Individuals with fixed sagittal imbalance, a condition where the normal curve of the lower spine is greatly reduced or absent altogether that can cause pain and difficulty balancing. Can chiropractic treatment, physical therapy, and exercise help improve the condition?
Fixed Sagittal Imbalance
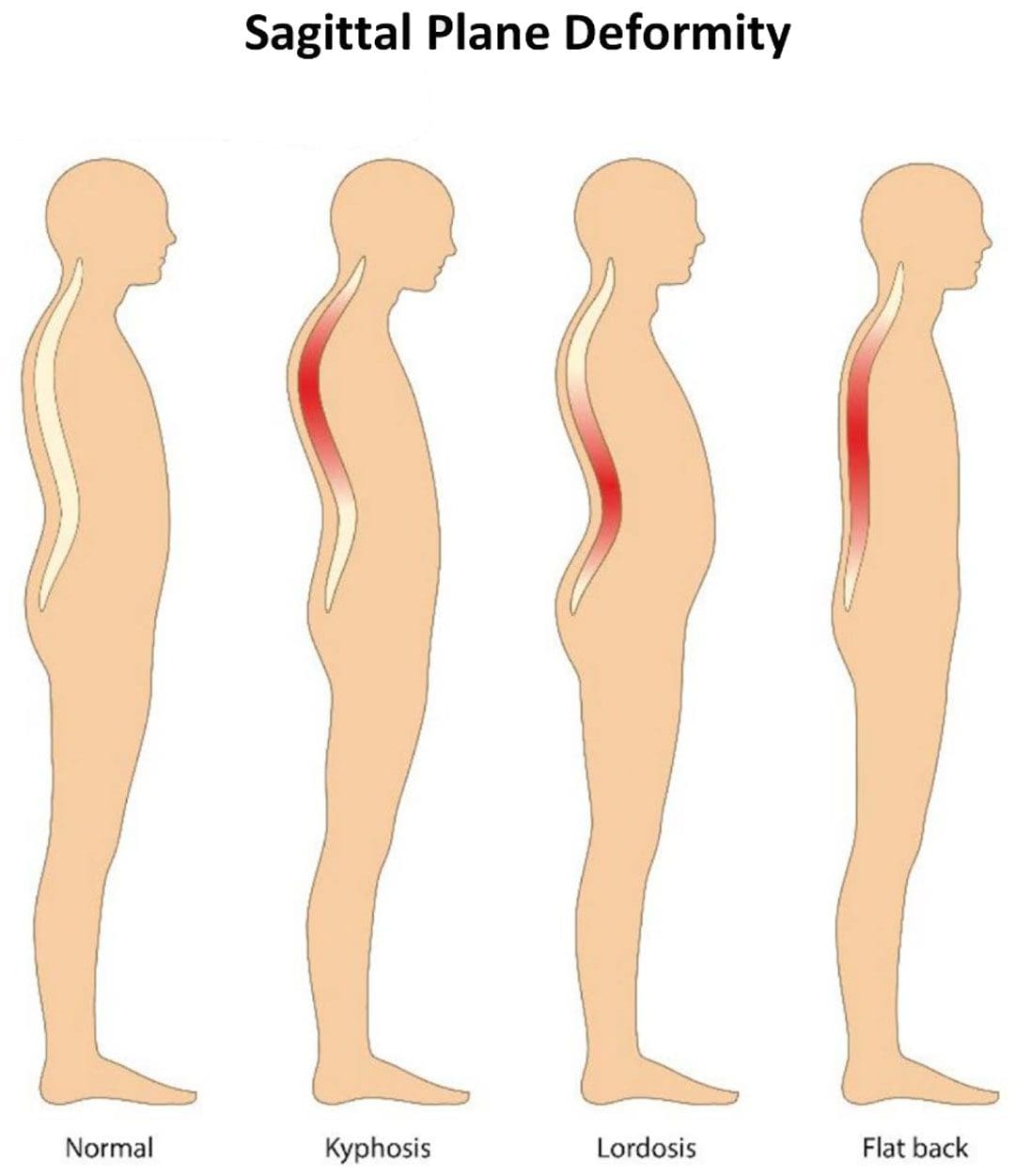
The condition is commonly known as flat back syndrome and can be present at birth or can happen as a result of surgery or a medical condition.
Individuals with flat back syndrome position their head and neck too far forward.
A major symptom is difficulty standing for long periods of time.
Symptoms
The spine has two curves. The lumbar spine in the lower back and cervical spine in the neck curve inward. The thoracic spine in the upper back curves outward. The curves are part of the spine’s natural alignment. They help the body balance and maintain the center of gravity.
If these curves begin to disappear the body can have trouble and difficulty standing up straight.
The loss of curvature causes the head and neck to pitch forward, making it hard to walk and do regular normal activities.
A chiropractor and/or physical therapist can recommend exercises and other forms of treatment. (Won-Moon Kim, et al., 2021)
Life-Changing Chiropractic Relief
References
Columbia University Irving Medical Center. Flatback syndrome.
National Health Service. Common posture mistakes and fixes.
Lee, B. H., Hyun, S. J., Kim, K. J., Jahng, T. A., Kim, Y. J., & Kim, H. J. (2018). Clinical and Radiological Outcomes of Posterior Vertebral Column Resection for Severe Spinal Deformities. Journal of Korean Neurosurgical Society, 61(2), 251–257. https://doi.org/10.3340/jkns.2017.0181
Kim, W. M., Seo, Y. G., Park, Y. J., Cho, H. S., & Lee, C. H. (2021). Effect of Different Exercise Types on the Cross-Sectional Area and Lumbar Lordosis Angle in Patients with Flat Back Syndrome. International journal of environmental research and public health, 18(20), 10923. https://doi.org/10.3390/ijerph182010923
Can combining chiropractic treatment with the common therapies of medication, exercise, and/or physical therapy help relieve sciatic endometriosis pain symptoms?
Sciatic Endometriosis
Sciatic endometriosis is a condition in which endometrial cells (tissue that resembles the lining of the uterus) grow outside of the uterine lining and compress the sciatic nerve. This places stress and pressure on the nerve causing back, pelvic, hip, and leg pain, especially before and during the menstrual cycle. It can also cause pain, irregular periods, and infertility. (The American College of Obstetricians and Gynecologists. 2021)
These areas of endometrial tissue growth are also known as lesions or implants.
Women with sciatic endometriosis often experience leg pain and weakness around the time of their menstrual cycle. (Lena Marie Seegers, et al., 2023)
Sciatic endometriosis can also cause pain when urinating, during a bowel movement, during sex, and fatigue, and irregular vaginal bleeding.
The abnormal growth may be caused by higher-than-normal levels of estrogen.
Researchers believe that endometriosis is related to retrograde menstruation, which causes menstrual blood to flow back into the pelvis instead of out through the vagina. (World Health Organization. 2023)
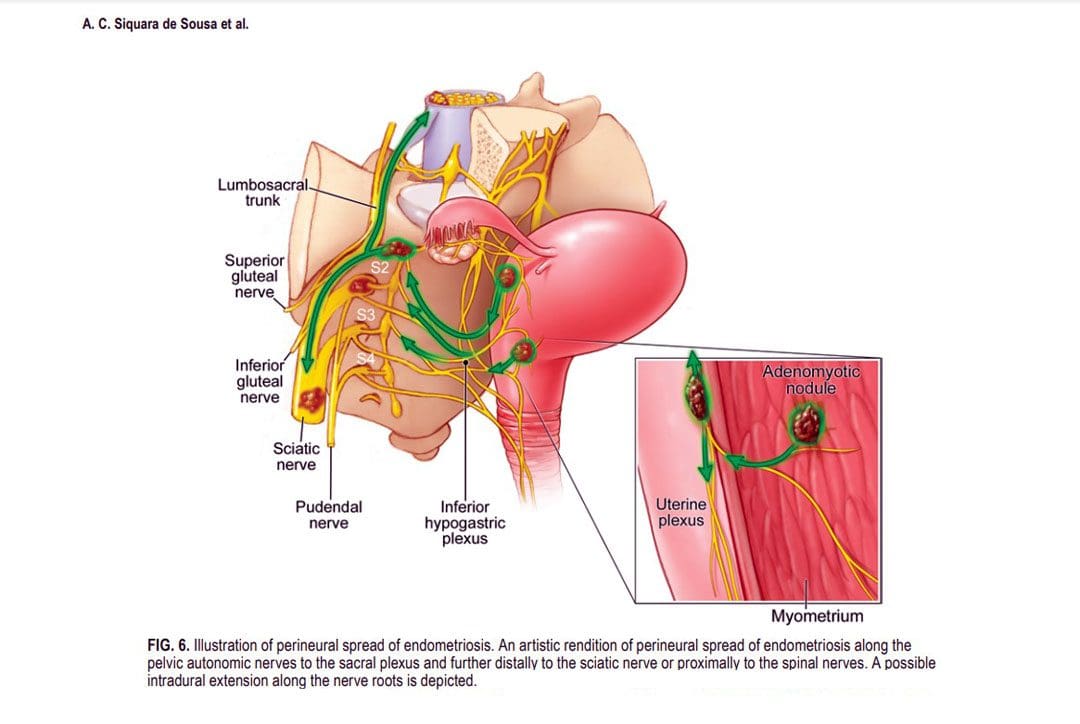
Sometimes, the cells grow in the area of the pelvis right above the sciatic nerve. (Adaiah Yahaya, et al., 2021)
The sciatic nerve is the longest nerve in the body and travels down the back of each leg. (Johns Hopkins Medicine. 2023)
When endometrial lesions place pressure on the sciatic nerve, they can cause irritation and inflammation leading to severe pelvic pain, which makes it harder to conceive. (Liang Yanchun, et al., 2019)
Symptoms
Some women with endometriosis experience no symptoms or misinterpret the symptoms as typical premenstrual syndrome/PMS signs. The most common signs and symptoms of sciatic endometriosis include:
Difficulty walking or standing.
Loss of sensation, muscle weakness, and reflex alteration.
Limping.
Balance problems.
Bloating and nausea.
Constipation or diarrhea before or after a period.
Painful, heavy, and/or irregular periods.
Bleeding between periods.
Pain during sex, urination, and bowel movements.
Pain in the stomach, pelvis, lower back, hips, and buttocks. (MedlinePlus. 2022)
Weakness, numbness, tingling, burning, or dull aching sensations in the back of one or both legs.
Endometriosis, including sciatic endometriosis, typically cannot be diagnosed with a pelvic examination or ultrasound by themselves. A healthcare provider may need to perform a biopsy using laparoscopy and discuss menstrual cycles, symptoms, and medical history.
The laparoscopy procedure involves making tiny incisions and taking a tissue sample with tools attached to a thin tube with a camera. (MedlinePlus. 2022)
Imaging tests, like magnetic resonance imaging/MRI, and computed tomography/CT scans, can help provide essential information about the location and size of any endometrial lesions. (The American College of Obstetricians and Gynecologists. 2021)
Treatment
Symptoms can sometimes be temporarily relieved with over-the-counter/OTC pain relievers. Depending on the condition and severity a healthcare provider may prescribe hormonal treatment to prevent new endometrial implants from growing. These can include:
Hormonal birth control.
Progestin – a synthetic form of progesterone.
Gonadotropin-releasing hormone – GnRH agonists.
If pain persists or worsens, individuals may need to undergo surgery to remove the tissue.
The American College of Obstetricians and Gynecologists. Endometriosis.
Seegers, L. M., DeFaria Yeh, D., Yonetsu, T., Sugiyama, T., Minami, Y., Soeda, T., Araki, M., Nakajima, A., Yuki, H., Kinoshita, D., Suzuki, K., Niida, T., Lee, H., McNulty, I., Nakamura, S., Kakuta, T., Fuster, V., & Jang, I. K. (2023). Sex Differences in Coronary Atherosclerotic Phenotype and Healing Pattern on Optical Coherence Tomography Imaging. Circulation. Cardiovascular imaging, 16(8), e015227. https://doi.org/10.1161/CIRCIMAGING.123.015227
World Health Organization. Endometriosis.
Yahaya, A., Chauhan, G., Idowu, A., Sumathi, V., Botchu, R., & Evans, S. (2021). Carcinoma arising within sciatic nerve endometriosis: a case report. Journal of surgical case reports, 2021(12), rjab512. https://doi.org/10.1093/jscr/rjab512
Johns Hopkins Medicine. Sciatica.
Yanchun, L., Yunhe, Z., Meng, X., Shuqin, C., Qingtang, Z., & Shuzhong, Y. (2019). Removal of an endometrioma passing through the left greater sciatic foramen using a concomitant laparoscopic and transgluteal approach: case report. BMC women’s health, 19(1), 95. https://doi.org/10.1186/s12905-019-0796-0
MedlinePlus. Endometriosis.
Center for Endometriosis Care. Sciatic endometriosis.
Chen, S., Xie, W., Strong, J. A., Jiang, J., & Zhang, J. M. (2016). Sciatic endometriosis induces mechanical hypersensitivity, segmental nerve damage, and robust local inflammation in rats. European journal of pain (London, England), 20(7), 1044–1057. https://doi.org/10.1002/ejp.827
Siquara de Sousa, A. C., Capek, S., Howe, B. M., Jentoft, M. E., Amrami, K. K., & Spinner, R. J. (2015). Magnetic resonance imaging evidence for perineural spread of endometriosis to the lumbosacral plexus: report of 2 cases. Neurosurgical focus, 39(3), E15. https://doi.org/10.3171/2015.6.FOCUS15208
Garlic tea is an herbal tonic made from garlic, lemon, and honey. What medicinal uses and benefits can garlic provide that is supported by scientific research?
Garlic Tea
Garlic tea:
Garlic – Allium sativum – is a perennial plant from Central Asia.
The plant produces a bulb that is used in cooking and in health remedies all over the world.
Garlic powder, oil, and supplements are available.
Supplements can be made from garlic oil or from fresh, dried, or aged garlic.
The tea is commonly made with garlic, lemon, and honey, but can be made with a variety of different ingredients.
It is used for cold symptoms like congestion and cough.
Health Benefits
Some, but not all benefits are supported by scientific evidence. It is important to keep in mind that these studies are analyzing garlic, and not necessarily garlic tea. The dose of garlic in tea may not be the same as a more concentrated dose that is used in the studies. Also, cooking or boiling garlic can change its therapeutic effects.
The scientific evidence about garlic’s benefits. Garlic is a healthy source of organosulfur compounds, including alliinase, which is released when it is crushed or chopped. (Leyla Bayan, Peir Hossain Koulivand, Ali Gorji. 2014)
Organosulfur compounds are believed to provide health benefits.
An overview of garlic studies found that there are promising health benefits, however, the researchers caution that larger studies are needed to confirm the results and verify the right dosage to get the results. (Johura Ansary, et al., 2020)
The current studies show the following possible benefits:
Some studies have also shown that garlic could be able to stimulate the immune system and decrease tumor growth in certain cancers, like colorectal cancer.
However, research investigating the cancer-preventing benefits has shown mixed results. (Xi Zhou, et al., 2020)
Common side effects of garlic consumption include bad breath, upset stomach, and body odor.
Garlic can also cause bloating, gas, and heartburn for some.
There are allergies to garlic and individuals with an allergy can experience more severe symptoms.
The NIH also advises that taking garlic may increase your risk of bleeding.
Individuals taking a blood thinner like warfarin or about to undergo surgery should discuss taking supplements or drinking garlic tea with their healthcare provider.
Garlic has been found to interfere with the effectiveness of some drugs that are used to treat HIV infection.
Lemon can cause tooth erosion so it is recommended to rinse teeth after drinking.
Honey has sugar content so it is recommended to use it in small quantities.
Healthy Diet and Chiropractic
References
National Center for Complementary and Integrative Health. Garlic.
Bayan, L., Koulivand, P. H., & Gorji, A. (2014). Garlic: A review of potential therapeutic effects. Avicenna journal of phytomedicine, 4(1), 1–14.
Ansary, J., Forbes-Hernández, T. Y., Gil, E., Cianciosi, D., Zhang, J., Elexpuru-Zabaleta, M., Simal-Gandara, J., Giampieri, F., & Battino, M. (2020). Potential Health Benefit of Garlic Based on Human Intervention Studies: A Brief Overview. Antioxidants (Basel, Switzerland), 9(7), 619. https://doi.org/10.3390/antiox9070619
Zhang, S., Liu, M., Wang, Y., Zhang, Q., Liu, L., Meng, G., Yao, Z., Wu, H., Xia, Y., Bao, X., Gu, Y., Wang, H., Shi, H., Sun, S., Wang, X., Zhou, M., Jia, Q., Song, K., & Niu, K. (2020). Raw garlic consumption is inversely associated with prehypertension in a large-scale adult population. Journal of human hypertension, 34(1), 59–67. https://doi.org/10.1038/s41371-019-0257-0
Zhou, X., Qian, H., Zhang, D., & Zeng, L. (2020). Garlic intake and the risk of colorectal cancer: A meta-analysis. Medicine, 99(1), e18575. https://doi.org/10.1097/MD.0000000000018575
Avci, A., Atli, T., Ergüder, I. B., Varli, M., Devrim, E., Aras, S., & Durak, I. (2008). Effects of garlic consumption on plasma and erythrocyte antioxidant parameters in elderly subjects. Gerontology, 54(3), 173–176. https://doi.org/10.1159/000130426
Burian, J. P., Sacramento, L. V. S., & Carlos, I. Z. (2017). Fungal infection control by garlic extracts (Allium sativum L.) and modulation of peritoneal macrophage activity in a murine model of sporotrichosis. Brazilian journal of biology = Revista brasleira de biologia, 77(4), 848–855. https://doi.org/10.1590/1519-6984.03716
Kato, Y., Domoto, T., Hiramitsu, M., Katagiri, T., Sato, K., Miyake, Y., Aoi, S., Ishihara, K., Ikeda, H., Umei, N., Takigawa, A., & Harada, T. (2014). Effect on blood pressure of daily lemon ingestion and walking. Journal of nutrition and metabolism, 2014, 912684. https://doi.org/10.1155/2014/912684
Samarghandian, S., Farkhondeh, T., & Samini, F. (2017). Honey and Health: A Review of Recent Clinical Research. Pharmacognosy Research, 9(2), 121–127. https://doi.org/10.4103/0974-8490.204647
Individuals who have suffered cervical acceleration-deceleration/CAD more commonly known as whiplash, can experience headaches, and other symptoms like neck stiffness, pain, fatigue, and shoulder/neck/back discomfort. Can non-surgical and conservative treatments help alleviate the symptoms?
Cervical Acceleration – Deceleration or CAD
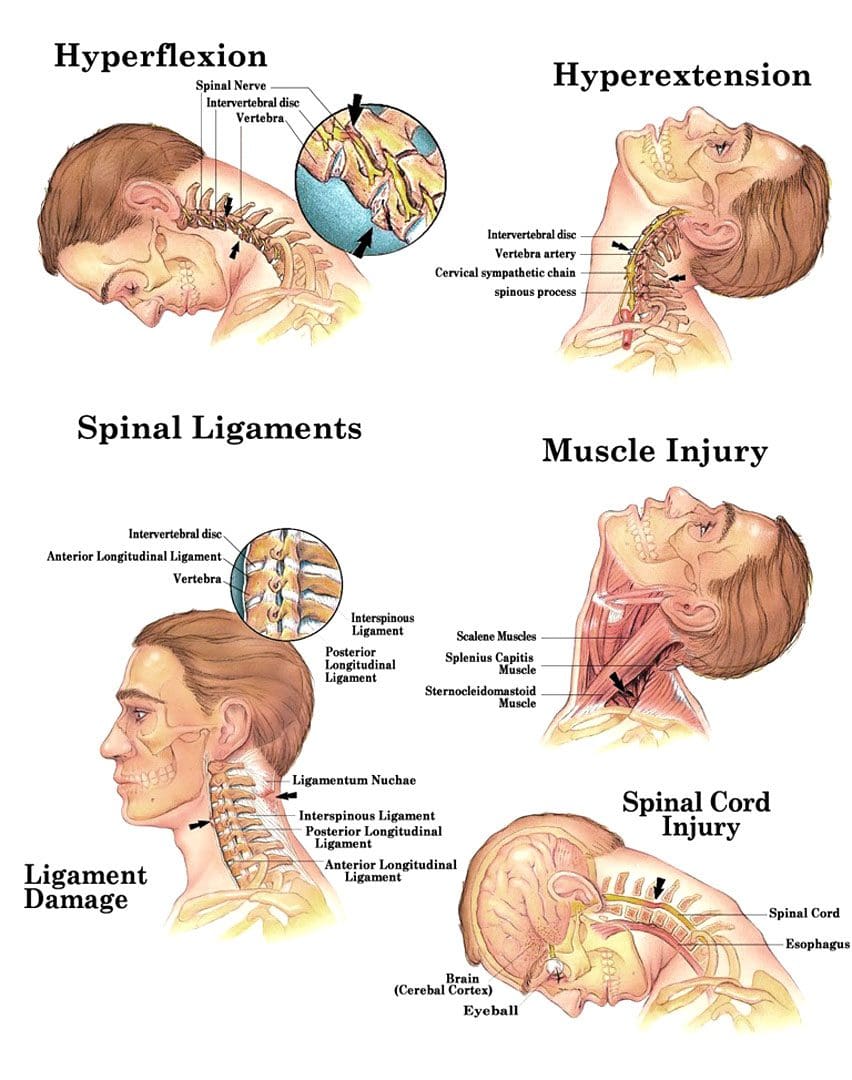
Cervical acceleration-deceleration is the mechanism of a neck injury caused by a forceful back-and-forth neck motion. It happens most commonly in rear-end vehicle collisions when the head and neck whip forward and backward with intense acceleration and/or deceleration causing the neck to flex and/or extend rapidly, more than normally, straining and possibly tearing muscle tissues and nerves, ligaments, dislocation of spinal discs and herniations, and cervical bone fractures.
For symptoms that do not improve or worsen after 2 to 3 weeks, see a healthcare provider or chiropractor for further evaluation and treatment.
Whiplash injuries strain or sprain the neck muscles and/or ligaments, but can also affect the vertebrae/bones, disc cushions between the vertebrae, and/or the nerves.
Whiplash symptoms can present right away, or after several hours to a few days after the incident, and tend to worsen in the days after the injury. Symptoms can last a few weeks to a few months, and can severely limit activity and range of motion. Symptoms can include: (National Institute of Neurological Disorders and Stroke. 2023)
Pain that extends into the shoulders and back.
Neck stiffness
Limited neck motion
Muscle spasms
Numbness and tingling sensations – paresthesias or pins and needles in the fingers, hands, or arms.
Headaches – A whiplash headache usually starts at the base of the skull and can vary in intensity. Most individuals experience pain on one side of the head and toward the back, though some can experience symptoms all over their head, and a small number experience headaches on the forehead or behind the eyes. (Monica Drottning. 2003)
The headaches can become aggravated by moving the neck around, especially when looking up.
Headaches are often associated with shoulder pain along with sensitive neck and shoulder muscles that when touched can increase pain levels.
Whiplash headaches can lead to chronic neck-related headaches known as cervicogenic headaches. (Phil Page. 2011)
It is also important to rest your neck area following the injury.
A cervical collar can be utilized temporarily to stabilize the neck, but for long-term recovery, it is recommended to keep the area mobile.
Physical activity reduction until the individual can look over both shoulders, and tilt their head all the way forward, all the way back, and from side to side without pain or stiffness.
Non-steroidal anti-inflammatories – NSAIDs – Ibuprofen or Naproxen.
Muscle relaxers
If symptoms do not improve, a healthcare provider may recommend physical therapy and/or stronger pain medications. For whiplash headaches that last for several months, acupuncture, or spinal injections may be recommended.
Neck Injuries
References
National Institute of Neurological Disorders and Stroke. Whiplash Information Page.
Drottning M. (2003). Cervicogenic headache after a whiplash injury. Current pain and headache reports, 7(5), 384–386. https://doi.org/10.1007/s11916-003-0038-9
Page P. (2011). Cervicogenic headaches: an evidence-led approach to clinical management. International journal of sports physical therapy, 6(3), 254–266.
For individuals with peanut allergies, can finding a peanut alternative be as satisfying as a real creamy or crunchy peanut butter sandwich?
Peanut Butter Sandwich Alternatives
For individuals who are unable to have a peanut butter sandwich due to an allergy, there are healthy satisfying alternatives. Tree nut butter, seed butter, and deli meats can all satisfy sandwich cravings and provide nutrition. Here are a few healthy, nutritious alternatives to try out:
Sunflower Seed Butter and Jam, Jelly, or Preserves
It can be substituted for a PBJ with jam, jelly, and preserves.
Ham and Cheese, Grainy Mustard on Rye Bread
Getting ham and cheese from the deli can potentially have cross-contamination with allergens during slicing and packaging.
Prepackaged and sliced ham and cheese is a safer bet in terms of allergens.
It is recommended to read the ingredient label for potential allergens, as processing in facilities can have cross-contamination issues. (William J. Sheehan, et al., 2018)
Turkey, Tomato, Lettuce, and Hummus on Whole Grain Bread
The same is true for turkey and is recommended to buy prepackaged and sliced.
Check the ingredients for possible allergens.
Hummus is made from chickpeas/garbanzo beans and tahini/ground sesame seeds.
Hummus comes in a variety of flavors that can be used as a dip or spread.
Although chick peas’ are a member of the legume family, hummus can be tolerated with peanut allergies. (Mathias Cousin, et al., 2017)
Check with a healthcare provider if unsure.
Pita Pocket with Salad and Hummus
Pita pockets are great with hummus stuffed with vegetables.
This is a delicious crunchy pocket sandwich loaded with protein, fiber vitamins, and minerals.
Cashew butter on a hot English muffin with raisins on top for a boost of iron is reminiscent of a cinnamon roll.
Pumpkin Seed Butter and Honey Sandwich
Pumpkin butter is made from the orange flesh of the pumpkin.
Pumpkin seed butter is made by roasting pumpkin seeds and grinding them to a butter consistency.
The seed butter can be spread on bread and drizzled with some honey on top for a nutritious and delicious snack.
There are tasty healthy peanut butter alternatives that can be mixed, matched, and reinvented into various satisfying sandwiches. Individuals are recommended to consult their healthcare provider or a dietician or nutritionist to find what works for them.
Smart Choices, Better Health
References
Lavine, E., & Ben-Shoshan, M. (2015). Allergy to sunflower seed and sunflower butter as a proposed vehicle for sensitization. Allergy, asthma, and clinical immunology: Official Journal of the Canadian Society of Allergy and Clinical Immunology, 11(1), 2. https://doi.org/10.1186/s13223-014-0065-6
U.S. Department of Agriculture: FoodData Central. Seeds, sunflower seed butter, with salt added (Includes foods for USDA’s Food Distribution Program).
Sheehan, W. J., Taylor, S. L., Phipatanakul, W., & Brough, H. A. (2018). Environmental Food Exposure: What Is the Risk of Clinical Reactivity From Cross-Contact and What Is the Risk of Sensitization. The journal of allergy and clinical immunology. In practice, 6(6), 1825–1832. https://doi.org/10.1016/j.jaip.2018.08.001
Gorrepati, K., Balasubramanian, S., & Chandra, P. (2015). Plant-based butters. Journal of food science and technology, 52(7), 3965–3976. https://doi.org/10.1007/s13197-014-1572-7
Cousin, M., Verdun, S., Seynave, M., Vilain, A. C., Lansiaux, A., Decoster, A., & Sauvage, C. (2017). Phenotypical characterization of peanut-allergic children with differences in cross-allergy to tree nuts and other legumes. Pediatric allergy and immunology: Official publication of the European Society of Pediatric Allergy and Immunology, 28(3), 245–250. https://doi.org/10.1111/pai.12698
Almond Board of California. Nutrient comparison chart for tree nuts.
American Academy of Allergy, Asthma and Immunology. Everything you need to know about a tree nut allergy.
The Q or quadriceps angle is a measurement of pelvic width that is believed to contribute to the risk of sports injuries in women athletes. Can non-surgical therapies and exercises help rehabilitate injuries?
Quadriceps Q – Angle Injuries
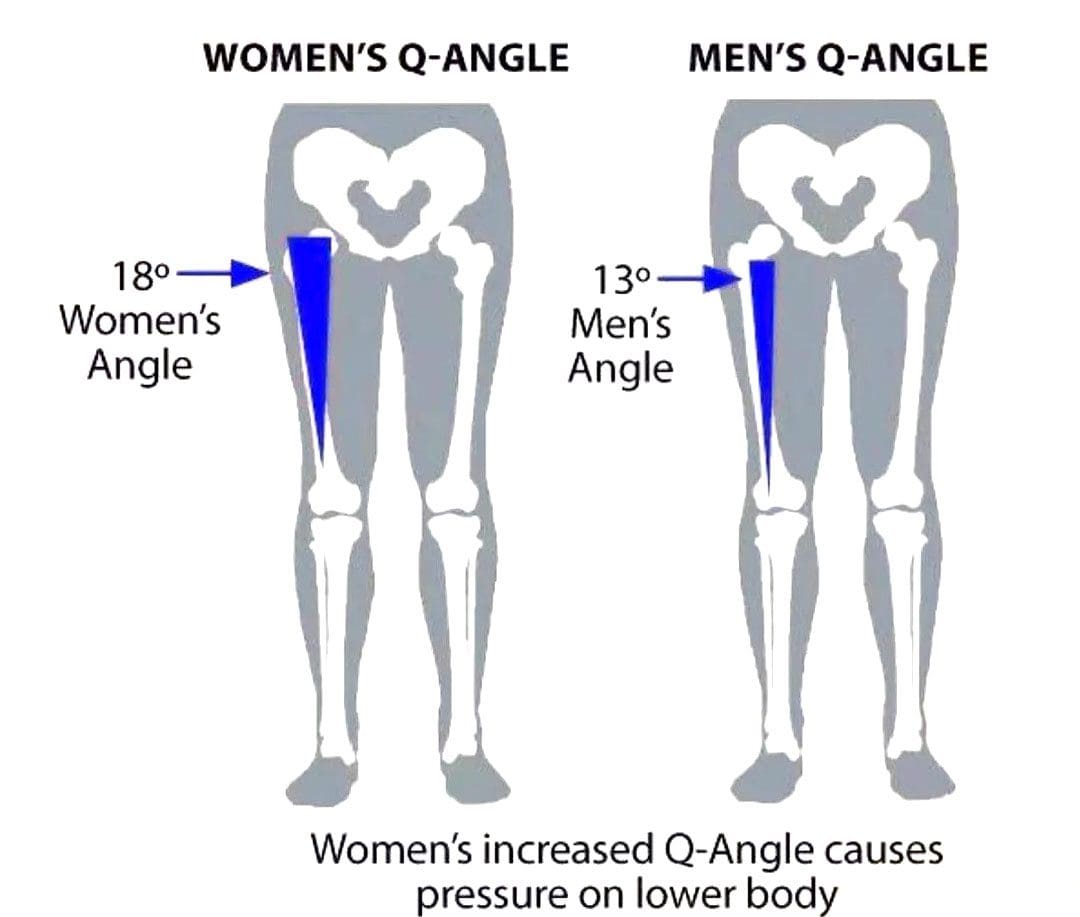
The Q angle is the angle where the femur/upper leg bone meets the tibia/lower leg bone. It is measured by two intersecting lines:
One from the center of the patella/kneecap to the anterior superior iliac spine of the pelvis.
The other is from the patella to the tibial tubercle.
On average the angle is three degrees higher in women than men.
Women have biomechanical differences that include a wider pelvis, making it easier to give birth. However, this difference can contribute to knee injuries when playing sports, as an increased Q angle generates more stress on the knee joint, as well as leading to increased foot pronation.
Injuries
Various factors can increase the risk of injury, but a wider Q angle has been linked to the following conditions.
Patellofemoral Pain Syndrome
An increased Q angle can cause the quadriceps to pull on the kneecap, shifting it out of place and causing dysfunctional patellar tracking.
With time, this can cause knee pain (under and around the kneecap), and muscle imbalance.
Foot orthotics and arch supports could be recommended.
Some researchers have found a link, while others have not found the same association. (Wolf Petersen, et al., 2014)
Chondromalacia of the Knee
This is the wearing down of the cartilage on the underside of the kneecap.
An increased Q angle can be a factor that increases stress and causes the knee to lose its stability.
However, this remains controversial, as some studies have found no association between the Q angle and knee injuries.
Chiropractic Treatment
Strengthening Exercises
ACL injury prevention programs designed for women have resulted in reduced injuries. (Trent Nessler, et al., 2017)
The vastus medialis obliquus or VMO is a teardrop-shaped muscle that helps move the knee joint and stabilize the kneecap.
Strengthening the muscle can increase the stability of the knee joint.
Strengthening may require a specific focus on muscle contraction timing.
Closed-chain exercises like wall squats are recommended.
Glute strengthening will improve stability.
Stretching Exercises
Stretching tight muscles will help relax the injured area, increase circulation, and restore range of motion and function.
Muscles commonly found to be tight include the quadriceps, hamstrings, iliotibial band, and gastrocnemius.
Foot Orthotics
Custom-made, flexible orthotics decrease the Q angle and reduce pronation, relieving the added stress on the knee.
A custom orthotic ensures that the foot and leg dynamics are accounted for and corrected.
Motion-control shoes can also help correct overpronation.
Knee Rehabilitation
References
Khasawneh, R. R., Allouh, M. Z., & Abu-El-Rub, E. (2019). Measurement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one, 14(6), e0218387. https://doi.org/10.1371/journal.pone.0218387
Petersen, W., Ellermann, A., Gösele-Koppenburg, A., Best, R., Rembitzki, I. V., Brüggemann, G. P., & Liebau, C. (2014). Patellofemoral pain syndrome. Knee surgery, sports traumatology, arthroscopy: Official journal of the ESSKA, 22(10), 2264–2274. https://doi.org/10.1007/s00167-013-2759-6
Vaienti, E., Scita, G., Ceccarelli, F., & Pogliacomi, F. (2017). Understanding the human knee and its relationship to total knee replacement. Acta bio-medica : Atenei Parmensis, 88(2S), 6–16. https://doi.org/10.23750/abm.v88i2-S.6507
Mitani Y. (2017). Gender-related differences in lower limb alignment, range of joint motion, and the incidence of sports injuries in Japanese university athletes. Journal of Physical Therapy Science, 29(1), 12–15. https://doi.org/10.1589/jpts.29.12
Nessler, T., Denney, L., & Sampley, J. (2017). ACL Injury Prevention: What Does Research Tell Us? Current reviews in musculoskeletal medicine, 10(3), 281–288. https://doi.org/10.1007/s12178-017-9416-5
Temporomandibular joint disorder causes pain and jaw locking that can be worsened with certain activities. How individuals can manage and prevent flare-ups by learning what not to do to worsen the condition?
What Not To Do Temporomandibular Joint Disorder
Tenderness, aching, pain, and jaw locking are symptoms of temporomandibular joint disorder or TMJ. The temporomandibular joint connects the jaw to the skull. It is used daily for eating, drinking, and talking. It is a small disc in the joint that allows the jaw bones to slip and slide correctly. With TMJ, the disc shifts out of place, leading to clicking, snapping, and limited jaw movement. It can also cause pain in the jaw and face, neck pain, and headaches, and the muscles around the jaw and neck can become sore and/or go into spasm. Any type of activity that stresses or overworks the joint can trigger a flare-up and worsen TMJ symptoms. (Schiffman E, et al. 2014) This article looks at avoiding activities that make TMJ worse and what not to do to help keep TMJ symptoms in check.
Chewing Gum
Gum chewing is not recommended for individuals with TMJ.
The jaw is one of the most used joints in the body.
Limiting excessive use alleviates pressure allowing the joints and muscles to rest.
Resting sore muscles and joints is the first step in injury recovery.
Eating Chewy and Hard Foods
Chewy and hard foods make the jaw have to work overtime.
Avoid eating hard foods like chewy candies, hard and chewy breads, vegetables like corn on the cob, and fruits like apples.
These foods can place excessive stress on the jaw, and prevent the joint from properly resting and healing.
Chewing Only On One Side
Many individuals chew their food on only one side of the mouth.
This can stress out one side of the temporomandibular joint and surrounding muscles, leading to pain and dysfunction. (Urbano Santana-Mora, et al., 2013)
Stay aware of chewing habits and make sure to utilize both sides of the mouth.
Individuals with dental issues or tooth pain are recommended to see a dentist.
Non-Functional Jaw Activities
Going through each day, individuals tend to do things unconsciously or out of habit.
For example, individuals:
Reading or writing might chew on a pen or pencil.
Bite their nails or chew on the inside of their mouth while watching TV or internet browsing.
These activities can place stress on the joint, worsen the condition, and extend the healing process.
Resting on The Chin
Individuals will rest their jaw in their hands while studying, on social media, or watching TV.
This position can be comfortable, but it can affect the jaw.
This position can build pressure against the side of the jaw and push against the joint, causing the disc to shift out of place affecting how the jaw opens and closes.
Breaking the chin resting habit can allow the joint to relax and heal correctly.
Teeth Clenching
Bruxism is the medical term for clenching the teeth.
This can occur during the day or during sleep.
Teeth clenching is often brought on by stress and can place incredible pressure on the jaw’s muscles and worsen TMJ.
A dentist can prescribe a mouth guard to be worn while sleeping to protect the teeth from excessive clenching. (Miriam Garrigós-Pedrón, et al., 2019)
Slouching
The function of the jaw is closely related to body posture.
The jaw operates optimally when the head is above the cervical spine and the posture is upright.
Slouching can change how the jaw muscles work and the way the jaw opens and closes.
Part of physical therapy for TMJ is working on posture adjustments and training.
This can involve strengthening the back and shoulder muscles and setting up posture reminders.
Sitting and standing correctly can keep the jaw operating properly.
Postponing Treatment
Many with musculoskeletal issues and symptoms wait for the pain to go away.
Individuals having problems with their jaw should not wait to get treatment.
TMJ has a positive rate of recovery with conservative treatment, which is all the more reason to seek treatment. (G Dimitroulis. 2018)
A dentist or healthcare provider can provide an accurate diagnosis if TMJ is suspected.
Individuals can benefit from visiting a physical therapist to learn exercises and strategies to self-treat the condition. (Yasser Khaled, et al., 2017)
Treatment
Treatment can involve:
Initial treatment focuses on pain relief and jaw function opens and closes improvement.
A guard can help with night teeth grinding/bruxism.
Anti-inflammatory treatments.
In severe cases, surgery may be recommended to correct the problem, as a last resort. (Meghan K Murphy, et al., 2013)
Follow recommendations on what not to do and avoid certain activities.
Quick Patient Initiation
References
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J. P., List, T., Svensson, P., Gonzalez, Y., Lobbezoo, F., Michelotti, A., Brooks, S. L., Ceusters, W., Drangsholt, M., Ettlin, D., Gaul, C., Goldberg, L. J., Haythornthwaite, J. A., Hollender, L., Jensen, R., … Orofacial Pain Special Interest Group, International Association for the Study of Pain (2014). Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. Journal of oral & facial pain and headache, 28(1), 6–27. https://doi.org/10.11607/jop.1151
Santana-Mora, U., López-Cedrún, J., Mora, M. J., Otero, X. L., & Santana-Penín, U. (2013). Temporomandibular disorders: the habitual chewing side syndrome. PloS one, 8(4), e59980. https://doi.org/10.1371/journal.pone.0059980
Garrigós-Pedrón, M., Elizagaray-García, I., Domínguez-Gordillo, A. A., Del-Castillo-Pardo-de-Vera, J. L., & Gil-Martínez, A. (2019). Temporomandibular disorders: improving outcomes using a multidisciplinary approach. Journal of multidisciplinary healthcare, 12, 733–747. https://doi.org/10.2147/JMDH.S178507
Dimitroulis G. (2018). Management of temporomandibular joint disorders: A surgeon’s perspective. Australian Dental Journal, 63 Suppl 1, S79–S90. https://doi.org/10.1111/adj.12593
Khaled Y, Quach JK, Brennan MT, NapeÑas JJ. Outcomes after physical therapy for the treatment of temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol, 2017;124(3: e190. doi:10.1016/j.oooo.2017.05.477
Abouelhuda, A. M., Khalifa, A. K., Kim, Y. K., & Hegazy, S. A. (2018). Non-invasive different modalities of treatment for temporomandibular disorders: a review of the literature. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 44(2), 43–51. https://doi.org/10.5125/jkaoms.2018.44.2.43
Murphy, M. K., MacBarb, R. F., Wong, M. E., & Athanasiou, K. A. (2013). Temporomandibular disorders: a review of etiology, clinical management, and tissue engineering strategies. The International journal of oral & maxillofacial implants, 28(6), e393–e414. https://doi.org/10.11607/jomi.te20
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine