Could older individuals who do not have symptoms of shoulder pain or loss of shoulder and arm function have a rotator cuff tear?
Rotator Cuff Tear Physical Therapy
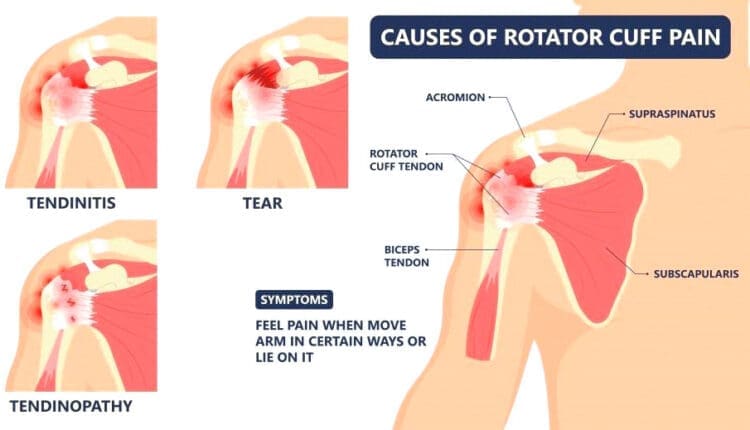
A rotator cuff tear is a common injury to the four muscles and tendons surrounding and stabilizing the shoulder joint. Studies have shown that (Geary M. B., & Elfar J. C. 2015)
30% of those under the age of 70
70% of those over age 80 have a rotator cuff tear.
Physical therapy is often recommended as a first-line initial treatment for rotator cuff pain. In most cases, a rotator cuff tear will not need surgical treatment. Determining when surgery is necessary depends on several factors a patient can discuss with their healthcare provider.
Causes
Overuse and repetitive motions
Trauma (e.g., falls, collisions)
Age-related degeneration
Symptoms
Shoulder pain, especially with overhead or rotational movements
Weakness and difficulty raising the arm
Clicking or grinding sounds in the shoulder
Limited range of motion
Treatment
The goal of physical therapy for a rotator cuff tear is not necessarily to heal the torn tendon but to relieve pain and improve strength by reducing inflammation and restoring shoulder joint mechanics. This is achieved through physical therapy, ice application, anti-inflammatory treatments like medications, and cortisone injections.
Physical Therapy
The goal of physical therapy is to improve the function of the muscles that surround the shoulder. Physical therapy targets the smaller muscles around the shoulder that are commonly neglected. By strengthening these muscles, the treatment can help compensate for damaged tendons and improve the mechanics of the shoulder joint. A chiropractic physical therapy team will develop a personalized exercise program. Generally, rehabilitation will start with gentle range of motion exercises that can be accomplished using the arms to lift a mobility stick/wand overhead.
Shoulder Pulleys
These improve shoulder range of motion and flexibility.
Isometric Exercises
These exercises are for the rotator cuff muscles and may then be started.
This exercise can improve the contracting of the muscles around the shoulder and offer more support to the shoulder joint.
Scapular Stabilization Exercises
These can also be done to improve the muscles surrounding the shoulder blade’s function.
This can help improve how the shoulder joint, arm, and scapulae move together when using the arm.
Advanced Strengthening
Advanced exercises can be done with a dumbbell or resistance band.
Consult your healthcare provider or physical therapist before starting these or any other exercises for a rotator cuff tear. Doing exercises correctly prevents further pain, injury, or shoulder problems. Specific, focused exercises can help expedite and regain normal shoulder function.
Injury Medical Chiropractic and Functional Medicine Clinic
The prognosis for rotator cuff tears depends on the severity of the tear and the individual’s overall health. With proper treatment, most people can regain the full function of their shoulders. However, some may experience ongoing pain or limitations in severe cases. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Shoulder Pain Chiropractic Treatment
References
Geary, M. B., & Elfar, J. C. (2015). Rotator Cuff Tears in the Elderly Patients. Geriatric orthopaedic surgery & rehabilitation, 6(3), 220–224. doi.org/10.1177/2151458515583895
An annular fissure is caused by age-related changes to the spine, which often do not cause symptoms but can cause back pain. Can understanding the causes help individuals manage lower back pain and help healthcare providers develop an effective treatment program?
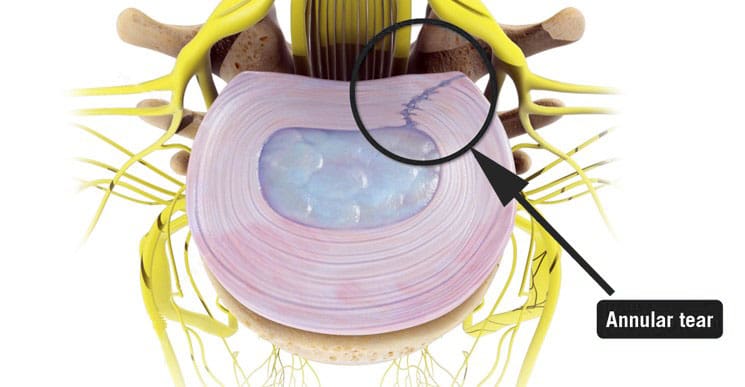
Annular Fissure
An annular fissure is a discogenic condition that affects the spine and can cause lower back pain. Also called an annular tear, it’s usually a wear-and-tear condition that happens over time rather than a condition caused by trauma. It usually happens when the fibers that make up the annulus or the tough outer covering of the intervertebral disc break or separate. To manage it, healthcare providers may recommend:
Making lifestyle changes.
Staying aware of how you go about daily activities and take steps to make adjustments, such as being mindful of unhealthy posture.
Start doing exercises that help make the back stronger.
Medical care if pain and other symptoms need to be managed.
Symptoms
Lower back pain may be a sign of an annular fissure, or there may be no symptoms. Symptoms can include:
Pain
Weakness
Numbness
Electrical sensations travel down one leg or arm if a cervical/neck tear is present.
Numbness and weakness may be caused by the nerves getting irritated or compressed near an annular tear. (Stadnik, T. W. et al., 1998)
These symptoms can also be similar to a herniated disc, which can be a complication of an annular fissure.
However, studies have shown that annular tears and herniated discs often go unnoticed because they have few obvious symptoms. (Jarvik, J. G. et al., 2005)
Annulus Function
The annulus comprises several layers of tough fibers/fibrocartilage that surround, contain, and protect the soft, liquid nucleus inside the disc. The layers of the annulus fibrosus crisscross to provide support. The nucleus is a shock absorber cushions the body’s weight on the spinal joints when sitting, standing, or moving. Its strength also allows the disc to buffer the jolts and jars it experiences. It also helps maintain the integrity of the intervertebral joint by supporting the space between the two vertebrae. When an annular fissure occurs, the fibers separate or tear off from insertion on the nearby spinal bone. A fissure can also be a break in the fibers of one or more layers. (Jarvik, J. G. et al., 2005)
Causes
An annular tear is not the standard term medical professionals use to describe or diagnose a fissure because the word tear suggests that trauma has led to the separation or break in the fibers. While an injury can cause an annular fissure, it’s usually caused by long-term wear and tear. (Guterl, C. C. et al., 2013) The tears are typically caused by age-related degenerative changes in the disc, which can also lead to degeneration in other areas of the spine. Wear and tear are caused by annular fissures due to an individual’s daily living habits, such as sitting, standing, walking, climbing stairs, and performing other routine movements.
Treatment
While a large annular fissure is not likely to improve without treatment, a small one could heal independently. However, once an area has torn, it becomes more likely to continue tearing. (Virginia Spine Institute, N.D.) Conservative treatment is usually enough to control pain and symptoms. Physical therapy and anti-inflammatory medication are the first line of treatment. (Cheng, J. et al., 2019) Medication can be over-the-counter or prescription. Physical therapy treatment includes exercises, traction, and other therapies. If these do not help with the symptoms, the provider may suggest a steroid injection to reduce inflammation and pain. It can take three to six months to recover from degenerative disc problems if doing a standard treatment plan that includes rest, low-impact therapy exercises, and anti-inflammatory treatments. (Cheng, J. et al., 2019)
In severe cases, surgery may be recommended, including disc replacement surgery. An annular tear is not a reason to have disc replacement surgery alone; it is only when there are degenerative changes in the vertebral disc that surgery might be necessary. (Yue, J. J. et al., 2012)
Improving Body Alignment
Not paying attention and being aware of how the body performs everyday activities can, over time, set the stage for an annular fissure and other musculoskeletal injuries. However, fixing daily movement and posture habits to prevent injuries can be done through simple adjustments. For example, strengthening the core and back muscles can reduce pressure on the spine and help prevent injuries. (Camp, C. L. et al., 2016) The idea is to improve joint and overall body alignment. Activities can include:
Strength training
Walking
Pilates classes
Yoga
Tai chi
Somatic exercises
These activities help with muscle balance and joint alignment, which are recommended prevention strategies that physical therapists use when working with individuals who need help with spinal problems.
Visiting a chiropractic and physical therapy team can help treat injuries and chronic pain syndromes, relieve pain, resolve musculoskeletal issues, and prevent future symptoms. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized care program for each patient through an integrated approach to treating injuries, improving flexibility, mobility, and agility to help return to normal and optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Back Pain Specialist
References
Stadnik, T. W., Lee, R. R., Coen, H. L., Neirynck, E. C., Buisseret, T. S., & Osteaux, M. J. (1998). Annular tears and disk herniation: prevalence and contrast enhancement on MR images in the absence of low back pain or sciatica. Radiology, 206(1), 49–55. doi.org/10.1148/radiology.206.1.9423651
Jarvik, J. G., Hollingworth, W., Heagerty, P. J., Haynor, D. R., Boyko, E. J., & Deyo, R. A. (2005). Three-year incidence of low back pain in an initially asymptomatic cohort: clinical and imaging risk factors. Spine, 30(13), 1541–1549. doi.org/10.1097/01.brs.0000167536.60002.87
Guterl, C. C., See, E. Y., Blanquer, S. B., Pandit, A., Ferguson, S. J., Benneker, L. M., Grijpma, D. W., Sakai, D., Eglin, D., Alini, M., Iatridis, J. C., & Grad, S. (2013). Challenges and strategies in the repair of ruptured annulus fibrosus. European cells & materials, 25, 1–21. doi.org/10.22203/ecm.v025a01
Cheng, J., Santiago, K. A., Nguyen, J. T., Solomon, J. L., & Lutz, G. E. (2019). Treatment of symptomatic degenerative intervertebral discs with autologous platelet-rich plasma: follow-up at 5-9 years. Regenerative medicine, 14(9), 831–840. doi.org/10.2217/rme-2019-0040
Yue, J. J., Telles, C., Schlösser, T. P., Hermenau, S., Ramachandran, R., & Long, W. D., 3rd (2012). Do presence and location of annular tear influence clinical outcome after lumbar total disc arthroplasty? A prospective 1-year follow-up study. International journal of spine surgery, 6, 13–17. doi.org/10.1016/j.ijsp.2011.09.001
Camp, C. L., Conti, M. S., Sgroi, T., Cammisa, F. P., & Dines, J. S. (2016). Epidemiology, Treatment, and Prevention of Lumbar Spine Injuries in Major League Baseball Players. American journal of orthopedics (Belle Mead, N.J.), 45(3), 137–143.
Individuals suffering from a jammed finger: Can knowing the signs and symptoms of a finger that is not broken or dislocated allow for at-home treatment and when to see a healthcare provider?
Jammed Finger Injury
A jammed finger, also known as a sprained finger, is a common injury when the tip of a finger is forcefully pushed toward the hand, causing the joint to become compressed. This can cause pain and swelling in one or more fingers or finger joints and cause ligaments to stretch, sprain, or tear. (American Society for Surgery of the Hand. 2015) A jammed finger can often heal with icing, resting, and taping. This is often enough to allow it to heal in a week or two if no fractures or dislocations are present. (Carruthers, K. H. et al., 2016) While painful, it should be able to move. However, if the finger cannot wiggle, it may be broken or dislocated and require X-rays, as a broken finger or joint dislocation can take months to heal.
Treatment
Treatment consists of icing, testing, taping, resting, seeing a chiropractor or osteopath, and progressive regular use to regain strength and ability.
Ice
The first step is icing the injury and keeping it elevated.
Use an ice pack or a bag of frozen vegetables wrapped in a towel.
Ice the finger in 15-minute intervals.
Take the ice off and wait until the finger returns to its normal temperature before re-icing.
Do not ice a jammed finger for over three 15-minute intervals in one hour.
Try To Move The Affected Finger
If the jammed finger does not move easily or the pain gets worse when trying to move it, you need to see a healthcare provider and have an X-ray to check for a bone fracture or dislocation. (American Society for Surgery of the Hand. 2015)
Try to move the finger slightly after swelling, and the pain subsides.
If the injury is mild, the finger should move with little discomfort for a short time.
Tape and Rest
If the jammed finger is not broken or dislocated, it can be taped to the finger next to it to keep it from moving, known as buddy taping. (Won S. H. et al., 2014)
Medical-grade tape and gauze between the fingers should be used to prevent blisters and moisture while healing.
A healthcare provider may suggest a finger splint to keep the jammed finger lined up with the other fingers.
A splint can also help prevent a jammed finger from re-injury.
Resting and Healing
A jammed finger must be kept still to heal at first, but eventually, it needs to move and flex to build strength and flexibility.
Targeted physical therapy exercises can be helpful for recovery.
A primary care provider might be able to refer a physical therapist to ensure the finger has a healthy range of motion and circulation as it heals.
A chiropractor or osteopath can also provide recommendations for helping rehabilitate the finger, hand, and arm to normal function.
Easing The Finger Back to Normal
Depending on the extent of the injury, the finger and hand can be sore and swollen for a few days or weeks.
It can take some time to start feeling normal.
Once the healing process begins, individuals will want to return to using it normally.
Avoiding using a jammed finger will cause it to lose strength, which can, over time, further weaken it and increase the risk of re-injury.
If the pain and swelling persist, see a healthcare provider to get it checked for a possible fracture, dislocation, or other complication as soon as possible, as these injuries are harder to treat if the individual waits too long. (University of Utah Health, 2021)
At Injury Medical Chiropractic and Functional Medicine Clinic, we passionately focus on treating patients’ injuries and chronic pain syndromes and improving ability through flexibility, mobility, and agility programs tailored to the individual. Our providers use an integrated approach to create personalized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine protocols. Our goal is to relieve pain naturally by restoring health and function to the body. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective clinical treatments.
Carruthers, K. H., Skie, M., & Jain, M. (2016). Jam Injuries of the Finger: Diagnosis and Management of Injuries to the Interphalangeal Joints Across Multiple Sports and Levels of Experience. Sports health, 8(5), 469–478. doi.org/10.1177/1941738116658643
Won, S. H., Lee, S., Chung, C. Y., Lee, K. M., Sung, K. H., Kim, T. G., Choi, Y., Lee, S. H., Kwon, D. G., Ha, J. H., Lee, S. Y., & Park, M. S. (2014). Buddy taping: is it a safe method for treatment of finger and toe injuries?. Clinics in orthopedic surgery, 6(1), 26–31. doi.org/10.4055/cios.2014.6.1.26
For athletes and sports enthusiasts, a torn triceps can be a serious injury. Can knowing their symptoms, causes, risk factors, and potential complications help healthcare providers develop an effective treatment plan?
Torn Triceps Injury
The triceps is the muscle on the back of the upper arm that allows the elbow to straighten. Fortunately, triceps tears are uncommon, but they can be serious. The injury affects men more often than women and usually occurs from trauma, sports, and/or exercise activities. Depending on the extent and severity of the injury, a torn triceps injury can require splinting, physical therapy, and possibly surgery to regain movement and strength. Recovery after a triceps tear typically lasts around six months. (The Ohio State University Wexner Medical Center. 2021)
Anatomy
The triceps brachii muscle, or triceps, runs along the back of the upper arm. It is named tri- because it has three heads – the long, medial, and lateral head. (Sendic G. 2023) The triceps originates at the shoulder and attaches to the shoulder blade/scapula and upper arm bone/humerus. At the bottom, it attaches to the point of the elbow. This is the bone on the pinky side of the forearm, known as the ulna. The triceps cause movement at the shoulder and the elbow joint. At the shoulder, it performs extension or backward movement of the arm and adduction or moving the arm toward the body. The main function of this muscle is at the elbow, where it performs extension or straightening of the elbow. The triceps work the opposite of the biceps muscle on the front of the upper arm, which conducts flexion or bending of the elbow.
Triceps Tear
Tears can occur anywhere along the length of a muscle or tendon, which is the structure that attaches the muscle to the bones. Triceps tears commonly occur in the tendon connecting the triceps to the back of the elbow. Muscle and tendon tears are graded from 1 to 3 based on severity. (Alberto Grassi et al., 2016)
Grade 1 Mild
These small tears cause pain that worsens with movement.
There is some swelling, bruising, and minimal loss of function.
Grade 2 Moderate
These tears are larger and have moderate swelling and bruising.
The fibers are partially torn and stretched.
Up to 50% loss of function.
Grade 3 Severe
This is the worst type of tear, where the muscle or tendon is completely torn.
These injuries cause severe pain and disability.
Symptoms
Triceps tears cause immediate pain in the back of the elbow and upper arm that worsens when trying to move the elbow. Individuals might also feel and/or hear a popping or tearing sensation. There will be swelling, and the skin will likely be red and/or bruised. With a partial tear, the arm will feel weak. If there is a complete tear, there will be significant weakness when straightening the elbow. Individuals may also notice a lump on the back of their arm where the muscles have contracted and knotted together.
Causes
Triceps tears usually occur during trauma, when the muscle is contracted and an external force pushes the elbow into a bent position. (Kyle Casadei et al., 2020) One of the most common causes is by falling on an outstretched arm. Triceps tears also occur during sports activities like:
Throwing a baseball
Blocking in a football game
Gymnastics
Boxing
When a player falls and lands on their arm.
Tears can also happen when using heavy weights during triceps-targeted exercises, such as the bench press.
Tears can also occur from direct trauma to the muscle, like a motor vehicle accident, but are less common.
Long-Term
Triceps tears can develop over time as a result of tendonitis. This condition usually occurs from repetitive use of the triceps muscle during activities like manual labor or exercise. Triceps tendonitis is sometimes referred to as weightlifter’s elbow. (Orthopedic & Spine Center. N.D.) The strain on tendons causes tiny tears that the body typically heals. However, if more strain is placed on the tendon than it can keep up with, the tiny tears can begin to grow.
Risk Factors
Risk factors can increase the risk of a triceps tear. Underlying medical conditions can weaken tendons, increasing the risk of injury, and can include: (Tony Mangano et al., 2015)
Diabetes
Rheumatoid arthritis
Hyperparathyroidism
Lupus
Xanthoma – fatty deposits of cholesterol under the skin.
Hemangioendothelioma – cancerous or noncancerous tumors caused by abnormal growth of blood vessel cells.
Chronic kidney failure
Chronic tendonitis or bursitis in the elbow.
Individuals who have had cortisone shots in the tendon.
Individuals using anabolic steroids.
Triceps tears tend to occur more commonly in males between 30 and 50. (Ortho Bullets. 2022) This comes from participating in activities like football, weightlifting, bodybuilding, and manual labor, which also increases the risk of injury.
Treatment
Treatment depends on which part of the triceps is affected and the extent of the damage. It may only need resting for a few weeks, physical therapy, or require surgery.
Nonsurgical
Partial tears in the triceps that involve less than 50% of the tendon can often be treated without surgery. (Mehmet Demirhan, Ali Ersen 2016) Initial treatment includes:
Splinting the elbow with a slight bend for four to six weeks allows the injured tissue to heal. (Ortho Bullets. 2022)
During this time, ice can be applied to the area for 15 to 20 minutes several times daily to help decrease pain and swelling.
Non-steroidal anti-inflammatory medications/NSAIDs – Aleve, Advil, and Bayer can help reduce inflammation.
Other over-the-counter medications like Tylenol can help decrease the pain.
Once the splint is removed, physical therapy will help restore movement and strength in the elbow.
Full movement is expected to return within 12 weeks, but full strength will not return until six to nine months after the injury. (Mehmet Demirhan, Ali Ersen 2016)
Surgery
Triceps tendon tears that involve more than 50% of the tendon require surgery. In some cases, however, surgery may still be recommended for tears smaller than 50% if the individual has a physically demanding job or plans to resume playing sports at a high level. Tears in the muscle belly or area where the muscle and tendon join are typically sewn back together. If the tendon is no longer attached to the bone, it is screwed back on. Recovery and physical therapy after surgery depend on the specific surgeon’s protocols. In general, individuals will spend a couple of weeks in a brace. Around four weeks after surgery, individuals will be able to start moving the elbow again. However, they won’t be able to start doing heavy lifting for four to six months. (Ortho Bullets. 2022) (Mehmet Demirhan, Ali Ersen 2016)
Complications
Complications can occur after triceps repair, whether there was surgery or not. For example, individuals may have problems regaining full elbow extension or straightening. They are also at a higher risk of re-rupture if they try to use the arm before it’s fully healed. (Mehmet Demirhan, Ali Ersen 2016)
Grassi, A., Quaglia, A., Canata, G. L., & Zaffagnini, S. (2016). An update on the grading of muscle injuries: a narrative review from clinical to comprehensive systems. Joints, 4(1), 39–46. doi.org/10.11138/jts/2016.4.1.039
Casadei, K., Kiel, J., & Freidl, M. (2020). Triceps Tendon Injuries. Current sports medicine reports, 19(9), 367–372. doi.org/10.1249/JSR.0000000000000749
Mangano, T., Cerruti, P., Repetto, I., Trentini, R., Giovale, M., & Franchin, F. (2015). Chronic Tendonopathy as a Unique Cause of Non Traumatic Triceps Tendon Rupture in a (Risk Factors Free) Bodybuilder: A Case Report. Journal of orthopaedic case reports, 5(1), 58–61. doi.org/10.13107/jocr.2250-0685.257
Individuals who participate in physical and sports activities could suffer an Achilles tendon tear. Can understanding the symptoms and risks help in treatment and return the individual back to their sports activity sooner?
Achilles Tendon
This is a common injury that occurs when the tendon attaching the calf muscle to the heel gets torn.
About the Tendon
The Achilles tendon is the largest tendon in the body.
In sports and physical activities, intense explosive movements like running, sprinting, quickly shifting positions, and jumping are exerted on the Achilles.
The injury often occurs without any contact or collision but rather the running, starting, stopping, and pulling actions placed on the feet.
Certain antibiotics and cortisone shots can increase the likelihood of Achilles tear injuries.
A specific antibiotic, fluoroquinolones, has been shown to increase the risk of Achilles tendon problems.
Cortisone shots are also associated with Achilles tears, which is why many healthcare providers don’t recommend cortisone for Achilles tendonitis. (Anne L. Stephenson et al., 2013)
Symptoms
A tendon tear or rupture causes sudden pain behind the ankle.
Individuals may hear a pop or a snap and often report the feeling as being kicked in the calf or heel.
Individuals have difficulty pointing their toes downward.
Individuals may have swelling and bruising around the tendon.
A healthcare provider will examine the ankle for continuity of the tendon.
Squeezing the calf muscle is supposed to cause the foot to point downwards, but in individuals with a tear, the foot will not move, resulting in positive results on the Thompson test.
A defect in the tendon can usually be felt after a tear.
X-rays may be used to rule out other conditions, including ankle fracture or ankle arthritis.
Fluoroquinolone antibiotics are commonly used for the treatment of respiratory infections, urinary tract infections, and bacterial infections. These antibiotics are associated with Achilles tendon rupture, but further research is needed to determine how they affect the Achilles tendon. Individuals taking these medications are advised to consider an alternative medication if Achilles tendon problems begin to develop. (Anne L. Stephenson et al., 2013)
Treatment
Depending on the severity of the injury, treatment can consist of non-surgical techniques or surgery.
The benefit of surgery is there is usually less immobilization.
Individuals can often return to sports activities sooner, and there is less chance of re-rupturing the tendon.
Thevendran, G., Sarraf, K. M., Patel, N. K., Sadri, A., & Rosenfeld, P. (2013). The ruptured Achilles tendon: a current overview from biology of rupture to treatment. Musculoskeletal surgery, 97(1), 9–20. doi.org/10.1007/s12306-013-0251-6
Stephenson, A. L., Wu, W., Cortes, D., & Rochon, P. A. (2013). Tendon Injury and Fluoroquinolone Use: A Systematic Review. Drug safety, 36(9), 709–721. doi.org/10.1007/s40264-013-0089-8
Pedowitz, D., & Kirwan, G. (2013). Achilles tendon ruptures. Current reviews in musculoskeletal medicine, 6(4), 285–293. doi.org/10.1007/s12178-013-9185-8
Yasui, Y., Tonogai, I., Rosenbaum, A. J., Shimozono, Y., Kawano, H., & Kennedy, J. G. (2017). The Risk of Achilles Tendon Rupture in the Patients with Achilles Tendinopathy: Healthcare Database Analysis in the United States. BioMed research international, 2017, 7021862. doi.org/10.1155/2017/7021862
When a groin strain injury happens, can knowing the symptoms help in the diagnosis, treatment, and recovery times?
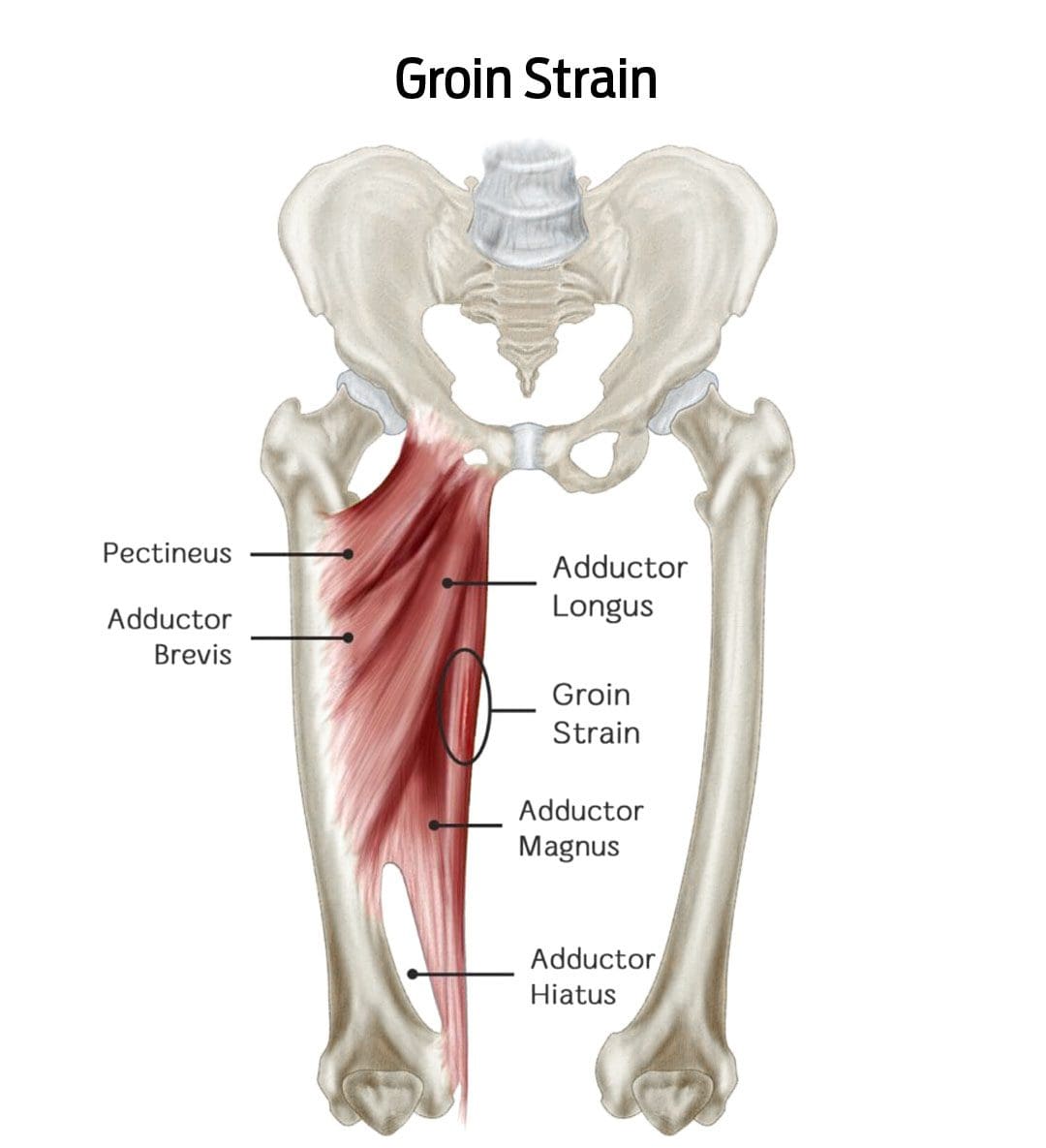
Groin Strain Injury
A groin strain is an injury to an inner thigh muscle. A groin pull is a type of muscle strain affecting the adductor muscle group (the muscles help pull the legs apart). (Parisa Sedaghati, et al., 2013) The injury is caused when the muscle is stretched beyond its normal range of motion, creating superficial tears. Severe strains can tear the muscle in two. (Parisa Sedaghati, et al., 2013)
A groin muscle pull causes pain and tenderness that worsens when squeezing the legs together.
There may also be swelling or bruising in the groin or inner thigh.
An uncomplicated groin pull takes four to six weeks to heal with proper treatment. (Andreas Serner, et al., 2020)
Symptoms
A groin pull can be painful, interfering with walking, navigating stairs, and/or driving a car. In addition to pain, other symptoms around the injured area include: (Parisa Sedaghati et al., 2013)
A popping sound or snapping sensation when the injury occurs.
Increased pain when pulling the legs together.
Redness
Swelling
Bruising of the groin or inner thigh.
Groin pulls are graded by severity and how much they impact mobility:
Grade 1
Mild discomfort but not enough to limit activities.
Grade 2
Moderate discomfort with swelling or bruising that limits running and/or jumping.
Grade 3
Severe injury with significant swelling and bruising can cause pain while walking and muscle spasms.
Signs of a severe groin strain
Difficulty walking
Groin pain while sitting or resting
Groin pain at night
A healthcare provider should see severe groin pulls because the muscle may have ruptured or be on the verge of rupturing.
In severe cases, surgery is necessary to reattach the torn ends.
Groin pulls are sometimes accompanied by a stress fracture of the pubis/forward-facing pelvic bones, which can significantly extend healing and recovery time. (Parisa Sedaghati et al., 2013)
Causes
Groin pulls are often experienced by athletes and individuals who play sports where they must stop and change directions quickly, placing excessive strain on the adductor muscles. (Parisa Sedaghati et al., 2013) The risk is increased in individuals who: (T. Sean Lynch et al., 2017)
Have weak hip abductor muscles.
Are not in adequate physical condition.
Have a previous groin or hip injury.
Pulls can also occur from falls or extreme activities without the proper conditioning.
Diagnosis
A healthcare provider will perform a thorough investigation to confirm the diagnosis and characterize the severity. This involves: (Juan C. Suarez et al., 2013)
Medical History Review
This includes any previous injuries and specifics about where and when the symptoms started.
Physical Examination
This involves palpating – lightly touching and pressing the groin region and manipulating the leg to understand better where and how extensive the injury is.
Imaging Studies
Ultrasound or X-rays.
If a muscle rupture or fracture is suspected, an MRI scan may be ordered to visualize soft tissue injuries and stress fractures better.
Differential Diagnosis
Certain conditions can mimic a groin pull and require different treatments. These include: (Juan C. Suarez, et al., 2013)
Sports Hernia
This type of inguinal hernia occurs with sports and work injuries.
It causes a portion of the intestine to pop through a weakened muscle in the groin.
Hip Labral Tear
This is a tear in the cartilage ring of the labrum outside the rim of the hip joint socket.
Hip Osteoarthritis
This is the wear-and-tear form of arthritis that can present with groin pain symptoms.
Osteitis Pubis
This is inflammation of the pubic joint and surrounding structures, usually caused by the overuse of the hip and leg muscles.
Referred Groin Pain
This nerve pain originates in the lower back, often due to a pinched nerve, but is felt in the groin.
Treatment
Beginning treatment is conservative and includes rest, ice application, physical therapy, and prescribed gentle stretching and exercises.
Individuals may need crutches or a walking device to reduce pain and prevent further injury if the pain is significant. (Andreas Serner, et al., 2020)
Physical therapy will be a part of the treatment plan.
Over-the-counter pain medications like Tylenol/acetaminophen or Advil/ibuprofen can help with pain relief short term.
If there is severe pain from a grade 3 injury, prescription medications may be used for a short period to help minimize pain. (Andreas Serner, et al., 2020)
Sedaghati, P., Alizadeh, M. H., Shirzad, E., & Ardjmand, A. (2013). Review of sport-induced groin injuries. Trauma monthly, 18(3), 107–112. doi.org/10.5812/traumamon.12666
Serner, A., Weir, A., Tol, J. L., Thorborg, K., Lanzinger, S., Otten, R., & Hölmich, P. (2020). Return to Sport After Criteria-Based Rehabilitation of Acute Adductor Injuries in Male Athletes: A Prospective Cohort Study. Orthopaedic journal of sports medicine, 8(1), 2325967119897247. doi.org/10.1177/2325967119897247
Lynch, T. S., Bedi, A., & Larson, C. M. (2017). Athletic Hip Injuries. The Journal of the American Academy of Orthopaedic Surgeons, 25(4), 269–279. doi.org/10.5435/JAAOS-D-16-00171
Suarez, J. C., Ely, E. E., Mutnal, A. B., Figueroa, N. M., Klika, A. K., Patel, P. D., & Barsoum, W. K. (2013). Comprehensive approach to the evaluation of groin pain. The Journal of the American Academy of Orthopaedic Surgeons, 21(9), 558–570. doi.org/10.5435/JAAOS-21-09-558
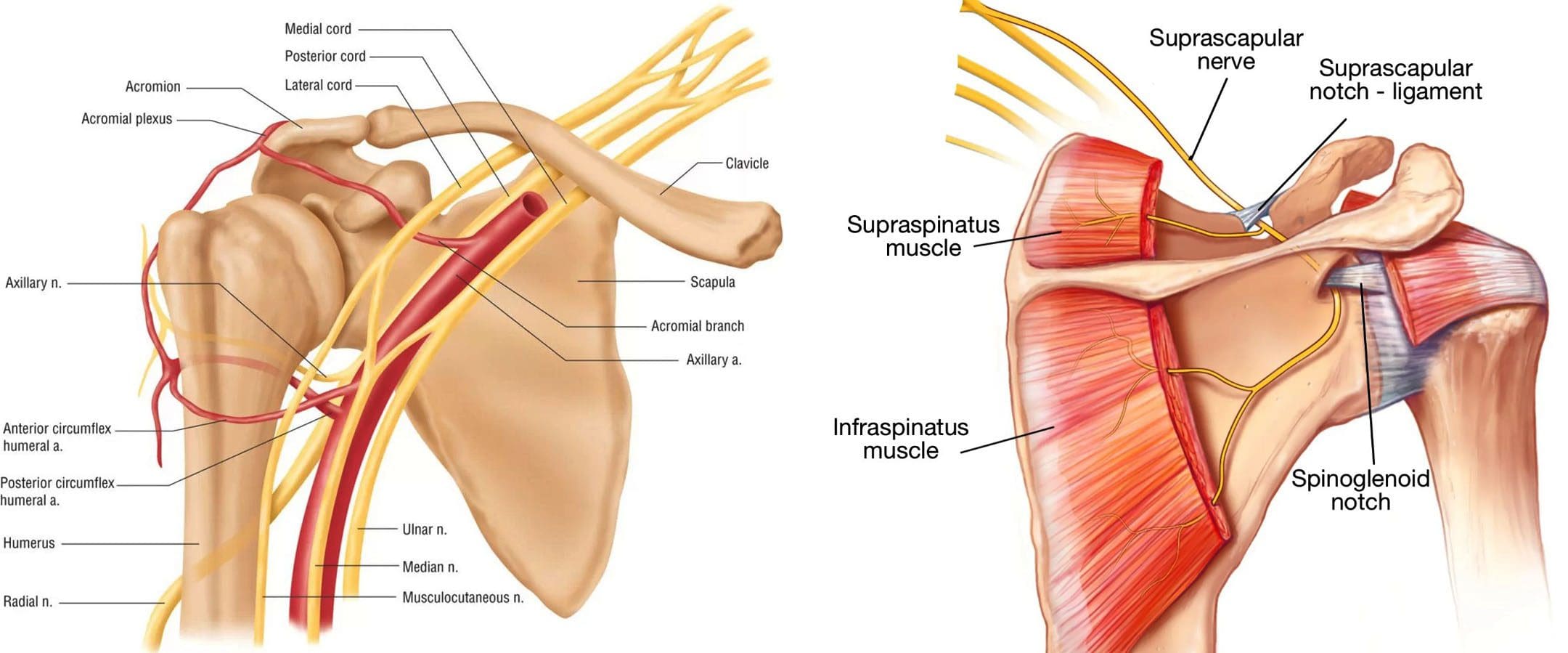
An acute injury or changes to the upper body over time can cause a compressed/pinched nerve in the shoulder. A pinched nerve in the shoulder happens when a muscle, ligament, tendon, or bone irritates or presses on a nerve exiting the neck. Shoulder nerve pain can develop from various sources, such as overuse work injuries, sports injuries, household chores, tendinitis, arthritis, torn cartilage, and other medical conditions, and injuries can contribute to symptoms. Chiropractors are highly qualified to treat pinched nerves. They are trained in whole-body realignment and rehabilitation techniques that find the root source and relieve pressure on compressed nerves.
Shoulder Nerve Pain
The shoulder joint is one of the most complex joints because of its wide range of motion. It is used so frequently that repetitive motion strain is common, often leading to injury. It is usually because of the continued use combined with an unhealed strain/injury that leads to shoulder nerve injury or when surrounding tissues like cartilage or tendons irritate or compress the nerves.
Pinched nerves also occur when a nerve root in the neck is damaged through wear and tear or an acute injury.
Individuals 50 years and older are likely to experience pinched nerves because of degeneration in the cervical spine and/or arthritis.
A nerve can become pinched when bone spurs form around the spinal discs.
Bone spurs are formations of bone that grow when discs weaken with age.
Bone spurs grow around the discs putting pressure on the nerve root.
Symptoms
Compressed Pinched Nerve/Cervical Radiculopathy
Pain sensations in the shoulder.
Tingling and/or pins and needles in fingers or hand.
Weakness in shoulder and arm muscles.
Symptoms have been known to overlap with shoulder arthritis, frozen shoulder, swimmer’s shoulder, or rotator cuff tears, so it’s always best to consult a chiropractor to understand possible causes. Other conditions with symptoms to compare:
Shoulder Arthritis
Stiffness in the joint.
Aching inside the shoulder.
Grinding when moving the joint.
Frozen Shoulder/Adhesive Capsulitis
Stiffness in the joint.
Pain in one shoulder.
Decreased range of motion and movement.
Swimmer’s Shoulder/Impingement
Pain and discomfort in the shoulder.
Weakness in the surrounding area.
Stiffness or tightness in the joint.
Impeded range of motion.
Rotator Cuff Tears
Pain and discomfort symptoms when moving the shoulder.
Weakness in the arm.
Deep aching sensations along the top and side of the joint.
Chiropractic Treatment
Chiropractors are experts on the neuromusculoskeletal system. First, a thorough medical examination will be conducted, including health history and regular activities, to understand the nature of the symptoms. Depending on the type of injury, tests, and exams may be needed to help diagnose and pinpoint the cause. Then the chiropractor will develop a personalized treatment plan. The objective is to relieve pressure and tension on the nerves and relax the muscles. In addition to adjusting the joint or other impacted areas, the therapy team will provide at-home exercises and stretches to maintain the adjustments and expedite healing.
Chiropractic Rehab
References
Kokkalis, Zinon T et al. “Nerve Injuries around the Shoulder.” Journal of long-term effects of medical implants vol. 27,1 (2017): 13-20. doi:10.1615/JLongTermEffMedImplants.2017019545
Leider, Joseph D et al. “Treatment of suprascapular nerve entrapment syndrome.” Orthopedic reviews vol. 13,2 25554. 11 Jul. 2021, doi:10.52965/001c.25554
Matzkin, Elizabeth, et al. “Swimmer’s Shoulder: Painful Shoulder in the Competitive Swimmer.” The Journal of the American Academy of Orthopaedic Surgeons vol. 24,8 (2016): 527-36. doi:10.5435/JAAOS-D-15-00313
Neviaser, Andrew S, and Jo A Hannafin. “Adhesive capsulitis: a review of current treatment.” The American Journal of sports medicine vol. 38,11 (2010): 2346-56. doi:10.1177/0363546509348048
Safran, Marc R. “Nerve injury about the shoulder in athletes, part 1: suprascapular nerve and axillary nerve.” The American Journal of sports medicine vol. 32,3 (2004): 803-19. doi:10.1177/0363546504264582
Strakowski, Jeffrey A, and Christopher J Visco. “Diagnostic and therapeutic musculoskeletal ultrasound applications of the shoulder.” Muscle & Nerve vol. 60,1 (2019): 1-6. doi:10.1002/mus.26505
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine