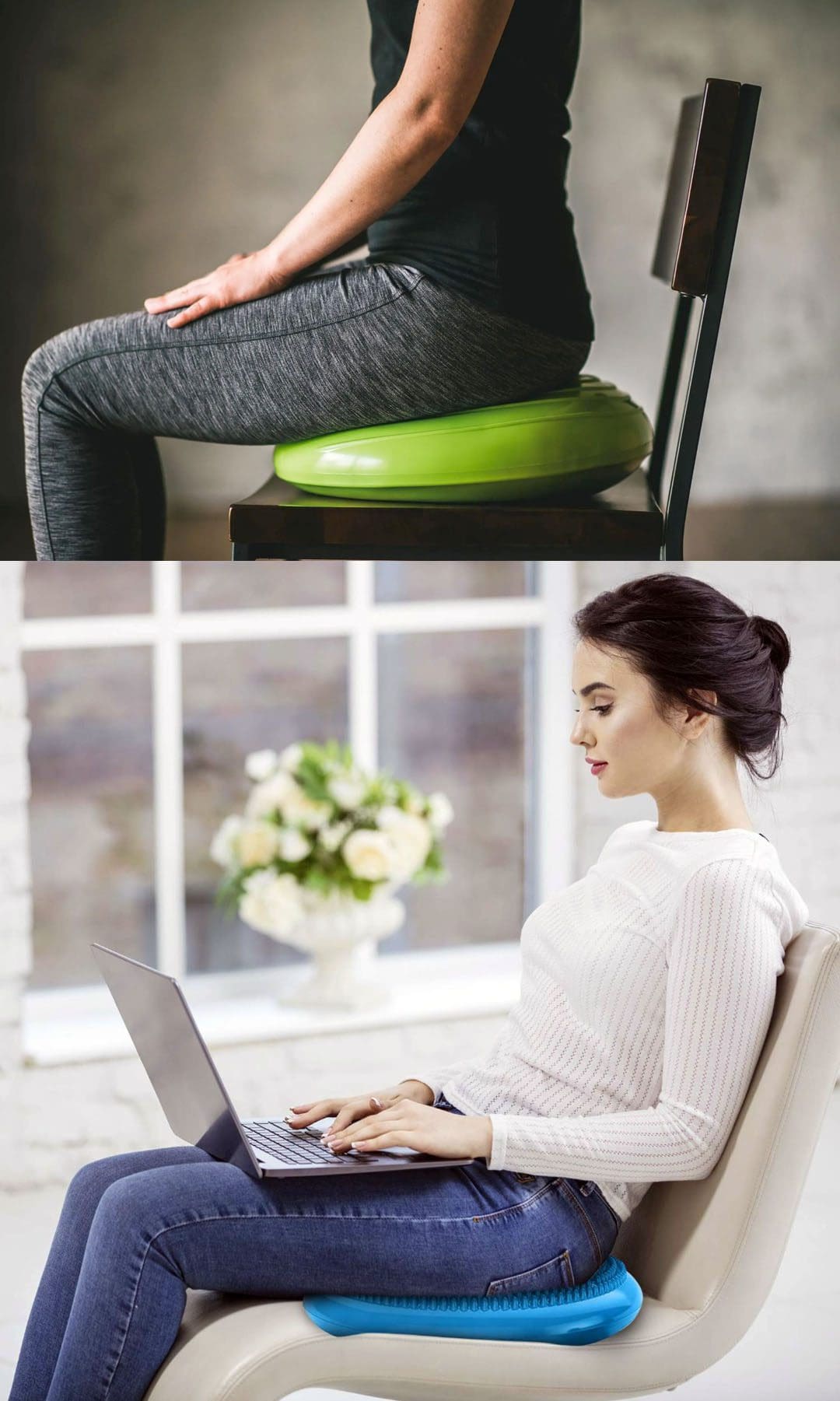
Wobble cushions are small round inflatable support pillows made of a flexible material that can be used to stand and sit on. The cushion creates instability, hence wobble, to engage the lower back, hips, and core muscles. They promote core stability, strengthen muscle tone, and improve balance and body posture. A flexible body helps in injury prevention. At Injury Medical Chiropractic and Functional Medicine Clinic, we utilize innovative techniques and therapies to reduce stress, assist in healing musculoskeletal damage from injuries, disease, or conditions, and keep the spine and whole body healthy.
Wobble Cushions
A common reason for back aches and pains is sitting for long periods. Individuals unintentionally slouch or hunch over as they go through their day, causing strain to the back muscles, gluteal muscles, core muscles, hips, and spine. This causes the lower half of the body to weaken and causes the top muscles to take up the slack to support the torso and lower body.
Muscle Spasms
Muscle spasms can be the acute type that is forceful and involuntary, and chronic sustained stiffness, tightness, cramping, and pain. Lower back discomfort and/or sciatica symptoms vary depending on the cause, location, and severity of the strain or injury. Signs could be dull, burning, or sharp at a single point or over a broad region that could spread into one or both legs. Types of low back discomfort:
Acute symptoms last less than three months. Most individuals with acute episodes will have at least one recurrence.
Recurrent means the acute symptoms return.
Chronic symptoms last longer than three months.
Cushion Benefits
Encouraging active sitting improves posture allowing individuals to sit and stay focused for longer as their body awareness improves, reducing hunching, slumping, slouching, and fidgeting. Other wobble cushion benefits include:
Decreased muscle stress and strain on the joints and ligaments, which improves proprioceptive sense or body awareness.
Increases blood circulation and oxygenation throughout the body.
Helps rehydrate the discs and circulate spinal fluid. Spinal discs do not have a direct blood supply; therefore, movement is required to pump and circulate healthy fluids.
Allows more flexibility in the spine, hips, and core muscles.
Improves overall posture.
The purpose of wobble cushions is not to provide comfort. They are supposed to be uncomfortable and unstable to make the individual sit up straight. The cushion can be placed on a chair or the floor to effectively practice balancing without putting pressure on the back, knees, or feet. They can also be used for practicing standing balance. Various factors to consider when looking for a cushion include:
Stability
Comfort
Resilience
Alignment
All play a role in determining the best option.
Discussing options with a doctor or chiropractor is recommended to ensure that the cushion meets your needs and preferences.
Spinal Hygiene
References
Alrwaily, Muhammad, et al. “Stabilization exercises combined with neuromuscular electrical stimulation for patients with chronic low back pain: a randomized controlled trial.” Brazilian journal of physical therapy vol. 23,6 (2019): 506-515. doi:10.1016/j.bjpt.2018.10.003
Haksever, Bunyamin et al. “The Dynamic Innovative Balance System Improves Balance Ability: A Single-Blind, Randomized Controlled Study.” International journal of sports physical therapy vol. 16,4 1025-1032. 1 Aug. 2021, doi:10.26603/001c.25756
Honert, Eric C, and Karl E Zelik. “Foot and shoe responsible for the majority of soft tissue work in the early stance of walking.” Human movement science vol. 64 (2019): 191-202. doi:10.1016/j.humov.2019.01.008
Ostelo, Raymond Wjg. “Physiotherapy management of sciatica.” Journal of physiotherapy vol. 66,2 (2020): 83-88. doi:10.1016/j.jphys.2020.03.005
Shahvarpour, A et al. “Active-passive biodynamics of the human trunk when seated on a wobble chair.” Journal of biomechanics vol. 49,6 (2016): 939-945. doi:10.1016/j.jbiomech.2016.01.042
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine