How are MRIs used to help diagnose bulging and herniated discs and help healthcare providers develop effective treatment programs for individuals experiencing back pain symptoms?
Herniated Bulging Disc MRI
A herniated bulging disc is often identified during magnetic resonance imaging (MRI); however, it’s usually an incidental finding that was done for other reasons where spinal problems and/or injuries are found. A bulging disc is relatively common, even in individuals who experience no symptoms. A herniated or bulging disc in the back can be identified with an MRI test, typically recommended when someone experiences back pain symptoms for at least six weeks. (American Academy of Neurological Surgeons, 2024) Normal wear and tear and age cause changes in the spinal disc/s cushion to bulge and become misaligned with the spine. (Brinjikji W. et al., 2015) And with a herniated disc, it can press against the spinal cord and nerves. Repeated heavy lifting, practicing unhealthy postures, a history of back injuries, or underlying health conditions are common causes.
Bulging Disc
Bulging discs are common even in healthy individuals but can be difficult to interpret independently on an MRI, so other symptoms and findings are as important in diagnosis.
Causes
A bulging disc is usually considered age-related degenerative changes that cause the disc to bulge downward with gravity. (Penn Medicine, 2018)
A significant bulge is expected to cause leg pain due to irritation to the nerves going down the legs. (Amin R. M., Andrade N. S., & Neuman B. J. 2017) As the condition progresses, more than one disc can be affected, leading to other spinal conditions, including spinal stenosis.
A Bulging Disc On MRI
A disc bulge will measure over 25% of the total disc circumference. Its displacement is usually 3 millimeters or less from the normal shape and position of the disc. (Radiopaedia, 2024)
Herniated Disc
A herniated disc shifts out of its correct position and compresses nearby spinal nerves, causing pain and mobility issues.
Herniated discs will measure less than 25% of the total disc circumference. However, herniation is based on the type and can include: (Wei B., & Wu H. 2023)
Disc Protrusion – the displacement is limited, and the ligaments are intact.
Disc Extrusion – part of the disc remains connected but has slipped through the annulus or outer covering of the disc.
Disc Sequestration – a free fragment has separated and broken off from the main disc.
Candidates For Spinal MRI
The MRI is generally safe for most, including those with implanted cardiac devices like newer-model pacemakers. (Bhuva A. N. et al., 2020) However, it’s important to ensure that the healthcare team is aware of cochlear implants or other devices so that necessary precautions can be taken. It is recommended for all individuals that symptoms be present for six weeks before an MRI. A specialist may want to see MRI results sooner, especially if symptoms include: (American Academy of Neurological Surgeons, 2024)
A specific injury, like a fall that caused the pain
Recent or current infection or fever with spinal symptoms
Significant weakness in arms or legs
Loss of pelvic sensation.
A history of metastatic cancer.
Loss of bladder or bowel control
An MRI may be needed if symptoms are rapidly worsening. However, many with a disc bulge don’t have symptoms at all. In most cases, an MRI is an outpatient procedure that can be completed in an hour or less but can take longer if contrast dye is used. The healthcare provider will provide specific instructions about MRI preparation.
Treatment
Treatment for a herniated or bulging disc depends on the cause and severity of symptoms.
Over-the-counter pain relief, including nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical therapy
In rare cases that have not resolved with conservative treatment, surgery may be recommended.
Remember that the MRI findings may not identify or rule out all conditions, including muscle strains or ligament injuries, which may require different treatments, such as targeted stretches and exercises. (Brinjikji W. et al., 2015) (Fujii K. et al., 2019)
Herniated Disc
Treatment depends on the cause and severity of symptoms, if any. It can include stand-alone or a combination of physical therapy, medication, and steroid injections. Cases usually resolve in six to 12 weeks (Penn Medicine, 2018). Electrical nerve stimulation may be performed through specialized devices and/or acupuncture to help with nerve compression. (National Institute of Neurological Disorders and Stroke, 2020) Surgery may be recommended if conservative treatments fail to achieve significant pain relief and healing. (Wang S. et al., 2023)
Injury Medical Chiropractic and Functional Medicine Clinic
A healthcare provider can discuss treatment options such as pain medication, physical therapy, and surgery. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Root Causes of Spinal Stenosis
References
American Academy of Neurological Surgeons. (2024). Herniated disc. https://www.aans.org/patients/conditions-treatments/herniated-disc/
Brinjikji, W., Diehn, F. E., Jarvik, J. G., Carr, C. M., Kallmes, D. F., Murad, M. H., & Luetmer, P. H. (2015). MRI Findings of Disc Degeneration are More Prevalent in Adults with Low Back Pain than in Asymptomatic Controls: A Systematic Review and Meta-Analysis. AJNR. American journal of neuroradiology, 36(12), 2394–2399. https://doi.org/10.3174/ajnr.A4498
Penn Medicine. (2018). Bulging Disc vs. Herniated Disc: What’s The Difference? Penn Musculoskeletal and Rheumatology Blog. https://www.pennmedicine.org/updates/blogs/musculoskeletal-and-rheumatology/2018/november/bulging-disc-vs-herniated-disc
Wu, P. H., Kim, H. S., & Jang, I. T. (2020). Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. International journal of molecular sciences, 21(6), 2135. https://doi.org/10.3390/ijms21062135
Amin, R. M., Andrade, N. S., & Neuman, B. J. (2017). Lumbar Disc Herniation. Current reviews in musculoskeletal medicine, 10(4), 507–516. https://doi.org/10.1007/s12178-017-9441-4
American Academy of Orthopaedic Surgeons. (2022). Herniated disk in the lower back. https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
Wei, B., & Wu, H. (2023). Study of the Distribution of Lumbar Modic Changes in Patients with Low Back Pain and Correlation with Lumbar Degeneration Diseases. Journal of pain research, 16, 3725–3733. https://doi.org/10.2147/JPR.S430792
Bhuva, A. N., Moralee, R., Moon, J. C., & Manisty, C. H. (2020). Making MRI available for patients with cardiac implantable electronic devices: growing need and barriers to change. European radiology, 30(3), 1378–1384. https://doi.org/10.1007/s00330-019-06449-5
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A., Halabi, S., Turner, J. A., Avins, A. L., James, K., Wald, J. T., Kallmes, D. F., & Jarvik, J. G. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American journal of neuroradiology, 36(4), 811–816. https://doi.org/10.3174/ajnr.A4173
Fujii, K., Yamazaki, M., Kang, J. D., Risbud, M. V., Cho, S. K., Qureshi, S. A., Hecht, A. C., & Iatridis, J. C. (2019). Discogenic Back Pain: Literature Review of Definition, Diagnosis, and Treatment. JBMR plus, 3(5), e10180. https://doi.org/10.1002/jbm4.10180
Wang, S., Zhao, T., Han, D., Zhou, X., Wang, Y., Zhao, F., Shi, J., & Shi, G. (2023). Classification of cervical disc herniation myelopathy or radiculopathy: a magnetic resonance imaging-based analysis. Quantitative imaging in medicine and surgery, 13(8), 4984–4994. https://doi.org/10.21037/qims-22-1387
National Institute of Neurological Disorders and Stroke. (2020). Low back pain fact sheet. Retrieved from https://www.ninds.nih.gov/sites/default/files/migrate-documents/low_back_pain_20-ns-5161_march_2020_508c.pdf
An axillary nerve injury can cause pain, weakness, and shoulder mobility loss. Can physical therapy help restore and maintain shoulder joint flexibility?
Axillary Nerve
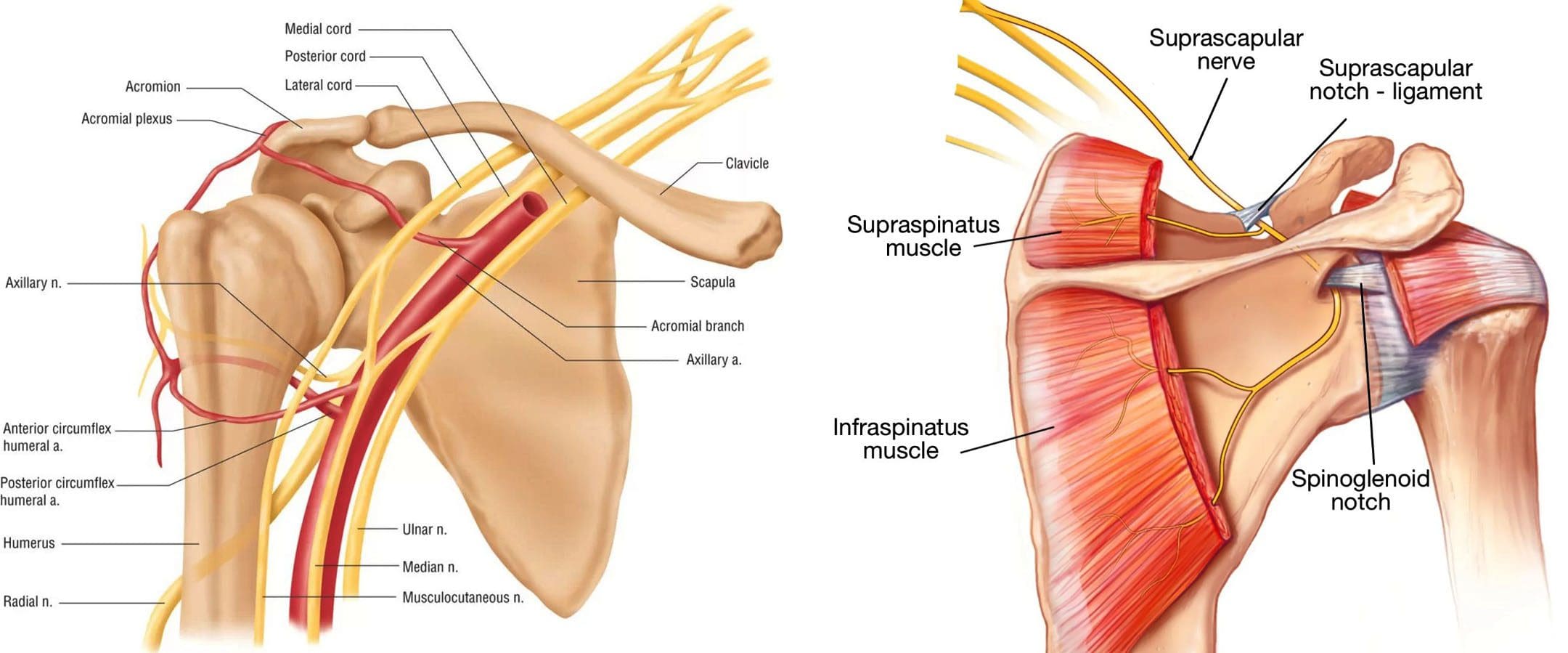
The axillary nerve, or the circumflex nerve, is a peripheral nerve that runs through the shoulder and supports movement and sensation in the upper limbs. It originates in the neck at the brachial plexus, a network of nerves that extends from the neck and upper torso to the shoulders and arms. Its primary purpose is to supply nerve function to the shoulder joint and three muscles in the arm and also innervates some skin in the region.
Anatomy
Except for the cranial nerves, all the body’s nerves branch off from the spinal cord, emerge from between vertebrae and continue to branch off as they travel to various muscles and other structures. The axillary nerve is named after the axilla, the medical name for the armpit. Individuals have two, one on each side. After leaving the spinal column, the axillary nerve runs behind the axillary artery and continues to the shoulder blade’s lower edge of the subscapularis muscle. It winds back and travels down the arm along the posterior humeral circumflex artery, which then passes through the quadrangular space (a small area of the shoulder blade just above the armpit where there is a gap in the muscles that allows nerves and blood vessels to pass through to the arm before it divides into terminal branches, which are:
Anterior Division
Supplies motor innervation to the deltoid’s anterior and middle heads, allowing the arm to abduct or move away from the body.
It winds around the neck of the humerus/funny bone, goes beneath the deltoid muscle, and then connects to the forward edge of the deltoid.
A few small cutaneous branches serve the skin in that area.
Posterior Division
Innervates the teres minor muscles and the lower part of the deltoid.
It enters the deep fascia and becomes the superior lateral cutaneous nerve.
It then wraps around the lower edge of the deltoid, connects to the skin over the lower two-thirds of the muscle, and covers the long head of the triceps brachii.
Articular Branch
Comes from the trunk of the axillary nerve and enters the glenohumeral joint, which is in the shoulder, below the subscapularis muscle.
Anatomical Variations
In a case report, healthcare providers noted an incidence of the nerve branching directly off the upper trunk of the brachial plexus rather than the posterior cord. (Subasinghe S. K. and Goonewardene S. 2016) In this case, it innervated the subscapularis muscle, latissimus dorsi, and the deltoid and teres minor muscles and also had a communicating branch to the posterior cord. Another case documented multiple abnormalities in the course of the axillary nerve in an individual with pain and severely limited shoulder mobility. (Pizzo R. A. et al., 2019) During reverse shoulder arthroplasty, the surgeon discovered that the axillary nerve ran beside the coracoid process instead of underneath and stayed close to the subscapularis muscle instead of traveling through the quadrangular space. The case noted earlier reports of axillary nerves not running through the quadrangular space. In those cases, the nerve pierced the subscapularis muscle or split into branches before reaching the quadrangular space.
Function
The axillary nerve functions as a motor nerve that controls movement and a sensory nerve that controls sensations like touch or temperature.
Motor
As a motor nerve, the axillary nerve innervates three muscles in the arm and includes:
Deltoid
Allows flexing of the shoulder joint and rotating the shoulder inward.
Long Head of the Triceps
It runs down the back of the outer arm, allowing straightening, pulling the upper arm toward the body, or extending it backward.
The radial nerve can also innervate this muscle.
Teres Minor
One of the rotator cuff muscles starts outside the shoulder and runs diagonally along the bottom edge of the shoulder blade.
It works with other muscles to allow for the external rotation of the shoulder joint.
Sensory
In its sensory role, the nerve carries information to the brain from the following:
Glenohumeral joint or the ball-and-socket joint in the shoulder.
The skin on the lower two-thirds of the deltoid muscle through the superior lateral cutaneous branch.
Injuries and Conditions
Problems with the axillary nerve can be caused by injuries anywhere along the arm and shoulder and by disease. Common injuries include:
Dislocations
Of the shoulder joint, which can cause axillary nerve palsy.
Fracture
Of the surgical neck of the humerus.
Compression
This stems from walking with crutches, also known as crutch palsy.
Direct Trauma
This can be from an impact sports, work, automobile accident, collision, or laceration.
Added Pressure
This can be from wearing a cast or splint.
Surgical Accidental Injury
An injury or damage can come from shoulder surgery, especially arthroscopic surgery on the inferior glenoid and capsule.
Quadrangular Space Syndrome
This is where the axillary nerve is compressed where it passes through that space, which is most common in athletes who perform frequent overhead motions)
Nerve Root Damage
Between the fifth and sixth cervical vertebrae, where the nerve emerges from the spinal cord, which can be caused by traction, compression, spinal disc prolapse, or a bulging disc.
Systemic Neurological Disorders
Example – multiple sclerosis
Erb’s Palsy
A condition often is the result of a birth injury called shoulder dystocia, in which a baby’s shoulder/s becomes stuck during childbirth.
Axillary Nerve Palsy
Damage can result in a type of peripheral neuropathy that can cause weakness in the deltoid and teres minor muscles.
This can result in losing the ability to lift the arm away from the body and weakness in various shoulder movements.
If the damage is severe enough, it can cause paralysis of the deltoid and other minor muscles, resulting in flat shoulder deformity, in which individuals cannot lay their shoulders flat when lying down.
Axillary nerve damage also can lead to a change, reduction, or loss of sensation in a small part of the arm just below the shoulder.
Nerve Injury Statistics
Three times more common in men than women.
It may be present in as many as 65% of shoulder injuries.
The risk of injury due to dislocation is significantly increased after age 50.
Tests
If a healthcare provider suspects a problem with axillary nerve function, they’ll test the shoulder’s range of motion and skin sensitivity. A difference in the range of motion between the shoulders can indicate a nerve injury. Individuals may be sent for electromyography and a nerve conduction study to verify nerve palsy. In some cases, an MRI and/or X-rays may be ordered, especially if the cause of possible nerve damage is unknown.
Rehabilitation
Depending on the severity and cause of the injury, non-surgical treatments may be recommended, with surgery as a last resort. Non-surgical treatment can include some combination of immobilization, rest, ice, physical therapy, and anti-inflammatory meds. Physical treatment typically lasts about six weeks and focuses on strengthening and stimulating the muscles to prevent joint stiffness, which can impair long-term function.
Surgery
If conservative treatments don’t work, surgery may be recommended, especially if several months have passed without improvement. Surgical outcomes are generally better if surgery is performed within six months of the injury, and regardless of the time frame, the prognosis is considered positive in about 90% of cases. Surgical procedures performed for axillary nerve dysfunction or injury include:
Neurolysis
This procedure involves targeted damage/degeneration of nerve fibers, interrupts the nerve signals, and eliminates pain while the damaged area heals.
Neurorrhaphy
This procedure stitches a severed nerve back together.
Nerve Grafting
Grafting involves transplanting a portion of another nerve, usually the sural nerve, to reconnect severed nerves.
This helps, especially when the damaged portion is too large to be repaired by neurorrhaphy.
It allows a pathway for signals and encourages the regrowth of nerve axons.
Neurotization or Nerve Transfer
Similar to grafting but used when the nerve is too damaged to heal.
This procedure involves transplanting a healthy but less important nerve, or a portion of a nerve, to replace the damaged one and restore function.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Shoulder Pain Chiropractic Treatment
References
Subasinghe, S. K., & Goonewardene, S. (2016). A Rare Variation of the Axillary Nerve Formed as Direct Branch of the Upper Trunk. Journal of clinical and diagnostic research : JCDR, 10(8), ND01–ND2. https://doi.org/10.7860/JCDR/2016/20048.8255
Pizzo, R. A., Lynch, J., Adams, D. M., Yoon, R. S., & Liporace, F. A. (2019). Unusual anatomic variant of the axillary nerve challenging the deltopectoral approach to the shoulder: a case report. Patient safety in surgery, 13, 9. https://doi.org/10.1186/s13037-019-0189-1
What type of concussion tests are there to help establish the extent of head injuries and help assess improvement during recovery?
Concussion Tests
A concussion is a temporary change in brain function that occurs from a traumatic brain injury or TBI. It can cause problems with thinking and mood and can take weeks to years to heal. Concussion tests are done after a suspected head injury and are also used after diagnosis to assess healing progress. They are noninvasive tests that measure brain functions. Several tests vary in how they are given and what they measure.
Tests
A mild or moderate traumatic brain injury can cause damage to the brain that is not detectable with brain imaging tests. However, the damage can cause serious symptoms, including headaches, emotional changes, difficulty concentrating, and memory problems. (Haider M. N. et al., 2021) The effects of a concussion can be hard to describe, but concussion testing can help identify and quantify these changes. For individuals who don’t have time to heal or experience further brain injuries while recovering, the effects can be prolonged and worsen. This is one reason why concussion testing is vital to get a diagnosis and follow medical recommendations to avoid further injury to the brain. Diagnosis can help set goals, adjust, and assess how the effects improve over time. With improvement, individuals can participate in rehabilitation and follow their doctor’s instructions for gradually returning to work, school, and other activities.
Measurements
Concussion tests can measure subtle aspects of brain function, like visual or auditory perception and response speed (Joyce A. S. et al., 2015). The damage sustained can impair these abilities, like slow decision-making. A traumatic brain injury can be associated with serious injuries, like a skull fracture, swelling, bruise, or bleeding in the brain. These injuries can be detected with imaging tests and often require surgery or other interventions. Brain damage from bleeding or swelling would cause focal neurological symptoms and signs, including partial vision loss, numbness, and weakness. Individuals can have a concussion along with detectable brain injuries or in the absence of detectable brain injuries.
Types of Tests
There are several types of concussion tests. Individuals may have one or more of these, depending on the standard test that is used in their school, sports league, or by their doctor. These can include:
Online Checklists
Several different online checklists are available for concussion screening.
These tests may include questions about symptoms and are often used as self-tests but are not intended to replace an evaluation by a medical professional.
Baseline and Post-Injury Tests
Many schools and sports leagues conduct preseason skill measurements, including memory tests or tests of speed and accuracy, either in an interview form or with computer testing.
Individuals might be asked to retake the test that is used as a comparison if they have experienced a traumatic brain injury.
Standardized Assessment of Concussion – SAC
This five-minute test can be done on the sidelines after a sports injury or later.
It evaluates orientation, immediate memory, neurologic function, concentration, and delayed recall. (Kaufman M. W. et al., 2021)
King-Devick Concussion Test
This two-minute test can be performed on the sidelines after a sports injury or later to assess language, eye movement, and attention. (Krause D. A. et al., 2022)
Post-Concussion Symptom Scale
This test includes 22 questions involving neurocognitive factors, including difficulty concentrating or remembering, physical symptoms like headaches and dizziness, and emotional symptoms like sadness or irritability. (Langevin P. et al., 2022)
Sport Concussion Assessment Tool – SCAT
This test includes an on-field assessment noting concussion symptoms, memory assessment using Maddocks questions (a short list of specific questions), Glasgow Coma Scale (GCS), and cervical spine assessment.
An off-field assessment involves the evaluation of cognitive, neurological, balance, and delayed recall. (Kaufman M. W. et al., 2021)
Buffalo Concussion Physical Examination – BCPE
A modified physical examination that assesses neck tenderness and range of motion, head, jaw, and face abnormalities, eye movements examination, and coordination. (Haider M. N. et al., 2021)
After a concussion, individuals will also have a physical examination, including a full neurological examination, in a doctor’s office.
Results
A doctor will diagnose based on symptoms, physical examination, and concussion test results. For example, for individuals who have broken several bones and are taking powerful pain medications, concussion test results can be abnormal even if they did not experience a concussion. The results of concussion testing can be compared with results before the head injury. Often, baseline testing is required for participation in certain sports leagues at professional and amateur levels. A low score can indicate that head injury has impaired brain function. Sometimes, testing can be done within a few hours of the head trauma and then again a few days later. Responses of individuals who did not have measurements taken before a head injury can be compared with the average results of people their age.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Lumbar Spine Injuries in Sports: Chiropractic Healing
References
Haider, M. N., Cunningham, A., Darling, S., Suffoletto, H. N., Freitas, M. S., Jain, R. K., Willer, B., & Leddy, J. J. (2021). Derivation of the Buffalo Concussion Physical Examination risk of delayed recovery (RDR) score to identify children at risk for persistent postconcussive symptoms. British journal of sports medicine, 55(24), 1427–1433. https://doi.org/10.1136/bjsports-2020-103690
Joyce, A. S., Labella, C. R., Carl, R. L., Lai, J. S., & Zelko, F. A. (2015). The Postconcussion Symptom Scale: utility of a three-factor structure. Medicine and science in sports and exercise, 47(6), 1119–1123. https://doi.org/10.1249/MSS.0000000000000534
Kaufman, M. W., Su, C. A., Trivedi, N. N., Lee, M. K., Nelson, G. B., Cupp, S. A., & Voos, J. E. (2021). The Current Status of Concussion Assessment Scales: A Critical Analysis Review. JBJS reviews, 9(6), e20.00108. https://doi.org/10.2106/JBJS.RVW.20.00108
Krause, D. A., Hollman, J. H., Breuer, L. T., & Stuart, M. J. (2022). Validity Indices of the King-Devick Concussion Test in Hockey Players. Clinical journal of sport medicine: official journal of the Canadian Academy of Sport Medicine, 32(3), e313–e315. https://doi.org/10.1097/JSM.0000000000000938
Langevin, P., Frémont, P., Fait, P., & Roy, J. S. (2022). Responsiveness of the Post-Concussion Symptom Scale to Monitor Clinical Recovery After Concussion or Mild Traumatic Brain Injury. Orthopaedic journal of sports medicine, 10(10), 23259671221127049. https://doi.org/10.1177/23259671221127049
Elbow pain from lifting is a common symptom among individuals who lift weights, heavy objects, children, grocery bags, etc. Depending on the underlying cause, can conservative treatments relieve and heal elbow pain?
Elbow Pain Caused By Lifting
Elbow pain from lifting can result from weight training, repetitive daily tasks, or job duties like lifting small children or heavy objects. Pain can manifest at the sides or the front of the elbow. Most minor injury cases can be treated with ice, rest, and medications at home. However, pain after lifting can also be a sign of a serious injury, such as a tendon rupture/tear.
Minor Pain From Lifting
Lifting puts pressure on the tendons connecting the wrist and upper arm to the bones in the elbow joint. Minor elbow pain can occur from temporary inflammation in any of these structures after lifting an object. Tendonitis occurs when a tendon becomes inflamed, often from overuse or lifting something too heavy, and ranges from mild to severe. Mild tendonitis typically causes pain during the activity and improves with rest. (American Academy of Orthopaedic Surgeons, 2020) Common forms of tendonitis include:
Tennis elbow – tendonitis on the outside of the elbow
Golfer’s elbow – tendonitis on the inside of the elbow.
Add ice to the affected area for up to 20 minutes daily to decrease elbow pain.
Rest
Avoid lifting heavy objects as much as possible when pain is present.
Wearing A Brace
If the pain is at the tendons on the inside or outside of your elbow, try wearing a wrist brace to limit the use of your wrist muscles that connect to this area.
Stretching
Gently stretching the wrist flexors and extensors can help reduce elbow pain after lifting. Stretches can be performed several times daily, even after symptoms have resolved. (American Academy of Orthopaedic Surgeons, 2024)
Hold the arm out in front with the palm down. Keep the elbow straight.
Bend the wrist down so that the fingers are pointing toward the ground.
With the other hand, gently pull the wrist further down until a stretch is felt along the back of the forearm.
Hold this position for 15 seconds.
Repeat five times.
Next, bend the wrist upward so the fingers point toward the ceiling.
Using the other hand, gently pull the hand backward until the stretch is felt along the front of the forearm.
Mild cases can improve after a few days of self-care, whereas more pronounced elbow symptoms can take several weeks, months, or even a year. (Kheiran A. Pandey, A. & Pandey R. 2021) If self-care doesn’t work, physical therapy may be recommended. A physical therapy team can use various modalities and treatments to help reduce pain and inflammation from elbow injuries. The therapy can include targeted exercises to strengthen weak muscles and stretch tight muscles that might contribute to the condition. In addition, the therapy team will help individuals modify their lifting technique to help prevent further injury.
A biceps tendon rupture is a rare but serious injury usually caused from lifting. In addition to other visible signs of the injury, there will be a bulge at the top of the upper arm because the muscle bunches up as it is no longer attached to the elbow. (American Academy of Orthopaedic Surgeons, 2022) Individuals may hear an audible popping sound if an elbow ligament or tendon gets torn while lifting. (Johns Hopkins Medicine, 2024)
Treatment
Treatment depends on the severity of the injury, but most cases resolve on their own with rest and, if necessary, physical therapy. Conditions that cause severe pain require orthopedic surgeon expertise. These physicians specialize in treating musculoskeletal system injuries. Imaging such as X-rays, MRIs, or CT scans are often used to determine the extent of damage. Individuals with tendon or ligament tears in the elbow may need surgery to regain full range of motion and strength in their arm. After surgery, physical therapy will help restore function.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other associated medical professionals to integrate a treatment plan to improve the body’s flexibility and mobility and resolve musculoskeletal issues.
Shoulder Pain Chiropractic Treatment
References
American Academy of Orthopaedic Surgeons. (2020). Sprains, strains, and other soft-tissue injuries. https://orthoinfo.aaos.org/en/diseases–conditions/sprains-strains-and-other-soft-tissue-injuries/
Kheiran, A., Pandey, A., & Pandey, R. (2021). Common tendinopathies around the elbow; what does current evidence say?. Journal of clinical orthopaedics and trauma, 19, 216–223. https://doi.org/10.1016/j.jcot.2021.05.021
American Academy of Orthopaedic Surgeons. (2024). Therapeutic exercise program for epicondylitis (tennis elbow/golfer’s elbow). https://orthoinfo.aaos.org/globalassets/pdfs/2024-therapeutic-exercise-program-for-lateral-and-medial-epicondylitis.pdf
American Academy of Orthopaedic Surgeons. (2023). What are NSAIDs? https://orthoinfo.aaos.org/en/treatment/what-are-nsaids/
American Academy of Orthopaedic Surgeons. (2022). Biceps tendon tear at the elbow. https://orthoinfo.aaos.org/en/diseases–conditions/biceps-tendon-tear-at-the-elbow
For athletes and individuals who want to engage in physical and sports activities, can focusing on health-related fitness components improve overall fitness and conditioning so that they can participate in various sports and other forms of exercise?
Fitness Components For Improved Physical and Sports Performance
Improving cardiovascular fitness, muscular strength and endurance, and flexibility will enhance athletes’ abilities and the daily lives of individuals who exercise and play sports. When enhancing performance in a specific activity, skill-related fitness training that focuses on that activity will be most beneficial. For instance, cardiovascular endurance and flexibility are necessary to play sports that require a lot of running, jumping, and changing positions quickly and to be able to play for the entire time, along with various skills that need to be practiced for agility, power, speed, and hand-eye coordination. Activity-related skills can differentiate two areas of fitness.
Getting In Shape and Improving Performance
Health-related fitness components are important for everyone in all walks of life, regardless of competition in or performing physical activities at an optimum level. These are:
Cardiovascular endurance
Flexibility
Muscle endurance
Muscle strength
Body composition
When improving cardiovascular endurance, the risk of heart disease is reduced. When improving flexibility, a healthy range of motion is maintained, enhancing the ability to perform activities of daily living, like household chores and tasks. These fitness components are crucial for physical health and contribute to positive lifestyle outcomes. (Garber C. E. et al., and American College of Sports Medicine 2011) The American College of Sports Medicine recommends:
Moderate-intensity Cardio
30 minutes a day, five days a week for a total of 150 minutes/week or
Vigorous-intensity Cardio
For 20 minutes a day, three days a week, or
A Combination
Moderate- and vigorous-intensity exercise, plus
Resistance Training
Two to three days a week, along with
Flexibility Training
Two days a week
Skill Related Components
Skill-related fitness components are:
Agility
Balance
Coordination – hand-eye and/or foot-eye
Power
Reaction time
Speed
The skill-related fitness components can help those who want more training for a specific fitness-related goal.(Zemková E. and Hamar D. 2018) For example, while everyone can benefit from daily walks, weightlifters can focus most of their effort on power, balance, and strength.
Power
Power combines speed and strength, which is how fast maximal force can be generated. Athletes exert maximum strength in short, all-out efforts. Jumping requires leg power, while jumping and striking involve a combination of upper- and lower-body power. Power can be improved by combining resistance and speed with fast-paced strength-training exercises that include:
Kettlebell swings
Clean lifts
Jerk lifts
Plyometric box jumps
Pushing a weighted sled
Sprinting
Speed
Athletes train differently but with a similar goal: to become faster in their sport. Speed training will differ based on the sport being trained for. High-intensity interval training, or HIIT, is one of the best ways to improve speed. Training involves working at an all-out or near all-out effort for set periods, followed by set rest periods. (Alansare A. et al., 2018) It repeatedly challenges the aerobic and anaerobic systems, teaching the muscles, heart, and lungs to grow accustomed to working at higher intensity levels. Depending on the sport, the length and intensity of the intervals will be longer or shorter, less challenging, or more difficult. Runners can try these example HIIT speed drills:
Marathon Training
Mile repeats – a style of interval training where the runner goes all-out for a full mile before resting and doing it again.
Sprint Training
Focuses on shorter, more intense intervals.
Ranging from 40 to 400 meters, running all out and resting before repeating.
These same concepts apply to other sports as well.
Agility
Agility is the ability to move and change direction quickly and easily. For example, soccer, basketball, football, and tennis players are incredibly agile and have to move in every direction, jumping, sliding, twisting, and backpedaling in quick response to the ball’s movement and other players. Their bodies must be trained to respond and change course. Agility drills commonly involve exercises that develop foot speed and direction change, that include:
Ladder Drills
Using an agility ladder can help develop quick and specific foot placement.
Cone Drills
Set up cones in a T shape, then sprint, slide, backpedal, or change direction depending on the cone.
Coordination
Sports and physical activities require well-honed hand-eye and foot coordination. They require seeing an external object and responding precisely with the hands and/or feet. Think of hitting a ball, running and catching a ball, throwing a frisbee, or blocking a shot. To improve coordination, try skill-related fitness exercises like:
Playing catch
Jumping rope
Dribbling a ball
Throwing or hitting balls or specific sports objects at targets
Balance
Balance refers to the ability to adjust the body position to remain upright. It involves proprioception, or knowing where the body is in space and being able to adjust position as the center of gravity changes during movement. (Aman J. E. et al., 2015) Sports and daily physical activities require balance for performance and safety. Jumping on a trampoline or rebounder, for example, can help individuals better sense where their bodies are as they move. To improve balance, try these exercises:
Practice standing on one foot.
Practice standing yoga poses.
BOSU balance ball workouts.
Use balance discs to perform squats, lunges, and push-ups.
Reaction Time
Reaction time refers to how quickly one responds to an external stimulus and focuses on the mind-body connection. The eyes see a stimulus, the mind interprets the stimulus, and the body reacts to that interpretation. This mind-body reaction relates to knowledge of the sport or activity and enables individuals to respond more quickly and accurately to the stimulus. Reaction-time training tends to be sport-specific, but skill-related fitness activities can help and include:
Using tools like reaction balls
Fielding a ball
Protecting a goal as other players try to score
Playing table tennis
Playing hacky sack
Injury Medical Chiropractic and Functional Medicine Clinic
Ask a qualified fitness coach or personal trainer if you are unsure where to begin. Other athletes, local teams, gyms, athletic clubs, and healthcare organizations can direct individuals in the right direction. At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you to relieve pain, restore function, and prevent injury. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Improving Athletic Performance Through Chiropractic
References
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., Lee, I. M., Nieman, D. C., Swain, D. P., & American College of Sports Medicine (2011). American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Medicine and science in sports and exercise, 43(7), 1334–1359. https://doi.org/10.1249/MSS.0b013e318213fefb
Zemková, E., & Hamar, D. (2018). Sport-Specific Assessment of the Effectiveness of Neuromuscular Training in Young Athletes. Frontiers in physiology, 9, 264. https://doi.org/10.3389/fphys.2018.00264
Alansare, A., Alford, K., Lee, S., Church, T., & Jung, H. C. (2018). The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. International journal of environmental research and public health, 15(7), 1508. https://doi.org/10.3390/ijerph15071508
Aman, J. E., Elangovan, N., Yeh, I. L., & Konczak, J. (2015). The effectiveness of proprioceptive training for improving motor function: a systematic review. Frontiers in human neuroscience, 8, 1075. https://doi.org/10.3389/fnhum.2014.01075
For individuals dealing with finger injuries, which can occur from various causes, including overuse, jobs, sports, and more, can knowing the cause of finger pain help healthcare providers determine what steps to take for treatment?
Finger Injuries
Finger injuries are common and can range from minor to serious. (van Veenendaal L. M. et al., 2014) Symptoms can result from an acute injury, including broken fingers and sprains, or chronic conditions like arthritis.
Fractures
Finger fractures can vary and can be serious and lead to permanent damage, deformity, and loss of function if not treated properly. What is important is that fractures are appropriately diagnosed so the proper treatment plan can be initiated. Most finger fractures can be addressed with simple treatments, while others may require surgery. (Oetgen M. E., and Dodds S. D. 2008)
Sprain and Dislocation
Sprains and dislocations are common finger injuries. (Prucz R. B. and Friedrich J. B. 2015) Both damage the ligaments that support the finger joints. In more severe injuries, a dislocation can occur, necessitating the finger to be put back into place or reduced. Individuals with a sprain or dislocation often notice finger swelling or stiffness for months after the injury.
Ligament Damage
Some call this injury skier’s or gamekeeper’s thumb, which results from a specific type of thumb dislocation. Here, the ulnar collateral ligament of the thumb is damaged. This ligament helps keep the thumb stable and supports grip and hand strength. However, this type of ligament injury often requires surgery. (Christensen T. et al., 2016)
Arthritis
Arthritis causes damage to normal joint surfaces where two bones come together. Fingers are one of the most common locations where arthritis occurs. (Spies C. K. et al., 2018) Two types of arthritis commonly affect the fingers: osteoarthritis and rheumatoid arthritis.
Arthritis of The Thumb
Arthritis of the thumb usually occurs at the joint where the thumb meets the wrist. This joint called the carpometacarpal/CMC joint, helps with gripping and pinching. Thumb arthritis is more common in women than men and increases in frequency over 40. (Deveza L. A. et al., 2017)
Trigger Finger
Trigger finger or stenosing tenosynovitis, is a common injury that causes pain and snapping of the fingers’ tendons, resulting in a sensation of locking or catching when bending and straightening the digits. (Makkouk A. H. et al., 2008) Other symptoms include pain and stiffness in the fingers and thumb. Treatments can vary from observation, rest, splinting, injections, and surgery.
Tendon Injuries
Mallet finger
A mallet finger is an injury to the tip of the finger. Usually, it occurs when the end of a straightened finger or thumb is hit, jamming the finger. After the injury, the individual may notice that they cannot fully straighten the tip of the finger. Treatment almost always uses a splint that has to stay on for about six weeks without removal. (Alla, S. R., Deal, N. D., and Dempsey, I. J. 2014) Very rarely is a surgical procedure necessary.
Jersey Finger
This is an injury to the finger flexor tendon. The flexor tendon pulls the finger into the palm when contracting the forearm flexor muscles. The injury occurs at the tip of the finger; typically, the tendon snaps back to the finger’s base or into the palm.
Ring Injuries
Injuries to the finger while wearing wedding bands or other finger jewelry can lead to serious complications. Even minor injuries can have devastating complications if the severity of the injury is not recognized and addressed. If an injury occurs while wearing the jewelry and there is soft tissue damage, including blood circulation being cut off, immediate medical attention is necessary.
Other Injuries
Bruises
The most common finger injury is caused by direct trauma to the skin and muscles. Symptoms include pain, swelling, tenderness, and discoloration of the skin.
Cuts and Scrapes
These can range from minor to more serious, such as injuries that cut through blood vessels, nerves, and tendons.
Injury Medical Chiropractic and Functional Medicine Clinic
After the initial inflammation and swelling have subsided, a doctor will recommend a treatment plan that usually involves physical therapy, self-performed physical rehabilitation, or supervision by a physical therapist or team. At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for you to relieve pain and restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Sports Injury Rehabilitation
References
van Veenendaal, L. M., de Klerk, G., & van der Velde, D. (2014). A painful finger as first sign of a malignancy. Geriatric orthopaedic surgery & rehabilitation, 5(1), 18–20. https://doi.org/10.1177/2151458514522125
Oetgen, M. E., & Dodds, S. D. (2008). Non-operative treatment of common finger injuries. Current reviews in musculoskeletal medicine, 1(2), 97–102. https://doi.org/10.1007/s12178-007-9014-z
Prucz, R. B., & Friedrich, J. B. (2015). Finger joint injuries. Clinics in sports medicine, 34(1), 99–116. https://doi.org/10.1016/j.csm.2014.09.002
Christensen, T., Sarfani, S., Shin, A. Y., & Kakar, S. (2016). Long-Term Outcomes of Primary Repair of Chronic Thumb Ulnar Collateral Ligament Injuries. Hand (New York, N.Y.), 11(3), 303–309. https://doi.org/10.1177/1558944716628482
Spies, C. K., Langer, M., Hahn, P., Müller, L. P., & Unglaub, F. (2018). The Treatment of Primary Arthritis of the Finger and Thumb Joint. Deutsches Arzteblatt international, 115(16), 269–275. https://doi.org/10.3238/arztebl.2018.0269
Deveza, L. A., Hunter, D. J., Wajon, A., Bennell, K. L., Vicenzino, B., Hodges, P., Eyles, J. P., Jongs, R., Riordan, E. A., Duong, V., Min Oo, W., O’Connell, R., & Meneses, S. R. (2017). Efficacy of combined conservative therapies on clinical outcomes in patients with thumb base osteoarthritis: protocol for a randomised, controlled trial (COMBO). BMJ open, 7(1), e014498. https://doi.org/10.1136/bmjopen-2016-014498
Makkouk, A. H., Oetgen, M. E., Swigart, C. R., & Dodds, S. D. (2008). Trigger finger: etiology, evaluation, and treatment. Current reviews in musculoskeletal medicine, 1(2), 92–96. https://doi.org/10.1007/s12178-007-9012-1
Alla, S. R., Deal, N. D., & Dempsey, I. J. (2014). Current concepts: mallet finger. Hand (New York, N.Y.), 9(2), 138–144. https://doi.org/10.1007/s11552-014-9609-y
Marshmallows and calories can add up when eating more than a single serving. Can marshmallows be consumed in moderation and still be healthy?
Marshmallows
Many enjoy marshmallows with hot chocolate, sweet potatoes, and s’mores. However, their nutritional value is not the healthiest, as the ingredients typically include water, sugar, corn syrup, gelatin, and sometimes other ingredients for flavor and color. The key ingredient is whipped air, giving marshmallows their signature texture.
Nutrition
A serving weighs about 28 grams, around four large marshmallows or a half-cup of mini marshmallows. If consumed in their original form, they contain about 80 calories. (United States Department of Agriculture, 2018)
Carbohydrates
Marshmallows are made of different types of sugar (sucrose and corn syrup), and most of their calories come from carbohydrates. One marshmallow contains a little under 6 grams of carbohydrates, and a single serving provides about 23 grams of carbohydrates, primarily sugar. The glycemic index is estimated to be 62, making it a high-glycemic food. The estimated glycemic load of one marshmallow is 15, which is low. However, the glycemic load takes serving size into account. Because the serving size is small, the glycemic load is lower than expected.
Fats
Very little fat, less than 1 gram, is in a single serving.
Protein
Marshmallows are not a recommended source of protein.
There is less than 1 gram of protein in a single serving.
Micronutrients
There is no significant vitamin or mineral intake by consuming marshmallows.
A single serving does contain a small amount of phosphorus, around 2.2 milligrams, and potassium, around 1.4 milligrams.
It also increases sodium intake by 22.4 mg, providing little selenium 0.5 micrograms.
Health Benefits
Marshmallows are processed and provide little to no health benefits, but there are ways to include them in a balanced, healthy diet. They are a low-calorie, nearly fat-free food, so for those watching their weight, eating a marshmallow is a quick and easy way to satisfy a sweet tooth. Also, adding marshmallows to certain foods might help increase the intake of healthy vegetables, such as adding marshmallows to sweet potatoes, which are almost always gluten-free. For gluten-intolerant individuals, marshmallows are probably safe to consume. Some brands have also developed vegan marshmallows that use tapioca starch or agar instead of gelatin.
Storage
Marshmallows have a long shelf life. A bag can last up to six or eight months if not opened. They can last four months or less if the bag is open. Some can be purchased in an airtight tin and stored that way. However, they are most often in a plastic bag. Therefore, they should be placed in an airtight plastic container or sealed tightly after opening. Marshmallows do not need refrigeration, but many cooks freeze them to make them last longer. An unopened bag can be frozen, forming cubes that may stick together. To prevent sticking, dust with powdered sugar and place in an airtight container. When they are thawed, they regain their fluffy texture.
Allergies
Allergies are rare. However, those allergic to gelatin may want to avoid marshmallows since gelatin is a primary ingredient in almost all prepared and homemade versions.(Caglayan-Sozmen S. et al., 2019)
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic providers use an integrated approach to create customized plans for each patient and restore health and function to the body through nutrition and wellness, chiropractic adjustments, functional medicine, acupuncture, Electroacupuncture, and sports medicine protocols. If other treatment is needed, patients will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Balancing Body and Metabolism
References
United States Department of Agriculture. FoodData Central. (2018). Candies, marshmallows. Retrieved from https://fdc.nal.usda.gov/fdc-app.html#/food-details/167995/nutrients
Caglayan-Sozmen, S., Santoro, A., Cipriani, F., Mastrorilli, C., Ricci, G., & Caffarelli, C. (2019). Hazardous Medications in Children with Egg, Red Meat, Gelatin, Fish, and Cow’s Milk Allergy. Medicina (Kaunas, Lithuania), 55(8), 501. https://doi.org/10.3390/medicina55080501
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine