Referred pain is the interpretation of feeling pain in a different location than the actual cause. For example, a pinched nerve in the spine/back causes pain not to show up not where it is pinching but further down in the buttock, leg, calf, or foot. Similarly, a pinched nerve in the neck could translate to shoulder or elbow pain. Referred pain is often caused by the muscles overcompensating weaker ones, like feeling pain outside the knee, with the actual injury stemming from hip joint dysfunction caused by weakened lateral hip muscles. The athletic referred pain could have been brought on by an acute sports injury, an overuse injury from the repetitive motion/s.
Athletic Referred Pain
Somatic referred pain originates from the muscles, skin, and other soft tissues and is not to be confused with visceral pain, which refers to the internal organs/viscera. However, the pain presents in regions supplied by the same nerve roots. Damaged or injured body structures can cause referred pain. This includes the muscles, nerves, ligaments, and bones.
Common Sites
Individuals can experience referred pain almost anywhere. Athletic referred pain commonly occurs in these areas:
The neck and shoulder where pain can be felt in the elbow, arm, and hand or cause headaches.
The back where pain can be felt in the hips, buttocks, and thighs.
The hip/s area, where pain can be felt in and around the low back and abdominal regions.
The groin, where pain can be felt in and around the abdominal region.
Problems with the vertebral discs, nerve root compression, muscle spasms, osteoarthritic changes, spinal fracture, or tumor/s can affect the body’s ability to transport sensory information, which can cause strange sensations and weakness of muscle tissues, and sometimes problems with coordination and movement. Part of an accurate diagnosis is knowing the patterns of referred pain in all the muscles and internal organs.
Pain Activation
Many nerve endings come together and share the same nerve cell group in the spinal cord. When signals travel through the spinal cord to the brain, some signals follow the same path as the pain signals from a different body part. Pain awareness is felt in a deeper center of the brain known as the thalamus, but the sensory cortex determines the perception of where the pain is coming from and the location of the pain. The intensity and sensation of the athletic referred somatic pain vary for different structures and depend on the inflammation level. For example:
Nerve pain tends to be sharp or shooting.
Muscle pain tends to be a deep dull aching or a burning sensation.
However, muscles can give a sensation of tingling where referred pain is presenting, but tingling is more commonly associated with a nerve injury.
Diagnosing referred pain injuries can be complex as there are various areas where the pain can show up. The source of damage needs to be identified; otherwise, achieving lasting pain relief will not last. A biomechanical analysis can help to find movement/motion patterns that may be causing pain and help identify the source.
Treatment
Athletic performance and spinal health are interconnected. Chiropractic treatment involves whole-body wellness that involves the spine and nervous system. Routine chiropractic care relieves neck, shoulder, arm, back, leg, and foot conditions/injuries and helps prevent disorders of joints and muscles. It calms the mind, provides pain relief, and educates individuals on being more aware of the body. Chiropractic adjustments improve blood flow and nerve function to increase agility, reaction times, balance, strength, and expedited healing of the body.
DRX9000 Decompression
References
Kapitza, Camilla, et al. “Application and utility of a clinical framework for spinally referred neck-arm pain: A cross-sectional and longitudinal study protocol.” PloS one vol. 15,12 e0244137. 28 Dec. 2020, doi:10.1371/journal.pone.0244137
Murray, Greg M. “Guest Editorial: referred pain.” Journal of applied oral science: Revista FOB vol. 17,6 (2009): i. doi:10.1590/s1678-77572009000600001
Weller, Jason L et al. “Myofascial Pain.” Seminars in neurology vol. 38,6 (2018): 640-643. doi:10.1055/s-0038-1673674
Wilke, Jan, et al. “What Is Evidence-Based About Myofascial Chains: A Systematic Review.” Archives of physical medicine and rehabilitation vol. 97,3 (2016): 454-61. doi:10.1016/j.apmr.2015.07.023
Forearm pain refers to soreness, aches, or discomfort between the wrist and the elbow. An injury or inflammation can affect any tissues, including muscles, bones, blood vessels, tendons, and the skin. The causes usually include overuse injuries, pinched nerves, accidents causing trauma, lifting or heaving heavy objects, sports injuries, and fractures. If left untreated, issues like chronic muscle pain and decreased and disrupted blood/nerve circulation can develop, leading to numbness and weakness. Chiropractic treatment can release tension, massage, reset, and stretch the muscles to expedite healing.
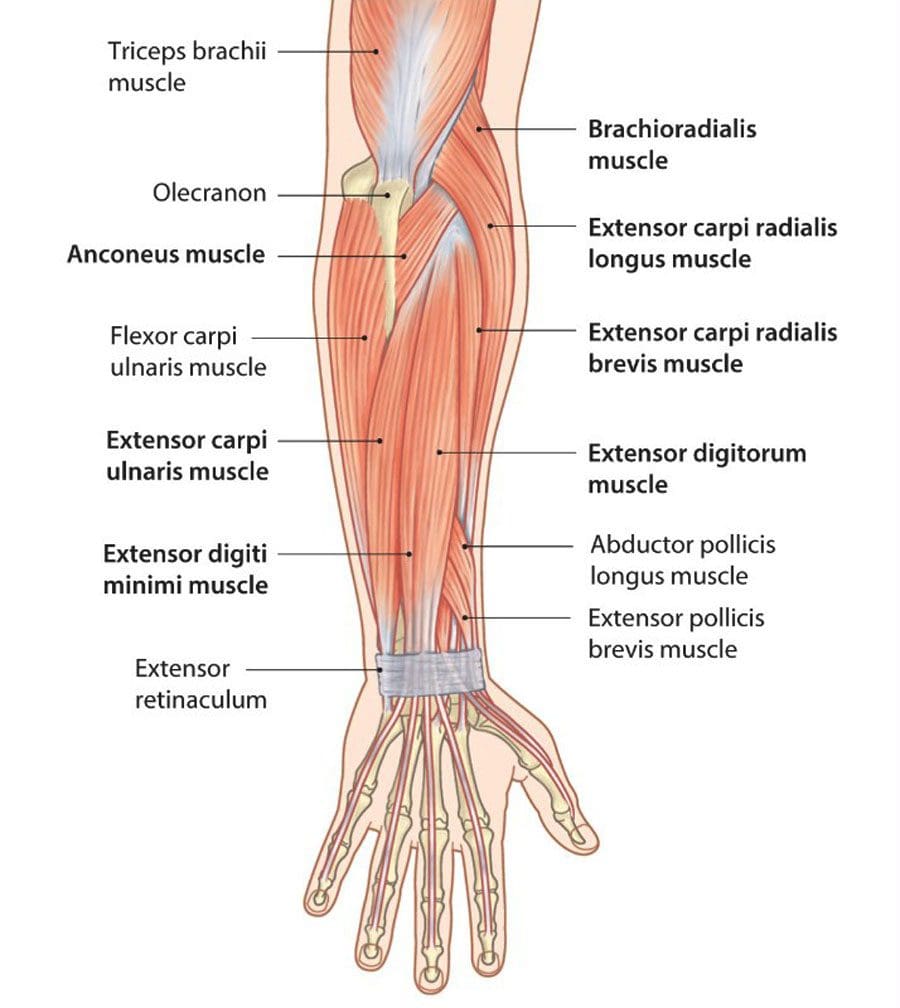
Anatomy
The forearm comprises the radius and ulna, which extend the forearm’s length and cross at the wrist.
The Radius
This bone starts at the elbow and connects to the wrist on the thumb side.
Ulna
This bone begins at the elbow and connects to the wrist on the side of the little finger.
Muscles
Several muscles operate to rotate the forearm up/supination and down/pronation and flex and extend the fingers.
Causes
Forearm pain can happen to anyone and is usually related to traumatic or repetitive use injury. In other cases, pain may be associated with a benign growth, like a cyst or possibly a malignant tumor. Common causes include:
Pulled and/or strained muscles
Muscle ruptures or small tears
A direct blow, fall, or any extreme twisting, bending or jamming action.
Tendonitis from tennis or golfers elbow.
Tennis elbow is caused by inflammation or tiny tears in the forearm muscles and tendons outside the elbow.
Golfers’ elbow is on the inside of the elbow.
Carpal Tunnel Syndrome is a repetitive stress disorder that affects the nerves and tendons of the wrist and forearm.
Musculoskeletal Causes
The musculoskeletal causes involve issues in how the forearm components operate together.
Repetitive actions like lifting, gripping, and typing can compress nerves and blood vessels throughout the forearm.
Forearm problems like dislocations or sprains can also lead to chronic inflammation and pain.
Traumatic Causes
Traumatic causes include those that result in injury to components of the forearm.
Anything that causes a direct injury to the forearm, including an automobile crash or accident, fall, or a direct hit, can fracture bones in the forearm.
A sprain can twist or stretch a ligament or tendon.
Activities that cause bending, twisting, quick sudden movement or direct impact can result in sprained multiple ligaments in the forearm.
Chiropractic Treatment
Healing forearm pain depends on the type of injury, location, and cause of the pain. Chiropractic addresses arm pain, tingling, and numbness in ways often overlooked by general physicians.
A chiropractor will perform a physical examination to determine if there are any underlying causes.
They may apply an ice pack to help control inflammation before the massage.
The chiropractor will perform gentle adjustments to the wrist, arm, and shoulder.
They may recommend a forearm brace to help retrain positioning and movement.
They will recommend exercises and stretches to strengthen and maintain the adjustments.
Carpal Tunnel Pain Treatment
References
Ellenbecker, Todd S et al. “Current concepts in examination and treatment of elbow tendon injury.” Sports health vol. 5,2 (2013): 186-94. doi:10.1177/1941738112464761
Shamsoddini, Alireza, and Mohammad Taghi Hollisaz. “Effects of taping on pain, grip strength and wrist extension force in patients with tennis elbow.” Trauma monthly vol. 18,2 (2013): 71-4. doi:10.5812/traumamon.12450
Suito, Motomu, et al. “Intertendinous epidermoid cyst of the forearm.” Case reports in plastic surgery & hand surgery vol. 6,1 25-28. 28 Jan. 2019, doi:10.1080/23320885.2018.1564314
Bicycling at any level is excellent healthwise, but the specific physical repetitive motions and postures can wear on a cyclist’s body, causing strains and injury to the:
Muscles
Ligaments
Tendons
Nerves
Spine
Injuries can be caused by falls, overused muscles, joints, posture, and/or balance problems, whether riding a bicycle for fun, health, or sport. Chiropractic decompression can treat cycling-related injuries and help prevent common injuries by helping cyclists with conditioning and exercises. Chiropractic adjustments, combined with health coaching and nutrition planning, can maximize the body’s overall athletic ability and increase/improve:
Many cyclists suffer from back pain overuse injuries that are caused by:
Incorrect saddle/seat height or an uneven seat/saddle
Not bending the knee at the end of a pedal stroke forces the cyclist to rock the pelvis side to side to generate enough power, placing added stress on the low back muscles.
Handlebars that are too far forward can cause over-stretching of the spine.
Constantly tilting the head can cause neck and shoulder pain.
Staying in the same position for an extended period strains the spine.
Repetitive hip flexion causes the muscles to become tight and perform less efficiently, straining the rest of the body to make up for the lost support.
Hamstrings that become tight can shorten in length, causing the body to pull on the pelvis and the spine.
Lack of core strength allows more stress to penetrate the glutes, back, and hips.
Riding on bumpy or rough terrain increases body jarring and spinal compression.
Chiropractic Decompression
Chiropractic decompression for cyclists can rehabilitate the body from injuries, alleviate pain, improve blood and nerve circulation and maintain the body’s flexibility. Advanced decompression techniques personalized to the individual realign and release the body from obstructions and toxins in the neural pathways. Nutritional and supplementation recommendations are incorporated to enhance the body’s natural healing abilities, and exercise/stretches to sustain the adjustments.
Spinal Decompress
References
Schultz, Samantha J, and Susan J Gordon. “Recreational cyclists: The relationship between low back pain and training characteristics.” International journal of exercise science vol. 3,3 79-85. 15 Jul. 2010
Silberman, Marc R. “Bicycling injuries.” Current sports medicine reports vol. 12,5 (2013): 337-45. doi:10.1249/JSR.0b013e3182a4bab7
Streisfeld, Gabriel M et al. “Relationship Between Body Positioning, Muscle Activity, and Spinal Kinematics in Cyclists With and Without Low Back Pain: A Systematic Review.” Sports health vol. 9,1 (2017): 75-79. doi:10.1177/1941738116676260
Thompson, M J, and F P Rivara. “Bicycle-related injuries.” American family physician vol. 63,10 (2001): 2007-14.
Many complex spinal surgeries take place in a hospital environment. The individual spends a night or two in the hospital, so medical staff can monitor them if any complications arise. However, outpatient surgeries have increased with new developments in minimally invasive procedures, pain management, and home rehabilitation. The improvements compared to traditional spinal surgical procedures are significant. These advancements have made it possible to perform more complex surgeries outside of a hospital. Outpatient surgeries have:
Accelerated recovery times
Decreased complications
Decreased infections
Healthier overall outcomes
Outpatient Surgery Candidates
Determining if outpatient surgery can be performed effectively depends on the injury/s and/or conditions that the individual is going through. An individual who is debilitated or has underlying medical conditions that increase their risk for complications or do not have support at home to assist with recovery and rehabilitation is recommended to have the surgery done in a hospital. To be considered for outpatient spine surgery, a surgeon looks at:
Standalone ambulatory surgery centers offer same-day surgical procedures for individuals that meet specific criteria. Medical staff assess the patient’s condition and determine recovery at home. If issues arise, the individual can be transferred to a hospital. Some facilities are single-specialty facilities, focusing on one medical specialty, and others are multi-specialty, meaning they offer a range of medical services from:
Orthopedic
Podiatry
Pain management services
Procedures
Anterior Cervical Discectomy and Fusion – ACDF
ACDF is a two-part surgery. First, the surgeon removes part of an intervertebral disc with bulged and compressed nerves from the spinal cord. Because there is less cushion, the vertebrae above and below are fused to prevent and eliminate painful movement. The discectomy:
Provides more accessible access to the vertebrae
Reduces healing time
Causes less pain
ACDF outpatient procedure treats several neck conditions that include:
Cervical spinal stenosis
Cervical radiculopathy
Neck-related degenerative disc disease
Herniated disc
Cervical spinal fracture
Individuals recover in the surgical center for one to several hours following the surgery before returning home. Traditional ACDF procedure takes three weeks to three months to recover.
Lumbar Discectomy
A lumbar discectomy is a minimally invasiveprocedure that repairs a lower back herniated disc compressing the surrounding nerves. This procedure provides compression relief and allows the nerve to heal. A traditional lumbar discectomy takes four to six weeks to recover.
Lumbar Laminectomy
This minimally invasive procedure removes thickened ligaments and lamina from the lower back. This opens the spinal canal space, relieving pressure and bringing pain relief. The surgery commonly treats lower-back spinal stenosis. A traditional laminectomy takes four to six weeks to recover.
Lumbar Spinal Fusion
Outpatient lumbar spinal fusion permanently connects two or more vertebrae in the lower back. The surgery helps stabilize the spine from severe arthritis or herniated disc removal. Spinal fusion has been found to be effective for correcting certain spinal deformities. The surgery involves a short recovery time at the outpatient center, after which the individual can return home the same day. A traditional or open spinal fusion requires a two-to-three-day hospital stay. After four to six weeks and with a doctor’s clearance, individuals can return to light activities, with full recovery requiring six months.
Chiropractic Spinal Decompression
References
International Journal of Spine Surgery. (April 16, 2021) “The expanding frontier of outpatient spine surgery.” https://pubmed.ncbi.nlm.nih.gov/33900984/
Mayo Clinic. (n.d.) “Spinal fusion.” https://www.mayoclinic.org/tests-procedures/spinal-fusion/about/pac-20384523
Neurosurgeons of New Jersey. (July 21, 2019) “Lumbar discectomy recovery timeline: Your guide to recovery.” https://www.neurosurgeonsofnewjersey.com/blog/lumbar-discectomy-recovery-time/#:~:text=The%20overall%20lumbar%20discectomy%20recovery,discectomy%20recovery%20time%20should%20progress
Rothman Orthopaedics. (March 2, 2017) “Outpatient spine surgery: A new way to look at surgery.” https://rothmanortho.com/stories/blog/outpatient-spine-surgery
Injury Medical Spinal Decompression: Spinal decompression therapy/treatment can be surgical or non-surgical, with differences in the procedure, recovery time, and results. Individuals who experience compression-related problems can have severe and prolonged spinal conditions that can lead to various health issues. Individuals experiencing persistent or chronic neck, back, or leg pain should know the differences between surgical and non-surgical spinal decompression. Spinal decompression aims to relieve pressure on the discs and reduce stress on the nervesto eliminate the pain associated with compression on the spine,restoring optimal circulation and improving spinal function.
Surgical Procedure
It is invasive, must be performed by a surgeon, and can have a recovery time of up to 6 weeks.
Surgery is usually suggested as a last resort after alternative therapies have not succeeded or when the compression is so severe that surgery is the only option.
Surgical spinal decompression is directed towards removal to reduce pressure instead of adjusting or stretching the discs.
In cases of severe nerve compression, surgery can be an effective option.
Risks include infection, damage to the spinal cord, and blood clots.
Types of Spinal Decompression Surgery
Types of surgeries; spinal fusion could be necessary to stabilize the spine. Common types of back surgery:
Discectomy
This procedure removes a portion of the disc to relieve pressure on nerves.
Laminotomy
The procedureremoves a small portion of the bone or a section of the bony arch to increase the size of the spinal canal and relieve pressure.
Laminectomy
The procedureremoves theentire bony arch or lamina to increase the size of the spinal canal and relieve pressure.
Foraminotomy
This procedure removes bone and other tissue to widen the openings for the nerve roots to pass through.
The procedure removes a vertebral body along with discs.
Injury Medical Spinal Decompression
Surgery for a damaged/injured spine is not always necessary. Treatment regimes vary depending on each individual’s medical condition. Non-surgical motorized spinal decompression is a non-invasive back treatment that uses a mechanized decompression table to slowly and gently stretch the spine. The therapy gradually relieves the pressure on the compressed nerve root/s resulting in reduced or complete alleviation of pain.
Oxygen, water, and nutrients circulate abundantly, promoting healing as the discs re-hydrate, and are re-nourished, improving and enhancing spine function. Individuals can enjoy increased levels of mobility, strength in the spine and muscles, and more flexibility.
Descompresión Espinal Con La DRX9000
References
American Spinal Decompression Association: “Spinal Decompression Therapy.”
Daniel, D.M. Chiropractic and Osteopathy, 2007.
Macario, Alex, and Joseph V Pergolizzi. “Systematic literature review of spinal decompression via motorized traction for chronic discogenic low back pain.” Pain practice: the official journal of World Institute of Pain vol. 6,3 (2006): 171-8. doi:10.1111/j.1533-2500.2006.00082.x
O’Hara K, editor. Decompression: a treatment for back pain. Vol. 11. National Association of Healthcare Professionals; 2004. pp. 1-2.http://www.naohp.com/menu/publications/mccu/bibliography.htm#10 [Google Scholar]
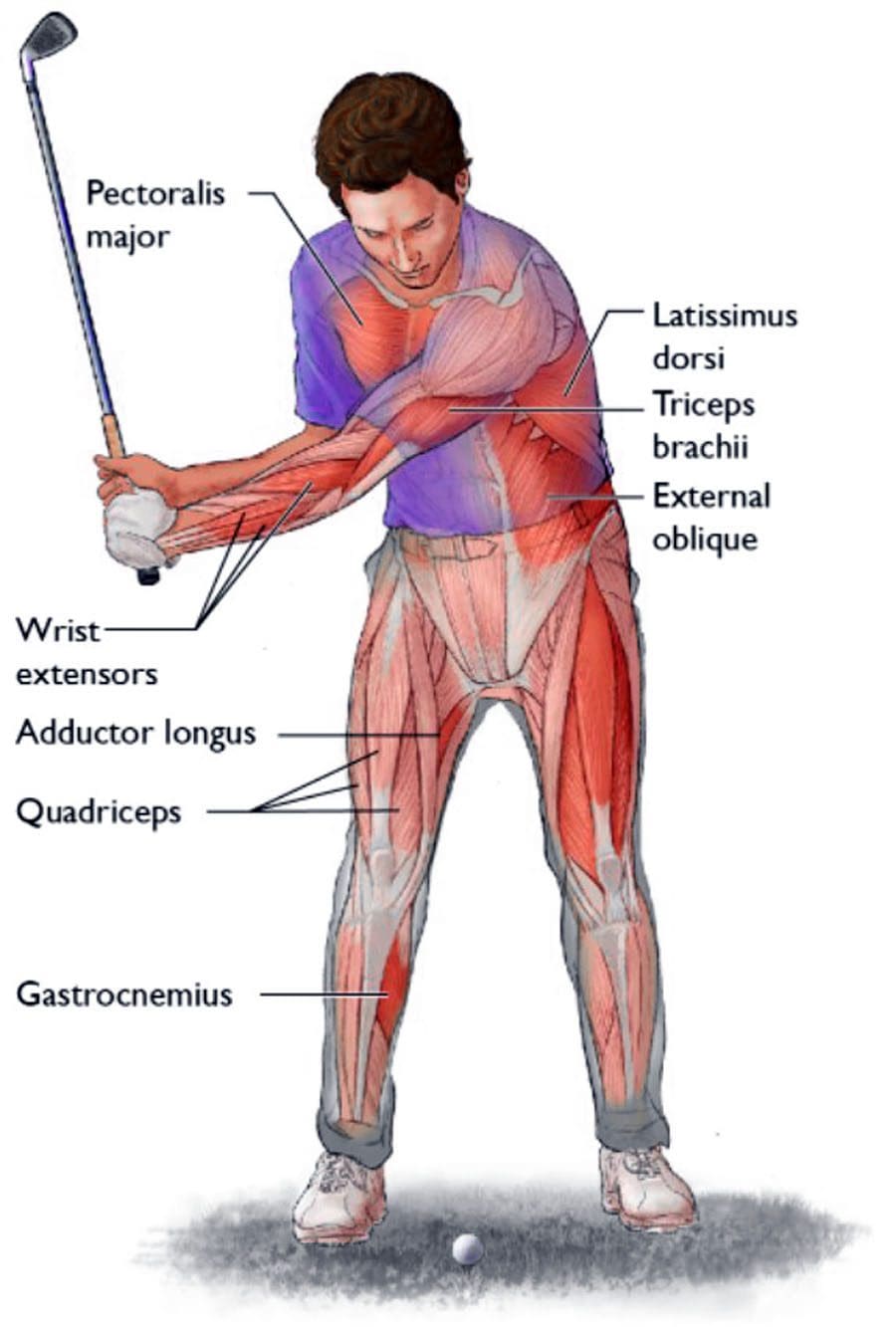
Golfing Back Injuries: Golf is an enjoyable game that can be played at all ages. It involves the foundation of the body’s range of motion, the spine. Because of the repetitive nature of a golfer’s unique swing, the repetitive rotating/twisting of the spine slowly degrades the integrity of the spinal discs causing them to bulge, herniate, or rupture. The slightest shift causing misalignment can leave the spine vulnerable to further injury. Non-surgical motorized decompression combined with chiropractic musculoskeletal adjustments can restore and maintain optimal health.
Golfing Back Injuries
Golfing involves muscle memory. Going through the walk, bending to tee the ball, recoiling for the swing, swinging and following through, walking to the hole, and bending down to retrieve the ball are all repetitive motions that can lead to:
Soreness
Inflammation
Back, hip, leg, and foot pain.
Strains
Other injuries to the muscles and discs.
The bending and twisting are the least tolerated motions by the spine. More than half of injuries sustained involve the back and/or neck. Having the spine correctly aligned is vital to retaining accuracy, power, and injury prevention. Common injuries include:
Sacroiliac Joint/SI Joint Dysfunction
The sacroiliac joint is located between the spine and the hip. Symptoms of sacroiliac joint pain include:
Low back pain.
Hip pain
Pain in the buttocks.
Pain radiating down the legs.
Groin pain
Pelvis pain
Burning sensation in the pelvis.
Numbness and weakness in the pelvis and legs.
SI Joint Pain Causes
The sacroiliac joint requires supported stability when transferring a load from the torso to the legs, specifically during the swing.
If there is compression, misalignment, or weakness, the motion will begin to wear away this stability and leave the sacroiliac joint open to further injury.
Sacroiliac joint injuries often occur from minor multi-incidents and not one major trauma.
With time the SI joint becomes misaligned, exposing the cartilage between joints, causing inflammation known as Sacroiliitis.
Facet Joint Syndrome
The facet joints are located between two vertebrae, allowing the ability to bend and twist.
Healthy facet joints have cartilage all around them, allowing the vertebrae to move smoothly in all directions.
Facet joint syndrome causes pain between the vertebrae.
Facet Joint Syndrome Causes
The leading cause of facet joint syndrome is excessive and repetitive swing movement.
Misalignment can expose and irritate the joints, causing pain, swelling, and inflammation.
Multi-micro-traumas and not one major trauma are often the cause of injury/s.
Muscle spasms are common.
Symptoms
Highly reduced range of motion
Muscle pain
Numbness
Weakness
Cervical Facet Syndrome affects the neck, shoulders, arms, and hands.
Lumbar Facet Syndrome affects the buttocks, legs, and feet.
The treatment is computer-controlled to provide gentle and painless decompression.
The therapist enters the program cycle.
The decompression table goes through brief moments of pulling and relaxing.
The spine’s bones are stretched slowly and methodically.
As the vertebrae are separated, a vacuum is formed, pulling the gel-cushion center of the disc back inside, removing the pressure on the spinal nerves and alleviating pain and disability.
The vacuum also draws oxygen and nutrients into the injured and degenerated discs to optimize healing.
DRX 9000
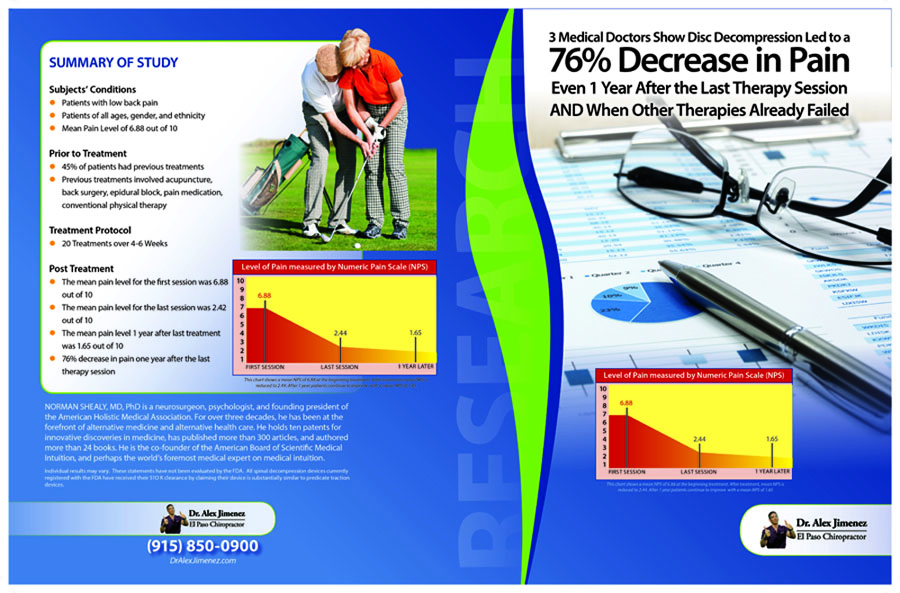
Long Term Success
References
Cole, Michael H, and Paul N Grimshaw. “The Biomechanics of the Modern Golf Swing: Implications for Lower Back Injuries.” Sports medicine (Auckland, N.Z.) vol. 46,3 (2016): 339-51. doi:10.1007/s40279-015-0429-1
Dydyk, Alexander M., et al. “Sacroiliac Joint Injury.” StatPearls, StatPearls Publishing, 4 August 2021.
Hosea, T M, and C J Gatt Jr. “Back pain in golf.” Clinics in sports medicine vol. 15,1 (1996): 37-53.
Lindsay, David M, and Anthony A Vandervoort. “Golf-related low back pain: a review of causative factors and prevention strategies.” Asian journal of sports medicine vol. 5,4 (2014): e24289. doi:10.5812/asjsm.24289
Smith, Jo Armour, et al. “Risk Factors Associated With Low Back Pain in Golfers: A Systematic Review and Meta-analysis.” Sports health vol. 10,6 (2018): 538-546. doi:10.1177/1941738118795425
Individuals drive to jobs, to school, run errands, take road trips, spending a lot of time on the road. Accidents and crashes happen more frequently with all kinds of injuries. The National Highway Traffic Safety Commission has found that 37% of car accidents and crashes involve leg injuries and damage. Chiropractic physical rehabilitation and functional medicine can help heal injuries getting the individual back to everyday life.
Bruising and cuts are typical from the impact and the body getting slammed around. Lacerations can be noticed right away, but bruising comes from blood pooling underneath the skin and can take time to present, possibly 24 to 48 hours. Most bruises and cuts heal independently from home first aid care. A standard recovery used to take care of bruising is R.I.C.E or rest, ice, compression, and elevation. This helps the healing process; however, if the injury/s are more severe, chiropractic can help with therapeutic massage to relieve pain and strengthen the injured muscles, tendons, and ligaments.
ACL Injuries
The femur or thigh bone has several bands of tissue connecting it to the patella or kneecap and tibia or shin bone. One of the bands is the anterior cruciate ligament or ACL. Injuries to this band of tissue are common in sports. Car accidents and crashes are another common cause, specifically tearing the ligament. Individuals experiencing a tear may notice some or all of the following symptoms:
A cracking or popping sound when the accident or crash took place.
Swelling in and around the knee.
Severe pain in and around the knee.
Unstable and unsteady when walking or standing.
Reduced range of motion that makes walking or moving difficult.
A chiropractor can help treat the injury and help correct any muscular imbalances.
Meniscus Tears
Tears to the meniscus are also common in car accidents and crashes. The meniscusis a part of the knee. Two wedge-shaped pieces of cartilage provide a cushion where the femur and tibia meet to absorb shock. The wedges are called menisci.
When the meniscus tears, individuals might feel or hear a pop and could feel the leg suddenly give out.
Swelling in the knee.
Some pain but still be able to walk.
The knee will be stiff for the next few days.
More difficulty bearing weight or walking.
The RICE method is a recommended method of self-care. Many meniscus tears do not require surgery to improve knee function. Mild to moderate meniscus tears can be successfully treated with chiropractic techniques like soft tissue work, corrective stretches, and exercises. Surgery could eventually be necessary for severe cases to repair the meniscus to prevent long-term complications.
Chiropractic care can help the body heal and recover from a bone fracture. A patient’s bone density is evaluated and tested with an individualized treatment plan to help regain and maintain optimal bone strength. The treatments strengthen the muscles, reduce stiffness, improve nutrition, and relieve pain. Manipulation adjustments, rehabilitation, relaxation techniques, and dietary health coaching help individuals heal faster and strengthen their bones. The objective is to help regain increased mobility and range of motion.
Sciatica
Car accidents and crashes are one instance where the spine can be damaged enough to bring on sciatic pain where no back problems were present before. The impact from a car accident can cause the discs to be knocked out of place, damaged, and/or rupture around the surrounding tissue. Any of these results can pinch the sciatic nerve, leading to pain and other sciatica symptoms. Chiropractic can realign the spine and relieve pressure from the nerve/s.
DOC Spinal Decompression Table
References
Atkinson, T, and P Atkinson. “Knee injuries in motor vehicle collisions: a study of the National Accident Sampling System database for the years 1979-1995.” Accident; analysis and prevention vol. 32,6 (2000): 779-86. doi:10.1016/s0001-4575(99)00131-1
Foulk, David M, and Brian H Mullis. “Hip dislocation: evaluation and management.” The Journal of the American Academy of Orthopaedic Surgeons vol. 18,4 (2010): 199-209. doi:10.5435/00124635-201004000-00003
Wilson, L S Jr et al. “Foot and ankle injuries in motor vehicle accidents.” Foot & ankle international vol. 22,8 (2001): 649-52. doi:10.1177/107110070102200806
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine