Chiropractor, Dr. Alexander Jimenez gives insight into the relevant anatomy and functional biomechanics of the piriformis muscle, highlights the role it plays in musculoskeletal dysfunction and looks at management options in cases of muscle dysfunction.
The piriformis muscle (PM) is well-known in the fraternity of sports medicine as a significant muscle in the posterior hip. It is a muscle that has a role in controlling hip joint rotation and abduction, and it is also a muscle made famous due to its �inversion of action� in rotation. Furthermore, the PM also grabs attention due to its role in the contentious �piriformis syndrome�, a condition implicated as a potential source of pain and dysfunction, not only in the general population but in athletes as well.
Relevant Anatomy
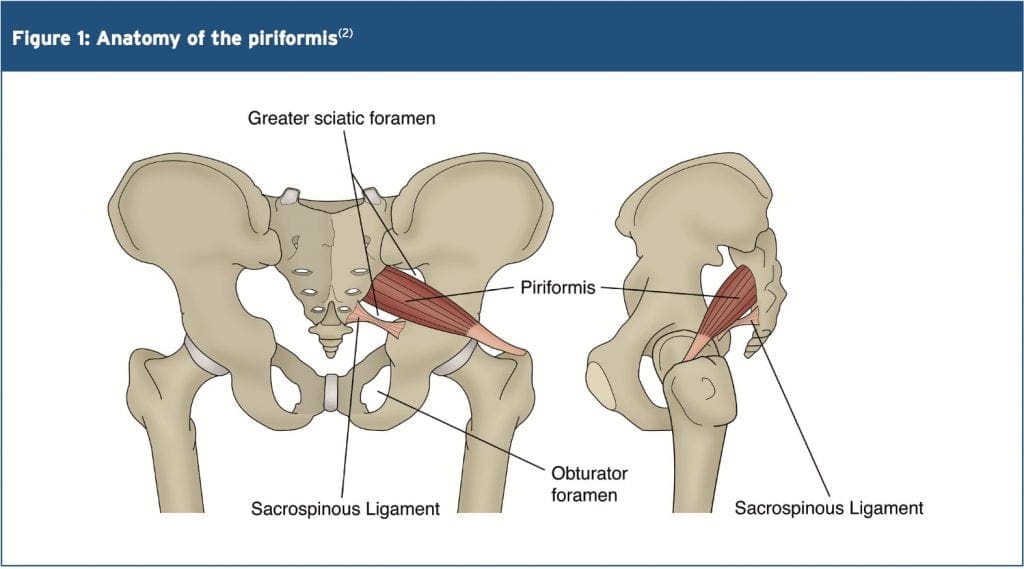
The name piriformis was first coined by Belgian Anatomist Adrian Spigelius in the early 17th century. Its name is derived from the Latin word �pirum� meaning �pear� and �forma� meaning �shape� � ie a pear shaped muscle (see Figure 1)(1).
The PM originates on the anterior surface of the sacrum and is anchored to it by three fleshy attachments between the first, second, third and fourth anterior sacral foramina(2). Occasionally its origin may be so broad that it joins the capsule of the sacroiliac joint above and with the sacrotuberous and/or sacrospinous�ligament below(3,4).
PM is a thick and bulky muscle, and as it passes out of the pelvis through the greater sciatic foramen, it divides the foramen into the suprapiriform and infra-piriform foramina(5). As it courses antero-laterally through the greater sciatic foramen, it tapers out to form a tendon that is attached to the superior-medial surface of the greater trochanter, commonly blending with the common tendon of the obturator internus and gemelli muscles(6).
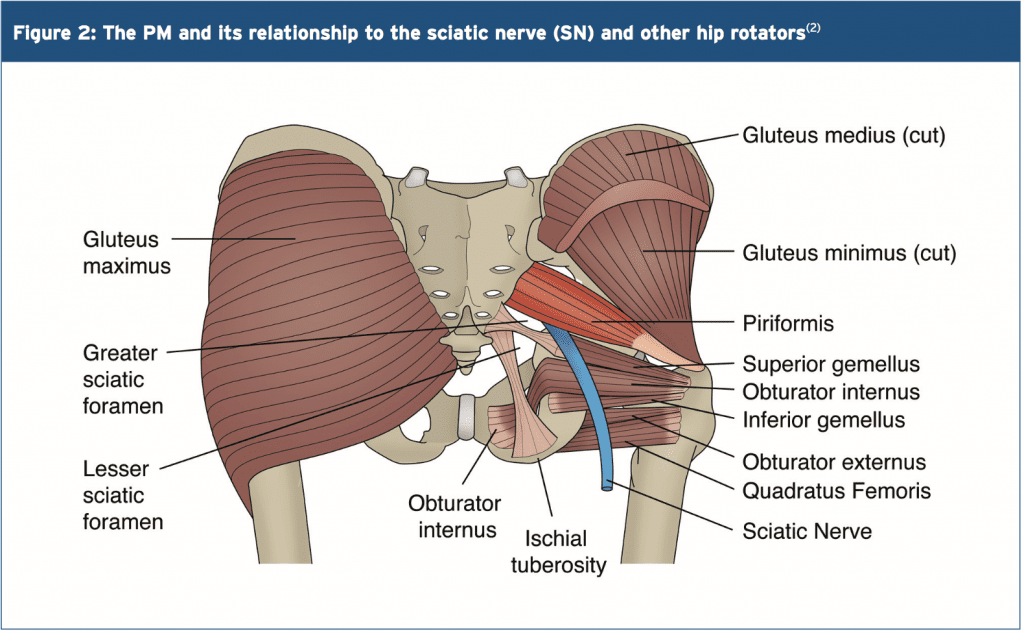
The nerves and blood vessels in the suprapiriform foramen are the superior gluteal nerve and vessels, and in the infra- piriforma fossa are the inferior gluteal nerves and vessels and the sciatic nerve (SN)(5). Due to its large volume in the greater sciatic foramen, it has the potential to compress the numerous vessels and nerves that exit the pelvis.
PM is closely associated with the other short hip rotators that lie inferior such as the superior gemellus, obturator internus, inferior gemellus and obturator externus(2). The primary difference between the PM and other short rotators is the relationship to the SN. The PM passes posterior to the�nerve whereas the other otators pass anterior (see figure 2).
Variants
A few anatomical variants have been found with the PM:
1. Additional medial attachments to the first and fifth sacral vertebrae and to the coccyx(7).
2. The tendon may fuse with the gluteus medius or minimus above, or superior gemellus below(7).
3. In less than 20% of cases it is divided into two distinct portions through which part or all of the sciatic nerve may pass(7).
4. It may blend with the posterior hip joint capsule as a conjoined tendon with the obturator internus(8).
5. The distal attachment of the PM has shown to vary in dimensions and position on the supero-medial surface of the greater trochanter. It can span a distance of between 25-64% of the anterior-posterior length on the greater trochanter, with 57% attaching more anterior and 43% more posterior(9).
6. Pine et al (2011) studied the insertion point extensively and found that four types of insertion existed and these were classified based on the relationship to the obturator internus(10). The variability in position and breadth of the distal attachment of the PM muscle may influence the validity of the concept known as �inversion of action� (see below).
The other hotly debated issue is the relationship between the PM and the SN. The conclusion is that there are several anatomical variations of the PM and its SN relationship. The sub-types of this variation include(11-13):
Type 1 (A below). Typical pear shape muscle with the nerve running anteriorly and inferiorly to this (in 70%-85% of cases).
Type 2 (B below). The PM is divided into two parts with the common peroneal nerve running between the two parts and the tibial nerve running anterior and below (found in 10-20% of cases).
Type 3 (C below). The peroneal portion loops over the top of the muscle and the tibial portion is below (found in 2-3% of cases).
Type 4 (D below). Undivided nerve passing through the PM (occurs in about 1% of cases).
It is also believed that two other very uncommon variations occur (see E and F below).
Type A is the most common variation, showing the SN passing below the PM
Functional Considerations
The primary functional roles of the PM are;
1. Hip external rotation(15).
2. Abductor at 90 degrees of hip flexion(15).
3. In weight-bearing, the PM restrains the femoral internal rotation during stance phase of walking and running(2).
4. Assists the short hip rotators in compressing the hip joint and stabilising the joint(6).
5. As it can exert an oblique force on the sacrum, it may produce a strong rotary shearing force on the sacroiliac joint (SIJ). This would displace the ipsilateral base of the sacrum anteriorly (forward) and the apex of the sacrum posteriorly(16).
As the PM is the most posterior of the hip external rotators due to its attachment on the anterior surface of the sacrum, it has the greatest leverage to exert a rotation effect on the hip joint. It is often seen clinically that the PM appears to be tight and hypertonic, while the other short hip�rotators that are closer to the axis of rotation become inhibited and hypotonic.
Inversion Of Action
The most contentious issue related to the function of the PM is its �reversal-of- function role� or �inversion of action� role. Many authors have suggested that as the hip approaches angles of 60-90 degrees and greater, the tendon of the PM shifts superiorly on the greater trochanter. As a result, its line of pull renders it ineffective as a hip external rotator; however it does contribute to internal hip rotation. Therefore it reverses its rotation role at high hip flexion angles(15,17,18).
The function of the PM at varying joint angles is an important consideration for the clinician who is evaluating and treating �piriformis syndrome�. Often it has been advocated to stretch the hip into flexion, adduction and external rotation to stretch the PM over the glutes by utilising the �reversal of function� concept.
However, more recent anatomical dissection studies have shown that the attachment of the PM onto the greater trochanter can be variable and in some instances it may insert in a position whereby it is unable to reverse its function, for example in a more posteriorly placed attachment(19). Therefore, stretching the PM into external rotation when the hip is flexed beyond 90 degrees � based upon reversal of function � would be ineffective as a treatment or misleading as an examination technique(19)
MSK Dysfunction & PM Syndrome
Many decades ago, the role that the PM played in creating sciatic-like symptoms was first suggested by Yeoman (1928) when it was considered that some cases of sciatica may originate outside the spine(20). This was supported soon after when Freiberg and Vinkle (1934) successfully cured sciatica by surgically dividing the PM(21). Based on cadaver dissections Beaton and Anson (1938) gave the hypothesis that the spasm of the PM could be responsible for the irritation of the SN(12).
The term �piriformis syndrome� was first coined by Robinson in 1947(22) and was applied to sciatica thought to be caused by an abnormality in the PM (usually traumatic in origin) with emphasis on ruling out more common causes of sciatica such as nerve root impingement from a disc protrusion. It soon became an accepted clinical entity � but with no consensus about the exact clinical signs and diagnostic tests to differentiate it from other sources of sciatica(23,24).
Piriformis syndrome can be defined as a clinical entity whereby the interaction�between the PM and SN may irritate the SN and produce posterior hip pain with distal referral down the posterior thigh, imitating �true sciatica�. Isolating the dysfunction to this region usually follows exclusion of the more common causes of buttock pain and sciatica.
More specifically, complaints of buttock pain with distal referral of symptoms are not unique to the PM. Similar symptoms are prevalent with the more clinically evident lower back pain syndromes and pelvic dysfunctions. Thus, a thorough evaluation of these regions must be performed to exclude underlying pathology(4). It has been suggested that piriformis syndrome� is responsible for 5-6% of cases of sciatica(25,26). In the majority of cases, it occurs in middle-aged patients (mean age 38 yr)(27) and is more prevalent in women(28).
Pathogenesis Of Piriformis Syndrome (PS)
PS may be caused by or relate to three primary causative factors;
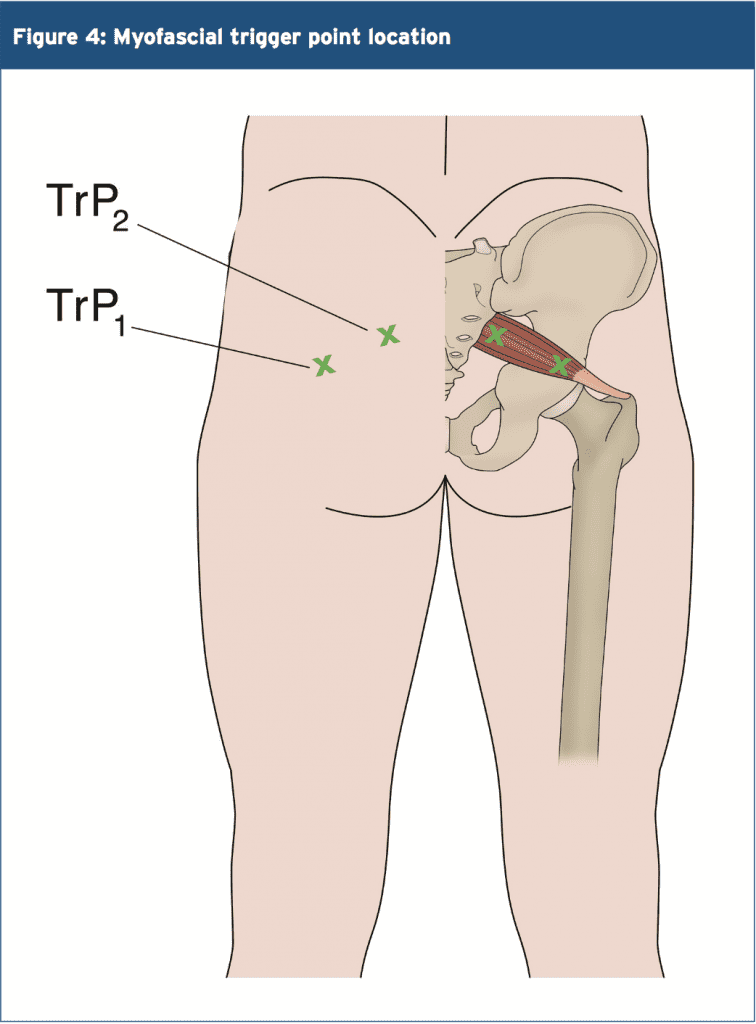
1. Referred pain due to myofascial trigger points (see Figure 4)(2,28-30). Examples include tight and shortened muscle fibres precipitated by muscle overuse such as squat and lunge movements in external rotation, or�direct trauma(16). This increases the girth of the PM during contraction, and this may the source of the compression/entrapment.
2. Entrapment of the nerve against the greater sciatic foramen as it passes through the infrapiriform fossa, or within a variant PM(29,31).
3. SIJ dysfunction causing PM spasm(29,32).
Janvokic (2013) has presented a number of causative factors in PS(29);
1. Gluteal trauma in the sacroiliac or gluteal areas.
2. Anatomical variations.
3. Myofascial trigger points.
4. Hypertrophy of the PM or spasm of the PM.
5. Secondary to spinal surgery such as laminectomy.
6. Space occupying lesions such as neoplasm, bursitis, abscess, myositis. 7. Intragluteal injections.
8. Femoral nailing.
Symptoms
Typical symptoms reported in piriformis syndrome include:
A tight or cramping sensation in the buttock and/or hamstring(33).
Gluteal pain (in 98% of cases)(34).
Calf pain (in 59% of cases)(34).
Aggravation through sitting and squatting(35), especially if the trunk is inclined forward or the leg is crossed over the unaffected leg(36).
Possible peripheral nerve signs such as pain and paraesthesia in the back, groin, buttocks, perineum, back of the thigh (in 82% of cases)(34).
Physical Findings & Examinations
Palpable spasm in and around the PM and obturator internus and external tenderness over the greater sciatic notch (in 59-92% of cases)(34,35). The patient is placed in the Sims position. The piriformis line overlies the superior border of the PM and extends from immediately above the greater trochanter to the cephalic border of the greater sciatic foramen at the sacrum. The line is divided into equal thirds. The fully rendered thumb presses on the point of maximum trigger-point tenderness, which is usually found just lateral to the junction of the middle and last thirds of the line.
Hip flexion with active external rotation or passive internal rotation may exacerbate the symptoms(36).
Positive SLR that is less than 15 degrees the normal side(37).
Positive Freiberg�s sign (in 32-63% of cases)(34,35). This test involves reproducing pain on passive forced internal rotation of the hip in the supine position � thought to result from passive stretching of the PM and pressure on the sciatic nerve at the sacrospinous ligament.
Pacers sign (in 30-74% of cases)(34,35). This test involves reproducing pain and weakness on resisted abduction and external rotation of the thigh in a sitting position.
Pain in a FAIR position(34). This involves the reproduction of pain when the leg is held in flexion, adduction and internal rotation.
An accentuated lumbar lordosis and hip flexor tightness predisposes one to increased compression of the sciatic nerve against the sciatic notch by a shortened piriformis(38).
Electro-diagnostic tests may prove useful (see below).
Investigations
Conventional imaging such as X-ray, CT scan and MRI tend to be ineffective in diagnosing piriformis syndrome.
However, some value may exist in electro- diagnostic testing.
It is beyond the scope of this paper to discuss in detail the process of electro- diagnostic testing; the reader is directed to references for more a more detailed description of how these tests are administered(35,36,39). However the purpose of these tests is to find conduction faults in the SN. Findings such as long-latency potentials (for example the H reflex of the tibial nerve and/or peroneal nerve) may be normal at rest but become delayed in positions where the hip external rotators are tightened(27,36,39).
It is accepted that the tibial division of the SN is usually spared, the inferior gluteal nerve that supplies the gluteus maximus may be affected and the muscle becomes atrophied(40). However testing of the peroneal nerve may provide more conclusive results as is more likely to be the�impinged portion of the SN. The H-wave may become extinct during the painful position of forced adduction-internal rotation of the affected leg(36).
The �Myth� Of Piriformis Syndrome
Stewart 2003 argues that piriformis syndrome is an often over-used term to describe any non-specific gluteal tenderness with radiating leg pain(41). He argues that only in rare cases is the PM implicated in nerve compression of the SN to truly qualify as a piriformis syndrome. He cites only limited evidence and cases where the diagnosis of piriformis syndrome can be made.
1. Compressive damage to the SN by the PM. Stewart cites studies whereby in few isolated studies, the SN was seen to be compressed by the PM in instances such as hypertrophy of the muscle,�usual anatomical anomalies such as a bifid PM, and due to compression by fibrous bands.
2. Trauma and scarring to the PM leading to SN involvement; it is possible that rare cases of true Piriformis Syndrome have been caused by direct heavy trauma to the PM due to a blunt trauma to the muscle. This is termed �post- traumatic PS�.
McCory (2001) supports this argument by stating that it is more likely that (given the anatomical relationship of the PM to the various nerves in the deep gluteal region) the buttock pain represents entrapment of the gluteal nerves, and the hamstring pain entrapment of the posterior cutaneous nerve of the thigh, rather than the SN alone(33). This would explain the clinically observed phenomenon in the absence of distal sciatic neurological signs. Whether the PM is the cause of the compression has not been clearly established. It is possible that the obturator internus/gemelli complex is an alternative cause of neural compression. He suggests using the term �deep gluteal syndrome� rather than piriformis syndrome.
Treatment
When it is believed that a piriformis syndrome exists and the clinician feels that a diagnosis has been made, the treatment will usually depend on the suspected cause. If the PM is tight and in spasm then initially conservative treatment will focus on stretching and massaging the tight muscle to remove the PM as being the source of the pain. If this fails, then the following have been suggested and may be attempted(23,36):
Local anaesthetic block � usually performed by anaesthesiologists who have expertise in pain management and in performing nerve blocks.
Steroid injections into the PM.
Botulinum toxin injections into the PM.
Surgical Neurolysis.
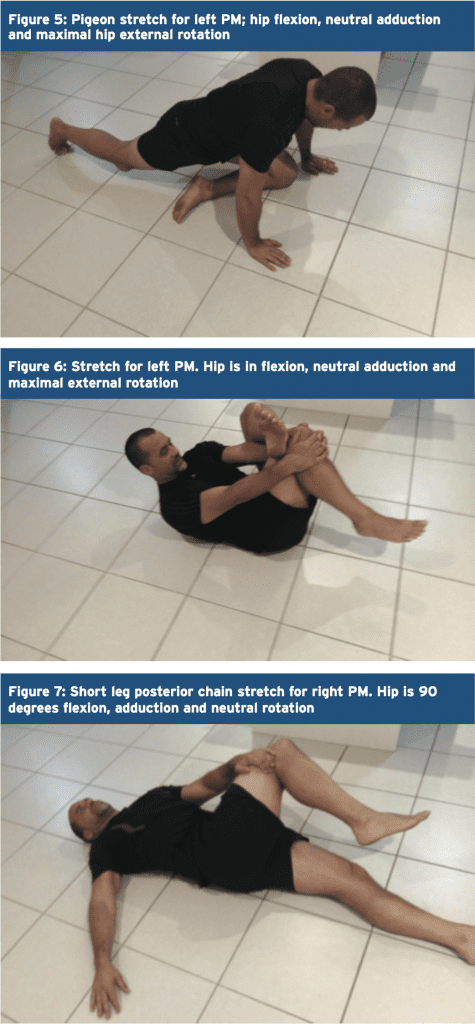
Here, we will focus on therapist-directed interventions such as stretching of the PM and direct trigger point massage. It has always been advocated that PM stretches are done in positions of hip flexion greater than 90 degrees, adduction and external rotation to utilize the �inversion of action� effect of the PM to isolate the stretch to this muscle independent of the other hip external rotators.
However, recent evidence from Waldner (2015) using ultrasound investigation discovered that there was no interaction between hip flexion angle and the thickness of the PM tendon in both internal and lateral hip rotation stretching � suggesting that the PM does not invert its action(19). Furthermore, Pine et al (2011)(9) and Fabrizio et al (2011)(10) in their cadaveric studies found that the PM insertion is a lot more complex and varied than first thought. It is possible that the PM may invert its action only in some subjects but not others.
Therefore, due to the disagreements and confusions over the �inversion of action� concept, it is recommended that the clinician �covers all bases� and performs two variations of a PM stretch � stretches in flexion, adduction and external rotation and stretches in flexion, adduction and internal rotation. Examples of these stretches are given in figures 5-7 below.
Trigger Points & Massage
(see Figure 8)
The best approach to palpate the PM trigger points is in the position suggested by Travel and Simons(2) and this is shown below. In this position, the clinician can feel for the deep PM trigger points and apply a sustained pressure to alleviate the trigger�points � and also apply a flush massage to the muscle in this position.�In this position the large gluteus maximus is relaxed and it is easier to feel the deeper PM.
Summary
The PM is a deep posterior hip muscle that is closely related anatomically to both the sacroiliac joint and the sciatic nerve. It is a hip external rotator at hip flexion angles of neutral to 60 degrees of hip flexion, an abductor when in flexion and also contributes to hip extension.
It has been previously accepted that the PM will �invert its action� or �reverse its function� after 60 degrees of flexion to become a hip internal rotator. However, recent ultrasound and cadaveric studies has found conflicting evidence that this �inversion of action� may in fact not exist.
PM is a muscle that is a dominant hip rotator and stabiliser, and thus has a tendency to shorten and become hypertonic. Therefore, stretching and massage techniques are best utilised to reduce the tone through the muscle. Furthermore, it has also been implicated in compression and irritation of the sciatic nerve � often referred to as piriformis syndrome�.
References
1. Contemp Orthop 6:92-96, 1983.
2. Simons et al (1999) Travell and Simons� Myofascial Pain and Dysfunction. Volume 1 Upper Half of the Body (2nd edition). Williams and Wilkins. Baltimore.
3. Anesthesiology; 98: 1442-8, 2003.
4. Joumal of Athletic Training 27(2); 102-110, 1996.
5. Journal of Clinical and Diagnostic Research. Mar, Vol-8(3): 96-97, 2014.
6. Clemente CD: Gray�s Anatomy of the Human Body, American Ed. 30. Lea & Febiger, Philadelphia, 1985 (pp. 568-571).
7. Med J Malaysia 36:227-229, 1981.
8. J Bone Joint Surg;92-B(9):1317-1324, 2010.
9. J Ortho Sports Phys Ther. 2011;41(1):A84, 2011.
10. Clin Anat;24:70-76, 2011.
11. Med Sci Monit, 2015; 21: 3760-3768, 2015.
12. J Bone Joint Surg Am 1938, 20:686-688,1938.
13. Journal of Clinical and Diagnostic Research. 2014 Aug, Vol-8(8): 7-9, 2014.
14. Peng PH. Piriformis syndrome. In: Peng PH, editor. Ultrasound for Pain Medicine Intervention: A Practical Guide. Volume 2. Pelvic Pain. Philip Peng Educational Series. 1st ed. iBook, CA: Apple Inc.; 2013 .
15. Kapandji IA. The Physiology of Joints. 2nd ed. London: Churchill Livingstone; 1970: 68.
16. J Am Osteopath Assoc 73:799-80 7,1974.
17. J Biomechanics. 1999;32:493-50, 1999.
18. Phys Therap. 66(3):351-361, 1986.
19. Journal of Student Physical Therapy Research. 8(4), Article 2 110-122, 2015.
20. Lancet. 212: 1119-23, 1928.
21. J Bone Joint Surg Am 16:126�136, 1934.
22. Am J Surg 1947, 73:356-358, 1947.
23. J Neurol Sci; 39: 577�83, 2012.
24. Orthop Clin North Am; 35: 65-71, 2004
25. Arch Phys Med Rehabil; 83: 295-301,2002.
26. Arch Neurol. 63: 1469�72, 2006.
27. J Bone Joint Surg Am; 81: 941-9,1999.
28. Postgrad Med 58:107-113, 1975.
29. Can J Anesth/J Can Anesth;60:1003�1012, 2013.
30. Arch Phys Med Rehabil 69:784, 1988.
31. Muscle Nerve; 40: 10-8, 2009.
32. J Orthop Sports Phys Ther;40(2):103-111, 2010.
33. Br J Sports Med;35:209�211, 2001.
34. Man Ther 2006; 10: 159-69, 2006.
35. Eur Spine J. 19:2095�2109, 2010.
36. Journal of Orthopaedic Surgery and Research, 5:3, 2010.
37. Muscle & Nerve. November. 646-649, 2003.
38. Kopell H, Thomnpson W. Peripheral Entrapment Neuropathies. Huntington, NY: Krieger, 1975:66.
39. Arch Phys Med Rehabil;73:359�64, 1992.
40. J Bone and Joint Surg, 74-A:1553-1559, 1992.
41. Muscle & Nerve. November. 644-646, 2003
Many people suffer from lower back pain that spreads downward to the limbs and feet. This can often be alleviated by doing a deep piriformis stretch � a stretch that releases tight piriformis muscles, and relaxes the sciatic nerve.
Constriction of the piriformis muscle can irritate the sciatic nerve because they lay in close proximity to each other. By irritating the sciatic nerve, the result is pain (either in the lower back or thigh), numbness and tingling along the back of the leg and into the foot.
What Is The Piriformis?
The piriformis muscle is a small muscle located deep in the buttock, behind the gluteus maximus. It connects the spine to the top of the femur and allows incredible flexibility in the hip region (it�s the main muscle that allows for outward movement of the hip, upper leg and foot from the body).
The sciatic nerve passes underneath this muscle on its route to the posterior thigh. However, in some individuals, the sciatic nerve can actually pass right through the muscle, leading to sciatica symptoms caused by a condition known as piriformis syndrome.
Unfortunately, for a lot of individuals, their sciatic nerve passes through the piriformis muscle, leaving them with pain that just won�t go away (as well as poor mobility and balance).
Causes Of Piriformis Syndrome
The exact causes of piriformis syndrome are unknown. The truth is, is that many medical professionals can�t determine a cause, so they cannot really diagnose it. Even with modern imaging techniques, the piriformis is difficult to identify.
Lower back pain caused by an impinged piriformis muscle accounts for 6-8% of those experiencing back pain (1).
Suspected causes of piriformis syndrome include (2):
� Tightening of the muscle, in response to injury or spasm � Swelling of the piriformis muscle, due to injury or spasm � Irritation in the piriformis muscle itself � Irritation of a nearby structure such as the sacroiliac joint or hip � Bleeding in the area of the piriformis muscle
Any one of the above can affect the piriformis muscle, as well as the adjacent sciatic nerve.
Also, a misaligned or inflamed piriformis can cause difficult and pain while sitting and when changing positions (from sitting to standing). I actually stretched too far in a yoga pose once, and irritated my piriformis muscle � this took about 1-2 years to fully heal. I had major pain while sitting, and when changing positions from sitting to standing. I remember it being a huge pain in the butt (pardon the bun), but I just stuck with stretching and trigger point release and eventually it went away.
It is important to note, too, that over-stretching can actually make the condition worse. Light, gentle stretching is best. �No pain, no gain� does NOT apply here. I over-stretched my piriformis and that�s what made it inflamed for 1-2 years (because I was still doing yoga daily, and over-doing it in stretches).
Make sure you warm up your muscles before you stretch, because you can create a different injury. To warm up, simply walk or march in place or climb up and down a flight of stairs slowly for a few minutes before stretching.
Exercising and stretching the piriformis is well worth it � try it now with these 10 stretches:
1. Supine Piriformis Stretch
1. Lie on your back with your legs flat.
2. Pull the affected leg toward the chest, holding the knee with the hand on the same side of the body and grabbing the ankle with the other hand.
3. Pull the knee towards the opposite shoulder�until stretch is felt.
4. Hold for 30 seconds, then slowly return to starting position.
There are many variations of this stretch, but here is a good video to demonstrate:
2. Standing Piriformis Stretch
1. If you have trouble balancing, stand with your back against a wall, and walk your feet forward 24 inches. Position your knees over your ankles, then lower your hips 45 degrees toward the floor.
2. Lift your right foot off the ground and place the outside of your right ankle on your left knee.
3. Lean forward and lower your chest toward your knees while keeping your back straight. 4. Stop when you feel the glute stretch. 5. Hold for 30-60 seconds, then switch legs and do the same.
3. Outer Hip Piriformis Stretch
1. Lie on your back and bend the right knee.
2. Use the left hand to pull the knee over to the left side. Keep your back on the ground, and as you do so, you should feel the stretch in the hip and buttocks.
3. Hold for 20-30 seconds, and repeat on the other side.
�4. Long Adductor (Groin) Stretch
1. Sitting on the floor, stretch your legs straight out, as far apart as you can.
2. Tilt your upper body slightly forward at the hips and place your hands next to each other on the floor.
3. Lean forward and drop your elbows to the floor if you can. You will feel the pelvis stretching.
4. Hold for 10-20 seconds, and release.
5. Short Adductor (Inner Thigh) Stretch
1. For this exercise, sit on the floor and put the soles of your feet together.
2. Use your elbows to apply downward pressure to your knees to increase the stretch.
3. You should feel the stretch on the inner thighs. For a deeper stretch, bend your upper torso forward with a straight back.
4. Hold for 30 seconds, release, and flutter your legs in the same position for 30 seconds.
6. Side Lying Clam Exercise
1. Lay on your side with the hip that needs help on top.
2. Bend your knees and position them forward so that your feet are in line with your spine. 3. Make sure your top hip is directly on top of the other and your back is straight.
4. Keeping your ankles together, raise the top knee away from the bottom one. Do not move your back or tilt your pelvis while doing so, otherwise the movement is not coming from your hip.
5. Slowly return the knee to the starting position. Repeat 15 times.
7. Hip Extension Exercise
1. Position yourself on all fours with your shoulders directly over your hands. Shift your weight a little off the leg to be worked.
2. Keeping the knee bent, raise the knee off the floor so that the sole of the foot moves towards the ceiling.
3. Slowly lower the leg, almost back to the starting position and repeat 15 times.
8. Supine Piriformis Side Stretch
1. Lie on the floor with the legs flat, and raise the affected leg by placing that foot on the floor outside the opposite knee.
2. Pull the knee of the bent leg directly across the midline of the body using the opposite hand or towel until a stretch is felt. Do not force anything and be gentle.
3. Hold the piriformis stretch for 30 seconds, then return to starting position and switch legs.
4. Aim for a total of 3 repetitions.
9. Buttocks Stretch for the Piriformis Muscle
1. Laying with your stomach on the ground, place the affected foot across and underneath the trunk of the body so that the affected knee is on the outside.
2. Extend the non-affected leg straight back behind the body and keep the pelvis straight. 3. Keeping the affected leg in place, move your hips back toward the floor and lean forward on the forearms until a deep stretch it felt.
4. Hold for 30 seconds, and then slowly return to starting position. Aim for a total of 3 stretches.
10. Seated Stretch
1. In seated position, cross your right leg over your left knee.
2. Bend slightly forward, making sure to keep your back straight.
3. Hold for 3-60 seconds and repeat on the other side.
According to Myofascial Pain and Dysfunction: The Trigger Point Manual, written by doctors Janet Travell and David Simons, myofascial trigger points (tiny knot contractions) in overworked gluteus minimus and piriformis muscles in the buttocks are the main cause of sciatica and all the symptoms that come with it.
Picking up a copy of the book, or even following instruction in the video below can help release these knot contractions.
Doctor of Chiropractic, Dr. Alexander Jimenez looks at high heels at what they do to the back.
Ladies, ever wonder why you suffer from regular bouts of lower back pain?� Achy hips?� How about crazy tight leg muscles?� Don�t blame it on your cycling class, or too many squats or, the trainer you only see once or twice a week.� Look down.� Are you wearing high heels?� Bingo!� You�ve heard high heels are bad for you.� But it�s not just because they cause all kinds of pain and trauma to your feet.� High heels are also messing up your physical fitness. �They throw you out of proper postural alignment causing your joints and spine to take on more�wear and tear, which means aches and pains.
Is it possible to still look rockin� and save your joints? �My suggestion is more Athleisure-wear. �I know some fashion hard-liners say, no way will I walk around in yoga pants on a weekday!� But we�ve come a long way since those flare-leg, fold-over yoga pants.
Let�s chat for a moment about the evils of high heels.
First there�s the obvious.� They make your feet hurt.� Blisters, calluses and swelling are par for the course.� And pointy toes, fuhgeddaboutit!� I�m sure they were invented by someone on the Marquis de Sade�s payroll.� Second, they can lead to foot injuries like plantar fasciitis (usually from a bone spur that makes your heels hurt), hammertoes, bunions, and neuromas.� �Then there�s the domino effect.
Not only do high heels make your feet hurt, but problems with the feet can travel up the leg and cause injuries in the back, knees and hips. �Your knees take on extra pressure from the weight being pushed forward onto the balls of the feet. �Walking in this position makes your hip flexors and calf muscles short and tight. �And it doesn�t stop there.� Back problems are incredibly common in women who don�t give up their high heels.
Back Problems are incredibly common in women who don�t give up their high heels
Here�s why:
ext”>
Postural changes:�The S-curve of your spine has cushiony discs in between the vertebrae that act as a shock absorbers to protect them from stress. Like when you�re bending or jumping. �Wearing heels causes the lower back to arch more than normal because the body weight is pushed forward.� To compensate, the upper body has to lean back to maintain balance.� This puts extra stress on the discs. ��Spending hours with your body in funky alignment can lead to muscle spasms and back pain. �Tight hamstring muscles, which�attach to back of the pelvis and lower back, can also make your back ache.
Anatomical changes: Wearing high heels on a daily, or very regular basis, over years, can actually cause anatomical changes to your body.� In addition to the extra strain on your back and knees, the calf muscles can also shorten and the tendons can get tighter and thicker.
And It Can Get Even Nastier If You Get One Of These Spine Injuries:
Spondylolisthesis: it�s a mouthful, but is a common injury that can happen in the lower back from too much hyperextension (arching the back).� It�s when one vertebra slips forward over another.
Foraminal stenosis: I have this one congenitally and it sucks. This is a spine and nerve issue that occurs when anatomical abnormalities reduce the spaces the nerves travel through as they exit the spinal column.� The spaces are called foramina, and when they get blocked, the nerves get squeezed.� The pain can radiate through the buttocks and down the legs.� Symptoms are shooting pains, numbness, tingling, muscle weakness, spasms and, or cramping.
Sciatica:�The sciatic nerve is the longest one in the body. �It runs from the bottom of the lumbar spine all the ways down the legs. �When the sciatic nerve gets compressed it causes radiating pain, tingling, numbness and muscle weakness down the leg and can The pain can travel all the way to the bottom of the foot.
What Can You Do? �My Case for Athleisure-Wear To Combat Back Pain
It�s time for stuffy office attire to retire. �Comfy clothes and flat shoes can be very chic. �Have you seen the boards on Pinterest?� Thanks to this hopefully permanent fashion style, my jeans and heels spend more time in my closet than on my body.� Leggings and cute kicks are my go to�s.� Night out?� No prob.� I reach for my sleek workout leggings, a ruched top or off the shoulder top with some high heel sneaks (they�re wedges so not nearly as bad for you). �I also discovered these by Bluprint which I put to the test at 2 huge conventions where I walking and standing for hours on end.� The soles made of memory foam � like those beds!
My podiatrist friend, Steven Rosenberg, DPM has been preaching the need for comfy shoes to his female clients for years. �(Fortunately for his practice, not everyone listens!) �Dr. Steve says, wearing shoes designed more for comfort can help you live more pain-free. ��Because comfort shoes are made of�soft cushiony materials�with soft foam innersoles, those are what you should turn to for shopping, walking or standing for long periods of time to avoid�blisters, muscle spasms or arch cramps.� � He also says to check for arch support in your shoes. �If there�s none, you can buy ones to put inside.
Even after reading this, you may still not be willing to give up high heels for good. �Me either.� I still get glammed up once in a while.
Here Are Some Tips For When You Must:
Wear them for as little time as possible.
Try to opt for heels around 2� high
Steer clear of pointy toes.
Buy shoes with leather insoles to so your foot doesn�t slide.
Buy arch inserts or use orthotics to support your arches.
Vary your footwear so you�re not wearing high heels every day.
Gradual or lower slopes are a little better, go for platforms or wedges instead of stilettos
Thicker heels are better than spiky heels
Stretch and strengthen the overworked muscles.
Here�s How:
Stretch your leg muscles and hip flexors before and after wearing heels.� For the calves, stand on a step and let one heel hang down until you feel a stretch.
Try this convenient device, the foot rocker by Vive.� It stretches the calf and the sole of the foot relieving pain from plantar fasciitis.
Front of the hip and thigh stretch for before and after wearing high heels
Hamstring stretch for before and after wearing high heels
Massage and stretch the muscles in the soles of your feet.� Roll your foot on a golf ball before and after wearing heels and, get regular foot massages.
Strengthen and increase the range of motion in your ankles and feet.� Put a rag on the floor.� Using your foot, write the letters of the alphabet.� Also put a bunch of marbles on the floor.� Pick one or a few of them up using just your foot.� Put them down about 6 inches away without lifting your foot off the floor.� Try that 10 times.� If you don�t have marbles, you can do it with a hand towel.
So next time you�re shopping for shoes, think about your foot fitness first. �Look for fashion that keeps you closer to the ground and that will hopefully keep you farther away from the doctor.
Injuries to the muscles and ligaments around the hip affect both competitive and recreational athletes. These injuries can interfere significantly with sports enjoyment and performance levels, and they occasionally will end participation completely. Excessive pronation and poor shock absorption have been found to be an underlying cause or a contributing factor for many leg injuries. Functional orthotics which have been custom-fitted to improve the biomechanics of the feet and reduce the extent of pronation can help to prevent many sport-related leg injuries.
Lower Extremity Problems in Athletes
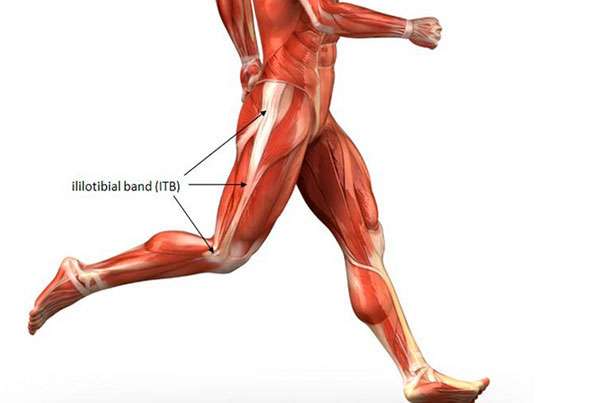
One study looked at the foot biomechanics of athletes who reported a recent foot or leg injury and compared them to an uninjured control group. The researchers determined that those athletes with more foot pronation had a much greater statistical probability of sustaining one of five leg injuries, including iliotibial band syndrome (which is due to excessive tightness of the hip abductor muscles).
This study helps us understand how providing appropriate functional foot orthotic support to patients who are involved in sports or recreational activities lowers their likelihood of developing both traumatic and overuse hip injuries.
In this paper, sixty-six injured athletes who ran at least once a week, and who had no history of traumatic or metabolic factors, were the study group. Another control group of 216 athletes were matched who did not have any symptoms of lower extremity injuries. The amount of pronation during standing and while running at �regular speed� was determined by measuring the angles of their footprints. The investigators found a significant correlation: Those athletes with more pronation had a much greater likelihood of having sustained one of the overuse athletic injuries.
Hip and Thigh Injuries
Many injuries experienced at the hip develop from poor biomechanics and gait asymmetry, especially when running. Smooth coordination of the muscles that provide balance and support for the pelvis is needed for optimum bipedal sports performance. This includes the hamstring muscles and the hip abductor muscles, especially the tensor fascia lata (the iliotibial band). When there is a biomechanical deficit from the feet and ankles, abnormal motions (such as excessive internal rotation of the entire leg) will predispose to pulls and strains of these important support muscles. The hamstrings (comprised of the biceps femoris, semimembranosus, and semitendinosus muscles) are a good example.
During running, the hamstrings are most active during the last 25% of the swing phase, and the first 50% of the stance phase. This initial 50% of stance phase consists of heel strike and maximum pronation. The hamstring muscles function to control the knee and ankle at heel strike and to help absorb some of the impact. A recent study has shown a significant decrease in electromyographic activity in the hamstrings when wearing orthotics. In fact, these investigators found that the biceps femoris (which is the most frequently injured of the three hamstring muscles) had the greatest decrease in activity of all muscles tested, including the tibialis anterior, the medial gastrocnemius, and the medial and lateral vastus muscles. The scientists in this study theorized that the additional support from the orthotics helped the hamstrings to control the position of the calcaneus and knee, so there was much less stress into the hip joint and pelvis.
Excessive Pronation and Hip Injuries
Using functional orthotics to correct excessive pronation and to treat hip problems requires an awareness of the various problems that can develop. The following is a list of the pathologies that are seen in the hip and pelvis secondary to pronation and foot hypermobility:
Iliotibial band syndrome����������������� Tensor fascia lata strain
Trochanteric bursitis����������������������� Hip flexor muscle strain
Piriformis muscle strain������������������ Hip adductor muscle strain
Hip joint capsulitis��������������������������� Anterior pelvic tilt
These conditions will develop much more easily in athletes, who push their musculoskeletal systems, and who seek more efficient and effective functional performances.
In 2002, researchers at Logan College of Chiropractic recruited a total of 40 male subjects that demonstrated bilateral pes planus or hyperpronation syndrome. Subjects were cast for custom made orthotics; their right and left Q-angles were measured with and without the orthotic in place. Thirty-nine of 40 test subjects showed reduced Q-angle, which was in the direction of correction, suggesting that wearing orthotics can improve stability and levelness of the pelvis, thus protecting the body to some degree from hip injury.
Conclusion
Excessive pronation and/or poor shock absorption have been shown to be an associated or causative factor in many leg injuries � from the foot itself, up the lower leg to the knee, thigh, and into the hip joint. The good news is that many of these conditions can be prevented with custom-fitted functional orthotics. Evaluation of foot biomechanics is a good idea in all patients, but is especially necessary for those who are recreationally active, or for anyone who has experienced hip problems.
To avoid potentially disabling hip injuries, competitive athletes must have regular evaluations of the alignment and function of their feet. Additional preventive measures include wearing well-designed and solidly-constructed shoes. When athletes are provided with custom-fitted functional orthotics, it can help prevent arch breakdown and biomechanical foot problems, and also treat numerous injuries of the lower extremities, including the hip joints.
Many injuries experienced at the hip develop from poor biomechanics and gait asymmetry, especially when running. Smooth coordination of the muscles that provide balance and support for the pelvis is needed for optimum bipedal sports performance. For Answers to any questions you may have please call Dr. Jimenez at 915-850-0900
Most people don�t go to a chiropractor for a better sex life, but that extra benefits is a pretty happy accident. �People come in with back pain, but after adjustments, they come back and tell me their sex life is so much better,� says Jason Helfrich, co-founder and CEO of 100% Chiropractic. �It�s no surprise to us�it�s amazing what the body will do when you take away the pressure on the nervous system.�
And what are those amazing feats, exactly?
Let�s start with what a chiropractor really does. Every function in your body is controlled from the nervous system, but when vertebra are off position�known as a subluxation�the nerves traveling between your brain and your muscles can become blocked, compromising your body�s ability to function as it needs to. Every chiropractor�s goal is to remove these subluxations, since they can both cause pain and impede feeling, Helfrich says.
But these fixes help more than just back pain. The lumbar region (your lower back) is a huge hub for the nerves that extend into your reproductive regions. Removing lumbar subluxations can improve nerve flow to your sexual organs, increasing things like blood flow to your clitoris or, for your husband, the penis.
The flow of nerve signals is a two-way street, though, meaning that adjustments also allow your organs to send messages to the brain more easily. This means that you not only do you become physically aroused faster, but your brain also registers that ready-for-action, heightened sense of pleasure more quickly, so you move past the mental obstacles that may be keeping you from orgasming, Helfrich explains.
The other key adjustment area for a better sex life?
Right below your brain stem, around the vertebrae known as C1 and C2. �Libido and fertility require a delicate balance of estrogen, progesterone, and other hormones, many of which are released in the upper cervical and neck area,� he explains. If there are any blockages right out of the brain, the impingement up there will have an effect all the way down.
Even your fertility is affected by the nerves and hormones coming out of the spine, as they control your reproductive cycle.
But beyond all of the physiological benefits of tweaking your spine to perfection, chiropractic adjustments can also simply give your muscles more range of motion. This means you can try previously impossible positions under the sheets.
�We want to improve people�s health, and health is about living life as its intended. Having a great sex life is huge part of that,� Helfrich adds. No arguments here!
Most people don�t go to a chiropractor for a better sex life, but the extra benefit is a pretty happy accident. �People come in with back pain, but after an adjustment, they come back and tell me their sex life is so much better.�
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Variants
Variants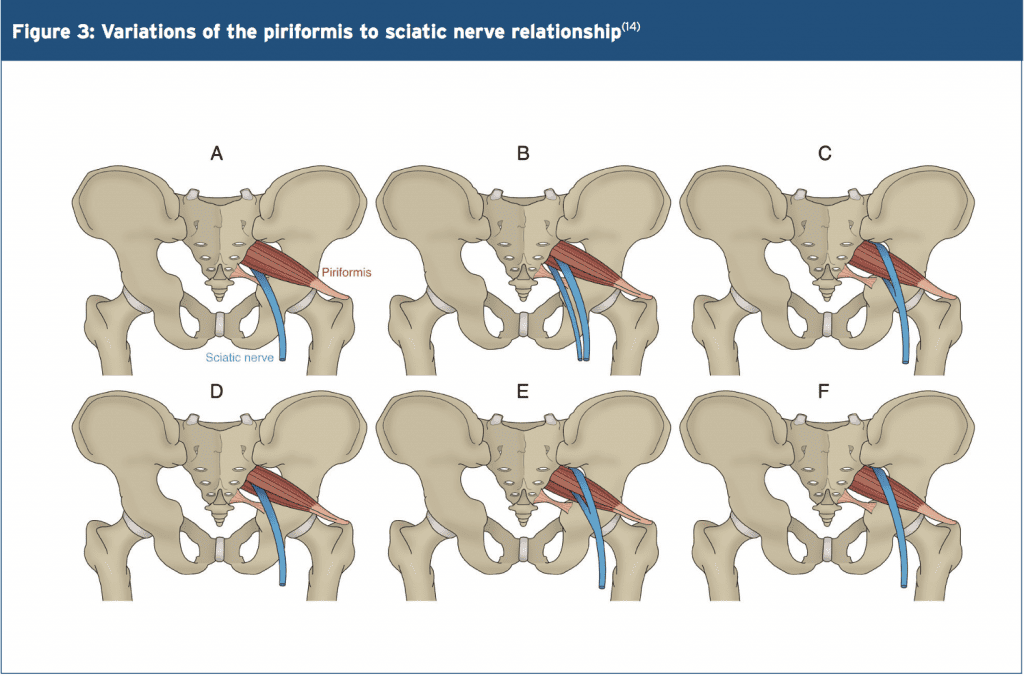
 Trigger Points & Massage
Trigger Points & Massage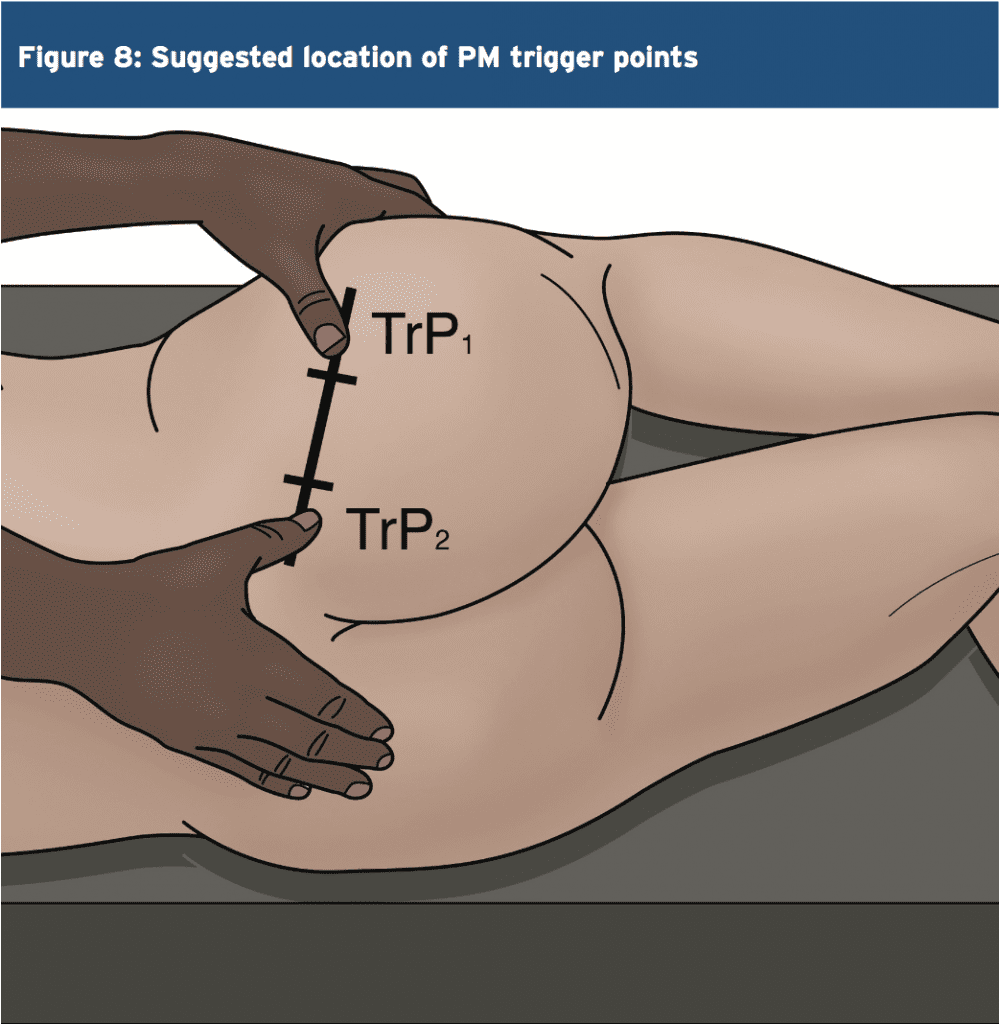













 Most people don�t go to a
Most people don�t go to a