Wrestling Injury: Louie Martinez has had the pleasure of being a wrestling coach for approximately 15 years. Through his experience, Coach Martinez understands the importance of chiropractic care for the wrestler. Sports injuries can commonly occur in wrestling, however, Louie Martinez explains how with Dr. Alex Jimenez, it’s only a matter of visiting his clinic to receive the proper treatment to return-to-play. Coach Louie Martinez also describes how Dr. Alex Jimenez helped his sons, whom are also wrestlers, develop their overall potential.
Sports injuries are injuries which occur in sports, exercise or athletic activities. In the United States, there are approximately 30 million teens and kids alone that participate in some type of organized physical activity. About 3 million athletes, about 14 years of age and under, experience sports injuries yearly, which causes loss of time participating in their specific sport, exercise or athletic activities. Prevention helps reduce potential sport injuries. It is important to set up involvement in warm-ups, stretching, and exercises which focus on primary muscle groups commonly utilized in the sport of interest.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
When we think of cheerleaders we usually think of pretty girls in colorful outfits, pom pom’s in hand, cheering for their team. They are way more than that though. Cheerleaders are serious athletes.
It has taken a while, but the public is finally starting to realize just how true this is. Data collected by the National Center for Catastrophic Sports Injury Research (NCCSIR), between 1982 and 2009 cheerleaders made up for more than 70 percent of catastrophic injuries in women�s college sports. At the high school level that number exceeded 60 percent.
Some claim that this high percentage of injuring among cheerleaders to be due to lax regulations at the state level. Some states refuse to recognize cheerleading as a sport and organizations such as the NCAA don�t either.
This leaves an already potentially dangerous activity without proper oversight of the government or regulating agencies. It also means that some people who manage cheer squads and organize competitions are not required to get the same coaching and safety training standards that those in other sports do.
Since chiropractic treats the whole body through not just structurally via spinal adjustments, but also through soft tissue techniques, patients can receive complete care after an injury and during rehabilitation. Cheerleaders are finding that chiropractic treatment provides numerous benefits and can even make them better athletes.
Cheerleaders
Chiropractic Helps To Improve Range Of Motion
Chiropractic care helps to improve a person�s range of motion which in turn helps to prevent injury and relieve the pain of injury. Chiropractic is growing in its popularity within the field of sports medicine because of its effectiveness. A 2010 study published in The Journal of the Canadian Chiropractic Association showed that chiropractic made a significant difference in performance.
Chiropractic Helps To Prevent Injury
Even when no injury is present, athletes can benefit from chiropractic care. This is especially true in high impact sports like cheerleading where athletes push their bodies beyond limits through acrobatics and some of the strenuous tricks that they do in the course of their sport. Chiropractic helps to loosen muscles, making them more pliable and flexible, thus less prone to injury.
Chiropractic Helps To Relieve Pain From Injury
A study published in the Journal of Manipulative and Physiological Therapeutics in March 2011 shows that chiropractic for pain relief can alleviate the pain of hamstring injury. The study was conducted over the course of a football season and involved 43 professional cheerleaders for football various football teams.
Throughout the study the cheerleaders received specific exercise intervention. At the end of the study those who had reported pain due to a hamstring injury experienced significant pain reduction after receiving chiropractic treatment.
Chiropractic Can Increase Physical Strength
While chiropractic is typically considered a therapy for alleviating skeletal and muscular complaints, a study in 2011 showed that it can also improve physical strength. The study involved judo athletes competing at the national level who used cervical spinal manipulative therapy (SMT). The final results of the study showed a 16 percent improvement in grip strength among the athletes who received only three SMT sessions.
The case for chiropractic treatment for athletes is very strong. It can help during training, recovery from injury, rehabilitation, and at every point in between. Although cheerleaders are still in their infancy of being recognized as serious athletes, the case for chiropractic care as a viable sports medicine therapy to improve performance and recover from injury is significant. The benefits that cheerleaders can receive from chiropractic treatment, as we can see, can really give them something to cheer about both on the field and off.
Sports Injury Treatment: PUSH-as-Rx ��: 915-203-8122 | Dr. Alex Jimenez � Chiropractor: 915-850-0900 PUSH-as-Rx ���is leading the field with laser focus supporting our youth sport programs.� The�PUSH-as-Rx ���System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. �Immediately,�we adjust our methods for our athletes in order to optimize performance.� This highly adaptive system with continual�dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics.��PUSH-as-Rx ���offers specialized extreme performance enhancements to our athletes no matter the age.
Sports Injury Treatment
Vincent Garcia, an athlete training in mixed martial arts, or MMA, suffered a knee injury and developed turf toe, but that hasn’t stopped him from participating in his regular training regimen. In order to return to as well as improve his original physical performance, Vincent Garcia found treatment with Dr. Alex Jimenez, doctor of chiropractic. Now recovering from his sports injuries, Vincent Garcia looks forward to regaining his strength, flexibility and mobility to return to sport.
Dr. Alex Jimenez D.C. – Treats Vince Garcia MMA Fighter for Sports Injuries, including knee pain and turf toe. Dr. Jimenez D.C can be reached at (915) 850-0900 or visit our website at www.DrAlexJimenez.com
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Baseball Injuries: The crack of a ball against your bat, good! The crack of a back or shoulder, bad!
Baseball, the nationwide pass time, heats up in summer. From little league on up, individuals enjoy swinging the bat and running the bases. Unfortunately, the movements baseball requires can wreak havoc on a person’s body, leaving them with strained backs, hurt shoulders, and pulled muscles. According to Livestrong, there are over 600,000 injuries from playing baseball per year, and 5-14 year olds suffer from 117,000 of them.
The aspects of the game � running, sliding, twisting, and jumping � cause the body to maneuver into awkward positions. If you or a loved one has slid into first and felt a pop, or twisted to catch a fly ball and felt a snap, chiropractic care offers several ways to help put you on the road to a complete recovery.
Baseball Injuries: Manage Pain
Baseball injuries frequently involve large muscles, resulting in a high degree of pain. Chiropractic treatment offers relief from severe pain of many injuries involving the spine, muscles, and joints.
Using spinal adjustments, a chiropractor is able to help the body align itself properly, and sooth the injured area. Once the body functions normally, pain is diminished. Sometimes this can be accomplished in one visit, while other injuries require a few sessions before pain diminishes.
Increase Mobility
A strained neck, pulled back, or overextended knee may cause the individual serious issues in being able to move. Limping around slowly is nobody’s idea of fun!
Chiropractic adjustments are proven to help reduce inflammation and improve mobility in many injury cases. If that last baseball game has you unable to put weight on your knee, your neck won’t twist without pain, or your shoulder won’t lift your arm, it may be time to visit a chiropractor for evaluation.
Promote Healing
The premise of chiropractic care is to treat the entire body as a whole, not just the injured part. As the body becomes better aligned, it functions at a higher capacity, and begins to heal itself.
Most injuries resulting from playing baseball, such as tendonitis, strained muscles, torn rotator cuffs, and the like, heal faster with chiropractic care. Increased blood flow to the injured area, and less pressure on the body part (usually due to misalignment of the spine) allow the injured area to regenerate, and a greater chance to begin healing faster than without chiropractic care.
Avoid Medication
Even over-the-counter pain and anti-inflammatory drugs cause side effects in certain individuals. Allergies, stomach issues, and other reasons result in many injured people steering clear of medication to relieve pain and inflammation.
Chiropractic care provides these individuals a drug-free, less invasive way to help manage the pain and promote healing. More people every year are choosing to visit a chiropractor for pain relief instead of popping pain medicine.
Before jumping into a baseball game, or even if you or your children play regularly, remember that prevention is worth its weight in gold. Take care of your body by stretching beforehand, being aware of your physical limits, maintaining proper posture, and staying hydrated during the game. With a little extra effort, the chance of a baseball injury can be dramatically decreased.
Summer fun often includes activities such as baseball, whether in a league or in your back yard with your family. Avoid suffering from an injury as best you can, and, if you or your child end up with an achy knee, twisted elbow, or smarting shoulder, call you chiropractor to schedule a thorough evaluation as quickly as possible.
Prevention, Recognition & Management Of Youth Sports Injuries
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Stay Hydrated: Summer fun means outside activities in the warm sun, from strenuous pursuits like biking, hiking, and volleyball-playing, to more leisurely enjoyments like sunbathing on a float. No matter how you plan to enjoy the steamy summer months, maintaining hydration should be right up there with sunscreen on your list of important hot weather priorities.
Dehydration is a condition that ranges from mild to serious, and can happen quicker than you think. Right Diagnosis defines dehydration as “an abnormal condition in which the body’s cells are deprived of an adequate amount of water.” One of the main situations factoring into a person becoming dehydrated is heat.
Think you drink enough water and don’t need to worry about dehydration? Consider these points:
The ability to recognize thirst diminishes in individuals in their late 30’s or older.
A person’s body is made up of roughly 70% water.
When you lose 2% of the body’s water content, you are considered dehydrated.
Dehydration symptoms range from unpleasant confusion, muscle weakness, and fatigue to extremely dangerous ones like seizures, kidney failure, and death. The good news is that if you stay hydrated in the first place is relatively easy if you take a few precautions up front.
#1: Drink Plenty Of Water
Make it a habit of carrying water with you during the summer months, and sipping on it throughout the day, especially if you are planning on outside activities. Invest in a couple of BPA-free water bottles for yourself and your family to tote with them on their summer adventures.
Not a big fan of plain water? Try adding lemon, cucumber, and mint sprigs to liven it up! Mix up in a big pitcher the night before so the flavor has time to penetrate. Another option is flavor packets, which are individual packets of flavors like green tea, watermelon, and peach.
#2: Eat The Right Foods
Liquids aren’t the only way your body gets water. Avoid dehydration by eating foods with a high water content.
Choices like celery, watermelon, cucumbers, carrots, and citrus fruits all offer exceptional hydrating ability. Pack these as snacks for the pool or beach, or to enjoy before and after an outdoor workout.
#3: Steer Clear Of Certain Drinks
As yummy and refreshing as an icy beer or frosty margarita tastes, alcohol can contribute to dehydration. If you decide to indulge, limit yourself to one or two, and drink a large glass of water along with your beverage to counteract the alcohol’s effects.
#4: Avoid Overexertion
Exercise is a wonderfully healthy pursuit; however, keep an eye on the temperature. If it is going to be exceptionally hot and humid, choose to exercise either early in the morning, or after sunset, when temperatures are lower and the sun isn’t beaming.
#5: Wear Proper Attire
Dress in light, airy clothing in fabrics that breathe. Protect your head with a cap or hat that shades your face. Avoid black clothing, which tends to absorb the sun and make you hotter.
#6: Stay Hydrated & Be Prepared
Extreme heat makes everyday issues like a flat tire or dead battery life-threatening. Visit a mechanic to confirm your vehicle is in good shape to lessen the chances of getting stranded. Carry extra water or sports drinks in your vehicle, and keep your cell phone charged. If your car breaks down, either stay in your car to wait for help, or stand in the grass instead of on the sizzling pavement.
When you stay hydrated is essential for good health all the time, and during the summer in particular. Implement these easy tips into your daily routine so you and your family maintain hydration and enjoy hot weather outdoor fun.
Chiropractic Treatment For Concussions
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Nutrition�Abstract: A number of factors contribute to success in sport, and diet is a key component. An athlete�s dietary requirements depend on several aspects, including the sport, the athlete�s goals, the environment, and practical issues. The importance of individualized dietary advice has been increasingly recognized, including day-to-day dietary advice and specific advice before, during, and after training and/or competition. Athletes use a range of dietary strategies to improve performance, with maximizing glycogen stores a key strategy for many. Carbohydrate intake during exercise maintains high levels of carbohydrate oxidation, prevents hypoglycemia, and has a positive effect on the central nervous system. Recent research has focused on athletes training with low carbohydrate availability to enhance metabolic adaptations, but whether this leads to an improvement in performance is unclear. The benefits of protein intake throughout the day following exercise are now well recognized. Athletes should aim to maintain adequate levels of hydration, and they should minimize fluid losses during exercise to no more than 2% of their body weight. Supplement use is widespread in athletes, with recent interest in the beneficial effects of nitrate, beta-alanine, and vitamin D on performance. However, an unregulated supplement industry and inadvertent contamination of supplements with banned substances increases the risk of a positive doping result. Although the availability of nutrition information for athletes varies, athletes will bene t from the advice of a registered dietician or nutritionist.
Introduction To The Importance & Influence Of Nutrition On Exercise
Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
Evidence supports a range of dietary strategies in enhancing sports performance. It is likely that combining several strategies will be of greater bene t than one strategy in isolation.5 Dietary strategies to enhance performance include optimizing intakes of macronutrients, micronutrients, and fluids, including their composition and spacing throughout the day. The importance of individualized or personalized dietary advice�is becoming increasingly recognized,6 with dietary strategies varying according to the individual athlete�s sport, personal goals, and practicalities (eg, food preferences). �Athlete� includes individuals competing in a range of sport types, such as strength and power (eg, weight-lifting), team (eg, football), and endurance (eg, marathon running). The use of dietary supplements can enhance performance, provided these are used appropriately. This manuscript provides an overview of dietary strategies used by athletes, the efficacy of these strategies, availability of nutrition information to athletes, and risks associated with dietary supplement intake.
Review Of Diet Strategies Employed By Athletes
Maximizing Muscle Glycogen Stores Prior To Exercise
Carbohydrate loading aims to maximize an athlete�s muscle glycogen stores prior to endurance exercise lasting longer than 90 minutes. Benefits include delayed onset of fatigue (approximately 20%) and improvement in performance of 2%�3%.7 Initial protocols involved a depletion phase (3 days of intense training and low carbohydrate intake) followed by a loading phase (3 days of reduced training and high carbo- hydrate intake).8,9 Further research showed muscle glycogen concentrations could be enhanced to a similar level without the glycogen-depletion phase,10 and more recently, that 24 hours may be sufficient to maximize glycogen stores.11,12 Current recommendations suggest that for sustained or intermittent exercise longer than 90 minutes, athletes should consume 10�12 g of carbohydrate per kg of body mass (BM) per day in the 36�48 hours prior to exercise.13
There appears to be no advantage to increasing pre- exercise muscle glycogen content for moderate-intensity cycling or running of 60�90 minutes, as signi cant levels of glycogen remain in the muscle following exercise.7 For exercise shorter than 90 minutes, 7�12 g of carbohydrate/kg of BM should be consumed during the 24 hours preceding.13 Some14,15 but not all16 studies have shown enhanced performance of intermittent high-intensity exercise of 60�90 minutes with carbohydrate loading.
Carbohydrate eaten in the hours prior to exercise (com- pared with an overnight fast) has been shown to increase muscle glycogen stores and carbohydrate oxidation,17 extend cycle time to exhaustion,5 and improve exercise performance.5,18 Specific recommendations for exercise of longer than 60 minutes include 1�4 g of carbohydrate/kg of BM in the 1�4 hours prior.13 Most studies have not found improvements in performance from consuming low glycemic�index (GI) foods prior to exercise.19 Any metabolic or performance effects from low GI foods appear to be attenuated when carbohydrate is consumed during exercise.20,21
Carbohydrate Intake During The Event
Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23
In longer events, carbohydrate improves performance primarily by preventing hypoglycemia and maintaining high levels of carbohydrate oxidation.6 The rate of exogenous carbohydrate oxidation is limited by the small intestine�s ability to absorb carbohydrate.6 Glucose is absorbed by the sodium- dependent transporter (SGLT1), which becomes saturated with an intake of approximately 1 g/minute. The simultaneous ingestion of fructose (absorbed via glucose transporter 5�[GLUT5]), enables oxidation rates of approximately 1.3 g/minute,24 with performance benefits apparent in the third hour of exercise.6 Recommendations reflect this, with 90 g of carbohydrate from multiple sources recommended for events longer than 2.5 hours, and 60 g of carbohydrate from either single or multiple sources recommended for exercise of 2�3 hours� duration (Table 1). For slower athletes exercising at a lower intensity,�carbohydrate requirements will be less due to lower carbohydrate oxidation.6 Daily training with high carbohydrate availability has been shown to increase exogenous carbohydrate oxidation rates.25
The �Train-Low, Compete-High� Approach
The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27
Fat As A Fuel During Endurance Exercise
There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues.
Nutrition: Protein
While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33
Fluid And Electrolytes
The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate.
Hydration requirements are closely linked to sweat loss, which is highly variable (0.5�2.0 L/hour) and dependent on type and duration of exercise, ambient temperature, and athletes� individual characteristics.35 Sodium losses linked to high temperature can be substantial, and in events of long duration or in hot temperatures, sodium must be replaced along with fluid to reduce risk of hyponatremia. 35
It has long been suggested that fluid losses greater than 2% of BM can impair performance,35 but there is controversy over the recommendation that athletes maintain BM by fluid ingestion throughout an event.37 Well-trained athletes who �drink to thirst� have been found to lose as much as 3.1% of BM with no impairment of performance in ultra-endurance events.38 Ambient temperature is important, and a review illustrated that exercise performance was preserved if loss was restricted to 1.8% and 3.2% of BM in hot and temperate conditions, respectively.39
Dietary Supplementation: Nitrates, Beta-Alanine & Vitamin D
Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
BA is a precursor of carnosine, which is thought to have a number of performance-enhancing functions including the reduction of acidosis, regulation of calcium, and antioxidant properties.45 Supplementation with BA has been shown to�2�state; 0.9% improvement in time trials), reduce fatigue, and�augment intracellular carnosine concentration.45 A systematic review concluded that BA may increase power output and working capacity and decrease feelings of fatigue, but that there are still questions about safety. The authors suggest caution in the use of BA as an ergogenic aid.46
Vitamin D is essential for the maintenance of bone health and control of calcium homeostasis, but is also important for muscle strength,47,48 regulation of the immune system,49 and cardiovascular health.50 Thus inadequate vitamin D status has potential implications for the overall health of athletes and performance. A recent review found that the vitamin D status of most athletes reflects that of the population in their locality, with lower levels in winter, and athletes who train predominantly indoors are at greater risk of deficiency.51 There are no dietary vitamin D recommendations for athletes; however, for muscle function, bone health, and avoidance of respiratory infections, current evidence supports maintenance of serum 25-hydroxy vitamin D (circulating form) concentrations of 80�100 nmol/L.51
Diets Specific For Post Exercise
Recovery from a bout of exercise is integral to the athlete�s training regimen. Without adequate recovery of carbohydrate, protein, fluids, and electrolytes, beneficial adaptations and performance may be hampered.
Muscle Glycogen Synthesis
Consuming carbohydrates immediately post exercise to coincide with the initial rapid phase of glycogen synthesis has been used as a strategy to maximize rates of muscle glycogen synthesis. An early study found delaying feeding by 2 hours after glycogen-depleting cycling exercise reduced glycogen synthesis rates.52 However the importance of this early enhanced rate of glycogen synthesis has been questioned in the context of extended recovery periods with sufficient carbohydrate consumption. Enhancing the rate of glycogen synthesis with immediate carbohydrate consumption after exercise appears most relevant when the next exercise session is within 8 hours of the first.53,54 Feeding frequency is also irrelevant with extended recovery; by 24 hours post exercise, consumption of carbohydrate as four large meals or 16 small snacks had comparable effects on muscle glycogen storage.55
With less than 8 hours between exercise sessions, it is recommended that for maximal glycogen synthesis, 1.0�1.2 g/kg/hour is consumed for the first 4 hours, followed by resumption of daily carbohydrate requirements.13 Additional protein has been shown to enhance glycogen�synthesis rates when carbohydrate intake is suboptimal.56 The consumption of moderate to high GI foods post exercise is recommended;13 however, when either a high-GI or low-GI meal was consumed after glycogen-depleting exercise, no performance differences were seen in a 5 km cycling time trial 3 hours later.57
Muscle Protein Synthesis
An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59
Only a few studies have investigated the effect of timing of protein intake post exercise. No significant difference in MPS was observed over 4 hours post exercise when a mixture of essential amino acids and sucrose was fed 1 hour versus 3 hours after resistance exercise.60 Conversely, when a protein and carbohydrate supplement was provided immediately versus 3 hours after cycling exercise, leg protein synthesis increased threefold over 3 hours.61 A meta-analysis found timed post exercise protein intake becomes less important with longer recovery periods and adequate protein intake,62 at least for resistance training.
Dose�response studies suggest approximately 20 g of high-quality protein is sufficient to maximize MPS at rest,63 following resistance,63,64 and after high-intensity aerobic exercise.65 Rate of MPS has been found to approximately triple 45�90 minutes after protein consumption at rest, and then return to baseline levels, even with continued availability of circulating essential amino acids (termed the �muscle full� effect).66 Since exercise-induced protein synthesis is elevated for 24�48 hours following resistance exercise67and 24�28 hours following high-intensity aerobic exercise,68 and feeding protein post exercise has an additive effect,58,64 then multiple feedings over the day post exercise might maximize muscle growth. In fact, feeding 20 g of whey protein every 3 hours was subsequently found to maximally stimulate muscle myofibrillar protein synthesis following resistance exercise.69,70
In resistance training, where post exercise intake of protein was balanced by protein intake later in the day, increased adaptation of muscle hypertrophy resulted in equivocal strength performance effects.71,72 Most studies have not found a subsequent bene t to aerobic performance with post exercise protein consumption.73,74 However, in two�well controlled studies in which post exercise protein intake was balanced by protein intake later in the day, improvements were seen in cycling time to exhaustion75 and in cycling sprint performance.76
Fluids And Electrolyte Balance
Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77
Availability Of Nutritional Information To Athletes At Varying Levels
The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78
Athletes eat several times per day, with snacks contributing to energy requirements.79 Dietary intake differs across sports, with endurance athletes more likely to achieve energy and carbohydrate requirements compared to athletes in weight-conscious sports.79 A review found daily intakes of carbohydrate were 7.6 g/kg and 5.7 g/kg of BM for male and female endurance athletes, respectively.80 Ten elite Kenyan runners met macronutrient recommendations but not guide- lines for fluid intake.81 A review of fluid strategies showed a wide variability of intake across sports, with several factors influencing intake, many outside the athlete�s control.82
Nutrition information may be delivered to athletes by a range of people (dietitians, nutritionists, medical practitioners, sports scientists, coaches, trainers) and from a variety of sources (nutrition education programs, sporting magazines, the media and Internet).83 Of concern is the provision of�nutrition advice from outside various professional�s scope of practice. For example, in Australia 88% of registered exercise professionals provided nutrition advice, despite many not having adequate nutrition training.84 A study of Canadian high-performance athletes from 34 sports found physicians ranked eighth and dietitians, 16th as choice of source of dietary supplement information.85
Risks Of Contravening The Doping Regulations
Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85
Athletes take supplements for many reasons, including for proposed performance benefits, for prevention or treatment of a nutrient deficiency, for convenience, or due to fear of �missing out� by not taking a particular supplement.41
The potential benefits (eg, improved performance) of taking a dietary supplement must outweigh the risks.86,87 There are few permitted dietary supplements available that have an ergogenic effect.87,89 Dietary supplementation cannot compensate for poor food choices.87 Other concerns include lack of efficacy, safety issues (toxicity, medical concerns), negative nutrient interactions, unpleasant side effects, ethical issues, financial expense, and lack of quality control.41,86,87 Of major concern, is the consumption of prohibited substances by the World Anti-Doping Agency (WADA).
Inadequate regulation in the supplement industry (com- pounded by widespread Internet sales) makes it difficult for athletes to choose supplements wisely.41,86,87 In 2000�2001, a study of 634 different supplements from 13 countries found that 94 (14.8%) contained undeclared steroids, banned by WADA.90 Many contaminated supplements were routinely used by athletes (eg, vitamin and mineral supplements).86 Several studies have confirmed these findings. 41,86,89
A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99
In an effort to educate athletes about sports-supplement use, the Australian Institute of Sport�s sports-supplement program categorizes supplements according to evidence�of efficacy in performance and risk of doping outcome.40 Category A supplements have sound evidence for use and include sports foods, medical supplements, and performance supplements. Category D supplements should not be used by athletes, as they are banned or are at high risk for contamination. These include stimulants, pro-hormones and hormone boosters, growth hormone releasers, peptides, glycerol, and colostrum.40
Conclusion
Athletes are always looking for an edge to improve their performance, and there are a range of dietary strategies available. Nonetheless, dietary recommendations should be individualized for each athlete and their sport and provided by an appropriately qualified professional to ensure optimal performance. Dietary supplements should be used with caution and as part of an overall nutrition and performance plan.
Disclosure
The authors report no conflicts of interest in this work.
Kathryn L Beck1 Jasmine S Thomson2 Richard J Swift1 Pamela R von Hurst1
1School of Food and Nutrition, Massey institute of Food Science and Technology, College of Health, Massey University Albany, Auckland, 2School of Food and Nutrition, Massey institute of Food Science and Technology, College of Health, Massey University Manawatu, Palmerston North, New Zealand
Blank
References:
1. Burke LM, Meyer NL, Pearce J. National nutritional programs for the
2012 London Olympic Games: A systematic approach by three different
countries. In: van Loon LJC, Meeusen R, editors. Limits of Human
Endurance. Nestle Nutrition Institute Workshop Series, volume 76.
Vevey, Switzerland: Nestec Ltd; 2013:103�120.
2. Hansen EA, Emanuelsen A, Gertsen RM, S�rensen SSR. Improved
marathon performance by in-race nutritional strategy intervention.
Int J Sport Nutr Exerc Metab. 2014;24(6):645�655.
3. Hottenrott K, Hass E, Kraus M, Neumann G, Steiner M, Knechtle B.
A scientific nutrition strategy improves time trial performance by ?6%
when compared with a self-chosen nutrition strategy in trained cyclists:
a randomized cross-over study. Appl Physiol Nutr Metab. 2012;
37(4):637�645.
4. Jeukendrup AE, Martin J. Improving cycling performance: how should
we spend our time and money. Sports Med. 2001;31(7):559�569.
5. Wright DA, Sherman WM, Dernbach AR. Carbohydrate feedings
before, during, or in combination improve cycling endurance
performance. J Appl Physiol (1985). 1991;71(3):1082�1088.
6. Jeukendrup A. A step towards personalized sports nutrition: carbohydrate
intake during exercise. Sports Med. 2014;44 Suppl 1:
S25�S33.
7. Hawley JA, Schabort EJ, Noakes TD, Dennis SC. Carbohydrateloading
and exercise performance. An update. Sports Med. 1997;24(2):
73�81.
8. Bergstr�m J, Hermansen L, Hultman E, Saltin B. Diet, muscle glycogen
and physical performance. Acta Physiol Scand. 1967;71(2):140�150.
9. Karlsson J, Saltin B. Diet, muscle glycogen, and endurance performance.
J Appl Physiol. 1971;31(2):203�206.
10. Sherman WM, Costill DL, Fink WJ, Miller JM. Effect of exercise-diet
manipulation on muscle glycogen and its subsequent utilization during
performance. Int J Sports Med. 1981;2(2):114�118.
11. Bussau VA, Fairchild TJ, Rao A, Steele P, Fournier PA. Carbohydrate
loading in human muscle: an improved 1 day protocol. Eur J Appl
Physiol. 2002;87(3):290�295.
12. Fairchild TJ, Fletcher S, Steele P, Goodman C, Dawson B, Fournier PA.
Rapid carbohydrate loading after a short bout of near maximal-intensity
exercise. Med Sci Sports Exerc. 2002;34(6):980�986.
13. Burke LM, Hawley JA, Wong SH, Jeukendrup AE. Carbohydrates for
training and competition. J Sports Sci. 2011;29 Suppl 1:S17�S27.
14. Raman A, Macdermid PW, M�ndel T, Mann M, Stannard SR. The
effects of carbohydrate loading 48 hours before a simulated squash
match. Int J Sport Nutr Exerc Metab. 2014;24(2):157�165.
15. Balsom PD, Wood K, Olsson P, Ekblom B. Carbohydrate intake and
multiple sprint sports: with special reference to football (soccer). Int J
Sports Med. 1999;20(1):48�52.
16. Abt G, Zhou S, Weatherby R. The effect of a high-carbohydrate diet
on the skill performance of midfield soccer players after intermittent
treadmill exercise. J Sci Med Sport. 1998;1(4):203�212.
17. Coyle EF, Coggan AR, Hemmert MK, Lowe RC, Walters TJ. Substrate
usage during prolonged exercise following a preexercise meal. J Appl
Physiol (1985). 1985;59(2):429�433.
18. Neufer PD, Costill DL, Flynn MG, Kirwan JP, Mitchell JB, Houmard J.
Improvements in exercise performance: effects of carbohydrate feedings
and diet. J Appl Physiol (1985). 1987;62(3):983�988.
19. Burke LM, Collier GR, Hargreaves M. Glycemic index � a new tool
in sport nutrition? Int J Sport Nutr. 1998;8(4):401�415.
20. Burke LM, Claassen A, Hawley JA, Noakes TD. Carbohydrate intake
during prolonged cycling minimizes effect of glycemic index of preexercise
meal. J Appl Physiol (1985). 1998;85(6):2220�2226.
21. Wong SH, Chan OW, Chen YJ, Hu HL, Lam CW, Chung PK. Effect of
preexercise glycemic-index meal on running when CHO-electrolyte
solution is consumed during exercise. Int J Sport Nutr Exerc Metab.
2009;19(3):222�242.
22. Burke LM, Maughan RJ. The Governor has a sweet tooth � mouth
sensing of nutrients to enhance sports performance. Eur J Sport Sci.
2015;15(1):29�40.
23. Gant N, Stinear CM, Byblow WD. Carbohydrate in the mouth immediately
facilitates motor output. Brain Res. 2010;1350:151�158.
24. Jentjens RL, Moseley L, Waring RH, Harding LK, Jeukendrup AE.
Oxidation of combined ingestion of glucose and fructose during
exercise. J Appl Physiol (1985). 2004;96(4):1277�1284.
25. Cox GR, Clark SA, Cox AJ, et al. Daily training with high carbohydrate
availability increases exogenous carbohydrate oxidation during endurance
cycling. J Appl Physiol (1985). 2010;109(1):126�134.
26. Bartlett JD, Hawley JA, Morton JP. Carbohydrate availability and
exercise training adaptation: too much of a good thing? Eur J Sport
Sci. 2015;15(1):3�12.
27. Burke LM. Fueling strategies to optimize performance: training high
or training low? Scand J Med Sci Sports. 2010;20 Suppl 2:48�58.
28. Yeo WK, Paton CD, Garnham AP, Burke LM, Carey AL, Hawley JA.
Skeletal muscle adaptation and performance responses to once a day
versus twice every second day endurance training regimens. J Appl
Physiol (1985). 2008;105(5):1462�1470.
29. Morton JP, Croft L, Bartlett JD, et al. Reduced carbohydrate availability
does not modulate training-induced heat shock protein adaptations but
does upregulate oxidative enzyme activity in human skeletal muscle.
J Appl Physiol (1985). 2009;106(5):1513�1521.
30. Horowitz JF, Mora-Rodriguez R, Byerley LO, Coyle EF. Lipolytic suppression
following carbohydrate ingestion limits fat oxidation during
exercise. Am J Physiol. 1997;273(4 Pt 1):E768�E775.
31. Volek JS, Noakes T, Phinney SD. Rethinking fat as a fuel for endurance
exercise. Eur J Sport Sci. 2015;15(1):13�20.
32. Stellingwerff T, Spriet LL, Watt MJ, et al. Decreased PDH activation
and glycogenolysis during exercise following fat adaptation
with carbohydrate restoration. Am J Physiol Endocrinol Metab.
2006;290(2):E380�E388.
33. van Loon LJ. Is there a need for protein ingestion during exercise?
Sports Med. 2014;44 Suppl 1:S105�S111.
34. Hillman AR, Turner MC, Peart DJ, et al. A comparison of hyperhydration
versus ad libitum fluid intake strategies on measures of
oxidative stress, thermoregulation, and performance. Res Sports Med.
2013;21(4):305�317.
35. Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ,
Stachenfeld NS; American College of Sports Medicine. American
College of Sports Medicine position stand. Exercise and fluid
replacement. Med Sci Sports Exerc. 2007;39(2):377�390.
36. Kristal-Boneh E, Glusman JG, Shitrit R, Chaemovitz C, Cassuto Y.
Physical performance and heat tolerance after chronic water loading and
heat acclimation. Aviat Space Environ Med. 1995;66(8):733�738.
37. Noakes TD. Drinking guidelines for exercise: what evidence is there that
athletes should drink �as much as tolerable�, �to replace the weight lost
during exercise� or �ad libitum�? J Sports Sci. 2007;25(7):781�796.
38. Hoffman MD, Stuempfle KJ. Hydration strategies, weight change
and performance in a 161 km ultramarathon. Res Sports Med.
2014;22(3):213�225.
The term �ergogenic� stems from the Greek roots � �Ergon� and �genes,� meaning �work� and �born,� respectively. Any means of enhancing energy production or utilization may be described as an ergogenic aid.1 Ergogenic aids have classically been classified into five categories: mechanical, psychological, physiologic, pharmacologic, and nutritional.2 The present use of the term �ergogenic aid� usually revolves around the physiologic, pharmacologic, and nutritional categories.
While ergogenic aids have been linked to athletic �doping,� the terms are not synonymous. Doping is a term used by the International Olympic Committee (IOC) to describe the administration or use of a substance by a competing athlete with the sole intention of increasing in an artificial and unfair manner his or her performance in competition.3 Not all ergogenic aids are banned by the IOC. A partial listing of substances banned by the United States Olympic Committee is found in Table 1.2,3 Table 2 provides a list of commonly used athletic ergogenic aids.
Ergogenic Aids:
Anabolic-Androgenic Steroids
Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3 Athletes have been using AAS since the 1940s in efforts to improve their performance.2 Concerned with widespread abuse of AAS among athletes, the IOC banned AAS use in the early 1960s.2 The Anabolic Steroids Control Act was legalized in 1990, making it a felony to possess or distribute AAS for non-medical purposes in the United States.3,4 Oral, parenteral, transdermal, and intra-nasal forms of AAS are available. The vast majority of AAS used by athletes is thought to be obtained on the �black market,� as only an estimated 10% to 15% of AAS used by athletes for performance enhancement are obtained by prescription.3
AAS are believed to exert their main effect by increasing anabolic processes and inhibiting catabolic processes via specific receptor mediated responses within the target cells.5 Effects of AAS include: the anabolic build-up of muscle mass, the androgenic development of secondary male sexual characteristics, an anti-catabolic reversal of cortisol�s action, and a direct psychological effect thought to allow a more intense and sustained workout.2,5-8 Early studies of AAS and athletes produced mixed results.5,6 More recent reviews support the notions that AAS can provide significant increases in muscle mass and strength in athletes.2,5,6 In order to maximize the effects of AAS on strength and power athletes, an adequate diet and exercise regimen is needed.5 There seems to be little advantage gained while using AAS in the untrained individual.5,9 Benefits obtained from AAS are more established in strength-dependent sports. Data supporting increased aerobic capacity and improved endurance with AAS use is limited and inconclusive.4 AAS effect on endurance sports is currently an area of great interest given the large number of endurance athletes who still use AAS.4,10
An intricate terminology describing the dosing practices of athletes has evolved. Athletes will commonly use AAS over 6 to 12 week �cycles.�4 �Pyramiding� describes a�gradual escalation in the dose of AAS taken over a cycle.2,11 �Stacking� involves the use of more than one AAS, usually with staggered cycles of the individual drugs.2-4 An �array� describes the practice of using other drugs to counteract side effects or enhance the effects of AAS.3 The practices of cycling, pyramiding, and stacking are used by athletes in an attempt to minimize the negative effects of AAS while maximizing the desired enhancements.2,4 At the current time, no solid scientific support exists for these practices.2,4,5
The adverse effects attributed to AAS abuse have been historically overstated.4,12 The majority of AAS side effects are considered minor and reversible following the cessation of use.4 While the incidence of serious side effects from AAS use has been low, devastating consequences have been reported.13 Documented fatalities from myocardial infarc- tion, stroke, and hepatocarcinoma have been attributed to AAS use.2,3 The long-term effects of AAS use are generally unknown.3,11
Dehydroepiandrosterone (DHEA)
Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15
The mechanism of action of DHEA is poorly understood but most likely revolves around the conversion of DHEA to testosterone in peripheral tissues.4,14 Preliminary studies suggest that DHEA may have a broad range of clinical uses including anti-Alzheimer and anti-Parkinson capabilities, however randomized, double-blinded clinical studies are�lacking.5
DHEA is a pre-cursor to testosterone and theoretically may enhance athletic performance in a manner similar to AAS. Investigations of DHEA use and athletic performance are scarce.14 Existing studies do not support a significant increase in lean body mass, strength, or testosterone levels with the use of DHEA in athletes.14,16-18
Long-term side effects of DHEA use are currently un- known but are probably similar to those associated with AAS use.6,14
Androstenedione
Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19
Similar to DHEA, the mechanism of action and side ef- fects attributed to androstenedione are poorly understood and thought to be related to the conversion of androstenedione to testosterone in the peripheral tissues.5
Despite manufacturers� claims to the contrary, there is little scientific evidence of the purported ergogenic aid effects of androstenedione.2,5,16,20 Recently concerns have grown over the unfavorable alterations in blood lipid and coronary heart disease profiles seen in men using androstenedione as an ergogenic aid.2,20,21
Dietary Supplements
The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter.
Ephedra
Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects.
Multiple studies of isolated ephedrine alkaloids have shown no significant enhancement of power or endurance at dosages considered to be safe.24,27-31 In contrast, the combination of caffeine with ephedrine has been associated with improvements in performance and may promote metabolic effects that are conducive to body fat loss.26,32
The actual content of ephedra alkaloids in 20 ephedra- containing dietary supplements was studied using high- performance liquid chromatography.33 Ten of the twenty supplements exhibited marked discrepancies between the label claim for ephedra content and the actual alkaloid content. Between 1995 and 1997, 926 cases of possible Mahuang toxicity were reported to the Food and Drug Ad- ministration.34 A temporal relationship between Mahuang use and severe complications including stroke, myocardial infarction, and sudden death was established in 37 of the 926 cases. In 36 of these 37 cases, the Mahuang use was reported to be within the manufacturers� dosing guidelines.
Ephedra and related ephedrine alkaloids are currently banned by the U.S.O.C. and cannot be recommended for general use given their association with potentially life- threatening side effects.2,34
Creatine
Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36
Creatine is synthesized from amino acids primarily in the liver, pancreas, and kidney and is excreted by the kidneys. Creatine is found in skeletal muscle, cardiac muscle, brain, retinal, and testicular tissues.2,37 The interest in creatine as an ergogenic aid revolves around its ability to participate as an energy substrate for muscle contraction.14 Creatine, which easily binds phosphorus, can act as a substrate to donate phosphorus for the formation of ATP. Furthermore, creatine-phosphate (PCr) can help buffer lactic acid because hydrogen ions are used when ATP is regenerated.14,36,38 This role of creatine in exercise is governed by the following reaction:
Normally PCr stores deplete within 10 seconds of short, high-intensity exercise.14,39 Increasing the level of PCr in skeletal muscle, in theory, should result in the ability to sustain high-power output longer and lead to a greater re-synthesis of PCr after exercise.14 The beneficial effects of creatine in response to resistance training are most likely mediated by the following sequence: increased muscle creatine concentration, increased training intensity, which lead to an enhanced physiologic adaptation to training with increased muscle mass and strength.36
Studies evaluating the effectiveness of creatine as an er- gogenic aid are mixed.2,36,40 Multiple reports do conclude that short-term creatine supplementation signi cantly enhances the ability to maintain muscular force and power output dur- ing high-intensity exercise.2,36,41,42 Data on results of creatine supplementation with highly trained athletes is inconclusive. While some papers report improvements with creatine use in highly trained individuals with regards to high-intensity exercise, many show no improvements.2,36,43
Most investigators agree that creatine supplementation does not seem to enhance aerobic-oriented activities.2,36,44
Human muscle is thought to have a maximum concen- tration of creatine that it can hold.14,45 There appears to be no additional bene ts of increasing creatine supplementa- tion above this storage capacity of muscle as the excess is simply excreted by the kidneys.2,46 Humans have differing baseline levels of muscle creatine.14 Accordingly, athletes with lower baseline levels of creatine may be more sensi- tive to creatine supplementation than those with a relatively higher baseline creatine level.14,36 The terms �responder� and �nonresponder� have been used to describe two groups of athletes: those with relatively low baseline creatine levels that may show signi cant performance enhancement with creatine supplementation, and those with high baseline creatine levels that do not show marked improvements with creatine supplementation.14,36,47 These differences in creatine concentrations are thought to play a signi cant role in the varied results on performance found in the literature examin- ing creatine supplementation.14
Reported side effects from creatine use have been scarce.2,14 The major reported side effect associated with creatine use is weight gain, which is thought to be primarily a result of water retention.2,14,48 Some reported longer-term side effects include dehydration, muscle cramping, nausea, and seizures.2,49 Given the relative lack of studies, caution still remains about the long-term effects of creatine usage.14 As creatine use among younger athletes continues to increase, concern is growing over the lack of studies that examine the possible side effects speci c to this age group.14,38
Human Growth Hormone
Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50
Potential benefits of hGH abuse in athletes revolve around�its anabolic effect on the body.4 Human growth hormone is thought to increase muscle mass, and spare muscle glycogen by stimulating lipolysis during exercise.2,3 The popularity of hGH among athletes is furthered by the fact that hGH re- mains extremely difficult to detect by current drug screening processes.3,51 Human growth hormone may be particularly attractive to female athletes as the virilization side effects associated with AAS use are not thought to occur with hGH.4
There are no studies that demonstrate signi cant increases in athletic performance with the use of hGH.3,52,53 Neither human or animal studies show any signi cant strength gains with supplemental hGH use in non-de cient individuals.4 The abuse of hGH is thought to be increasing despite the lack of scienti c evidence linking hGH to improved athlete performance.3,52 A survey of high school males revealed that as many as 5% reported past or present use of hGH.54 The purity of hGH abused by athletes may be poor as Drug Enforcement Agency estimates project that up to 30% to 50% of the hGH products sold are phony.4,55
Adverse effects of exogenous hGH use are extrapolated from the ndings seen in patients with endogenous over- secretion of hGH.2 Adults with high levels of hGH are at risk for the clinical syndrome of acromegaly. Medical complications associated with acromegaly include: diabetes, hypertension, coronary heart disease, cardiomyopathy, men- strual irregularities, and osteoporosis.2,4 High levels of hGH in individuals with open physis may lead to gigantism.2
Erythropoietin (EPO)
Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3
There are few studies evaluating the use of r-EPO in healthy athletes; however, numerous studies have shown a signi cant increase in work capacity due to r-EPO use in patients with renal disease.14 Berglund and Ekblom reported an increased maximal oxygen consumption and increased time to exhaustion in male athletes after a 6 week trial of r-EPO.56
The risks associated with r-EPO abuse involve the potential for dangerously high hematocrit levels.14 A resulting hyperviscosity syndrome may lead to a decreased cardiac output, hypertension, and potential heart failure.3 Further- more, thrombosis could be manifest as myocardial infarction, pulmonary embolism, or cerebrovascular accidents.2,3 Although the use of r-EPO has been banned by the IOC since 1990, its use is extremely difficult to detect with current drug screening measures.2,14
Antioxidants
The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA).
Beta-Hydroxy-Beta-Methylbutyrate
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61
HMB is a relatively new ergogenic aid and published results are considered preliminary.14,58 Although there is evidence for a potential ergogenic aid advantage with HMB use in resistance and endurance training, its use can not be recommended until more studies are performed and potential side effects are elicited.
Caffeine
Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6
Side effects associated with caffeine use include anxiety, diuresis, insomnia, irritability and gastrointestinal discom- fort.2,6 Higher doses of caffeine ingestion can lead to more serious consequences such as cardiac arrhythmia, hallucina- tions, and even death.2,3
The legal urine level of caffeine for athletes is 12 ?g/ml (IOC standards) and 15 ?g/ml (National Collegiate Athletics Association standards).6 An athlete would need to drink six to eight cups of coffee in one sitting and be tested within 2 to 3 hours to reach urine levels over the IOC legal limit.3 The amount of caffeine needed to produce ergogenic benefits is potentially far less than that required to exceed the athletic�legal limit.3
Ergogenic Aids: Summary
Claims championing exotic substances that produce healing or ergogenic powers have been around for centuries. The�competitive, peer-pressured environment enveloping today�s athletes and adolescences makes these groups particularly susceptible to the uproar surrounding the current ergogenic aid market. Presently, it seems that rumor and anecdotal information overwhelms the available scientific data. While there is evidence that some touted ergogenic aids do indeed enhance performance, there are many unanswered questions about product safety, efficacy, and long-term consequences. A working knowledge of specific ergogenic aids is essential for the treating physician in order to best advise patients and athletes as to the possible benefits and risks of any substance they may be using.
By Adam Bernstein, M.D., Jordan Safirstein, M.D., and Jeffrey E. Rosen, M.D.
Americans’ Perception Of Chiropractic
Blank
References
1. Williams MH: Ergogenic and ergolytic substances. Med Sci
Sports Exerc 24(9 Suppl):S344-S348, 1992.
2. Silver MD: Use of ergogenic aids by athletes. J Am Acad
Orthop Surg 9(1):61-70, 2001.
3. KnoppWD,WangTW,Bach JrBR: Ergogenic drugsin sports.
Clin Sports Med 16(3):375-392, 1997.
4. Sturmi JE, Diorio DJ: Anabolic agents. Clin Sports Med
17(2):261-282, 1998.
5. Blue JG, Lombardo JA: Steroids and steroid-like compounds.
Clin Sports Med 18(3):667-689, 1999.
6. Ahrendt DM: Ergogenic aids: counseling the athlete.Am Fam
Physician 63(5):913-922, 2001.
7. Adolescents and anabolic steroids:A subjectreview.American
Academy of Pediatrics. Committee on Sports Medicine and
Fitness. Pediatrics 99(6):904-908, 1997.
8. Haupt HA: Anabolic steroids and growth hormone. Am J
Sports Med 21(3):468-474, 1993.
9. Kuipers H, et al: Influence of anabolic steroids on body composition,
blood pressure, lipid profile and liver functions in
body builders. Int J Sports Med 12(4):413-418, 1991.
10. Lombardo JA: Medical and performance-enhancing effects
of anabolic steroids. Psychiatr Ann 22:19-23, 1992.
11. YesalisCE,Bahrke MS:Anabolic-androgenic steroids: current
issues. Sports Med 19(5):326-340, 1995.
12. Friedl KE: Effects of anabolic steroids on physical health.
In:Yesalis CE (ed): Anabolic Steroids in Sports and Exercise
(2nd ed). Champaign, IL: Human Kinetics Publishers, Inc.,
2000, pp. 35-48.
13. Bahrke MS, Yesalis CE, Brower KJ: Anabolic-androgenic
steroid abuse and performance-enhancing drugs among adolescents.
Child Adolesc Psychiatr Clin N Am 7(4):821-838,
1998.
14. Stricker PR: Other ergogenic agents. Clin Sports Med
17(2):283-297, 1998.
15. Dehydroepiandrosterone (DHEA). Med Lett Drugs Ther
38(985):91-92, 1996.
16. Wallace MB, et al: Effects of dehydroepiandrosterone vs
androstenedione supplementation in men. Med Sci Sports
Exerc 31(12):1788-1792, 1999.
17. Nestler JE, et al: Dehydroepiandrosterone reduces serum
low density lipoprotein levels and body fat but does not alter
insulin sensitivity in normal men. J Clin Endocrinol Metab
66(1):57-61, 1988.
18. Welle S,Jozefowicz R, Statt M: Failure of dehydroepiandrosterone
to influence energy and protein metabolism in humans.
J Clin Endocrinol Metab 71(5):1259-1264, 1990.
19. Saden-Krehula M, Tajic M, Kolbah D: Testosterone, epitestosterone
and androstenedione in the pollen of Scotch pine
P. silvestris L. Experientia 27(1):108-109, 1971.
20. King DS, et al: Effect of oral androstenedione on serum testosterone
and adaptationsto resistance training in young men:
a randomized controlled trial.JAm MedAssoc 281(21):2020-
2028, 1999.
21. Broeder CE, et al: The Andro Project: physiological and
hormonal influences of androstenedione supplementation in
men 35 to 65 years old participating in a high-intensity resistance
training program.Arch Intern Med 160(20):3093-3104,
2000.
22. Benning JR: Nutrition for exercise and sports performance. In:
Mahan LK (ed): Krause�s Food, Nutrition and Diet Therapy.
Philadephia: W.B. Saunders Co., 2000, pp. 534-557.
23. SkolnickAA: Scientific verdictstill out on DHEA.JAm Med
Assoc 276(17):1365-1367, 1996.
24. Bucci LR: Selected herbals and human exercise performance.
Am J Clin Nutr 72(2 Suppl):624S-636S, 2000.
25. Anonymous: The Ephedras. Lawrence Rev Nat Prod, 1989.
26. DiPasquale M: Stimulants and adaptogens: Part I. Drug Sports
1:2-6, 1992.
27. Sidney KH, Lefcoe NM: The effects of ephedrine on the
physiological and psychological responsesto submaximal and
maximal exercise in man. Med Sci Sports 9(2):95-99, 1977.
28. Bright TP, Sandage Jr BW, Fletcher HP: Selected cardiac and
metabolic responsesto pseudoephedrine with exercise.J Clin
Pharmacol 21(11-12):488-492, 1981.
29. DeMeersman R, Getty D, Schaefer DC: Sympathomimetics
and exercise enhancement: all in the mind? Pharmacol Biochem
Behav 28(3):361-365, 1987.
30. SwainRA, et al: Do pseudoephedrine or phenylpropanolamine
improve maximum oxygen uptake and time to exhaustion?
Clin J Sport Med 7(3):168-173, 1997.
31. Gillies H, et al: Pseudoephedrine is without ergogenic effects
during prolonged exercise. J Appl Physiol 81(6):2611-2617,
1996.
32. Bell DG, Jacobs I, Zamecnik J: Effects of caffeine, ephedrine
and their combination on time to exhaustion during
high-intensity exercise. Eur J Appl Physiol Occup Physiol
77(5):427-433, 1998.
33. Gurley BJ, Gardner SF, Hubbard MA: Content versus label
claims in ephedra-containing dietary supplements. Am J
Health Syst Pharm 57(10):963-969, 2000.
34. Samenuk D, et al: Adverse cardiovascular events temporally
associated with ma huang, an herbal source of ephedrine.
Mayo Clin Proc 77(1):12-16, 2002.
35. Juhn MS: Orla creatine supplementation: Separating fact from
hype. Phys Sportsmed 27:47-56, 1999.
36. Kraemer WJ, Volek JS: Creatine supplementation: Its role in
human performance. Clin Sports Med 18(3):651-666, 1999.
37. Williams MH: The use of nutritional ergogenic aidsin sports:
is it an ethical issue? Int J Sport Nutr 4(2):120-131, 1994.
38. MetzlJD, et al: Creatine use among young athletes. Pediatrics
108(2):421-425, 2001.
39. Spriet LL: Ergogenic aids: recent advances and retreats. In:
Lamb DR, Murray R (eds): Perspectives in Exercise Science
and Sports Medicine. Indianapolis, IN: Benchmark Press,
1998, pp. 185-238.
40. Johnson WA, Landry GL: Nutritional supplements: fact vs.
fiction. Adolesc Med 9(3):501-513, 1998.
41. Williams MH, Branch JD: Creatine supplementation and
exercise performance: an update. J Am Coll Nutr 17(3):216-
234, 1998.
42. Mujika I, Padilla S: Creatine supplementation as an ergogenic
aid forsports performance in highly trained athletes: a critical
review. Int J Sports Med 18(7):491-496, 1997.
43. Kreider RB, et al: Effects of creatine supplementation on body
composition,strength, and sprint performance. Med Sci Sports
Exerc 30(1):73-82, 1998.
44. Balsom PD, et al: Creatine supplementation per se does not
enhance endurance exercise performance.Acta Physiol Scand
149(4):521-523, 1993.
45. Harris RC, Soderlund K, Hultman E: Elevation of creatine in
resting and exercised muscle of normal subjects by creatine
supplementation. Clin Sci (Lond) 83(3):367-374, 1992.
46. Clark JF: Creatine: A review of its nutritional applications in
sport. Nutrition 14(3):322-324, 1998.
47. Casey A, et al: Creatine ingestion favorably affects performance
and muscle metabolism during maximal exercise in
humans. Am J Physiol 271(1):E31-E37, 1996.
48. Volek JS: Creatine supplementation: its effect on human
muscular performance and body composition.J Strength Cond
Res 10:200-210, 1996.
49. Feldman EB: Creatine: a dietary supplement and ergogenic
aid. Nutr Rev 57(2):45-50, 1999.
50. Yarasheski KE: Growth hormone effects on metabolism, body
composition, muscle mass, and strength. Exerc Sport Sci Rev
22:285-312. 1994.
51. Risser WL: Sports medicine. Pediatr Rev 14(11):424-431,
1993.
52. Bidlingmaier M, Wu Z, Strasburger CJ: Doping with growth
hormone. J Pediatr Endocrinol Metab 14(8):1077-1083,
2001.
53. Jenkins PJ: Growth hormone and exercise: physiology, use and
abuse. Growth Horm IGF Res 11(Suppl A):S71-S77, 2001.
54. Rickert VI, et al: Human growth hormone: a new substance
of abuse among adolescents? Clin Pediatr (Phila) 31(12):723-
726, 1992.
55. Council Report: Drug abuse in athletes, anabolic steroids and
human growth hormone. J Am Med Assoc 259:1703-1705,
1988.
56. Berglund B, Ekblom B: Effect of recombinant human erythropoietin
treatment on blood pressure and some haematological
parameters in healthy men. J Intern Med 229(2):125-130,
1991.
57. Williams MH: Nutritional supplements for strength trained
athletes. Sports Sci Exchange 6:1-6, 1993.
58. Williams MH: Facts and fallacies of purported ergogenic
amino acid supplements. Clin Sports Med 18(3):633-649,
1999.
59. Vukovich MD, Dreifort GD: Effect of beta-hydroxy betamethylbutyrate
on the onset of blood lactate accumulation
and VO2 peak in endurance-trained cyclists. J Strength Cond
Res 15(4):491-497, 2001.
60. Knitter AE, et al: Effects of beta-hydroxy-beta-methylbutyrate
on muscle damage after a prolonged run. J Appl Physiol
89(4):1340-1344, 2000.
61. Jowko E, et al: Creatine and beta-hydroxy-beta-methylbutyrate
(HMB) additively increase lean body mass and muscle
strength during a weight-training program. Nutrition 17(7-
8):558-566, 2001.
62. Graham TE, Spriet LL: Performance and metabolic responses
to a high caffeine dose during prolonged exercise. J Appl
Physiol 71(6):2292-2298, 1991.
63. KalmarJM, Cafarelli E: Effects of caffeine on neuromuscular
function. J Appl Physiol 87(2):801-808, 1999.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




 Promote Healing
Promote Healing
 #4: Avoid Overexertion
#4: Avoid Overexertion
 Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
Nutrition is increasingly recognized as a key component of optimal sporting performance, with both the science and practice of sports nutrition developing rapidly.1 Recent studies have found that a planned scientific nutritional strategy (consisting of fluid, carbohydrate, sodium, and caffeine) compared with a self-chosen nutritional strategy helped non-elite runners complete a marathon run faster2 and trained cyclists complete a time trial faster.3 Whereas training has the greatest potential to increase performance, it has been estimated that consumption of a carbohydrate�electrolyte drink or relatively low doses of caffeine may improve a 40 km cycling time trial performance by 32�42 and 55�84 seconds, respectively.4
 Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23
Carbohydrate ingestion has been shown to improve performance in events lasting approximately 1 hour.6 A growing body of evidence also demonstrates beneficial effects of a carbohydrate mouth rinse on performance.22 It is thought that receptors in the oral cavity signal to the central nervous system to positively modify motor output.23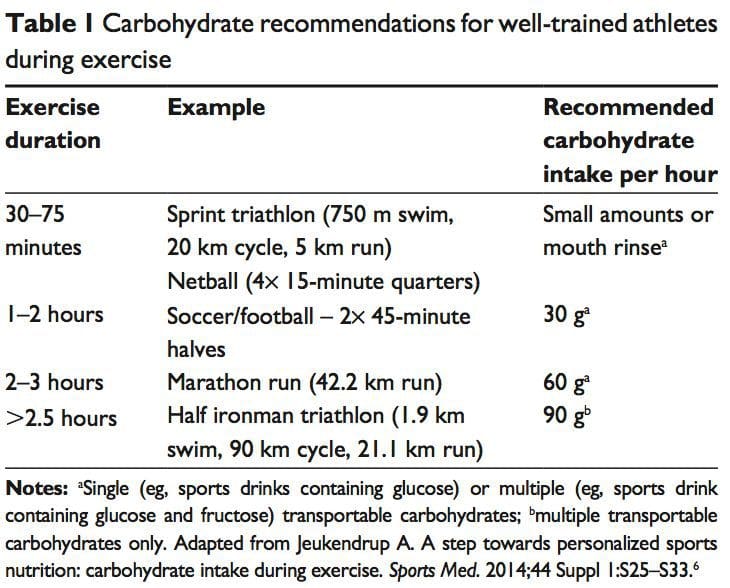
 The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27
The �train-low, compete-high� concept is training with low carbohydrate availability to promote adaptations such as�enhanced activation of cell-signaling pathways, increased mitochondrial enzyme content and activity, enhanced lipid oxidation rates, and hence improved exercise capacity.26 However, there is no clear evidence that performance is improved with this approach.27 For example, when highly trained cyclists were separated into once-daily (train-high) or twice-daily (train-low) training sessions, increases in resting muscle glycogen content were seen in the low-carbohydrate- availability group, along with other selected training adaptations.28 However, performance in a 1-hour time trial after 3 weeks of training was no different between groups. Other research has produced similar results.29 Different strategies have been suggested (eg, training after an overnight fast, training twice per day, restricting carbohydrate during recovery),26 but further research is needed to establish optimal dietary periodization plans.27 There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues.
There has been a recent resurgence of interest in fat as a fuel, particularly for ultra endurance exercise. A high-carbohydrate strategy inhibits fat utilization during exercise,30 which may not be beneficial due to the abundance of energy stored in the body as fat. Creating an environment that optimizes fat oxidation potentially occurs when dietary carbohydrate is reduced to a level that promotes ketosis.31 However, this strategy may impair performance of high-intensity activity, by contributing to a reduction in pyruvate dehydrogenase activity and glycogenolysis. 32 The lack of performance benefits seen in studies investigating �high-fat� diets may be attributed to inadequate carbohydrate restriction and time for adaptation.31 Research into the performance effects of high fat diets continues. While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33
While protein consumption prior to and during endurance and resistance exercise has been shown to enhance rates of muscle protein synthesis (MPS), a recent review found protein ingestion alongside carbohydrate during exercise does not improve time�trial performance when compared with the ingestion of adequate amounts of carbohydrate alone.33 The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate.
The purpose of fluid consumption during exercise is primarily to maintain hydration and thermoregulation, thereby benefiting performance. Evidence is emerging on increased risk of oxidative stress with dehydration.34 Fluid consumption prior to exercise is recommended to ensure that the athlete is well-hydrated prior to commencing exercise.35 In addition,�carefully planned hyperhydration ( fluid overloading) prior to an event may reset fluid balance and increase fluid retention, and consequently improve heat tolerance.36 However, fluid overloading may increase the risk of hyponatremia 37 and impact negatively on performance due to feelings of fullness and the need to urinate. Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
Performance supplements shown to enhance performance include caffeine, beetroot juice, beta-alanine (BA), creatine, and bicarbonate.40 Comprehensive reviews on other supplements including caffeine, creatine, and bicarbonate can be found elsewhere.41 In recent years, research has focused on the role of nitrate, BA, and vitamin D and performance. Nitrate is most commonly provided as sodium nitrate or beetroot juice.42 Dietary nitrates are reduced (in mouth and stomach) to nitrites, and then to nitric oxide. During exercise, nitric oxide potentially influences skeletal muscle function through regulation of blood ow and glucose homeostasis, as well as mitochondrial respiration.43 During endurance exercise, nitrate supplementation has been shown to increase exercise efficiency (4%�5% reduction in VO at a steady attenuate oxidative stress.42 Similarly, a 4.2% improvement in performance was shown in a test designed to simulate a football game.44
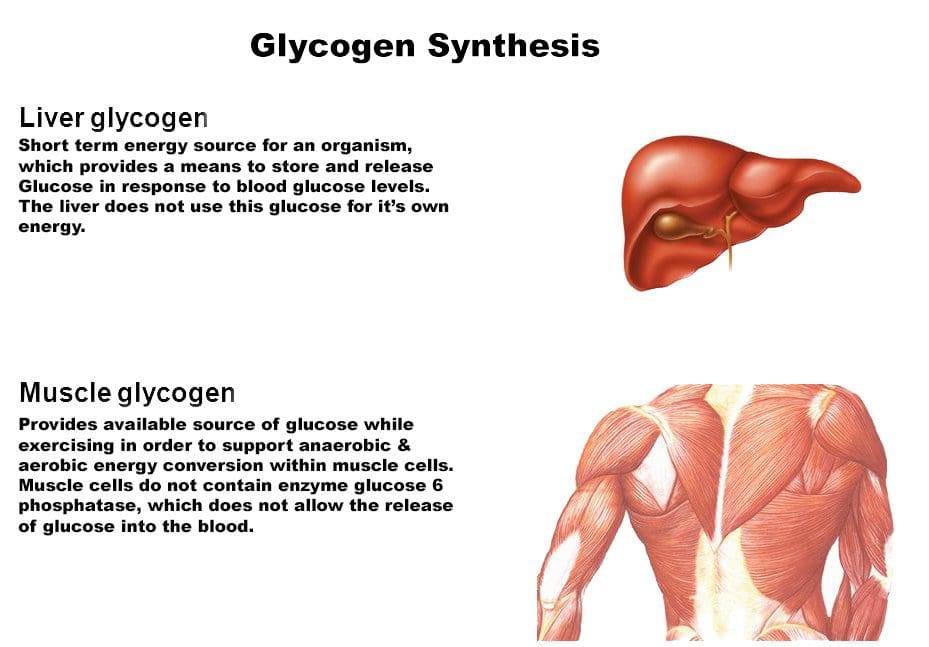 Consuming carbohydrates immediately
Consuming carbohydrates immediately  An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59
An acute bout of intense endurance or resistance exercise can induce a transient increase in protein turnover, and, until feeding, protein balance remains negative. Protein consumption after exercise enhances MPS and net protein balance,58 predominantly by increasing mitochondrial protein fraction with endurance training, and myofibrillar protein fraction with resistance training.59 Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77
Fluid and electrolyte replacement after exercise can be achieved through resuming normal hydration practices. However, when euhydration is needed within 24 hours or substantial body weight has been lost (.5% of BM), a more structured response may be warranted to replace fluids and electrolytes.77 The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78
The availability of nutrition information for athletes varies. Younger or recreational athletes are more likely to receive generalized nutritional information of poorer quality from individuals such as coaches.78 Elite athletes are more likely to have access to specialized sports-nutrition input from qualified professionals. A range of sports science and medicine support systems are in place in different countries to assist elite athletes,1 and nutrition is a key component of these services. Some countries have nutrition programs embedded within sports institutes (eg, Australia) or alternatively have National Olympic Committees that support nutrition programs (eg, United States of America).1 However, not all athletes at the elite level have access to sports-nutrition services. This may be due to financial constraints of the sport, geographical issues, and a lack of recognition of the value of a sports-nutrition service.78 Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85
Supplement use is widespread in athletes.86,87 For example, 87.5% of elite athletes in Australia used dietary supplements88 and 87% of Canadian high-performance athletes took dietary supplements within the past 6 months85 (Table 2). It is difficult to compare studies due to differences in the criteria used to define dietary supplements, variations in assessing supplement intake, and disparities in the populations studied.85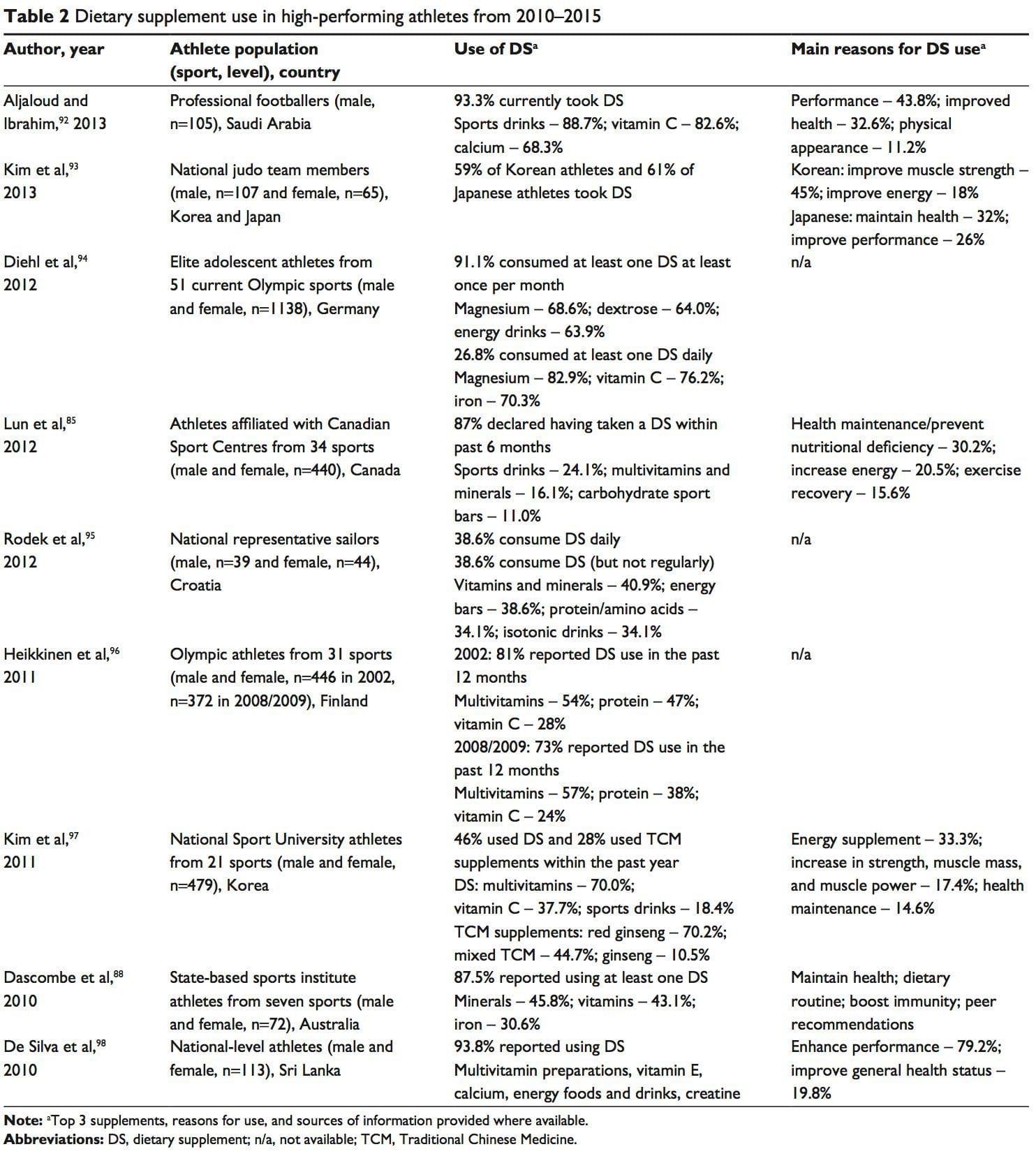 A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99
A positive drug test in an athlete can occur with even a minute quantity of a banned substance.41,87 WADA maintains a �strict liability� policy, whereby every athlete is responsible for any substance found in their body regardless of how it got there.41,86,87,89 The World Anti-Doping Code (January 1, 2015) does recognize the issue of contaminated supplements.91 Whereas the code upholds the principle of strict liability, athletes may receive a lesser ban if they can��show �no significant fault� to demonstrate they did not intend to cheat. The updated code imposes longer bans on those who cheat intentionally, includes athlete support personnel (eg, coaches, medical staff), and has an increased focus on anti-doping education.91,99


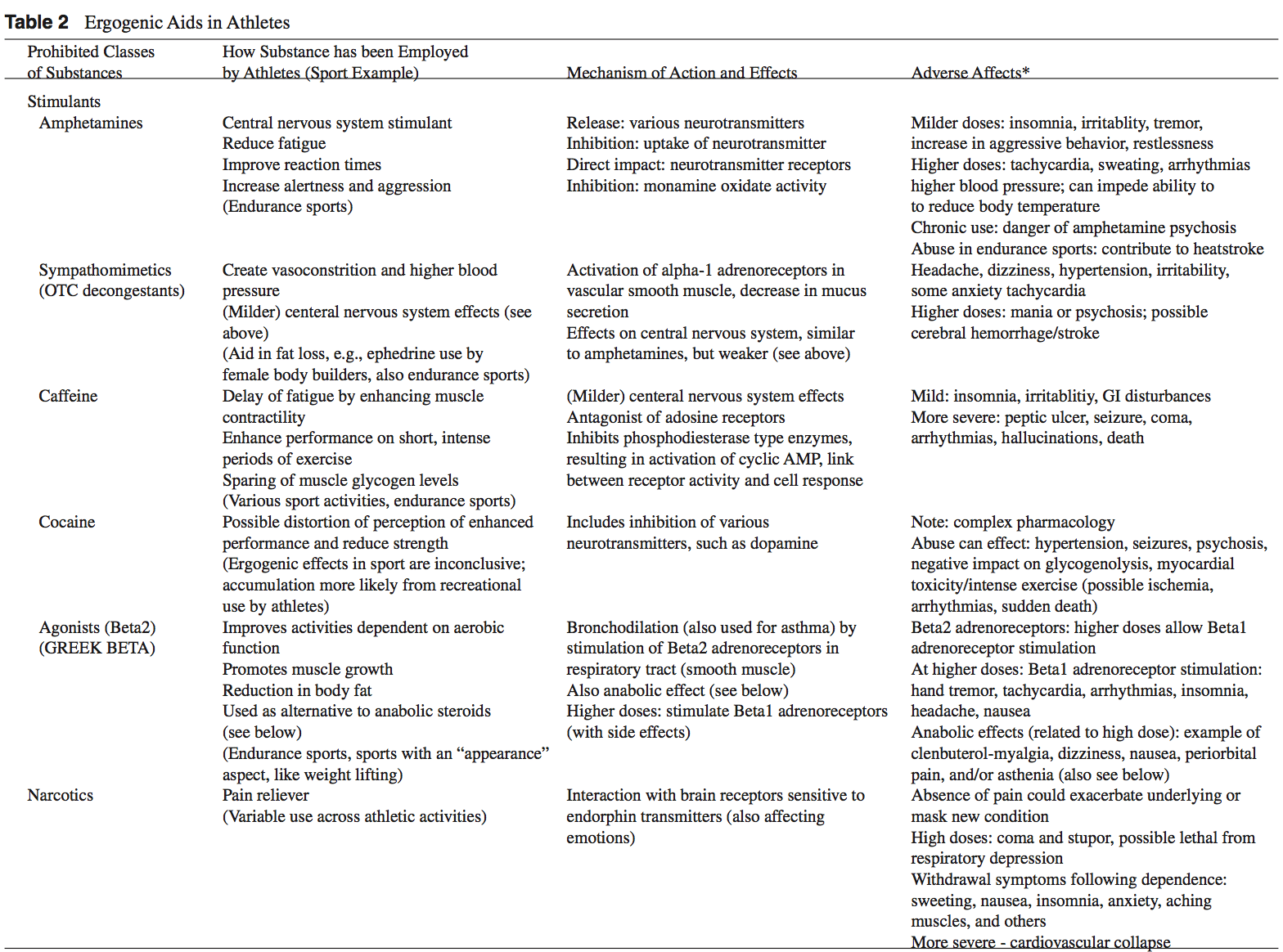
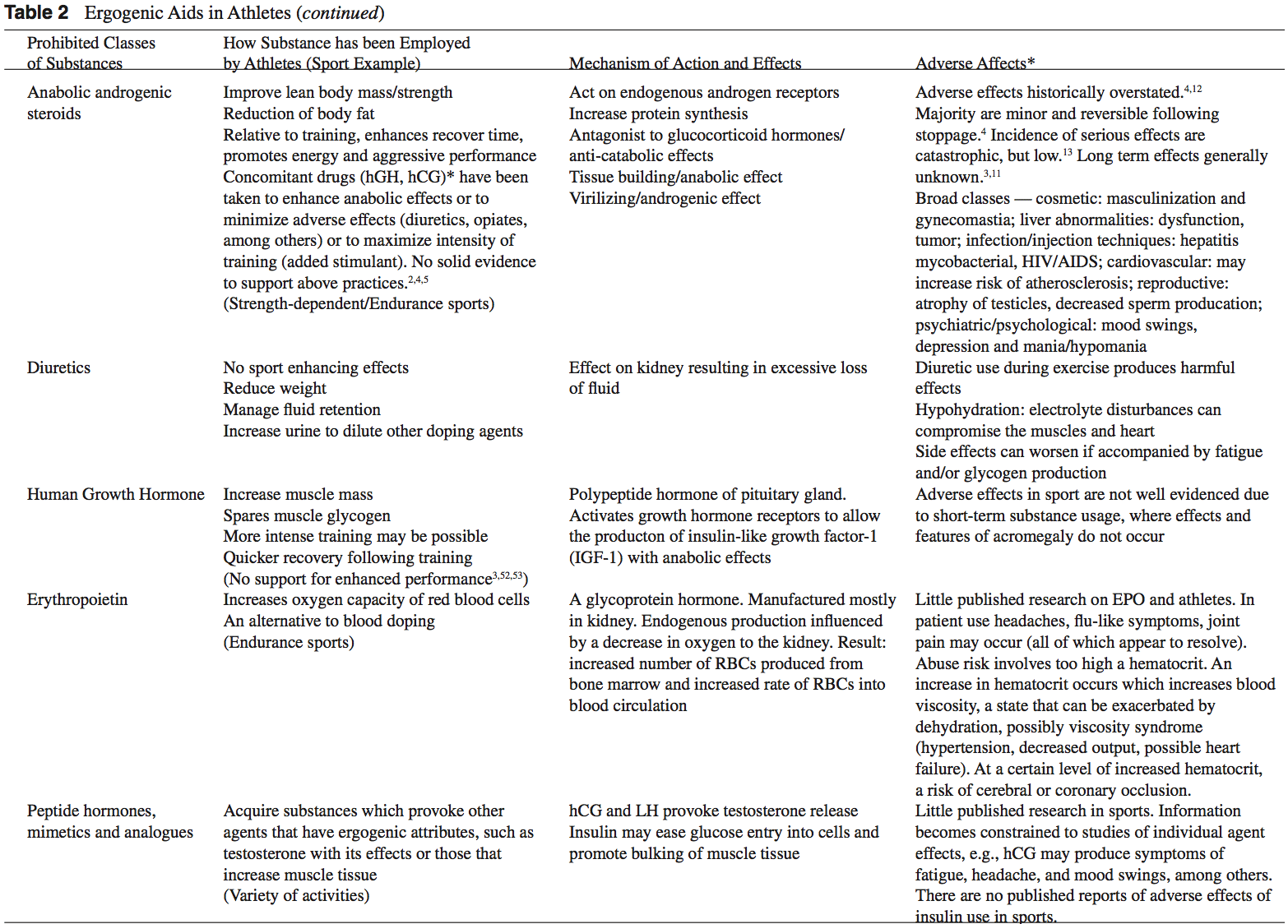 Anabolic-Androgenic Steroids
Anabolic-Androgenic Steroids Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3
Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3  Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15
Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15 Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19
Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19 The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter.
The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter. Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects.
Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects. Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36
Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36 Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50
Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50 Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3
Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3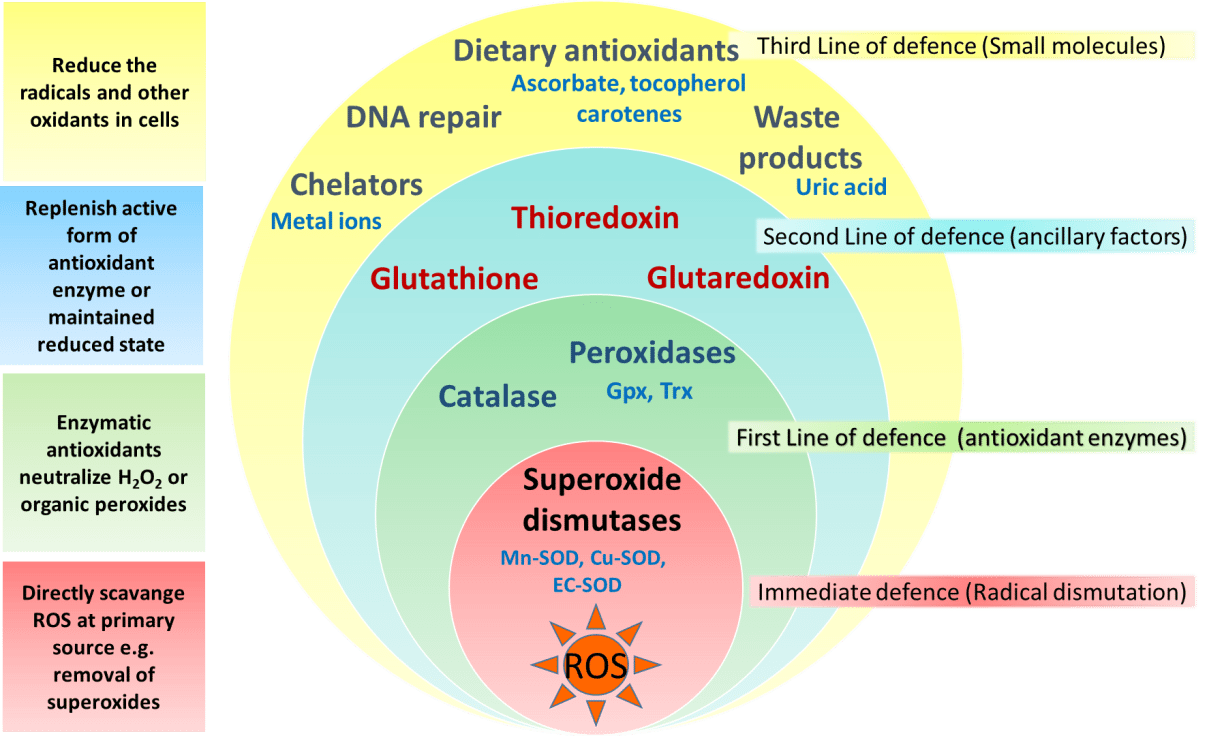 The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA).
The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA). Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61 Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6
Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6