For individuals experiencing tightness in the lower back and hamstrings, can utilizing the sit and reach test help determine an individual’s risk for future pain and injury?
Sit and Reach Test
Lower back and hamstring tightness and pain symptoms are usually brought on by muscle stiffness. The sit-and-reach test is one of the most common ways to measure lower back and hamstring flexibility. Exercise physiologists, physical therapists, chiropractors, and fitness trainers use the sit-and-reach test to measure lower back and hamstring flexibility to assess baseline flexibility. The test has been around since 1952 (Katharine F. Wells & Evelyn K. Dillon 2013) and has an extensive database of results across all age groups and genders.
Individuals can use the sit-and-reach test to compare flexibility to the average result for individuals of the same gender and age.
For healthcare providers, the test may be repeated after several weeks to determine flexibility progress.
Measurement
The test can be a valuable measurement of functional flexibility to sit with the legs straight in front and reach the toes. Jobs, sports, and everyday tasks regularly require bending over, reaching, and lifting objects. These are real-life examples of how having a healthy back and hamstring flexibility is vital in preventing pain symptoms and injuries. New flexibility assessments are currently being developed, and many trainers and therapists use their own versions with patients and clients. But even with more advanced specialized flexibility tests, the sit and reach test can be a functional testing tool for tracking general flexibility changes over time. (Daniel Mayorga-Vega et al., 2014)
Performing The Test
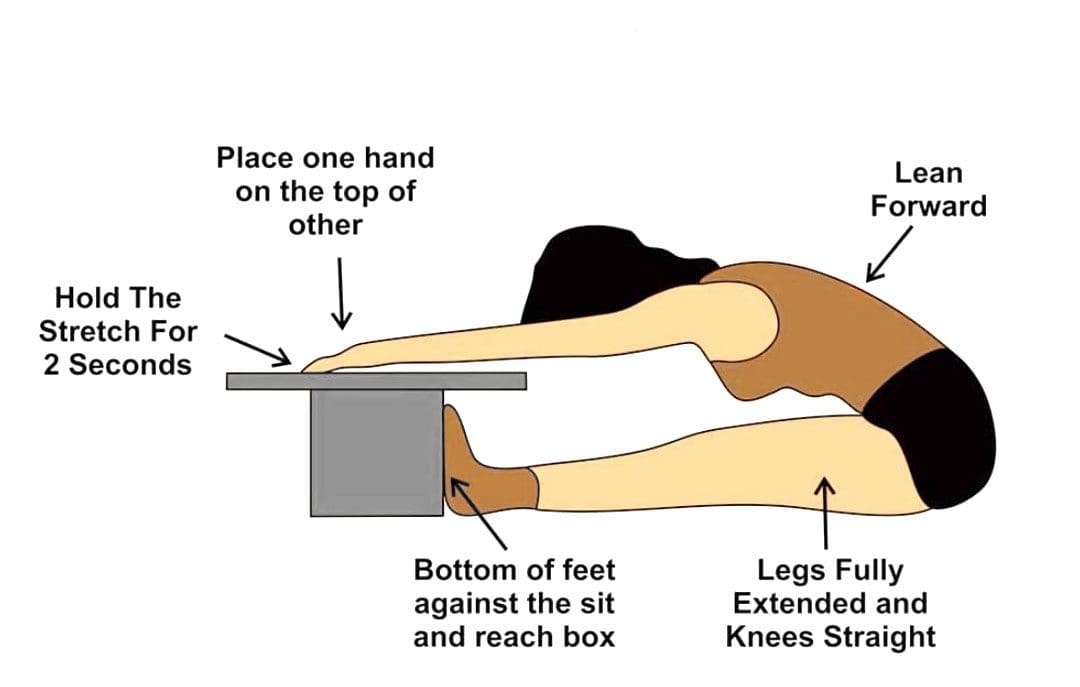
A special sit-and-reach testing box is used; however, individuals can make their own testing box by finding a heavy-duty box around 30cm or 11.811 inches tall. Set a measurement ruler/stick on top of the box so that 26 cm or 10.2362 inches of the ruler extends over the front edge toward the individual being tested. The 26cm mark should be at the edge of the box.
Get into position – Remove shoes and sit on the floor with legs stretched out in front with the knees straight and feet flat against the front end of the test box.
Start the movement – In a slow, steady motion, lean forward, keeping the knees straight, and slide the hands up the ruler as far as possible.
Stretch and repeat – Extend as far as possible, record the results, rest, and repeat three times.
Calculate the results – Average the results.
Results
Results compare flexibility over time to norms, or averages, for gender and age. Adequate flexibility is reaching the toes – the 26-cm mark on the ruler while keeping the legs straight.
Adult Women
37cm or 14.5669 inches or above: Excellent
33 to 36cm or 12.9921 inches: Above average
29 to 32cm or 11.4173 inches: Average
23 to 28cm or 9.05512 inches: Below average
Below 23cm or 8.66142 inches: Poor
Adult Men
34cm or 13.3858 inches or above: Excellent
28 to 33cm or 11.0236 inches: Above average
23 to 27cm or 9.05512 inches: Average
16 to 22cm or 6.29921 inches: Below average
Below 16cm or 5.90551 inches: Poor
Alternatives
Individuals can test their own hamstring and lower back flexibility with some easy at-home tests. Use these methods while working on flexibility, and keep a record to see improvements. (Brittany L. Hansberger et al., 2019) One alternative is the V-sit reach test.
To perform this, make a line on the floor with tape, then place a measuring tape perpendicular to the tape, making a cross.
Sit with the feet in a V shape, touching the tape, feet about a foot apart, with the measuring tape between the legs; the 0 end starts where the legs part.
Overlap hands with arms outstretched in front.
Repeat three times, leaning forward and reaching with hands out.
Then, repeat and take note of how far the hands could reach.
Individuals will need someone to measure the distance between their fingertips and the floor.
Warm up with a few practice stretches of standing and bending toward the floor.
Then, measure how far from the floor the fingertips are.
The ability to touch the floor is a good sign.
Improving Flexibility
Individuals with less than adequate flexibility are recommended to work on stretching the major muscle groups in both the upper and lower body on a regular basis to improve and maintain body flexibility.
Individuals can incorporate dynamic stretching, which consists of active movements utilizing a full range of motion as part of warming up for workouts, sports, or other activities.
Static stretching is recommended when cooling down after the muscles are warmed up and joints are lubricated.
The American College of Sports Medicine recommends 2 to 3 sessions a week of flexibility training and learning to stretch daily.
Stretches should be held for 15 to 30 seconds, then released and repeated 2 to 4 times. (Phil Page 2012)
This will take time and dedication, but with the help of trained specialists, regaining flexibility and full range of motion can be accomplished.
Benefits of Stretching
References
Katharine F. Wells & Evelyn K. Dillon (1952) The Sit and Reach—A Test of Back and Leg Flexibility, Research Quarterly. American Association for Health, Physical Education and Recreation, 23:1, 115-118, DOI: 10.1080/10671188.1952.10761965
Mayorga-Vega, D., Merino-Marban, R., & Viciana, J. (2014). Criterion-Related Validity of Sit-and-Reach Tests for Estimating Hamstring and Lumbar Extensibility: a Meta-Analysis. Journal of sports science & medicine, 13(1), 1–14.
Hansberger, B. L., Loutsch, R., Hancock, C., Bonser, R., Zeigel, A., & Baker, R. T. (2019). EVALUATING THE RELATIONSHIP BETWEEN CLINICAL ASSESSMENTS OF APPARENT HAMSTRING TIGHTNESS: A CORRELATIONAL ANALYSIS. International journal of sports physical therapy, 14(2), 253–263.
Page P. (2012). Current concepts in muscle stretching for exercise and rehabilitation. International journal of sports physical therapy, 7(1), 109–119.
Individuals that have gone through a back injury may develop a synovial spinal cyst as a way to protect the spine that could cause pain symptoms and sensations. Can knowing the signs help healthcare providers develop a thorough treatment plan to relieve pain, prevent worsening of the condition and other spinal conditions?
Spinal Synovial Cysts
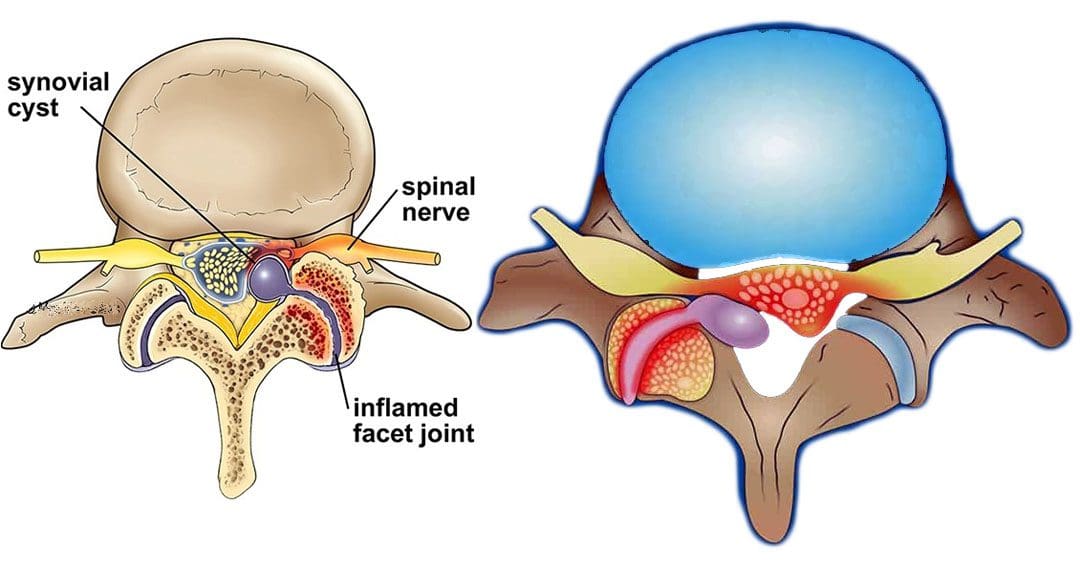
Spinal synovial cysts are benign fluid-filled sacs that develop in the spine’s joints. They form because of spinal degeneration or injury. The cysts can form anywhere in the spine, but most occur in the lumbar region/lower back. They typically develop in the facet joints or junctions that keep the vertebrae/spinal bones interlocked.
Symptoms
In most cases, synovial cysts don’t cause symptoms. However, the doctor or specialist will want to monitor for signs of degenerative disc disease, spinal stenosis, or cauda equina syndrome. When symptoms do present, they typically cause radiculopathy or nerve compression, which can cause back pain, weakness, numbness, and radiating pain caused by the irritation. The severity of symptoms depends on the size and location of the cyst. Synovial cysts can affect one side of the spine or both and can form at one spinal segment or at multiple levels.
Effects Can Include
Radiculopathy symptoms can develop if the cyst or inflammation caused by the cyst comes into contact with a spinal nerve root. This can cause sciatica, weakness, numbness, or difficulty controlling certain muscles.
Neurogenic claudication/impingement and inflammation of spinal nerves can cause cramping, pain, and/or tingling in the lower back, legs, hips, and buttocks. (Martin J. Wilby et al., 2009)
If the spinal cord is involved, it may cause myelopathy/severe spinal cord compression that can cause numbness, weakness, and balance problems. (Dong Shin Kim et al., 2014)
Symptoms related to cauda equina, including bowel and/or bladder problems, leg weakness, and saddle anesthesia/loss of sensation in the thighs, buttocks, and perineum, can present but are rare, as are synovial cysts in the middle back and neck. If thoracic and cervical synovial cysts develop, they can cause symptoms like numbness, tingling, pain, or weakness in the affected area.
Causes
Spinal synovial cysts are generally caused by degenerative changes like osteoarthritis that develop in a joint over time. With regular wear and tear, facet joint cartilage/the material in a joint that provides protection, a smooth surface, friction reduction, and shock absorption begins to waste away. As the process continues, the synovium can form a cyst.
Traumas, large and small, have inflammatory and degenerative effects on joints that can result in the formation of a cyst.
Around a third of individuals who have a spinal synovial cyst also have spondylolisthesis.
This condition is when a vertebrae slips out of place or out of alignment onto the vertebra underneath.
It is a sign of spinal instability.
Instability can occur in any spine area, but L4-5 are the most common levels.
This segment of the spine takes most of the upper body weight.
Epidural corticosteroid injections can reduce inflammation and could be an option to relieve pain.
Patients are recommended to receive no more than three injections per year.
Surgical Options
For severe or persistent cases, a doctor may recommend decompression surgery to remove the cyst and surrounding bone to relieve pressure on the nerve root. Surgical options range from minimally invasive endoscopic procedures to larger, open surgeries. The best surgical option varies based on the severity of the situation and whether associated disorders are present. Surgical options include:
Laminectomy – Removal of the bony structure that protects and covers the spinal canal/lamina.
Hemilaminectomy – A modified laminectomy where a smaller portion of the lamina is removed.
Facetectomy – The removal of part of the affected facet joint where the synovial cyst is located, usually following a laminectomy or hemilaminectomy.
Fusionof the facet joints and vertebra – Decreases vertebral mobility in the injured area.
Most individuals experience immediate pain relief following a laminectomy or hemilaminectomy.
Fusion can take six to nine months to heal completely.
If surgery is performed without fusion where the cyst originated, the pain could return, and another cyst could form within two years.
Surgery Complications include infection, bleeding, and injury to the spinal cord or nerve root.
How I Gained My Mobility Back With Chiropractic
References
Wilby, M. J., Fraser, R. D., Vernon-Roberts, B., & Moore, R. J. (2009). The prevalence and pathogenesis of synovial cysts within the ligamentum flavum in patients with lumbar spinal stenosis and radiculopathy. Spine, 34(23), 2518–2524. https://doi.org/10.1097/BRS.0b013e3181b22bd0
Kim, D. S., Yang, J. S., Cho, Y. J., & Kang, S. H. (2014). Acute myelopathy caused by a cervical synovial cyst. Journal of Korean Neurosurgical Society, 56(1), 55–57. https://doi.org/10.3340/jkns.2014.56.1.55
Epstein, N. E., & Baisden, J. (2012). The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surgical neurology international, 3(Suppl 3), S157–S166. https://doi.org/10.4103/2152-7806.98576
For individuals trying to achieve healthy posture, could using posture awareness training be effective in treatment and prevention?
Posture Awareness
Spinal curves help support the body’s weight, movement, and balance. Five areas include the neck, upper back, lower back, sacrum, and coccyx. The bottom of the spine or sacrum rests between the two hip bones that comprise the pelvis. Because of this location, the movements made with the pelvis significantly affect the spine. (Ibrahim Alkatout, et al., 2021) When the pelvis moves, the spine moves.
Posture-related back pain and associated symptoms are often caused by a weakened strength and flexibility ratio between the opposing muscle groups that hold the body upright.
Achieving healthy posture requires technique and consistent practice for maintaining a healthy pelvis and low back curve. (DeokJu Kim, et al., 2015)
Finding the low back curve and exploring how it responds when moving the pelvis is important to effective posture awareness training.
Kim, D., Cho, M., Park, Y., & Yang, Y. (2015). Effect of an exercise program for posture correction on musculoskeletal pain. Journal of physical therapy science, 27(6), 1791–1794. https://doi.org/10.1589/jpts.27.1791
Alkatout, I., Wedel, T., Pape, J., Possover, M., & Dhanawat, J. (2021). Review: Pelvic nerves - from anatomy and physiology to clinical applications. Translational neuroscience, 12(1), 362–378. https://doi.org/10.1515/tnsci-2020-0184
Żurawski, A. Ł., Kiebzak, W. P., Kowalski, I. M., Śliwiński, G., & Śliwiński, Z. (2020). Evaluation of the association between postural control and sagittal curvature of the spine. PloS one, 15(10), e0241228. https://doi.org/10.1371/journal.pone.0241228
Zemková, E., & Zapletalová, L. (2021). Back Problems: Pros and Cons of Core Strengthening Exercises as a Part of Athlete Training. International journal of environmental research and public health, 18(10), 5400. https://doi.org/10.3390/ijerph18105400
For women experiencing lower back and pelvic pain, could understanding symptoms help in the diagnostic process, treatment options, and prevention?
Low Back and Pelvic Pain In Women
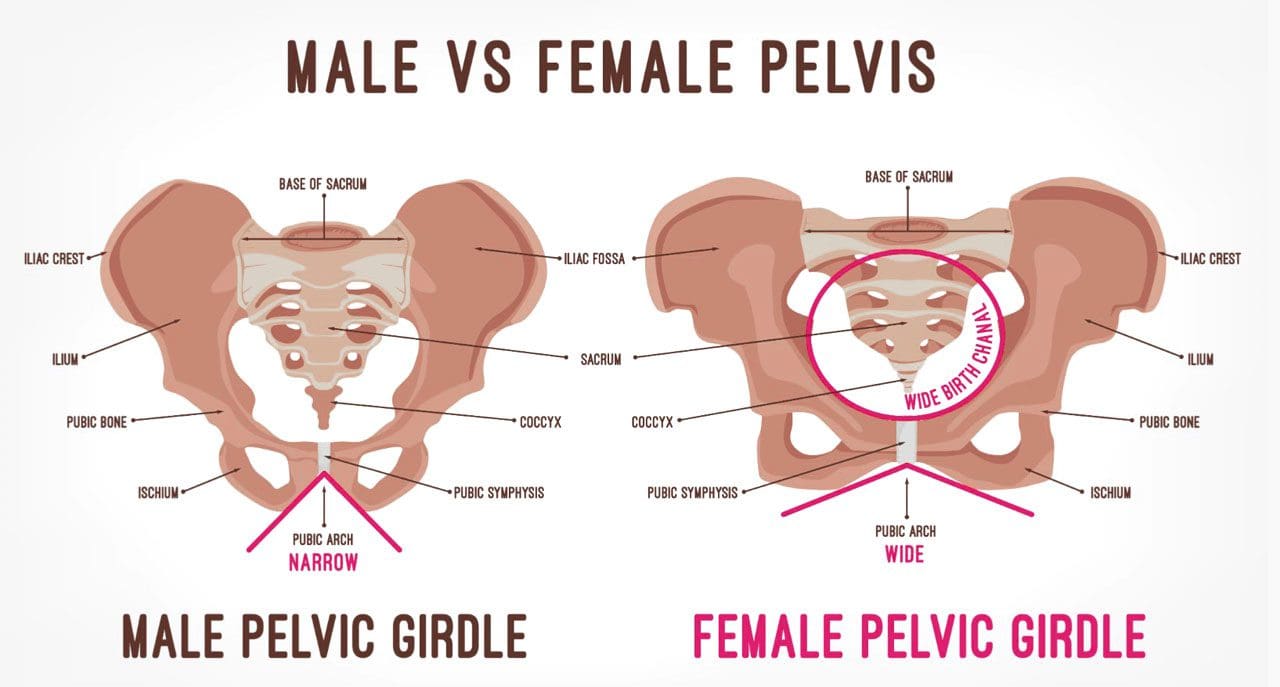
In women, lower back and hip pain that radiates to the front pelvis area can have a variety of causes. The pain can feel dull, sharp, or burning. The main causes of lower back and pelvic pain in women fall into two categories. (William S. Richardson, et al., 2009)
Musculoskeletal and nervous system
Related causes of pain affect how your muscles, nerves, ligaments, joints, and bones move.
Examples include sciatica, arthritis, and injury.
Other organ system-based
Causes may stem from the following:
Acute/chronic conditions or infections
Kidneys – stones, infection, and other ailments or conditions.
Reproductive system – such as the ovaries.
Gastrointestinal system – inguinal hernias or appendix.
Musculoskeletal and Nervous System Causes
Musculoskeletal and nervous system-related causes can be from injuries like a fall or practicing unhealthy posture.
Overuse Injuries and Trauma
Frequent use and repetitive movements can lead to overuse injuries to the muscles, ligaments, and joints. :
Exercises, sports, and physical activities that require repetitive twisting and bending.
Lifting, carrying, and placing objects that require movements that are repeated regularly.
Trauma from vehicle collisions, accidents, falls, or sports accidents can inflict acute and chronic bodily injuries, like strained muscles or broken bones.
Depending on the type of trauma, healing and recovery time and treatment vary.
Both types of injuries can lead to numbness, tingling, pain, stiffness, popping sensations, and/or weakness in the legs.
Mobility Problems
Over time, a decreased range of motion and mobility in muscles and joints can cause discomfort and pain. Causes include:
Long periods of time spent in the same position.
Sitting for extended periods.
The pain often feels dull, achy, and stiff.
It can also lead to muscle spasms characterized by quick episodes of sharp and intense pain.
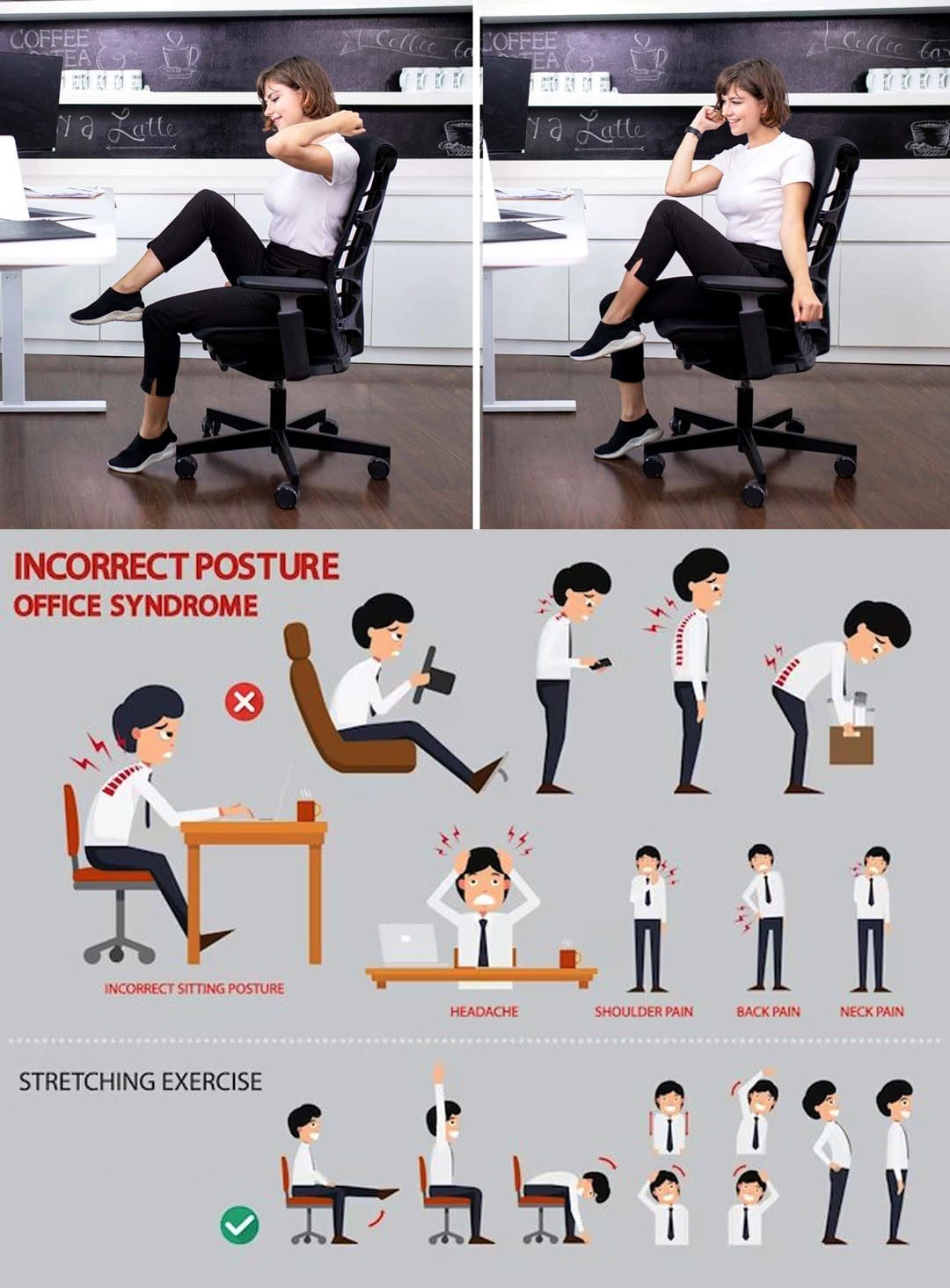
Posture
Posture while sitting, standing, and walking affects the body’s range of motion.
It can affect the nerves and blood circulation to the back and pelvic region.
Prolonged unhealthy postures can contribute to lower back pain and muscle strain.
Posture-related symptoms can feel achy and stiff and lead to quick episodes of severe or intense pain, depending on the position.
Sciatica and Nerve Compression
A bulging or herniating vertebral disc most commonly causes sciatica and pinched or compressed nerves.
The sensations can be sharp, burning, electrical, and/or radiating pain along the nerve pathway.
Arthritis
Arthritis inflammation causes swelling, stiffness, pain, and the breakdown of cartilage that cushions the joints.
Hip arthritis causes groin pain that can radiate to the back and becomes more intense when standing or walking.
Thoracic and lumbar spine arthritis, or degenerative disc disease, are other common causes of back pain.
Sacroiliac Joint Dysfunction
The sacroiliac joints connect the lower spine and pelvis.
When these joints move too much or too little, it can cause sacroiliac joint pain, leading to a burning sensation in the lower back and pelvic area. (Daisuke Kurosawa, Eiichi Murakami, Toshimi Aizawa. 2017)
Renal and Urinary Causes
Kidney Stones
Kidney stones are the build-up of minerals and salts, which form into hard stones in the kidneys.
When the kidney stone begins to move to the bladder, pain symptoms will present.
It can trigger severe back and side pain that radiates to the pelvic region.
Other symptoms include – a change in urine color, pain when urinating, nausea, and vomiting.
Kidney Infection and Urinary Tract Infections
Urinary tract and kidney infections are also causes of lower back and pelvic pain in women.
They cause fever, continued urge to urinate, and painful urination.
Gynecological Causes
Pelvic Inflammatory Disease
Infections, known as pelvic inflammatory disease, occur when sexually transmitted bacteria spread through the vagina, womb, fallopian tubes, or ovaries. Symptoms include:
Pain during intercourse.
Bleeding between periods.
Vaginal discharge.
Pain in the lower abdomen or groin.
Fever.
Ovarian Cysts
The cyst can be a solid or fluid-filled sac on the surface or within an ovary.
Small ovarian cysts are unlikely to cause pain.
Large cysts or those that rupture can cause mild to severe pain.
The pain can occur during menstruation or intercourse and present acutely in the back, pelvis, or lower abdomen.
During Pregnancy
Back pain and discomfort in the pelvis area are common.
As the body adjusts, the bones and round ligaments in the pelvis move and stretch, which can cause discomfort.
Symptoms are usually normal but should be discussed with a healthcare provider during check-ups.
Pain in the lower back and groin can be a sign of miscarriage or labor – including preterm labor.
Sexually Transmitted Infection
Sexually transmitted infections, like chlamydia or gonorrhea, can cause lower back and groin pain.
Other symptoms can include – painful urination, vaginal discharge, intercourse pain, and bleeding between periods.
Yeast Infection
A yeast infection – overgrowth of the fungus candidiasis.
A common vaginal infection with symptoms including – itching, swelling, irritation, and pelvic pain.
Other Causes
Appendicitis
When the appendix becomes blocked, infected, and inflamed.
In most cases, a major symptom is pain that starts near or around the belly button.
In other cases, it can start in the lower back and radiate to the right side of the pelvic area. (Johns Hopkins Medicine. 2023)
Associated pain can worsen over time or when coughing, moving, or taking deep breaths.
It involves soft tissue and part of the intestine, pushing through weak groin muscles.
Pain presents in the abdomen, lower back, or pelvis, especially when bending or lifting objects.
Pancreatitis
Inflammation in the pancreas.
Infection, bile stones, or alcohol can cause it.
One symptom is abdominal pain that radiates to the back.
The pain becomes worse during and after eating.
Other symptoms include nausea, vomiting, and fever.
Enlarged Lymph Nodes
Lymph nodes lie in the internal and external regions of the iliac artery in the pelvis.
These can become enlarged by infection, injury, and, in rare cases, cancer.
Symptoms include pain, swelling, redness, skin irritation, and fever.
Enlarged Spleen
The spleen is located behind the left side of the rib cage.
It filters the blood and supports new blood cell creation.
Infections and diseases can cause the spleen to become enlarged.
An enlarged spleen – a condition known as splenomegaly – causes pain in the upper left part of the belly and sometimes the left shoulder and upper back.
However, some individuals with an enlarged spleen experience abdominal symptoms – not being able to eat without discomfort. (Mount Sinai. 2023)
Diagnosis
Depending on the cause of your pain, a healthcare provider may be able to diagnose it with a physical exam and by asking questions about your condition.
Other tests may be needed to find the cause, particularly blood work and imaging (X-ray or magnetic resonance imaging).
Treatment
Treatment of symptoms depends on the cause.
Once a diagnosis is made, an effective treatment plan will be developed and contain a combination of therapies:
Lifestyle Adjustments
For injuries caused by muscle strains, joint sprains, overuse, and smaller traumas, pain can be resolved with:
Rest
Ice therapy
Over-the-counter pain relievers – acetaminophen or ibuprofen.
Braces or compression wraps can help support the body and alleviate symptoms during healing and recovery.
Exercises to improve posture
Paying attention to form when lifting objects
Stretching can help ease the pain.
Medication
Medications can be used in a variety of ways to help in the treatment of lower back and pelvic pain. If an infection is the cause, medications will be prescribed to remove the infection and resolve the symptoms, which can include:
Antibiotics
Antifungals
Antivirals
Medications may also be prescribed to help manage pain symptoms and may include:
Medication to relieve nerve pain
Muscle relaxants
Steroids
Physical Therapy
A physical therapist can help to correct problems with:
Posture
Decreased mobility
Walking gait
Strengthening
A physical therapist will provide exercises to help increase and maintain strength, range of motion, and flexibility.
Pelvic Floor Therapy
This is physical therapy that focuses on the muscles, ligaments, and connective tissues in the pelvis.
It helps with pain, weakness, and dysfunction in the pelvic area.
A treatment plan will be developed to help with strength and range of motion in the pelvic muscles.
Chiropractic Care
Chiropractors offer spinal and hip adjustments to realign the joints of the spine.
Some more severe conditions could require surgery.
Ovarian cysts, hernias, and other infections sometimes require surgery to remove infected or unhealthy tissue – ruptured ovarian cysts or appendicitis.
Recommended surgeries can include:
A hernia repair.
Hip replacement.
Gallbladder removal to prevent recurring pancreatitis.
Prevention
Not all conditions and diseases cause lower back and pelvic pain. Symptoms can be prevented and reduced by adopting lifestyle changes. Prevention recommendations can include:
Staying hydrated.
Using proper bending and lifting techniques.
Eating healthy foods.
Regularly engaging in some form of physical activity – walking, swimming, yoga, cycling, or strength training.
Maintaining a healthy weight.
Pregnancy and Sciatica
References
Richardson, W. S., Jones, D. G., Winters, J. C., & McQueen, M. A. (2009). The treatment of inguinal pain. Ochsner journal, 9(1), 11–13.
Kurosawa, D., Murakami, E., & Aizawa, T. (2017). Groin pain associated with sacroiliac joint dysfunction and lumbar disorders. Clinical neurology and neurosurgery, 161, 104–109. https://doi.org/10.1016/j.clineuro.2017.08.018
Santilli, V., Beghi, E., & Finucci, S. (2006). Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. The spine journal : official journal of the North American Spine Society, 6(2), 131–137. https://doi.org/10.1016/j.spinee.2005.08.001
Individuals dealing with chronic knee discomfort, hip tightness, and lower back pain could be experiencing dormant gluteal-butt syndrome. Can recognizing the symptoms and signs and incorporating lower body and core fitness help prevent and treat the condition?
Dormant Gluteal Butt Syndrome
Knee, hip, and lower back problems could be traced back to weakened buttocks. Some scientists call the condition “dormant butt syndrome” (Ohio State University, .2023). However, researchers are learning about the important role the gluteal muscles provide in maintaining the lower body strong and healthy. (Hal David Martin, Manoj Reddy, Juan Gómez-Hoyos. 2015)
What Is It?
The syndrome is defined as weak buttock muscles and tight hip flexors. Experts from the Ohio State Wexner Medical Center have worked with individuals dealing with knee, hip, or back injuries and believe many of these issues are linked to weakened gluteal muscles. (Ohio State University.2023) The glutes are the muscles of the hips and buttocks. Weakened muscles fail to absorb the shock they’re supposed to during activities, which results in overloading the surrounding muscles and joints and increases the risk of injury. (Ohio State University, .2023)
Dormant gluteal-butt syndrome can result from a sedentary lifestyle and prolonged inactivity, like sitting for long periods.
The condition also occurs in runners and other physically active individuals who forget about these muscles with targeted exercises.
Exercises
Exercises to target the gluteals and prevent dormant gluteal-butt syndrome include activities/exercises that work the hips and core.
When walking properly, the gluteals should execute hip extension naturally.
Unhealthy postures, excessive sitting, and continued dysfunctional biomechanics mean walking without achieving optimal hip extension. (Hadi Daneshmandi. 2017)
When this happens, the gluteal muscles never get to fully function work, ending up with a series of aches and pains.
Pilates exercises can be adjusted to address order, repetition, and variation to strengthen the gluteals. (Laís Campos de Oliveira, 2015)
Hamstring Curls
Lie face down on an exercise mat.
Use your hands to create a cushion for the forehead.
Bend both knees so the feet point up towards the ceiling.
Let the knees be slightly apart, but keep the heels together.
Squeeze the heels together and tighten the gluteal muscles.
Hold for 3 seconds, then release the buttocks.
Repeat 10 times and then rest.
Hamstring curls can also be done using a weight machine.
Place the hands just behind the backside with the fingers pointing forward if possible.
Raise the body up.
Keep your head up and look straight ahead.
Raise one leg as high as possible.
Hold for as long as possible.
Lower and raise the other leg.
Repeat for a total of 3 reps.
Lining Up With A Wall Posture Helper
Standing posture is important to proper buttock function. Lining the body up with a wall can help train the body to maintain proper posture.
Find a wall and stand against it from the heels to the back of the head.
Work the backs of the legs and spine as firmly as possible into the wall.
Work to get the back of the skull into the wall as well.
Add some abdominal work by working the waistline inward and upward.
Hold for up to one minute.
The alignment is how you want to hold your body.
As you move off the wall, learn to maintain that posture throughout the day and night.
Repeat the wall exercise several times for reinforcement.
If aching of the hip, back, or knee is part of daily struggles, working out the gluteal muscles may be the solution. Contact the Injury Medical Chiropractic and Functional Medicine Clinic for a full consultation.
Martin, H. D., Reddy, M., & Gómez-Hoyos, J. (2015). Deep gluteal syndrome. Journal of hip preservation surgery, 2(2), 99–107. https://doi.org/10.1093/jhps/hnv029
Daneshmandi, H., Choobineh, A., Ghaem, H., & Karimi, M. (2017). Adverse Effects of Prolonged Sitting Behavior on the General Health of Office Workers. Journal of lifestyle medicine, 7(2), 69–75. https://doi.org/10.15280/jlm.2017.7.2.69
Campos de Oliveira, L., Gonçalves de Oliveira, R., & Pires-Oliveira, D. A. (2015). Effects of Pilates on muscle strength, postural balance and quality of life of older adults: a randomized, controlled, clinical trial. Journal of physical therapy science, 27(3), 871–876. https://doi.org/10.1589/jpts.27.871
Individuals with fixed sagittal imbalance, a condition where the normal curve of the lower spine is greatly reduced or absent altogether that can cause pain and difficulty balancing. Can chiropractic treatment, physical therapy, and exercise help improve the condition?
Fixed Sagittal Imbalance
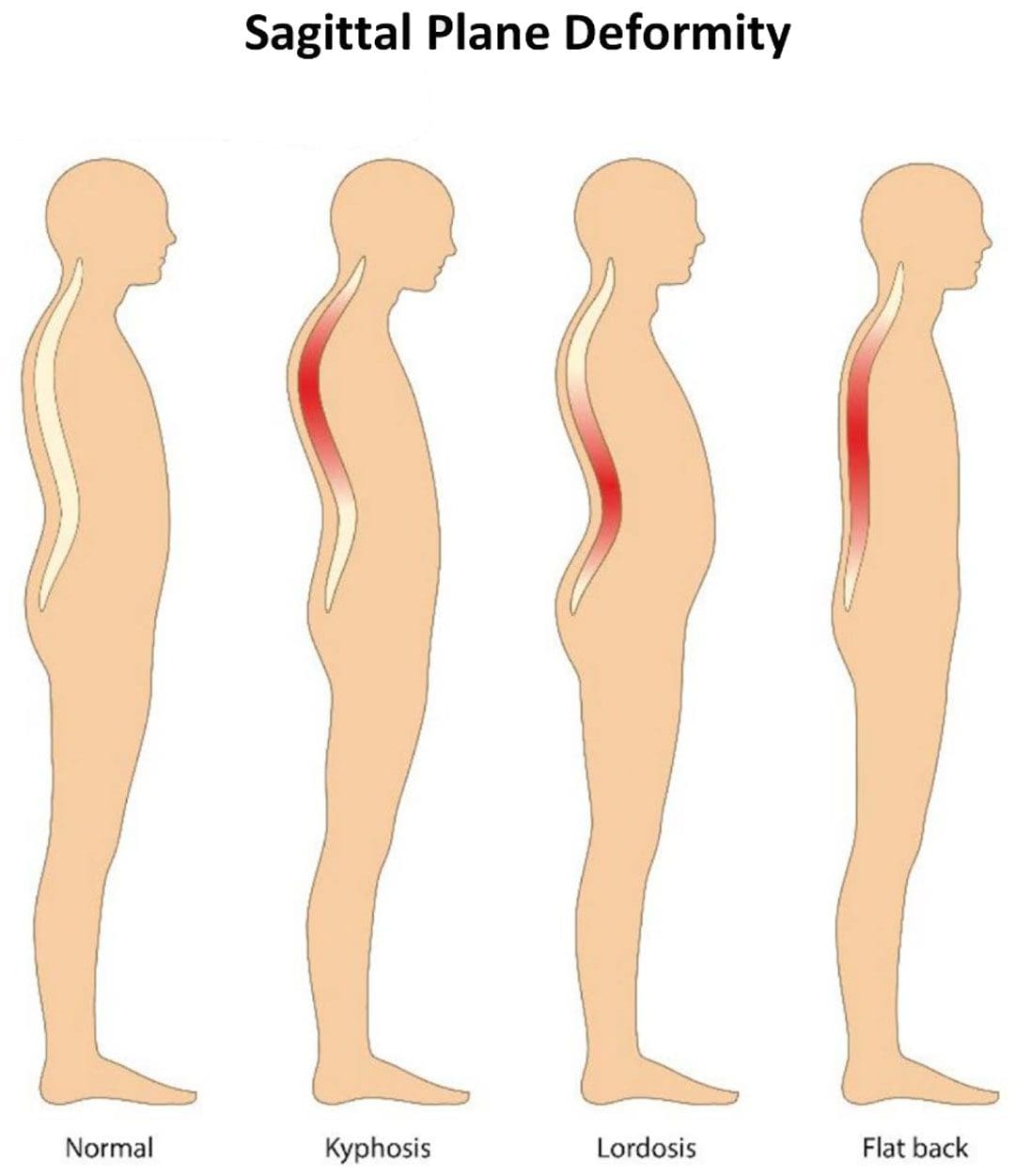
The condition is commonly known as flat back syndrome and can be present at birth or can happen as a result of surgery or a medical condition.
Individuals with flat back syndrome position their head and neck too far forward.
A major symptom is difficulty standing for long periods of time.
Symptoms
The spine has two curves. The lumbar spine in the lower back and cervical spine in the neck curve inward. The thoracic spine in the upper back curves outward. The curves are part of the spine’s natural alignment. They help the body balance and maintain the center of gravity.
If these curves begin to disappear the body can have trouble and difficulty standing up straight.
The loss of curvature causes the head and neck to pitch forward, making it hard to walk and do regular normal activities.
A chiropractor and/or physical therapist can recommend exercises and other forms of treatment. (Won-Moon Kim, et al., 2021)
Life-Changing Chiropractic Relief
References
Columbia University Irving Medical Center. Flatback syndrome.
National Health Service. Common posture mistakes and fixes.
Lee, B. H., Hyun, S. J., Kim, K. J., Jahng, T. A., Kim, Y. J., & Kim, H. J. (2018). Clinical and Radiological Outcomes of Posterior Vertebral Column Resection for Severe Spinal Deformities. Journal of Korean Neurosurgical Society, 61(2), 251–257. https://doi.org/10.3340/jkns.2017.0181
Kim, W. M., Seo, Y. G., Park, Y. J., Cho, H. S., & Lee, C. H. (2021). Effect of Different Exercise Types on the Cross-Sectional Area and Lumbar Lordosis Angle in Patients with Flat Back Syndrome. International journal of environmental research and public health, 18(20), 10923. https://doi.org/10.3390/ijerph182010923
The lumbosacral plexus is located on the posterolateral wall of the lesser pelvis, next to the lumbar spine. A plexus is a network of intersecting nerves that share roots, branches, and functions. The sacral plexus is a network that emerges from the lower part of the spine. The plexus then embeds itself into the psoas major muscle and emerges in the pelvis. These nerves provide motor control to and receive sensory information from portions of the pelvis and leg. Sacral nerve discomfort symptoms, numbness, or other sensations and pain can be caused by an injury, especially if the nerve roots are compressed, tangled, rubbing, and irritated. This can cause symptoms like back pain, pain in the back and sides of the legs, sensory issues affecting the groin and buttocks, and bladder or bowel problems. Injury Medical Chiropractic and Functional Medicine Clinic can develop a personalized treatment plan to relieve symptoms, release the nerves, relax the muscles, and restore function.
Sacral Plexus
Anatomy
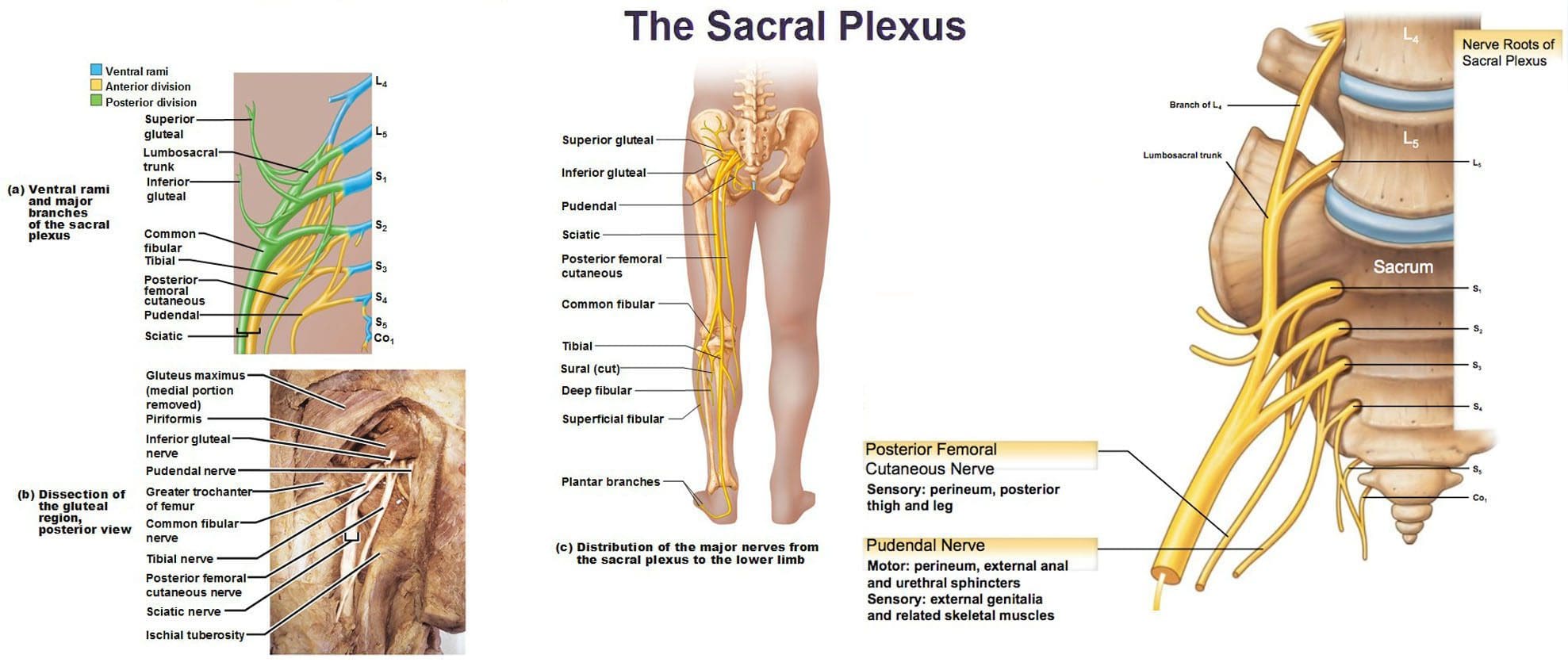
The sacral plexus is formed by the lumbar spinal nerves, L4 and L5, and sacral nerves S1 through S4.
Several combinations of these spinal nerves merge together and then divide into the branches of the sacral plexus.
Everybody has two sacral plexi – plural of plexus – one on the right side and left side that is symmetrical in structure and function.
Structure
There are several plexi throughout the body. The sacral plexus covers a large area of the body in terms of motor and sensory nerve function.
Spinal nerves L4 and L5 make up the lumbosacral trunk, and the anterior rami of sacral spinal nerves S1, S2, S3, and S4 join the lumbosacral trunk to form the sacral plexus.
Anterior rami are the branches of the nerve that are towards the front of the spinal cord/front of the body.
At each spinal level, an anterior motor root and a posterior sensory root join to form a spinal nerve.
Each spinal nerve then divides into an anterior – ventral – and a posterior – dorsal – rami portion.
Each can have motor and/or sensory functions.
The sacral plexus divides into several nerve branches, which include:
Superior gluteal nerve – L4, L5, and S1.
Inferior gluteal nerve – L5, S1, and S2.
The sciatic nerve – is the largest nerve of the sacral plexus and among the largest nerves in the body – L4, L5, S1, S2, and S3
The common fibular nerve – L4 through S2, and tibial nerves – L4 through S3 are branches of the sciatic nerve.
Posterior femoral cutaneous nerve – S1, S2, and S3.
Pudendal nerve – S2, S3, and S4.
The nerve to the quadratus femoris muscle is formed by L4, L5, and S1.
The obturator internus muscle nerve – L5, S1, and S2.
The piriformis muscle nerve – S1 and S2.
Function
The sacral plexus has substantial functions throughout the pelvis and legs. The branches provide nerve stimulation to several muscles. The sacral plexus nerve branches also receive sensory messages from the skin, joints, and structures of the pelvis and legs.
Motor
Motor nerves of the sacral plexus receive signals from the brain that travel down the column of the spine, out to the motor nerve branches of the sacral plexus to stimulate muscle contraction and movement. Motor nerves of the sacral plexus include:
Superior Gluteal Nerve
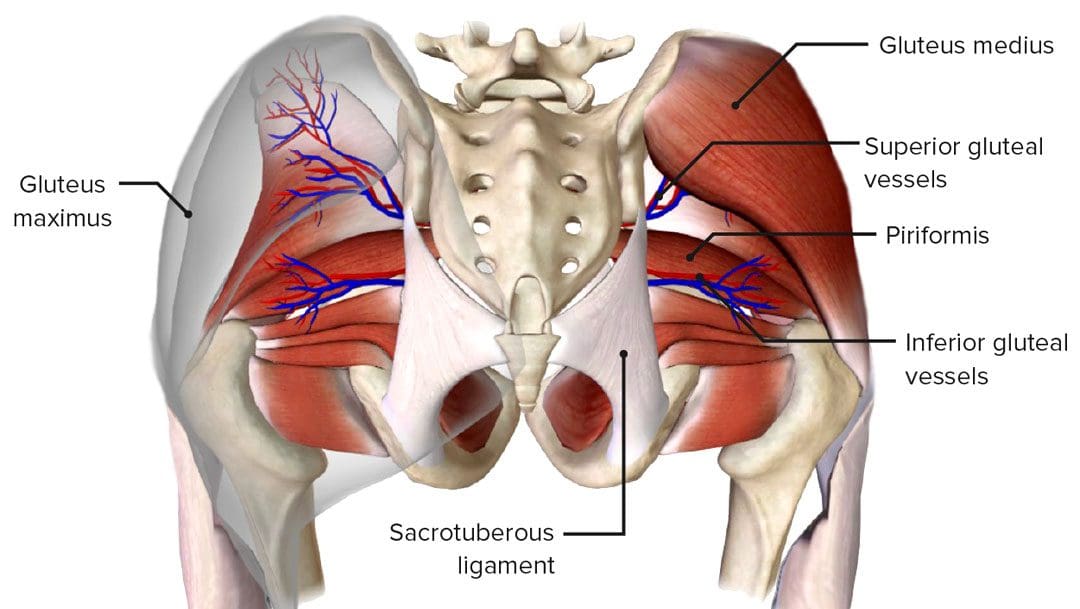
This nerve provides stimulation to the gluteus minimus, gluteus medius, and tensor fascia lata, which are muscles that help move the hip away from the center of the body.
Inferior Gluteal Nerve
This nerve provides stimulation to the gluteus maximus, the large muscle that moves the hip laterally.
Sciatic Nerve
The sciatic nerve has a tibial portion and a common fibular portion, which have motor and sensory functions.
The tibial portion stimulates the inner part of the thigh and activates muscles in the back of the leg and the sole of the foot.
The common fibular portion of the sciatic nerve stimulates and moves the thigh and knee.
The common fibular nerve stimulates muscles in the front and sides of the legs and extends the toes to straighten them out.
Pudendal Nerve
The pudendal nerve also has sensory functions that stimulate the muscles of the urethral sphincter to control urination and the muscles of the anal sphincter to control defecation.
The nerve to the quadratus femoris stimulates the muscle to move the thigh.
The nerve to the obturator internus muscle stimulates the muscle to rotate the hips and stabilize the body when walking.
The nerve to the piriformis muscle stimulates the muscle to move the thigh away from the body.
Conditions
The sacral plexus, or areas of the plexus, can be affected by disease, traumatic injury, or cancer. Because the nerve network has many branches and portions, symptoms can be confusing. Individuals may experience sensory loss or pain in regions in the pelvis and leg, with or without muscle weakness. Conditions that affect the sacral plexus include:
Injury
A traumatic injury of the pelvis can stretch, tear, or harm the sacral plexus nerves.
Bleeding can inflame and compress the nerves, causing malfunction.
Neuropathy
Nerve impairment can affect the sacral plexus or parts of it.
Neuropathy can come from:
Diabetes
Vitamin B12 deficiency
Certain medications – chemotherapeutic meds
Toxins like lead
Alcohol
Metabolic illnesses
Infection
An infection of the spine or the pelvic region can spread to the sacral plexus nerves or produce an abscess, causing symptoms of nerve impairment, pain, tenderness, and sensations around the infected region.
Cancer
Cancer developing in the pelvis or spreading to the pelvis from somewhere else can compress or infect the sacral plexus nerves.
Treatment of the Underlying Medical Condition
Rehabilitation begins with the treatment of the underlying medical condition causing the nerve problems.
Cancer treatment – surgery, chemotherapy, and/or radiation.
Antibiotic treatment for infections.
Neuropathy treatment can be complicated because the cause may be unclear, and an individual can experience several causes of neuropathy simultaneously.
Major pelvic trauma like a vehicle collision can take months, especially if there are multiple bone fractures.
Motor and Sensory Recovery
Sensory problems can interfere with walking, standing, and sitting.
Adapting to sensory deficits is an important part of treatment, rehabilitation, and recovery.
Chiropractic, decompression, massage, and physical therapy can relieve symptoms, restore strength, function, and motor control.
Sciatica Secrets Revealed
References
Dujardin, Franck et al. “Extended anterolateral transiliac approach to the sacral plexus.” Orthopaedics & traumatology, surgery & research: OTSR vol. 106,5 (2020): 841-844. doi:10.1016/j.otsr.2020.04.011
Eggleton JS, Cunha B. Anatomy, Abdomen and Pelvis, Pelvic Outlet. [Updated 2022 Aug 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557602/
Garozzo, Debora et al. “In lumbosacral plexus injuries can we identify indicators that predict spontaneous recovery or the need for surgical treatment? Results from a clinical study on 72 patients.” Journal of brachial plexus and peripheral nerve injury vol. 9,1 1. 11 Jan. 2014, doi:10.1186/1749-7221-9-1
Gasparotti R, Shah L. Brachial and Lumbosacral Plexus and Peripheral Nerves. 2020 Feb 15. In: Hodler J, Kubik-Huch RA, von Schulthess GK, editors. Diseases of the Brain, Head and Neck, Spine 2020–2023: Diagnostic Imaging [Internet]. Cham (CH): Springer; 2020. Chapter 20. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554335/ doi: 10.1007/978-3-030-38490-6_20
Norderval, Stig, et al. “Sacral nerve stimulation.” Tidsskrift for den Norske laegeforening : tidsskrift for praktisk medicin, ny raekke vol. 131,12 (2011): 1190-3. doi:10.4045/tidsskr.10.1417
Neufeld, Ethan A et al. “MR Imaging of the Lumbosacral Plexus: A Review of Techniques and Pathologies.” Journal of Neuroimaging: official journal of the American Society of Neuroimaging vol. 25,5 (2015): 691-703. doi:10.1111/jon.12253
Staff, Nathan P, and Anthony J Windebank. “Peripheral neuropathy due to vitamin deficiency, toxins, and medications.” Continuum (Minneapolis, Minn.) vol. 20,5 Peripheral Nervous System Disorders (2014): 1293-306. doi:10.1212/01.CON.0000455880.06675.5a
Yin, Gang, et al. “Obturator Nerve Transfer to the Branch of the Tibial Nerve Innervating the Gastrocnemius Muscle for the Treatment of Sacral Plexus Nerve Injury.” Neurosurgery vol. 78,4 (2016): 546-51. doi:10.1227/NEU.0000000000001166
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine