Painful symptoms may influence a person’s everyday physical actions. Patients with neck pain and spine pain caused by an assortment of health problems, including automobile accidents, have found tremendous relief from their symptoms with Dr. Alex Jimenez. Chiropractic care is a safe and effective, alternative treatment option which concentrates on the diagnosis, treatment, and prevention of injuries and/or conditions related to the musculoskeletal and nervous systems. Dr. Alex Jimenez has enhanced the quality of life of many patients by carefully restoring the integrity of their spine and improving debilitating symptoms. Patients highly recommend Dr. Alex Jimenez since the non-surgical selection for neck pain and spine pain, among other health problems, in El Paso, Tx.
Non-Surgical Care
�
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Many healthcare professionals highly recommend that patients with multiple sclerosis, or MS, avoid dairy. Several research studies have demonstrated a high correlation between MS and dairy, especially cow�s milk. By way of instance, some of the proteins in cow�s milk are targeted by the immune cells of patients with multiple sclerosis. These include butyrophilin and bovine serum albumin, or BSA. Moreover, injecting those same cow�s milk proteins into test animals caused lesions to appear in their central nervous systems.
Some proteins in cow�s milk imitate part of the myelin oligodendrocyte glycoprotein, or MOG, the section of myelin believed to initiate the autoimmune reaction associated with multiple sclerosis. Furthermore, this can trick the immune system into initiating an attack on the MOG, subsequently causing demyelination. Another research study involving more than 135,000 men and women in the United States determined a connection between cow�s milk and the degenerative neurological disorder, Parkinson�s Disease. Researchers have speculated that dairy products, especially cow’s milk, may have a generally toxic effect on nervous tissue.
Lactose intolerance is common throughout the general population, and it is most notably frequent in Mediterranean, Asian, and African populations. People with lactose intolerance experience a variety of symptoms, including bloating, cramps, diarrhea, and nausea. Given the high potential risks for people with MS consuming dairy products, despite a lack of conclusive evidence, healthcare professionals recommend avoiding the consumption of dairy products, among other types of foods. The purpose of the article below is to discuss the nutrition facts in multiple sclerosis, including which types of foods patients with MS should avoid, such as dairy.
Abstract
The question whether dietary habits and lifestyle have influence on the course of multiple sclerosis (MS) is still a matter of debate, and at present, MS therapy is not associated with any information on diet and lifestyle. Here we show that dietary factors and lifestyle may exacerbate or ameliorate MS symptoms by modulating the inflammatory status of the disease both in relapsing-remitting MS and in primary-progressive MS. This is achieved by controlling both the metabolic and inflammatory pathways in the human cell and the composition of commensal gut microbiota. What increases inflammation are hypercaloric Western-style diets, characterized by high salt, animal fat, red meat, sugar-sweetened drinks, fried food, low fiber, and lack of physical exercise. The persistence of this type of diet upregulates the metabolism of human cells toward biosynthetic pathways including those of proinflammatory molecules and also leads to a dysbiotic gut microbiota, alteration of intestinal immunity, and low-grade systemic inflammation. Conversely, exercise and low-calorie diets based on the assumption of vegetables, fruit, legumes, fish, prebiotics, and probiotics act on nuclear receptors and enzymes that upregulate oxidative metabolism, downregulate the synthesis of proinflammatory molecules, and restore or maintain a healthy symbiotic gut microbiota. Now that we know the molecular mechanisms by which dietary factors and exercise affect the inflammatory status in MS, we can expect that a nutritional intervention with anti-inflammatory food and dietary supplements can alleviate possible side effects of immune-modulatory drugs and the symptoms of chronic fatigue syndrome and thus favor patient wellness.
Keywords:complementary alternative medicine, gut microbiota, inflammation, lifestyle, multiple sclerosis, nutrition
Introduction
Multiple sclerosis (MS) is a chronic, inflammatory, and autoimmune disease of the central nervous system (CNS), leading to widespread focal degradation of the myelin sheath, variable axonal and neuronal injury, and disabilities in young adults, mostly women. The disease is characterized by disseminated and heterogeneous perivascular inflammatory processes at the blood�brain barrier (BBB), with involvement of autoreactive T cells, B lymphocytes, macrophages, and microglial cells against brain and spinal cord white matter (McFarland and Martin, 2007; Constantinescu and Gran, 2010; Kutzelnigg and Lassmann, 2014).
Antibodies (Krumbholz et al., 2012), activated complement (Ingram et al., 2014), cytokines, mitochondrial dysfunction (Su et al., 2009), reactive oxygen species (ROS; Gilgun-Sherki et al., 2004), and matrix metalloproteinases (MMPs; Liuzzi et al., 2002; Rossano et al., 2014) may cooperate to yield the pathology.
From the clinical point of view, there are at least two main forms of the disease: the relapsing-remitting MS (RRMS; about 85% of clinical cases) and the primary-progressive MS (PPMS; about 15% of the clinical cases) (Dutta and Trapp, 2014; Lublin et al., 2014). In RRMS, which usually evolves in secondary-progressive MS (SPMS), relapses are associated with increased systemic inflammation and formation of lesions in the brain, followed by more or less complete remissions, whereas the pathogenesis of PPMS is characterized by progressive neurological damages rather than relapses and remissions.
At present, there are at least 10 disease-modifying therapies that have been found to slow disease progression and prevent some disability symptoms, but only in the case of RRMS. However, as the disease is complex in nature and unique in the individual course, no patient responds to therapy in the same way (Loleit et al., 2014). Similarly, there are no truly reliable biomarkers that allow for everyone to evaluate the effectiveness of treatment and it is therefore important to discover novel markers of the disease (Fernandez et al., 2014).
The lack of response to immune-modulatory therapies in the case of PPMS, otherwise effective in the treatment of RRMS, may be due to different pathogenic mechanisms acting in RRMS and PPMS. However, this is not true with regard to inflammation: A significant association between inflammation and neurodegeneration has been observed in the brain not only in acute and relapsing MS but also in the secondary and primary progressive MS (Frischer et al., 2009; Lassmann, 2013), and active MS lesions are always associated with inflammation (Kutzelnigg and Lassmann, 2014). Thus, inflammation must be the target for the treatment of both forms of the disease.
Linking Inflammation with Dietary Habits and Lifestyle
What causes the inflammatory processes in MS? MS is a complex disease, and the genetic and the immunological components are not sufficient to explain its origin. Actually, MS has a multifactorial nature and various environmental factors or metabolic conditions may have a role in its development (Ascherio, 2013): viral infections (Ascherio et al., 2012; Venkatesan and Johnson, 2014), heavy metal poisoning (Latronico et al., 2013; Zanella and Roberti di Sarsina, 2013), smoking (Jafari and Hintzen, 2011), childhood obesity (Munger, 2013), low vitamin D status (Ascherio et al., 2014), or incorrect lifestyle, including wrong dietary habits (Riccio, 2011; Riccio et al., 2011; Riccio and Rossano, 2013).
None of the above-mentioned environmental factors alone can explain the disease; however, the following considerations make more attractive the involvement in MS of dietary habits and lifestyle, rather than infections or smoking, as factors that may influence the course of the disease:
Geographical distribution: MS is more prevalent in Western countries with the highest income and most distant of the equator. Features of these countries are a sedentary lifestyle, a high-calorie diet rich in saturated fats of animal origin (Western diet), and low sunshine exposure (WHO and MSIF, 2008).
Effect of migration: With the migration from an area of high incidence of MS to another place with low incidence before age of 15 years, the low risk is acquired, while the migration after this age does not change the level of risk. This aspect may be linked with nutritional, rather than with infectious or toxicological environmental factors (McLeod et al., 2011).
Low availability of vitamin D: Another environmental factor related to diet and geographical distribution is the availability of vitamin D, which is lower at latitudes with lower exposure to sunlight. Patients with MS have a low content of vitamin D (Ascherio et al., 2014), but this is true also for other chronic inflammatory diseases (Yin and Agrawal, 2014).
Postprandial inflammation: High animal fat/high sugar and refined carbohydrate diet is associated with postprandial inflammation (Erridge et al., 2007; Ghanim et al., 2009; Margioris, 2009).
High body mass index: High body mass index (BMI) before age 20 is associated with 2� increased risk (Hedstr�m et al., 2012). Note that BMI is correlated with gut microbiota status.
Similarity with other inflammatory diseases related to wrong dietary habits: MS has some similarities with inflammatory bowel disease (IBD; Cantorna, 2012): both have low vitamin D and are influenced from environmental factors (Dam et al., 2013). Furthermore, glatiramer acetate (GA, or Copolymer 1/Copaxone) is beneficial in both diseases (Aharoni, 2013) and there is an increased incidence of IBD among MS patients.
How Food Affects the Course of Inflammatory Diseases: A Basic Approach
The observations reported above suggest that the nutritional status may influence the course of MS. However, the question arises of how dietary molecules could exacerbate or ameliorate MS symptoms, and in general how they could favor or downregulate inflammation at molecular level. In particular, it is important to clarify what are the targets of dietary molecules and the molecular mechanisms involved, if any.
Fundamentally, we can say that the food we consume has a broad impact on our development, behavior, health condition, and lifespan by acting on two main targets: (A) the cells of our body and (B) the commensal gut microbiota (Figure 1).
On one hand, different kind and amount of dietary factors can interact with enzymes, transcription factors, and nuclear receptors of human cells. This may induce specific modifications of cellular metabolism toward either catabolism or anabolism and modulate the inflammatory and autoimmune responses in our body (Desvergne et al., 2006).
On the other hand, we have to consider the impact of diet and lifestyle on our intestinal microflora. We are indeed metaorganisms living with trillions (1014) of microbial cells (roughly 10 times the cells of our body) and thousands of different microorganisms known as the gut microbiota. This complex ecosystem is an essential part of our organism and influences both our immune system and our metabolism. Therefore, it has a strong impact on our health.
In health, there is a close mutualistic and symbiotic relationship between gut microbiota and humans, and gut microbiota provides a number of useful metabolic functions, protects against enteropathogens, and contributes to normal immune functions. This is the normal state of the human intestinal microbiota, called eubiosis. Distortion from eubiosis, linked with a decrease of intestinal biodiversity and increase of pathogenic bacteria, is called dysbiosis. The most common consequence of a dysbiotic gut microbiota is the alteration of the mucosal immune system and the rise of inflammatory, immune, metabolic, or degenerative diseases (Chassaing and Gewirtz, 2014).
Different kinds and amounts of dietary factors elicit the selection of specific gut microbial populations changing type and number of microbial species toward eubiosis or dysbiosis, simply acting through the preferential feeding of one or the other microbial population. If our diet favors the change to a dysbiotic gut microbiota, this may lead to gut inflammation, alteration of intestinal immunity, and then to systemic inflammation and chronic inflammatory diseases.
How Dietary Factors Influence the Metabolism of Human Cells and Modulate Inflammation
To understand how dietary molecules can directly influence the metabolism of human cells, it is necessary to describe first what are the enzymes and transcription factors involved in catabolism or anabolism in the cell.
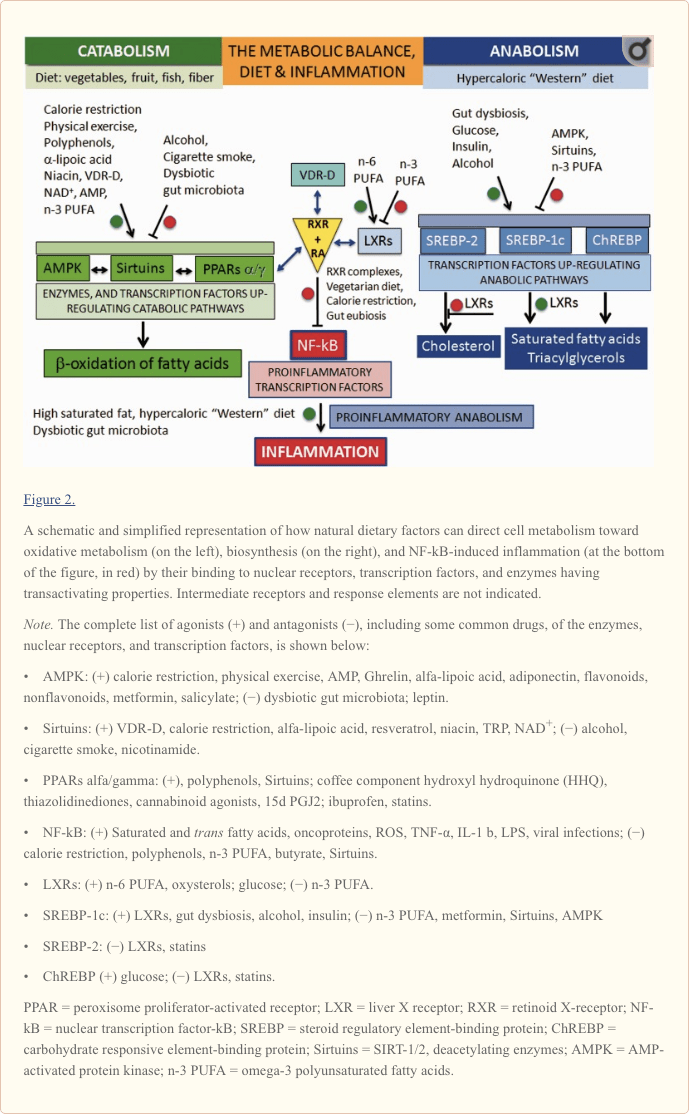
As shown on the left in Figure 2, oxidative metabolism is upregulated by two enzymes and a nuclear receptor. The enzymes are the AMP-activated protein kinase (AMPK; Steinberg and Kemp, 2009) and the Sirtuins (SIRT), a group of histone deacylating enzymes, which are activated by NAD+ (Zhang et al., 2011; Rice et al., 2012). The nuclear receptor is represented by the isotypes of the peroxisome proliferator-activated receptors (PPARs; Desvergne and Wahli, 1999; Burns and VandenHeuvel, 2007).
�
PPAR isotypes upregulate the transcription of genes involved in the beta-oxidation of fatty acids in mitochondria and peroxisomes and form a network with AMPK and Sirtuins pathways. The AMPK-Sirtuins-PPAR pathway is activated by a lifestyle based on calorie restriction and physical exercise, as well as by some bioactive molecules (polyphenols, found in vegetables and fruits, and omega-3 (n-3) long-chain polyunsaturated fatty acids [PUFA], found in fish). Ligand-activated PPAR isotypes form heterodimeric complexes with the retinoid X-receptor (RXR), which, in turn, is activated by 9-cis-retinoic acid (RA).
Conversely, as shown on the right in Figure 2�like on the other dish of an imaginary balance�high intake of energy-dense nutrients leads to the upregulation of anabolism, including lipogenesis and cell growth, through the activation of the sterol regulatory element-binding proteins, SREBP-1c and SREBP-2 (Xu et al., 2013), and the carbohydrate responsive element-binding protein, ChREBP (Xu et al., 2013). SREBP-1c and SREBP-2 are under the control of the nuclear receptors called the liver X receptors (LXR; Mitro et al., 2007; Nelissen et al., 2012). LXR isotypes, which are activated by the cholesterol derivatives oxysterols and glucose, have a relevant role in the synthesis of lipids by activating SREBP-1c and the synthesis of triacylglycerols, while inhibiting SREBP-2 and the synthesis of cholesterol.
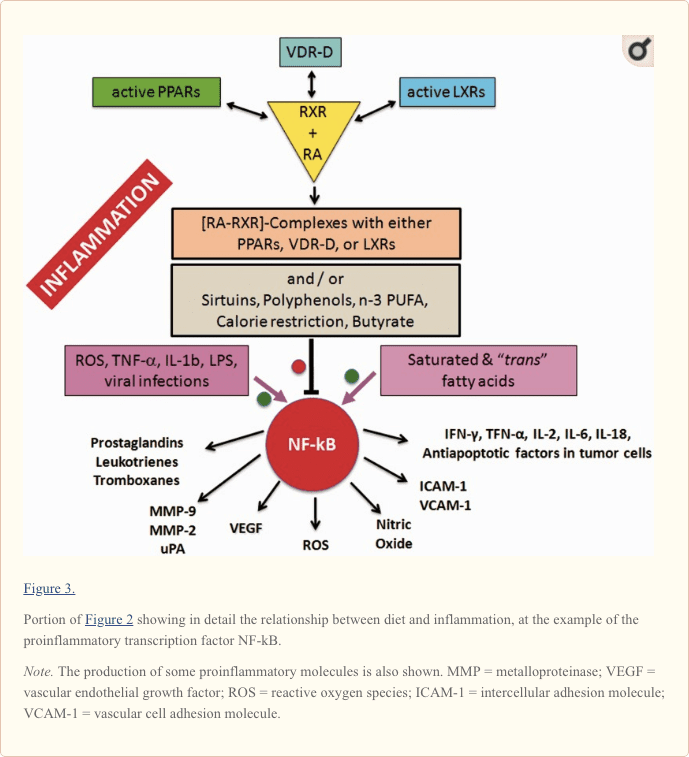
Central to the understanding of the link between diet and inflammation are two transcription factors involved in inflammation and autoimmunity: the nuclear transcription factor-kB (NF-kB) and the activator protein (AP-1; Yan and Greer, 2008). In MS, both NF-kB and AP-1 are activated and induce the expression of several proinflammatory genes and the production of proinflammatory molecules. The cause of their activation in MS is not known but, as shown in Figure 2 for NF-kB, this can be activated not only by viruses, cytokines, and oxidative stress but also by some dietary components such as saturated fatty acids or trans unsaturated fatty acids, which therefore can be considered proinflammatory.
Downregulation of the proinflammatory NF-kB can be achieved by the inhibitory binding of the RA-activated forms of the retinoid X-receptor isotypes (RXRs; P�rez et al., 2012; Zhao et al., 2012; Fragoso et al., 2014).
As shown in the center of Figure 2 and more in detail in Figure 3, the active forms of RA-RXRs are heterodimers resulting from their association with specific ligand-activated nuclear receptors, namely PPARs, LXRs, and vitamin D receptor (VDR).
All three nuclear receptors�PPAR, LXR, and VDR�must be activated by specific ligands. As indicated in Figure 2, the ligands can be specific dietary factors and this clarify how cells respond to changes in nutritional status and regulate energy homeostasis but represents also the molecular key to understanding how nutrients can influence the course of chronic inflammatory diseases (Heneka et al., 2007; Zhang-Gandhi and Drew, 2007; Krishnan and Feldman, 2010; Cui et al., 2011; Schnegg and Robbins, 2011; Gray et al., 2012).
Therefore, each of the three nuclear receptors�PPAR, LXR, and VDR�competes for the binding to RA-RXR and forms hetero-complexes that can inhibit NF-kB and exert a tight control over the expression of inflammatory genes, thus integrating metabolic and inflammatory signaling. It is clear that there is competition between the three receptors PPAR, LXR, and VDR-D, for the binding with RA-RXR, but this competition should have an influence only on metabolism and not on inflammation, because it is not yet known which of the three heterodimers is more effective in inhibiting NF-kB.
Obviously, the production of proinflammatory molecules in the course of relapses is a biosynthetic process: It is sustained by hypercaloric diets and counteracted by low-calorie diets. In principle, what favors anabolism will promote the inflammatory processes, while what favors catabolism will contrast them (Figure 4).
How Dietary Factors Influence Composition and Biodiversity of Gut Microbiota and Alter Host�Microbiota Relationship
The Link Between Lifestyle, Dietary Habits, and Gut Microbiota Composition
The composition of the intestinal microflora is highly individual and is influenced by many factors such as diet, physical activity, stress, medications, age, and so forth. Each of us has a unique set of at least 100 to 150 species of bacteria.
An easy way to discuss about the effect of food and lifestyle on gut microflora is to restrict the overview to only two dominant bacterial divisions�the Bacteroidetes and the Firmicutes�accounting for about 90% of the total, as it has been shown that the ratio Bacteroidetes/Firmicutes (B/F) is influenced by long-term dietary habits (Cani and Delzenne, 2009; Wu et al., 2011; Lozupone et al., 2012; Tremaroli and B�ckhed, 2012; Panda et al., 2014).
A comparative study of De Filippo et al. (2010) in children from Florence and from Burkina Faso in Africa showed that long-term dietary habits have significant effects on human gut microbiota.
In this study, the Burkina Faso diet was based on the consumption of plant polysaccharides such as millet and sorghum (10 g fibers/day and 662�992 kcal/day), whereas the diet of Italian children was Western style, based on proteins, animal fat, sugar-sweetened drinks, and refined carbohydrates (5.6 g fibers/day and 1,068�1,512 kcal/day). Analysis of fecal samples in the children from Africa showed the prevalence of the Bacteroidetes (73%)�mainly Prevotella and Xylanibacter�and low levels of Firmicutes (12%). On the contrary, a prevalence of Firmicutes (51%) over the Bacteroidetes (27%) was observed in Italian children, but the Bacteroidetes shifted from Prevotella and Xylanibacter to Bacteroides. These latter are usually selected among the Bacteroidetes because they can use also simple sugars in addition to complex glycans, and simple sugars are normal components of Western diets.
In conclusion, the B/F ratio increases in association with a diet rich in complex carbohydrates (nondigestible by our enzymes) because the symbiotic and usually nonharmful Bacteroidetes, such as Prevotella and Xylani bacter, love to have complex glycans to eat. Bacteria consuming complex glycans produce butyrate, which down regulate the activation of proinflammatory NF-kB (Figure 3).
Conversely, Western, energy-dense diets change the gut microbiota profile and increase the population of Firmicutes (including the Mollicutes), more suited to extract and harvest energy, but often pathogenic (Moschen et al., 2012).
The Link Between Dysbiotic Gut Microbiota and Chronic Inflammation
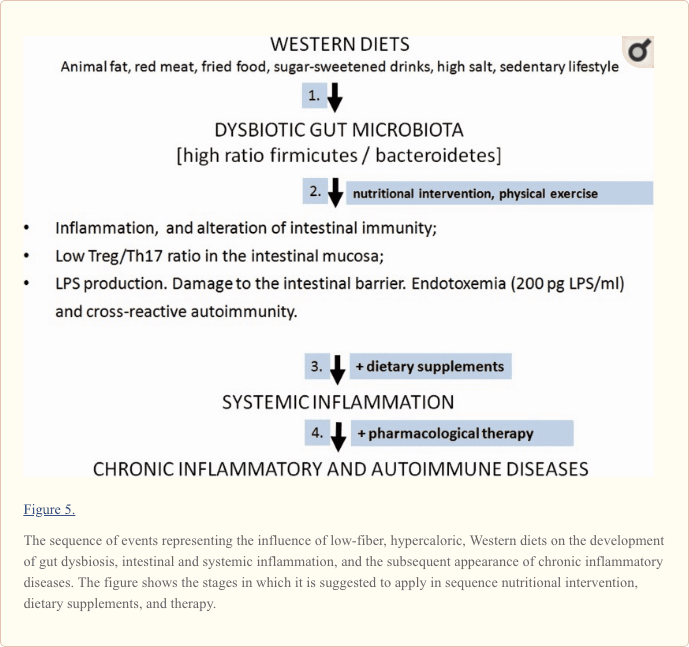
In a dysbiotic gut microbiota, the B/F ratio is low and the possibly pathogenic Firmicutes prevail over Bacteroidetes (Figure 5). The failure of microbial balance and the decrease of biodiversity occurring in dysbiosis lead to the disruption of the complex interplay between the microbiota and its host and contribute to low-grade endotossemia, and chronic intestinal and systemic inflammation. With the onset of systemic inflammation, the risk of chronic inflammatory and immune-mediated diseases increases (Tilg et al., 2009; Brown et al., 2012; Maynard et al., 2012).
Actually, in the presence of a dysbiotic microbiota, gut endotoxin/lipopolysaccharide (LPS) is increased, regulatory T cells (Treg) are defective, and the aryl hydrocarbon receptors and proinflammatory Th17 cells are activated (Cani et al., 2008; Veldhoen et al., 2008).
LPS leads to the dysfunction of the mucosal barrier and affects other tissues when its plasma level increases above 200 pg/ml serum. The increased gut permeability due to the dysbiotic gut microbiota may be exemplified by the passage of IgA and IgG antibodies against gluten and gliadin, also observed in MS patients (Reichelt and Jensen, 2004).
The Link Between Dysbiotic Gut Microbiota and MS
In our previous work, we have proposed that the model linking microbiota alteration�due to Western diet and lifestyle�and the failure of the correct communication between the microbiota and the intestine, leading to low-grade endotoxemia and systemic autoimmune inflammation, might be valid also for the pathogenesis of MS (Fern�ndez et al., 2012; Riccio, 2011). In fact, MS shares with other chronic inflammatory diseases common mechanisms, all probably based on the persistence of low-grade endotoxemia related to wrong lifestyle and dietary habits together with a latent dysbiosis. Moreover, the existence of a gut microbiota-brain axis, which is now more than an emerging concept, suggests that intervention on gut microbiota may be a fruitful strategy for future treatment of complex CNS disorders (Cryan and Dinan, 2012).
The possible direct link between gut microbiota and MS has been shown experimentally by Berer et al. (2011). Using transgenic mice, Berer et al. have shown that gut commensal bacteria can trigger a relapsing-remitting autoimmune disease driven by myelin-specific CD4+ T cells and demyelination, given the availability of MOG�the autoantigen myelin oligodendrocyte glycoprotein. In another study, it was shown that antibiotic treatment directed to alter gut microflora suppresses experimental allergic encephalomyelitis (EAE; Yokote et al., 2008).
These findings suggest that gut microbiota may play a crucial role in the starting phase of MS and may also predispose host susceptibility to other CNS autoimmune diseases as well as to neuropsychiatric disorders such as autism, depression, anxiety, and stress. A new concept of gut microbiota-brain axis is emerging (Wang and Kasper, 2014).
On these grounds, understanding the role of gut microbiota in health and disease can lay the foundation to treat chronic diseases by modifying the composition of gut microbiota through the choice of a correct lifestyle, including dietary habits. Moreover, direct manipulation of the gut microbiota may improve adaptive immune response and reduce inflammatory secretions. For example, because a specific role of intestinal Th17 cells has been suggested in MS immunopathology (Sie et al., 2014), promoting Treg cell differentiation and reducing pathogenic Th17 cells might prevent recurrence of autoimmunity in MS patients (Issazadeh-Navikas et al., 2012).
On these grounds, the discovery that the defect of the Treg/Th17 balance observed in MS models is also present in MS patients, could have important clinical implications, as this defect can be modulated by changes in the microbiota composition, which in turn is modulated by dietary changes (David et al., 2014).
Proinflammatory Dietary Factors
The components of the diet whose intake must be controlled to avoid the rise of inflammatory processes in MS, as well as in other chronic inflammatory diseases, are as follows:
Saturated fatty acids of animal origin;
Unsaturated fatty acids in the trans configuration (hydrogenated fatty acids);
Red meat;
Sweetened drinks, and in general hypercaloric diets rich in refined (low-fiber) carbohydrates, in addition to animal fat;
Increased dietary salt intake;
Cow�s milk proteins of the milk fat globule membrane (MFGM proteins).
Fat of Animal Origin
Saturated fatty acids of animal origin, which are found in foods such as whole milk, butter, cheese, meat, and sausages, are the components of the diet taken into account more frequently for their deleterious influence on the course of MS.
In 1950, Swank suggested that the consumption of saturated animal fat is directly correlated with frequency of MS, but a link between restricted intake of animal fat and remission of MS was reported only in 2003 (Swank and Goodwin, 2003). According to Swank and Goodwin, high-fat diets lead to the synthesis of storage lipids and cholesterol and cause a decrease of membrane fluidity and possible obstruction of capillaries, and the onset or increase of inflammation.
Other more recent studies indicate that the action of saturated fat is controlled at the transcriptional level and influence both gene expression, cell metabolism, development, and differentiation of cells. More in general, the assumption of animal fat is often linked to a high-calorie intake, which is on its own a detrimental factor for many chronic inflammatory diseases. Finally, as described later in this article, an excess of saturated animal fat leads to a dysbiotic intestinal microbiota, dysfunction of intestinal immunity, and low-grade systemic inflammation and represents a possible cause of some human chronic disorders.
Trans Fatty Acids
Trans fatty acids (TFAs) are unsaturated fatty acids that contain at least one nonconjugated double bond in the trans configuration (Bhardwaj et al., 2011).
As products of partial hydrogenation of vegetable oils, they were introduced in the 1960s to replace animal fat, but only much later it was found that they have the same deleterious effect on the metabolism and, as the saturated fatty acids, increase the levels of cholesterol and promote the formation of abdominal fat and weight gain. TFAs intake was found to be positively associated with gut inflammation and the upregulation of proinflammatory citokines in Th17 cell polarization (Okada et al., 2013). Moreover, TFAs interfere with the metabolism of natural unsaturated fatty acids, which have the cis configuration.
TFAs are found in margarine and other treated (hydrogenated) vegetal fat, in meat and dietary products from ruminants and in snacks. They may be present also in French fries and other fried food, as they are also formed in the frying.
Red Meat
Red meat contains more iron heme than white meat. The iron is easily nitrosylated and this facilitates the formation of endogenous nitroso-compounds (NOCs; Joosen et al., 2010). Red meat intake shows indeed a dose�response relation with NOCs formation, whereas there is no such relation for white meat. NOCs are mutagenic: induce nitrosylation and DNA damage. Processed (nitrite-preserved) red meat increases the risk. Heterocyclic amines are formed during cooking of meat at high temperatures, but this is not specific for red meat (Joosen et al., 2010).
Abnormal iron deposits have been found at the sites of inflammation in MS (Williams et al., 2012) and consumption of red meat is associated with higher levels of ?-GT and hs-CRP (Montonen et al., 2013).
Noteworthy, we do not have N-glycolylneuraminic acid (Neu5Gc), a major sialic acid, because an inactivating mutation in the CMAH gene eliminated its expression in humans. Metabolic incorporation of Neu5Gc from dietary sources�particularly red meat and milk products�can create problems, as humans have circulating anti-Neu5Gc antibodies and this implies the possible association with chronic inflammation (Padler-Karavani et al., 2008).
Finally, meat contains arachidonic acid (the omega-6 (n-6) PUFA, which is the precursor of proinflammatory eicosanoids [prostaglandins, thromboxanes, and leukotrienes]) and activates the Th17 pathway (Stenson, 2014).
High Intake of Sugar and Low Intake of Fiber
The high intake of sugar-sweetened beverages and refined cereals, with low fiber content, increases rapidly the number of calories and glucose level. The subsequent increase of insulin production upregulates the biosynthetic pathways and inter alia the production of arachidonic acid and its proinflammatory derivatives.
Increased Dietary Salt Intake
Increased dietary salt intake might be an environmental risk factor for the development of autoimmune diseases, as it has been found that it can induce pathogenic Th17 cells and related proinflammatory cytokines in EAE (Kleinewietfeld et al., 2013; Wu et al., 2013). Th17 cells have been involved in the development of MS.
Cow�s Milk Fat and the Proteins of the Milk Fat Globule Membrane
Milk fat is dispersed in a homogeneous way and protected from oxidation, thanks to a membrane made of lipids and particular proteins called proteins of the milk fat globule membrane (MFGM; Riccio, 2004). These proteins, which account for only 1% of milk proteins, have an informational rather than a nutritional value. In human lactation, they are needed for the correct formation of the digestive, nervous, and immune systems in infants. This flow of information is obviously not relevant, or not required at all, in adulthood and, as well, in the case of cow�s milk taken for human nutrition. In adult age, MFGM proteins of cow�s milk no longer have an informational role and may be eliminated from the diet together with milk fat.
The removal of MFGM proteins from whole cow�s milk is particularly relevant in the case of MS. The most representative MFGM protein (40% of total MFGM proteins), butyrophilin (BTN), is indeed suspected to have a role in MS, as it is very similar to MOG, one of the candidate autoantigen in MS. BTN and MOG share the same behavior in MS experimental models, and MOG/BTN cross-reactive antibodies have been found in MS, in autism and in coronary heart disease (CHD; Riccio, 2004). On these grounds, the patient with MS should avoid the intake of whole cow�s milk and prefer skimmed milk, which, in addition, has no animal fat.
Another point of view is that of Swanson et al. (2013). They have found that BTN or BTN-like molecules might have a regulatory role in immunity and therefore they suggest that BTN or BTN-like molecules could be useful to induce Treg development.
Hypercaloric Diets and Postprandial Inflammation
After each meal, we may experience a transient and moderate oxidative stress and a moderate inflammatory response depending on type and quantity of food. Dietary habits based on a frequent and persistent exposure to meals with high intake of salt/animal fat and trans fat/sugar-sweetened drinks stresses our immune/metabolic system and the subsequent possible failure of homeostasis may lead to immune and metabolic disorders of diverse nature.
Taken together, the diet-dependent stress might be due to following reasons: (a) calorie intake: the higher the calories, the more the oxidative stress induced; (b) glycemic load of a meal: acute postprandial glycemic peaks may induce a release of insulin much higher than necessary; (c) lipid pattern: saturated animal fat, trans fatty acids, and omega-6 (n-6) long-chain PUFA promote postprandial inflammation. As reported in the following sections, postprandial inflammation is attenuated or suppressed by n-3 PUFA and polyphenols, calorie restriction, and physical exercise.
Anti-Inflammatory Natural Bioactive Compounds: Useful to Tackle MS and Prevent Relapses?
Specific bioactive dietary molecules are able to counteract the effects of pathogenic microbial agents and downregulate the expression of inflammatory molecules. Among them, the most important compounds are the polyphenols and carotenoids from vegetables, n-3 PUFA from fish, vitamins D and A, thiol compounds such as lipoic acid, and oligoelements such as selenium and magnesium.
Most of the above-mentioned compounds, with exception of PUFA, which are not antioxidant, are known for their antioxidant properties. The rationale for the use of antioxidants in MS is based on the observation that oxidative stress is one of the most important components of the inflammatory process leading to degradation of myelin and axonal damage. However, it is now known that dietary antioxidants have additional biological properties going far beyond the simple antioxidant activity. Indeed, they are able to counteract the negative effects of microbial agents and saturated or trans fatty acids, downregulating the expression of proinflammatory molecules, oxidative stress, and angiogenesis.
Polyphenols
All polyphenols�which are present in vegetables, cereals, legumes, spices, herbs, fruits, wine, fruit juices, tea, and coffee�have anti-inflammatory, immune-modulatory, anti-angiogenic, and antiviral properties and stimulate the catabolic pathways (Gupta et al., 2014; Wang et al., 2014). They are found in plants in the form of glycosides, esters, or polymers, too large to enter the intestinal membrane. Aglycons released from gut microbiota are conjugated to glucuronides and sulfates in intestine and liver. Their solubility and bioavailability are very poor (�M; Visioli et al., 2011).
From a structural point of view, polyphenols include flavonoids and nonflavonoids molecules (Bravo, 1998). The most important flavonoids are quercetin (onions, apples, citrus fruit, and wine; Min et al., 2007; Sternberg et al., 2008), catechins (green tea; Friedman, 2007), and daidzein and genistein (soy; Castro et al., 2013; Zhou et al., 2014). The most important nonflavonoids are resveratrol (chocolate, peanuts, berries, black grapes, and red wine; Das and Das, 2007; Cheng et al., 2009; Shakibaei et al., 2009), curcumin (spice turmeric of ginger family, curry; Prasad et al., 2014), and hydroxytyrosol (olive oil; Hu et al., 2014).
It has been found that the anti-inflammatory effect of polyphenols in vitro may depend on their chemical structure (Liuzzi et al., 2011). Thus, a mixture of flavonoids and nonflavonoids may be more effective than supplementation with only one polyphenol.
Two examples of the most studied polyphenols are quercetin and resveratrol. Quercetin is present mainly as a glucoside. Most of its effects are additive to those of interferon-?. Quercetin is not toxic, but its oxidation product, quercetin quinone, is very reactive toward the SH groups of proteins and glutathione and may be toxic (Boots et al., 2008). Addition of lipoic acid or N-acetylcysteine can limit the toxic effects.
Resveratrol is glucuronated in the liver and absorbed in this form mainly in the duodenum but only in very limited amount. Depending on its concentration, resveratrol can induce the death of a wide variety of cells by necrosis or apoptosis. In this regard, it is commonly accepted that resveratrol has neuroprotective effects; however, it has been also reported that it can exacerbate experimental MS-like diseases (Sato et al., 2013). These discrepancies can be attributed to the different concentrations used in vitro or bioavailable in vivo, as resveratrol has opposite effects at concentrations of 10?5 M (proliferation of human mesenchimal cells) and 10?4 M (inhibition of proliferation). In our experience, resveratrol has a neurotrophic effect on cortical neurons in culture only at very low concentration, whereas at higher concentration, it may have toxic effect. But in the case of oxidative stress, resveratrol has neuroprotective properties also at the higher concentrations.
Vitamin D, Vitamin A, Carotenoids, Other Vitamins, and Oligoelements
Other compounds and elements that may be useful as supplements in MS are the vitamins D, A, E, C, B12 (Mastronardi et al., 2004), and niacin (Penberthy and Tsunoda, 2009), and oligoelements such as selenium (Boosalis, 2008) and magnesium (Galland, 2010).
Vitamin D has immune-modulatory roles and represents the most promising dietary molecule for the treatment of chronic inflammatory diseases such as MS (Smolders et al., 2008; Pierrot-Deseilligny, 2009; Cantorna, 2012; Ascherio et al., 2014). As already mentioned, it is generally believed that the special geographical distribution of MS in the world can also be attributed to the reduced availability of vitamin D3, due to insufficient exposure to sunlight in some countries, and the lack of active vitamin D may be another possible cause of environmental origin of MS. However, low levels of active vitamin D may be due also to its altered metabolism or function not only to the exposure to sunlight. In fact, the failure of vitamin D3 (cholecalciferol) supplementation to show beneficial effects on body weight or on the course of inflammatory diseases may be due to the persistence of its deficiency despite its administration.
Vitamin D3 (cholecalciferol), formed after exposure to sunshine, is hydroxylated in the liver to 25-(OH) D3 (calcidiol) by the P450 enzymes CYP27A1 or CYP2R1, and subsequently activated in the kidney by CYP27B1 to 1?, 25-(OH)2 D3 (calcitriol). This latter, the active form of vitamin D, is inactivated by CYP24A1 to 1?, 24,25-(OH)3 D3 (calcitroic acid). This means that the levels of active vitamin D depend on the relative rates of its synthesis via CYP27B1 and its modifications via CYP24A1 (Schuster, 2011). High CYP24A1 expression, induced by endogenous compounds and xenobiotics, might lead to low levels of vitamin D and cause or enhance chronic inflammatory diseases and cancer. On these grounds, it is important to follow up the level of vitamin D in the course of vitamin D administration. If vitamin D levels remain low, the expression of CYP24A1 mRNA should be examined, and determination of CYP27B1 and CYP24A1 activities and their inhibition should be tested (Chiellini et al., 2012, K�sa et al., 2013).
Another important aspect regards the VDR. The active metabolite of vitamin D�1?, 25-dihydroxyvitamin D�binds to VDR, and the complex VDR-D controls the expression of several genes involved in processes of potential relevance to chronic diseases. As represented in Figures 2 and and3,3, the VDR-D complex competes with ligand-activated PPARs or LXRs for the binding to RA-RXR. The heterodimeric complexes bind to the proinflammatory transcription factor NFkB and downregulate the synthesis of proinflammatory molecules. In this context, when evaluating the effectiveness of vitamin D supplementation in the course of MS, one should consider the eventual polymorphisms affecting the VDR, which has been recently associated with obesity, inflammation, and alterations of gut permeability (Al-Daghri et al., 2014).
Moreover, the finding that that VDR-D activate the Sirtuin SIRT-1 (An et al., 2010; Polidoro et al., 2013) suggests that vitamin D has an influence also on cell metabolism and therefore may have properties similar to those of many other natural dietary supplements: upregulate oxidative metabolism and downregulate inflammation.
Finally, it should be considered that there are differences between data in humans and experimental models. Actually, in humans, unlike in mice, obesity is associated with poor vitamin D status (Bouillon et al., 2014).
Among the carotenoids, the most important is lycopene (tomato, water melon, and pink grape fruit; Rao and Rao, 2007). Besides to be a very strong antioxidant, lycopene can give beta-carotene and retinoic acid, and the latter can activate the RXR receptor (Figure 2). Although higher intakes of dietary carotenoids, vitamin C, and vitamin E did not reduce the risk of MS in women (Zhang et al., 2001), the relevance of lycopene and vitamin A against inflammation cannot be disregarded.
Omega-3 (n-3) Essential Fatty Acids and Poly-Unsaturated Fatty Acids from Vegetables, Seafood, and Fish Oil
n-3 essential fatty acids (EFA) and PUFA represent a valid alternative to saturated fatty acids of animal origin.
Vegetable and vegetable oils contain the essential fatty acids linoleic acid (n-6) and linolenic acid (n-3). n-6 and n-3 fatty acids have opposite effects and their presence in the diet should be equivalent (Schmitz and Ecker, 2008). However, in Western diets, the ratio n-6/n-3 is increased from 6 to 15 times and this leads to a higher incidence of cardiovascular and inflammatory diseases. In fact, the linoleic acid leads to the formation of arachidonic acid (20:4), the precursor of the proinflammatory eicosanoids prostaglandins-2, leukotrienes-4, and thromboxanes-2. The synthesis of these eicosanoids is favored by insulin, and inhibited by aspirin, as well as by the n-3 long-chain PUFA EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid), which derive from n-3 linolenic acid.
Both DHA and EPA are found in seafood and fish oil. Both show remarkable anti-inflammatory, anti-thrombotic, and immune-modulatory activities, comparable with those of statins (Calder, 2006; Farooqui et al., 2007). n-3 PUFA inhibit inflammatory processes and the synthesis of fatty acids and cholesterol, and instead they stimulate the oxidation of fatty acids. On this basis, in chronic inflammatory diseases such as MS, n-3 essential fatty acids (EFA) and n-3 PUFA should prevail in the diet over the n-6 fatty acids. It is interesting to note that DHA is present in high concentrations in the brain and its levels decrease in patients with MS.
In cultured microglial cells activated by LPS, fish oil is as effective as interferon-? in inhibiting the expression of MMP-9 (gelatinase B), an important mediator of neuro-inflammation (Liuzzi et al., 2004, 2007). Moreover, n-3 PUFA significantly decreased MMP-9 levels in few clinical trials, indicating that n-3 PUFA may represent a good complementary treatment in the course of MS (Weinstock-Guttman et al., 2005; Mehta et al., 2009; Shinto et al., 2009). Fish oil has been also found to improve motor performances in healthy rat pups (Coluccia et al., 2009).
n-3 PUFA act in synergy with aspirin on AMPK and COX enzymes but with different mechanisms. Noteworthy, in the presence of aspirin, EPA and DHA form new anti-inflammatory bioactive molecules called resolvins, protectins, and maresins, which are able to reduce cellular inflammation and inflammatory pain (Xu et al., 2010; Hong and Lu, 2013; Serhan and Chiang, 2013). This may be a relevant aspect related to the nutritional intervention in MS. Indeed, the inflammatory processes associated to MS could be also due to the low ratio omega-3 (anti-inflammatory)/omega 6 (inflammatory) PUFA and thereby to the low production of adequate amounts of resolution-inducing molecules lipoxins, resolvins, and protectins that suppress inflammation. Hence, administration of omega-3 PUFA together with aspirin or directly of lipoxins, resolvins, and protectins may form a new approach in the prevention and treatment of MS and other neuroinflammatory diseases. Furthermore, other anti-inflammatory and antiangiogenic eicosanoids can also be produced by the P450 CYP enzymes from EPA and DHA (Yanai et al., 2014). In this context, it should be taken into consideration that statins may interfere negatively with the metabolism of n-3 and n-6, as they can decrease the n-3/n-6 ratio. Thus, treatment with statins should be associated with n-3 PUFA supplementation (Harris et al., 2004).
Seeds oils, from sunflower, corn, soybean, and sesame, contain more n-6 fatty acids than n-3 fatty acids and therefore their assumption should be limited in MS, in order to limit the level of proinflammatory eicosanoid production. On the other hand, coconut oil has a high content of saturated fatty acids. Among vegetable oils, olive oil should be preferred for the good ratio between saturated and unsaturated fatty acids, and because it contains the antioxidant hydroxytyrosol.
Thiolic compounds as Dietary Supplements
Compounds containing thiol groups (�SH) such as ?-lipoic acid (ALA), glutathione, and N-acetylcysteine (NAC) should be taken into consideration as possible dietary supplements to be used for the complementary treatment of MS.
As polyphenols, ALA (Salinthone et al., 2008; green plants and animal foods) has immunomodulatory and anti-inflammatory properties. ALA stabilizes the integrity of the BBB and stimulates the production of cAMP and the activity of protein kinase A. Also NAC might be useful in neurological disorders. It passes through the BBB and protects from inflammation (Bavarsad Shahripour et al., 2014).
The Mediterranean Diet
A recent systematic review and meta-analysis of intervention trials provide evidence that Mediterranean diet patterns reduce inflammation and cardiovascular mortality risk and improves endothelial functions (Schwingshackl and Hoffmann, 2014). These findings are as much encouraging as you think that the true Mediterranean diet is a little different from the one currently described.
It is generally agreed that the Mediterranean diet is based on consumption of extra-virgin olive oil, unrefined cereals, legumes, diverse vegetables (in particular tomatoes) and fruits, dairy products (mostly as pecorino cheese, ricotta, mozzarella, and yogurt), fish and fishery products, and low consumption of animal fat and meat. However, currently, the Mediterranean diet tends to a high consumption of pasta and bread, which means a high intake of gluten.
Once, in true Mediterranean diet, in Southern Italy, meat was eaten two or at most three times a week, only olive oil was used for cooking (extra-virgin quality and the most possible raw), but notably the intake of gluten was about half compared with the current intake. The pasta was eaten with the classic home-made tomato sauce, but in alternative, it was most often mixed with other gluten-free foods. The most common recipes were pasta and potatoes; pasta with either green beans, or artichokes, zucchini, eggplant, turnips, or cabbage; pasta with a mix of vegetables and legumes (minestrone: vegetable soup); and pasta with chickpeas, beans, or lentils. The sugar-sweetened drinks of today were not known. A high assumption of gluten-rich food may lead to nonceliac asymptomatic gluten sensitivity, mucosal intestinal damage, changes in gut microbiota, and low-grade intestinal inflammation. In conclusion, the Mediterranean diet is good, but the intake of gluten must be limited and must be whole grains.
Inflammatory and Anti-Inflammatory Lifestyle
Smoking (Proinflammatory)
Only a few studies have been carried out on the impact of smoking on the course of MS and results are conflicting, perhaps because its effects are difficult to ascertain and enucleate from other factors. Weiland et al. (2014) have found no association between smoking and relapse rate or disease activity, but do not exclude that smokers might have a significantly lower health-related quality of life than non-smokers, whereas Manouchehrinia et al. (2013) found that smoking is associated with more severe disease.
However, as it is shown in Figure 2, it can be expected that cigarette smoke may worsen the course of MS, as it may inhibit the anti-inflammatory activity of Sirtuins (Caito et al., 2010). The oxidative and carbonyl stress induced by cigarette smoke can be reversed by resveratrol (Liu et al., 2014).
Alcohol Consumption (Proinflammatory)
Recent studies shows that alcohol (beer, wine, or liquor) consumption is not associated to MS risk (Massa et al., 2013; Hedstr�m et al., 2014). However, as also shown in Figure 2, alcohol may inhibit the Sirtuin SIRT1 and activate the transcriptional activity of SREBP-1c (You et al., 2008), thus promoting the biosynthesis of lipids and inflammation at the expense of oxidative metabolism.
There are other two aspects of ethanol that should be considered. First, the metabolism of ethanol converts a large number of NAD+ molecules to NADH, limiting the availability of NAD+ required for the activity of Sirtuins. Second, as a substrate of the P450 enzymes, ethanol can interfere with the metabolism of drugs, which are transformed by the same enzymes. The result may be the prolongation and the enhancement of drug action. Altogether, alcohol should be considered as a molecule that interferes with the normal metabolism and facilitates the inflammatory process, complicating the possibility of improving the wellbeing of the patient.
Calorie Restriction (Anti-Inflammatory)
High-calorie intake and a meal rich in refined carbohydrates and sugar increase insulin level and favors biosynthesis, including the production of proinflammatory molecules and the production of free radicals. Calorie restriction, obtained by decreasing food intake or by intermittent fasting (one day and the other not), upregulates the level of SIRT1 (Zhang et al., 2011), increases the level of AMP and upregulates AMPK, increases adiponectin levels and upregulate or activate its receptors (Lee and Kwak, 2014), and downregulates oxidative damage, lymphocyte activation, and the progression of experimental models of MS (Piccio et al., 2008, 2013). The effects of calorie restriction can be mimicked by agonists (resveratrol and other polyphenols), acting on the same targets (SIRT1, AMPK).
Physical Exercise (Anti-Inflammatory)
Physical exercise is now an almost accepted practice also for MS patients and is commonly applied in order to decrease the symptoms of chronic fatigue and prevent or slow the onset of disability. However, the importance of physical exercise goes beyond that of simple muscle activity and should be rather considered in a holistic context in which diet, exercise, therapy, and social interchange, all play a role for the wellness of MS patients (Gacias and Casaccia, 2013).
Dietary control and exercise practice have been proposed by the WHO (2010) to attenuate or prevent human chronic diseases.
From a molecular point of view, physical exercise exerts its beneficial effect by acting on the protein kinase AMPK axis and the AMPK�Sirtuins�PPAR-? network, upregulating oxidative metabolism and downregulating biosynthetic pathways and inflammation (Narkar et al., 2008). As AMPK has a key role in energy balance, it is important to mention its agonists. Resveratrol and AMPK agonists such as metformin, a drug used in type 2 diabetes, can mimic or enhance the effect of physical activity and are effective in experimental encephalitis (Nath et al., 2009).
Physical exercise influences the quality of life and may stimulate the production of anti-inflammatory cytokines (Florindo, 2014). Furthermore, physical exercise lowers plasma levels of leptin and reduces gene expression of leptin receptors in the liver (Yasari et al., 2009), while increasing adiponectin levels and adiponectin receptors activity (Lee and Kwak, 2014).
The association of physical exercise with calorie restriction leads to a significant reduction of inflammatory markers (Reed et al., 2010).
Recent studies carried on adult C57BL/6 J male mice have shown that exercise stimulate brain mitochondrial activity, potentiate neuroplasticity, and is associated to mood improvement, as it decrease anxiety-like behaviors in the open field and exert antidepressant-like effects in the tail suspension test (Aguiar et al., 2014). Other studies performed on rats showed that exercise can alter the composition and diversity of gut bacteria (Petriz et al., 2014).
On these grounds, MS patients should practice mild physical exercise (brisk walking, swimming, or even dancing), if possible in the course of a rehabilitation program.
Nutritional Clinical Trials in MS So Far
Unfortunately, nutritional clinical trials in MS are only very few. Some of them were based on diets low in saturated fat, either without supplements (Swank and Goodwin, 2003) or with omega-3 fat supplements (Nordvik et al., 2000; Weinstock-Guttman et al., 2005). Other clinical trials were based on the administration of single dietary supplements only: either vitamin D, or fish oil (n-3 PUFA), or lipoic acid. Clinical trials with single polyphenols were performed only in cancer. Dietary supplements have never been used together and have never been associated with dietary prescription.
Taken together, clinical attempts to clarify the role of nutrition in MS were considered only promising of poor quality or with no clear results (Farinotti et al., 2007, 2012). In particular, as reported by Farinotti et al. in their Cochrane review (2012), supplements such as n-3 PUFA seem to have no major effect on the main clinical outcome in MS, but they may reduce the frequency of relapses over 2 years. Data available were considered to be insufficient or of uncertain quality to assess a real effect from PUFA supplementation. In some studies, slight possible benefits in relapse outcomes were found with omega-6 fatty acids, but data were characterized by the reduced validity of the endpoints. In general, trial quality was found to be poor. Studies on vitamin supplementation were not analyzed as none met the eligibility criteria, mainly due to lack of clinical outcomes. Thus, evidence on the benefits and risks of vitamin supplementation and antioxidant supplements in MS is lacking.
Suggestions for a Nutritional Intervention in MS: The Choice of Diet and Dietary Supplements
At the end, the goal of a nutritional intervention in MS must be the control of inflammation and this, as shown in this review, can be achieved mainly by controlling postprandial inflammation, the composition of gut microbiota and intestinal and systemic inflammation, and immunity. This can be achieved by a long-term dietary intervention, with a hypocaloric diet, prebiotics, probiotics, and dietary supplements.
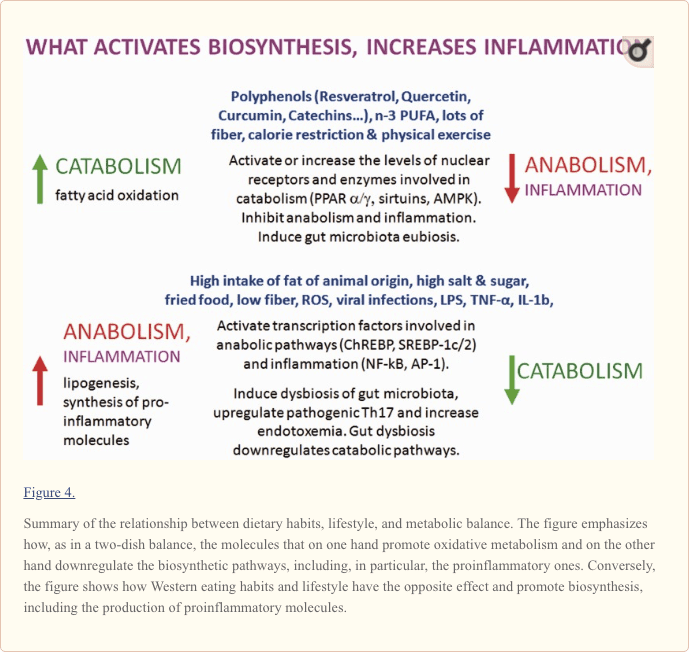
As reported in this article, healthy dietary molecules, calorie restriction, and exercise are able to direct cell metabolism toward catabolism and downregulate anabolism and inflammation by interacting at different levels with specific enzymes, nuclear receptors, and transcriptional factors. Furthermore, in association with fiber, they can shift gut dysbiosis to eubiosis.
As a result, low-calorie meals (1,600�1,800 kcal) based on vegetables, whole cereals, legumes, fruit, and fish may slow down the progression of the disease and ameliorate the wellness of MS patients, whereas hypercaloric diets with high intake of salt, saturated animal fat, fried food, and sugar-sweetened drinks may lead to the onset of postprandial inflammation and systemic low-grade inflammation.
Diet should be integrated with prebiotics, probiotics, specific vitamins (D, A, B12, and nicotinic acid), oligoelements (magnesium and selenium), and dietary supplements such as polyphenols, n-3 PUFA, and lipoic acid.
Prebiotics for MS should include inulin, bran, lactosucrose, and oligofructose, preferential nutrients for colonocytes and capable to inactivate NF-kB. Probiotics, such as lactococcus lactis, bifidobacterium lactis, and clostridium butyricum, which can improve the intestinal microbial balance, can be used to change the composition of colonic microbiota. The combination of prebiotics and probiotics is highly recommended. Bowel functions and weight should always be under control.
A more drastic therapeutic approach aimed to restore gut eubiosis and downregulate inflammation may be represented by fecal microbiota transplantation (FMT; Smits et al., 2013). The method seems to be very effective but still primitive, not completely safe, and in a way also disgusting. The field should move beyond fecal transplants, identify the organisms that may be essential for a particular condition, and provide those organisms in a much simpler fashion than FMT (�Critical Views in Gastroenterology & Hepatology,� 2014).
Dietary supplements, with the only exception of omega-3 PUFA, which are normal constituents of our body, are useful at the beginning of the nutritional intervention, or in the course of relapses, to facilitate the recovery of a healthy condition, but their use should be restricted to only a limited period of time (3�4 months). This is particularly valid for the polyphenols. Polyphenols are not well-known molecules with regard to their bioavailability and their biological effects and special precautions should be used when supplementing the diet with them. On one hand, they can downregulate the synthesis of proinflammatory molecules in the course of inflammatory processes; on the other hand, they can stimulate cell activity in resting cells, but a persistent stimulation can induce the apoptosis of healthy cells. Taken together, these considerations suggest that administration of purified polyphenols should be performed on the basis of preliminary clinical trials to test their effectiveness as dietary supplements and to determine their long-term safety and the right dosage.
In general, a nutritional intervention with anti-inflammatory food and dietary supplements decreases the biosynthesis of proinflammatory compounds and therewith makes more effective the use of immune-modulatory drugs, and eventually might limit their possible adverse effects, alleviate the symptoms of chronic fatigue syndrome, and favor patient wellness. However, diet and dietary supplements should not be treated as drugs and as a substitute of therapy. Similarly, proinflammatory food is not toxic and there is no need to exclude it completely. You can eat a nice steak or fried food without risk or guilt, if you are in a basically healthy condition. What hurts are the wrong eating habits in the long run.
Multiple sclerosis, or MS, is a chronic, progressive disease involving damage to the myelin sheaths of nerve cells. The epidemiology of MS suggests that various factors are often involved in the clinical expression of the health issue. However, numerous research studies have primarily evaluated the role of diet on the development of multiple sclerosis. For several years, healthcare professionals believed there was a correlation between the consumption of dairy in patients with multiple sclerosis. According to various research studies, a significant correlation between cow milk and the prevalence of multiple sclerosis was found, suggesting a possible role of dairy products in the multifactorial etiology of MS. Dr. Alex Jimenez D.C., C.C.S.T.
Conclusions
So, at first glance, MS does not seem to have any of the characteristics of chronic inflammatory diseases, which could be related to wrong dietary habits and lifestyle, or even to a dysbiotic gut microbiota. There is apparently nothing in an exacerbation of the disease that may be linked to food or the state of the intestinal microbiota. In fact, when we began our studies on the impact of nutrition on MS, there was not even the slightest clue that there could exist a real link between them, and the idea of the involvement of gut microbiota in MS was considered only very speculative. To date, the idea that dietary habits might influence the course of MS is still struggling to establish itself. Not so in cardiovascular diseases and other chronic inflammatory conditions, in which the influence of dietary habits is almost accepted, and not even in cancer, which is increasingly considered as a metabolic disorder (Seyfried et al., 2014).
At present, MS therapy is not associated to any particular diet, probably due to lack of information on the effects of nutrition on the disease. However, the majority of patients with MS is looking for complementary and alternative treatments (CAM), and in particular is trying to change dietary habits, almost without the advice of the physician (Schwarz et al., 2008; Leong et al., 2009). A recent study based on data provided by MS patients in response to a questionnaire on their dietary habits seems to support a significant association of healthy dietary habits with better physical and mental health-related quality of life and a lower level of disability (Hadgkiss et al., 2014). These data reinforce the idea of the need for randomized controlled trials of nutritional intervention for people with MS. It should be emphasized that nutritional treatments should be complementary, but not alternative to therapy, be part of a holistic approach and performed under medical control.
As there are no data available from clinical trials yet, our work is aimed to rationalize dietary choices on the basis of known and established effects of dietary factors and lifestyle at the molecular level. Data reported in Figure 2 are obviously not complete but may be useful to provide guidelines for nutritional interventions. In principle, proinflammatory food upregulate the biosynthetic and inflammatory pathways, as shown on the right and at the bottom of Figure 2, whereas anti-inflammatory food upregulates oxidative metabolism and downregulates anabolism and inflammation.
As shown in this article, the finding that calorie restriction, exercise, and particular dietary factors can influence the degree of inflammatory responses by acting on both cellular metabolism (Figure 2) and composition of gut microbiota (Figure 5), suggests that an appropriate nutritional intervention may ameliorate the course of the disease and may be therefore taken in consideration as a possible complementary treatment in MS. As inflammation is present in both RRMS and PPMS, nutritional advices are indicated for both forms of the disease. This is particularly important in the case of PPMS, for which no cure is presently available. Conversely, as specific dietary habits may be detrimental and may promote a chronic state of low-grade inflammation, a wrong diet may be considered a possible contributory cause of relapses in MS.
Taken together, we have now a better knowledge of the possible influence of dietary factors on cell metabolism and gut microbiota, and on their possible effects on the disease, but, clearly, we are only just beginning to understand the role of nutrition and gut microbiota in MS and much work remains in terms of understanding the nature of the interactions of gut microbiota with the host�s immune system, especially at sites distal to the intestine.
On these grounds, future prospects in MS research should regard the following points: (a) assess gut microbiota composition; (b) evaluate defects in intestinal immune system; (c) clarify the role of polyphenols and vitamin D metabolism; (d) study the impact of dietary factors, herbs, and drugs on AMPK, Sirtuins, PPAR, or directly on NF-kB. Noteworthy, some drugs used to treat type II diabetes, such as the PPAR-? agonists thiazolidinediones (Bernardo et al., 2009), and the AMPK agonist metformin (Nath et al., 2009) have anti-inflammatory effects comparable with those of anti-inflammatory dietary factors; (e) define possible interferences between dietary supplements and MS drugs; (f) promote a campaign aimed to educate about the importance to follow a healthy diet during therapy, for instance, encouraging patients to include fiber or complex carbohydrates in their diet, supplementing with probiotics, choosing n-3 fats over proinflammatory n-6 fats, and limiting meat and animal fat consumption. The choice of good recipes, such as those described by Mollie Katzen (2013), can make the diet more acceptable.
Overall, immune-modulatory conventional MS therapies have been almost successful; however, drugs that can protect and favor repair mechanisms are still missing. We can decide to help people stay healthy by providing nutritional guidance and physical activity opportunities. For the moment, there are only good prospects for improving the wellbeing of patients with MS. We are only at the beginning of the story.
Summary
As both relapsing-remitting MS and primary-progressive MS are inflammatory diseases, they can be influenced by proinflammatory or anti-inflammatory dietary habits and lifestyle through their action on cell metabolism and gut microbiota. Nutritional advice to MS patients may favor their wellness.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Italian Foundation for Multiple Sclerosis (FISM) with grants 2007/R/15 for the Project �Healthy and Functional Foods for MS patients,� 2010/R/35 for the Project �The Molecular Basis for Nutritional Intervention in Multiple Sclerosis,� and 2014/S/2 (2014�2015) for the project �Nutritional Facts in Multiple Sclerosis: Why They Are Important and How They Should Be Managed� to P. R.
Many doctors greatly recommend that patients with multiple sclerosis, or MS, avoid dairy because various research studies have demonstrated a high correlation between MS and dairy, especially cow�s milk. This is largely due to the fact that the proteins in cow�s milk are generally targeted by the immune system of patients with multiple sclerosis. Furthermore, some proteins in cow�s milk imitate part of the myelin oligodendrocyte glycoprotein, or MOG, the section of myelin which triggers the autoimmune response in multiple sclerosis that can trick the immune system to attack and destroy the MOG. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
The knee is the largest joint in the human body, where the complex structures of the lower and upper legs come together. Consisting of three bones, the femur, the tibia, and the patella which are surrounded by a variety of soft tissues, including cartilage, tendons and ligaments, the knee functions as a hinge, allowing you to walk, jump, squat or sit. As a result, however, the knee is considered to be one of the joints that are most prone to suffer injury. A knee injury is the prevalent cause of knee pain.
A knee injury can occur as a result of a direct impact from a slip-and-fall accident or automobile accident, overuse injury from sports injuries, or even due to underlying conditions, such as arthritis. Knee pain is a common symptom which affects people of all ages. It may also start suddenly or develop gradually over time, beginning as a mild or moderate discomfort then slowly worsening as time progresses. Moreover, being overweight can increase the risk of knee problems. The purpose of the following article is to discuss the evaluation of patients presenting with knee pain and demonstrate their differential diagnosis.
Abstract
Knee pain is a common presenting complaint with many possible causes. An awareness of certain patterns can help the family physician identify the underlying cause more efficiently. Teenage girls and young women are more likely to have patellar tracking problems such as patellar subluxation and patellofemoral pain syndrome, whereas teenage boys and young men are more likely to have knee extensor mechanism problems such as tibial apophysitis (Osgood-Schlatter lesion) and patellar tendonitis. Referred pain resulting from hip joint pathology, such as slipped capital femoral epiphysis, also may cause knee pain. Active patients are more likely to have acute ligamentous sprains and overuse injuries such as pes anserine bursitis and medial plica syndrome. Trauma may result in acute ligamentous rupture or fracture, leading to acute knee joint swelling and hemarthrosis. Septic arthritis may develop in patients of any age, but crystal-induced inflammatory arthropathy is more likely in adults. Osteoarthritis of the knee joint is common in older adults. (Am Fam Physician 2003;68:917-22. Copyright� 2003 American Academy of Family Physicians.)
Introduction
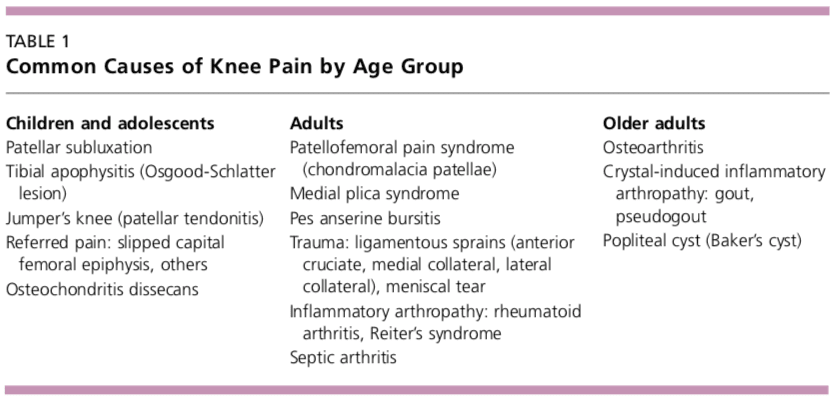
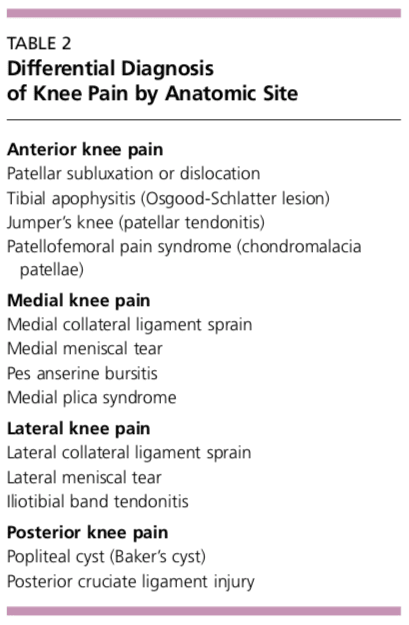
Determining the underlying cause of knee pain can be difficult, in part because of the extensive differential diagnosis. As discussed in part I of this two-part article,1 the family physician should be familiar with knee anatomy and common mechanisms of injury, and a detailed history and focused physical examination can narrow possible causes. The patient�s age and the anatomic site of the pain are two factors that can be important in achieving an accurate diagnosis (Tables 1 and 2). �
�
�
Children and Adolescents
Children and adolescents who present with knee pain are likely to have one of three common conditions: patellar subluxation, tibial apophysitis, or patellar tendonitis. Additional diagnoses to consider in children include slipped capital femoral epiphysis and septic arthritis.
Patellar Subluxation
Patellar subluxation is the most likely diagnosis in a teenage girl who presents with giving-way episodes of the knee.2 This injury occurs more often in girls and young women because of an increased quadriceps angle (Q angle), usually greater than 15 degrees.
Patellar apprehension is elicited by subluxing the patella laterally, and a mild effusion is usually present. Moderate to severe knee swelling may indicate hemarthrosis, which suggests patellar dislocation with osteochondral fracture and bleeding.
Tibial Apophysitis
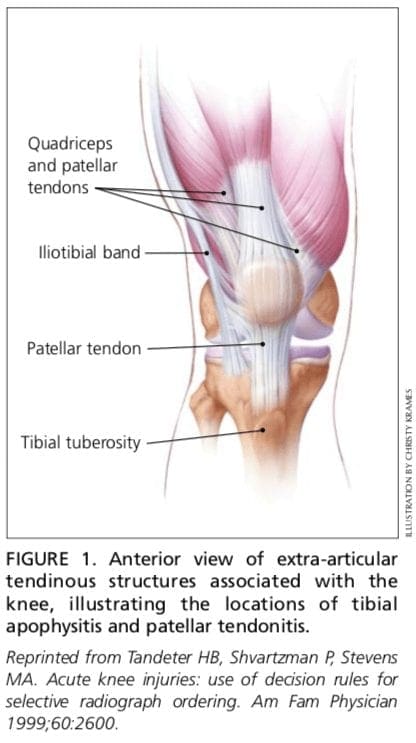
A teenage boy who presents with anterior knee pain localized to the tibial tuberosity is likely to have tibial apophysitis or Osgood- Schlatter lesion3,4 (Figure 1).5 The typical patient is a 13- or 14-year-old boy (or a 10- or 11-year-old girl) who has recently gone through a growth spurt.
The patient with tibial apophysitis generally reports waxing and waning of knee pain for a period of months. The pain worsens with�squatting, walking up or down stairs, or forceful contractions of the quadriceps muscle. This overuse apophysitis is exacerbated by jumping and hurdling because repetitive hard landings place excessive stress on the insertion of the patellar tendon.
On physical examination, the tibial tuberosity is tender and swollen and may feel warm. The knee pain is reproduced with the resisted active extension or passive hyperflexion of the knee. No effusion is present. Radiographs are usually negative; rarely, they show avulsion of the apophysis at the tibial tuberosity. However, the physician must not mistake the normal appearance of the tibial apophysis for an avulsion fracture. �
�
�
�
Patellar Tendonitis
Jumper�s knee (irritation and inflammation of the patellar tendon) most commonly occurs in teenage boys, particularly during a growth spurt2 (Figure 1).5 The patient reports vague anterior knee pain that has persisted for months and worsens after activities such as walking down stairs or running.
On physical examination, the patellar tendon is tender, and the pain is reproduced by resisted knee extension. There is usually no effusion. Radiographs are not indicated.
Slipped Capital Femoral Epiphysis
A number of pathologic conditions result in referral of pain to the knee. For example, the possibility of slipped capital femoral epiphysis must be considered in children and teenagers who present with knee pain.6 The patient with this condition usually reports poorly localized knee pain and no history of knee trauma.
The typical patient with slipped capital femoral epiphysis is overweight and sits on the examination table with the affected hip slightly flexed and externally rotated. The knee examination is normal, but hip pain is elicited with passive internal rotation or extension of the affected hip.
Radiographs typically show displacement of the epiphysis of the femoral head. However, negative radiographs do not rule out the diagnosis in patients with typical clinical findings. Computed tomographic (CT) scanning is indicated in these patients.
Osteochondritis Dissecans
Osteochondritis dissecans is an intra-articular osteochondrosis of unknown etiology that is characterized by degeneration and recalcification of articular cartilage and underlying bone. In the knee, the medial femoral condyle is most commonly affected.7
The patient reports vague, poorly localized knee pain, as well as morning stiffness or recurrent effusion. If a loose body is present, mechanical symptoms of locking or catching of the knee joint also may be reported. On physical examination, the patient may demonstrate quadriceps atrophy or tenderness along the involved chondral surface. A mild joint effusion may be present.7
Plain-film radiographs may demonstrate the osteochondral lesion or a loose body in the knee joint. If osteochondritis dissecans is suspected, recommended radiographs include anteroposterior, posteroanterior tunnel, lateral, and Merchant�s views. Osteochondral lesions at the lateral aspect of the medial femoral condyle may be visible only on the posteroanterior tunnel view. Magnetic resonance imaging (MRI) is highly sensitive in detecting these abnormalities and is indicated in patients with a suspected osteochondral lesion.7 �
�
A knee injury caused by sports injuries, automobile accidents, or an underlying condition, among other causes, can affect the cartilage, tendons and ligaments which form the knee joint itself. The location of the knee pain can differ according to the structure involved, also, the symptoms can vary. The entire knee may become painful and swollen as a result of inflammation or infection, whereas a torn meniscus or fracture may cause symptoms in the affected region. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Adults
Overuse Syndromes
Anterior Knee Pain. Patients with patellofemoral pain syndrome (chondromalacia patellae) typically present with a vague history of mild to moderate anterior knee pain that usually occurs after prolonged periods of sitting (the so-called �theater sign�).8 Patellofemoral pain syndrome is a common cause of anterior knee pain in women.
On physical examination, a slight effusion may be present, along with patellar crepitus on the range of motion. The patient�s pain may be reproduced by applying direct pressure to the anterior aspect of the patella. Patellar tenderness may be elicited by subluxing the patella medially or laterally and palpating the superior and inferior facets of the patella. Radiographs usually are not indicated.
Medial Knee Pain. One frequently overlooked diagnosis is medial plica syndrome. The plica, a redundancy of the joint synovium medially, can become inflamed with repetitive overuse.4,9 The patient presents with acute onset of medial knee pain after a marked increase in usual activities. On physical examination, a tender, mobile nodularity is present at the medial aspect of the knee, just anterior to the joint line. There is no joint effusion, and the remainder of the knee examination is normal. Radiographs are not indicated.
Pes anserine bursitis is another possible cause of medial knee pain. The tendinous insertion of the sartorius, gracilis, and semitendinosus muscles at the anteromedial aspect of the proximal tibia forms the pes anserine bursa.9 The bursa can become inflamed as a result of overuse or a direct contusion. Pes�anserine bursitis can be confused easily with a medial collateral ligament sprain or, less commonly, osteoarthritis of the medial compartment of the knee. �
�
�
The patient with pes anserine bursitis reports pain at the medial aspect of the knee. This pain may be worsened by repetitive flexion and extension. On physical examination, tenderness is present at the medial aspect of the knee, just posterior and distal to the medial joint line. No knee joint effusion is present, but there may be slight swelling at the insertion of the medial hamstring muscles. Valgus stress testing in the supine position or resisted knee flexion in the prone position may reproduce the pain. Radiographs are usually not indicated.
Lateral Knee Pain. Excessive friction between the iliotibial band and the lateral femoral condyle can lead to iliotibial band tendonitis.9 This overuse syndrome commonly occurs in runners and cyclists, although it may develop in any person subsequent to activity involving repetitive knee flexion. The tightness of the iliotibial band, excessive foot pronation, genu varum, and tibial torsion are predisposing factors.
The patient with iliotibial band tendonitis reports pain at the lateral aspect of the knee joint. The pain is aggravated by activity, particularly running downhill and climbing stairs. On physical examination, tenderness is present at the lateral epicondyle of the femur, approximately 3 cm proximal to the joint line. Soft tissue swelling and crepitus also may be present, but there is no joint effusion. Radiographs are not indicated.
Noble�s test is used to reproduce the pain in iliotibial band tendonitis. With the patient in a supine position, the physician places a thumb over the lateral femoral epicondyle as the�patient repeatedly flexes and extends the knee. Pain symptoms are usually most prominent with the knee at 30 degrees of flexion.
Popliteus tendonitis is another possible cause of lateral knee pain. However, this condition is fairly rare.10
Trauma
Anterior Cruciate Ligament Sprain. Injury to the anterior cruciate ligament usually occurs because of noncontact deceleration forces, as when a runner plants one foot and sharply turns in the opposite direction. Resultant valgus stress on the knee leads to anterior displacement of the tibia and sprain or rupture of the ligament.11 The patient usually reports hearing or feeling a �pop� at the time of the injury and must cease activity or competition immediately. Swelling of the knee within two hours after the injury indicates rupture of the ligament and consequent hemarthrosis.
On physical examination, the patient has a moderate to severe joint effusion that limits the range of motion. The anterior drawer test may be positive, but can be negative because of hemarthrosis and guarding by the hamstring muscles. The Lachman test should be positive and is more reliable than the anterior drawer test (see text and Figure 3 in part I of the article1).
Radiographs are indicated to detect possible tibial spine avulsion fracture. MRI of the knee is indicated as part of a presurgical evaluation.
Medial Collateral Ligament Sprain. Injury to the medial collateral ligament is fairly common and is usually the result of acute trauma. The patient reports a misstep or collision that places valgus stress on the knee, followed by the immediate onset of pain and swelling at the medial aspect of the knee.11
On physical examination, the patient with medial collateral ligament injury has point tenderness at the medial joint line. Valgus stress testing of the knee flexed to 30 degrees reproduces the pain (see text and Figure 4 in part I of this article1). A clearly defined endpoint on valgus stress testing indicates a grade 1�or grade 2 sprain, whereas complete medial instability indicates full rupture of the ligament (grade 3 sprain).
Lateral Collateral Ligament Sprain. Injury of the lateral collateral ligament is much less common than the injury of the medial collateral ligament. Lateral collateral ligament sprain usually results from varus stress to the knee, as occurs when a runner plants one foot and then turns toward the ipsilateral knee.2 The patient reports acute onset of lateral knee pain that requires prompt cessation of activity.
On physical examination, point tenderness is present at the lateral joint line. Instability or pain occurs with varus stress testing of the knee flexed to 30 degrees (see text and Figure 4 in part I of this article1). Radiographs are not usually indicated.
Meniscal Tear. The meniscus can be torn acutely with a sudden twisting injury of the knee, such as may occur when a runner suddenly changes direction.11,12 Meniscal tear also may occur in association with a prolonged degenerative process, particularly in a patient with an anterior cruciate ligament-deficient knee. The patient usually reports recurrent knee pain and episodes of catching or locking of the knee joint, especially with squatting or twisting of the knee.
On physical examination, a mild effusion is usually present, and there is tenderness at the medial or lateral joint line. Atrophy of the vastus medialis obliquus portion of the quadriceps muscle also may be noticeable. The McMurray test may be positive (see Figure 5 in part I of this article1), but a negative test does not eliminate the possibility of a meniscal tear.
Plain-film radiographs usually are negative and seldom are indicated. MRI is the radiologic test of choice because it demonstrates most significant meniscal tears.
Infection
Infection of the knee joint may occur in patients of any age but is more common in those whose immune system has been weakened by cancer, diabetes mellitus, alcoholism,�acquired immunodeficiency syndrome, or corticosteroid therapy. The patient with septic arthritis reports abrupt onset of pain and swelling of the knee with no antecedent trauma.13
On physical examination, the knee is warm, swollen, and exquisitely tender. Even slight motion of the knee joint causes intense pain.
Arthrocentesis reveals turbid synovial fluid. Analysis of the fluid yields a white blood cell count (WBC) higher than 50,000 per mm3 (50 ? 109 per L), with more than 75 percent (0.75) polymorphonuclear cells, an elevated protein content (greater than 3 g per dL [30 g per L]), and a low glucose concentration (more than 50 percent lower than the serum glucose concentration).14 Gram stain of the fluid may demonstrate the causative organism. Common pathogens include Staphylococcus aureus, Streptococcus species, Haemophilus influenza, and Neisseria gonorrhoeae.
Hematologic studies show an elevated WBC, an increased number of immature polymorphonuclear cells (i.e., a left shift), and an elevated erythrocyte sedimentation rate (usually greater than 50 mm per hour).
Older Adults
Osteoarthritis
Osteoarthritis of the knee joint is a common problem after 60 years of age. The patient presents with knee pain that is aggravated by weight-bearing activities and relieved by rest.15 The patient has no systemic symptoms but usually awakens with morning stiffness that dissipates somewhat with activity. In addition to chronic joint stiffness and pain, the patient may report episodes of acute synovitis.
Findings on physical examination include decreased range of motion, crepitus, a mild joint effusion, and palpable osteophytic changes at the knee joint.
When osteoarthritis is suspected, recommended radiographs include weight-bearing anteroposterior and posteroanterior tunnel views, as well as non-weight-bearing Merchants and lateral views. Radiographs show�joint-space narrowing, subchondral bony sclerosis, cystic changes, and hypertrophic osteophyte formation.
Crystal-Induced Inflammatory Arthropathy
Acute inflammation, pain, and swelling in the absence of trauma suggest the possibility of a crystal-induced inflammatory arthropathy such as gout or pseudogout.16,17 Gout commonly affects the knee. In this arthropathy, sodium urate crystals precipitate in the knee joint and cause an intense inflammatory response. In pseudogout, calcium pyrophosphate crystals are the causative agents.
On physical examination, the knee joint is erythematous, warm, tender, and swollen. Even minimal range of motion is exquisitely painful.
Arthrocentesis reveals clear or slightly cloudy synovial fluid. Analysis of the fluid yields a WBC count of 2,000 to 75,000 per mm3 (2 to 75 ? 109 per L), a high protein content (greater than 32 g per dL [320 g per L]), and a glucose concentration that is approximately 75 percent of the serum glucose con- centration.14 Polarized-light microscopy of the synovial fluid displays negatively birefringent rods in the patient with gout and positively birefringent rhomboids in the patient with pseudogout.
Popliteal Cyst
The popliteal cyst (Baker�s cyst) is the most common synovial cyst of the knee. It originates from the posteromedial aspect of the knee joint at the level of the gastrocnemio-semimembranous bursa. The patient reports insidious onset of mild to moderate pain in the popliteal area of the knee.
On physical examination, palpable fullness is present at the medial aspect of the popliteal area, at or near the origin of the medial head of the gastrocnemius muscle. The McMurray test may be positive if the medial meniscus is injured. Definitive diagnosis of a popliteal cyst may be made with arthrography, ultrasonography, CT scanning, or, less commonly, MRI.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
In conclusion, although the knee is the largest joint in the human body where the structures of the lower extremities meet, including the femur, the tibia, the patella, and many other soft tissues, the knee can easily suffer damage or injury and result in knee pain. Knee pain is one of the most common complaints among the general population, however, it commonly occurs in athletes. Sports injuries, slip-and-fall accidents, and automobile accidents, among other causes, can lead to knee pain.
As described in the article above, diagnosis is essential towards determining the best treatment approach for each type of knee injury, according to their underlying cause. While the location and the severity of the knee injury may vary depending on the cause of the health issue, knee pain is the most common symptom. Treatment options, such as chiropractic care and physical therapy, can help treat knee pain. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez �
�
�
Additional Topic Discussion: Relieving Knee Pain without Surgery
�
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Calmbach WL, Hutchens M. Evaluation of patients presenting with knee pain: part I. History, physical examination, radiographs, and laboratory tests. Am Fam Physician 2003;68:907-12.
2. Walsh WM. Knee injuries. In: Mellion MB, Walsh WM, Shelton GL, eds. The team physician�s hand- book. 2d ed. St. Louis: Mosby, 1990:554-78.
3. Dunn JF. Osgood-Schlatter disease. Am Fam Physi- cian 1990;41:173-6.
4. Stanitski CL. Anterior knee pain syndromes in the adolescent. Instr Course Lect 1994;43:211-20.
5. Tandeter HB, Shvartzman P, Stevens MA. Acute knee injuries: use of decision rules for selective radiograph ordering. Am Fam Physician 1999;60: 2599-608.
6. Waters PM, Millis MB. Hip and pelvic injuries in the young athlete. In: DeLee J, Drez D, Stanitski CL, eds. Orthopaedic sports medicine: principles and practice. Vol. III. Pediatric and adolescent sports medicine. Philadelphia: Saunders, 1994:279-93.
7. Schenck RC Jr, Goodnight JM. Osteochondritis dis- secans. J Bone Joint Surg [Am] 1996;78:439-56.
8. Ruffin MT 5th, Kiningham RB. Anterior knee pain: the challenge of patellofemoral syndrome. Am Fam Physician 1993;47:185-94.
Sandra Rubio discusses the symptoms, causes, and treatments of neck pain. Headaches, migraines, dizziness, confusion, and weakness in the upper extremities are some of the most common symptoms associated with neck pain. Trauma from an injury, such as that from an automobile accident or a sports injury, or an aggravated condition due to improper posture can commonly cause neck pain and other symptoms. Dr. Alex Jimenez utilizes spinal adjustments and manual manipulations, among other chiropractic treatment methods like deep-tissue massage, to restore the alignment of the cervical spine and improve neck pain. Chiropractic care with Dr. Alex Jimenez is the non-surgical choice for restoring a patient’s overall well-being.
Neck Pain Symptoms & Chiropractic Treatment
Neck pain is a common health issue, with approximately two-thirds of the population being affected by neck pain at any time throughout their lives. Neck pain�that originates in the cervical spine, or upper spine, can be caused by numerous other spinal health issues. Neck pain can result due to the pinching of the nerves emanating from the vertebrae, or because of muscular tightness in both the upper spine and the neck. Joint disruption in the neck can generate a variety of other common symptoms, which�include�headaches, head pain, and migraines. There can also be a spinal joint discomfort. Neck pain affects about 5 percent of the global population as of 2010, according to statistics.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Dr. Alex Jimenez is excellent, he’s patient, he gets right to the point of the situation, and then helps you with your stretching and therapy to make sure that it doesn’t continue. I recommend him for everybody in El Paso, the whole state of Texas. He should be in every town, move to San Antonio. -�Ottis Hamlet
Are you aware of how dependent you are on the use of your hands for everyday tasks? As humans, we rely tremendously on the proper function of our hands, wrists and elbows to perform many physical activities. Many people may not understand how essential this can be until they encounter an injury or condition which impedes them from using their hands.
Hand, wrist and elbow pain can cause a wide variety of problems, preventing you from being able to take part in even some of the simplest, ordinary chores without experiencing painful symptoms. Based on the severity of the pain, health issues affecting your hands, wrists or elbows can prevent people from driving, utilizing a computer or other electronic devices, cooking dinner and it can even make working difficult.
To make matters worse, the condition of your hands can ultimately affect the entire condition of your upper extremities. An injury or aggravated condition along a single part of the hand, such as a finger, could cause pain to radiate through the wrist and elbow, into the arm and shoulder. Below, we will discuss the common causes of hand pain and their treatment.
Common Causes of Hand Pain
While many instances of hand pain, wrist pain and elbow pain may resolve on their own, a minor inconvenience can quickly become a much bigger health issue if left untreated. Painful symptoms can slow us down as we’re attempting to go about our day and chances are that the need to finish a job will continue to aggravate the pain and cause discomfort. If you experience chronic hand pain symptoms, you may want to visit a doctor immediately.
Because our arms and hands are interconnected, an injury or condition to any part of the upper extremities can end up causing anything from tingling sensations and numbness in the fingers to pain and discomfort in the arms. A qualified and experienced healthcare professional, such as a chiropractor, can help you understand the source of your hand pain as well as determine the best treatment option for your specific health issue.��
There are many health issues which might lead to pain and discomfort in the hands, elbows and wrists. Common causes of hand pain include:
Joint pain
Arthritis
Tendonitis
Tennis/Golf Elbow
Fractures
Sprains
Carpal tunnel syndrome
Carpal Tunnel Syndrome
One of the most common causes of hand pain is the result of a chronic condition called carpal tunnel syndrome. Carpal tunnel syndrome, or CTS, is a painful syndrome caused by a pinched nerve in the wrist which causes pain, tingling sensations and numbness in the hand and arm. The pain usually feels like a�profound and intense hand cramp although cramping is not a common symptom associated with carpal tunnel syndrome.
Carpal tunnel syndrome develops due to heightened stress and pressure on the median nerve, frequently due to highly repetitive movements with the hand and wrist. Some of the most common tasks in today’s society,�such as writing, typing on a keyboard, playing with video games, gardening, and anything else which requires repetitive alternative or lifting hand motions, have become one of the leading causes of carpal tunnel syndrome.
As mentioned above, several common symptoms of carpal tunnel syndrome, or CTS, may cause�severe pain in the hand, wrist and elbow, as well as result in tingling sensations and numbness which may radiate from the fingers up to the arm. Research studies have also found that patients who may be experiencing hormone fluctuations are at an increased risk of developing the condition. However, people who are most at risk of developing CTS have been found to be those who work in a position that requires them to engage in repetitive motions with their hands.
Many healthcare professionals recommend surgical interventions to treat carpal tunnel syndrome but many patients have experienced relief from their hand pain through the use of alternative treatment options, such as chiropractic care,. Moreover, wearing a brace, working to counteract repetitive motions and taking steps to decrease stress and pressure on the hand can help improve pain associated with carpal tunnel syndrome.
While a number of these treatment techniques and methods can be performed at home by the patient, it’s essential to seek immediate medical attention from a qualified and experienced healthcare professional to avoid further damage. A chiropractor can help treat hand pain. Below, we will describe how chiropractic care may improve chronic hand pain symptoms.
Because we depend tremendously on the use of our hands, injuries and/or conditions which result in hand pain, such as carpal tunnel syndrome, can be very debilitating, ultimately affecting every aspect of an individual’s quality of life. Chiropractic care is a safe and effective, alternative treatment option which can help treat hand pain. Through a series of exercise and physical activity programs, chiropractic care can help restore normal hand function and reduce hand pain. -�Dr. Alex Jimenez D.C., C.C.S.T.
Chiropractic Care for Hand Pain
Chiropractic care is a healthcare profession which utilizes spinal adjustments and manual manipulations to treat a variety of injuries and conditions associated with the musculoskeletal and nervous system. For a doctor of chiropractic, or chiropractor, the first step for managing hand, wrist or elbow pain is to evaluate the source of the symptoms.�
After the diagnosis, the chiropractor’s next priority is to use a series of alternative treatment options to relieve the patient’s hand pain as soon as possible. A chiropractor may use spinal adjustments and manual manipulations to carefully correct any spinal misalignments, or subluxations, which may be causing referred hand pain.
After that, a chiropractor may recommend a series of lifestyle modifications, including exercise and physical activity programs, in order to promote recovery and begin focusing on building the patient’s assortment of motion, particularly flexibility maneuvers. Stretches and exercises for building strength will be included following the patient’s treatment plan, in order to ensure no additional damage occurs.
When you’re ready to start, contact a chiropractor to set up an appointment to get yourself on the road to relieving your hand, wrist and/or elbow pain.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
One of my friends recommended me, over and over, and just extended how good he�(Dr. Alex Jimenez, D.C.) was. So I gave it a shot. I had really bad sciatica and it was killing me, I couldn’t walk, but he has been helping me out, I can walk now… I couldn’t walk more than 25 yards, it (sciatica) was really affecting me. I had to get some help. I can’t say enough about Dr. Jimenez, he’s been helping me out, I can walk.
Edgar M. Reyes
According to the American Association of Neurological Surgeons, approximately 75 to 85 percent of individuals in the United States alone will experience some form of back pain throughout their lifetime, where 50 percent will suffer more than one episode within a year. Back pain is one of the most common complaints frequently reported among the general population and it is often a symptom which could indicate the presence of another underlying condition. Back pain can be caused by a variety of factors, some due to bad habits, such as improper posture, and others due to injuries from accidents. Other health issues, such as degenerative disc disease, or DDD, and arthritis can also result in back pain.�While the causes can vary, they share the same symptoms.
Bak pain can include upper back pain, middle back pain and lower back pain, often connected to sciatica, or sciatic nerve pain, a condition characterized by the compression or impingement of the sciatic nerve found in the low back. Back pain and sciatica have been closely associated with several common health issues. Often times, sciatica, or sciatic nerve pain, is caused by an underlying health issue along the lumbar spine. The sciatic nerve is the longest nerve in the human body, which connects to nerve roots in the region of the lower back and runs through the buttocks, down along the hips and into the back of each leg. Further sections of this nerve then branch out from the calf to the foot and into the toes. Sciatica can be identified by the following symptoms.
Low back pain which radiates down one or both legs
Leg and/or foot pain along with tingling and burning sensations
Numbness in the leg, feet and/or toes
Persistent pain and discomfort on one or both sides of the buttocks
Intense painful symptoms in the lower extremities
Having difficulties when sitting and while getting up
It’s essential to understand that back pain and sciatica are not generally considered to be a specific health issue themselves but rather, they are usually only considered to be a collection of several symptoms associated with an underlying injury and/or condition. A proper diagnosis of the root cause of your symptoms is additionally important in order to safely and effectively treat back pain and sciatica. As mentioned above, numerous factors can cause back pain and sciatica symptoms. Below, we will discuss some of the most common spine health issues which can cause back pain and sciatica, including degenerative disc disease, lumbar spinal stenosis, lumbar herniated disc and spondylolisthesis. Approximately 90 percent of sciatica cases are due to disc herniations.
Degenerative Disc Disease
The degeneration of the intervertebral discs, found between each vertebrae of the spine, is a natural process which often occurs with age, while for some individuals, however, it can begin to develop earlier than usual. In a healthy spine, the intervertebral discs function as shock absorbers between the bones of the spine, which ultimately provide height and allow the back to remain flexible while resisting forces. As we begin to get older, these rubbery discs begin to shrink and lose integrity. Almost everyone will demonstrate signs of wear-and-tear along their spinal discs over time, but not everyone will experience degenerative disc disease, or DDD. Although not actually a disease, DDD refers to a condition in which pain with the degeneration of the intervertebral discs.
One or more degenerated discs along the length of the spine may irritate a nerve root and cause sciatica. This condition is commonly characterized when a reduced disc becomes exposed. Bone spurs can also develop with disc degeneration and can lead to sciatica. Symptoms of degenerative disc disease, or DDD, frequently occur along the lower back, however, they can also develop in the neck, depending on the location of the degenerated discs. Common symptoms of DDD include, pain and discomfort, particularly when sitting, bending, lifting or twisting, tingling sensations and/or numbness in the extremities, and lessened symptoms when walking and moving, as in with changing positions or lying down. Weakness in the leg muscles or foot drop may be a sign that there is damage to the nerve root.
Lumbar Spinal Stenosis
Another common cause of back pain and sciatica is lumbar spinal stenosis. The natural degeneration of the spine which occurs with age can cause a variety of changes to the spine. Lumbar spinal stenosis is brought on by a gradual narrowing of the spinal canal that is common in the aging process and it generally affects people over the age of 50. When the space around the spinal cord narrows, it can place unnecessary amounts of pressure on the spinal cord and nerve roots. Additionally, it can be the result of a bulging disk, enlarged aspect joints, or an overgrowth of tissue. Only a small number of individuals are born with spine health issues which can develop into lumbar spinal stenosis. This is known as congenital spinal stenosis and it is frequently diagnosed in men.
Arthritis, or the degeneration of any joint in the body, has been attributed to be the most common cause of spinal stenosis. As the intervertebral discs begin to wear-and-tear naturally begin, they can lose water content and eventually dry out, ultimately losing height and even collapsing. This can place pressure on the facet joints, the joints which provide flexibility and movement to the spine, resulting in arthritis. As a result, the ligaments around the structures of the spine can increase in size, lessening the space for the nerves. Also, the human body may respond by growing new bone, additionally narrowing the space for the nerves to pass through. Symptoms of lumbar spinal stenosis may include, pain, tingling or burning sensations, numbness and weakness, as well as less painful symptoms when leaning forward or sitting.
Lumbar Herniated Disc
A herniated disc is a condition which can occur anywhere along the length of the spine, however, it most commonly affects the lower back or lumbar spine. It may also be referred to as a bulging, protruding or ruptured disc. A lumbar herniated disc is considered to be one of the most common causes of back pain in the lower back, as well as sciatica. An intervertebral disc begins to herniate when the soft, jelly-like nucleus, known as the nucleus pulposus, pushes against its outer ring, known as the annulus fibrosus, due to wear-and-tear or a sudden injury. With persistent pressure, the jelly-like nucleus may push through the disc’s outer ring or it may cause the ring to bulge, putting additional pressure on the spinal chord and its surrounding nerve roots.
Moreover, the intervertebral disc material can release chemicals and/or substances which may ultimately irritate the surrounding structures of the spine, contributing to nerve inflammation. When a nerve root becomes irritated, it can potentially lead to symptoms of pain and discomfort, numbness and weakness in one or both legs, otherwise referred to as sciatica, or sciatic nerve pain. An individual may also develop a herniated disc without ever experiencing any symptoms. A lumbar herniated disc is generally caused by the natural degeneration of the spine and discs, however, trauma and/or injury may also result in lumbar disc herniations. Symptoms of a lumbar herniated disc includes sciatica, tingling sensations, numbness, weakness, and loss of bladder or bowel control in severe cases. This last symptoms will require immediate medical attention.
Spondylolisthesis
Spondylolisthesis is another common cause of back pain and sciatica, particularly in young athletes. Repeated stress on the lower back, or lumbar spine, can create a crack or stress fracture in one of the vertebrae. In these cases, however, the stress fracture can often weaken the bone so much, to the point where it is unable to maintain its proper position in the spine, ultimately causing the vertebra to begin to shift or slip out of place. This condition is what is commonly known as spondylolisthesis. In children and adolescents, spondylolisthesis can occur through periods of rapid growth, by way of instance, during an adolescent growth spurt. This condition frequently occurs as a result of overuse, overstretching, or hyperextension, and even due to genetics.
Many healthcare professionals characterize spondylolisthesis as either low grade or high grade, depending on how much the vertebrae have shifted or slipped out of place. A high grade slip is generally identified when more than 50 percent of the width of the fractured vertebra slips forwards onto the vertebra beneath it. Individuals with high grade cases of spondylolisthesis will commonly describe experiencing significant levels of pain and discomfort as well as nerve injury. In the majority of instances, however, individuals with spondylolisthesis will not experience any obvious symptoms, as a matter of fact, most are unaware of the condition till an x-ray is taken for an unrelated injury and/or condition. Individuals with spondylolisthesis may experience back pain and sciatica, including muscle spasms, back stiffness and tight hamstrings.
Dr. Alex Jimenez’s Insight
Back pain is one of the most common reasons why individuals often miss days from work or go to the doctor, as it has also become one of the leading causes of disability worldwide. As a matter of fact, it has been statistically determined that approximately 80 percent of people will or have experienced back pain at least once throughout their life. Fortunately, a variety of treatments are available which can help ease the symptoms of back pain. It’s essential to understand back pain and sciatica, a collection of symptoms commonly associated with spine health issues along the lower back, in order to seek proper diagnosis and continue with an appropriate treatment plan in order to relieve your symptoms of back pain and sciatica.
Treatment for Back Pain and Sciatica
Chiropractic care is a well-known, alternative treatment option commonly utilized to help diagnose, treat and prevent back pain and sciatica. Since there are many factors which can contribute to symptoms of back pain and sciatic nerve pain, a doctor of chiropractic’s, or chiropractor’s, initial step would be to determine the root cause of the patient’s symptoms. Determining a diagnosis involves a thoughtful review of the patient’s health history, and a physical and neurological examination. Diagnostic testing may involve an x-ray, MRI, CT scan and/or electrodiagnostic tests, such as a nerve conduction speed evaluation or an electromyography. These examinations and tests help determine possible contraindications to treatment.
The aim of chiropractic care is to help promote the human body’s potential to heal itself. It is based on the scientific principle that limited spinal motion results in pain and reduced function and performance. Chiropractic care is non-invasive, or non-surgical, and drug-free. The type of chiropractic treatment provided is dependent upon the cause of the individual’s back pain and sciatica. A treatment program may include many distinct treatments and therapies, like ice/cold therapies, ultrasound, TENS, and spinal adjustments or manual manipulations. If the doctor of chiropractic decides that the patient’s spinal health issue requires treatment by a different kind of physician, then the individual may be referred to another healthcare professional.
Physical therapeutics for these conditions is also effective and generally has two components: active and passive. Passive physical therapeutics consist of ultrasound, electric stimulation, heat and ice packs as well as iontophoresis. Active physical therapeutics modalities include stretching exercises, back exercises and low-impact aerobic conditioning. Manual physical therapeutics, such as spinal adjustments and/or manual manipulations, might be integrated in part by a chiropractor. Physical therapists normally recommend 20 minutes of dynamic lumbar stabilization exercises every day. Core muscle strengthening is also important in treating back pain. Low-impact aerobics are also important and include water therapy, biking, and walking.
Physical therapeutics are an important element of treating spinal health issues. If you meet with a physical therapist, there will be a full assessment. Tests will be performed and an individualized treatment plan will be developed based on the patient’s goals. If you’re experiencing back pain or sciatica, don’t wait any longer for relief. Contact a healthcare professional to establish a one-on-one consultation and complete evaluation. Many chiropractors and physical therapists are certified, experienced and dedicated to helping you feel better. They have helped many others recover from spinal health issues and can help you too. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
It has been compared to the worst possible type of pain anyone can imagine. Other people say it’s even worse than labor because the pain doesn’t seem to have an end to it. These are some of the most common descriptions of sciatica, where a severe case of this excruciating nerve pain can bring anyone to their knees. That’s why lots of patients don’t simply say they have sciatica, they’re victims of its symptoms.
Sciatic nerve pain, or sciatica, is associated with many well-known symptoms, however, is sciatica really that common? What type of treatments are available to help alleviate sciatic nerve pain?And does a person’s everyday activities play a part in whether they will develop sciatica in the first place? Dwight Tyndall, MD, FAAOS answers several of the most commonly asked questions patients need to know regarding their sciatica.�Dr. Tyndall is a pioneer in the area of outpatient spine surgery, however, he is also a strong proponent of non-surgical treatment methods, including chiropractic care, to manage back pain and sciatica. Dr. Tyndall shares his perspectives on sciatic nerve pain and discusses what may indicate a need for surgery in severe cases of sciatica.
What is Sciatica?
According to Dr. Tyndall, sciatica is both a spinal disorder and a catch-all term for a group of symptoms. Sciatic nerve pain, best referred to as sciatica, is a spinal condition characterized by nerve pain which radiates down the length of the sciatic nerve. The sciatic nerve is the largest nerve in the entire human body, and it’s made up of spinal nerves from the vertebrae level L4 in the lumbar spine down to the vertebrae level S1 in the sacrum. Anything which impacts those nerves can lead to sciatica. Moreover, sciatica’s symptoms may be grouped under the medical term dysesthesia, meaning any sort of abnormal sensation. Most patients describe sciatica as an odd feeling radiating out of their lower back into their buttocks and down to their thigh and calf, often radiating as far down into the foot.
What are the Symptoms of Sciatica?
Dr. Tyndall explains that sciatica’s hallmark symptom include pain in the low back or buttocks which radiates down one or both legs. Signs and symptoms which shouldn’t be ignored include pain which doesn’t respond to non-surgical treatment options and/or pain which greatly restricts an individuals activity level and quality of life. Some red flags which may signal the need for surgical interventions associated with sciatic nerve pain include: reduced motor function in one part of the leg, usually a drop foot at which the patient can’t lift thei foot off the ground, weakness in one or both legs and bladder or bowel changes.
Is Sciatica the Same as Lumbar Radiculopathy?
“Most people see sciatica to be more severe than lumbar radiculopathy, but radiculopathy, which comes from the Latin radix significance origin, is a condition that affects the nerve during its origin as it exits the spinal cord. Sciatica and lumbar radiculopathy can be brought on by a pinched nerve from the spinal column due to a disc herniation or stenosis, but kidney problems or a sinus issue, like endometriosis, may also pose sciatica-like symptoms,” states Dr. Dwight Tyndall.
Who’s at Risk of Developing Sciatica?
“By my clinical experience, men and women have exactly the same identical risk of developing sciatica. Obesity also doesn’t play a role, either. Concerning age classes, however, sciatica has been estimated to peak during the ages of 30 and 40, and the risk usually declines as people begin reach their 50’s,” added Dr. Tyndall.
How Common is Sciatica?
As mentioned by Dr. Dwight Tyndall, sciatica and low back pain frequently occur together, but sciatica is much less common. While 80 percent of individuals experience low back pain at any point in their lives, just 2 to 3 percent will actually develop sciatica.
When Should a Person with Sciatica See a Healthcare Professional?
According to Dr. Tyndall, an individual with symptoms of sciatic nerve pain will need to see a healthcare professional if their pain is not reacting to over-the-counter (OTC) medications, or if these create weakness in the leg. Also, a person ought to see a doctor if their pain is so severe that their well-being is affected. Should the sciatica include bladder or bowel changes, the individual must seek immediate medical attention for their health issues. Furthermore, it’s important for a person with sciatica to seek the help of a healthcare professional to rule out any possible underlying causes which may be responsible for their symptoms.
What Type of Healthcare Professional Can Help Treat Sciatica?
According to Dr. Tyndall, any healthcare professional qualified and experienced in spine health issues, such as a chiropractor, can help diagnose, treat and even prevent sciatica. A doctor of chiropractic, or chiropractor, is a healthcare professional who utilizes spinal adjustments and manual manipulations, among other non-invasive treatment methods, to help correct any spinal misalignments, or subluxations, which may be causing sciatic nerve pain. A chiropractor may also recommend a series of stretches and exercises, as well as lifestyle modifications, to help speed up the patient’s recovery process. Chiropractic care is often the preferred alternative treatment option to help alleviate sciatica without the need for drugs and/or medications or surgery. However, if a patient is experiencing any of the red flag symptoms mentioned above, it may be necessary to visit a spine surgeon in order to discuss the treatment options. Always make sure to consider surgical interventions as a final alternative if your sciatica doesn’t respond to non-surgical treatment methods.
What are the Causes of Sciatica?
“There are many external factors, but among the greatest is your occupation. Someone who operates in a manual labor industry, like construction, has a higher likelihood of developing sciatica since they put more wear and tear on their back. Tiger Woods is an example of this. He acquired sciatica because his career as a golfer placed significant stress on his spine. There is a genetic element as well, as a few young men and women who do not operate in a strenuous job develop sciatica, however, the genetic tie is not clearly defined. Lastly, pregnancy may also result in sciatica. As the infant develops, it can put pressure on the lumbar spine, pelvis, and sciatic nerve. However, delivering the infant is usually enough to eliminate sciatica caused by pregnancy,” says Dr. Tyndall.
How Often is Sciatica Likely to Re-Occur?
“This question isn’t easy to answer because many factors contribute to whether a person will develop sciatica more than once. Sciatica is likely to re-occur if the spinal disc that led to sciatica the very first time is severely damaged. The more damaged the disk, the more likely it is to re-herniate and lead to sciatica again. Also, if the patient continues to work in a high-physical stress environment, the risk of re-ocurrence increases.
How is Sciatica Diagnosed?
“The physical examination is essential to a sciatica diagnosis. The straight-leg raise test is the traditional diagnostic tool during a physical examination. In this test, a patient be asked to lift up their leg when lying down. If that induces pain down their leg, the patient could have sciatica. Other physical tests healthcare professionals frequently utilize are knee extension tests, where the patient expands their knee to a straight position, like a straight-leg lift. Additionally, healthcare professionals will as patients to walk on their tip toes or on their heel to measure their potency. Other healthcare professionals will also observe how strong they are going down stairs or simply walking. Many doctors can determine a sciatica analysis from a physical examination, but if imaging studies are needed to learn more, the physician may recommend a magnetic resonance imaging (MRI) scan.
What Treatments are Effective for Sciatica?
As mentioned before by Dr. Dwight Tyndall, there is a variety of treatment options available to help alleviate the symptoms of sciatica. Approximately 80 percent of patients will improve with non-surgical treatment options. Several OTC medications, such as NSAIDs (eg, ibuprofen), are also effective in the management of sciatic nerve pain. If the sciatica does not subside, the doctor may prescribe a low-dose steroid pack (to be obtained over one week). If this doesn’t manage the sciatic nerve pain, then the patient may receive an epidural steroid injection (you will first need an MRI to pin-point the injection region).
Other non-surgical treatment options which are commonly utilized to help alleviate the symptoms of sciatica, include, acupuncture, chiropractic care and physical therapy, and needless to say, time normally works wonders such as pain. Chiropractic care is the most commonly used alternative treatment option for the treatment of sciatica. Chiropractic care focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Through spinal adjustments and manual manipulations, a doctor of chiropractic, or chiropractor, can help reduce unnecessary pressure in the structures surrounding the spine, improving strength, mobility and flexibility. Chiropractic care and physical therapy alike, can also help improve a patient’s overall health and wellness, aside from improving their sciatica, through physical activities and nutritional advice.
Is Surgery Ever Necessary to Treat Sciatica?
“It may certainly be so, however, the good thing is that the vast majority of people with sciatica don’t need surgery. And, your doctor may ask you to explore non-surgical treatment options, however, your tolerance for pain is the real predictor as to when you have to consider another option for treatment. Surgery may be necessary if symptoms worsen despite trying non-surgical alternatives, if you have weakness in your leg, or if you experience bladder and/or bowel changes,” explained Dr. Dwight Tyndall.
“The surgical procedure to treat sciatica is also called a lumbar microdiscectomy. It is a normal procedure with very positive individual outcomes when used accordingly. A lumbar microdiscectomy is similar to a traditional lumbar discectomy. Technological advances, like the advent of surgical microscopes, allow surgeons to create smaller incisions that are minimally traumatic to the body and result in a much quicker recovery for the patient”, added Dr. Tyndall.
Can Surgery be Performed in an Outpatient Setting?
“Yes, lumbar microdiscectomy can surely be carried out in an outpatient setting. Many patients like the cozy environment and are able to go home the exact same day of operation,” concluded�Dwight Tyndall, MD, FAAOS.
Is Sciatica Preventable?
As thoroughly explained by Dr. Dwight Tyndall, sciatica can be preventable if the individual doesn’t put significant and repeated stress in their back, which will reduce the chance of damaging or injuring a nerve. Nonetheless, in the present society, through our tasks and daily stresses of modern life, it’s difficult to accomplish that. Fortunately, with the abundance of treatment choices available, people can get relief from sciatic nerve pain with the appropriate healthcare professional’s help.
Dr. Alex Jimenez’s Insight
Many people will experience symptoms of low back pain at least once throughout their lifetime, however, only a few individuals will develop true sciatica symptoms. Sciatica is medically referred to as a collection of symptoms, rather than a single condition, and it’s generally characterized by pain and discomfort, followed by tingling or burning sensations and numbness along the length of the sciatic nerve. The sciatic nerve is the largest nerve in the human body and it travels from the lower back down the buttocks and thighs into the legs and feet. Sciatic nerve pain, or sciatica, has become a common health issue for many people, therefore, its important to be educated regarding this prevalent complaint in order to follow up with the most appropriate treatment.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine