Gardening is a favorite warm-weather activity for many people. Unfortunately, it can often send them straight to the chiropractor with back pain and stiffness. If you enjoy your garden but your back doesn�t take heart. An estimated�80% of the population has experienced back pain�or will experience it at some point in their lifetime.
It is common, but it doesn�t have to keep you from doing the things you enjoy. There are some fairly simple things you can do to make it easier and less painful.
Stretching is a good way to prevent back pain for nearly any activity. The more limber you are and the more warmed up your muscles are, the more comfortable you will be while you are gardening and afterward.
Stretches for gardeners�aren�t all that different from stretches for other activities. You need to address your hamstrings, triceps, and of course your back. Then you will be ready to get in the dirt and do what you love.
Use Back Friendly Tools and Gardening Methods
It may feel wonderful to get close to the dirt as you dig, breathing in its earthiness, feeling at one with nature, but your back likely does not hold the same appreciation. You can mix it up a little, but allow at least part of your gardening time to the use of tools that are �back friendly.�
Long handled and telescopic tools allow you to do your garden work without overworking your back. This is also great for people who don�t have full range of motion in their backs or who have trouble getting up and down.
Another back saver is a raised container garden. This will put your garden within easy reach, saving you from trying to get on the ground or, worse, feeling like you have to forego a garden because you can�t get around like you once did.
You can set the containers at whatever height you choose and include benches and seats for more comfortable gardening. If you do get on the ground, knee pads or a mat can help reduce some of the stress and prevent some pain.
Change Your Position Frequently
It�s easy to get in the zone and lose track of time, only for your body to remind you when you try to move and are met with painful stiffness. Carry a small timer with you and set it so that you are reminded every 30 minutes to stop, walk around, and stretch a little. This not only prevents pain and stiffness, but it also helps with your circulation and blood flow, even digestion.
You can also vary your garden tasks so that you don�t over-tax a single muscle group. You may weed for a while, then move to your potting bench for a while or pruning trees or shrubs. It isn�t good to stay in one position for too long no matter what you are doing. A physical activity like gardening, though, requires more movement.
Take Care when Bending, Reaching, and Lifting
Gardening involves a lot of reaching, bending, and lifting. When you don�t do it correctly you would wind up with a�sore back�� or worse.
To lift:�Don�t bend at your waist. Squat, grasp the object with both hands while pulling it close to your body. Straighten your legs slowly, letting those muscles to the work of lifting. You may also use a dolly, wheelbarrow, or wagon to move heavy items around and minimize the need to lift them.
Push:�Pushing doesn�t strain the back as much as pulling does. Push your seeder, wheelbarrow, and lawnmower and try to avoid pulling as much as possible.
Reaching:�Be careful when you reach, especially if you are reaching to lift. Even something that doesn�t weigh much can throw off your balance or cause you to twist your back. Try to minimize lifting while reaching as much as possible.
Bending:�Keep your knees soft when you bend and try bending from the waist. If you are doing a task that requires bending, take frequent breaks where you can stand upright. If you bend to lift, make sure you use proper lifting techniques.
Gardening can be wonderful for the mind, body, and spirit. It can also be painful if you don�t take the necessary precautions. When you go out to tend your plants, remember these back-saving gardening tips. Your back will thank you.
aka Spondylodiscitis and vertebral osteomyelitis overall are relatively infrequent and may present with bimodal distribution: children and adults >50’s
Occasionally considered as two separate entities due to variations in the blood supply of pediatric vs. adult spines
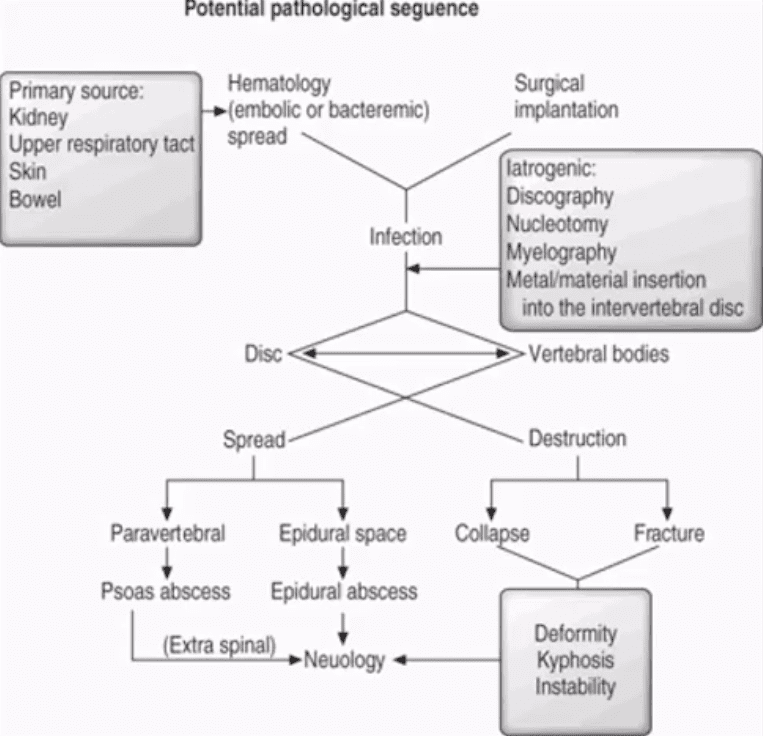
Risk factors/causes: distant site of infection in the body (25-35%), e.g., oropharynx, urogenital infections, bacterial endocarditis, indwelling catheters, florid skin infections furunculosis/abscess, etc.
Iatrogenic:�operative (e.g., discectomy) interventional or diagnostic/therapeutic procedures
Penetrating trauma
Immunocompromised patients
Diabetics
Malnourished patients or patients with low protein
IV drug users
Chronic disease patients, cancer patients etc.
Potential Pathological Sequence
Clinical Presentation
Back pain with or w/o high fever and other “septic” signs. Fever may only present in 50% of children
Exacerbation of pre-existing back pain in post-surgical cases
Neurological complications in advanced cases of vertebral destruction and epidural abscess
Meningitis, septicemia etc.
Labs: Blood tests are unspecific, may or may not indicate elevated ESR/CRP, WBC
Diagnostic imaging is important but
If clinical suspicion is strong, prompt I.V. antibiotics are needed to prevent serious complications
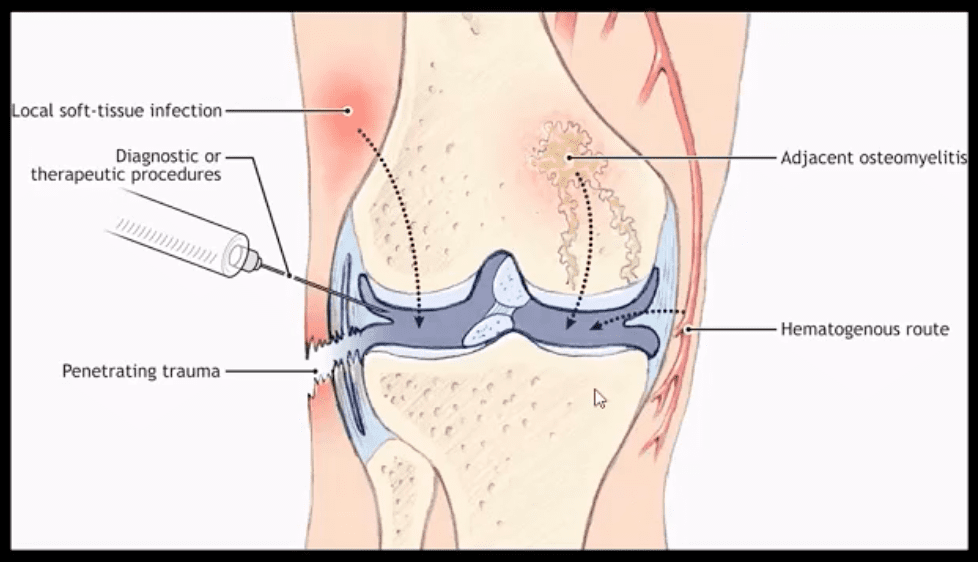
Routes of Infection
Infection routes to the spine are similar to bone in general
3-distinct routes:
1) Hematogenous spread as bacteremia (most common)
2) Adjacent site of infection (e.g., soft tissue abscess)
3)Direct inoculation (e.g., iatrogenic or traumatic)
M/C organism Staph. Aureus
Mycobacterium TB (tuberculous spinal osteomyelitis) aka Pott’s disease can be presented in cases of re-activated or disseminated pulmonary TB
Mechanisms of Spinal Infection
May vary depending on the patients’ age
In children, the IVD receives direct blood supply and can be infected directly spreading to adjacent bone and causing spondylodiscitis
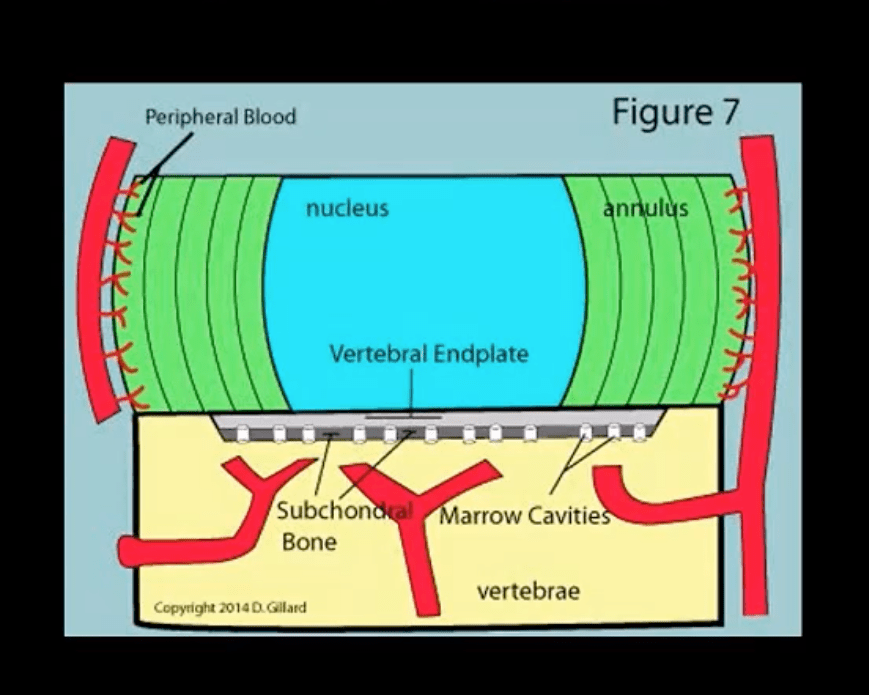
In Adults
The disc is avascular
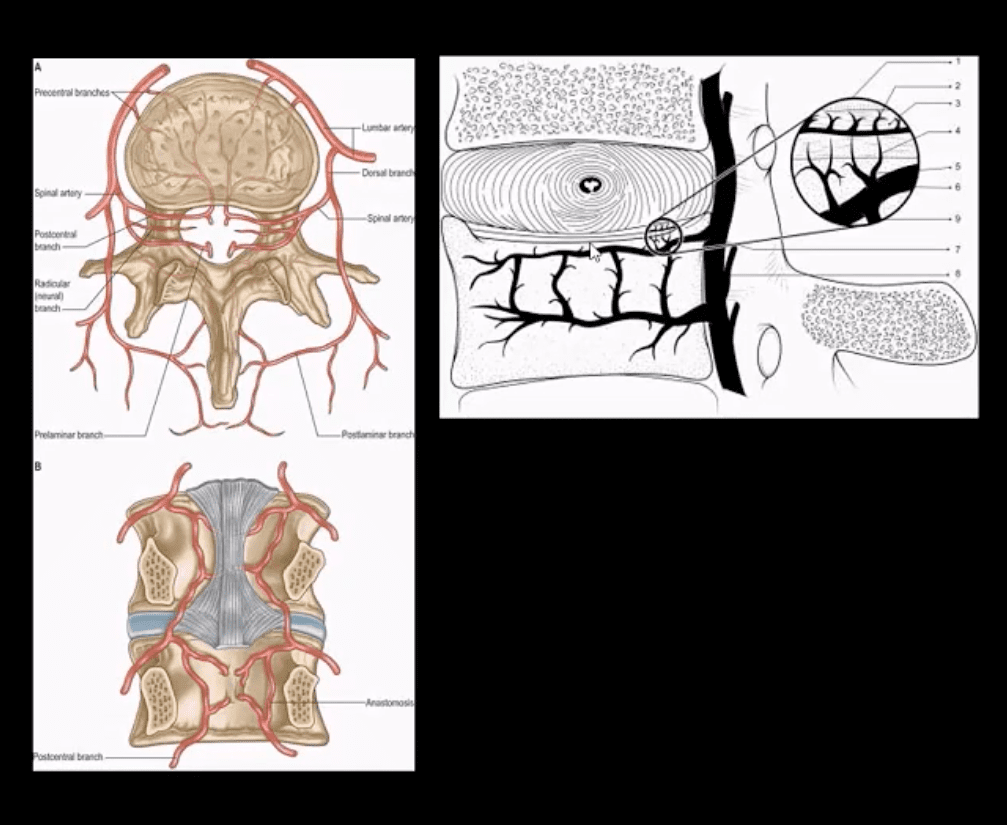
Pathogens invade adjacent vertebral end-plates via end-arterial supply of the vertebral body that may facilitate infection due to slow, turbulent flow
Organisms may then quickly gain access to disc substance rich in nutrients (discitis) often w/o significant initially visible destruction to the bone
Thus, one of the earliest rad. findings of spinal infection or sudden reduction of disc height
Later end-plate irregularity/sclerosis may develop, subsequently affecting the entire adjacent vertebral bodies
Diagnostic Imaging
Initially, in most cases of MSK complaints, radiography is the 1st imaging step
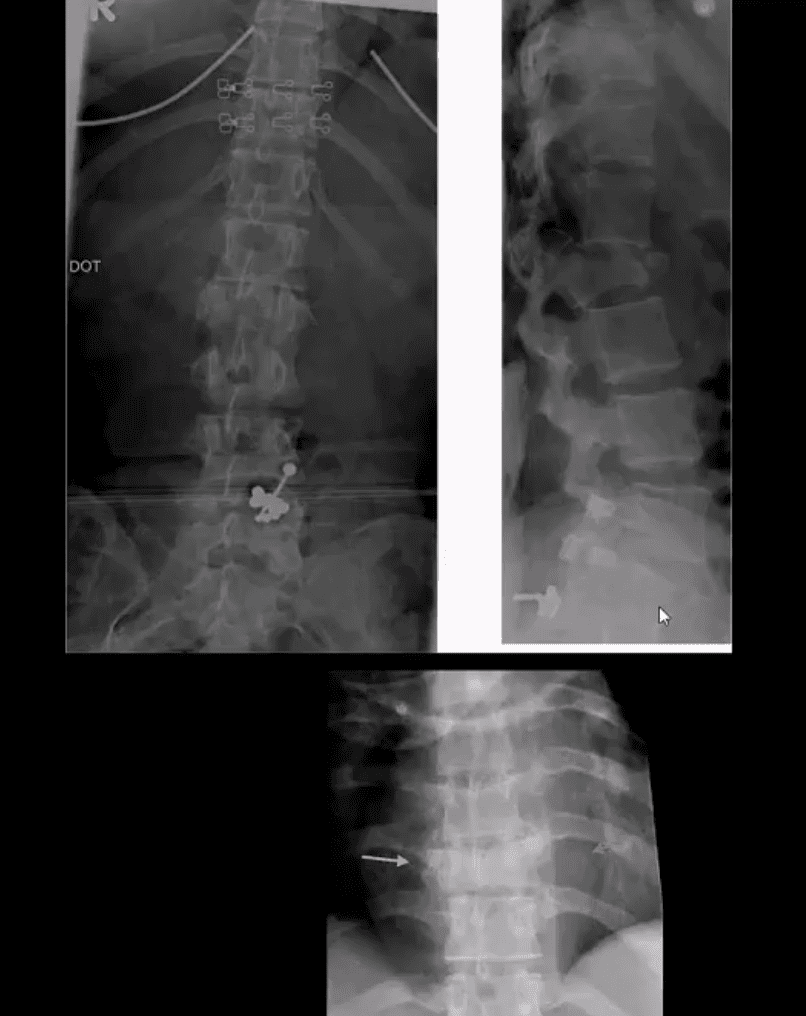
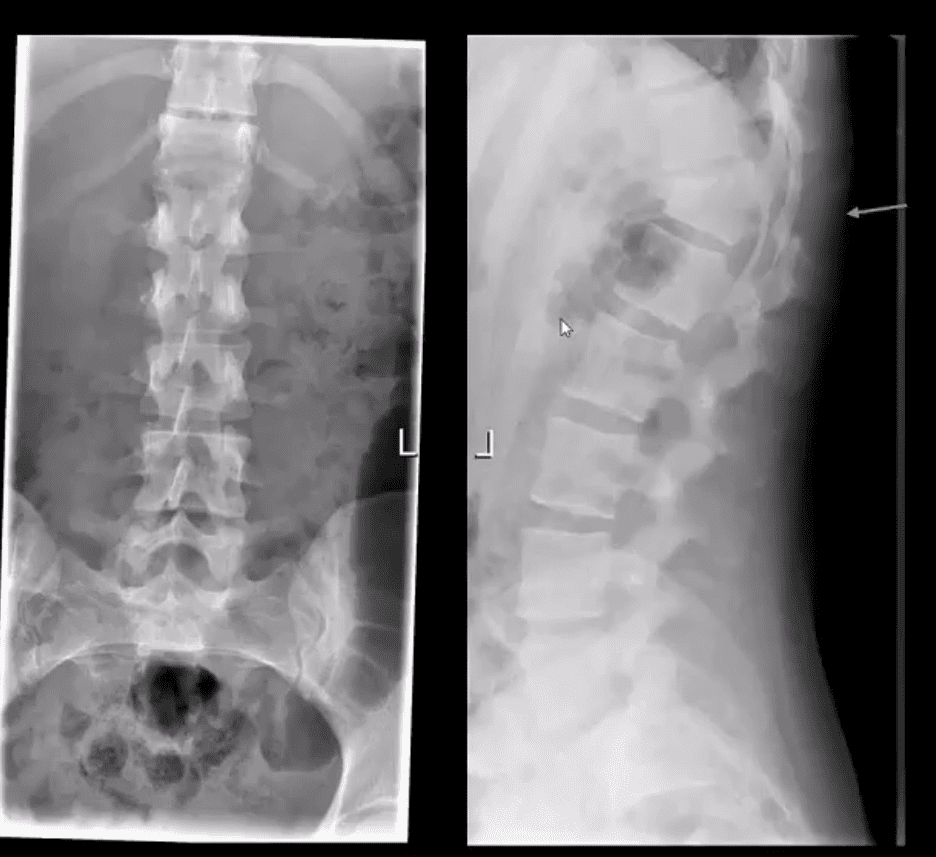
Initially, X-radiography is often unrewarding and may appear unremarkable for 7-10 days or presents with some subtle soft tissue changes (e.g., obscuration of Psoas shadows etc.)
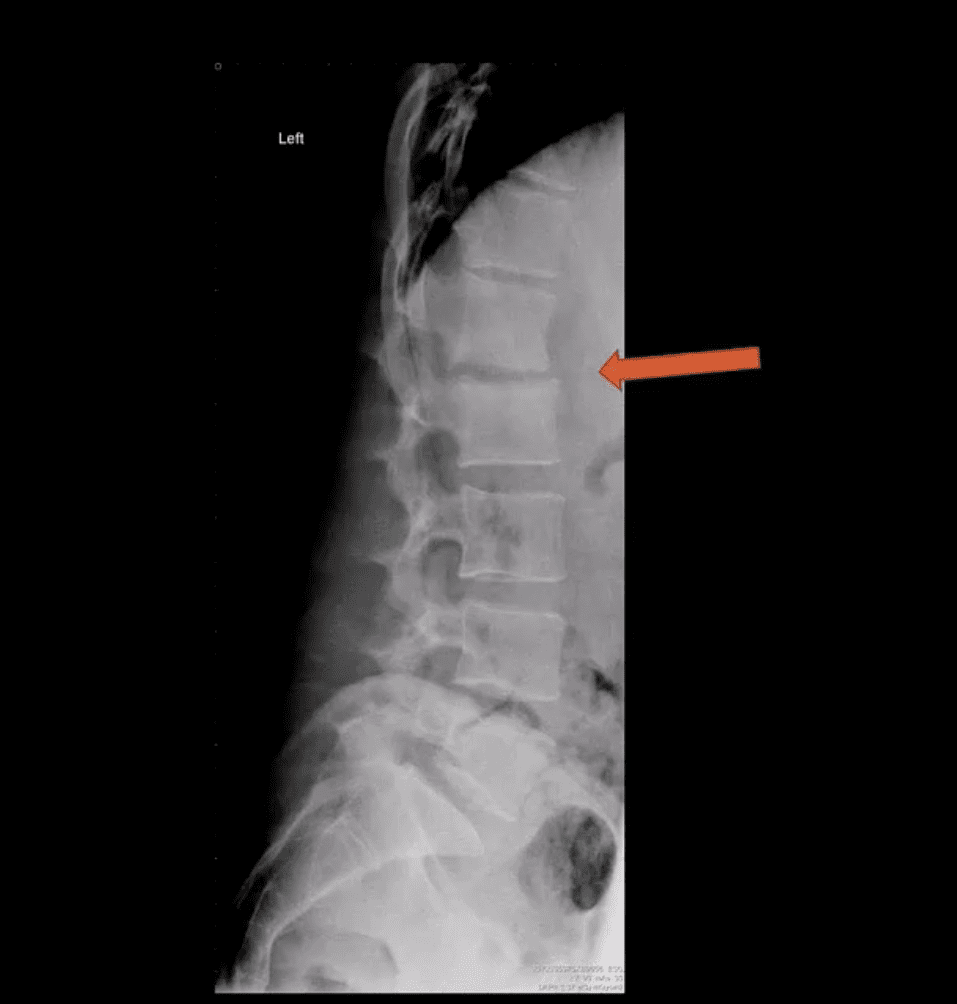
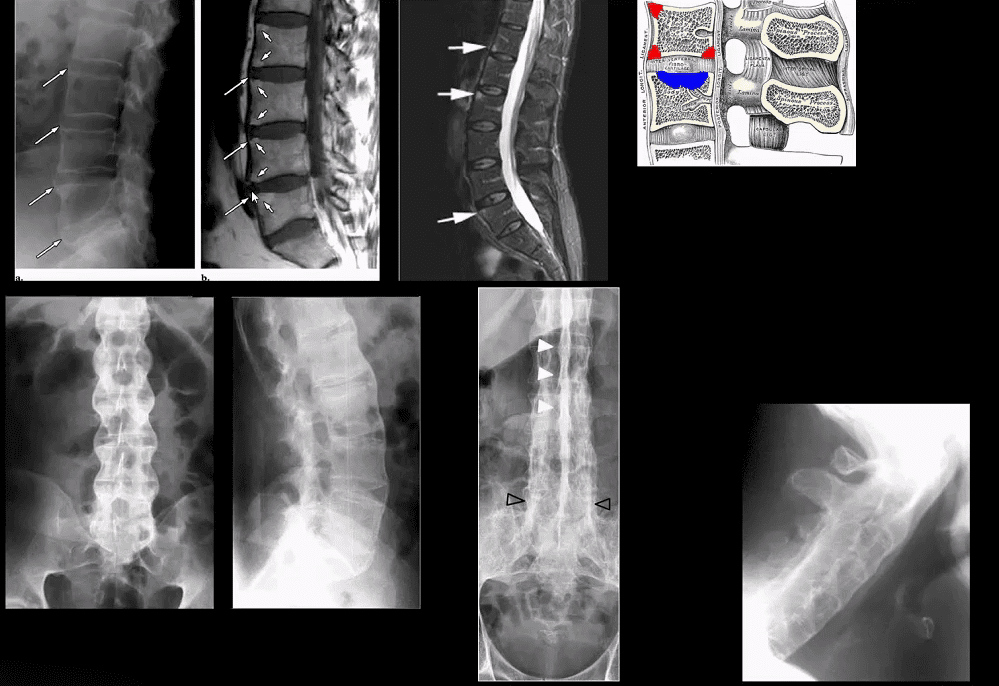
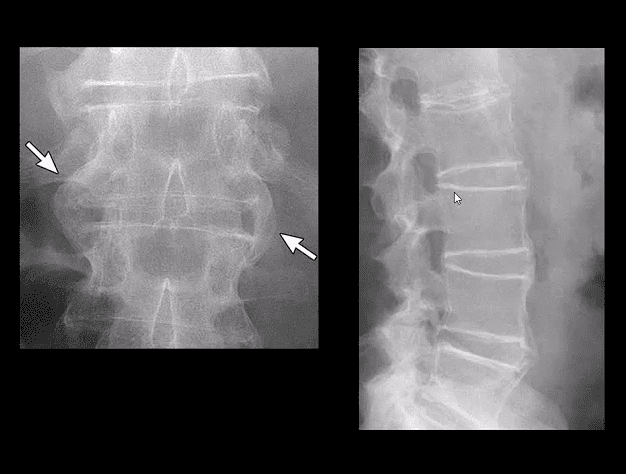
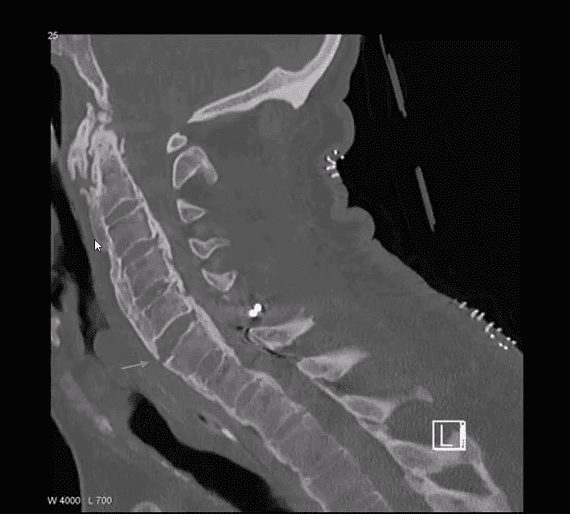
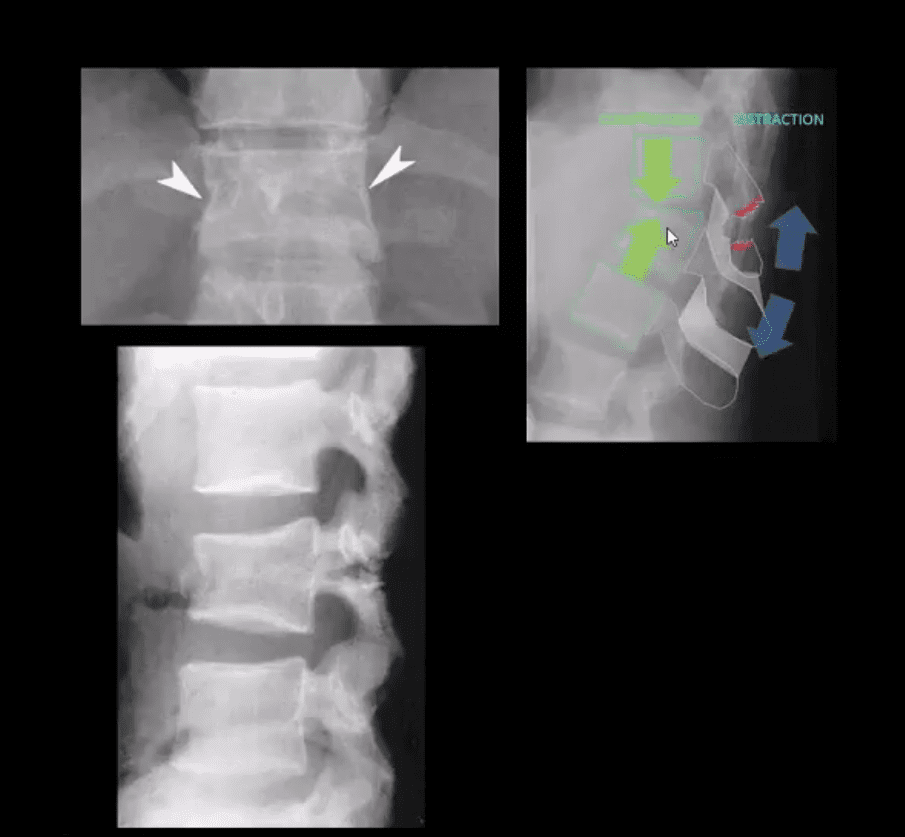
Some of the earliest x-ray signs of pyogenic spondylodiscitis: sudden reduction of disc height (above arrow) during initial 7-10 days
Subsequently (10-20 days) some end-plate irregularity and adjacent sclerosis may be noted
In more advanced cases, subsequent vertebral destruction and collapse may occur
N.B. Reliable feature to DDx between spinal infection and metastasis is the preservation of disc height in the latter
Note:�sudden disc narrowing with no appreciable spondylosis (above the first image) is suspicious for infection (discitis)
MRI +C is required to evaluate suspected infection
N.B. 50-60% of pyogenic spondylodiscitis occur in the lumbar region
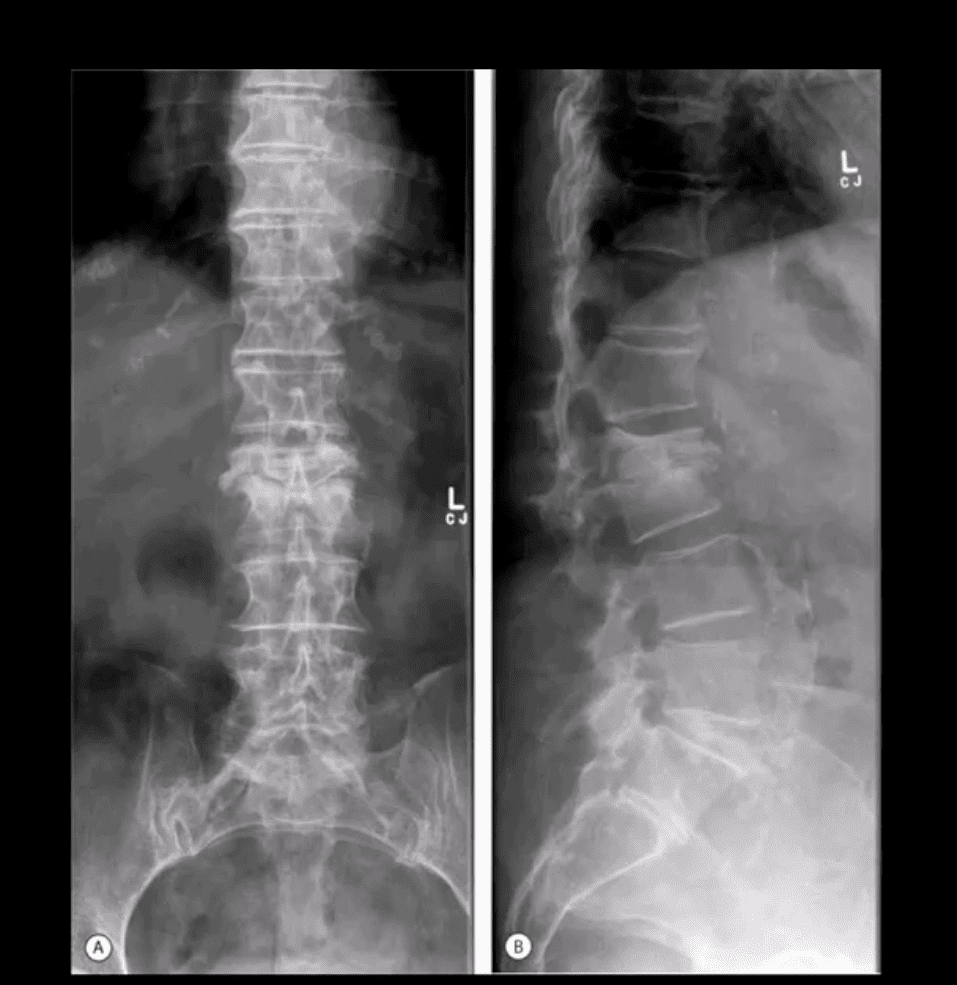
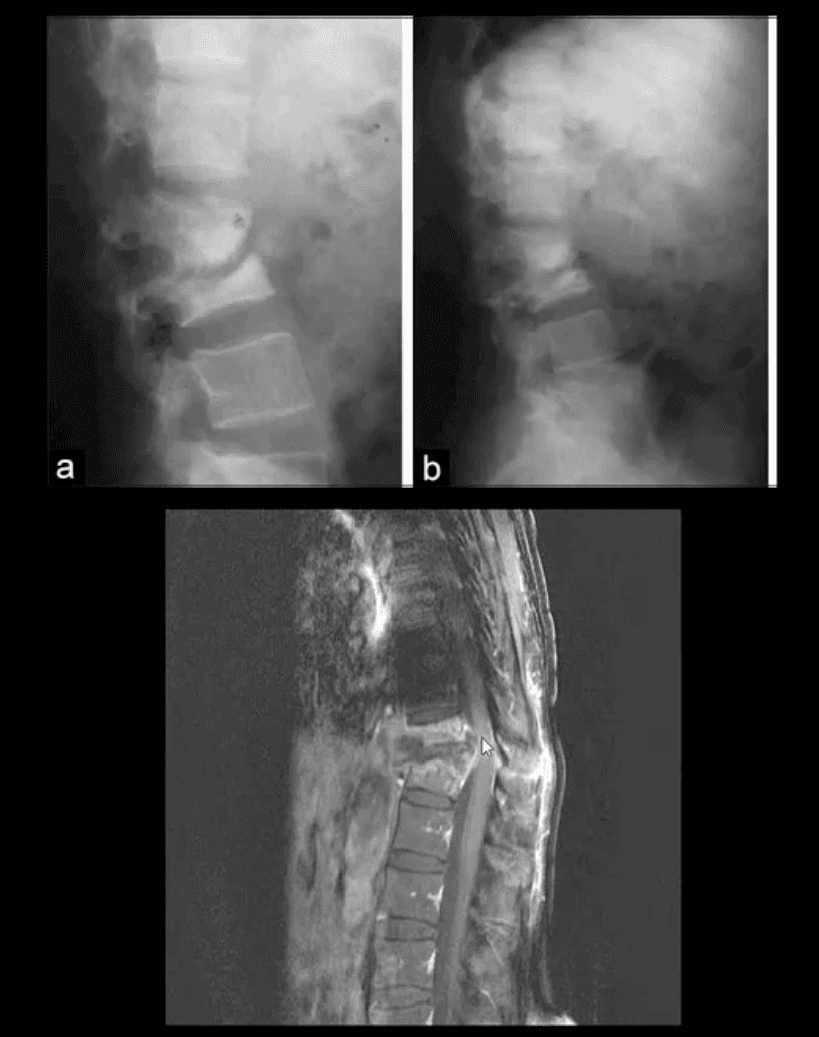
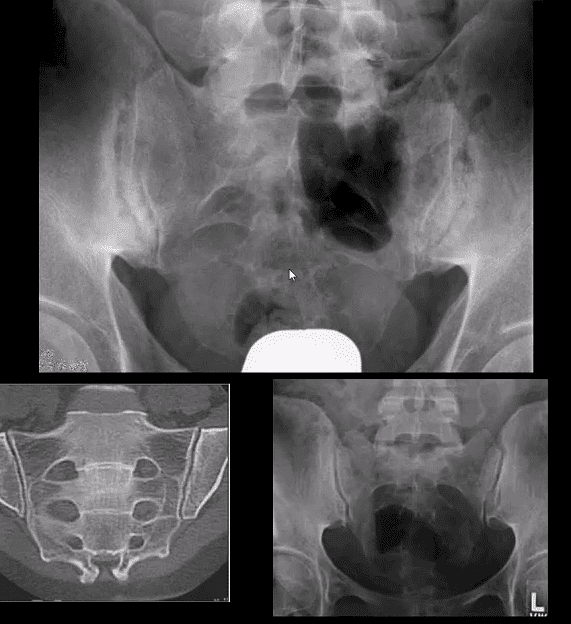
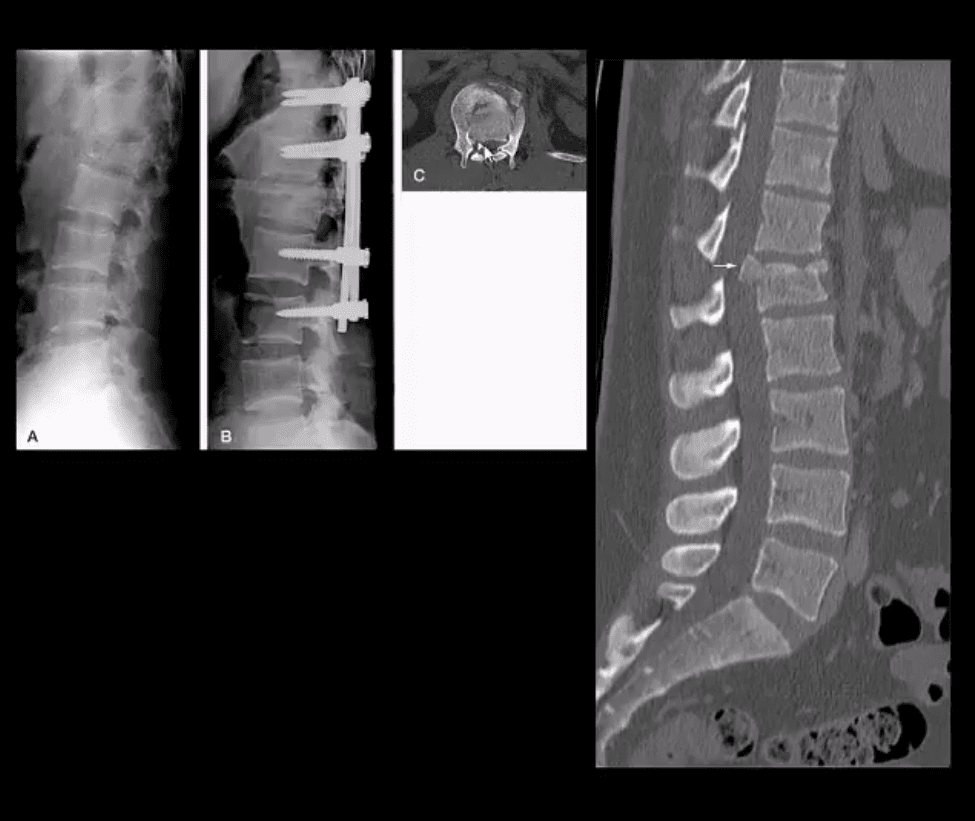
AP & Lateral Lumbar Radiographs
Note severe disc narrowing and adjacent vertebral body destruction at L1-L2 in a 68 -y.o.-female with a known Hx of type 2 DM
Additional imaging modalities should be used to support the Dx
Final Dx: Pyogenic Spondylodiscitis
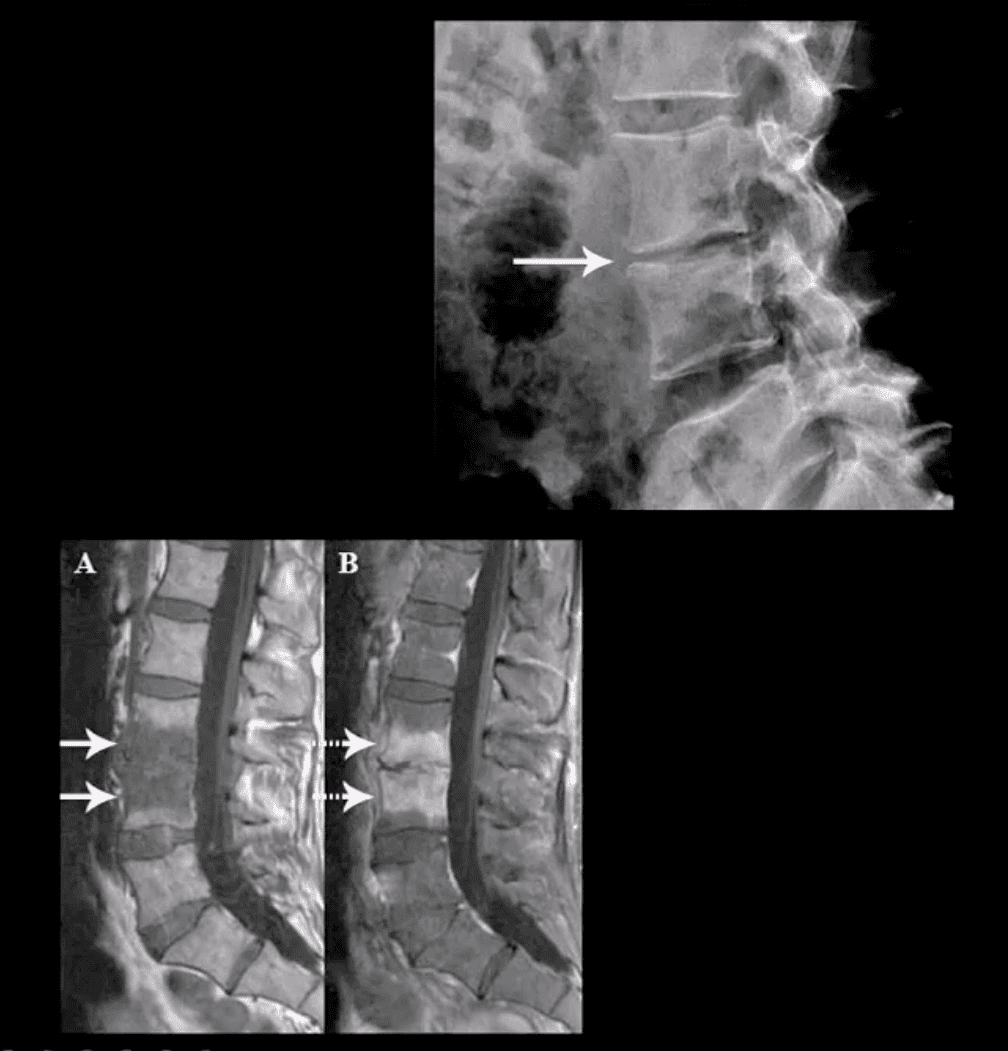
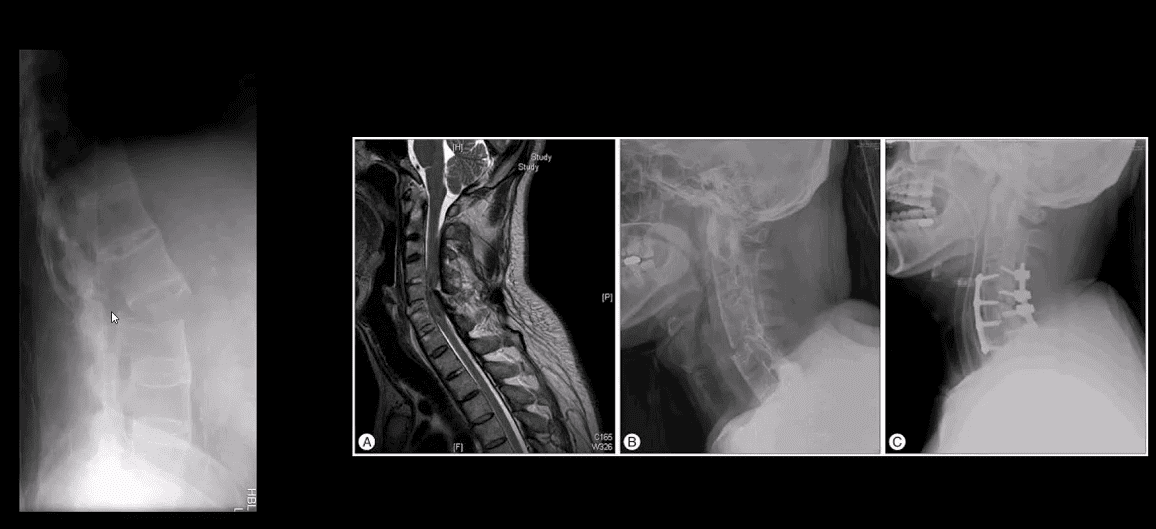
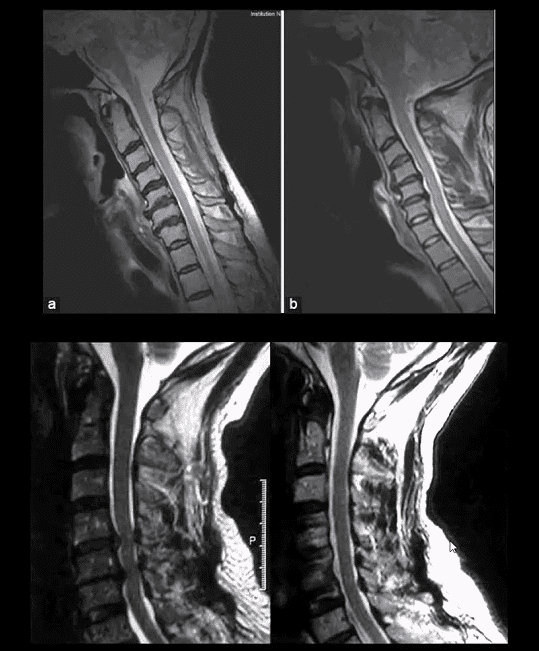
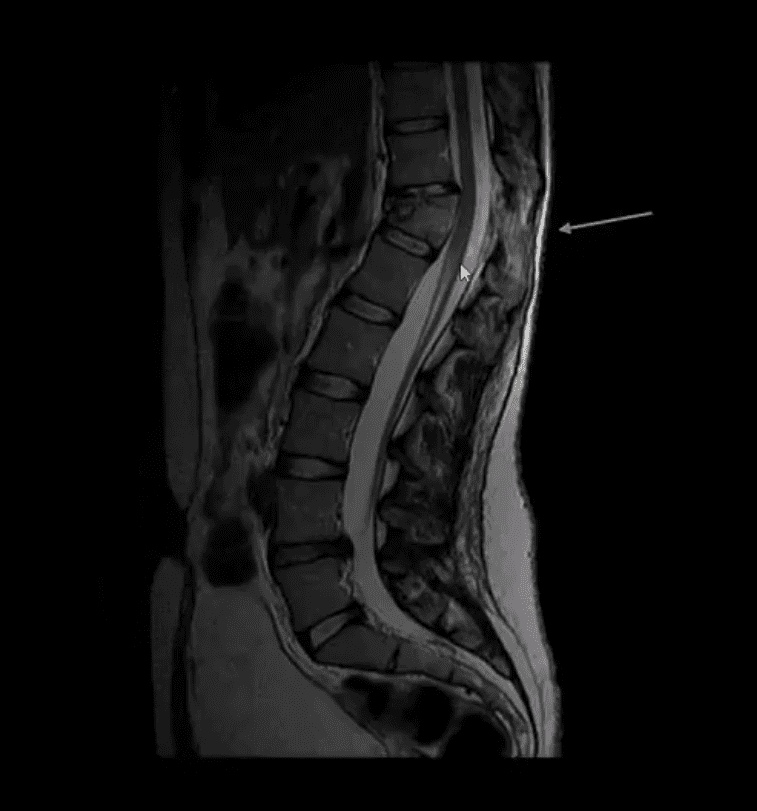
Sagittal T1 & T2 MRI
Weighted MRI slices of a patient who had laminectomy at L4
MR imaging with gad contrast is the modality of choice for Dx of spinal infection
Early septic changes affecting the disc and adjacent vertebral end-plates are readily demonstrated as a low signal on T1 and high T2/STIR d/t edema and inflammation
T1 FS +C gad images show avid enhancement of the lesion due to granulation tissue around the phlegmon. Peripheral enhancement is also characteristic of an abscess.
Epidural extension/abscess can also be successfully detected my MRI
N.B. 50% of epidural abscess cases present with neurological signs
STIR & T1 FS +C Gad Sagittal MRI
Marked septic collection and edema affecting L4-5 disc and vertebral body with some epidural extension and paraspinal soft tissue edema. Avid contrast enhancement is noted surrounding low signal foci within the bone and disc tissue, some gad. Enhancement is noted in posterior paraspinal muscles and dural spaces
Management: Dx of spondylodiscitis requires prompt I.V antibiotics. If instability and neurological complications develop referral to a Neurosurgeon is required
MRI Unavailable or Contraindicated
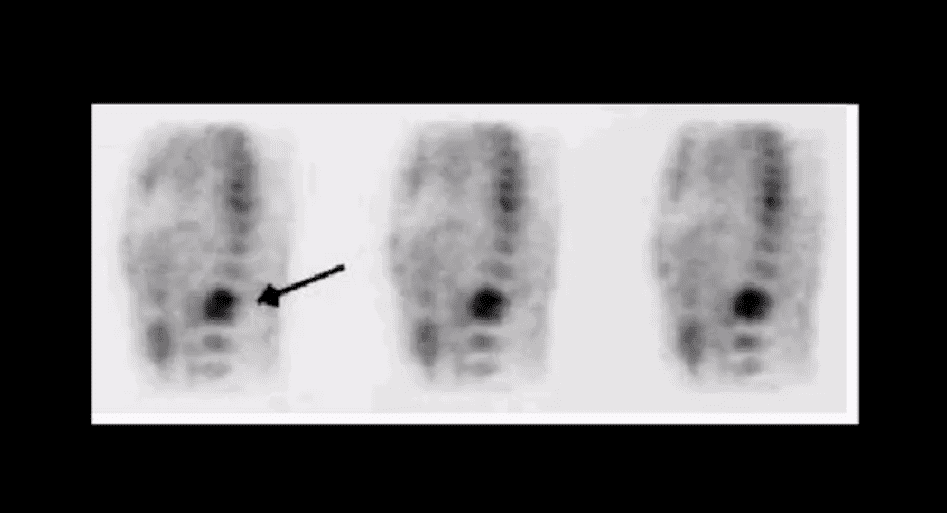
Bone scintigraphy is very sensitive but non-specific for spinal infection but overall is of great value d/t higher sensitivity than x-rays and relatively low cost.
An area of increased flow with radiopharmaceutical uptake is characteristic but not specific sign of spondylodiscitis
If neurological signs are present and MRI is contraindicated than CT myelography may be used
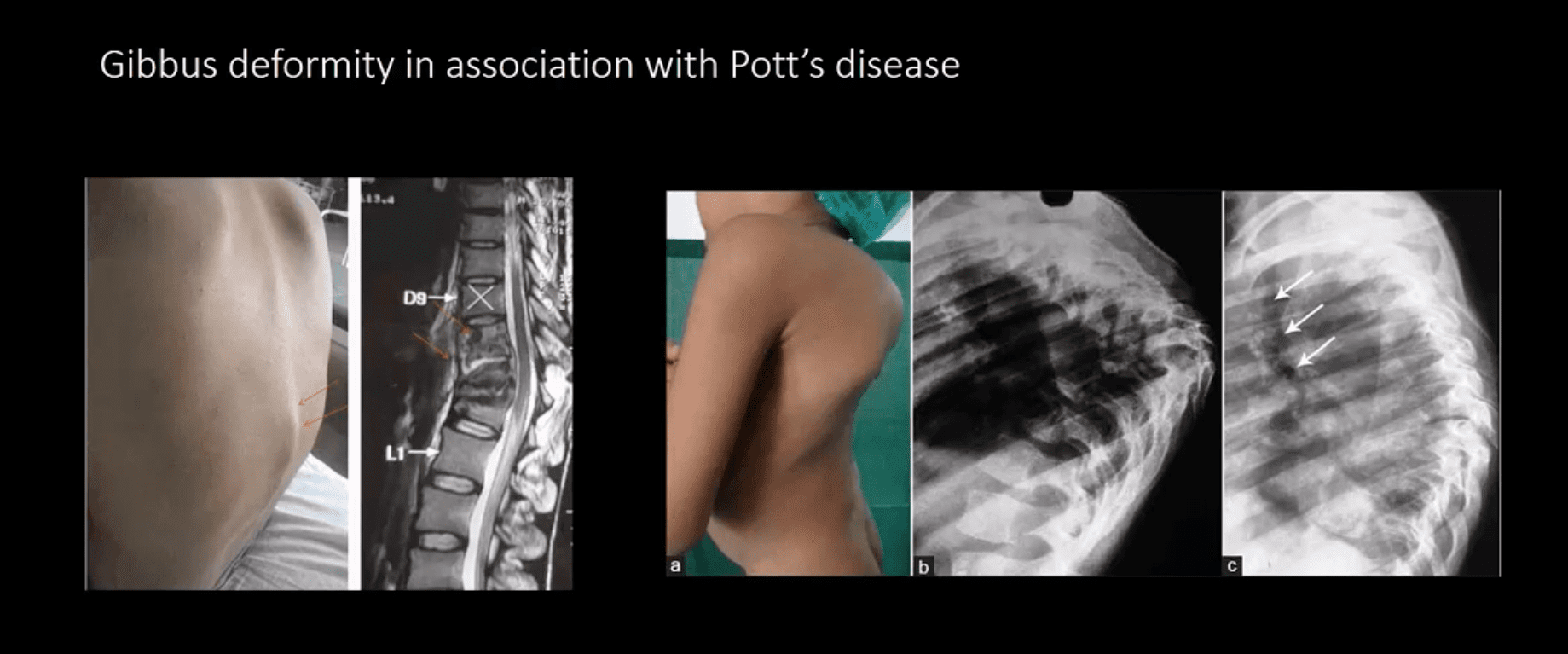
TB Osteomyelitis aka Pott’s Disease
TB osteomyelitis is increasing d/t HIV and other immunocompromised states. Extrapulmonary TB m/c affects the spine and especially the thoracic spine (60%)
Radiographic Pathology:�TB bacillus infects the vertebral body and often spreads subligamentously. “Cold” paraspinal abscess collection may develop and spreads along fascial planes, e.g., Psoas abscess. Disc spaces are preserved until v. late and skip areas are noted helping to DDx TB from pyogenic infection. Severe vertebral destruction aka Gibbus deformity may develop (>60-degree sometimes) and may become permanent. Neurologic and many regional complications may develop
Imagingapproach:�CXR with spinal x-rays 1st step that may be unrewarding but may potentially reveal VB destruction w/o disc narrowing. CT scanning is more superior than x-rays. MRI with gad C is a modality of choice
The vast majority of clinically suspected bone Mets are found in the axial skeleton and proximal femurs/humeri
Radiography is the most cost-effective and readily available initial imaging tool to investigate bone Mets but often fails early metastatic detection
Tc99 bone scintigraphy is the most sensitive and cost-effective imaging modality to demonstrate metastatic foci
MR imaging may help� regional identification of bone Mets especially if x-radiography is unrewarding
Significant limitations of MRI: inability to perform a whole-body MRI scan
Cost and other contraindications such as cardiac pacemakers and cochlear implants may be another limiting factor
Marrow Based Neoplasms
Malignancy originating from the marrow cells are often referred to as “round-cell tumors.”
Multiple Myeloma (MM)
Lymphoma
Ewing’s sarcoma
The last two are less frequent than MM
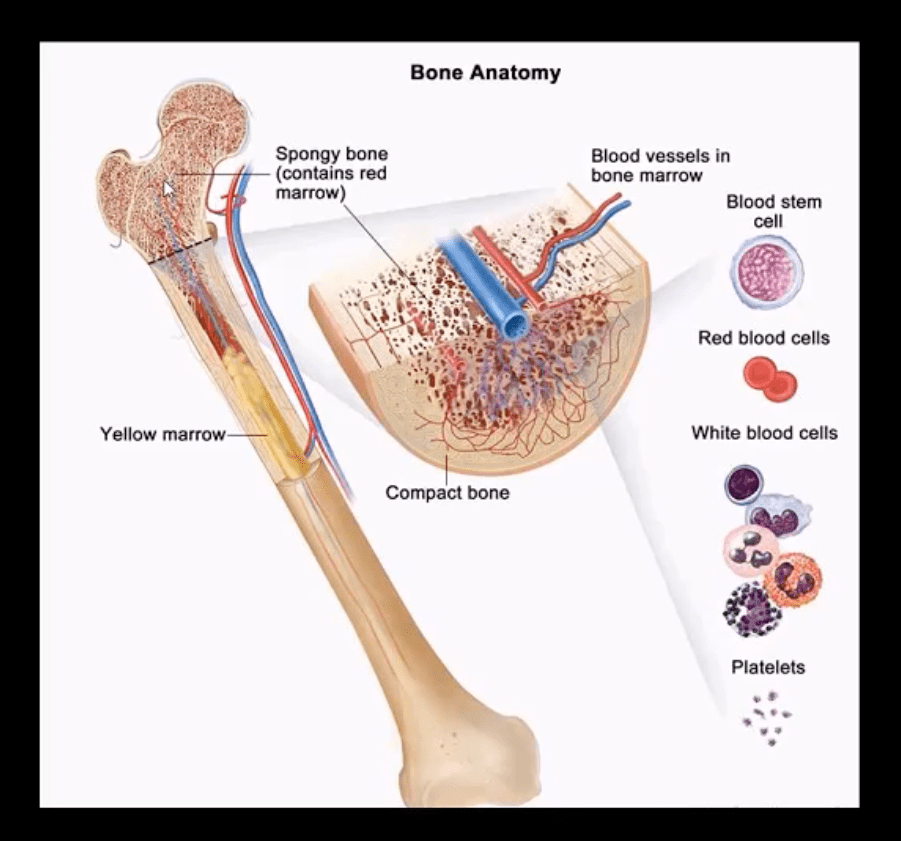
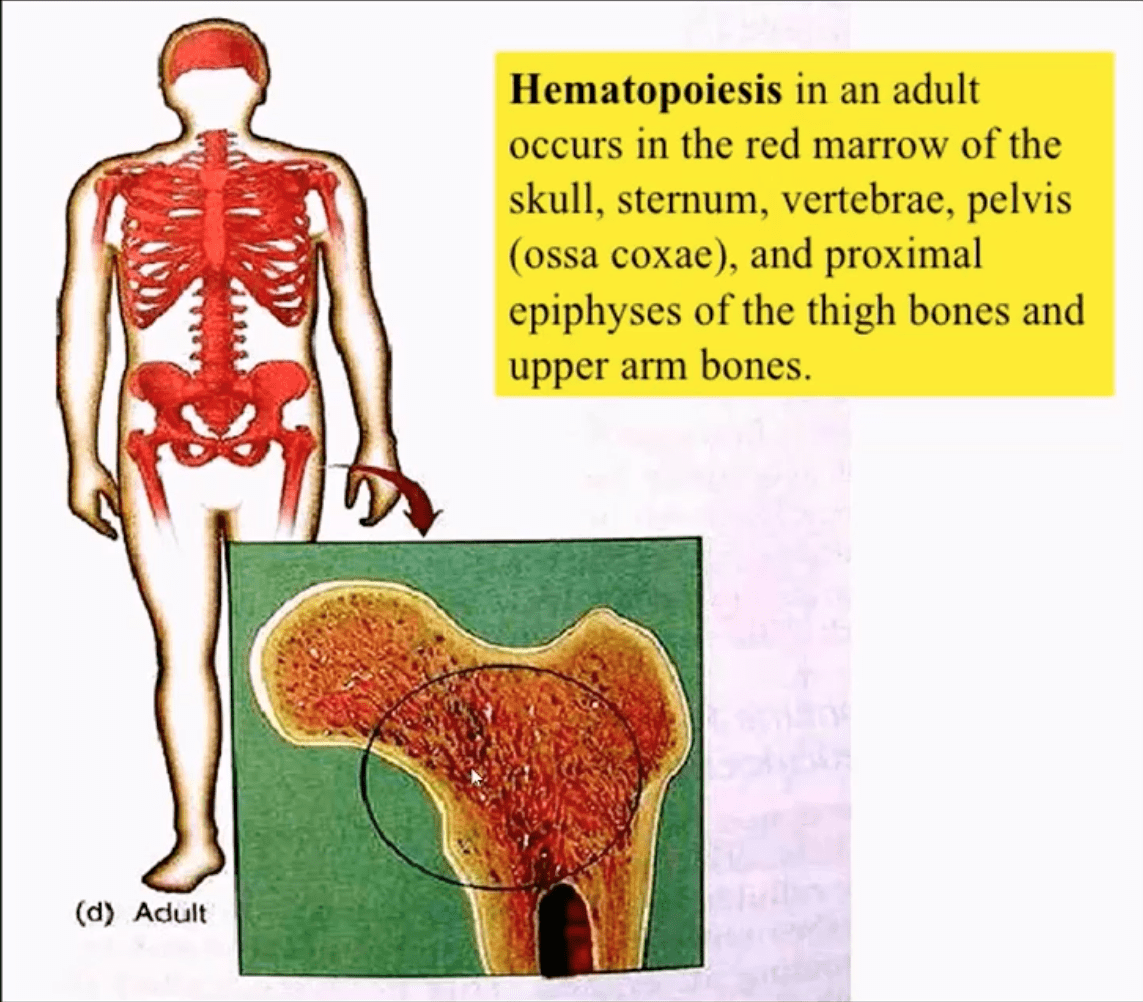
Red marrow in adults is in the axial skeleton and proximal femurs/humeri d/t gradual marrow “retraction” following the childhood
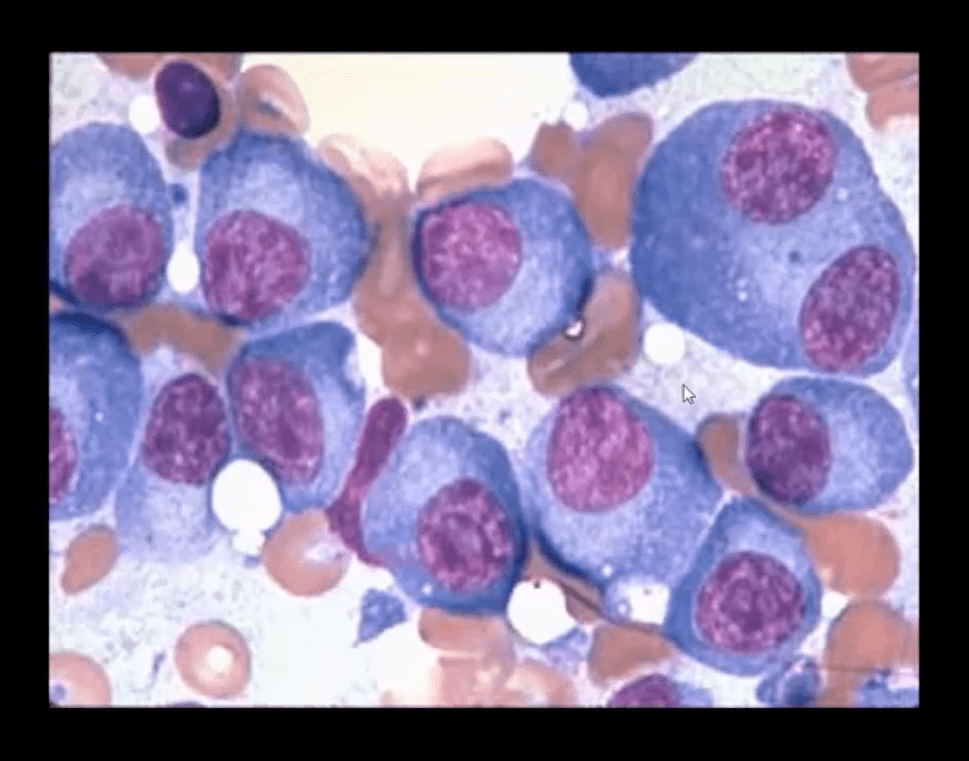
Note bone marrow biopsy histopathology specimen of MM with abnormal plasma cells replacing regular marrow residents (above image)
Multiple Myeloma (MM) is the most common primary bone neoplasm in adults>40s. Etiology is unknown, but many theories exist (e.g., genetic, environmental, radiation, chronic inflammation, MGUS)
MM: malignant proliferation of plasma cells >10% of red marrow, with subsequent replacement of normal marrow cells by myeloma cells and overproduction of monoclonal antibodies paraproteins (M protein) with heavy chains IgG (52%), IgA (21%), IgM (12%) and light chains kappa or lambda aka Bence-Jones proteins
Clinical Presentation of MM
MM is occasionally detected as unexplained anemia on routine blood studies for unrelated complaints
Common MSK symptoms: Bone pain/Pathologic fractures
Diagnostic imaging plays an essential role during the Dx of MM
Bone marrow aspiration biopsy, blood tests, and serum protein electrophoresis may be used
Imaging approach: bone pain is investigated with initial x-radiographs if radiographs are unrewarding MR imaging may help to reveal bone marrow abnormality. MRI is recommended as myeloma survey
Currently, MRI protocol known as “whole body myeloma scan” consisting of T1, T2-fat suppressed, and T1+C coronal sequences can detect MM in the skull, spine, pelvis, ribs and femurs/humeri. This technique is much more superior to radiographic “skeletal myeloma survey.”
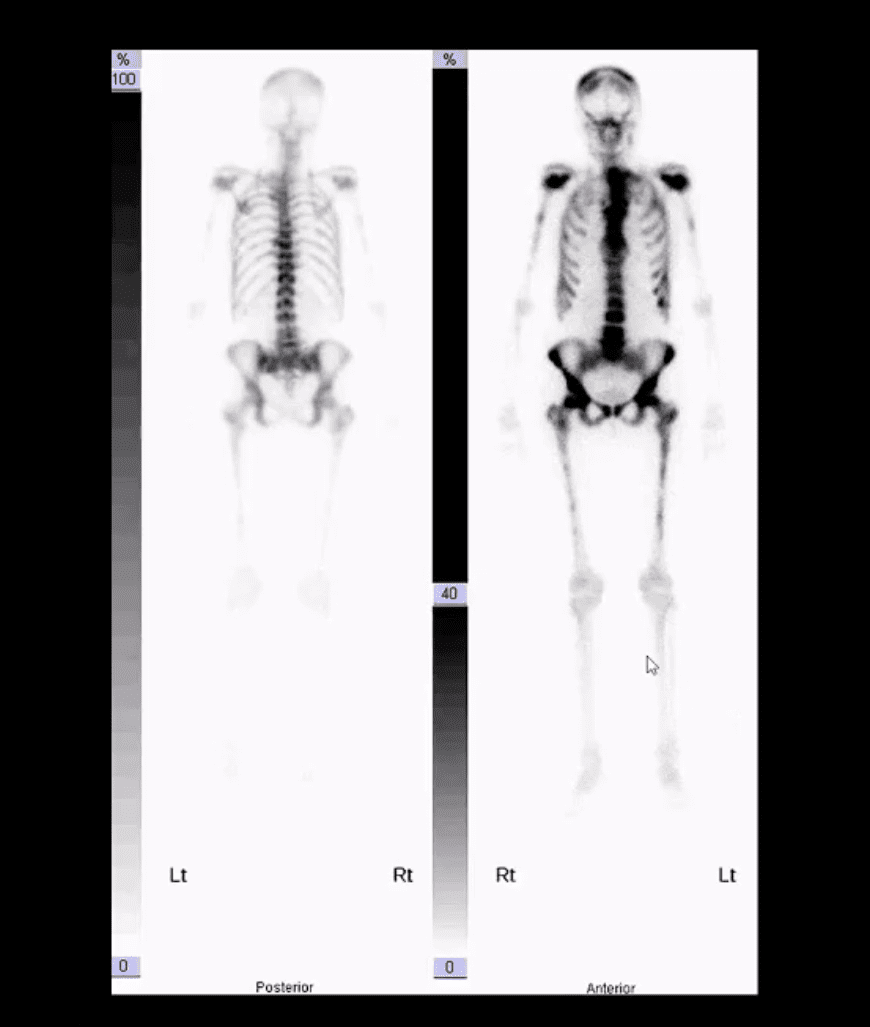
Tc99 bone scintigraphy is not typically used for MM because over 30% of MM lesions are “cold” or photopenic on radionuclide bone scan d/t highly lytic nature of MM with osteoclasts outpacing osteoblasts.
A radiographic skeletal survey is considered more sensitive than bone scintigraphy in MM
PET-CT scanning of MM is gaining popularity due to the high level of detection of multiple sites of MM
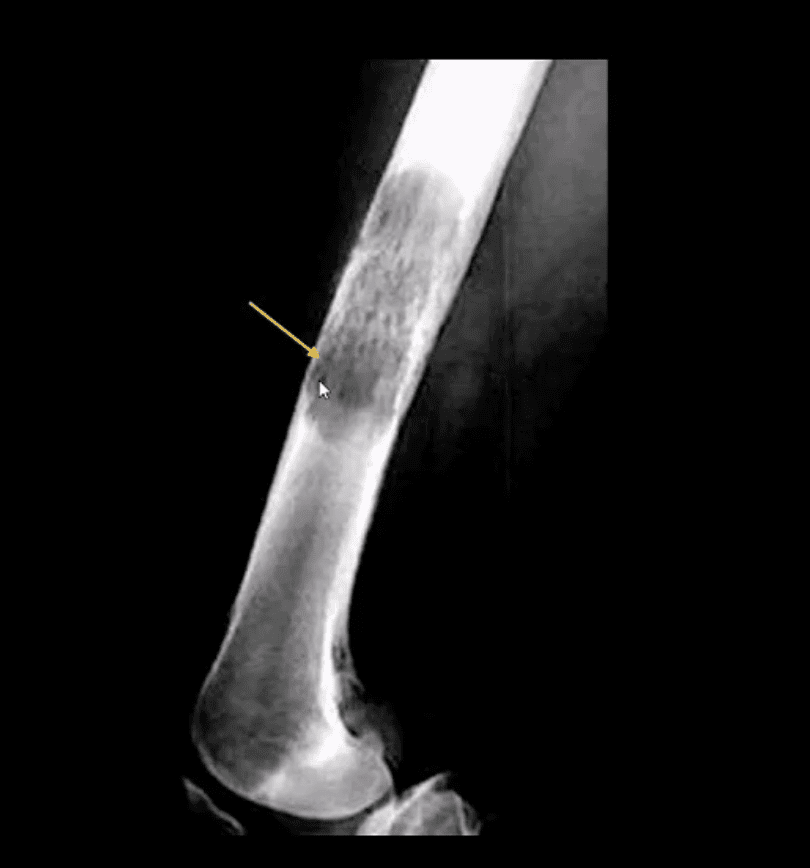
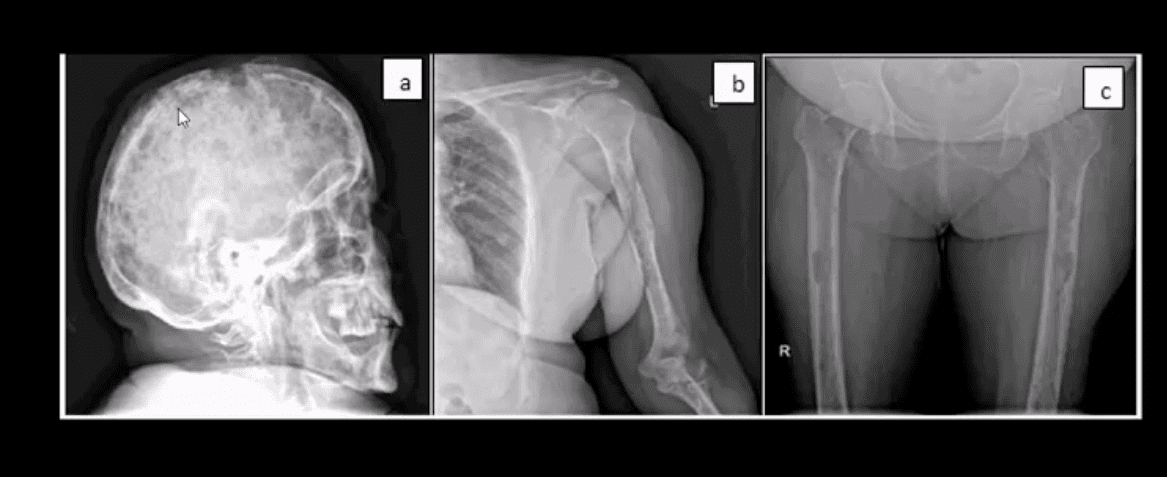
Radiographic Dx of MM: consists of identification of characteristically localized focal osteolytic “punched out” or “moth-eaten” lesions of variable sizes following the distribution of adults red marrow
Note rad abnormality is known as “raindrop skull” is characteristic of MM
Radiographic appearance of MM may vary from “punched out” round radiolucencies to “moth-eaten” or permeating osteolytic lesion producing endosteal scalloping (yellow arrow)
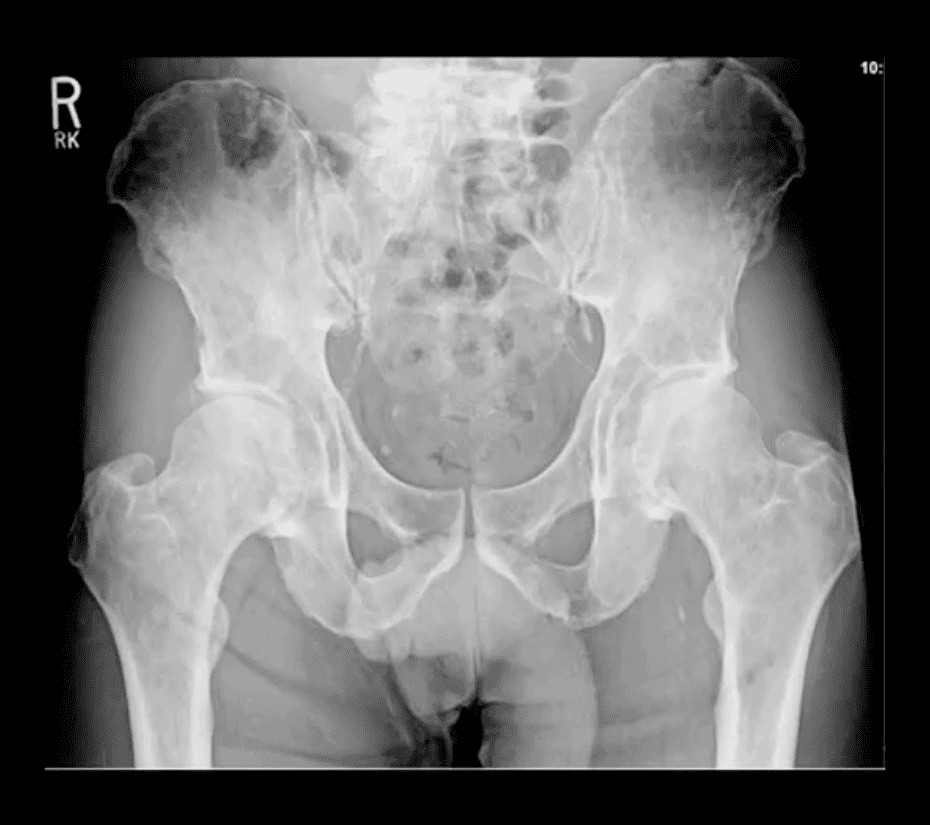
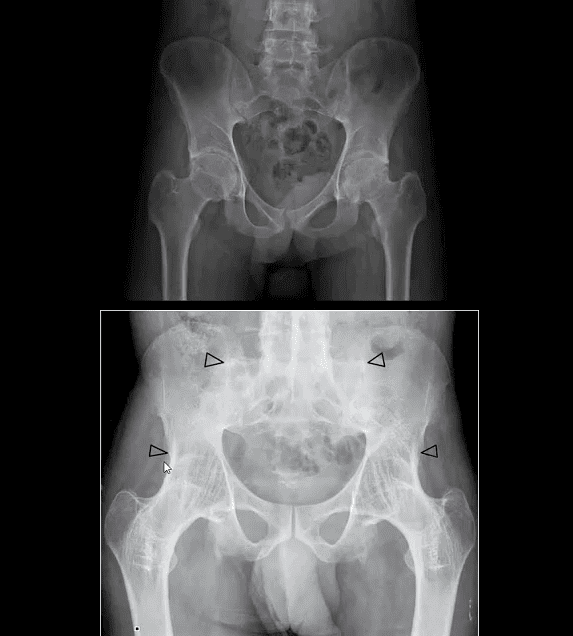
Pelvis and femurs are commonly affected by MM and present radiographically as round lytic punched out or moth-eaten lesions
N.B. Occasionally MM may pose radiographic dilemma by presenting as generalized osteopenia in the spine that can be difficult to differentiate from age-related osteoporosis
MR imaging of MM reveals� marrow changes with low signal on T1, a high signal on fluid-sensitive sequences and bright contrast enhancement on T1+C gad d/t increased vasculature and high activity of� MM cells
Example of full-body MRI of “whole body myeloma scan” with T2-fat suppressed (A), T1 (B) and T1+C (C) pulse sequences produced in coronal slices
Note multiple foci of bone marrow changes in the spine pelvis and femurs
Miscellaneous Neoplasms of the Spinal Column
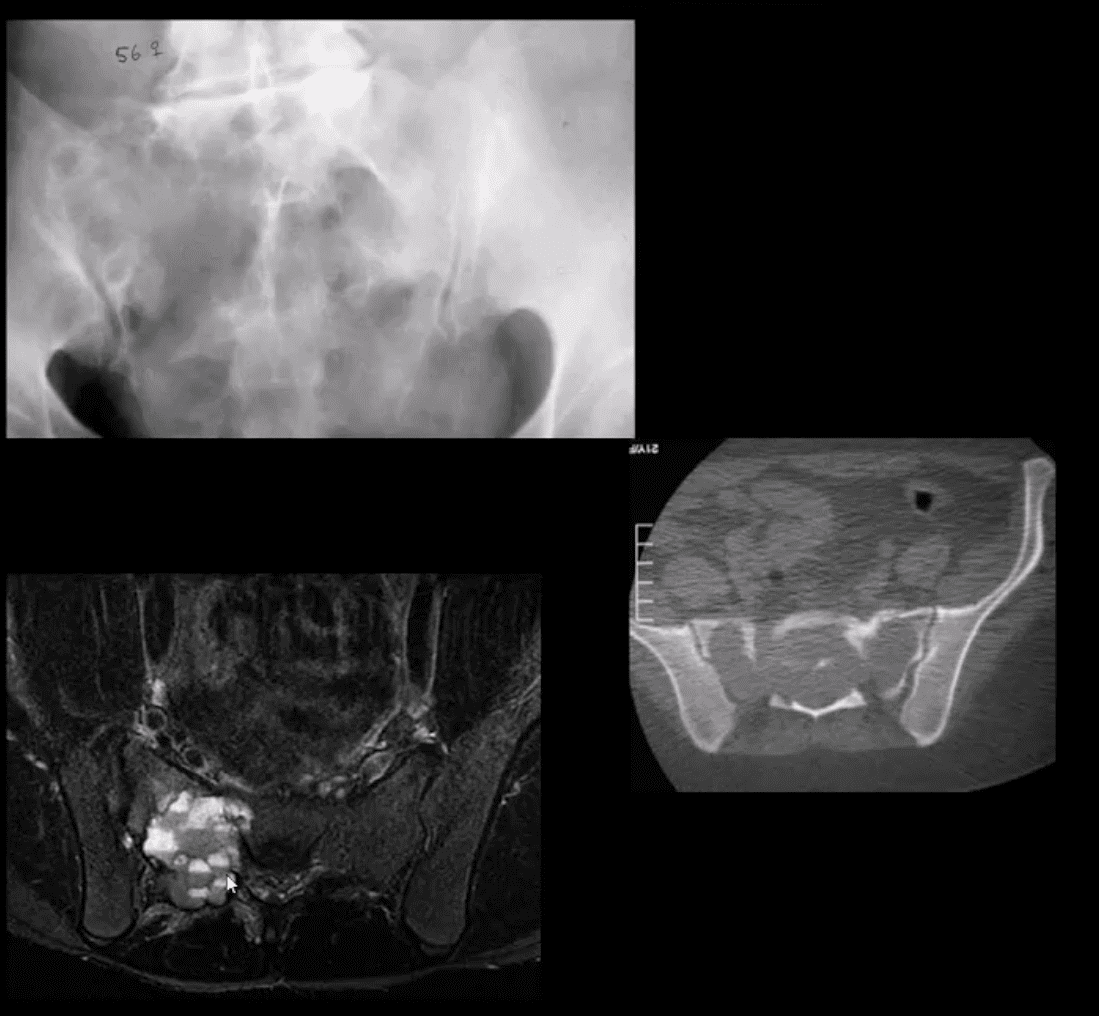
Chordoma: is relatively uncommon but considered the m/c primary malignant neoplasm that only affects the spine. D/t slow growth is often misdiagnosed for a considerable length of time as LBP
Pathology: derives from malignant transformation of notochordal cells presented as mucoid, gelatinous mass containing physaliphorous cells
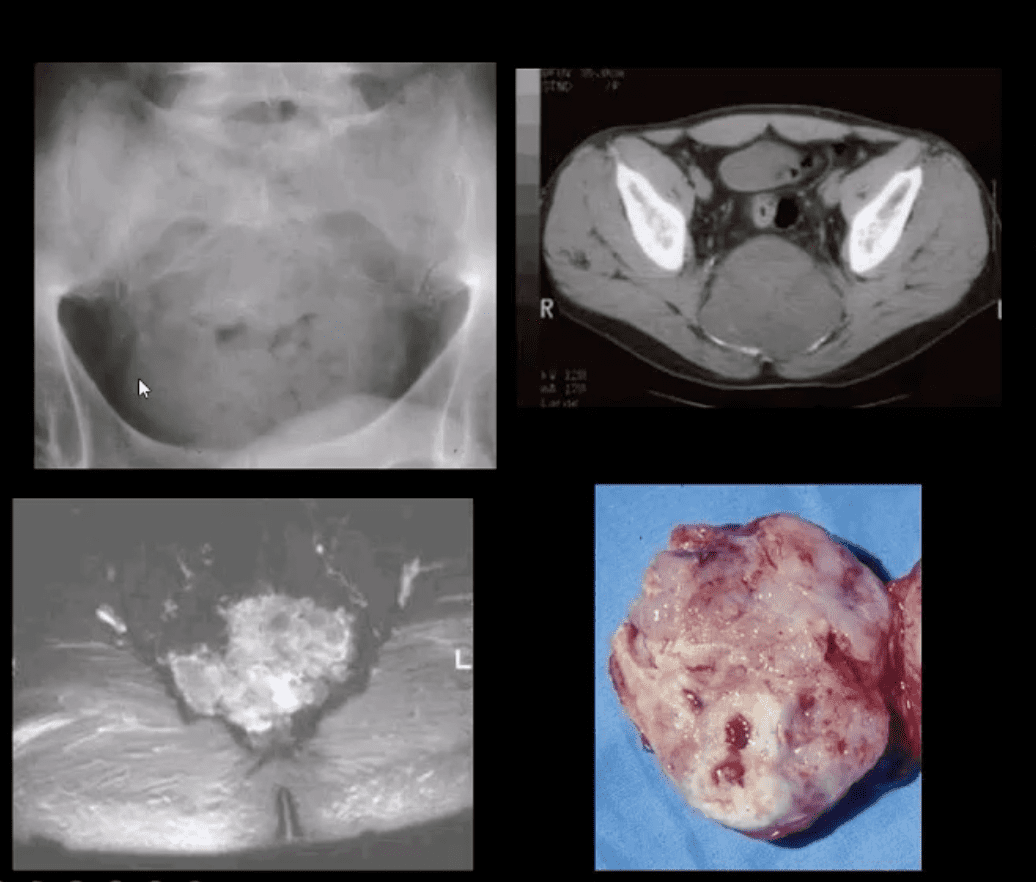
Demo:�M: F 3:1 (30-70S). 50%-sacrococcygeal, 35% spheno-occipital 15%-spine
Clinically: asymptomatic for a long time until non-specific LBP, changes in bladder & bowel, neurological signs are less common d/t midline “outward” growth & inferior to S1. Local invasion worsens prognosis. 60%-survive 5-years, 40%-10-years, Mets are delayed, poor prognosis d/t local invasion. >50% can be id. on DRE.
Imaging:�x-rays often tricky d/t overlying gas/feces. CT is >sensitive to id the bone mass and internal calcifications. MRI: T2 bight signal, T1 heterogeneously low and high d/t mucus/blood decomposition, MRI best detects local invasion and essential for care planning. Rx:� complete excision is often impossible d/t local vascular invasion.
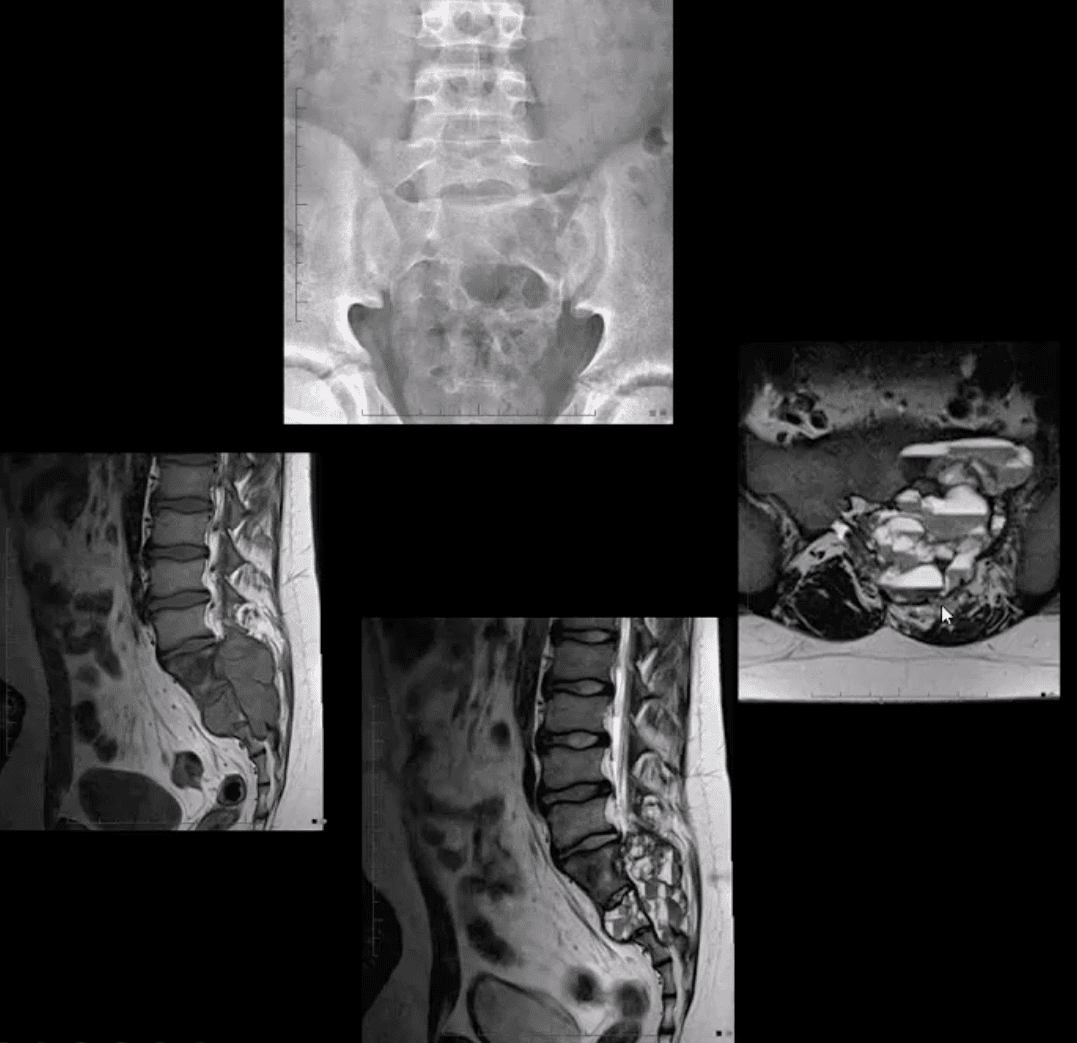
Giant cell tumor (GCT):�2nd most common primary sacral tumor. It is a histolgically benign neoplasm containing multinucleated Giant cells of Monocyte-Osteoclast origin
Imaging Dx:�x-radiography is the 1st step usually in response to complaints of LBP. Often challenging to id on x-rays d/t bowel gas/feces
Key rad feature: osteolytic expansile lesion noted by destruction of sacral arcuate lines. CT may id the lesion better. MRI is the modality of choice following x-rays. MRI: T1 low to intermediate signal. Heterogeneously high d/t edema with areas of low signal on T2 d/t blood degradation and fibrosis. Characteristic fluid-fluid levels may be noted especially if ABC develops within a GCT. Rx: operative. Prognosis is less favorable than GCT in long bones d/t lung Mets (deposits) in 13.7%
Aneurysmal Bone Cysts (ABC) are benign expansile tumor-like bone lesions (not a true neoplasm) composed and filled with numerous blood-filled channels. Thus the term “blood sponge.” ABC is m/c id in children and adolescents
Unknown etiology: trauma and pre-existing bone neoplasm (e.g., GCT) often reported. Clinically: pain that may be progressive d/t rapid nature of ABC expansion. In the spine, ABC m/c affects posterior elements and presented as expansile, soap-bubbly or lytic lesion.
DDx: can be broad, but Osteoblastoma and GCT are the top DDxs.
Imaging: x-rays demo expansile mass in posterior elements, CT is more sensitive than x-rays, MRI will demo characteristic fluid-fluid levels and mixed high and low signal d/t edema and blood decomposition/aging with some septations.
N.B. MRI fluid-fluid levels are not exclusive to ABC, and DDx includes GCT, osteoblastoma, telangiectatic osteosarcoma.
Rx: operative curettage and bone grafting, fibrosing agents. Recurrence 10-30%.
Metastatic Bone Disease (aka Mets) or “Secondaries.” Are the most common malignant bone neoplasms affecting the spine, aka spinal neoplasms (>70%) and the rest of the skeleton in adults.
5-Primaries are m/c involved:
Breast (16-37%)
Lung (12-15%)
Thyroid (4%)
Renal (3-6%)
Prostate (9-15%)
Spine, pelvis, proximal femurs & proximal humeri are m/c affected in that particular order of frequency
Thoracic & upper Lumbar spine considered the m/c site of spinal Mets
Pathophysiology & Etiology of Metastasis
Malignant cells a very good at evading immune detection and elimination
They gain�access to circulation expressing Vascular Endothelial Adhesion Molecules (e.g., integrines & selectins)
Once reaching their target organs, malignant cells stimulate the production of various vasogenic growth factors and by exiting blood vessels invade their target tissues
Lung, Liver, and Bone are particularly at risk due to the character of their blood supply
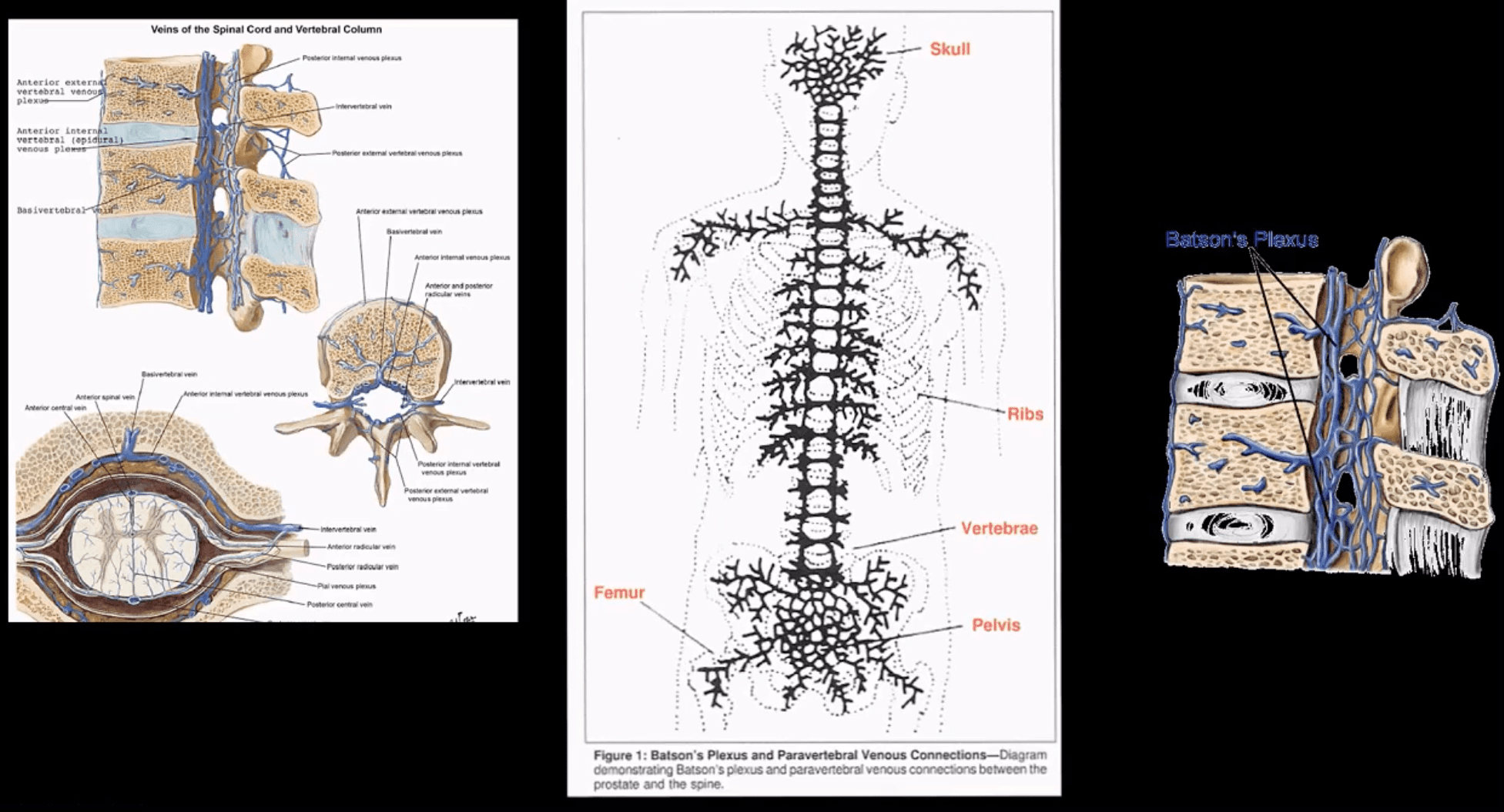
Baston venous plexus-is a network of valveless freely communicating� veins connecting axial skeleton/meninges and proximal femurs/humeri with abdomino-pelvic and thoracic cavities
The risk of Mets is increased during daily variations in the intra-abdominal and intra-thoracic pressure
In adults, the axial skeleton is involved in hematopoiesis, and it is particularly vulnerable to metastatic deposits via an abundant network of sinusoids within a spongy bone
The vast majority of bone Mets will be detected in the axial skeleton
Clinical Presentation
Back pain often mimicking “mechanical back pain” is the m/c and often misleading symptom
Chiropractors and other manipulators should be particularly aware of this dangerous pitfall.
Nocturnal pain or pain unresponsive to NSAID may be reported in more advanced cases
Advanced cases may also present with a neurological deficit due to pathologic vertebral fractures and spinal cord/nerves compression
Metastatic hypercalcemia may occasionally develop in severe cases and considered a medical emergency that potentially presents with confusion, muscle weakness, and renal signs
Imaging plays a significant role in the Dx and management of bone metastasis
Lab tests are of limited value, but hypercalcemia and alkaline phosphatase (Alk Phos) may be elevated
In some cases, a bone biopsy may be used to confirm bone Mets
When Bone Mets are Detected, Patients Prognosis is Significantly Worsened
Median survival:
Thyroid – 48 – months
Prostate – 40 – months
Breast – 24 – months
Renal Cell – may vary, can be as low as 6 – months
Lung – 6 – months
Imaging Diagnosis
Begins with radiography investigating a clinical complaint of back/bone pain
If radiographs are unrewarding or equivocal, unique imaging modalities are required
MRI may help to show marrow replacement by Mets foci but limited to specific regions
Tc99 radionuclide bone scan (scintigraphy) is considered one of the most sensitive and reliable imaging steps in evaluating bone Mets
Bone scintigraphy is good at detecting both lytic and blastic Mets
However, very aggressive/vascular osteolytic Mets and Multiple Myeloma often appear “cold” or photopenic on bone scan due to greater stimulation/activation of osteoclasts which “outpace” osteoblasts ability to uptake the radiopharmaceutical
CT scanning is an excellent modality to show bone destruction, but it is not widely used during bone Mets Dx especially if radiography, bone scintigraphy, and MRI provide adequate information about the process
CT scanning may be particularly helpful with delineation of pathological fractures
General Radiographic Features of Bone Mets
Osteolytic (lytic), osteoblastic (blastic) aka sclerotic Mets or misec Mets can be identified radiographically
However, it takes between 30-50% of lamella (cortical) bone and 50-75% of trabecular (cancellous) or spongy bone to be destroyed before it can be detected on plain film radiographs
This can make early radiographic detection of bone Mets very difficult, requiring particular imaging modalities (e.g., MRI)
Also, bowel gas/fecal matter and numerous soft tissue densities in the abdomino-pelvic and thoracic cavities may pose challenges of bone Mets detection
Different tumors often manifest with different metastatic appearance, depending on tumor activity and release of cytokines (IL6, IL11), endothelin 1 or other growth factors that will be responsible for either osteolytic, osteoblastic or mixed Mets
For example: purely lytic bone Mets are noted in Lung, Thyroid, and Renal cell CA (very vascular)
Breast CA may present with 60% of blastic Mets
Prostate CA presents with 90% of blastic Mets
Other blastic Mets may derive from urinary bladder, melanoma and GI adenocarcinomas
Sclerotic foci may also represent as previously treated primaries
Very vascular� Mets like Renal cell and Thyroid may present with markedly� lytic and expansile foci often called “blow out Mets.”
Mets found distal to elbows and knees (acro-metastasis) are commonly associated with Lung CA
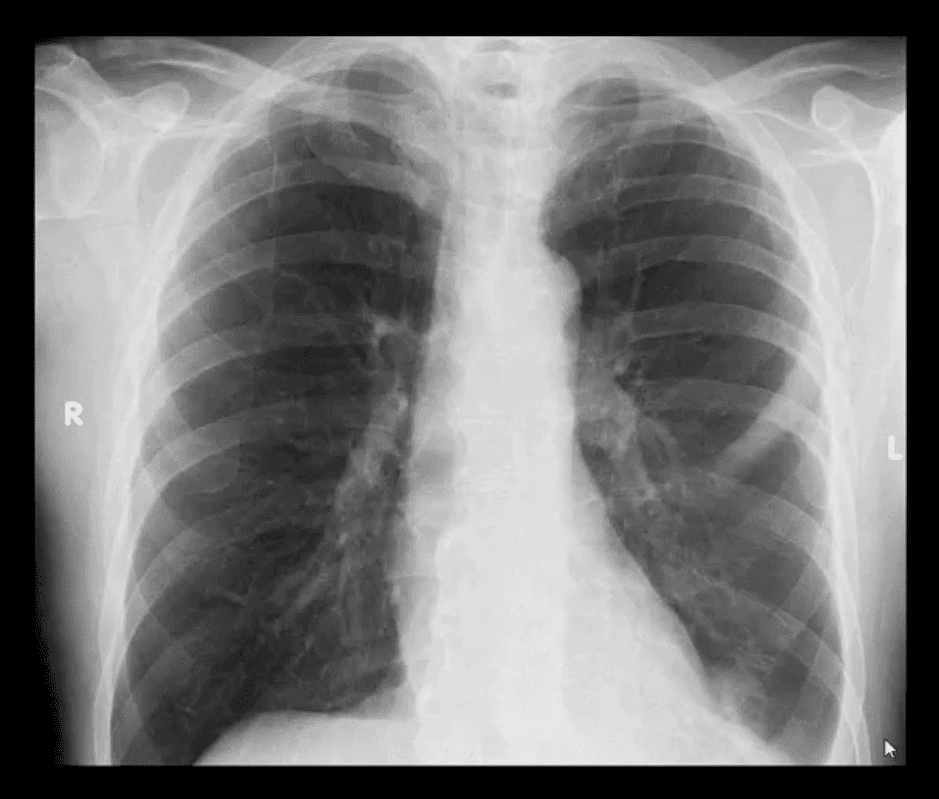
PA chest view of a routinely screened patient with a known Hx of Prostatic adenocarcinoma
Note sclerotic lesion identified in the left posterior Rib 5
What imaging modality is required next?
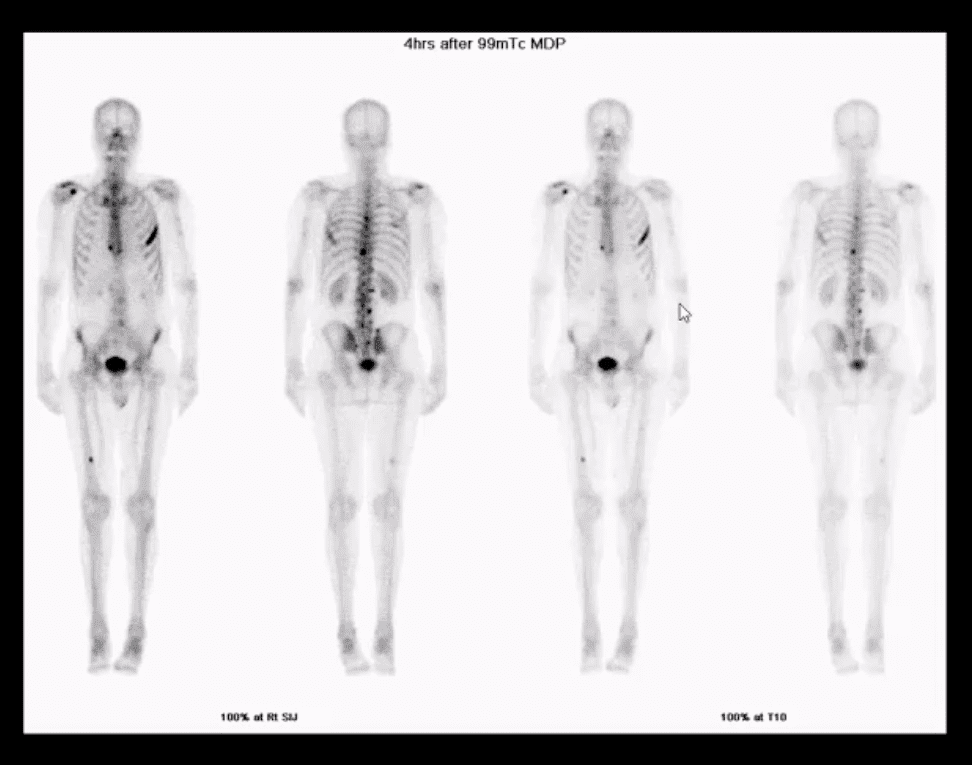
Radionuclide bone scan should be suggested
Multiple foci of high uptake of the Tc99 radiopharmaceutical
This is due to Mets and increased osteoblastic activity in the thoracic and lumbar spine, ribs and other sites of the skeleton
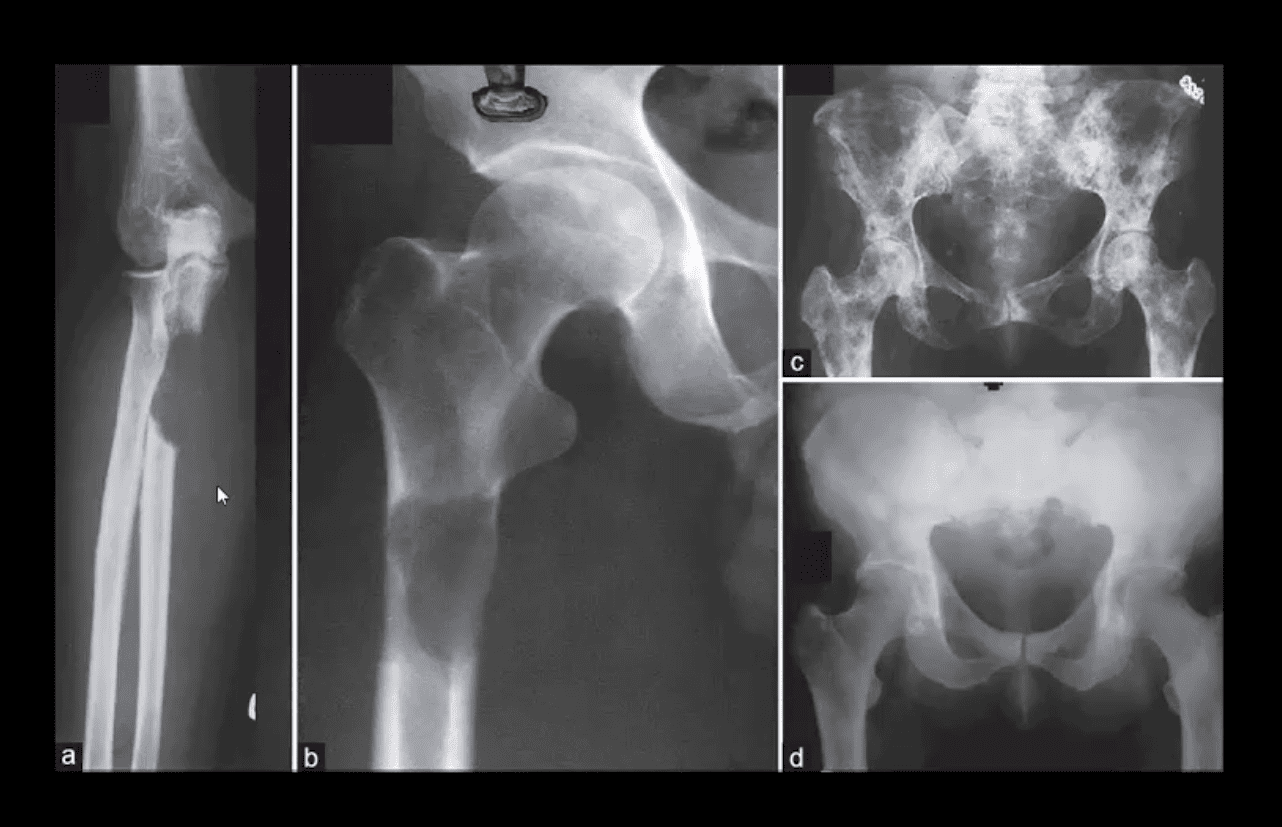
Comparison of purely lytic (a and b) versus blastic (d) and mixed (c) Mets
What primaries to consider?
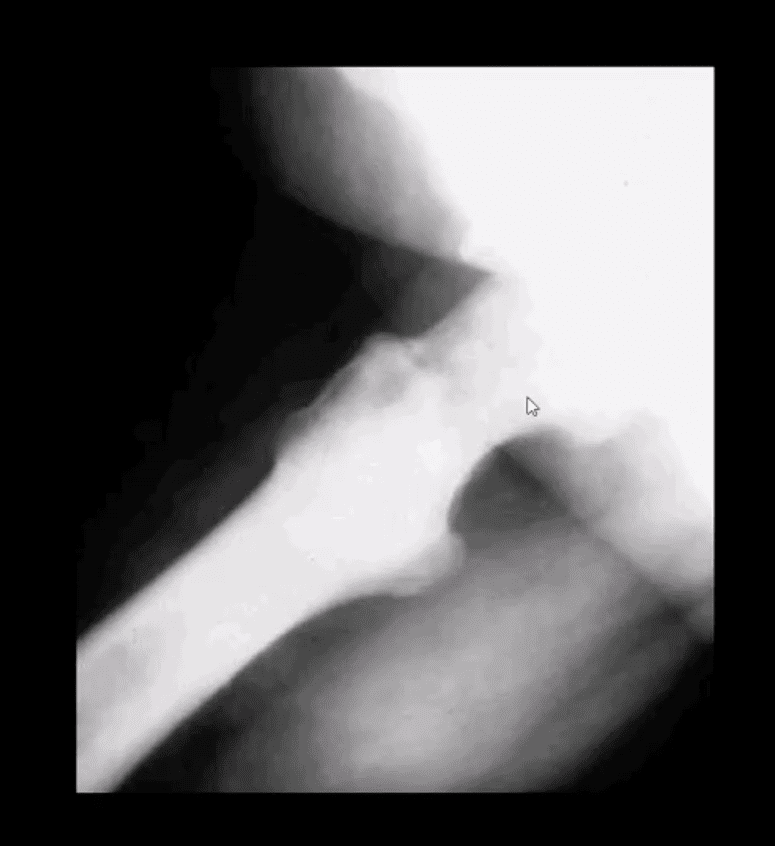
Frog leg view of the hip
Clinical Dx: Prostatic adenocarcinoma
Note diffuse blastic Mets in the proximal femur
Hx: severe shoulder and arm pain unrelieved by rest
Rad DDx: Mets, Myeloma or less frequently Lymphoma
This classic DDx is used by the majority of Radiologists when aggressive osteolytic bone lesions are noted
The patient had a known Hx of Breast CA
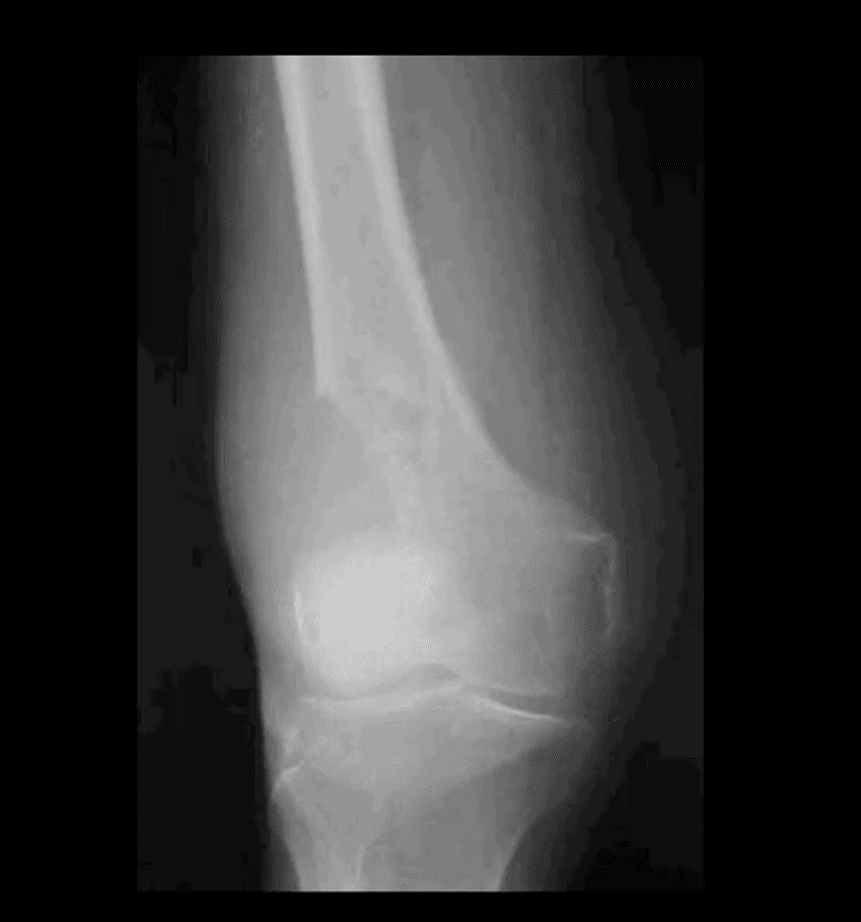
A 51-year-old female with Breast CA
Large lytic destructive lesion in the distal femoral metaphysis characteristic of aggressive osteolytic Mets
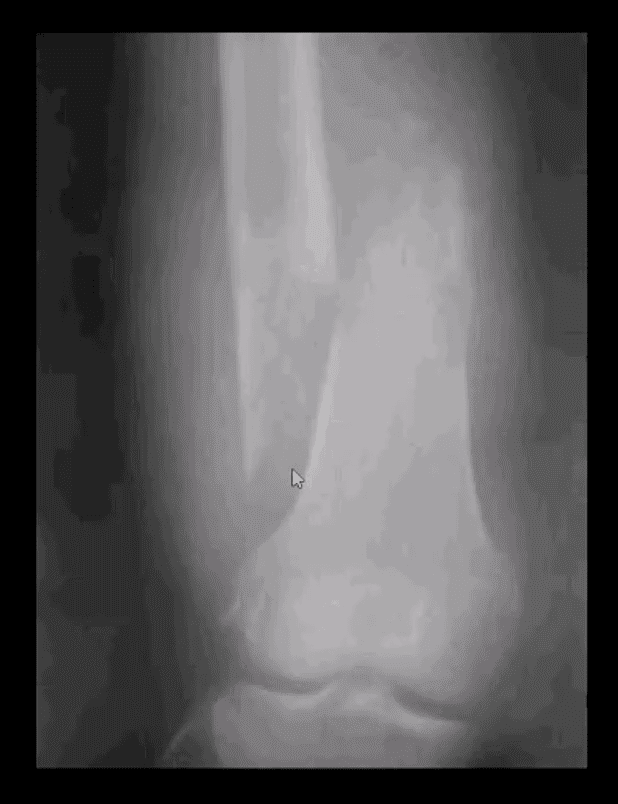
Sudden onset of severe leg pain and inability to stand in a 53-year-old female with Breast CA
Dx: Pathological fracture through the distal femoral shaft
Pathological Mets fractures in the spine and extremities are dreaded by most Oncologists due to higher association with severe complications and poor clinical prognosis
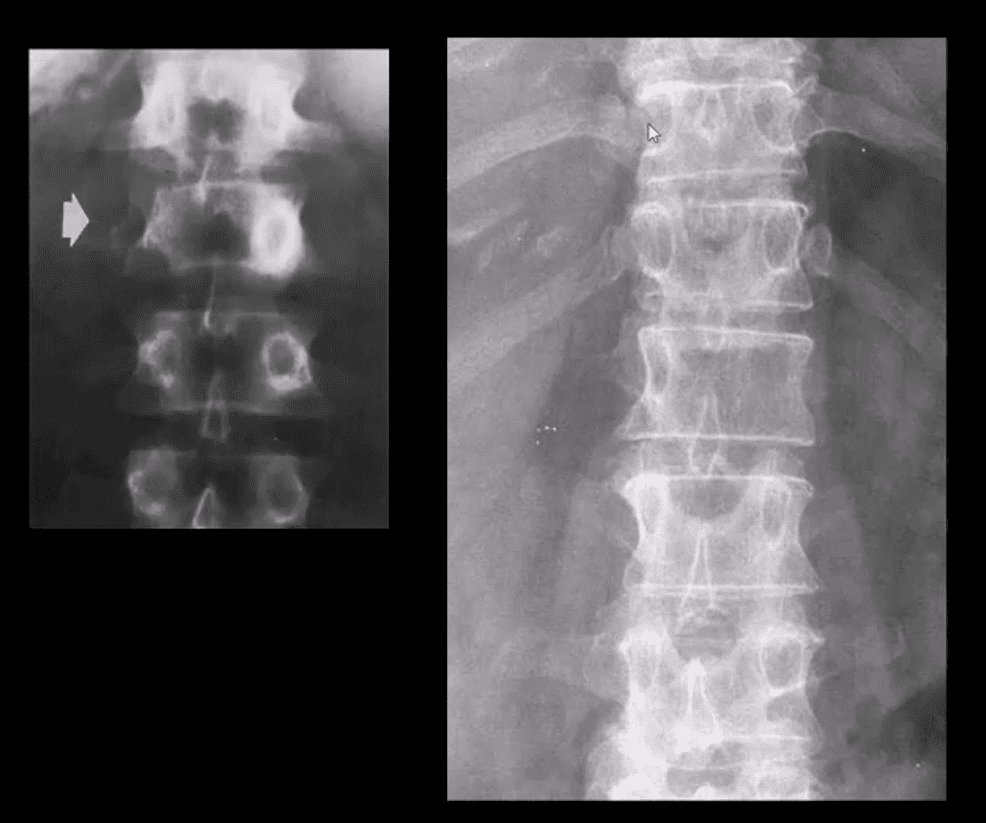
Radiographic Dx of vertebral Mets should be suspected if a “missing pedicle sign” aka “winking owl sign” is noted
DDx: pedicle agenesis (above left) shows hypertrophy and sclerosis of a contralateral pedicle d/t increased mechanical stress
Pedicle Mets are often thought of as the m/c initial site of spinal Mets
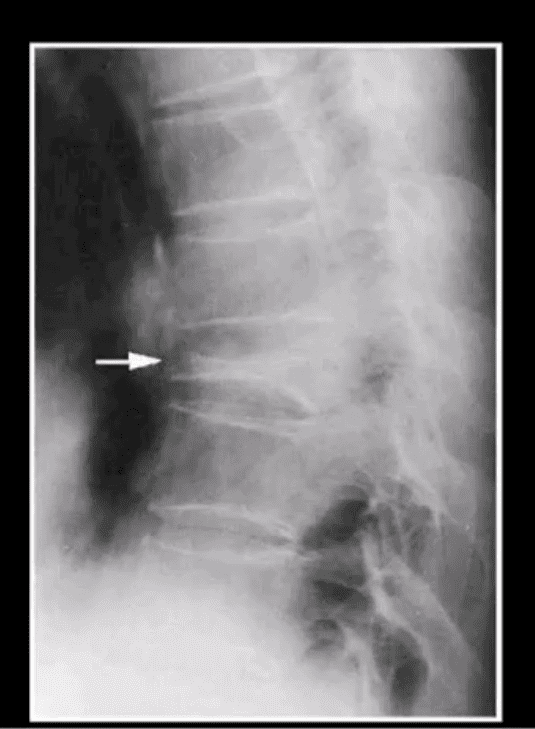
Vertebral Body Pathologic Fracture (VERTEBRA PLANA)
Isolated compression fracture at the T8 segment noted (above arrow)
The loss of the posterior and anterior height suggest an underlying pathologic condition for which the differential diagnosis includes:
Differentiating Pathological Fx of the vertebral body from an osteoporotic insufficiency Fx can be a significant challenge
Close inspection of the posterior body height is helpful but often not reliable
In metastasis, the posterior body is collapsed
In OSP, the posterior body may be maintained appearing more as anteriorly wedge fracture
MR imaging and/or radionuclide bone scan need to be performed
A skeletal radiographic survey may be used occasionally for the evaluation of bone Mets especially in well-established cases
It includes bilateral AP & lateral Thoracic and Lumbar views, AP pelvis, humeri, femurs, and the skull
Availability of special imaging has supplanted the use of skeletal radiographic survey
However, in a clinical practice skeletal radiographic study of Multiple Myeloma may still be used primarily if the diagnosis was previously established
Technetium-99 (99mTc) bone scintigraphy is very sensitive and cost-effective study:
For the detection/localization of Mets and often an assessment of their biologic activity and response to treatment
This modality is a well-established part of the workup for known as well as unknown primaries
It may also help with determination of lesions that will be most accessible and easy to biopsy
When the burden of Mets is significantly high as shown in the case above
The radiotracer uptake is being almost entirely taken in by metastatic lesions
No material is left for the kidneys to excrete
This is known as a “super scan”
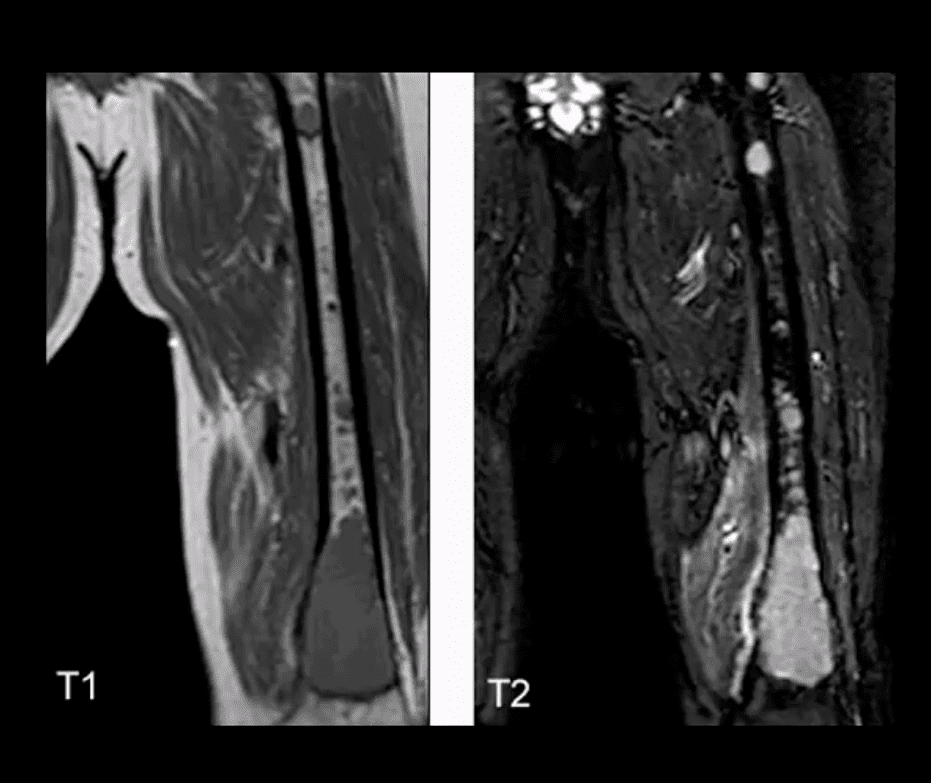
Sagittal Lumbar and Lower Thoracic MRI. Multiple metastasis are noted on T1 (above right) and T2 (above left)� WI as hypointense foci of marrow replacement of the vertebral bodies in a patient with Hx of Prostate CA
MR imaging protocol with T1, T2, and T1+C gad can be used in many cases if x-radiography is unrewarding or questionable
�MRI can reveal bone marrow changes due to bone marrow replacement by Mets and surrounding edema
Typically blastic Mets appear as abnormally decreased signal intensity (hypointense) lesions on T1 and T2 pulse sequences
Purely lytic Mets often appear as hypo-intense on T1 and hype-intense on T2
Increased gadolinium uptake may also be evident on T1+C fat suppressed sequence d/t increased vascularity of malignant foci especially in very aggressive vascular neoplasms
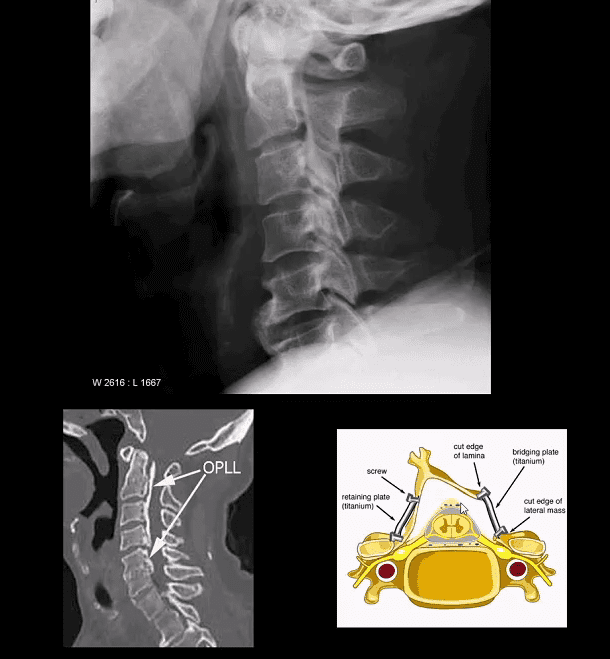
Ossification of Posterior Longitudinal Ligament (OPLL). Less frequent than DISH.
Greater clinical importance d/t spinal canal stenosis and cervical myelopathy
Asian patients are at higher risk
Both OPLL & DISH may co-exist and increase the risk of Fx
Imaging: x-rad: linear radioopacity consistent with OPLL
Imaging modality of choice: CT scanning w/o contrast
MRI may help� to evaluate myelopathy
Care: surgical with laminoplasty (above right image) that has been pioneered and advanced in the Far East
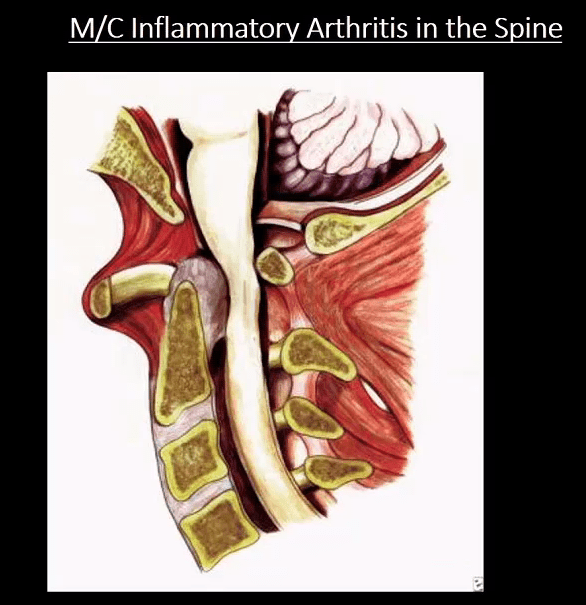
M/C Inflammatory Arthritis In Spine
Rheumatoid spondylitis (Rheumatoid arthritis) d/t inflammatory synovial proliferation pannus rich in lymphocytes, macrophages, and plasma cells
C/S RA may affect 70-90% of patients
Variable severity from mild to destructive disabling arthropathy
RA IN C/S m/c affects C1-C2 due to an abundance of rich synovial tissue
Typically infrequent in the thoracic/lumbar region
Sub-axial C/spine may be affected later due to facets, erosions, ligament laxity and instability showing “Stepladder” appearance
Clinically: HA, neck pain, myelopathy, etc. inc. Risk of Fx/subluxation. Any spinal manipulation HVLT ARE STRICTLY CONTRAINDICATED.
Rx: DMARD, anti-TNF-alfa, operative for subluxations, etc.
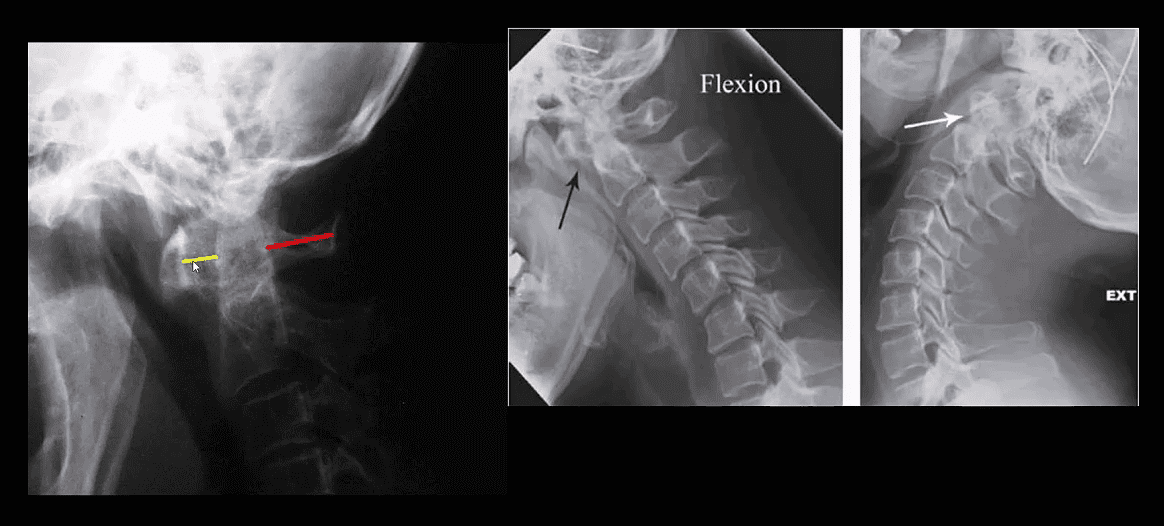
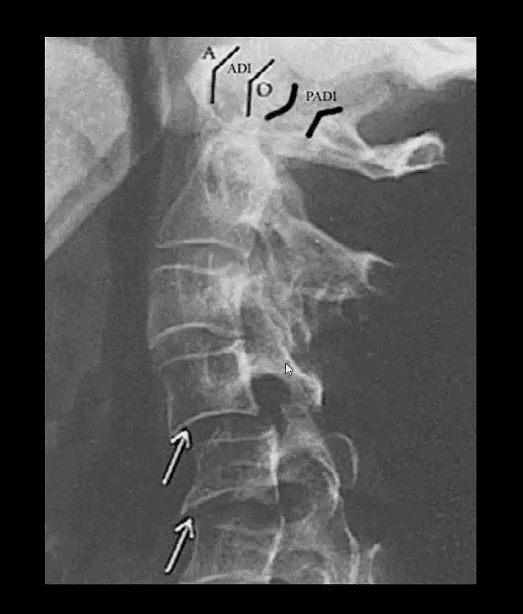
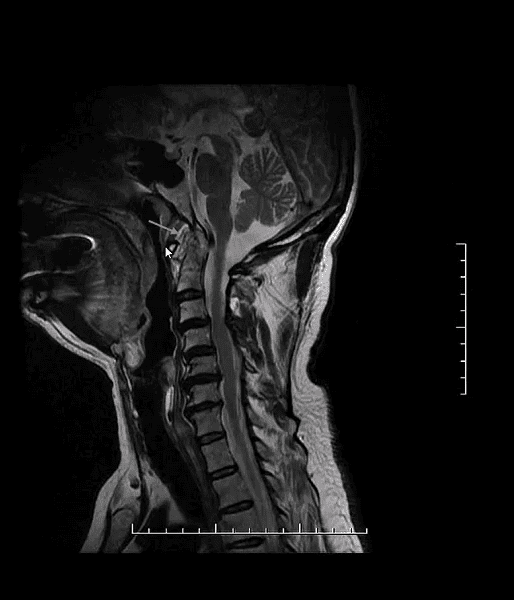
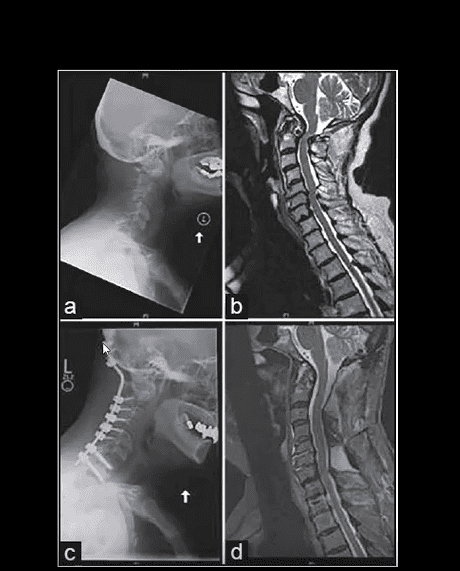
Rheumatoid Spondylitis C1-C2. Perform X-radiography initially with flexed-extended views. Note Dens erosion, C1-2 subluxation (2.5 mm) that changes on mobility
RA spondylitis: an erosion of the odontoid with the destruction of C1-C2 ligaments and instability
M:F 4:1, age: 20-40 m/c. Clinic LBP/stiffness, reduced rib expansion <2 cm is > specific than HLA-B27, progressive kyphosis, risk of Fx’s.
Imaging steps: 1st step-x-rays to id. Sacroiliitis/spondylitis.�MRI & CT may help if x-rays are unrewarding.
Labs: HLA-B27, CRP/ESR, RF-
Dx: clinical+labs+imaging.
Rx: NSAID, DMARD, anti-TNF factor therapy
Key Imaging Dx: always presents initially as b/l symmetrical sacroiliitis that will progress to complete ankylosis. Spondylitis presents with continuous ascending discovertebral osteitis (i.e., marginal syndesmophytes, Romanus lesion, Anderson lesion), facets and all spinal ligament inflammation and fusion with a late feature of “bamboo spine, trolley track, dagger sign,” all indicating complete spinal ossification/fusion. Increasing risk of Fx’s.
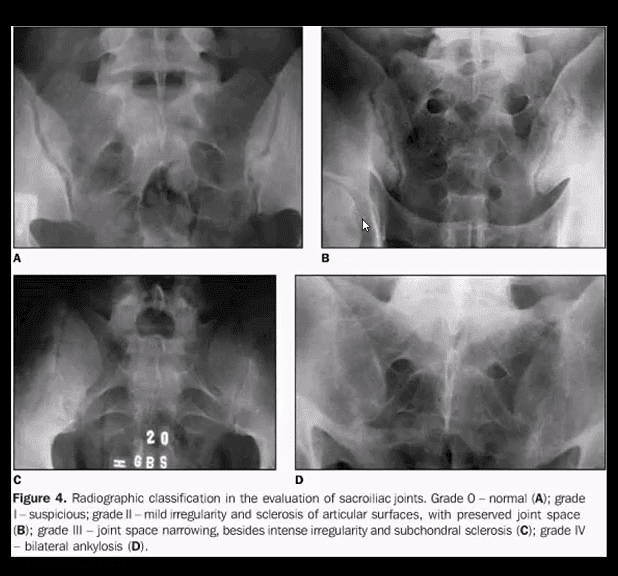
Key Dx of Sacroiliitis
Blurring, cortical indistinctness/irregularity with adjacent reactive subchondral sclerosis initially identified primarily on the iliac side of� SIJs.
Normal SIJ should maintain a well defined white cortical line. Dimension 2-4 mm. May look incongruous d/t 3D anatomy masked by 2D x-rays.
Key Imaging Dx In Spine
Marginal syndesmophytes and inflammation at the annulus-disc (above arrows) at the earliest dx; by MRI as marrow signal changes on T1 and fluid sensitive imaging (above top images).
These represent enthesitis-inflammation that will ossify into bamboo spine.
Lig ossification: trolley track/dagger sign
AS in extraspinal joints: root joints, hips, and shoulders
Symphysis pubis
Less frequent in peripheral joints (hands/feet)
All seronegatives may present with heel pain d/t enthesitis
Complication: Above Carrot-stick/chaulk-stick Fx
PsA & ReA (formerly Reiter’s) present with b/l sacroiliitis that virtually identical to AS
In the spine PsA & ReA DDx from AS by the formation of non-marginal syndesmophytes aka bulky paravertebral ossifications (indicate vertebral enthesitis)
For a clinical discussion of Spondyloarthropathies refer to:
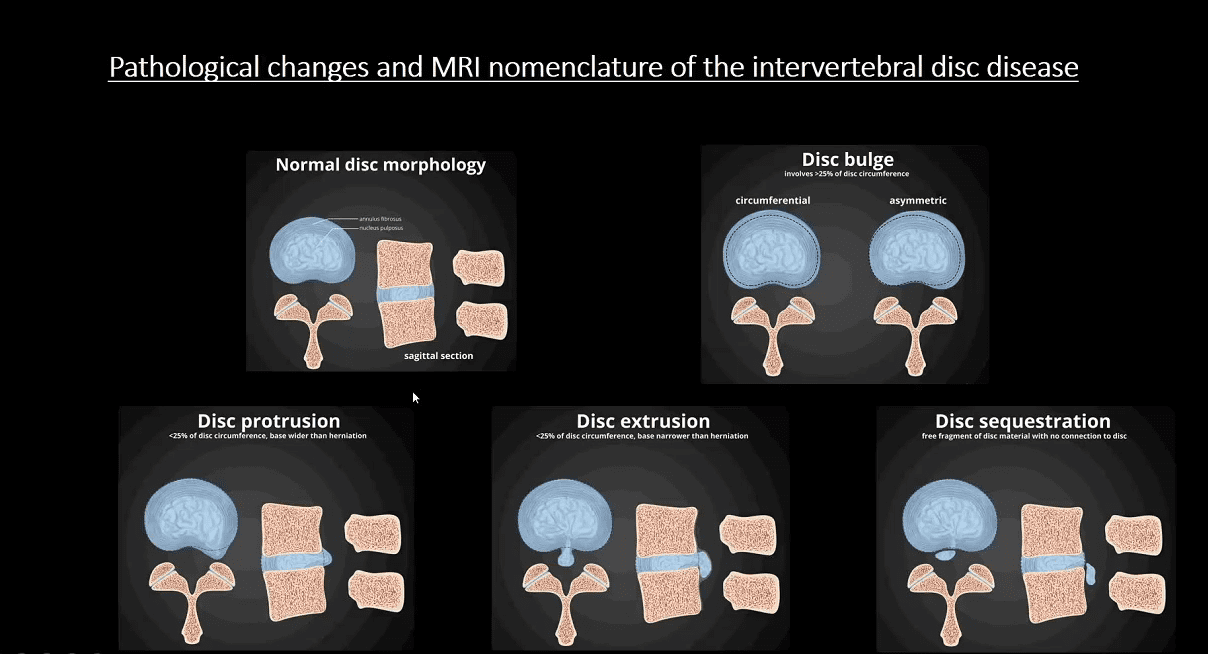
Spondylosis aka Degenerative disease of the spine represents an evolution of changes affecting most mobile spinal segments beginning with:
Intervertebral disc (IVD) dehydration (desiccation) and degeneration aka Degenerative Disc Disease (DDD) with an abnormal increase in mechanical stress and degeneration of posterior elements affecting 4-mobile synovial articulations ( true osteoarthritis)
2-Facets in the L/S & 2-Facets & 2-Uncovertebral joints in the C/S
Imaging plays a significant role in the diagnosis, grading, and evaluation of neurological complications (e.g., spondylotic myelopathy/radiculopathy)
X-radiography with AP, Lateral & Oblique spinal views provides Dx and classification of Spondylosis
MR imaging may help to evaluate the degree of neurological changes associated with degenerative spinal canal and neural foraminal stenosis
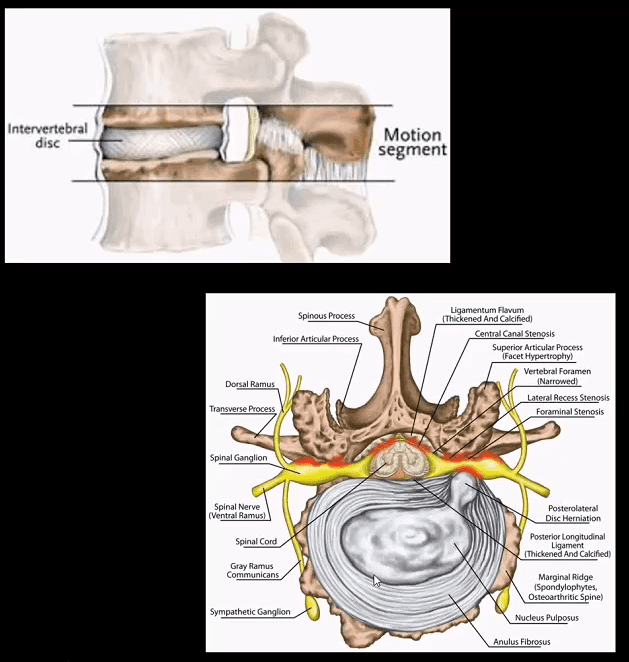
Spinal motion segment:
2-adjacent vertebrae
IVD (fibrocartilage)
2-facets (synovial)
Pathology: loss of disc height increases mechanical stress on mobile elements
Ligamentum flavum “hypertrophy” or thickening due to buckling
Loss of normal lordosis with or w/o reversal or kyphosis
Vertebral canal & neural foraminal stenosis
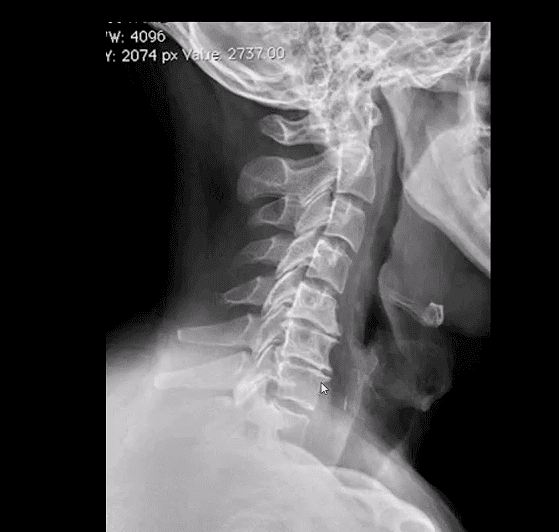
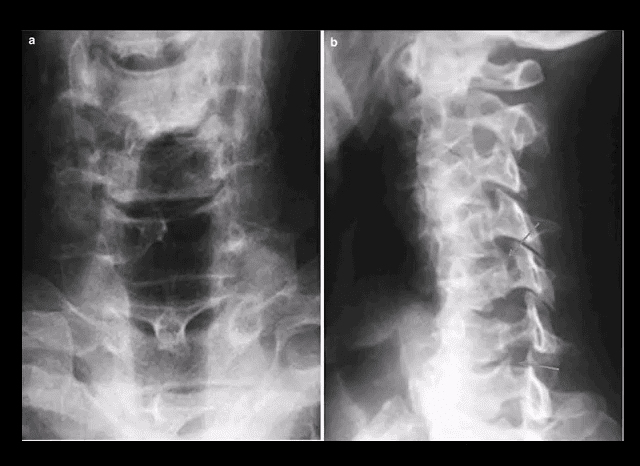
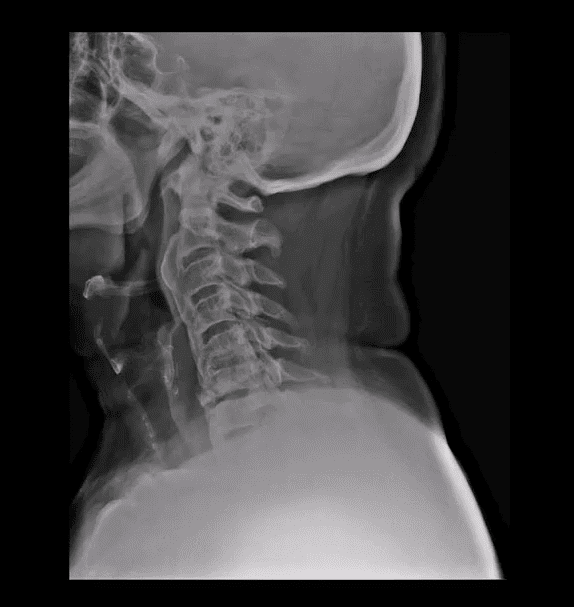
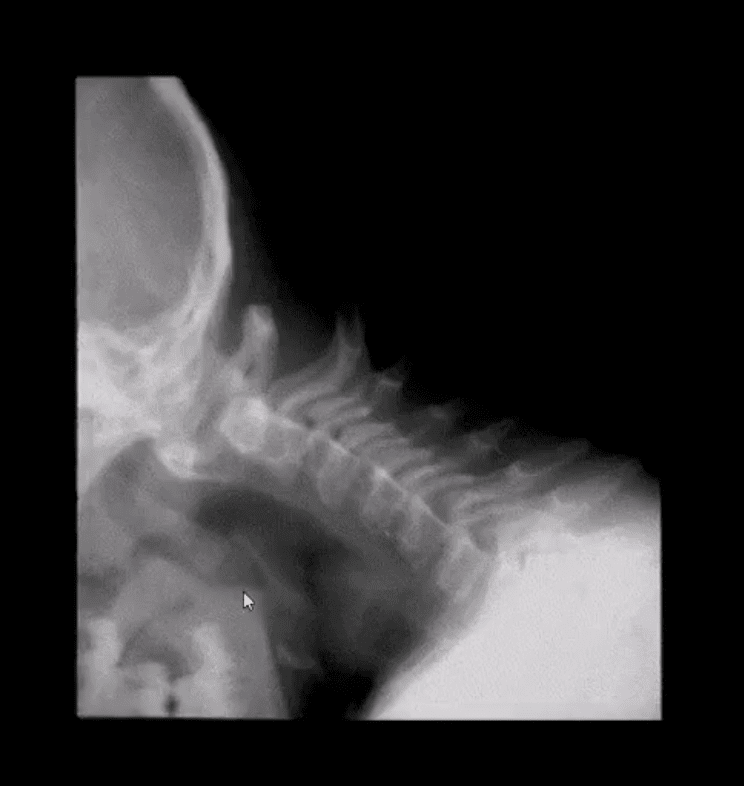
Neutral lateral cervical radiograph: note mild to moderate disc narrowing and spondylophyte formation at C5-6 & C6-C7 (most common levels affected by cervical spondylosis). Straightening or flattening with mild reversal of cervical lordosis. Some mild facet proliferation is noted at the above levels
On radiographs: evaluate for disc height (mild, moderate or severe) loss
End-plate sclerosis & spondylophytes; mild, moderate or severe
Facet and uncinate irregularity, hypertrophy/degeneration; mild, moderate or severe
Key Dx: correlate with a clinical presentation: neck/back pain with or w/o neurological disturbance ( myelopathy vs. radiculopathy or both)
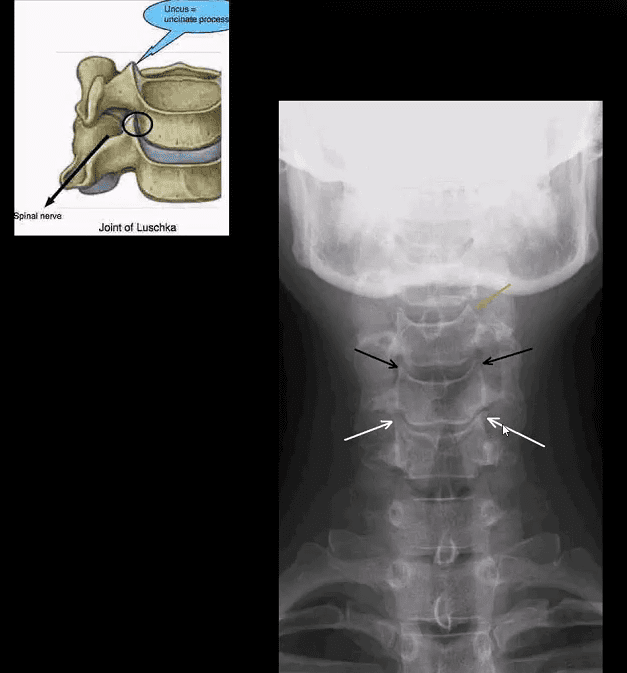
Uncinate processes undergo degeneration/proliferation resulting in uncovertebral arthrosis
Early findings present with mild bone proliferation along the cortical margin (white and black arrows) if compared to normal uncinate (orange arrow)
Later, more extensive bone proliferation extending into and narrowing vertebral canal and neural osseous foramina (IVF’s) may be noted. The latter may contribute to spinal/IVF stenosis and potential neurological changes
Posterior oblique views may help further
AP lower cervical (a) and posterior oblique (b) views
Note mild uncinated process proliferation with neural foraminal narrowing (arrows)
Typically if less than a third of IVF becomes narrowed, patients may present w/o significant neurological signs
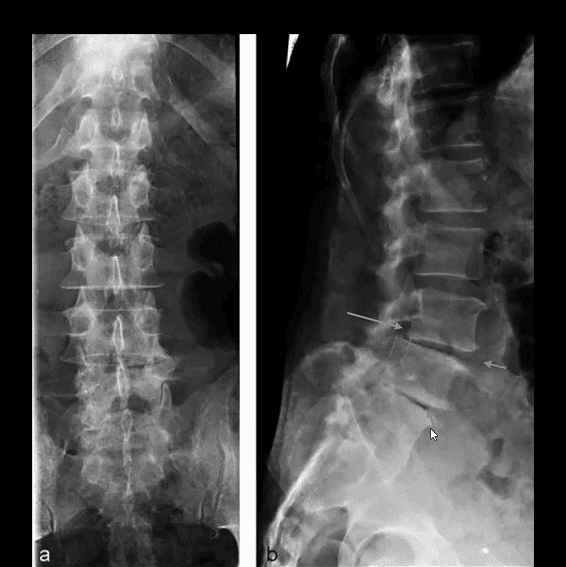
Lumbar spondylosis is evaluated with AP and lateral views with additional AP L5-S1 spot view to examine lumbosacral junction
Typical features include disc height loss/degeneration
Intra-discal gas (vacuum) phenomenon (blue arrow) along with spondylophytes
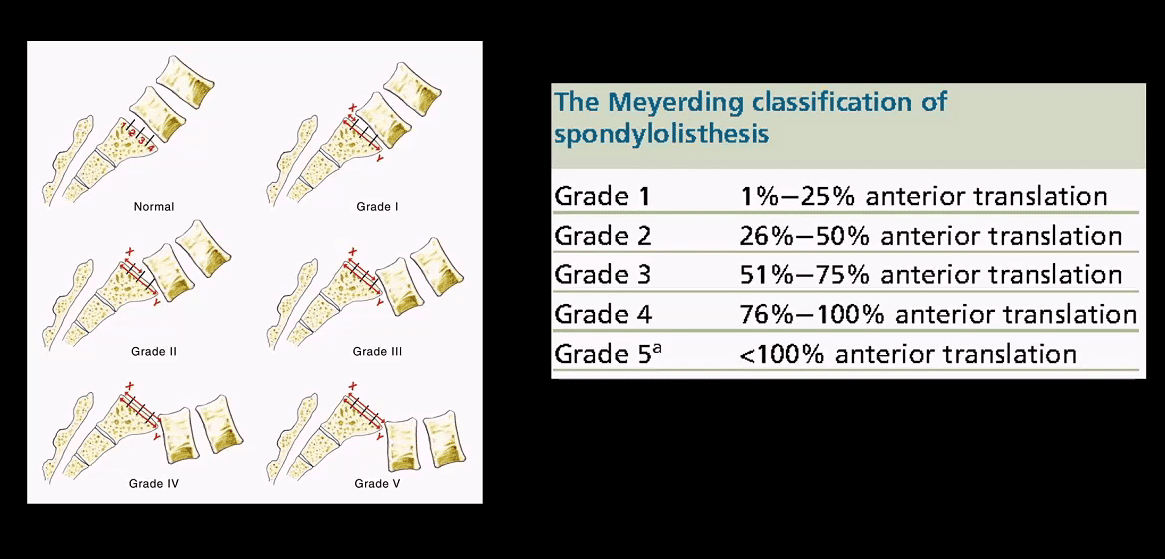
Degenerative spondylolisthesis and/or retrolisthesis (green arrow) may follow disc and facet degeneration and can be graded by the Meyerding classification
In most cases, degenerative spondylolisthesis rarely progresses beyond Grade 2
Lumbar facet degeneration seen as bone proliferation/sclerosis and IVF narrowing
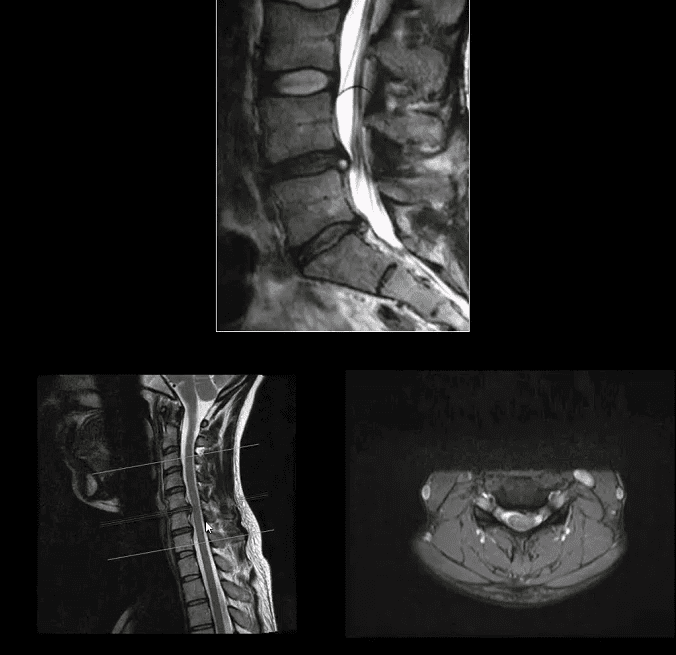
MR imaging w/o gad C is an effective modality to evaluate clinical signs of spondylosis & associated neurological complications with pre-surgical evaluation
Case: 50-y.o Fe with neck pain. Case b-45-y.o.M (top a b images). MRI reveals: loss of disc hydration or desiccation, spondylophytes and disc herniation w/o neurological changes
(Bottom images) Left: preoperative and right postoperative MRI slices of the patient presented with clinical signs of cervical spondylotic myelopathy. Note disc herniation, ligam flavum hypertrophy and canal stenosis (left)
Sagittal MRI slice of lumbar DDD manifested with disc desiccation and posterior herniation effacing thecal sac
Correlating sagittal and axial slices will be more informative to evaluate canal stenosis and potential degree of neurological involvement (above-bottom images)
Use the following resources to learn more on MRI evaluation and diagnosis of Degenerative Disc Disease:
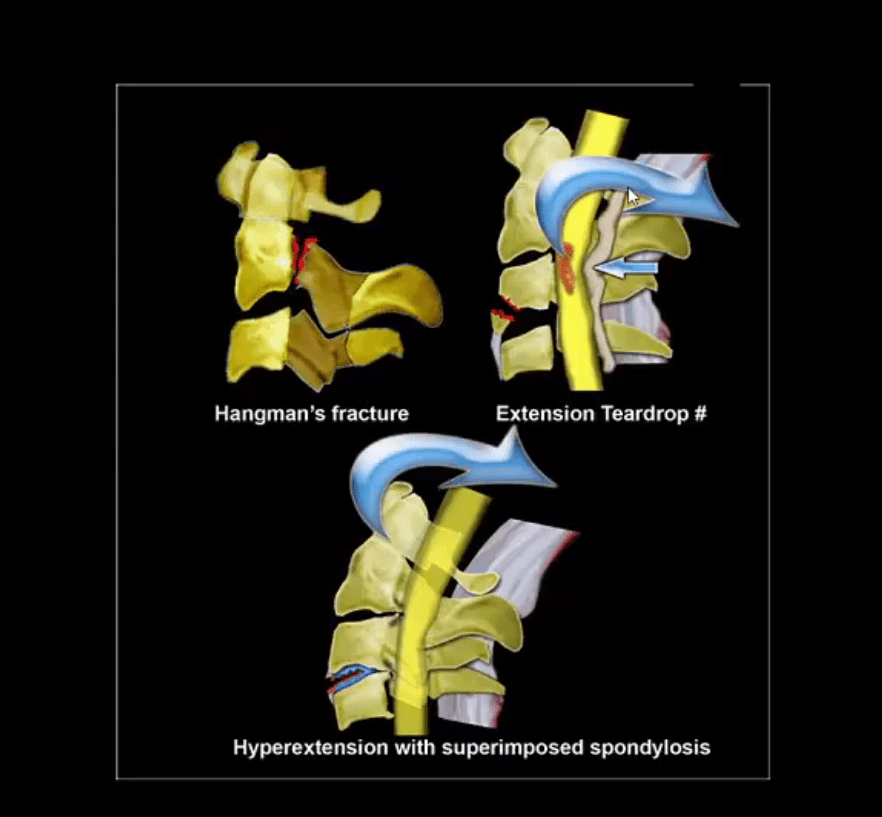
Hangman’s Fx aka traumatic spondylolisthesis of C2 with a fracture of pars interarticularis or pedicles (unstable)
MVA is the most common cause
Mechanism: acute hyperextension of upper C/S similar to judicial hanging (never actually seen and most deaths are due to asphyxiation)
Secondary flexion may tear PLL and disc
Associated injuries: 30% have other c-spine fx especially Extension teardrop at C2 or C3 due to avulsion by ALL
Cord paralysis may only present in 25% due to bony fragments dissociation and canal widening
Hangman fx and extension teardrop
Cervical degeneration and previous fusion is a key predisposing factor due to the lack of mobility and suppleness, rendering C/S easy to fracture
Imaging: initial x-radiography then CT that helps to delineate another injury such as facet/pedicle Fx further. MRI may help if complicated by Vertebral A. damage
Management: if type 1 injury then closed reduction and rigid collar for 4-6 weeks, halo bracing if type 2 (>3-5mm displacement) Fx/instability, anterior or posterior spinal fusion at C2-3 if type 3 Fx (>5-mm displacement)
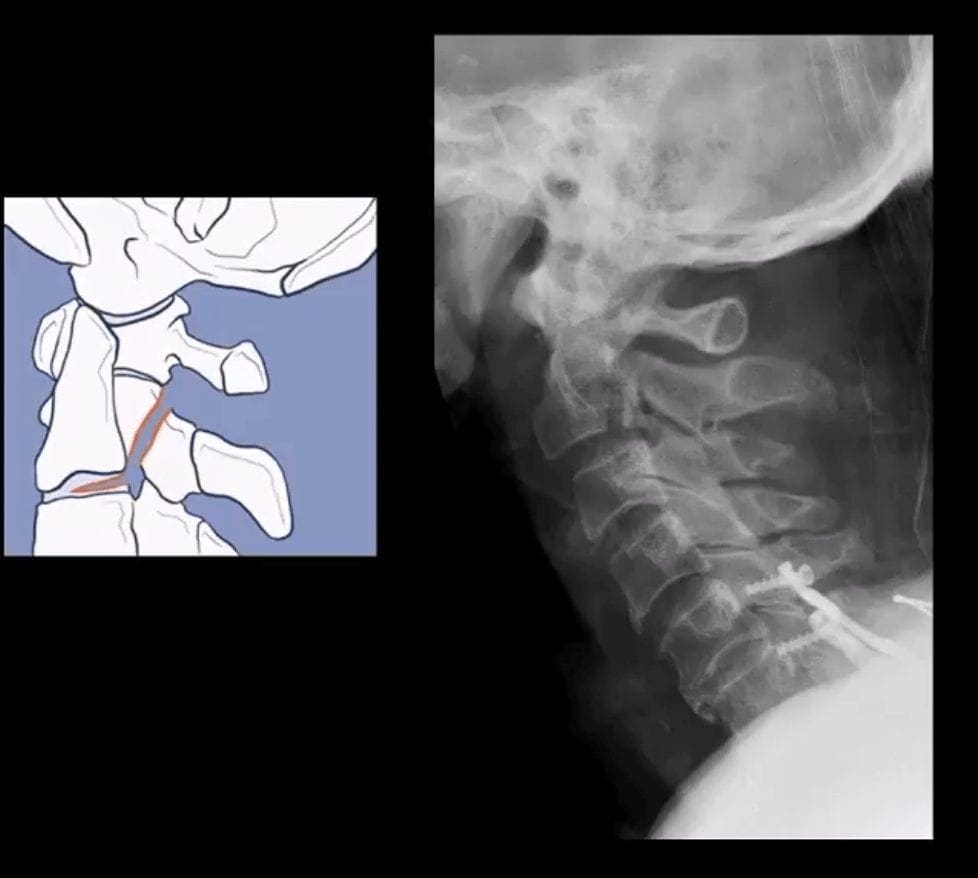
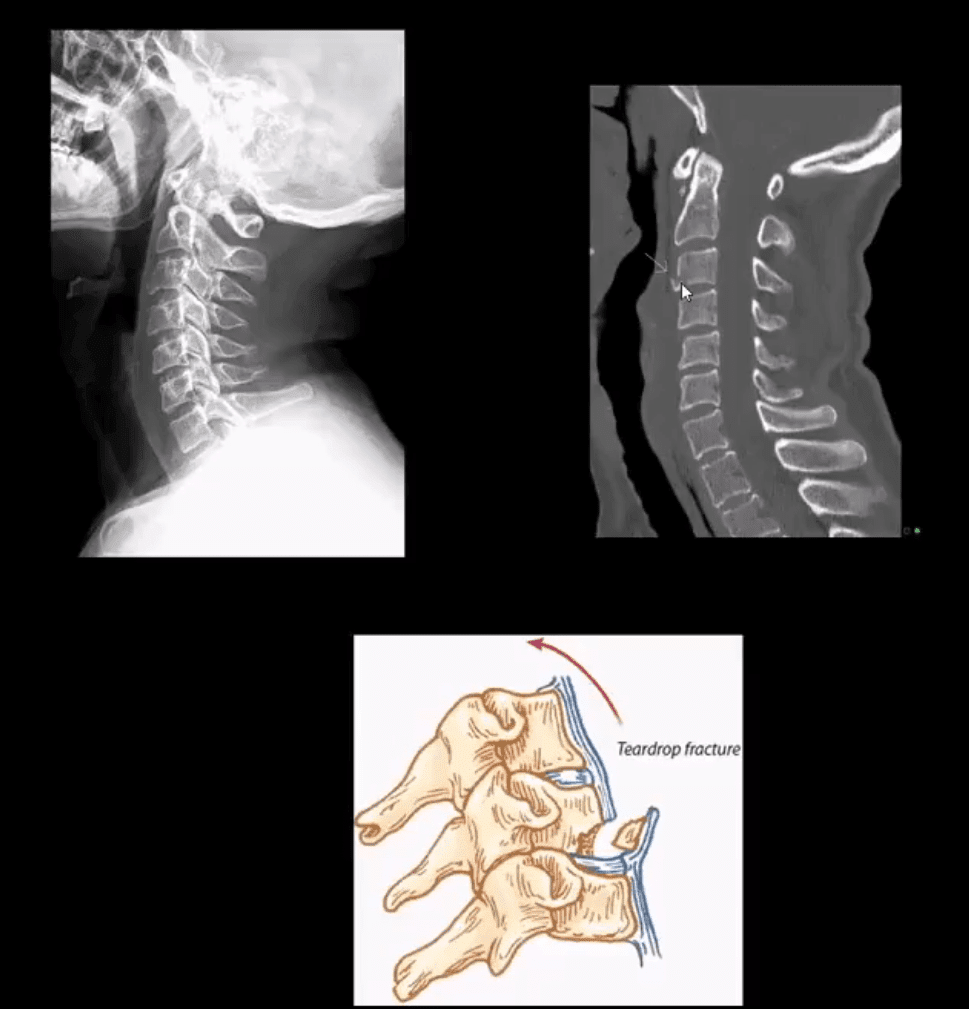
Extension teardrop Fx (stable) potentially unstable if put in extension
Avulsion of an inferior anterior body by ALL. More seen in elderly with superimposed C/S spondylosis
Key radiography: a smaller anterior-inferior body corner, no disruption of ligamentous alignment. Typically at C2 or C3 due to sudden hyperextension and ALL avulsion
Complication: central cord syndrome (m/c incomplete cord injury) esp. in superimposed spondylosis and canal stenosis by the laxity of ligamentum flavum and osteophytes
Management: hard collar isolation
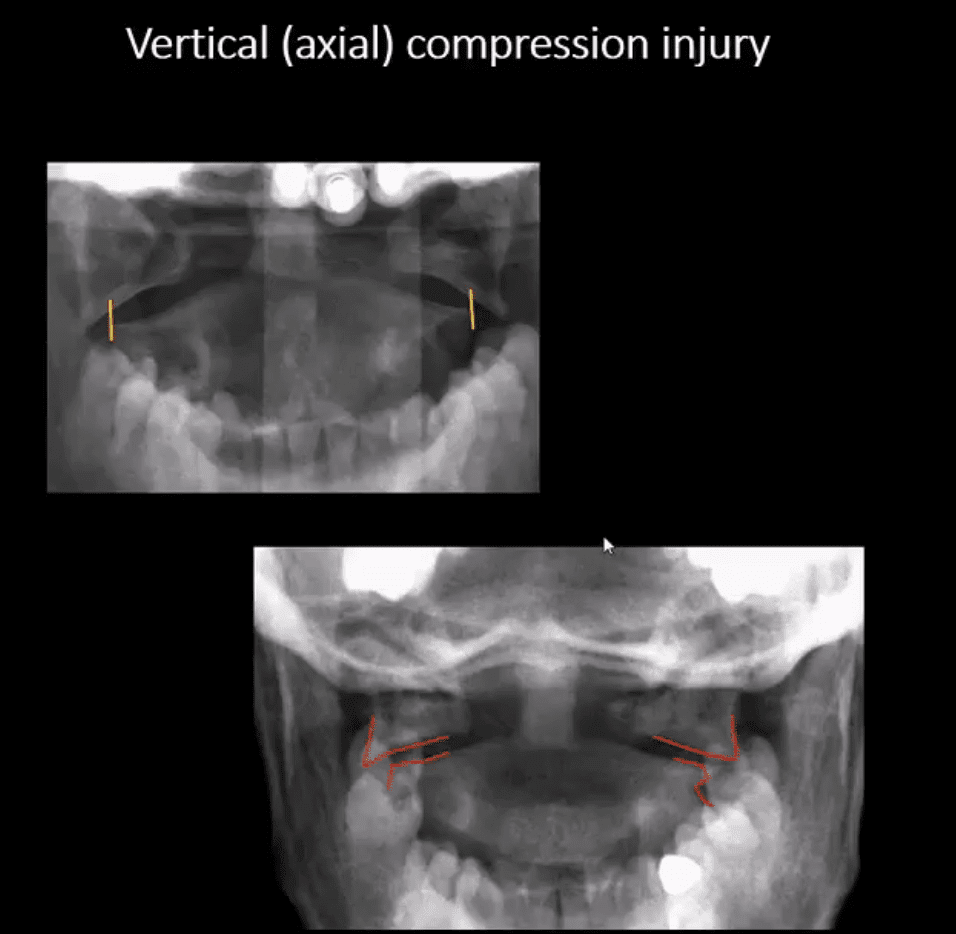
Vertical (axial) Compression Injury
Jefferson Fx (named after British neurosurgeon who defined it) (unstable but neurologically intact Fx) 7% of all C/S injuries. Stability is dependent if the transverse ligament is intact or torn, which can be noted by overhanging of C1 lateral masses over C2 >5-mm combined (left image)
Mechanism: C1 compression (e.g., diving into shallow waters) causing burst Fx-classically 4-parts of the anterior and posterior arch of C1. Variations exist.
Complications: 50% show other C/S Fx, 40% show Odontoid C2 Fx esp. if extension and axial loading occur
Imaging: x-radiography followed by CT scanning to evaluate subaxial injury and complexity of C1 injury. Note Jefferson Fx with pillar and transverse foramina fx requiring posterior occipital-cervical fusion (below right image).
Management: rigid collar immobilization if the transverse ligament is intact. Halo brace or fusion if the transverse ligament is ruptured
Cervical Injuries With Variable Mechanisms of Trauma
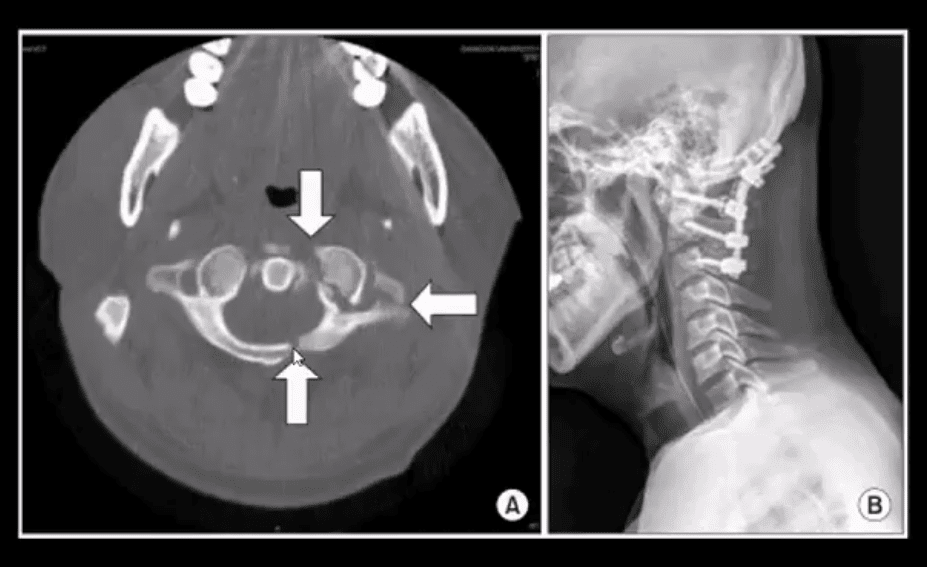
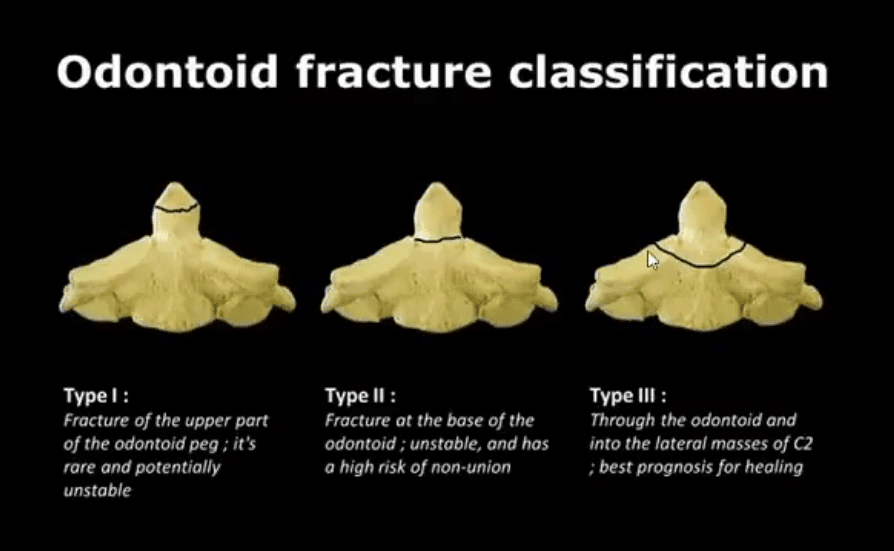
Odontoid process fractures:
These occur�with a variety of mechanisms, flexion, extension, lateral flexion. Elderly with superimposed spondylosis are at higher risk.
Anderson & D’Alonzo classification (below). Type 2 is the most common and most unstable. Type 3 has the best chance of healing d/t more massive bleed into C2 body and better healing potential.
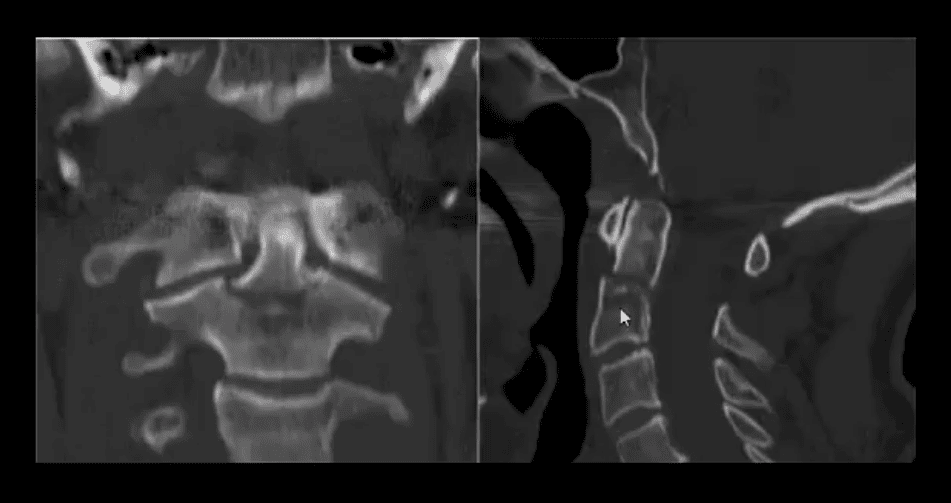
Imaging: x-radiography can miss some Fx. CT scanning is essential.
On x-radiography note tilting of the Dens on lateral and APOM views. CT will reveal the injury and classify it.
Complications: cord injury, non-union
CT scanning: type 2 odontoid fracture (unstable)
Management: type 1 (alar ligament avulsion) most stable�observed and treated with rigid collar.
In young patients, Halo brace is used to treat type 2
Older patients do not tolerate Halo
Operative C1-2 fusion if unstable is Dx and cord signs or other complicating factors are present
Normal Radiographic Variants & Anomalies Simulating Pathology
Pediatric spine appears different especially in children younger than 10-years old.
Normal variations; ADI 5-mm and may increase or decrease on flexed/extended views by 1-2-mm
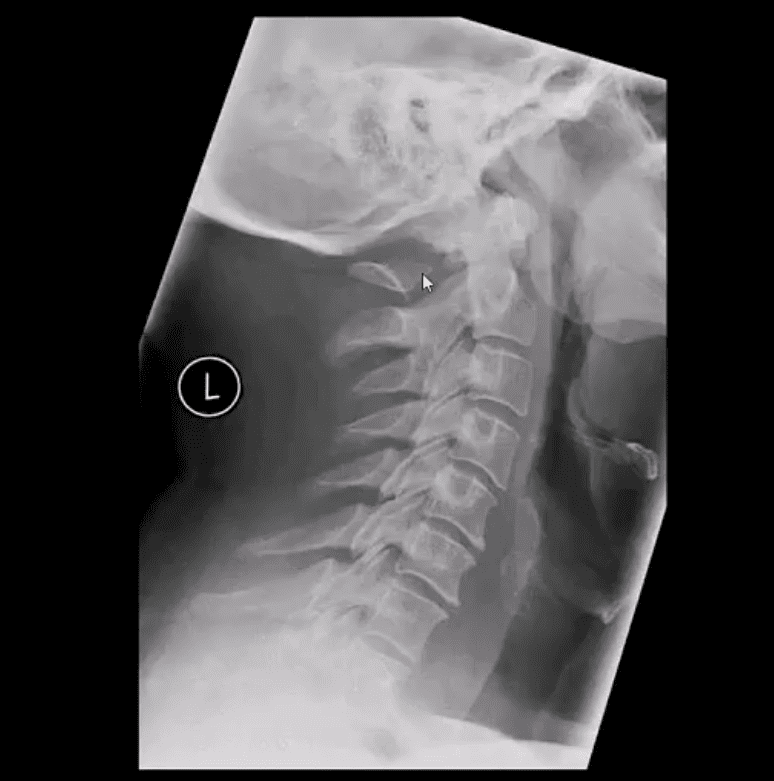
C2-3 may appear as pseudo-subluxation due to normal ligamentous laxity in children (below arrow)
Pediatric vertebral bodies usually are narrower and anteriorly wedged due to the presence of cartilaginous tissue
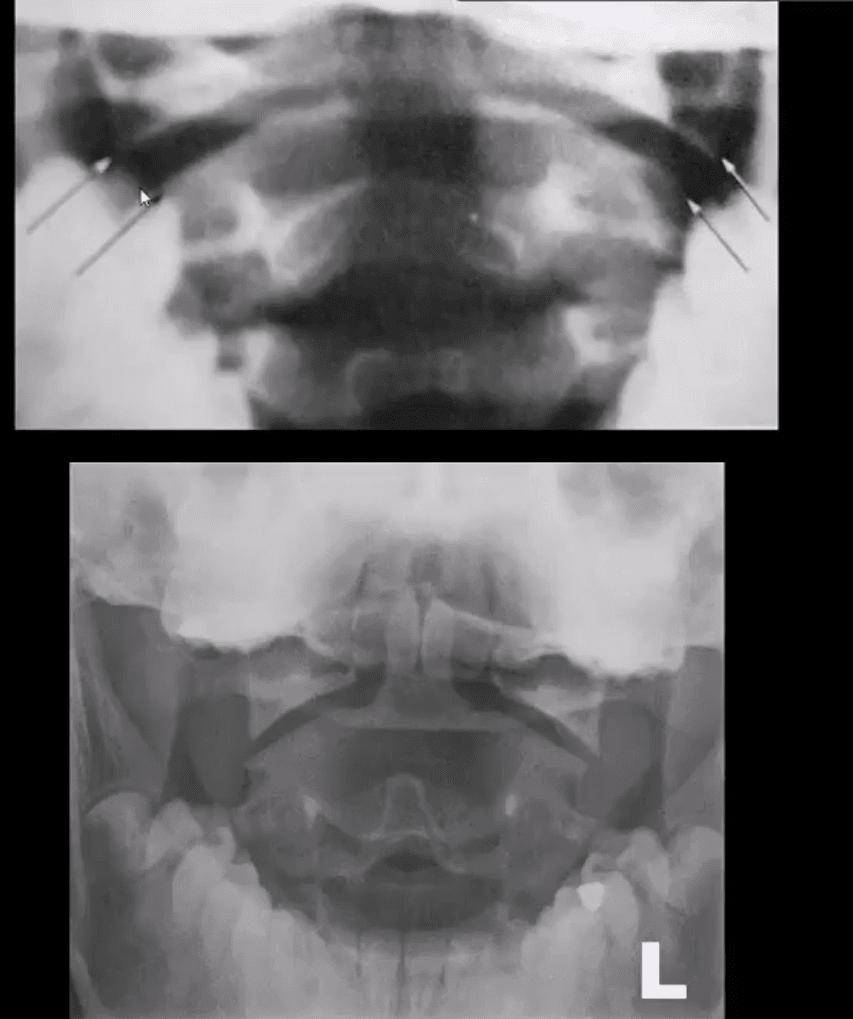
APOM view appears different in children, and some asymmetry of C1 articular masses is normal (below top image) and should not be confused with Jefferson Fx
In adults, any asymmetry or “overhanging” of C1 articular masses is pathological and may indicate Jefferson fx
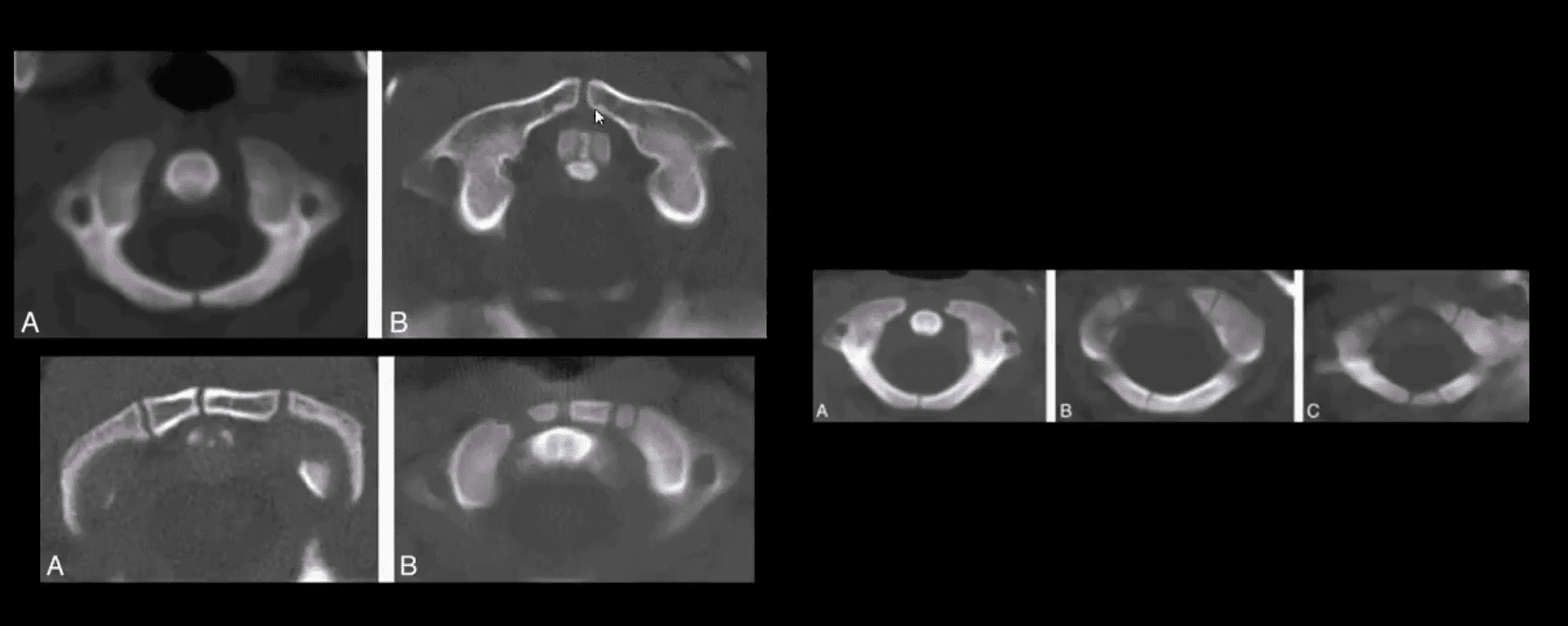
Standard ossification centers of the Atlas synchondrosis in children should not be mistaken for fractures
Persistent ossiculum terminal of Bergman is a typical variant/anomaly of tenacious un-united ossification center and should not be confused with type odontoid fx
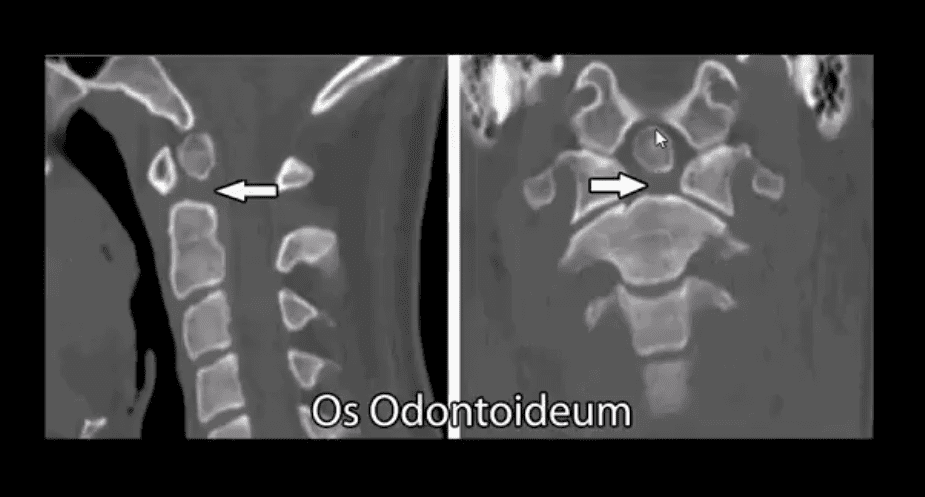
Os odontoideum
Un-united growth center that currently considered as an un-noticed injury that disturbed normal growth in a child younger than 5-years-old
It may be a cause of C1-2 instability and should be evaluated with flexed and extended cervical views
Should not be confused with type 2 Dens fracture because it typically more demonstrates greater mineralization of bone
Incomplete bilateral agenesis of the C1 posterior arch
Anomalous closure of C1 posterior arch
Should not be confused with a fracture
However, local or cord symptoms may develop after trauma in some cases
Relatively rare anomaly developing due to failed chondrogenesis and ossification of posterior ossification centers of the Atlas
Patients with Down syndrome may suffer from increased ligamentous laxity and other abnormalities
Increased risk of subluxation at C1-2
Burst Fx (unstable) 2-columns are damaged
Mechanism: axial loading with frequent flexion after falls and MVAs
The thoracolumbar region is the most vulnerable due to the increased fulcrum of motion
Key radiography: acute compression fracture and�collapse of body height, retropulsion of posterior body and acute kyphotic deformity on the lateral view
On the frontal view: interpedicular widening (below yellow arrow), regional soft tissue swelling (below green arrow)
Imaging: x-radiography should be followed by CT scanning w/o contrast
MRI if neurologically unstable due to cord or conus injury
Complications: cord damage by acutely retropulsed bone fragments
Management: non-operative if neurologically intact and <50% body retropulsed with minimal kyphosis
Operative (fusion) if 50% or more body retropulsed, laminar/pedicle Fx, neuro compromised
18-Year Old Female Following Trampoline Accident
AP & lateral L/S views
Note acute compression fracture, a vertebral body extending to posterior elements
Widening of the inter-spinous distance between T11-T12 (below arrow)
Radiolucent fracture line is seen through the T12 body on the AP projection
CT scanning was performed
Sagittal reconstructed Thoracic and Lumbar CT slices in bone window
Note acute compression fracture, the T12 body extending into pedicle and lamin
Dx: Chance fracture of T12
MR imaging was performed
T2 Wl sagittal MRI
Findings: acute compression fracture T12 body extending to posterior elements causing rapture of interspinous and flavum ligaments
Mild compression of the distal cord above the conus is noted with a minimal signal abnormality
Dx: Chance fracture
Chance Fx aka (Seatbelt Fx) – is a flexion-distraction injury (unstable)
M/C in lower thoracic-upper lumbar
All 3-columns fail: column 3 torn by distraction, columns 1 and 2 fail on compression (Denis classification)
Causes: MVA, falls
Imaging: initial x-radiography should be followed by CT scanning w/o contrast to assess bone fragments retropulsion/canal compression. MRI may help to evaluate potential cord damage and ligaments tearing
Management: non-operative immobilization if neuro intact
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine