Daniel Alvarado, owner of PUSH Fitness, in order to participate in his activities that are physical, he depends on his health. After fighting with shoulder pain during the course of several months, Daniel Alvarado went to visit Dr. Alex Jimenez, chiropractor, to receive shoulder pain rehabilitation. Chiropractic care is a treatment for subluxations, which might be causing symptoms, or an alternative treatment option used to cautiously help restore any misalignments. Dr. Alex Jimenez assisted Daniel Alvarado to enhance his strength, flexibility, and freedom through using spinal adjustments and manual manipulations. Daniel Alvarado was able to come back to his daily physical tasks after receiving shoulder pain rehabilitation together with Dr. Alex Jimenez, chiropractor. Daniel Alvarado highly recommends Dr. Alex Jimenez because he is the non-surgical pick for shoulder pain.
Chiropractic Rehab
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Proximal humeral Fx account for 4-6% of all Fxs. Osteoporotic (OSP) Fx in >60 y.o associated with minimal trauma with F: M 2:1 ratio. In young patients, acute high energy trauma predominates.
Complications: AVN humeral head, Axillary N paralysis.
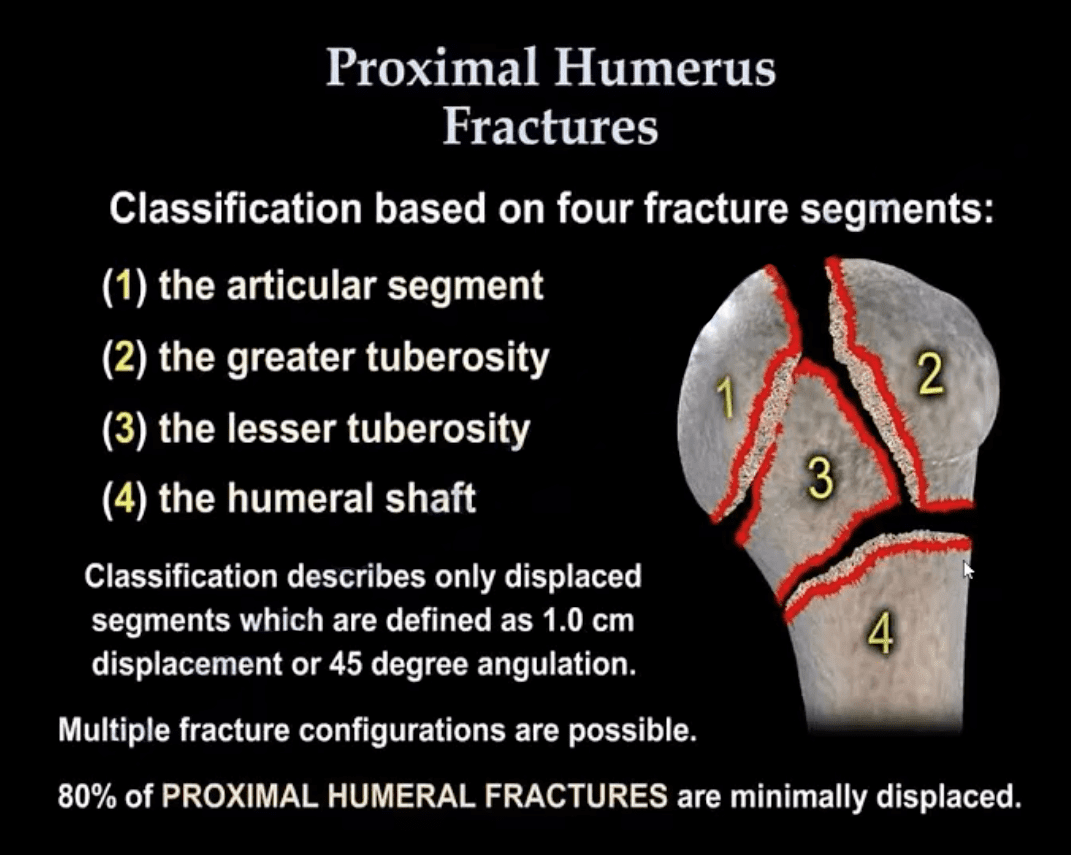
Neer Classification: considers fractures along 4-anatomical lines with or w/o displacement >1-cm & 45-degree angulation
One part Neer Fx- no displacement or very minimal <1-cm/45-degree. Can affect 1-4 lines and M/C at greater tuberosity. 80% of proximal humeral Fx are one-part Neer.
Two-part Fx: 1-part is displaced >1-cm/45-degrees. m/c involves the surgical neck
Three-part Fx: 2-parts are displaced >1-cm/45-degrees.
Four-part Fx: all 4-parts can be displaced. Uncommon <1%
Imaging: 1st step-radiography, CT may be used in more complex cases. Orthopedic referral
Management: Neer one-part Fx is treated with Sling Immobilisation and progressive rehab
The vast majority of Fx in the elderly are treated non-operatively
Younger patients (40-65) may occasionally require hemiarthroplasty if 3 or 4-part Neer Fx present. Greater risk of AVN
Proximal Humerus Fractures
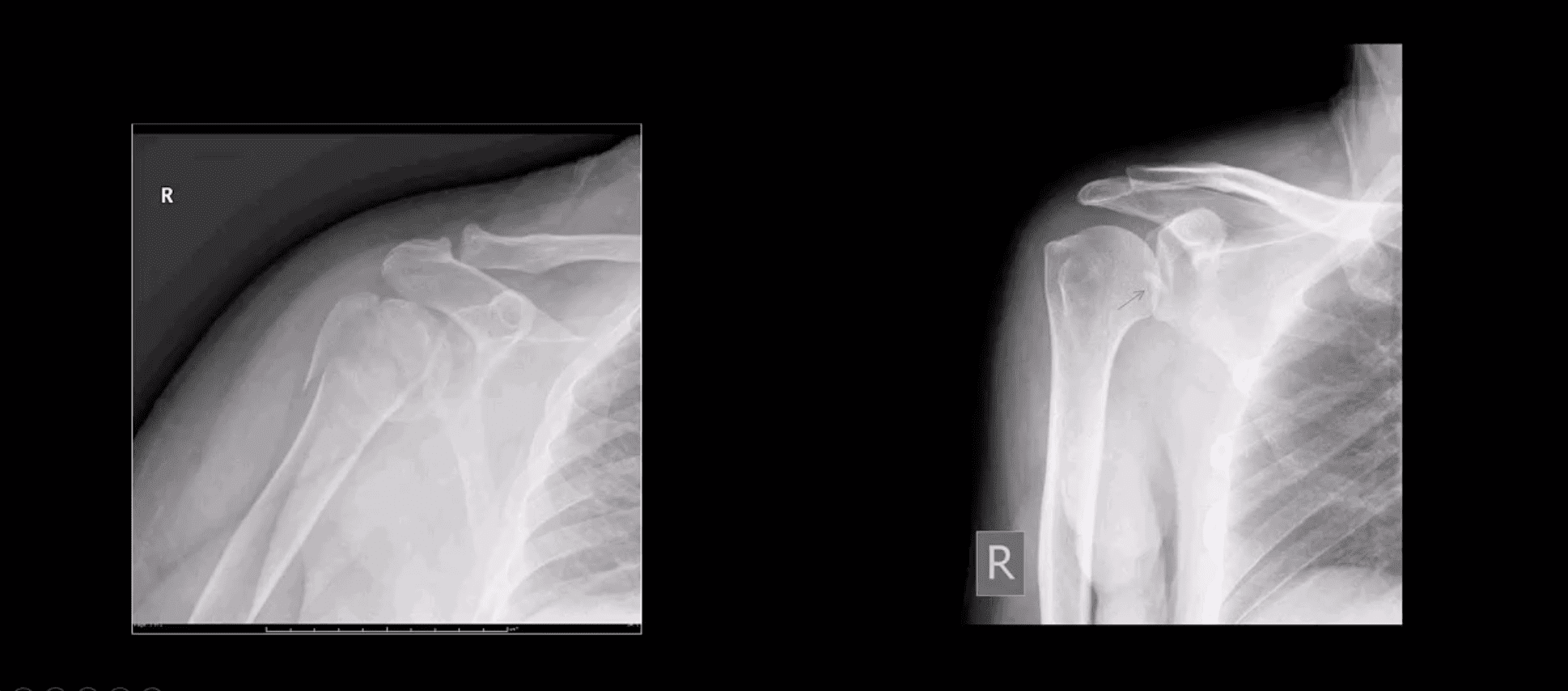
Note: Left image: Fx involving the anatomical neck and the greater tuberosity with minimal displacement <1-cm/45-degree thus Dx as one-part Fx. Right image: Small avulsion Fx of the greater tuberosity with significant displacement (>45-degrees & 1-cm) thus Dx as two-part Fx
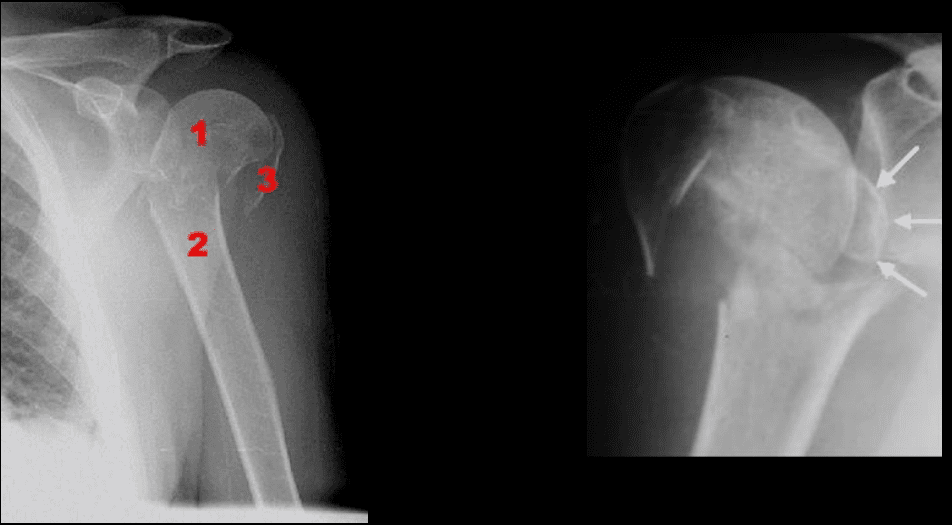
Note: three-part Neer Fx (left) and four-part Neer Fx (right)> Management: operative in most cases in younger (40-65) patients
Refers to complete separation of the humerus from scapula glenoid. In 20-40s M: F 9:1 ratio, in60-80S M: F 3:1
Anatomy: Shoulder stability is sacrificed for mobility, and overall GHJD is the m/c among large joints in the body
Protective falls (e.g., FOOSH) and MVA are m/c causes. GHJ is most vulnerable in abduction, extension and external rotation. Anatomical factors: shallow glenoid, laxed ant-inferior capsule and GH ligaments. GHJD will induce severe tearing of major GHJ restraints. Associated osseous and labral injuries are common and may lead to chronic instability, DJD,�and functional changes
3-types: Anterior GHJD (95%)
Posterior GHJD (4%) especially associated with epileptic seizures, electrocution and can occur b/l
Inferior GHJD aka Laxatio Erecta (<1%) associated with severe trauma
Clinically: AGHJD presents with severe pain, the arm is externally rotated and adducted, severe limitation of movement. GHJD may persist as chronic dislocation.
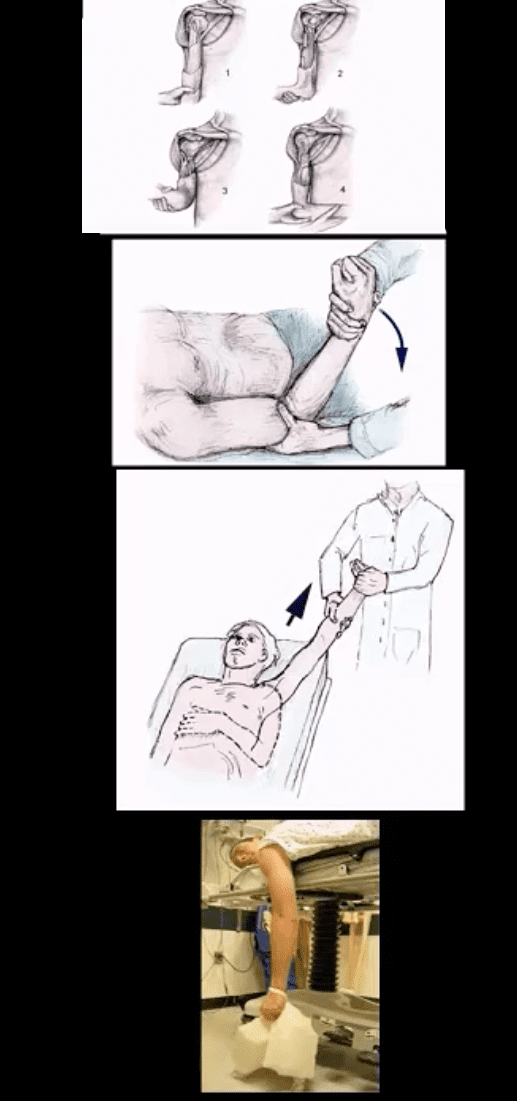
Management: prompt reduction in ED under anesthesia or heavy sedation with Kocher technique top image (not used), External rotation method (middle) or Milch technique (can be used w/o anesthesia) and a few other methods. Delay in reduction correlates with greater risk of immediate and long-term�complications
Diagnostic Imaging Approach
Shoulder series x-radiography is sufficient. Additional Imaging with CT scanning and MRI may be helpful to Dx osseous, cartilage, labral/ligaments pathology
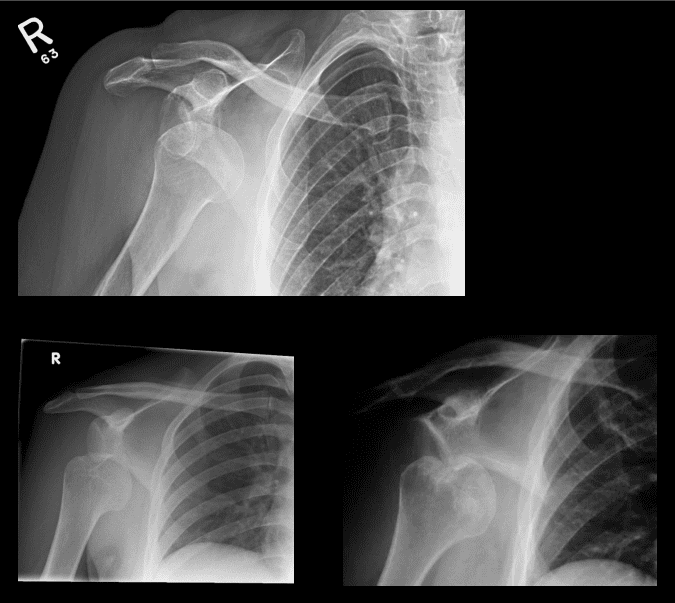
Anterior GHJD (95%). Subcoracoid position(top right) of the humerus is the m/c
Anterior GHJD may also occur as subglenoid(bottom left)and infrequently as subclavicular
Key to radiographic search is to evaluate associated Bankart and Hill-Sachs injuries
Bankart Lesion
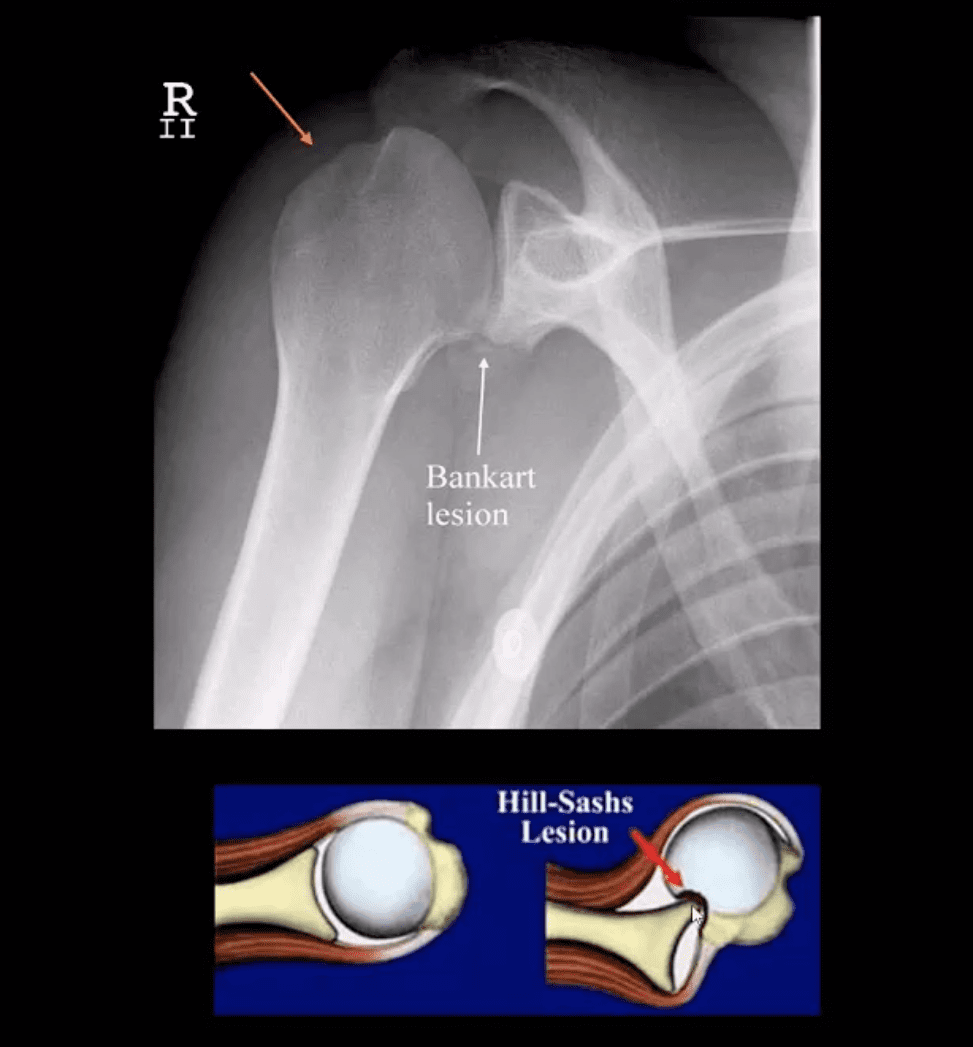
Occurs during anterior GHJD d/t impaction of the head into anterior-inferior glenoid. Variations exist (see next slide). BonyBankart can be seen on x-rays. So-called soft tissue Bankart requires MRI. Cartilage (soft)Bankart is the m/c.
Hill-Sachs aka Hatchet deformity (arrow postreduction)occurs during the same mechanism as Bankart, i.e., compression and impaction of posterolateral aspect of the head against the glenoid producing wedge-shape Fx. Hill-Sachs lesion may predispose to recurrent/chronic GHJD.
Bankart lesion may heal, but operative suture anchors are needed sometimes
CT arthrogram and MRI may be helpful
Types of Bankart Lesion
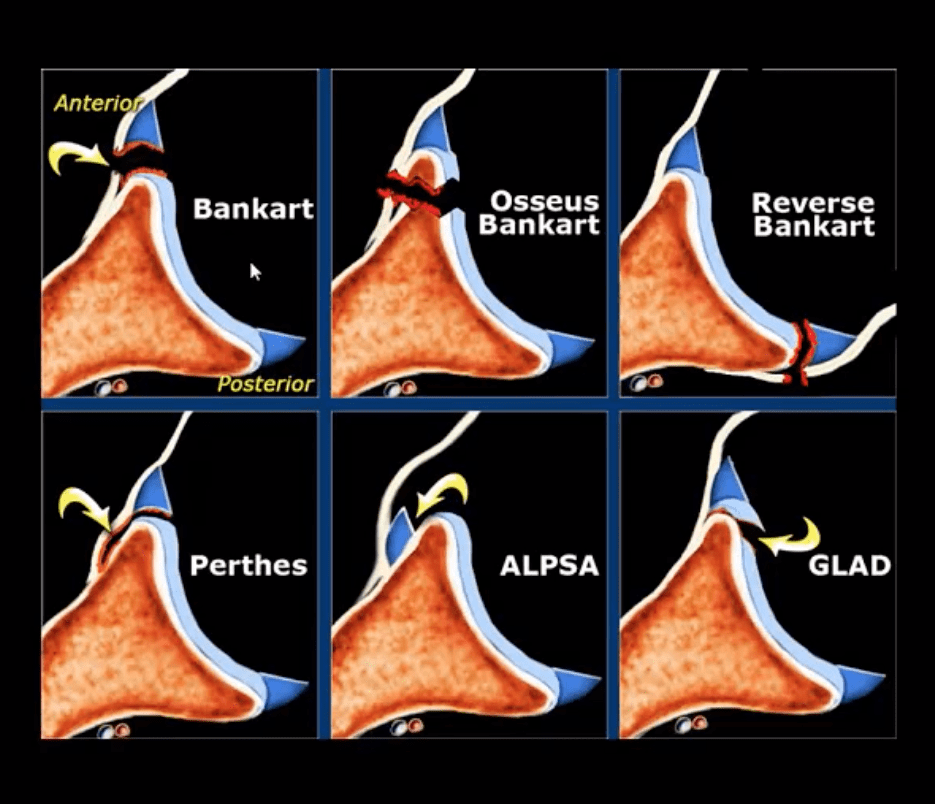
Note different types of Bankart lesion. Onlyosseous Bankart can be seen radiographically. Soft tissue Bankart requires MRI with and without intra-articular gadolinium(arthrogram).
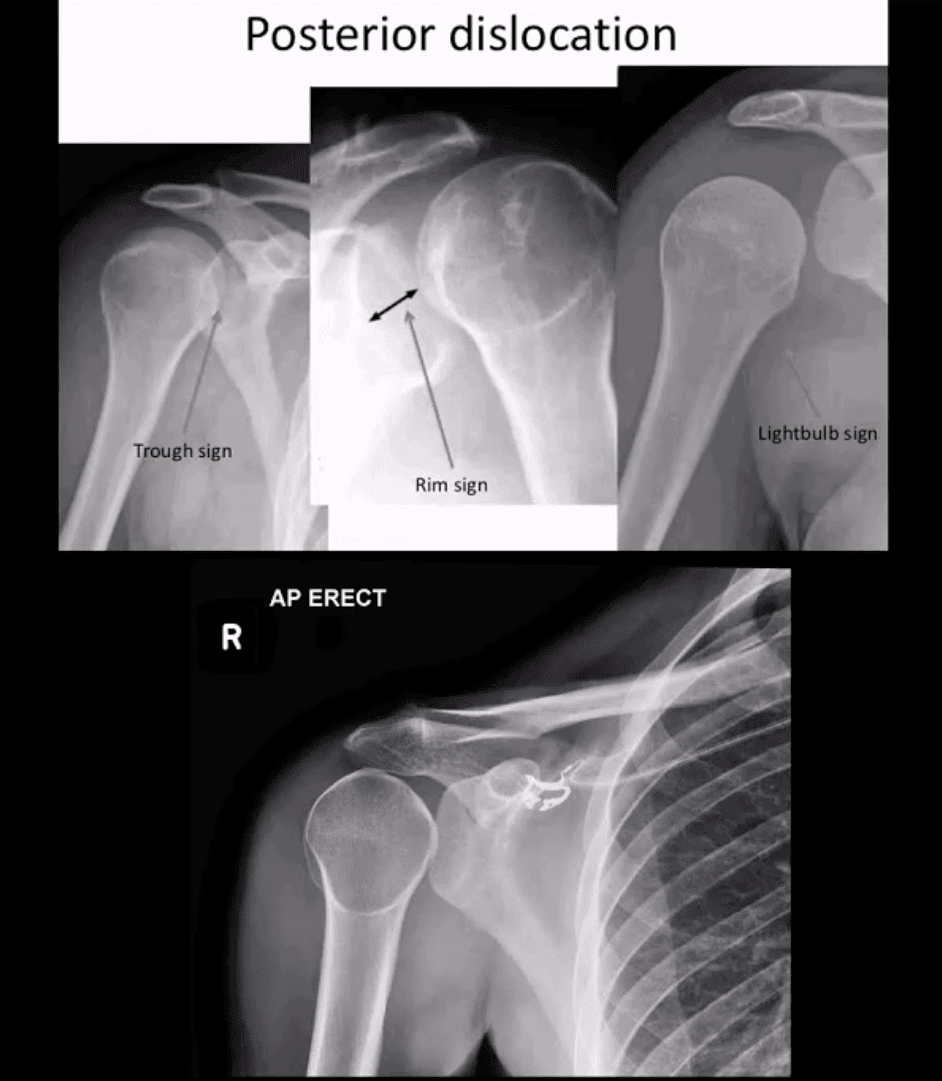
Posterior Dislocation
Note: posterior GHJD with its characteristic signs:
Trough sign aka reverse Hill-Sachs. Occurs d/t anterolateral head impaction Fx
Rim sign: only occurs in the PGHJD d/t posterior position of the head and anterior glenoid-to humeral head distance 6-mm or greater
Light-bulb sign: d/t acute internal rotation of the humerus (head)
Inferior GHJD
Inferior GHJD aka Laxatio Erecta
Severe hyperabduction and inferior displacement of the humerus. Greater chances of severe neurovascular injury and acromial Fx
The dislocated arm is hyperabducted and fixed with the elbow flexed and the arm above the head
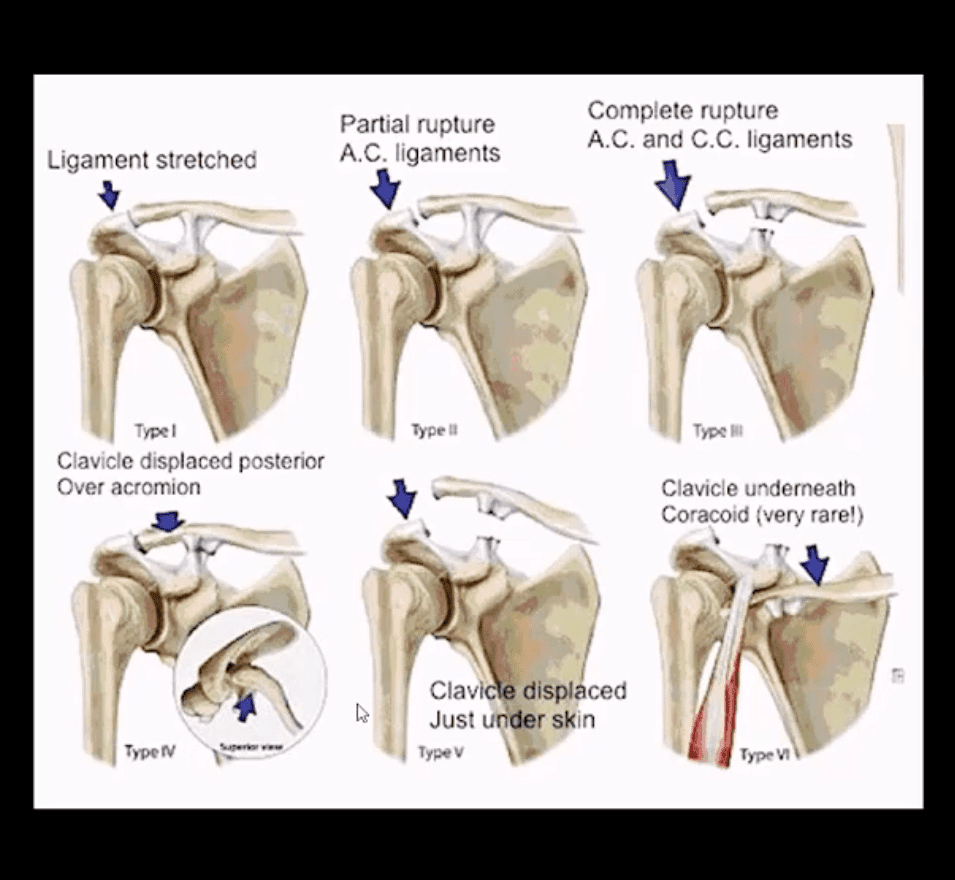
ACJ Dislocation (ACJD)
ACJD: common injury, 9% of shoulder girdle injuries esp. in male athletes by a direct blow
Rockwood classification (left) evaluates tearing of AC and CC ligaments and regional muscles
Type1, 2, 3 among the m/c
Type 1: sprain of ACL w/o tearing
Type 2: tear of ACL and sprain of CCL
Type 3: tear of AC & CCL. The clavicle is elevated above the acromion. If <2-cm good results with conservative Rx.
Imaging: x-radiography with b/l ACJ views with and w/o weights to compare both ACJs. In complex cases CT scanning esp. if Fx is considered
Management: Type 3 (>2-cm) & Types 4-6Operative
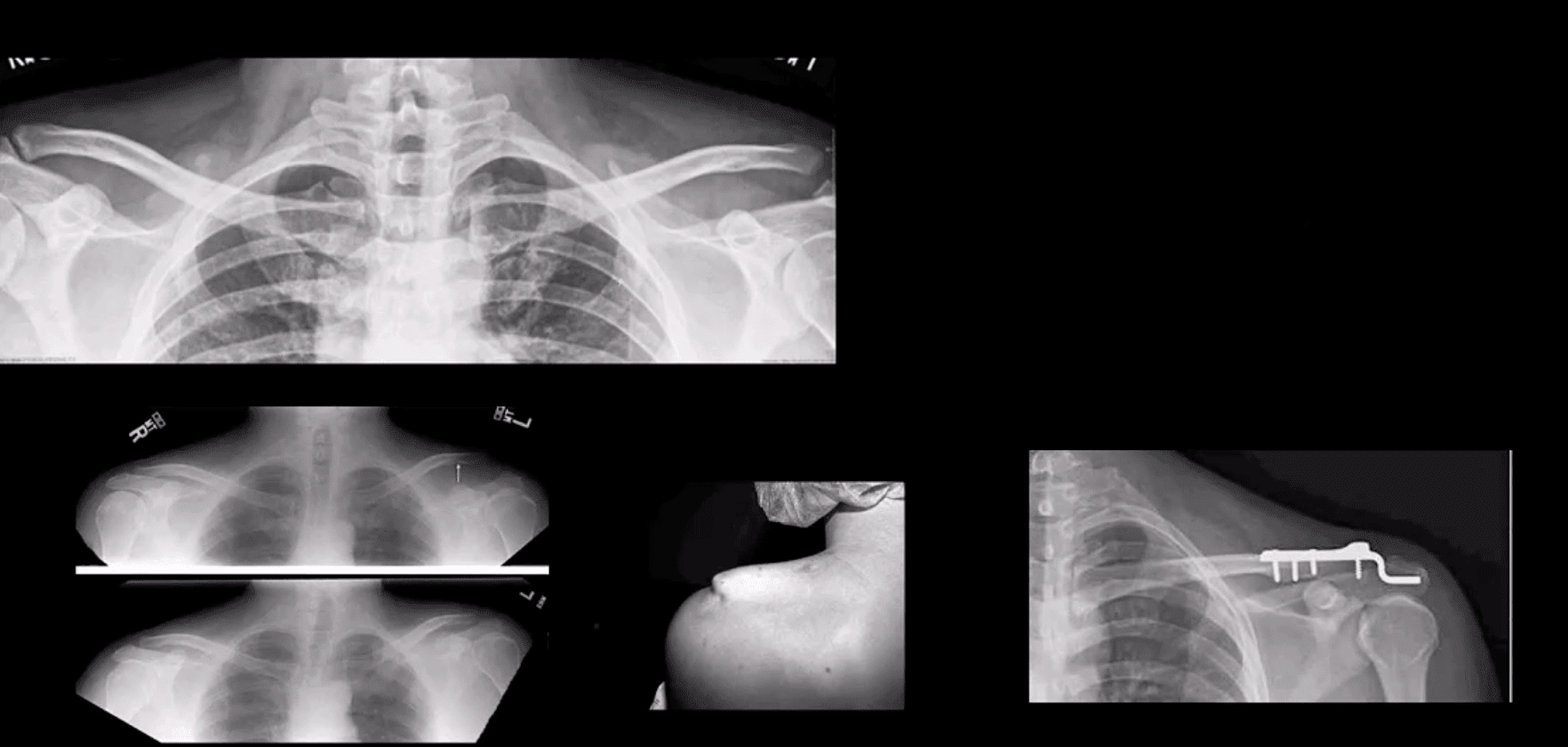
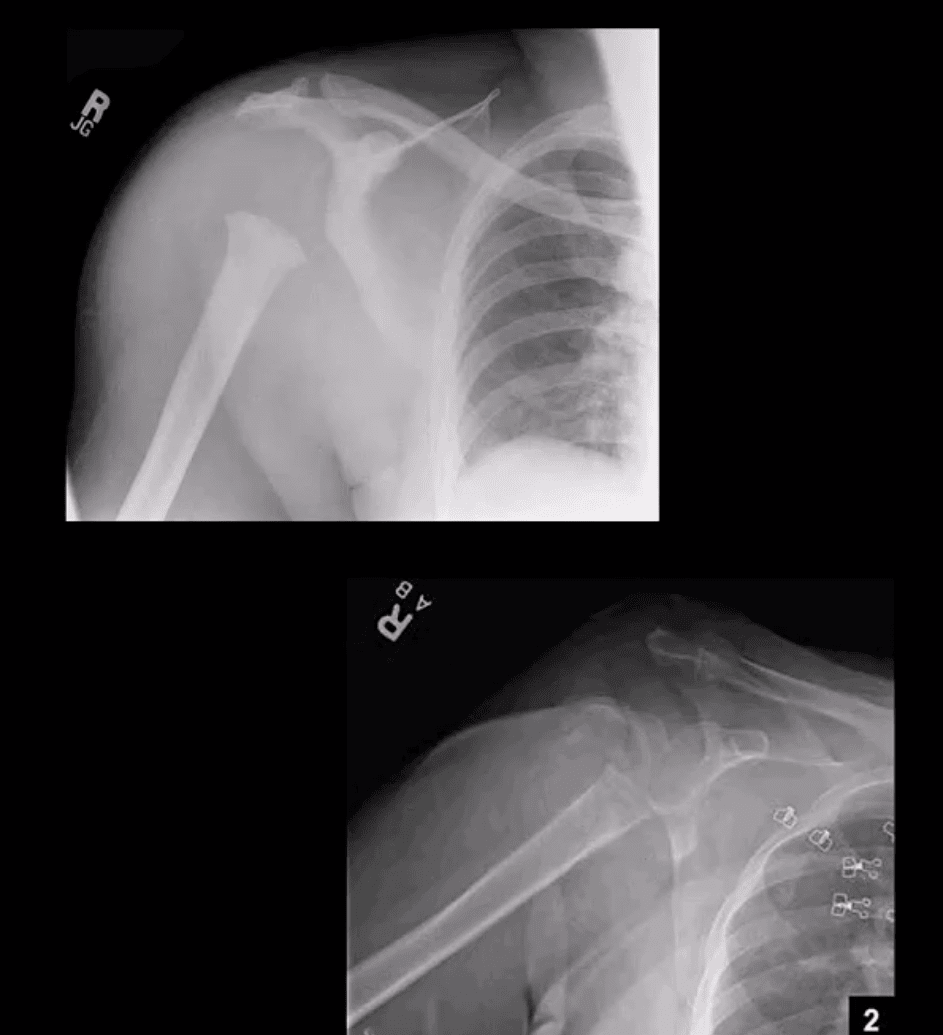
Type 3 ACJ Separation
Type 3 ACJ separation (top left)
More significant ACJD (bottom images) with clinical sign of acromion under the skin and resultant ORIF
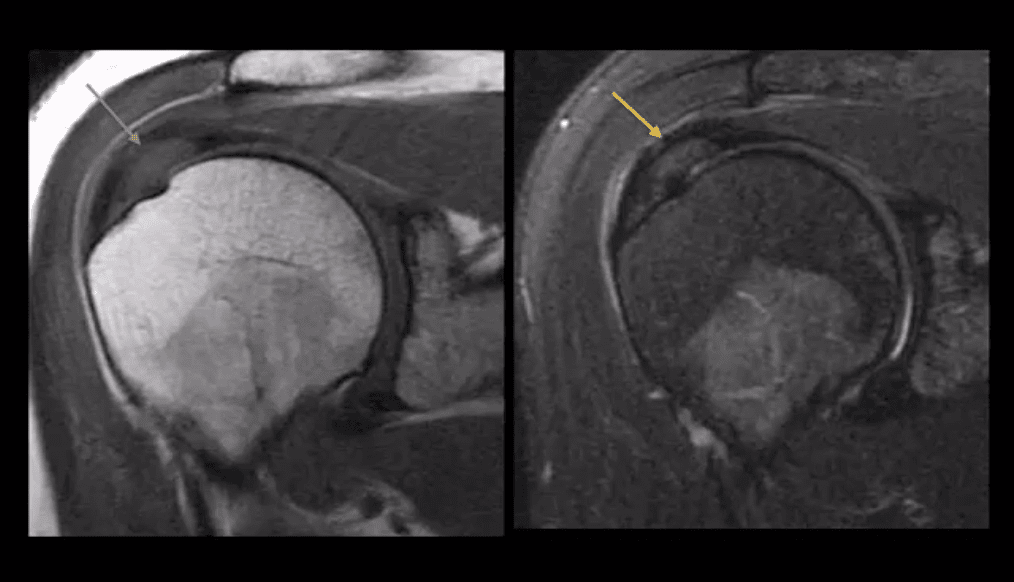
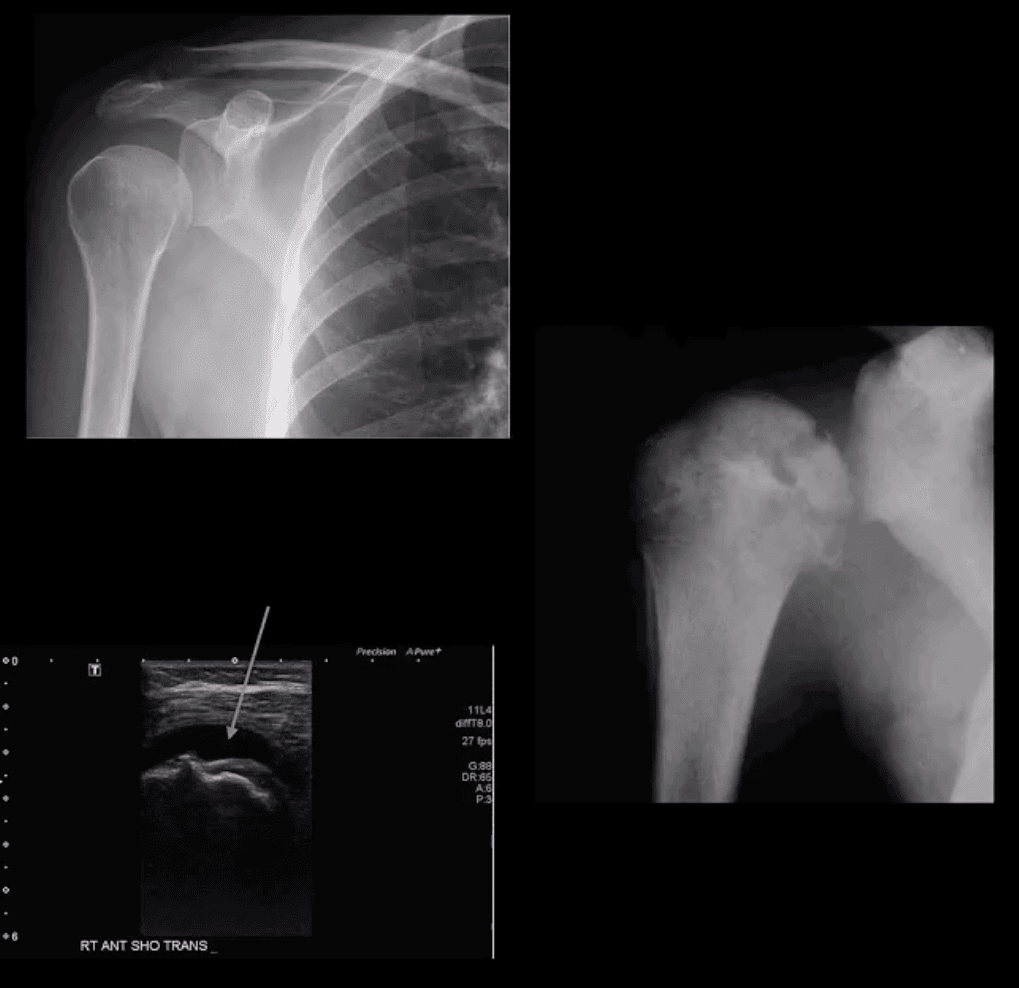
Rotator Cuff Muscles (RCM) Pathology
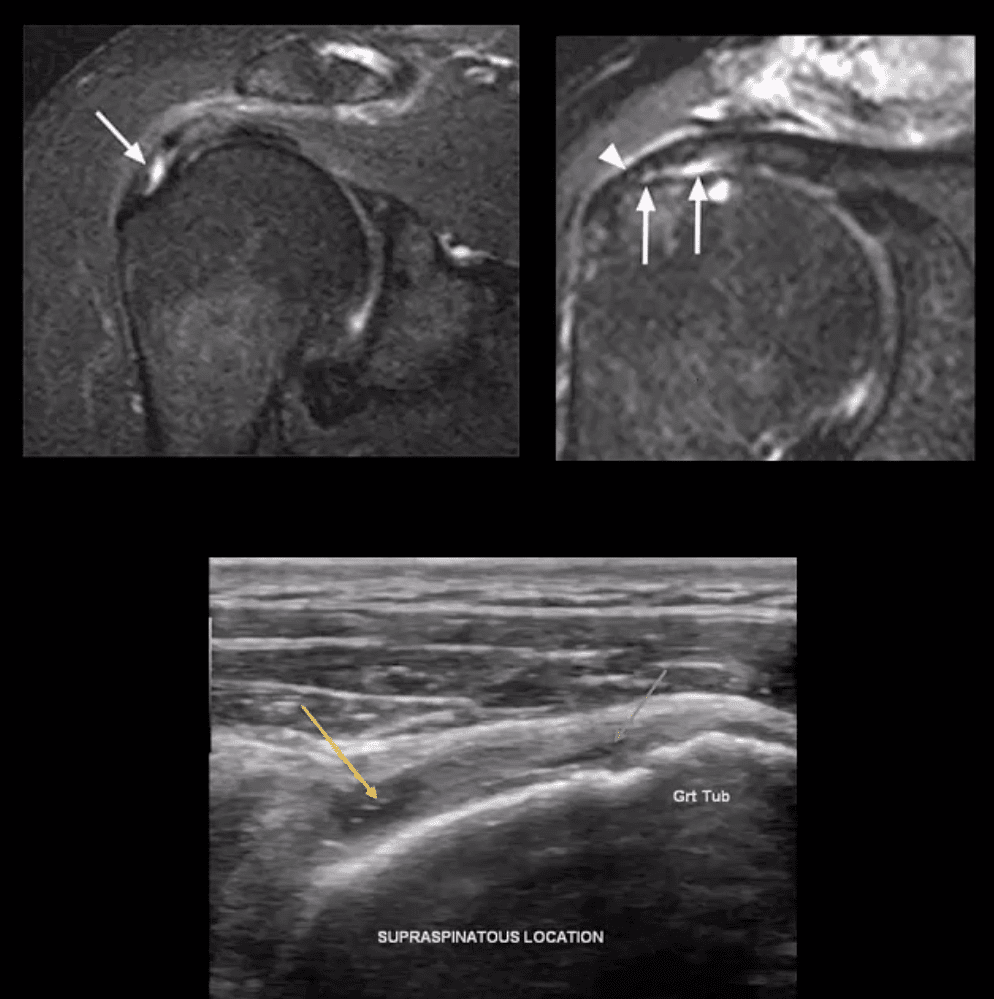
RCM tendinopathy: collagenous degeneration of RCM particularly Supraspinatus M. tendon(SSMT) d/t overuse/degeneration-micro tearing with collagenous replacement. Impingement syndrome is a 2nd extrinsic cause. Presented clinically as pain and limited ROM
Imaging Dx: MSK US can be as accurate as MRI and better in some cases d/t dynamic evaluation v. cost effective
Key MRI clue is thickened inhomogeneous SSMTwith increased signal on all pulse sequences d/t fatty degeneration and inflammation (left images: T1 & T2 FS)
MSKUS findings: thickening of the SSMTsubstance with a change�in normal echogenicity.MSKUS is good to DDx with SSMT tears. US advantages are that it allows dynamic evaluation of painful structures
Partial tear of SSMT: partial (incomplete) tear ofSSMT may occur at the bursal and articular surface or interstitial, i.e., intra-substance/noncommunicating. Etiology: sub-acromial impingement, acute strain, and chronic microtrauma tendinosis
Clinically: pain on abd and flexion, impingement tests, Hawkins-Kennedy tests, etc. Pearls: partial tears can be more painful than complete tears
Imaging Dx: MSKUS is as good as MRI (N.B.some studies indicated MSKUS is more superior to MRI). Key MRI findings: gap/incomplete tear of SSMT filled with joint fluid +/- granulation tissue
MSKUS: decreased echogenicity of SSMT, thinning and partial tearing filled with fluid(anechoic areas arrows). Lost convexity of tendon bursal or articular interface.
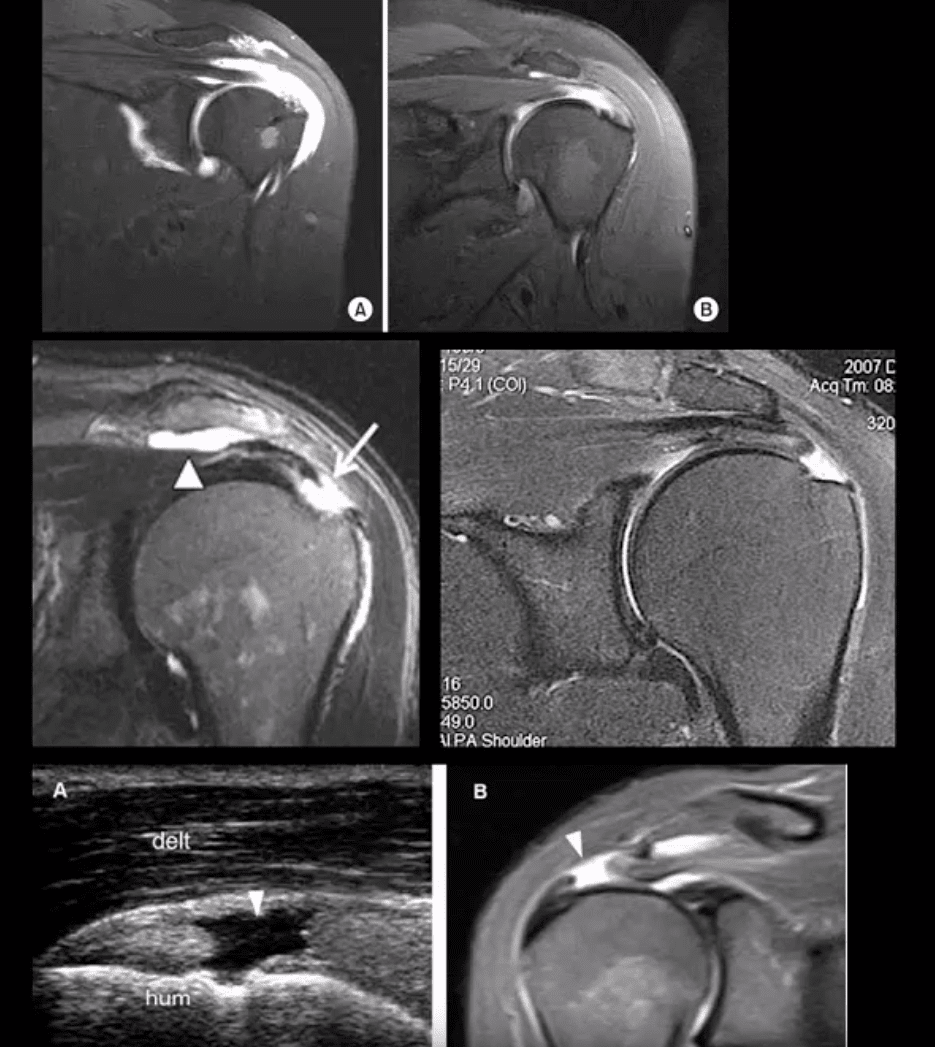
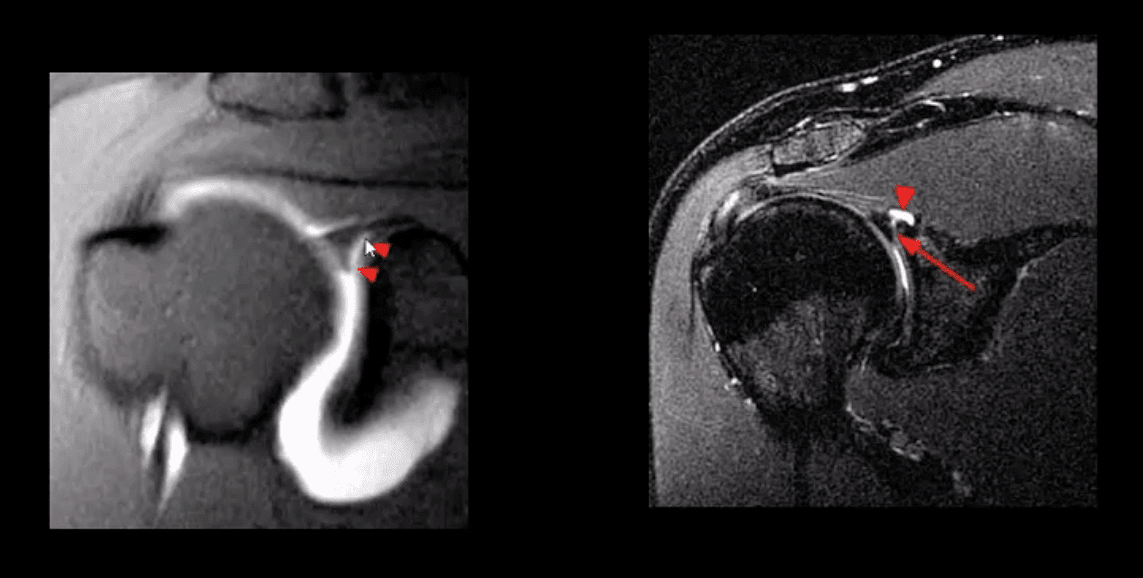
Full Thickness SSMT (rot cuff) tear: degeneration/tearing of rot cuff. 2nd to impingement by Hooked acromion, overhead overuse or acute trauma. 7-25% of shoulder pain in the general population. Clinically: pain on impingement tests.
Imaging Dx: MSKUS is as good as MRI.Limitations: poor Dx of labral pathology. Key USDx: focal tendon interruption, an anechoic gap (fluid filled), hypoechoic tendon, tendon retraction, uncovered cartilage sign (bottom left, A: US B: MRI)
MRI: key Dx: insertional tear extending through entire SSMT crescent, retraction with fatty degeneration of SSMT and the muscle. If retraction is at 12 o�clock or greater (top images), it may not be anchored operatively
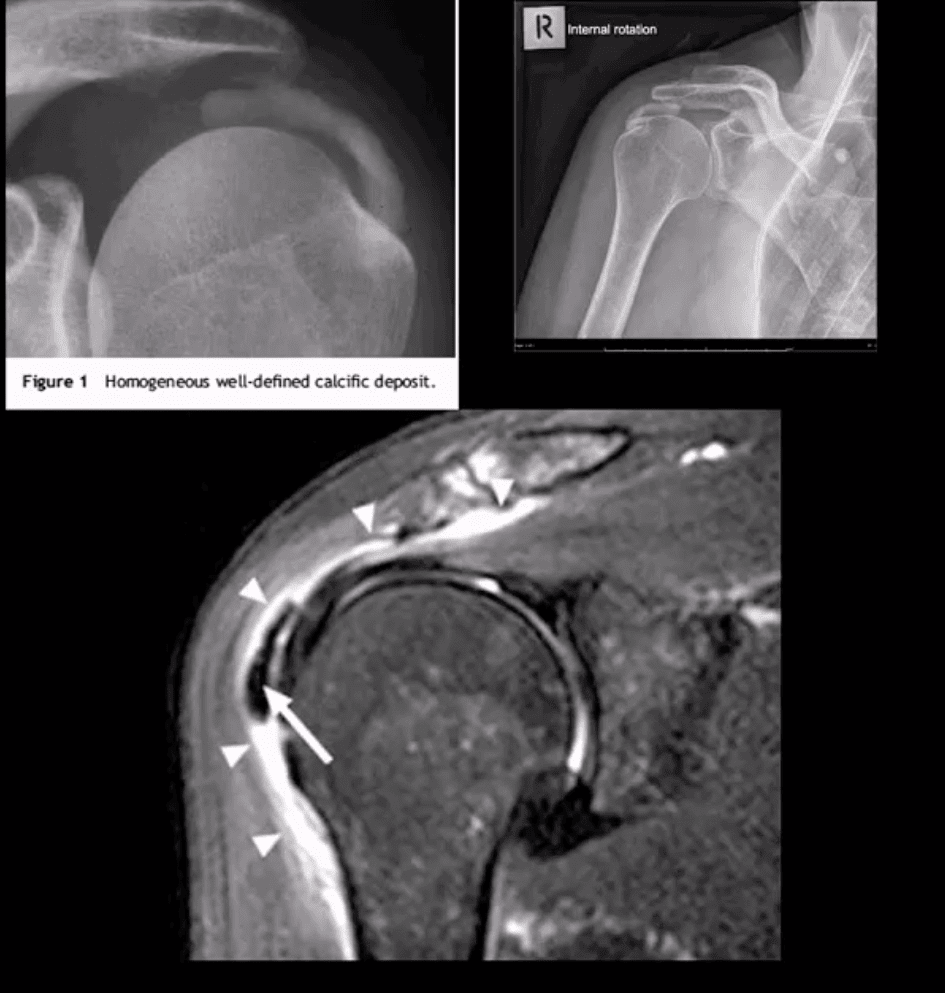
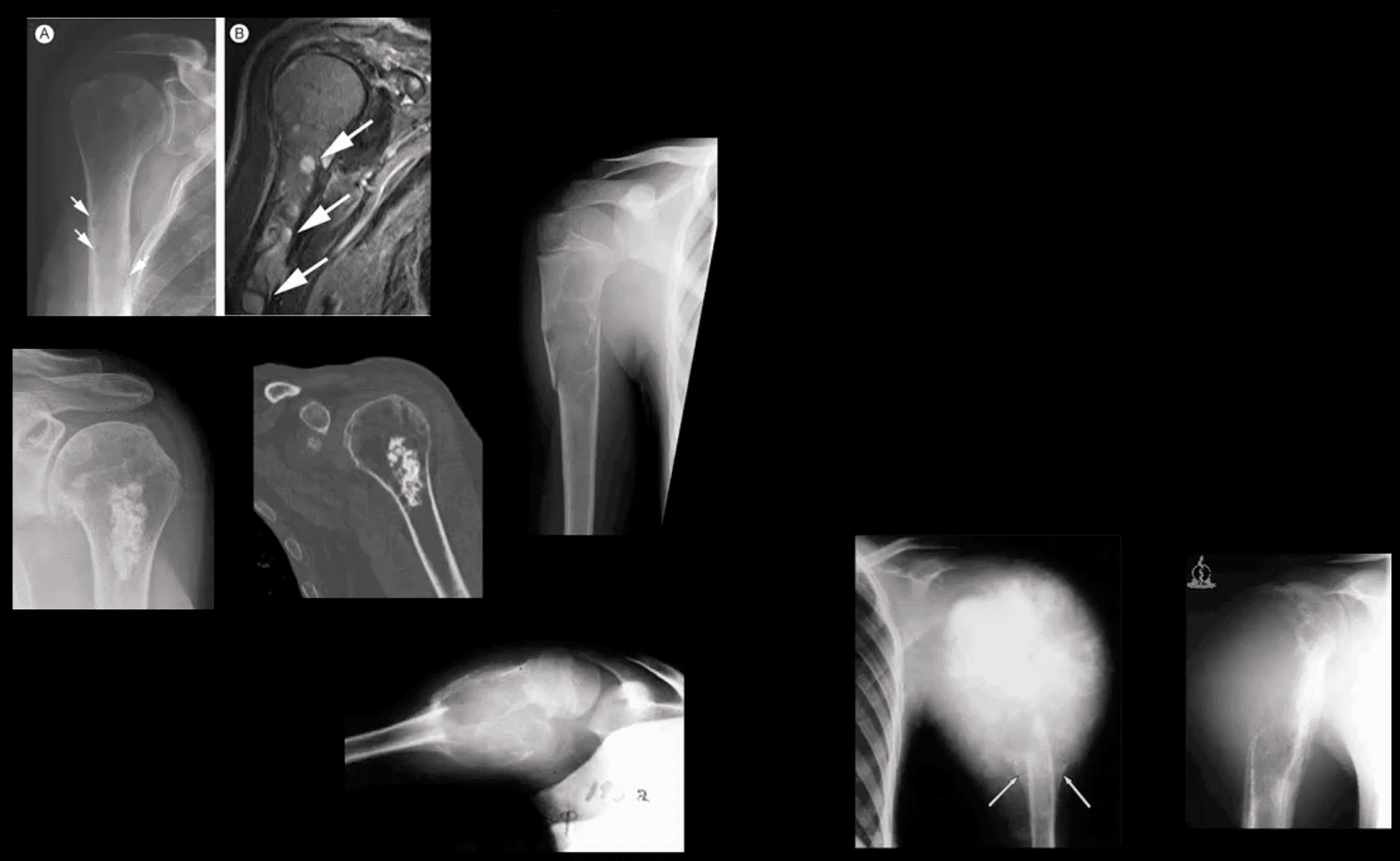
Rotator Cuff (RTC) Calcific Tendinitis: usually d/t calcium HADD crystals. Middle-aged women are most affected. Ranges from asymptomatic imaging finding to severe destructive arthropathy or Milwaukee shoulder(infrequent)
HADD has 3-pathological phases: formation resting-resorption.Mild-to-moderate pain esp. in resting phase.
Imaging: x-radiography: homogenous ovoid mineralization within RTCMT, m/c in SSMT. MRI: ovoid/globular decreased signal on all pulse sequences often with surrounding edema (bottom left)
Rx: self-resolution occurs. Advanced cases: operative aspiration etc.
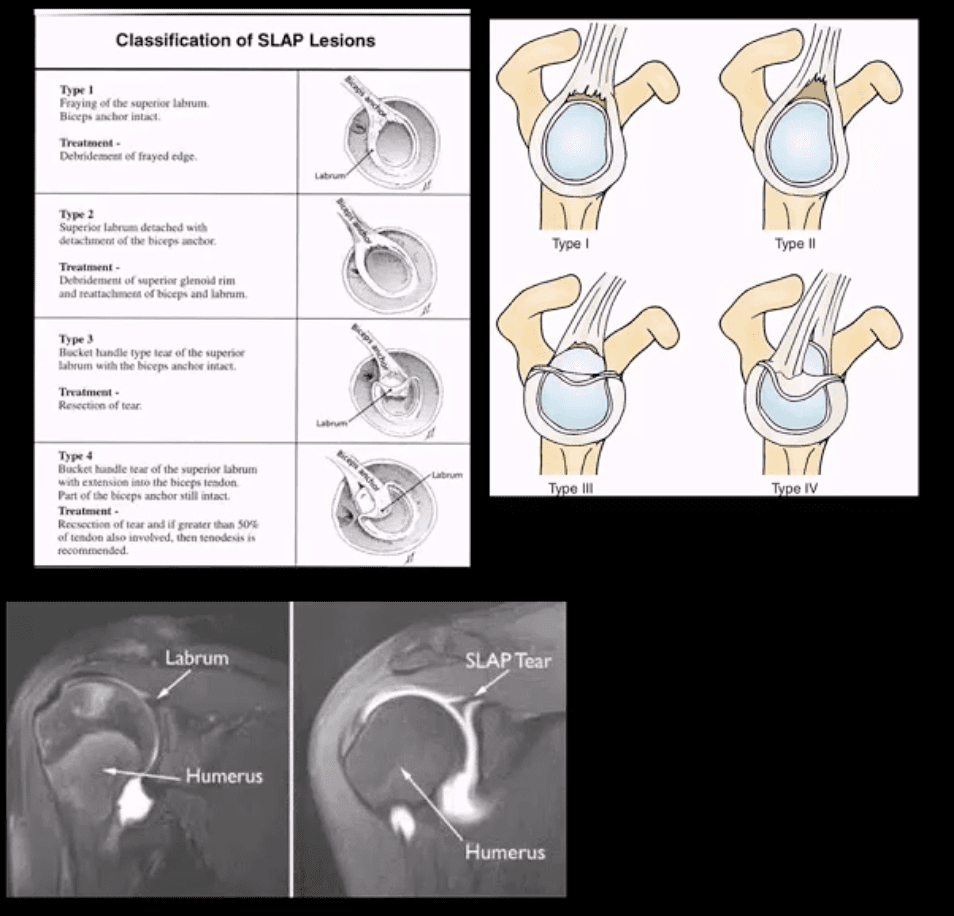
Superior Labrum Anterior to Posterior (SLAP) Lesions/Tears
SLAP tears: FOOSH and throwing sports or chronic shoulder instability aka Multidirectional shoulder instability (in 20%). Type 1-9 exist but the M/C areType 1-4
In all 4-types superior labrum is affected with or w/oLHBMT anchor tear (see pictures). Clinically: pain, limitation of AROM with active compression tests, typically non-specific findings mimicking RTCpathology
Imaging is crucial: best imaging is MRI arthrography. Key signs: hyperintense linear fluid signal within superior labrum +/- extending along the LHBT on fat-suppressed fluid sensitive imaging and FS T1 arthrogram. Best observed on coronal slices.
Rx: small tears may heal, but unstable tears require operative care.
Key DDx: anatomical variants like Buford complex andSub-labral foramen
SLAP tear with a paralabral cyst (bottom right)
Normal variant DDx: sub labral foramen(bottom left) note: MR arthrography with contrast undercutting the labrum but w/o extending posteriorly to the LHBT
Shoulder Arthritis
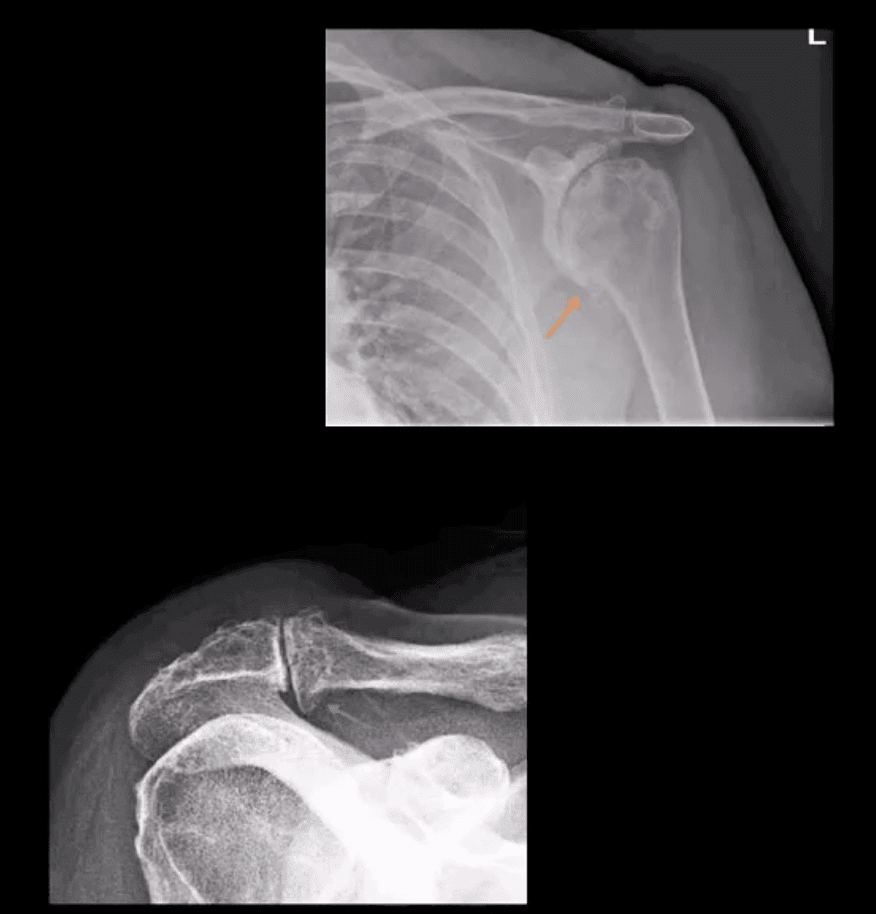
GHJ DJD: usually associated with a 2nd cause: trauma, instability, AVN, CPPD, etc. Presented with pain, crepitus and decreased ROM/function. Associated RTC disease may be present. Imaging; x-radiography is sufficient and provides grading/care planning.Major findings: joint narrowing, osteophytosis esp. at the inferior-medial head (orange arrow), subchondral sclerosis/cysts. Often noted superior head migration d/t RTC disease.
ACJ OA: common and typically primary with aging. Presents with ACJ loss and osteophytes. Osteophytes along the undersurface of the ACJ �keel osteophytes�(blue arrow) may lead to RTC muscle tear. Regional bursitis is other clinical feature of ACJ arthrosis.
Management: usually conservative depending on clinical signs/symptoms
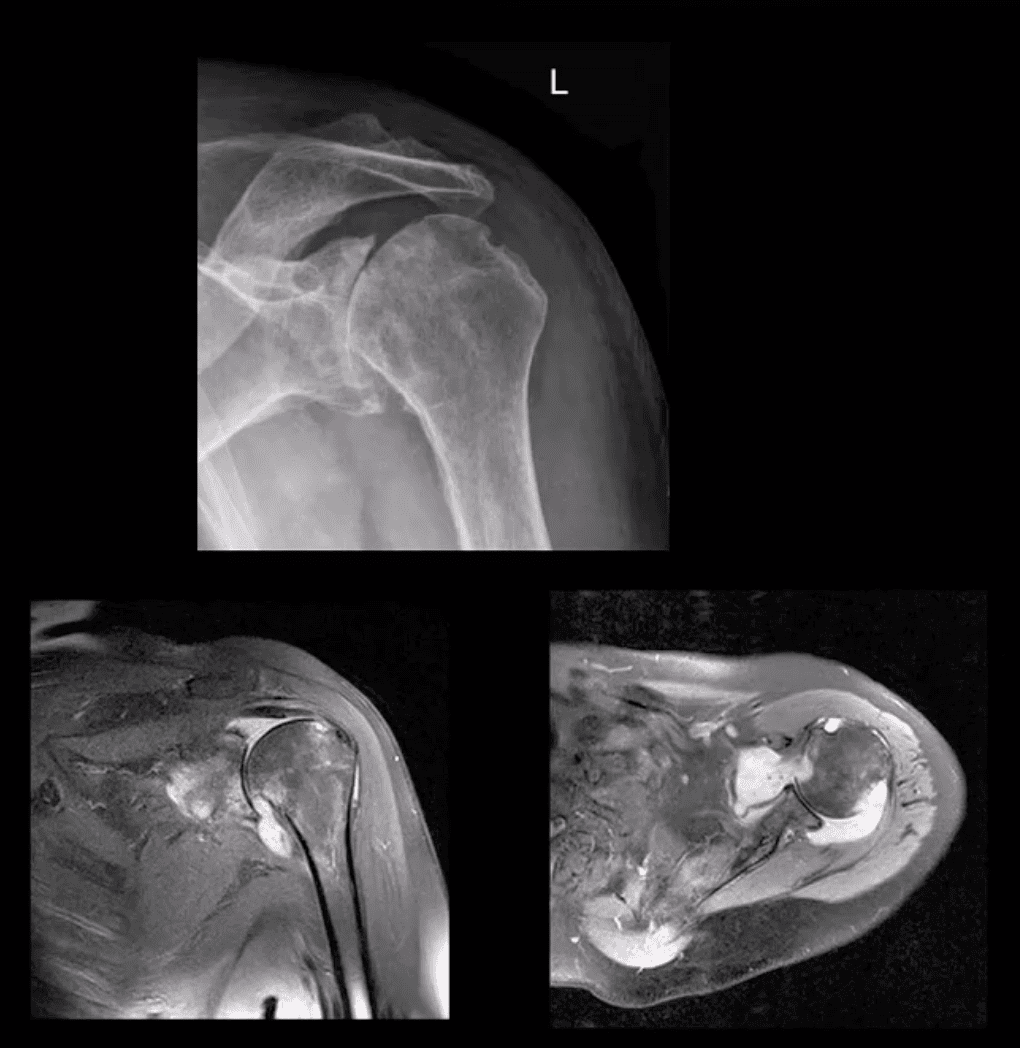
Rheumatoid Arthritis GHJ: RA is a multisystem inflammatory disease affecting multiple joints lined by the synovium. GHJ RA is common (m/c large joints in RA knees/shoulders). Clinically: pain, limited ROM and instability, muscle weakness/wasting. Hands, feet,�and wrists are m/c affected. Imaging: x-radiography reveals periarticular erosions, uniform joint space loss, juxta-articular osteoporosis, subluxations,�and soft tissue swelling. MRI can help detect�commonly associated RTC tearing and instability. Early changes can be detected by MSKUS esp. with power Doppler use indicating hyperemia/inflammation.
Note: L shoulder x-ray revealing cartilage destruction and symmetrical joint loss, multiple erosions, and likely loss of RTCM support with superior head migration, ST effusion present.
Note: PDFS coronal and axial MRI slices of GHJ RA indicating marked inflammatory joint effusion, bone erosion/edema, synovial pannus formation and likely tear in RTC m. Management: Rheumatological referral and pharmacotherapy with DMARD. Operative care asRTCM repair. 10% of patients are disabled d/t RA
Neuropathic Osteoarthropathy aka Charcot’s shoulder: d/t neurovascular and neural periarticular damage. Multiple causes exist.M/c develops in diabetics in midfoot. Shoulder Charcot is m/c in Syringomyelia (25%), trauma paralysis, MS, etc. Dx: clinical(50% pain/swelling 50% painless destruction). Imaging is crucial. X-radiography is sufficient in well-established cases, but early Dx is challenging. MRI may help with early Dx and delayed complications. Rad Dx: Shoulder Charcot is m/c presented as atrophic type destructive arthropathy with humeral head appearing as if surgically amputated along with intra-articular debris, density, distention, dislocation, and other key features
Septic Shoulder: shoulder is the 3rd m/c followingknee>hips. Patients at risk: diabetics, RA pts, immunocompromised, I.V. drug users, indwelling catheters, etc. Routes: hematogenous (m/c), direct inoculation (iatrogenic, trauma etc.) adjacent spread(e.g. OM). Staph. Aureus (>50%) m/c.
Clinically: joint pain and dec. ROM, fever 60% only, toxemia, inc. ESR/CRP. Dx: imaging and joint aspiration/culture. RadDx: early x-rays often unremarkable except ST effusion/fat planes obscuration, joint widening. Later7-12 days patchy osteopenia, moth-eaten/permeating bone resorption, articular destruction, joint narrowing. May progress to severe joint destruction and ankyloses. Early Dx & I.V. antibiotics are crucial even before culture. Operative irrigation and joint drainage in some cases. Complications are possible esp. if Rx is delayed. MSKUS with needle aspiration may help. Note: (top image) non-traumatic joint widening with inferolateral head displacement d/t septic A dx: by needle aspiration Staph. Aures.
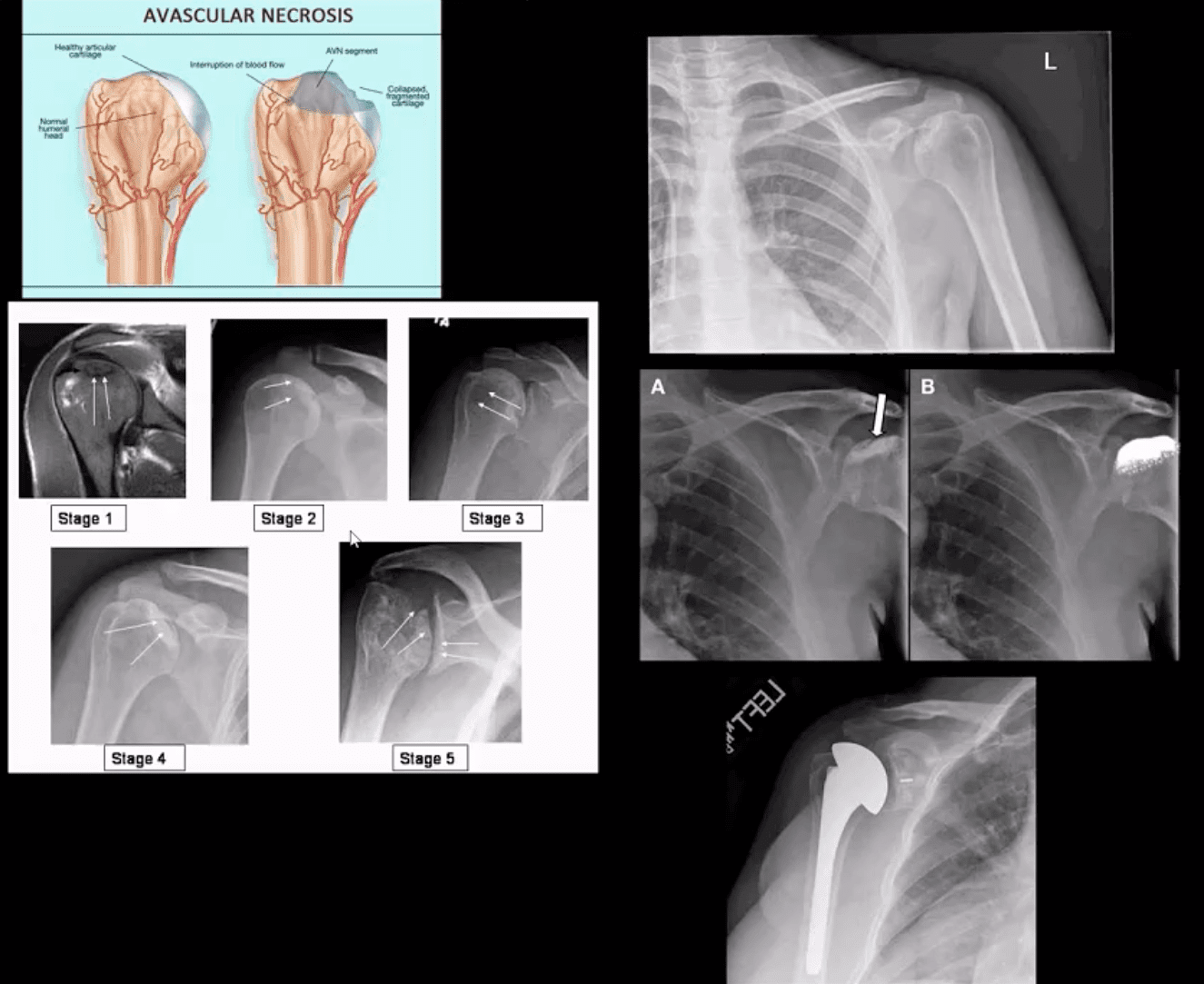
Ischemic Osteonecrosis
Ischemic Osteonecrosis of the humeral head may occur d/t trauma (Neer four-part Fx), Steroids, Lupus, Sickle cell, Alcoholism, Diabetes,�and many other conditions. Imaging is crucial: MRI detects earliest changes as intraosseous edema. X-ray features are late, presented as a collapse of subchondral bone with sclerosis �snow cap� sign, fragmentation, and progressive severe DJD
Management: orthopedic referral, core decompression in early cases, hemiarthroplasty in moderate and total arthroplasty in severe cases.
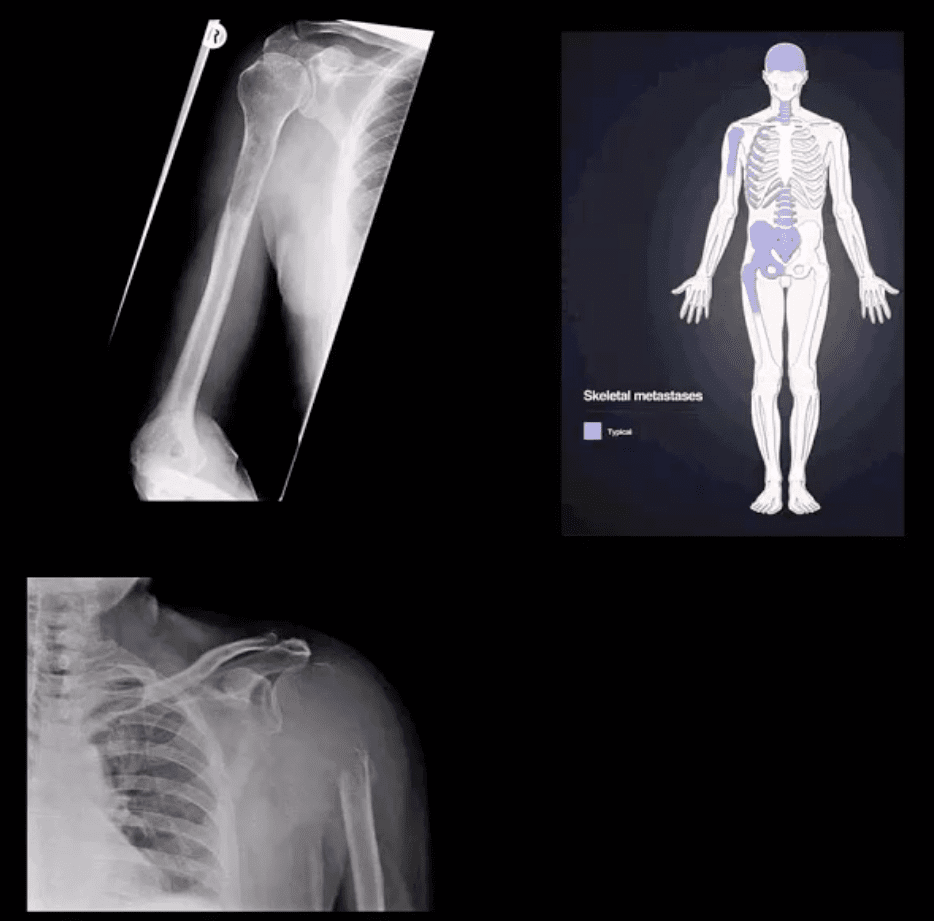
Shoulder Neoplasms
In adults >40, bone Mets d/t lung, breast, renal cell, thyroid CA & prostate are the m/c causes. Clinically: may mimic pain resemblingRTC/joint changes. Should be evaluated carefully. Key to Dx: Hx, PE and Imaging esp.in pts with known primary
Imaging: 1st step x-rays, MRI can help, Tc99bone scintigraphy helps to detect regional and distant disease. X-ray features: destructive lytic changes typically in prox humerus(red marrow) with or w/o path Fx. DDx: Mets, MM, lymphoma
Clinically: night pain, pain at rest, etc. Lab tests: unrewarding, in severe cases hypercalcemia may be noted.
Primary Malignant bone neoplasms (shoulder) Adults: M. Myeloma or Solitary plasmacytoma, Chondrosarcoma may transform from an enchondroma and some others. In children/teenagers: OSA vs. Ewing�s
Primary benign bone neoplasms (shoulder). Adults: Enchondroma (patients in their 20-30s)GCT. In children: Simple bone cyst (Unicameral Bone cyst), Osteochondroma, Aneurysmal Bone Cyst, Chondroblastoma (rare)
Imaging: 1st step x-radiography
MRI is essential to Dx. Especially in cases of primary malignant neoplasms Evaluate extent, soft tissue invasion, preoperative planning, staging, etc.
Roberto Varela was always actively involved with chores at home before he started to experience neck, shoulder and leg pain. Due to his symptoms, Mr. Varela had difficulties engaging in regular physical activities, such as driving. However, after being recommended by his wife, he first received chiropractic care with Dr. Alex Jimenez, and Roberto Varela experienced tremendous relief from his neck, shoulder and leg pain, regaining his quality of life. Mr. Varela highly recommends Dr. Alex Jimenez and his staff for their services.
Shoulder Pain Treatment
Shoulder pain or leg pain is common; however, sometimes these problems don’t originate in the location of the symptoms. Shoulder and leg pain may also occur due to health issues in the neck or cervical spine. A variety of injuries and conditions can have their roots in improper posture, sports injuries or automobile accident injuries, causing misalignments, or subluxations, in the cervical spine or neck. Many healthcare professionals will discuss how damage to the cervical spine can be an underlying cause for shoulder pain and leg pain, among other symptoms.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
On my first visit, I automatically felt better but along came with soreness. I did continue treatment, I saw him (Dr. Alex Jimenez) maybe two or three times out of the week. Shortly after that I started noticing change.�
Denise
The shoulder consists of a number of joints which merge together with other complex structures, including muscles, tendons and ligaments, to provide a wide range of movement in the arm, like scratching your back.
This increased range of motion, however, can cause a variety of health issues. It might lead to problems with impingement or it might even result in instability on the bony structures or the soft tissues of the shoulder. Shoulder pain might be felt continuously or it might occur through movements of the shoulder. Moreover, shoulder pain can be temporary or it might become chronic and require proper diagnosis and treatment.
The article below describes a few of the common causes of shoulder pain and discusses various treatment approaches to help improve shoulder pain. A qualified and experienced healthcare professional may be able to provide you with more information regarding your shoulder pain.
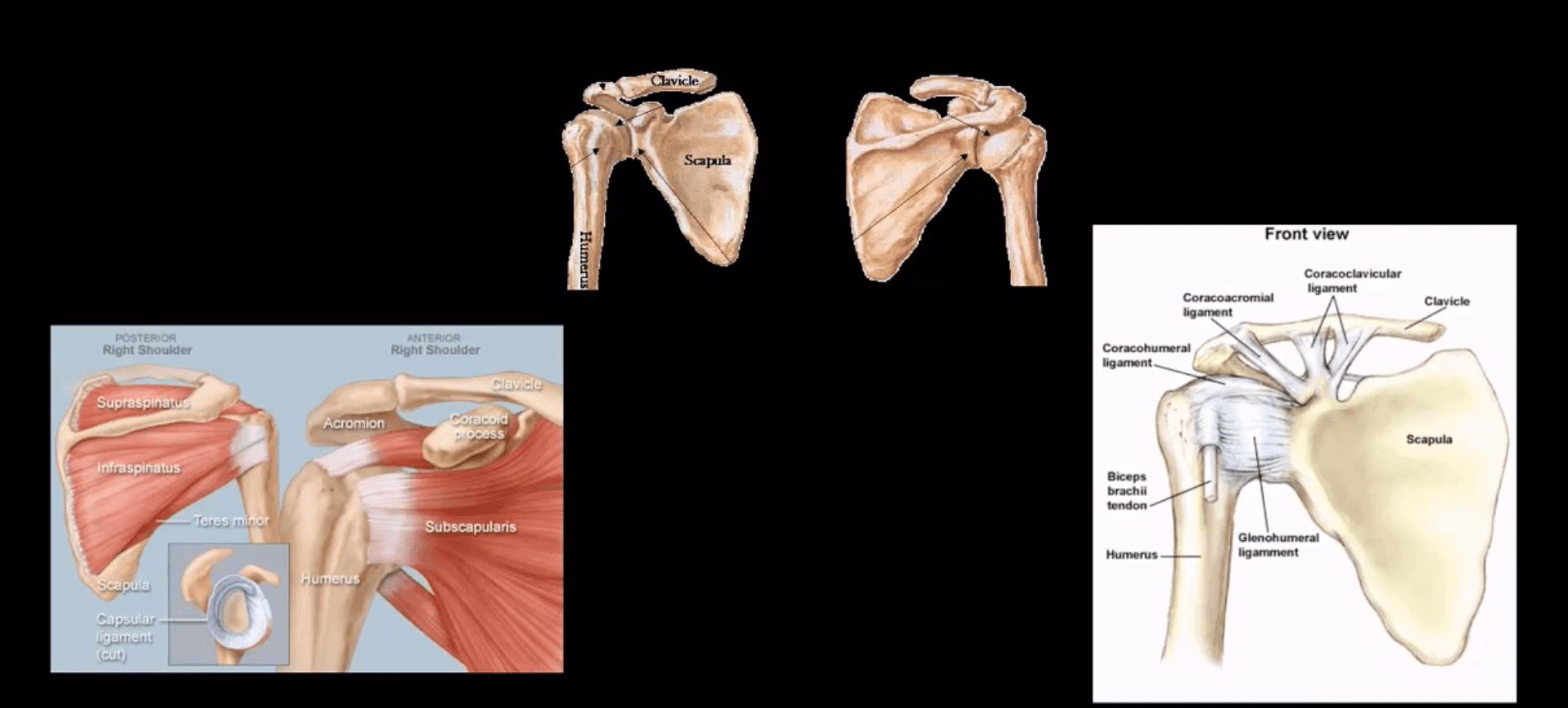
Anatomy of the Shoulder
The shoulder is a complex structure which is made up of three bones: the upper arm bone, also known as the humerus, the shoulder blade, also known as the scapula, along the collarbone, also known as the clavicle.
The head of the upper arm bone fits into a round socket on the shoulder blade, called the glenoid. A variety of ligaments, tendons and muscles then function by holding the upper arm bone. These collection of soft tissues are referred to as the rotator cuff. The main function of the rotator cuff is to both attach and cover the head of the upper arm bone in the shoulder.
Causes of Shoulder Pain
Most health issues that cause shoulder pain fall into four big categories:
Tendon inflammation, bursitis and tendinitis, or a tendon tear
Instability
Arthritis
Fracture or broken bone
Other much less common causes of shoulder pain can include factors such as tumors, disease or aggravated conditions, and nerve-related problems. Below, we will discuss the common causes of shoulder pain in detail.
Bursitis
The bursae are small, fluid-filled sacs which are found between joints throughout the entire body, including the shoulder. These function by decreasing friction between the bone and the muscles as well as act as cushions between the soft tissues and the bones.
Occasionally, excessive utilization of the shoulder can contribute to the swelling and inflammation of the bursa between the rotator cuff and a part of the shoulder blade called the acromion. The outcome measure of this health issue is a condition known as bursitis.
Bursitis often occurs in association with rotator cuff tendinitis, discussed below. The soft tissues in the shoulder can then become painful and inflamed. As a result, daily tasks, such as cleaning or brushing your hair and getting dressed, can become challenging to perform.
Tendinitis
A tendon is a cord which connects the muscles to the bones at different sites. Tendinitis is a consequence of inflammation in this soft tissue.
Ordinarily, tendinitis is frequently categorized as one of two types:
Acute. Overhead physical activities or ball projecting during a sport game or work may result in acute tendinitis.
Chronic. Degenerative diseases like arthritis or degenerative wear and tear as a result of age, may lead to chronic tendinitis.
The joints in the shoulder most commonly affected with tendinitis include the four rotator cuff tendons, particularly the shoulder tendons. The rotator cuff consists of four muscles and their respective tendons which keep the shoulder stable and protect the head of the upper arm bone. The rotator cuff provides equilibrium and shoulder movement.
Tendon Tears
The splitting and tearing of the tendons may by caused by severe damage or trauma from an injury as well as from degenerative changes in the joints due to the normal aging process, long-term overuse and the general wear-and-tear of the joints. These tears may divide the tendon completely out of its attachment or they may only be partial. Normally of tears, the tendon is entirely separated from the bone. Rotator cuff and biceps tendon injuries are among the most common types of tendon tears.
Impingement
Shoulder impingement happens when the cap of the shoulder blade, known as the acromion, places pressure on the underlying soft tissues once the arm is raised away from the torso. When the arm is raised, the acromion rubs, or “impinges” on, the rotator cuff tendons and bursa. This may result in tendinitis and bursitis, restricting motion and causing pain.
Instability
Shoulder instability occurs when the head of the upper arm bone is forced out from the shoulder socket. This can occur as a consequence of a sudden injury or even due to the excessive use of the shoulder.
Shoulder dislocations may only be partial, where only a part of the head of the upper arm may come out partially from the socket. This is also referred to as a subluxation. A complete dislocation usually means that the ball of the upper arm at the shoulder comes out all of the way from the socket.
When the ligaments, tendons, and muscles around the shoulder become torn or loose, dislocations can happen differently. Dislocations, which might be complete or partial, cause unsteadiness and pain when the arm is moved or lifted. Episodes of dislocations or subluxations result in an increased chance of developing arthritis in the shoulder joint, among others.
Arthritis
Health issues resulting in shoulder pain may also lead to arthritis. There are various kinds of arthritis. The most common kind of arthritis in the shoulder is osteroarthritis, also called the “wear-and-tear” arthritis. Osteoarthritis symptoms can include pain, stiffness and swelling which may begin during the day and may worsen throughout the day.
Osteoarthritis might also be associated with work or sports accidents as well as chronic wear-and-tear problems. Other kinds of arthritis could be linked to rotator cuff tears or an inflammation of the joint lining.
Many times, individuals who already have arthritis in the shoulder joints will attempt to prevent moving their shoulder in an effort to reduce arthritis pain and discomfort, However,�this often contributes to the stiffening or the tightening of the soft tissues surrounding the shoulder joints, leading to a painful restriction of movement.
Fracture
Fractures are frequently referred to as broken bones. Shoulder fractures commonly involve the clavicle, or the collarbone, the humerus, or the upper arm bone, and the scapula, or the shoulder blade.
Shoulder fractures in elderly patients are frequently the consequence of a fall from standing height. In the average person, harm from a motor vehicle accident or a sports accident often causes shoulder fractures.
Fractures frequently cause acute pain, swelling, and bruising concerning the shoulder. If a shoulder fracture is suspected, it’s important for the person to seek immediate medical attention by a healthcare professional.
Diagnosis for Shoulder Pain
In the instance of any of the health issues mentioned above resulting in extreme shoulder pain, seek medical attention as soon as possible to receive a proper diagnosis. While many cases of shoulder pain may resolve on their own, make sure to see a doctor if symptoms persist or worsen.
A healthcare professional will conduct a comprehensive evaluation so as to ascertain the cause of the patient’s shoulder pain before providing them with the appropriate treatment options for their health issues.
Medical History
The first step for diagnosis is a comprehensive look at the patient’s medical history. The doctor will ask how the problem has been previously treated and how the pain began, if they are aware of that information. Moreover, additional questions will help determine the causes of the patient’s shoulder pain. Since certain actions may improve or worsen symptoms, a record may be an important tool in discovering the origin of shoulder pain.
Physical Evaluation
A thorough examination will help to discover the source of a patient’s shoulder pain. A doctor will assess for tender places and will try to find physical abnormalities, swelling, deformity or muscular fatigue. They will also observe the shoulder’s strength, flexibility and movement.
Tests
The healthcare professional may additionally order certain tests to help identify the reason for the patient’s shoulder pain and help determine if the symptoms are due to other health issues. The following list demonstrates the variety of tests which can help determine the diagnosis.
X-rays. These images will reveal bone injuries.
Magnetic resonance imaging, or MRI and ultrasound. These imaging studies produce images of soft tissues. MRI can help your doctor identify injuries to the ligaments and tendons.
Computed tomography, or CT, scan. This instrument joins computer technologies and x-rays to make a better, much detailed image of the bones located in the shoulder region.
Electrical studies. The doctor may order an evaluation, including an EMG, or electromyogram, to assess neural function.
Arthrogram. In this study, dye is injected to show the joint and its surrounding soft tissues. It might be used together with an MRI.
Arthroscopy. During this procedure, a doctor looks inside the joint using a camera. Arthroscopy may reveal soft tissue injuries that aren’t apparent in evaluations along with the exam. Arthroscopy can be used to fix the problem and help find the reason for symptoms.
Dr. Alex Jimenez’s Insight
As the most mobile joint in the human body, the shoulder joint is often vulnerable to experience a variety of problems which can result in shoulder pain. Shoulder pain can tremendously affect an individual’s ability to perform everyday tasks and, if lest untreated, it can progress into neck and back pain as well as cause other severe symptoms. Understanding the cause of a patient’s shoulder pain can help diagnose their problem in order to recommend the best treatment option.
Treatment for Shoulder Pain
Chiropractic Care
Chiropractic care is a safe and effective, alternative treatment option which can help manage shoulder pain by relieving discomfort and swelling, among other painful symptoms. A chiropractor will utilize chiropractic adjustments and manual manipulations to reduce joint restrictions and correct spinal misalignments, in an effort to improve function.
Lifestyle Modifications
Furthermore, a doctor of chiropractic, or chiropractor, will recommend a series of lifestyle modifications to help promote a faster recovery process. Changing a patient’s actions through a balance of rest and physical therapeutics can help improve shoulder endurance. Avoiding overexertion can also help prevent further harm and shoulder pain.�
Drugs & Medications
A doctor may also prescribe drugs and/or medications to decrease shoulder pain and inflammation. It needs to be taken only as directed, however, if medicine is prescribed to ease pain. A physician can also recommend shots of numbing steroids to alleviate pain.
Surgery
Surgical interventions can be used to help treat the causes attributing to shoulder pain, however, it should only be considered as a last resort. A majority of patients will react positively to alternative treatment options like chiropractic care and through lifestyle modifications.�
For certain types of shoulder problems, like recurring dislocations and a few rotator cuff tears, alternative treatment options may not be recommended and surgery may be considered, in this instance.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Approximately a couple of years ago, Denise was the victim of a car accident that led to upper body problems, such as shoulder pain. As a result of her debilitating symptoms, Denise was not able to participate in her routine physical actions. While she continued to encounter issues with her automobile accident injuries, she made a decision to look for chiropractic shoulder pain therapy with Dr. Alex Jimenez. Since her very first treatment session, Denise noticed enormous modifications to her symptoms and she was once more able to go back to her original routines ahead of the episode. Denise positively advocates Dr. Alex Jimenez because he’s the best the non-invasive pick for shoulder pain therapy since locating relief.
Chiropractic Treatment Shoulder Pain
Upper body problems, such as shoulder pain, are a few of the most frequent causes of physician visits. The shoulder is the most mobile joint in the human body, though, because of its increased range of movement, it’s also a very unstable joint. This can raise the risk of joint injury, frequently resulting in the degeneration of these soft tissues surrounding the backbone. Shoulder pain may be categorized as localized, along with other health problems causing shoulder pain. The force in the effect of a crash, including an auto accident or a sports accident, is a popular trigger for shoulder problems.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Jesus Rabelo makes a living as an 18 wheeler truck driver at El Paso, TX. After being involved in a crash, Mr. Rabelo suffered from back and shoulder pain that influenced his private life and function, forcing him to need to start all over again. In reference to a highly appreciated recommendation, Jesus Rabelo found Dr. Alex Jimenez, chiropractor in El Paso, TX. Mr. Rabelo describes receiving outstanding service from the team and he highly recommends Dr. Alex Jimenez himself.
18 Wheeler Accident Chiropractic Treatment
In 2013, 54 million individuals sustained injuries from traffic crashes. This led in 1.4 million deaths in 2013, up from 1.1 million deaths in 1990. Automobile accidents can be grouped into various kinds, such as head-on, rear-end, side accidents, and rollovers. Psychological issues may happen because of auto accidents. A variety of injuries and ailments could result in the blunt force injury brought on by a crash, such as whiplash and back pain, among others.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Bobby Gomez describes how each visit with Dr. Alex Jimenez and to PUSH Fitness with Daniel Alvarado has resulted in great improvements in the stability of his shoulders as well as in the placement of his hips. Although Bobby Gomez’s recovery has been progressing gradually, he discusses the tremendous changes he has experienced mentally, emotionally and physically. Bobby Gomez highly recommends Dr. Alex Jimenez as the non-surgical choice for neck and back pain, as well as shoulder and hip pain.
Shoulder Pain Treatment
Cerebral palsy (commonly known as CP) affects ordinary motion in various areas of the human body and has many degrees of severity. CP causes problems with posture, gait, muscle tone and coordination of movement. Some children with CP have coexisting conditions, such as eyesight and hearing impairment. These disorders are brought on by brain damage and aren’t a direct result of cerebral palsy. Cerebral palsy does not affect life expectancy. Based on the way in which the condition is handled, motor abilities can improve or decrease over time. While severity and symptoms vary, most individuals with this condition go on to direct a rich, fulfilling life.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine