Spinal injections are exactly what the name says. They are administered direct injections of medicine/s in a specific location of the spine. These are used to treat various conditions affecting the spine when non-invasive treatment/s are not working.
This could be an area along the upper cervical/neck spine all the way down to the sacrum. Injections are also utilized in helping to diagnose neck or back pain that radiates or spreads into an individual�s arms and legs. These are known as:
Cervical radiculopathy
Lumbar radiculopathy
Spinal injection/s for diagnostic or treatment purposes could be a part of an overall treatment plan along with chiropractic/physical therapy and possible medication.
�
�
The medicine in the injection
The medicine could be comprised of a local anesthetic on its own, steroid on its own, or a combination of the two. Steroids are short for corticosteroid, which is a strong anti-inflammatory medication. A contrast dye like an x-ray dye could be added to the injection mix. This dye acts as a guide for precise placement of the needle using image guidance.
�
Spinal disorders that could benefit
Proceeding with an injection treatment plan is based on an individual’s unique factors that apply to their condition/state. This decision will be made after consultation, and diagnosis with your doctor, spine specialist, or chiropractor.
Healthcare providers recommend conservative treatment first. A treatment plan typically runs around 4-6 weeks. If there is no change or improvement in the individual’s condition from the conservative therapy then injection treatment/s could be recommended. Conditions, where injection/s are used, include:
Disc herniation
Facet joint pain
Failed back syndrome
Sacroiliac joint pain
Sciatica
Spinal stenosis
�
Spinal injection and nerve block difference
Spinal injections are a general term that could mean any type of injection involving the spine. Nerve blocks are a precise type of injection that targets a specific nerve. As the medicine is injected into the target nerve/s, it blocks or creates a blockade of the pain signals being sent from the area (ex. neck, low back, etc.) that is generating the pain.
�
Injection types
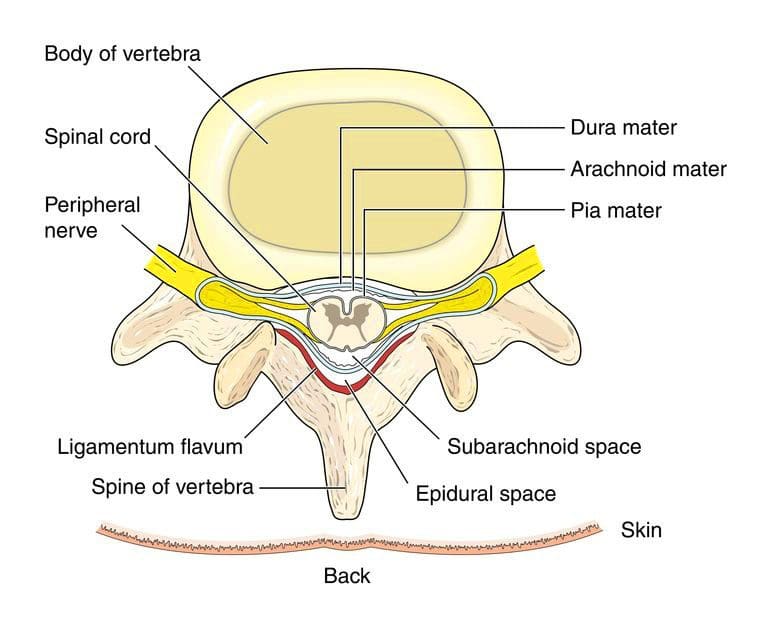
Epidural
An epidural means an injection on the dura. The dura is the outermost layer that encloses the spinal cord. �
�
3 types of epidurals. They are named according to the direction and angle the needle takes to get to the dura.
Caudal epidural:
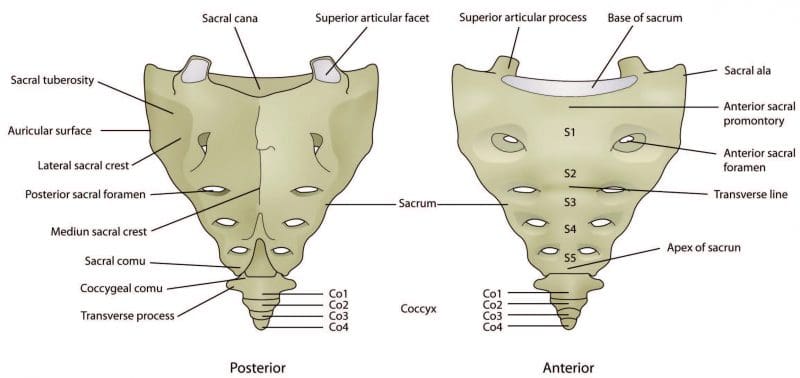
The spinal canal ends at an opening at the end of the sacrum called the spinal hiatus. The medicine is injected into the epidural space through the sacral hiatus. This is the method that is used to provide anesthesia to pregnant women when they’re in labor. �
�
Transforaminal epidural:
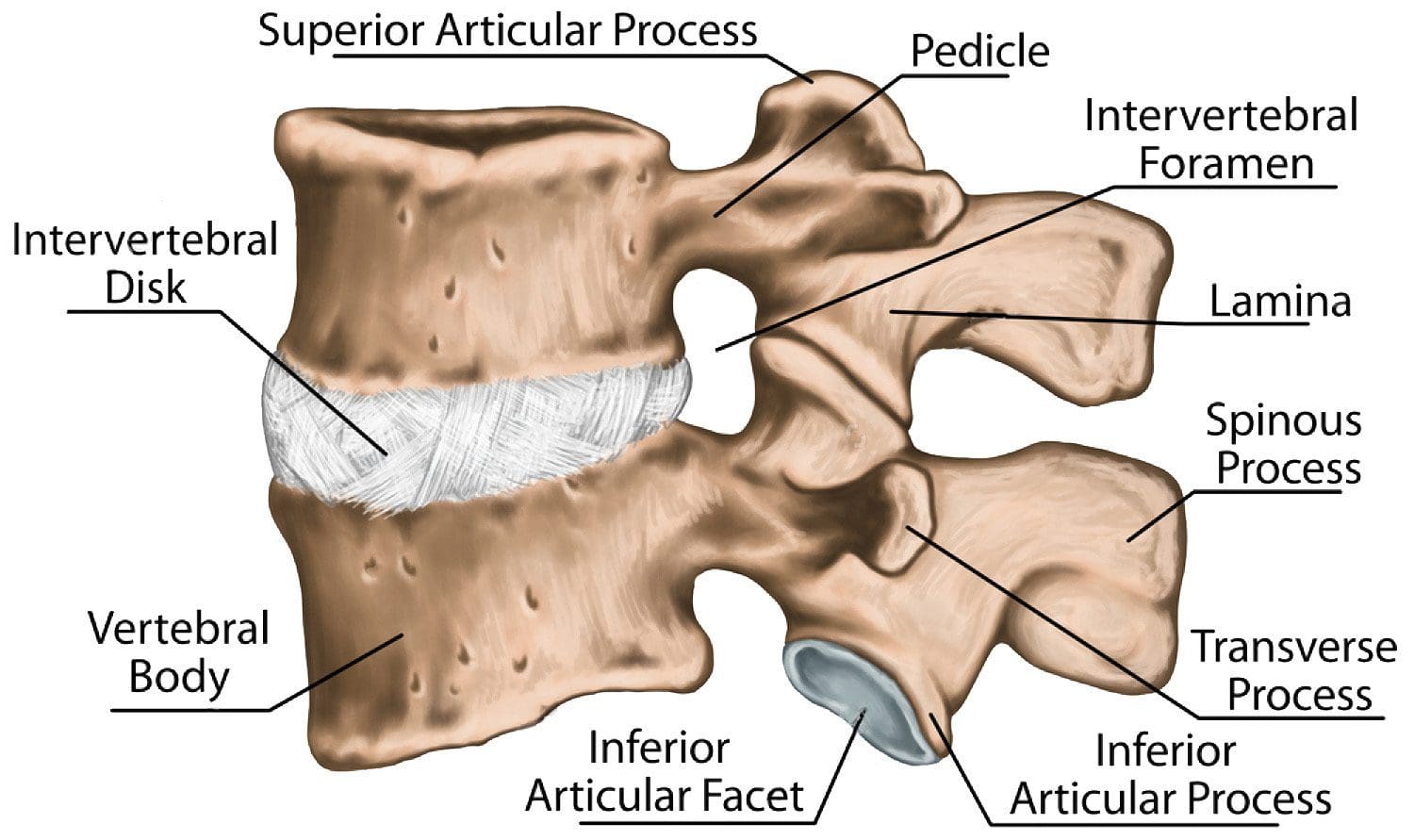
There are nerve roots that come out of the spinal canal at each level through a bony opening called the intervertebral foramen or neuroforamen. The medicine is injected into the epidural space in these areas.
Interlaminar epidural:
The lamina is a section that forms the arch of each level and forms the spinal canal. The lamina at each level lays on top of the lamina right below. The needle is inserted between the lamina for delivery of the medicine into the epidural space. �
�
Selective Nerve Root Block – SNRB
These involve the injection of a local anesthetic onto a targeted nerve. They are typically used for diagnostic purposes. For individuals with multi-spinal compression/s, these combined with:
Medical history
Physical exam
MRI
These can help identify the pain generator such as spinal stenosis.
�
Medial Branch Block – MBB
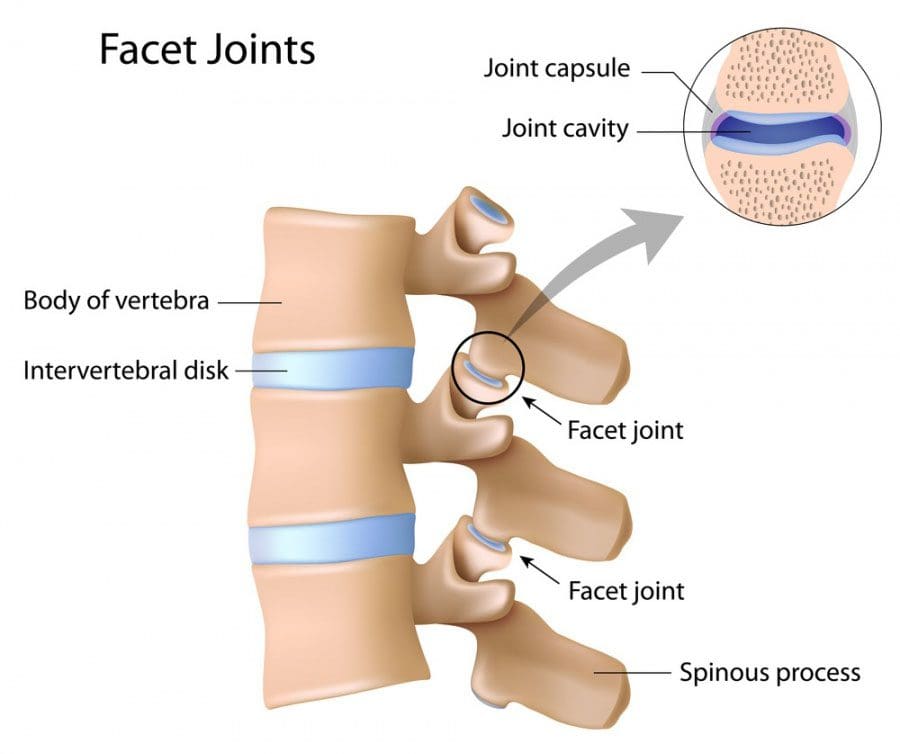
The facet joints are bony projections that connect a vertebral level to the levels above and below. These can become arthritic and is responsible for different forms of back pain.
This type of spinal injection is local anesthetic injected on the medial branch nerves. These are the nerves that send pain signals from the facet joint/s. They are useful in determining if the facet joint is the pain generator. �
�
Facet Joint
These are injections directly into the facet joint itself. Much like injecting anti-inflammatory and pain meds into a knee with arthritis.
�
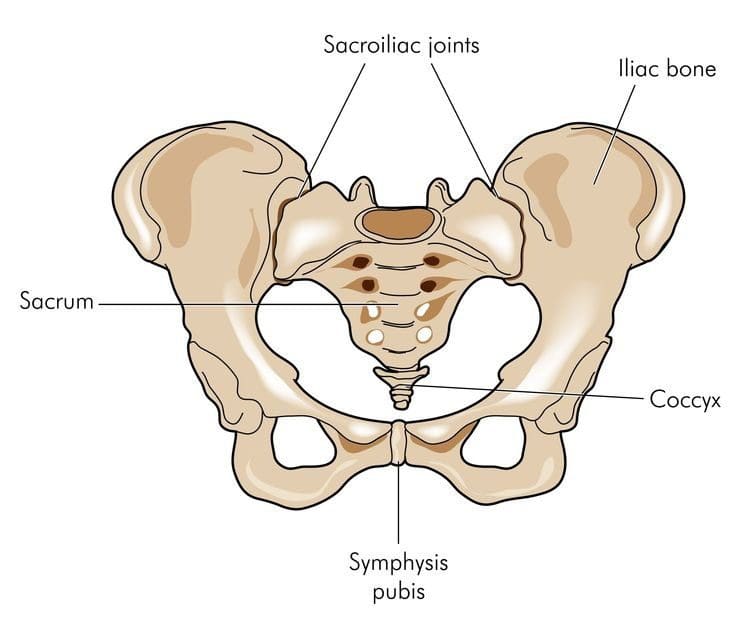
Sacroiliac Joint
The two sacroiliac joints help connect either side of the sacrum to the hip joint. Like other joints, these can get inflamed and cause painful symptoms. This is an injection directly into one or both of the sacroiliac joints.
�
Administration of the spinal injection or nerve block
Injections are only to be performed by doctors trained specifically in spinal injections. Injections are usually performed by an:
Anesthesiologist
Neurologist
Neurosurgeon
Orthopedic surgeon
Physiatrist
Radiologist
�
Role of these procedures
Reasons why an injection could be used:
Help as a diagnostic to identify the pain generator
Therapeutically to provide pain relief
As a prognostic pain predictor of the relief, an individual could expect from a more invasive procedure like nerve ablation.
�
How often
A maximum of 6 injections for one year is the recommended treatment protocol. Each injection should be based on the effect/s of the previous injection.
�
Potential benefits
The main benefit is to bring pain relief and the ability to function.
Major complications happen in less than one percent of those undergoing the treatment. Individuals with diabetes could see a temporary elevation of their blood sugar.
�
Lasting effects
How long the medicine lasts is different for everyone and comes with variables like:
Type of injection
Type of pathology
Diagnosis
Cause
How long the symptoms last
Most can expect to have one and a half to three months of relief. However, with some, they may only provide minimal relief, while others may see improvements for up to a year.
�
Treating Severe & Complex Sciatica Syndromes
�
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Steroid injections into the cervical spine can help with�radiating�neck pain. Neck pain affects people all over the world. Although it is not as common as back pain, neck pain can really take a toll on a person�s quality of life and ability to work.� This comes in the form of:
Sleep problems
Radiating/Spreading pain
Mental health issues and more
Much like back pain neck pain can be hard to treat effectively without identifying the root cause known as the pain generator. If natural treatments like chiropractic aren’t working then injections could be the next phase.
Injections can help with:
Identifying the source/root cause of the pain as a diagnostic
Treats the pain as a therapeutic
The most commonly used are cervical epidural steroid injections,medial branch blocks (MBBs), and facet joint injections. Learn about what they are, what they treat, and the scientific research behind their risks and benefits.
Cervical Epidural Steroid
The phrase cervical epidural steroid injection:
Injection means that medicine is delivered through a needle.
Cervical means the cervical spine, which is the neck.
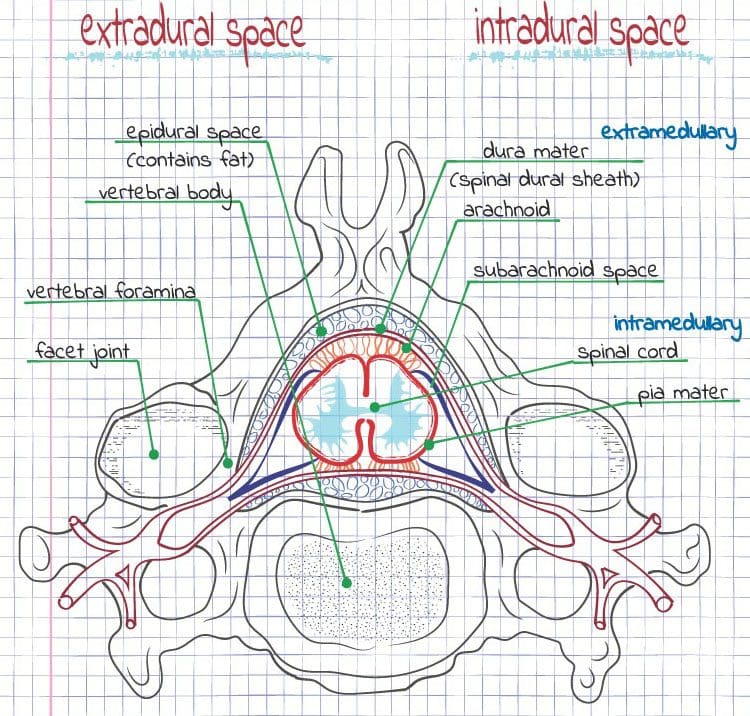
Epidural means the dura or outer layer of the soft tissue that encases the spinal cord, nerve roots, and cerebrospinal fluid. Epidural means the medicine goes into the space around the dura.
Spine specialists use image guidance with a contrast dye called fluoroscopy ensuring the medicine gets delivered to the proper area.
2 Types
The needle enters the space through a transforaminal approach or interlaminar approach. Words like epidural just refer to where the needle goes. These injections also called nerve root blocks, are performed by entering the epidural space through the opening where the nerve roots branch out. This space is known as the intervertebral foramen.
When it is called a selective nerve root block, this is for cases where multiple nerve roots are being compressed and the injection is being used in a diagnostic purpose to identify which nerve is the pain generator. The needle in an interlaminar epidural injection goes through the opening that exists between two adjacent vertebrae.
Candidates
Cervical epidural steroid injections may be appropriate for someone who has severe neck pain with:
Numbness
Weakness
Altered sensation in the arm, shoulder, or between the shoulder blades
Cervical epidural steroid injections are reserved as a second-line treatment for individuals that have neck pain that does not stop for more than 4 weeks despite conservative treatment like physical therapy, chiropractic, or medical pain management using NSAIDs or acetaminophen.
The source of the pain is usually what determines if injections are appropriate.
With a patient�s:
Past medical and surgical history
Pain history
Physical exam findings
Imaging Results like CT computed tomography scan, MRI magnetic resonance imaging or a nerve test like an EMG�electromyography test all can help in finding the source of the pain.
If a spine specialist thinks the nerve compression was brought on by a disc herniation, spondylolisthesis or the shifting of vertebral levels, scarring, or arthritic conditions is causing the pain, then an injection may be appropriate. If the pain comes from an infection or cancer, then this treatment is unlikely to be recommended.
Potential Benefits
The effects of injections are different for everyone, because of the variables:
The Duration of symptoms
The Cause of symptoms
Any Additional treatment
More than 50% will have at least 50% improvement in their pain for around 4 weeks. Then there are individuals that experience relief, up to 6 months. There are no significant differences in outcomes between the transforaminal and interlaminar approaches.
Overall alleviation from the pain is enhanced/improved when the injections are combined with a full-on treatment plan that includes physical therapy/chiropractic and pain medications.
Possible Risks
Common complications associated with injections are usually minor and temporary. These are:
Headache/s
Facial flushes
Light Headedness
Rash
Pain increase
Extended Numbness
Major complications are rare, but they can happen. These include�infection, paralysis, stroke, and death. However, this happens in less than 1% of individuals undergoing this treatment. These complications are thought to happen from direct spinal cord penetration of the needle, bleeding into the spinal canal, or the medicine inadvertently getting injected into the blood vessels. Surgical groups and facilities have strict guidelines to limit these complications.
This treatment is commonly used, and when done correctly can be a powerful tool in the treatment of persistent, severe neck pain. Everyone is different so if you are considering a cervical epidural spinal injection find a qualified spine specialist or consult with a chiropractor to find out if injections are necessary.
Many Americans in the United States will visit a healthcare professional’s office reporting some type of pain. While most cases of pain are considered acute, or temporary, resolving after the injury or condition causing the symptoms has healed, a large percentage of individuals will still report pain long after the source has disappeared. This is known as chronic pain. Fortunately, there are a variety of treatment methods which can also help ease these symptoms.
Are injections used to treat chronic pain?
From physical therapy and chiropractic care, to drugs and medications, numerous types of treatment methods and therapies can be used to treat chronic pain, each more beneficial to certain people than others. Epidural steroid injections and facet joint injections are some of the most common types of injections utilized to ease chronic pain symptoms. For some individuals, injections may be more useful than other forms of treatment. As with any medical procedure, however, it’s important to understand how helpful these can be for each, individual patient.
Epidural Corticosteroid Injections for Chronic Pain
Although epidural steroid injections (also called epidural corticosteroid injections) can be helpful to confirm a diagnosis, they should be used primarily after a specific presumptive diagnosis has been established. Additionally, injections shouldn’t be used in isolation, but rather in combination with a program strengthening, stressing muscle flexibility, and operational recovery, most commonly associated with chronic pain, in this case.
Appropriate follow-up after shots to rate ability and the individual’s treatment response to progress in the rehabilitation program is indispensable. Observation of this response is necessary prior to a second or third shot, although a number of injections can be attempted to decrease pain. Epidural steroid injections are an adjunct treatment, which facilitates participation in an active exercise program and may assist in avoiding the need for surgical intervention.
Treatment Rationale
The rationale for the use of epidural corticosteroid injection has enhanced with the signs of an inflammatory basis for radicular pain from disc herniation. Although prospective trials are lacking, epidural steroids have been proven to be effective in pain reduction in patients with referred pain. If used in the initial weeks after onset the efficacy is increased.
The goal of these injections would be to facilitate an active exercise program and also to progress sufferers through the pain and inflammation phase of healing as quickly as possible. As with all injections, it needs to be a part of a comprehensive treatment plan involving active exercise programs.
How the Injection Is Applied
To ensure proper needle placement of corticosteroids, fluoroscopic guidance is recommended. Meaning a healthcare professional will use special imaging gear during the injection to be sure the needle is going in at the right place. Some patients may require more than one injection. Repeat shots should be based on goals and the response after the injection. It is not necessary for many patients to experience a set number or “series” of injections. If minimal to no advancement is found following two shots, then further similar shots aren’t warranted. The recent usage of the approach allows the medicine to be delivered in a fashion to the ventral part of the spinal canal. All patients must be followed by consecutive injections (10-14 days later) to assess therapeutic reaction.
Utilization of Epidural Steroid Injections
Epidural shots and intradiscal injections have been used in treating non-radicular degenerative disc disorder with limited success. In addition, epidural steroids are used in patients with neurogenic claudication from spinal stenosis with mixed outcomes. A number of shots can be tried to decrease pain thought to be at least in part mediated by inflammation.
Facet Joint Injections for Chronic Pain
The therapeutic advantage of facet injections remains controversial. The controversy starts with the significance of the background and examination with lower back pain. Many patients will complain of back and lower extremity pain with standing, walking, and extension-type pursuits. The examination is normal, and also tests for nerve root inflammation are often negative. Many patients may have increased pain on passive expansion, or extension and rotation.
Additionally, radiographic and bone scanning imaging hasn’t been useful in selecting appropriate patients for facet injections. Consequently, the primary job of facet injections remains diagnostic. There is support for the impact of shots or ablations of the nerves. Facet injections should be used for patients who have failed a guided non-operative treatment program that incorporates various manipulation/mobilization methods. They should be done under fluoroscopic guidance and are not suggested in the initial four to six weeks of treatment.
Goal of Facet Joint Injections
The goal of facet injections is to verify the diagnosis and perhaps assist with pain reduction to be able to alleviate an active physical treatment program. If prior injections were helpful and there’s a recurrence of pain, they can be replicated replicate injections should be limited. This process should be used only in people failing a comprehensive application and in no manner should be considered at the initial management of an incident of acute low back pain.
Be sure to seek the proper guidance from an experienced and qualified healthcare professional before attempting any medical procedure, method or therapy. Injections for chronic pain are only one form of treatment used for the mentioned symptoms. Other treatment options can be used alongside these or in place of the above.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Corticosteroid injections are widely used to aid injury rehabilitation but we still understand very little about their mechanism. Chiropractor, Dr. Alexander Jimenez examines the current thinking and discusses how this potentially impacts treatment options…
Corticosteroids are used for their anti- inflammatory and pain reducing effects. They can also reduce muscle spasms and influence local tissue metabolism for faster healing. Injection therapy is now widely available from specially trained general practitioners, physiotherapists and consultants, and can be offered for a wide range of clinical conditions. Because of this wide availability and the growing desire for injury �quick fixes�, it is important that they are used correctly and the full consequences are understood prior to injection.
The main indications for corticosteroid injection use are(1):
Acute and chronic bursitis
Acute capsulitis (tight joint capsule)
Chronic tendinopathy
Inflammatory arthritis
Chronic ligament sprains
Steroid injections of hydrocortisone are a synthetic form of a naturally produced hormone within the body called cortisol. Cortisol is important for regulating carbohydrate, protein and fat metabolism. It is also involved in metabolic responses in times of stress such as emotional problems, trauma, and infection, where levels of inflammation are elevated. Steroid injections work on the immune system by blocking the production of chemicals that activate the inflammatory reactions, therefore reducing inflammation and pain within injury locations.
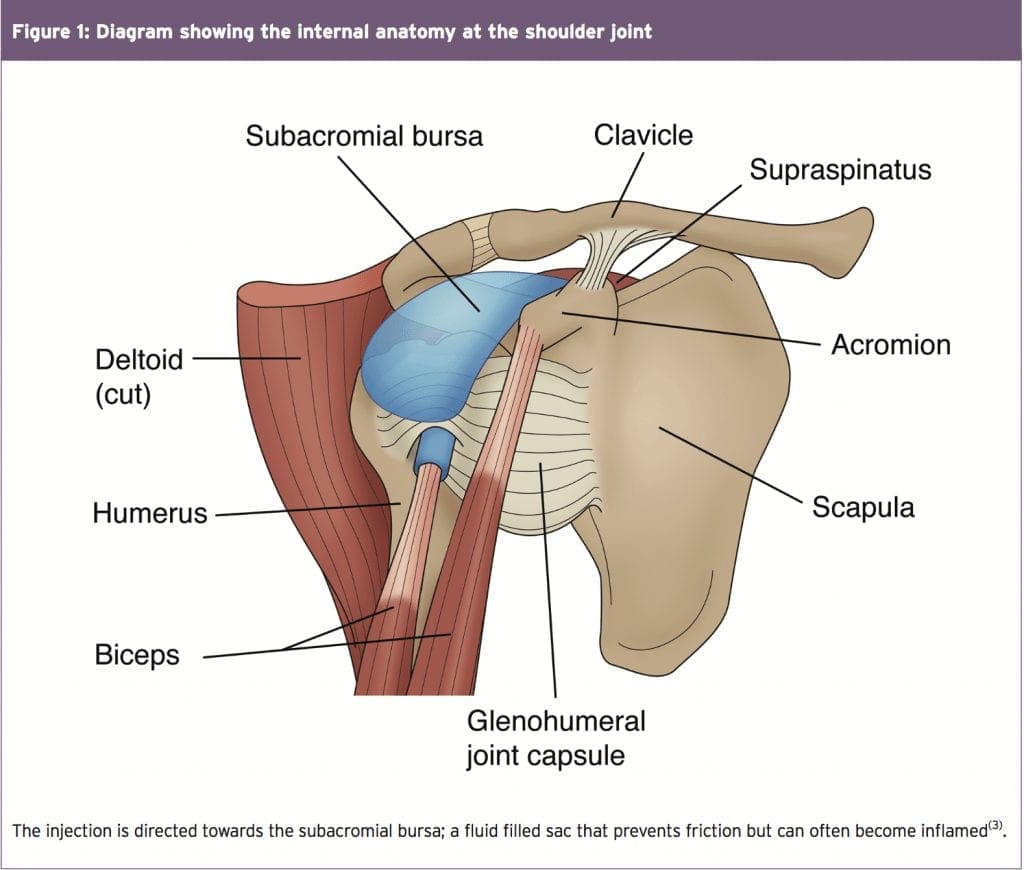
Steroid injections can be directed into a joint, muscle, tendon, bursa, or a space around these structures. Figure one shows an injection aiming for the bursa within the shoulder joint. This is often a source of irritation and causes impingement when the shoulder moves. The location will depend on what tissue is causing the symptoms. When injected locally to the specific structure, the effects are primarily only produced there and widespread detrimental effects are minimal(2).
When To Use
Identifying the correct time to issue a steroid injection following injury requires careful consideration. The mechanical status of the tissue is important because this will vary depending on the stage of healing and therefore the effectiveness of the injection will also vary.
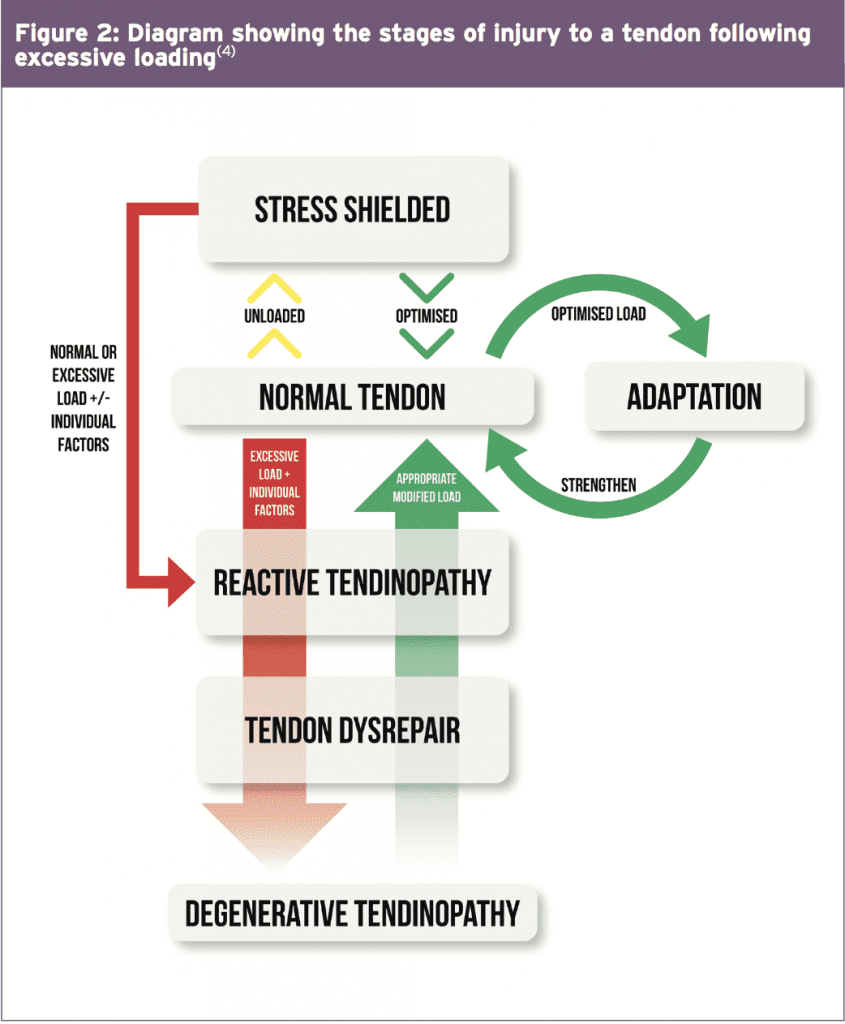
Figure 2 shows the different stages that a tendon can progress through following trauma. This is equally applicable to muscles, fascia, and other tissues too. A reactive tendinopathy (tendon degeneration/damage) will present shortly after injury/trauma/stress/ excessive loading, and will display acute swelling and inflammation. The initial care should be 2-3 weeks of rest, analgesia, ice application and gentle physiotherapy. If symptoms have not significantly improved after this period, then the introduction of a corticosteroid injection is appropriate for providing symptomatic relief by reducing inflammation and eliminating the occurrence of further damage because mechanical normality will be quickly restored(3).
If the tendon continues to be placed under excessive load, swelling and inflammation will remain or escalate, and continuous loading will eventually cause micro trauma and further tendon degeneration. If this is prolonged for long enough then the tendon will fail structurally(4).
The use of corticosteroids here is questionable because there is unlikely to be inflammation present to combat, and the injection alone will not repair this physical damage. Injection treatment at this stage may only be indicated if the athlete is in too much pain to participate in any significant rehabilitation. The symptomatic relief the injection may bring at this point could allow exercises to be performed, which can help accelerate the repair of physical damage. Ultimately, physical exercise is a key component in recovery following corticosteroid injections.
Impact On Treatment & Performance
For the best outcome, post-injection care � particularly with respect to timing � is important. Relative rest is recommended for the first two weeks post-injection. During this first two weeks the tissues are weakened and their failing strengths are reduced by up to 35%; this means the strength at which they would fail (tear) is much lower and more susceptible to rupturing(8).
By six weeks the bio-mechanical integrity is reestablished and the tissues are deemed �normal� again, with increased strength and function(8). Benefits are optimal within this 6-week period and often short-lived; therefore the athlete must comply strictly to a rehabilitation program to gradually load the tissues and ensure the correct load is applied during this period(9). Research has also shown that at twelve weeks post-injection�there is little significance in the difference between those who received a steroid injection and those who focused on exercise therapy alone, suggesting this early symptom relief should be used to enhance rehabilitation(10). If loading is accelerated in the early stages the athlete risks re-aggravation of the injury, delayed healing, further weakening and thus rupture.
If this rehabilitation protocol is followed, the athlete will likely maximise their outcome. They can return to training, and with the severity of their symptoms reduced, this can allow progression to the next stage of training. If the injury is severe enough that surgery may be considered within three months, a steroid injection should not be performed as this can affect the success of the surgery.
Evidence For Sports Injuries
Here we will consider some of the more common sports injuries and summarize what the current evidence regarding steroid injection suggests.
Shoulders
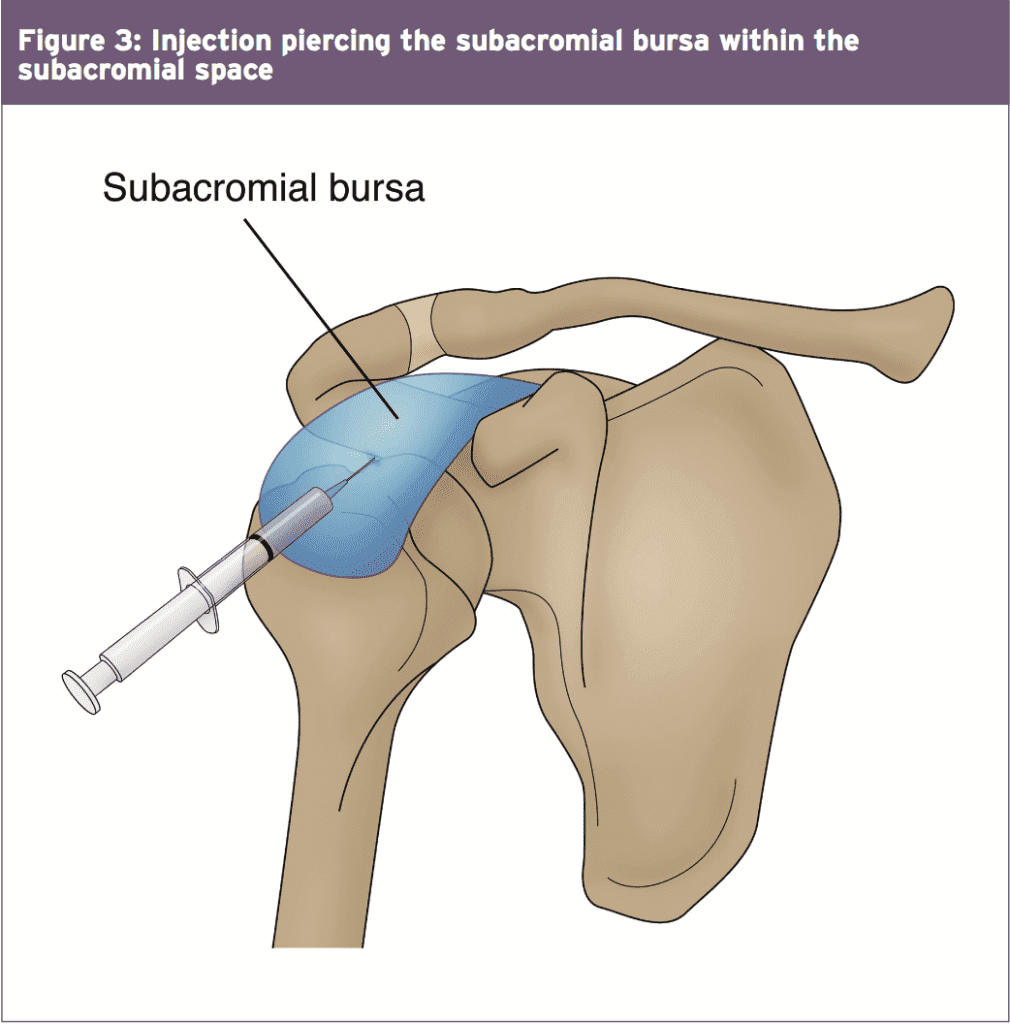
Injection therapy is indicated in subacromial impingement or bursitis (as in Figure 3 below) to allow the inflammation reduction and restoration of normal movement. It is also indicated in rotator cuff pathology where the tendons are again inflamed, but also damaged and unable to undergo exercise therapy. Shoulder injections are shown to produce early improvements in pain and function with a high level of patient satisfaction(10). Symptoms are similar to those without injection at 12 weeks however, suggesting physical therapy is also important(10). Injection is not appropriate for shoulder instability as it can make the joint more unstable. Exercise therapy alone is recommended for this condition.
Hip Pain
Two soft tissue conditions that benefit the most from injection are piriformis syndrome (muscle tightness running deep to the buttock muscles), and greater trochanter pain syndrome (affecting the bursa surrounding the hip joint, or the gluteal tendons that are all in close proximity to the lateral hip)(11). Injection success is reported to be approximately 60-100% if the diagnosis is accurate and the correct protocols are adhered to(12). Other regions such as the adductor and hamstring tendons can also be treated for tendinitis or groin pains. However, injections into these�regions are deep and painful, and require extensive rest afterwards.
Knee Pain
Knee joint injections for arthritic conditions are most commonly used, with injection to the soft tissues much less common due to the complex diagnosis, and risk of detrimental side effects. The various bursa around the knee, the iliotibial band, and quadriceps and patellar tendons have all been shown to significantly benefit in the short-term; however accurate location is essential to ensure the tendon itself is not penetrated � only the surrounding regions(13).
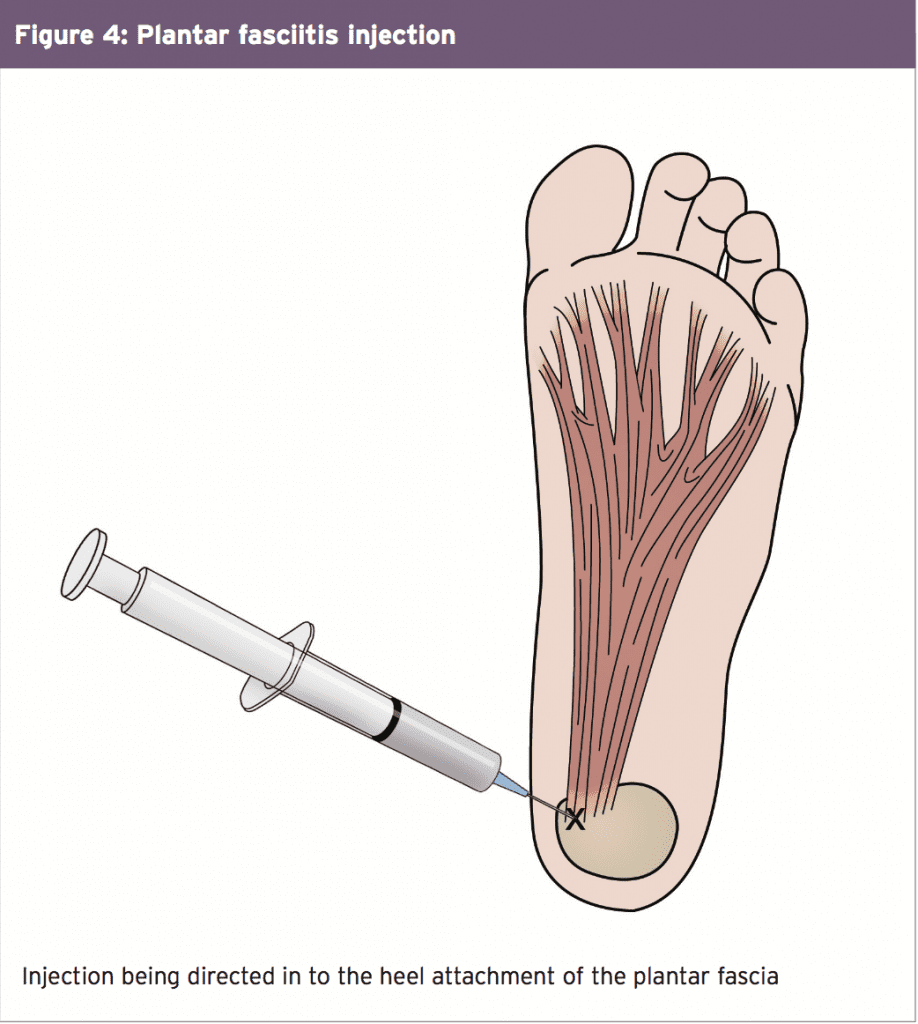
Plantar Fasciitis
This is a painful injection to receive, and pain can last for well over one week post- injection (see figure 4). There is an approximate 2-4% risk that the fascia can rupture. In addition, there�s a risk of local nerve damage and wasting of the fat pad within the heel. Studies have demonstrated that at 4 weeks post-injection pain and thickness of the injured plantar fascia are reduced and these benefits remain three months later, suggesting a good outcome if the risks are avoided(14).
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine







 Hip Pain
Hip Pain